
Abstract
Background
According to GLOBOCAN 2020 Breast cancer is the most common cancer among women and the prevalence is increasing worldwide and in Ethiopia. This review assessed studies conducted in Ethiopia on the clinical features and epidemiology of breast cancer.
Methods
Data base search conducted PubMed, Google Scholar African Journals Online (AJOL), Cumulative Index of Nursing and Allied Health Literature (CINAHL) and Hinari without time restrictions. The search keywords included; prevalence and pattern, clinical presentation, histological and molecular subtypes, and management. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline to identify, search, extract articles, and report this systematic review. The protocol was registered in PROSPERO, ID: CRD42023403320.
Results
Twenty studies were included in the review with 33,369 participants and 3 were community-based and 17 were hospital-based. In all except two reviewed studies, breast cancer is the most common cancer among women of Ethiopia. The most frequent presenting symptom was a breast lump/mass and commonly affected side was right breast. Most patients presented at a late stage and they were premenopausal age group. The commonest histology type is ductal carcinoma, that the most prevalent receptor was estrogen receptor positive, and the most common molecular subtype was Luminal A in pathology samples. Surgery is main stay of treatment and the most common surgical technique practiced in Ethiopia is modified radical mastectomy.
Conclusion
Breast cancer incidence is rising, and it accounts for the major cancer burden in the country. There is a need for additional awareness-raising and health education because delayed presentation are critical problems throughout Ethiopia. For planning and monitoring cancer patterns, comprehensive demographic and clinical data from a population or facility-based registry are needed in the regions. The available treatment options are still limited in Ethiopia it needs infrastructural development.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The World Health Organization (WHO) report shows that in 2020, 2.3 million women were diagnosed with breast cancer, making it the most common cancer with 685,000 deaths worldwide. It continues to cause more disability-adjusted life years (DALYs) in women worldwide than any other cancer. Deaths from breast cancer are high in African countries due to poor health infrastructure, poor vital records, delayed health-seeking behavior, and low community awareness [1].
Breast cancer incidence and mortality rates in the world have increased over the last three decades. Study done on Breast cancer incidence and mortality from 1990 to 2016. In 60 out of 102 countries, the incidence of breast cancer has more than doubled, while the death rate has doubled in 43 out of 102 countries [2]. By 2030, it is predicted that there will be 2.7 million new cases worldwide each year and 0.87 million deaths from breast cancer [3].
A country assessment showed that breast cancer is the most common cancer illness in Ethiopia, accounting for 16,133 (20.9%) of all cancer cases and 9,061 (17.5%) of all cancer-related deaths [4]. Approximately 80% of breast cancer cases in sub-Saharan Africa are detected at late stages (stage III or IV), compared to 15% in high-income countries [5].
Breast cancer arises from the epithelium lining the milk ducts, known as invasive ductal carcinoma. This is the most common subgroup (50–80%), followed by the group arising from the glandular tissue of the breast lobules [6]. Based on mRNA gene expression levels, breast cancer can be classified into molecular subgroups. The four main intrinsic subtypes of breast cancer (Luminal A, Luminal B, HER2-enriched, and basal-like). Regarding Hormone status of breast cancers ER-positive tumors account for almost 70% of all breast cancers in Western populations [7, 8]. The TNM system for cancer staging refers to the classification of a tumor based on a list of factors, including the degree of disease affecting the main tumor (Tis to T4), regional lymph node status (N0 to N3), and distant metastases (M0 or M1) (0 to IV) [9].
When choosing a treatment plan, the type of breast cancer and its stage are often considered. Patients with breast cancer are often given several types of treatment. The current choices are radiation therapy, surgery, chemotherapy, hormonal therapy, biological therapy, and chemotherapy [10]. According to studies from underdeveloped countries, stage I and stage II have five-year survival rates of 90% and 65%, respectively, while stage III and stage IV have rates of only 33% and 6%, respectively [11].
Until April 2022, the Tikur Anbesa Specialized Hospital (TASH) was the only center in the country that offered radiotherapy. As of April 2022, Ethiopia has two additional functional radiation therapy centers: Jimma University Medical Center (JUMC) in the southwest of the country and Hiwot Fana Specialized Hospital at Haramaya University in the eastern part of the country.
Rationale of the study
Based on a preliminary search, we couldn’t find compressive evidence at the country level regarding breast cancer patients’ epidemiology and clinical profile. Therefore, a thorough examination of the existing evidence on breast cancer would aid in understanding breast cancer epidemiology and clinical profile in the country. This review provides evidence for the development of future strategies that are especially suited to the Ethiopian population.
Study objective
This study aimed to generate country wide evidence on epidemiology and clinical characteristics of breast cancer in Ethiopia.
Methods
The PROSPERO international prospective register of systematic review database checked for already-done or ongoing systematic reviews with the same objective before the data collection process started. The protocol of this review is registered in ID: CRD42023403320. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline to identify, search, extract articles, and report this systematic review [12].
Search strategy
The electronic databases and search engines PubMed, Google Scholar African Journals Online, Cumulative Index of Nursing and Allied Health Literature and Hinari were searched until June 20, 2023. The MeSH terms and key words were as follows: breast cancer, breast neoplasm, prevalence, epidemiology, Sign, Symptom Presentation, histology, molecular subtype, and management of breast cancer. The MeSH keywords were combined using Boolean operators (AND/OR), and Ethiopia’s name was appended at the end. To enhance the number of articles included and lower the number of missing articles, hand searching was done on the citations and references listed in the eligible articles ( Tables 1 and 2).
Eligibility criteria
Selection of study and extraction
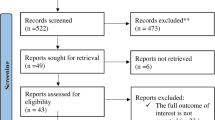
As shown in the PRISMA flowchart, all articles identified from the electronic database searches were imported into Zotero and Duplicates were removed. Further Exclusion of articles conducted using title and abstract screening. Articles with full text were assessed for eligibility and further full text exclusion done on those articles which do not have a clearly written result. FGD and BTT extracted data simultaneously and independently, and any disagreements were resolved after independent review by the TGD and YDS. Finally, we extracted relevant information from each literature using an Excel spreadsheet template to avoid missing important information when preparing the results of the review or for future cross-checking. The extracted data includes first author’s name, year of publication, study design, location, prevalence and pattern, Presenting Symptom, Stage at presentation, Histology findings, Molecular Features and Treatment.

PRISMA flowchart for article Search and Selection Process
Data analysis
The extracted data were further categorized into institution-based and community-based according to the setting in which the studies took place and further sorted according to the institution in which the studies were conducted. The methodological quality of the included studies was assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist [13].
Results
Study selection and characteristics
A total of 352 articles were found from electronic data base searching on the search engines and databases. All of these search results exported to Zotero computer software, where 140 duplicate records were removed and 149 were removed after being screened based on title and abstract. Further 43 articles were removed based on an objective of the review. Finally, 20 eligible articles, which enrolled 33,369 participants, were included in the systematic review (Fig. 1).
Most of the studies were conducted in Tikur Anbesa specialized hospital (TASH)(6/20), which was only hospital with radiotherapy treatment in the country until April 2022. Articles based on the study setting: 3 (15%) articles were community-based, and 17 (85%) articles were hospital-based. Based on study design, 9 (45%) articles were cross-sectional, 10 (50%) retrospective chart reviews, and one retrospective cohort.
Prevalence and pattern
Five studies assessed the prevalence and pattern of breast cancer in the country. All hospital-based studies showed the prevalence of breast cancer compared to other cancers. Breast cancer accounts for 15.2–26% of all cancers [14, 15] and from female cancer 29.3–37% [11, 16].
A community-based study done using the Addis Ababa City Cancer Registry (AACCR) showed the incidence of breast cancer (2012–2013) to be 31.5% of all female cancers [17] and a study done during 2012–2015 from AACCR and six regions showed breast cancer constituted 33% of all cancers in women and 23% of all cancers [18].
According to a study done at Hawassa University Comprehensive Specialized Hospital (HUCSH) from 2013 to 2019, the number of women diagnosed with breast cancer in hospitals has increased from 69 (12.3%) In 2013, 106 (19%) in 2019 [19].
A study from Gondar University Comprehensive Specialized Hospital (GUCSH), showed breast cancer accounts for 76 (14.1%) of all cancers [15] and finding from TASH showed breast cancer accounts for 26% of female cancers [14].
A study conducted at St. Paul’s Hospital Millennium Medical College (SPHMMC), of all malignancies, breast cancer accounted for 587 (29.3%) in 2019, making it the second most common disease after cervical CA [16].
Presenting symptom
Fourteen studies reported Age at diagnosis. The median age ranges 38-55.8 years [19, 20] and mean age ranges 42.1–47.5 years [16, 21].
Premenopausal patients represent the majority of female breast cancer patients at the time of diagnosis, with the median age being between 40 and 46 years (14,15,17,19,23,2829). Breast lumps or masses were the most common presenting symptoms in all studies, followed by breast pain and ulceration [20, 22,23,24,25]. A study conducted at the GUCSH, where 65 (79%) patients presented with breast mass and breast ulceration in 15 patients (18%) [26].
Similar findings from two university hospitals (Gondar and Felege Hiwot University Comprehensive Specialized Hospital) (GUCSH and FHCSH) revealed that breast lump or mass was the most common presentable symptom in 328 (88.4%), followed by painful wound in 161 (43.4%) [22].
A study at Dessie Referral Hospital (DRH) showed 117 (57.4%) patients presented with breast lumps, followed by breast pain in 70 (34.3%) [25]. A multicenter study in Addis Ababa showed that breast lumps were found in 344 (78.0%) patients, followed by pain in 53 (10.2%) patients [24].
Regarding lymph node involvement, the findings from GUCSH and FHCSH showed that (320, 86.3%) and DRH 30, (14.7%), had a lymph node involvement at presentation [22, 25]. According to studies done at the GUCSH and TASH, breast CA commonly affects the right breast 48 (59%), and, 160 (38.4%) respectively (26, 19 and 27)and unlike others finding from HUCSH showed left breast in is commonly affected 302 (54%), and the upper outer quadrant was the most commonly involved according to the findings from TASH 154 (78.2%) ,40 (9.6%) [27, 28].
Stage at presentation
Nine studies included stage at presentation. Eight studies showed most of the patients presented in late stages (stage III and stage IV), and the prevalence of advanced stages ranges from 57 to 71.2% in (22, 19, 29, and 25). This was shown in a study conducted in GUCSH and FHCSH, in which 53 (14.3%) patients were diagnosed at stage IV and 211 (56.9%) patients were diagnosed at stage III [22]. According to HUCSH findings, 24 (12.2%) were diagnosed with stage IV disease, 113 (57.4%) with stage III disease, and 160 (30.4%) with early-stage disease [19].
Findings from DRH showed 82 (40.2%) and 53 (25.5%) were diagnosed with stage IV and stage III, and early stage presentation was 69 (33.8%) [27]. TASH stages at diagnosis: 74 (57%) were diagnosed at stages III and IV. Stage III: 63 (48.5%); Stage IV: 11 (8.5%) [29].
Unlike the previous papers, a finding from the TASH showed that the majority of patients 56(59%) of patients presented with early and late stages accounted for 40(41%) [30].
Histology findings
Nine studies included histologic findings and in all reviewed studies, ductal carcinoma is the most prevalent histology type. The prevalence of ductal carcinoma in studies done in SPHMMC, (GUCSH and FHCSH), GUCSH, and HUCSH studies was 479 (81.6%), 347 (93.5%), 61 (74%), and 156 (79.2), respectively [16, 22, 26, 28]. Out of nine studies 5 studies were from TASH. Ductal carcinoma is the most common histology type in TASH, followed by lobular carcinoma, with a prevalence ranging from 55.3 to 83.7% [20, 27, 29,30,31].
Regarding the level of differentiation, studies conducted in TASH and HUCSH, showed that moderate differentiation carcinoma is the commonest type (177 (31.7%) and 91 (46.2%), followed by poor differentiation (155 (27.7%) and 72 (36.5%), respectively [28, 31]. Unlike the previous study findings, those from northern Ethiopia (GUCSH and FHCSH) and GUCSH showed that poor differentiation was the most common among types 140 (45.6%) and 30 (37%), followed by moderate differentiation in patients 79 (40.7%) and 14 (17%), respectively [22, 26].
Molecular features
Two studies from TASH looked at the prevalence of hormone receptors and molecular subtypes. Both papers showed that the most prevalent receptor was estrogen receptor positive, and the most common molecular subtype was Luminal A in pathology samples. In a study from TASH in 2018, the prevalence of estrogen receptor positivity was 74 (65%), progesterone receptor positivity was 49 (43%), and HER2 positivity was 26 (23%). Regarding molecular subtype, the prevalence of Luminal A (ER + and/or PR+, HER2-) was 45 (40%), Luminal B (ER + and/or PR+, HER2+) was 30 (26%), HER2-enriched (ER-, PR-, HER2+) was 11 (10%), and Triple Negative/Basal like (ER-, PR-, HER2-) was 26 (23%) [30]. In a similar study from the same institution (2017), 137 biopsies were found to be ER+ (65.5%), PR+ (58%), and HER2 positive (28%) in a study, and the prevalence of molecular subtypes was shown to be Luminal A (54%), Luminal B (22%), HER2-enriched (6%), and Triple 29 Negative/Basal-like (18%) [29].
Treatment
Studies included in this review Reported modalities of treatment, including surgery, chemotherapy, radiotherapy, and hormonal therapy. Surgery remain the mainstay of management in many settings in Ethiopia, and the most prevalent surgical technique was modified radical mastectomy (MRM) [19, 22, 25].
Finding from GUCSH showed, surgery was done for all 82 patients of which 51 (62%) of patients underwent MRM, and 79 (96%) received chemotherapy. The commonest chemotherapy regimen is Adriamycin and Cyclophosphamide (AC). Hormonal treatment given to 60 (73%) and Tamoxifen 18 (22%) was the commonest type [26].
Surgery was performed in 357 (96.2%) patients by two university hospitals (GUCSH and FHCSH); chemotherapy was performed in 163 (43.9%); and hormone therapy was performed in 50 (13.5%) [22].
According to a study conducted at HUCSH, chemotherapy provided for all 559 (100%) patients and Doxorubicin, cyclophosphamide, and paclitaxel were the chemotherapy regiment was commonest. Hormonal therapy provided 168(30%) and Tamoxifen regiment was commonest hormonal therapy patients, and surgery (modified radical mastectomy) was done for 196 (35.1%) [19].
Chemotherapy was given for 275 (90.7) patients in TASH in 2019, with the most prevalent regimen being 5-fluorouracil, doxorubicin, and cyclophosphamide (FAC) in 66.9% of cases. Surgery was done for 257 (85%) , combination therapy (surgery, chemotherapy, and palliative care) delivered to 189 (55.8%) and Radiotherapy was provided for 107 (35%) [21].
A similar study from TASH on 2013 Surgery was done for 902 (87%), and the majority had a modified radical mastectomy of 880 (95%). The majority of patients 893 (83%) also received chemotherapy, mainly anthracycline-containing chemotherapy (FAC)782 (73%). Hormonal therapy provided for 864 (81%) [31].
According to a study conducted at ACSH, 121 (65.1%) patients had surgery and 33 (17.7%) had chemotherapy, while the rest had both surgery and chemotherapy [30]. In TASH(2017), 192 (74%) patients received surgical intervention, the commonest being mastectomy 126, (65.6%); radiotherapy was provided for 53 (20.5%); and chemotherapy was provided for 231 (89.2%) patients [29].
Discussion
Breast cancer is the most common type of cancer in Ethiopia in most reviewed studies, where the prevalence ranges from 15.2 to 26% from all cancers [14, 15] and from female cancer 29.3–37% [11, 16]. The pattern of breast cancer is increasing in Ethiopia. A study from HUCSH showed the breast cancer rate in hospitals has increased from 69 (12.3%) in 2013 to 106 (19%) in 2019 [19] and Results from TASH showed changes in breast cancer between 1997 and 2012, with a prevalence in 2012 has increased by more than seven times compared 1997 [32].
finding from different studies support this review’s finding which shows incidence increased by 1.44% per year from 1990 to 2017 and as for regional changes in incidence, all regions of breast cancer had increased incidence except North America, and the Middle East and North Africa had the largest increase in overall incidence [33]. In a similar study conducted between 2000 and 2012, incidence rates of breast cancer increased in South Korea, China, and the United Kingdom while decreasing in the United States [34]. The breast cancer incidence in Africa continues to increase and is projected to double by 2050.
This review showed commonest age group was from 40 to 46 years (7, 22, 23, 21, 16, 28, and 20) which similar finding other African studies [35,36,37].
Regarding stage at presentation, most of the patients presented with late stages (stages 3 and 4), with a prevalence range of 57–71.2% [19, 22, 25, 29]. which is supported by papers from Africa showed with 89.6% and 72.8% of breast patients in Kenya and Nigeria respectively presenting with advanced stage disease [38,39,40]. Studies in South Africa reported an advanced stage breast cancer incidence of 50 and 55% [40]. This review showed that early-stage (stages I and II) accounts for 15–35% [6, 8, 15, 27]. Similar findings were found in other developing countries, where only 20–50% of patients in the majority of low- and middle-income countries were diagnosed in these earlier stages [39].
Breast lump or mass is the most common presenting symptom in all studies from various parts of the country, ranging from 57.4 to 88.4% [22, 24,25,26].
Regarding histological findings of breast cancer in Ethiopia, the commonest histology is ductal carcinoma, followed by lobar carcinoma in all reviewed research and prevalence ranges (55.3–93.5%) [16, 20, 22, 26,27,28,29, 31, 41].
The prevalence of hormone receptors and molecular subtypes is high; estrogen receptor positivity is the most common receptor and is found in more than 65% of breast cancer patients. In terms of molecular subtype, Luminal A (ER + and/or PR+, HER2-) is the most common finding in breast cancer biopsies, accounting for more than 40% of cases, while Triple Negative/Basal-like cases account for more than 15% of cases [20, 29]. Similar finding from studies from south Africa showed Estrogen Receptor is the commonest hormone receptors [39, 40].
This review showed surgery is the mainstay treatment for breast cancer in Ethiopia, and radiotherapy is only provided in the capital city on TASH. A similar study from Africa showed a mastectomy rate greater than 85% and a huge difference from Europe’s breast cancer mastectomy of 30% [41].
Limitations of the study
Only English language articles were included.
Conclusion and recommendation
This review summarized the epidemiology, clinical and histological characteristics, and treatment modalities of breast cancer in Ethiopia. Breast cancer incidence is rising, and it accounts for the major cancer burden in the country. There is a need for additional awareness-raising and health education because delayed presentation is a critical problem throughout Ethiopia. For planning and monitoring cancer patterns, comprehensive demographic and clinical data from a population- or facility-based registry are needed. Currently, only one exists in the capital, the Addis Ababa City Cancer Registry (AACCR). There is a need to establish and strengthen histologic and pathology labs, as most hospitals are doing surgeries without histologic, molecular, or receptor identification since it helps with targeted therapy, according to what current best practice suggests. The available treatment options are still limited in Ethiopia; it needs Expanding radiation facilities is a major step toward improving outcomes for breast cancer patients.
Data availability
All data generated or analysed during this study are included in supplementary file.
Abbreviations
- AACCR:
-
Addis Ababa City Cancer Registry
- ACSH:
-
Ayder Comprehensive Specialized Hospital
- BC:
-
Breast Cancer
- CA:
-
Cancer
- DRH:
-
Dessie Referral Hospital
- EPHI:
-
Ethiopian Public Health Institute
- ER:
-
Estrogen Receptor
- FHCSH:
-
Felege Hiwot Comprehensive specialized hospitals
- GUCSH:
-
Gondar University Comprehensive Specialized Hospital
- HER2:
-
Human Epidermal Receptor
- HUCSH:
-
Hawassa University Comprehensive Specialized Hospital
- IRB:
-
Institutional Review Board
- JUMC:
-
Jimma University Medical Center
- LMIC:
-
Low- and Middle-Income Country
- MeSH:
-
Medical Subjects Headings
- MRM:
-
Modified Radical Mastectomy
- PR:
-
Progesterone Receptor
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- SPHMMC:
-
St. Paul’s Hospital Millennium Medical Collage
- TASH:
-
Tikur Anbesa specialized hospital
- WHO:
-
World Health Organization
References
WHO. Breast Cancer diagnosis, prevention and screening. World Health Organization, last Updated 26 March 2021.
Sharma R. Breast cancer incidence, mortality and mortality-to-incidence ratio (MIR) are associated with human development, 1990–2016: evidence from global burden of Disease Study 2016. Breast Cancer. 2019;26:428–45. [CrossRef].
Ferlay J, Laversanne M, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F. Global Cancer Observatory: Cancer Tomorrow. International Agency for Research on Cancer: Lyon, France, 2020; Available online: https://gco.iarc.fr/tomorrow (accessed on 9 July 2021).
GLOBOCAN. 2020: The Global Cancer Observatory (GCO).
Dalal S, Beunza JJ, Volmink J, Adebamowo C, Bajunirwe F, Njelekela M, Mozaffarian D, Fawzi W, Willett W, Adami HO, Holmes MD. Non-communicable diseases in sub-saharan Africa: what we know now. Int J Epidemiol. 2011;40(4):885–901. https://doi.org/10.1093/ije/dyr050.
Weigelt B, Horlings HM, Kreike B, Hayes MM, Hauptmann M, Wessels LFA, de Jong D, van de Vijver MJ, Van’t Veer LJ, Peterse JL. Refinement of breast cancer classification by molecular characterization of histological special types. J Pathol. 2008;216(2):141–50. https://doi.org/10.1002/path.2407.
Koboldt DC, Fulton RS, McLellan MD, Schmidt H, Kalicki-Veizer J, McMichael JF, Fulton LL, Dooling DJ, Ding L, Mardis ER, Wilson RK, Ally A, Balasundaram M, Butterfield YSN, Carlsen R, Carter C, Chu A, Chuah E, Chun HJE, Palchik JD. Comprehensive molecular portraits of human breast tumours. Nature. 2012;490(7418):61–70. https://doi.org/10.1038/nature11412.
Howlader N, Altekruse SF, Li CI, Chen VW, Clarke CA, Ries LAG, Cronin KA. US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J Natl Cancer Inst. 2014;106(5). https://doi.org/10.1093/jnci/dju055.
Edge SB, Byrd DR, Compton CC, et al. AJCC Cancer Staging Manual. 7th ed. New York: Springer; 2009. pp. 419–60.
Centre for Disease Control and Prevention. How is breast cancer treated? Breast Cancer, https://www.cdc.gov/cancer/breast/basic_info/treatment.htm (2018, accessed 22 March 2019).
Kibret YM, Leka YA, Tekle NF, Tigeneh W. Patterns of cancer in Wolaita Sodo University Hospital: South Ethiopia. PLoS ONE. 2022;17(10):e0274792. https://doi.org/10.1371/journal.pone.0274792.
PRISMA_2020_checklist (1).docx.
JBI Critical Appraisal Tools | JBI [Internet]. [cited 2023 Oct 20]. https://jbi.global/critical-appraisal-tools
Tigeneh W, Molla A, Abreha A, Assefa M. Pattern of Cancer in Tikur Anbessa Specialized Hospital Oncology Center in Ethiopia from 1998 to 2010. Int J Cancer Res Mol Mech. 1998;1. https://doi.org/10.16966/2381.
Tefera B. (2019). patterns-of-cancer-in-university-of-gondar-hospital-northwest-ethiopia. annalsofoncology.org/article/S0923-7534(21)00727-. https://doi.org/10.1016/S0923-7534(21)00727-4
Hailu HE, Mondul AM, Rozek LS, Geleta T. Descriptive epidemiology of breast and gynecological cancers among patients attending Saint Paul’s Hospital Millennium Medical College, Ethiopia. PLoS ONE. 2020;15(3). https://doi.org/10.1371/journal.pone.0230625.
Timotewos G, Solomon A, Mathewos A, Addissie A, Bogale S, Wondemagegnehu T, Aynalem A, Ayalnesh B, Dagnechew H, Bireda W, Kroeber ES, Mikolajczyk R, Bray F, Jemal A, Kantelhardt EJ. First data from a population based cancer registry in Ethiopia. Cancer Epidemiol. 2018;53:93–8. https://doi.org/10.1016/j.canep.2018.01.008.
Memirie ST, et al. Estimates of Cancer incidence in Ethiopia in 2015 using population-based registry data. J Glob Oncol. 2018;4:1–11.
Gebretsadik A, Bogale N, Negera DG. (2021). Epidemiological Trends of Breast Cancer in Southern Ethiopia: A Seven-Year Retrospective Review. Cancer Control, 28. https://doi.org/10.1177/10732748211055262
Ersumo T. (n.d.). Breast Cancer in an Ethiopian Population, Addis Ababa. In East and Central African Journal of Surgery (Vol. 11, Issue 1).
Dagne S, Abate SM, Tigeneh W, Engidawork E. Assessment of breast cancer treatment outcome at Tikur Anbessa Specialized Hospital Adult Oncology Unit, Addis Ababa, Ethiopia. Eur J Oncol Pharm. 2019;2(2). https://doi.org/10.1097/OP9.0000000000000013.
Tesfaw A, Tiruneh M, Tamire T, Yosef T. Factors associated with advanced-stage diagnosis of breast cancer in north-west Ethiopia: a cross-sectional study. Ecancermedicalscience. 2021;15. https://doi.org/10.3332/ECANCER.2021.1214.
Ruhama Yoseph. 2021. Retrospective Analysis of Breast Cancer Cases Operated in Jush within Four Years Time Period, Jimma, Ethiopia, International Journal of Sciences, Office ijSciences, vol. 10(10), pages 4–21, October.
Gebremariam A, Addissie A, Worku A, Assefa M, Pace LE, Kantelhardt EJ, Jemal A. Time intervals experienced between first symptom recognition and pathologic diagnosis of breast cancer in Addis Ababa, Ethiopia: a cross-sectional study. BMJ Open. 2019;9(11). https://doi.org/10.1136/bmjopen-2019-032228.
Hassen AM, Hussien FM, Asfaw ZA, Assen HE. Factors associated with delay in breast cancer presentation at the only oncology center in North East Ethiopia: a cross-sectional study. J Multidisciplinary Healthc. 2021;14:681–94. https://doi.org/10.2147/JMDH.S301337.
Deressa BT, Cihoric N, Badra EV, Tsikkinis A, Rauch D. Breast cancer care in northern Ethiopia-cross-sectional analysis. BMC Cancer. 2019;19(1). https://doi.org/10.1186/s12885-019-5612-6.
jgo.org JGO-Journal of Global Oncology. Adequacy of pathologic reports of invasive breast Cancer from mastectomy specimens at Tikur. Anbessa Specialized Hospital Oncology Center in Ethiopia; 2018.
Gemta EA, Bekele A, Mekonen W, Seifu D, Bekurtsion Y, Kantelhardt EJ. Patterns of breast Cancer among Ethiopian patients: presentations and histopathological features. J Cancer Sci Therapy. 2019;11(2). https://doi.org/10.4172/1948-5956.1000581.
Shenkutie B, Mekonnen Y, Seifu D, Abebe E, Ergete W, Damie A, Labisso L, W. Biological and Clinicopathological characteristics of breast Cancer at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. J Cancer Sci Therapy. 2017;9(12). https://doi.org/10.4172/1948-5956.1000504.
Hadgu E, Seifu D, Tigneh W, Bokretsion Y, Bekele A, Abebe M, Sollie T, Merajver SD, Karlsson C, Karlsson MG. Breast cancer in Ethiopia: evidence for geographic difference in the distribution of molecular subtypes in Africa. BMC Women’s Health. 2018;18(1). https://doi.org/10.1186/s12905-018-0531-2.
Kantelhardt EJ, Zerche P, Mathewos A, Trocchi P, Addissie A, Aynalem A, Wondemagegnehu T, Ersumo T, Reeler A, Yonas B, Tinsae M, Gemechu T, Jemal A, Thomssen C, Stang A, Bogale S. Breast cancer survival in Ethiopia: a cohort study of 1,070 women. Int J Cancer. 2014;135(3):702–9. https://doi.org/10.1002/ijc.28691.
SM A. Trends of breast Cancer in Ethiopia. Int J Cancer Res Mol Mech (ISSN. 2016;2(1):2381–3318. https://doi.org/10.16966/2381-3318.121.
Lima SM, Kehm RD, Terry MB. Global breast cancer incidence and mortality trends by region, age-groups, and fertility patterns. EClinicalMedicine. 2021;38. https://doi.org/10.1016/j.eclinm.2021.100985.
Feuchtner J, Mathewos A, Solomon A, Timotewos G, Aynalem A, Wondemagegnehu T, Gebremedhin A, Adugna F, Griesel M, Wienke A, Addissie A, Jemal A, Kantelhardt EJ. Addis Ababa population-based pattern of cancer therapy, Ethiopia. PLoS ONE. 2019;14(9):e0219519.
Othieno-Abinya NA, Nyabola LO, Abwao HO, Ndege P. Postsurgical management of patients with breast cancer at Kenyatta National Hospital. East Afr Med J. 2002;79:156–62.
Amir H, Kaaya EE, Kwesigabo G, Kiitinya JN. Breast cancer before and during the AIDS epidemic in women and men: a study of Tanzanian Cancer Registry Data 1968 to 1996. J Natl Med Assoc. 2000;92:301–5.
Fregene A, Newman LA. Breast cancer in sub-saharan Africa: how does it relate to breast cancer in African-American. Women? Cancer. 2005;103:1540–50.
Jedy-Agba E, McCormack V, Adebamowo C, Dos-Santos-Silva I. Stage at diagnosis of breast cancer in sub-saharan Africa: a systematic review and meta-analysis. Lancet Glob Health. 2016;4(12):e923–35. https://doi.org/10.1016/S2214-109X(16)30259-5. PMID: 27855871; PMCID: PMC5708541.
Cubasch H, Joffe M, Hanisch R, Schuz J, Neugut AI, Karstaedt A, van den Broeze N, McCormack V, Jacobson JS. Breast cancer characteristics and HIV among 1,092 women in Soweto, South Africa. Breast Cancer Res Treat. 2013;140:177–86.
Langenhoven L, Barnardt P, Neugut AI, Jacobson JS. Phenotype and treatment of breast cancer in HIV-positive and -negative women in Cape Town, South Africa. J Glob Oncol. 2016;2(5):284–91.
Bhikoo R, Srinivasa S, Yu TC, Moss D, Hill AG. Systematic review of breast cancer biology in developing countries (part 1): Africa, the middle East, Eastern Europe, Mexico, the Caribbean and South America. Cancers (Basel). 2011;3:2358–81.
Acknowledgements
Not applicable.
Funding
No fund received for this work.
Author information
Authors and Affiliations
Contributions
FGD and BTT developed the protocol, reviewed the reference list, extracted data, and conducted the analyses. TDD and YDS assessed the quality of the data, ensured the absence of errors and arbitrated in case of disagreement. FGD developed the draft manuscript and TDD critically reviewed it. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Dandena, F.G., Teklewold, B.T., Darebo, T.D. et al. Epidemiology and clinical characteristics of breast cancer in Ethiopia: a systematic review. BMC Cancer 24, 1102 (2024). https://doi.org/10.1186/s12885-024-12822-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-024-12822-5