
Abstract
Background
Geographical disparities in cancer incidence are observed at different scales and may highlight areas of high risk that need special attention to improve health policies. In Guadeloupe, a French archipelago in the Caribbean, environmental and socioeconomic factors are potential factors associated with cancer incidence. Our objective was to describe geographical variations of cancer incidence in Guadeloupe at a small-area level, in order to identify potential clusters.
Methods
We conducted spatial analyses for the 18 most frequent cancer sites, using data collected by the population-based cancer registry of Guadeloupe over the period 2008–2017. For each cancer sites, we used the Besag, York and Mollié model to estimate smoothed standardized incidence ratios (SIRs) at a sub-municipality level. In addition, we performed ascendant hierarchical clustering of these smoothed SIRs to describe the relationship between the different cancer sites and to identify geographical clusters.
Results
We observed geographical disparities with a spatial pattern that varied across cancer sites. Clustering of the smoothed SIRs showed aggregations between breast cancer and multiple myeloma, thyroid and stomach cancer, cervical and head and neck cancers, lung and rectal cancers, ovarian and endometrial cancers. Cluster analysis also identified six geographical clusters. Features of these clusters suggest alcohol consumption, exposure to pesticides, pollution generated by open landfills, and ethnicity as possible explanatory factors.
Discussion/conclusion
Our study provided for the first time an extensive description of geographical disparities in cancer incidence in Guadeloupe, in a region where socioeconomic and environmental issues are major concerns. Although the identification of underlying factors was out of the scope of the present study, we highlighted areas of special interest and put forward some hypotheses that warrant to be further investigated in more in-depth analyses.
Similar content being viewed by others


Background
With more than 19 million new cases and nearly 10 million deaths in 2020 [1], cancer is a major cause of morbidity and mortality in the world. Cancer is a multifactorial disease and causes include genetic, infectious, lifestyle and environmental risk factors. Geographical variation of cancer incidence is observed at different scales. Spatial analysis at a small-area level may highlight areas of high risk that need special attention and may improve health policies such as resource planning or access to preventive care. Geographic patterns for each cancer site may also provide clues for possible risk factors and help formulate etiological hypotheses. These hypotheses can be refined if several aggregates show similarities, and the analysis can be supplemented by analyzing several cancers simultaneously. In particular, cluster analysis, although rarely used, is an exploratory tool to classify the geographical areas according to the correlation between the incidence of different cancer sites [2], which could allow identifying shared risk factors.
Guadeloupe is a French overseas territory in the Caribbean, composed of five islands (Grande-Terre, Basse-Terre, Les Saintes, Marie-Galante, La Désirade) with a population of about 400,000 inhabitants (Fig. S1). The population is multi-ethnic but mostly from African descent. The population faces a high prevalence of cardiovascular and metabolic diseases, with 48% of the population being overweight or obese [3]. Cancer incidence is generally lower than in metropolitan France, but it is higher for prostate, stomach and cervical cancers. In general, the incidence rates of cancers in Guadeloupe are between those of metropolitan France and those of the other Caribbean countries [1]. This is reflected in the prevalence of cancer risk factors, which is in the French West Indies in-between mainland France and other Caribbean territories [4] In Guadeloupe, the prevalence of daily tobacco smoking is 12%, the prevalence of daily alcohol drinking is 6.3% [3]. Socioeconomically, compared to the French national average, the population of Guadeloupe has a lower median income, a lower educational level, a higher rate of unemployment, and a larger proportion of people who get income support [5]. The French health insurance system provides in principle universal social security coverage. From an environmental point of view, Guadeloupe suffers from natural phenomena such as sand mists from the Sahara [6] or the invasion of brown sargassum algae [7] and is characterized by an extensive use of pesticides [8].
Our objective was to describe geographical variations of cancer incidence in Guadeloupe, at a small-area level in order to identify potential clusters.
Material and methods
Data
We used data from the Guadeloupe cancer registry, which collects all new cancer cases of patients residing in Guadeloupe since 2008. The registry routinely collects for all cancer sites: the date of diagnosis, the topographical and morphological codes of the International Classification of Diseases for Oncology, (ICD-O3) and sociodemographic data (sex, date of birth and exact address of the place of residence). The registry belongs to the French Network of Cancer Registries (FRANCIM) and meets high quality criteria; the completeness and data quality are regularly assessed by the “Comité d'évaluation des registres” (CER).
We conducted spatial analysis for the 18 most frequent cancer sites: prostate (code ICD-O3 C61; 4418 cases), breast (C50; 1772 cases), colon (C18-C19;1007 cases), rectum (C20_C21;272 cases), stomach (C16;712 cases), esophagus (C25;178 cases), pancreas (C15;246 cases), liver (C22;141 cases), multiple myeloma and plasmocytoma (C42.1 and morphology codes 9731 to 9734; 669 cases), cervix (C53;218 cases), uterus corpus (C54;334 cases), ovary (C56;148 cases), kidney (C64;190 cases), brain (C71;102 cases), thyroid (C73;190 cases)), upper aero-digestive tract (UADT) (C00 to C14 and C30 to C32;527 cases) and melanoma (C44 and morphological code from 8720 to 8770;91 cases). We studied only invasive tumors over the period 2008–2016, i.e., 12,397 tumors.
As a geographical level, we used a sub-municipality level, the IRIS level (for Ilots regroupés pour l’information statistique; Merged Islet for Statistical Information). The IRIS is the smallest geographical census unit available in France. There are 136 IRIS in Guadeloupe. For each patient, the address was geocoded to assign the IRIS of residence. Population for each IRIS by sex and age group (0–14; 15–29; 30–44; 45–59; 60–74; ≥75) was obtained from census data for the years 2008–2016.
Statistical analysis
We first conducted spatial analyses of cancer incidence for the 18 main cancer sites. We used the Besag, York and Mollié model [9] to estimate smoothed SIRs (Standardized Incidence Ratios) for each IRIS. Let Oi the number of observed cases in IRIS i, assumed to follow a Poisson distribution, Ei the number of expected cases calculated with indirect standardization for age and sex, θi = Oi/Ei the SIR in IRIS i. The BYM model is written as follows:
log \({\hat{\theta}}_i\) = α + ui + vi.Where:
α is the intercept
u i represents the non-spatial random effects and \({u}_i\sim N\left(0,{\sigma}_u^2\right)\), vi represents the spatial heterogeneity and was modeled by a conditional autoregressive model (CAR).
The convergence of the model was verified with the Geweke criterion [10]. The graphical representation and the BYM model were implemented with WINBUGS.1.41 and R.4.0.2.
We then performed ascendant hierarchical clustering (AHC) of the smoothed SIRs, using Ward’s method implementation (ward. D2) in the hclust function of R stats package [11]. Two AHCs were performed [2]. First, in order to highlight the relationships between the incidence of different cancers, we performed an AHC of the 18 cancer sites. We also calculated Spearman’s correlation coefficients between the smoothed SIRs. Then, we performed an AHC of the 136 IRIS in order to define geographical clusters. The optimal number of clusters was determined with the elbow method using total within-cluster sum of square as criterion and from examination of the clustering dendrogram.
Results
Table 1 shows for all cancers and several cancer sites the estimated age-standardized incidence rates in 2020 for Guadeloupe, mainland France, the United States and the Caribbean [1]. Guadeloupe has the highest standardized incidences for prostate and stomach cancers, and the lowest for cancers of the corpus uterus, head and neck, liver, lung, and brain.
Smoothed SIRs by cancer site
Excess risks of head and neck, colon, rectum and liver cancers were observed in the eastern part of Guadeloupe (Grande-Terre Island). The western part of Guadeloupe (Basse-Terre) showed an excess risk of esophageal, stomach and pancreatic cancers. Marie-Galante, the island located in the south-east had high incidence areas for all digestive cancers, excluding those of the pancreas, as well as for head and neck cancers. In this territory SIRs were particularly elevated for esophageal and liver cancers (Fig. 1).

Smoothed SIRs for head and neck and digestive cancers. a Head and neck cancer. b Esophageal cancer. c- Stomach cancer. d Colon cancer. e Rectal cancer. f Liver cancer. g Pancreatic cancer
High incidence areas for cancers of the corpus uteri and ovary were mainly found in Basse-Terre. The areas of high incidence of breast and cervical cancers were mostly found in Grande-Terre. Areas with an excess risk of prostate cancer were in the center of Grande-Terre, in the north of Basse Terre and in Marie-Galante. La Désirade, the island located to the east, presented an excess risk of breast, cervical and ovarian cancers (Fig. 2).

Smoothed SIRs for urogenital cancers. a Breast cancer. b Cervical cancer. c Uterine corpus cancer. d Ovary cancer. e Prostate cancer
Regarding other cancer sites, areas with an excess risk of brain cancer and multiple myeloma were mainly found in Grande-Terre, whereas Basse-Terre had the majority of the areas with an excess risk of thyroid cancer and melanoma. La Désirade was an area of excess incidence for lung cancer, melanoma, brain cancer and thyroid cancer. (Fig. 3)

Smoothed SIRs for other cancers. a Lung cancer. b Brain cancer. c Thyroid cancer. d Melanoma. e Multiple myeloma
Cluster analysis
Figure 4 represents the dendrogram of the ascending hierarchical clustering of the 18 cancer sites. The more marked aggregations were found between breast cancer and myeloma, thyroid and stomach cancer, cervical and head and neck cancers, lung and rectal cancers and ovarian and corpus uteri cancers. Associations between these cancer sites are supported by the correlation coefficients between the smoothed SIRs (Fig. 5).

Dendrogram showing the relationships between the smoothed SIRs of the 18 cancer sites

Spearman’s correlation coefficients between the smoothed SIRs
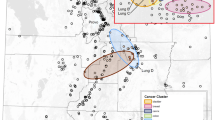
The ascending hierarchical clustering of the 136 IRIS resulted in an optimal number of 6 classes. Figure 6 shows the geographical representation of these 6 clusters. In order to describe the profile of each cluster we calculated the average smoothed SIRs by cancer site (Table 2). Cluster 1 was characterized by a high incidence of stomach and thyroid cancers and a low incidence of cancers of the uterus, ovary, liver, brain and kidney. Cluster 2 presented high SIRs for liver and brain cancers. In Cluster 3, SIRs were above 1 for most cancer sites, and were particularly high for cervical and head and neck cancer. Cluster 4 showed a high incidence of cancer of the uterus, ovary, thyroid, melanoma and kidney. Cluster 5 presented high SIRs for most digestive cancers and head and cancer, as well as for lung, brain and kidney cancer. On the other hand, the incidence of breast and cervical cancer, multiple myeloma and melanoma was low. Cluster 6 was characterized by a low incidence of most cancer sites, and a very high incidence of melanoma, and to lesser extent of breast, pancreatic and brain cancers. We also examined sociodemographic characteristics of the 6 clusters (Table S1). The proportion of women was the highest in cluster 3 and the lowest in cluster 6. The population was older in clusters 5 and 6 than in the other clusters. The proportion of unemployed varied from 15.2% in cluster 6 to 23.6% in cluster 1. Educational level was lower in clusters 5 and 6. These two clusters were also characterized by a higher proportion of farmers and fishermen.

Clustering of the IRIS based on smoothed SIRs of different cancers
Discussion
We observed geographical disparities, with a spatial pattern that varied across cancer sites. Environmental, socioeconomic factors, as well as ethnicity may partially explain these disparities. Our objective was not to identify precisely the underlying causes, but rather to provide leads for further study and to generate hypotheses. Nevertheless, some potential explanatory factors are briefly discussed below.
For prostate cancer, the most frequent cancer in Guadeloupe, no clear spatial pattern emerged. Prostate cancer has been related to exposure to pesticides in general, and in Guadeloupe particularly has been found to be associated with chlordecone, an insecticide previously used in banana plantations [12]. However, the spatial distribution of prostate cancer cases does not specifically match agricultural areas, located in the South East of Basse Terre (banana) and the North of Grande Terre (sugarcane). Instead, high incidence areas were found in urban areas including most health care facilities, which may suggest a role of opportunistic screening. For breast cancer, the second cancer in Guadeloupe, with an incidence rate however lower than in European countries, most SIRs were below 1.1, except for a limited number of high incidence areas, which are characterized by a high proportion of population of European origin, and/or the presence of open landfills.
For digestive cancers, the spatial distribution of cancers of the colon differed markedly from that of rectal cancers. The cancer sites are often grouped in epidemiological studies, despite possible differences in risk factors [13]. The incidence of stomach cancer is high in Guadeloupe, and within Guadeloupe the highest SIRs were found in the North-West and South-East of Basse-Terre. These areas comprise most of the banana plantations and are also characterized by a high social deprivation [14] possibly related to a high prevalence of helicobacter pylori.
Besides the spatial analysis of each cancer site, results of the cluster analysis may help formulate hypotheses by identifying areas with high incidence of several cancer sites that may share common risk factors. Some of the six identified clusters warrant further attention. Cluster 1, in the North of Basse-Terre, is characterized by a high incidence of stomach and thyroid cancer, for which we were not able to identify a common risk factor. Cluster 2 in the center of Guadeloupe, is an area where the majority of sugarcane plantations are located as well as the main sugar and rum factories. This area showed an excess incidence of liver cancer, the main risk factor being alcohol consumption [15], and an excess incidence of brain cancer, potentially related to exposure to pesticides [16]. Cluster 3 is the only cluster composed of two non-adjacent parts. A common feature of these two parts is a high population density. Living in an urban area is a risk factor for breast and cervical cancers [17]. The sedentary lifestyle associated with urban living could explain the higher incidence of colon cancer [18]. Another potential risk factor could be the pollution generated by the open landfills present in the two distinct areas. Finally, the high incidence of head and neck and cervical cancer observed in this cluster may be due to a high circulation of Human Papilloma Virus (HPV), associated with both cancer sites [19, 20]. Cluster 4 includes large areas with banana plantations, with an extensive use of pesticides, including endocrine disruptors such as the organochlorine insecticide chlordecone. Several cancers (ovarian, endometrial, and thyroid) displaying a high incidence in this area are hormone-sensitive [21]. However, there was no excess of breast and prostate cancer. This may be partially explained by the relatively large proportion of people from Indian descent in the cluster population, for whom reported incidence rates of breast and prostate cancer are usually lower than for Afro-descendent people.
Cluster 5 corresponds to the island of Marie-Galante, with many sugar cane plantations and a sugar factory. This area showed the highest incidence for most of the cancer sites, particularly for alcohol-related cancers [15]. Unfortunately, data on alcohol consumption in Guadeloupe are only available for the whole population, and are not collected at any geographical level. Cluster 6 corresponds to the islands of Les Saintes, where the population is from European descent in its vast majority. This may explain the higher incidence of breast cancer [22] and melanoma [23]. In addition, sun exposure in fishermen, an important activity in these islands, may also contribute to the high incidence of melanoma.
An important limitation of our study is the relatively small number of cases for most cancer sites, which notably precluded separate analyses in men and women. Small numbers also prevented the analysis of rare cancer sites, although some of them were of special interest, such as subtypes of hematological malignancies. These shortcomings will be overcome when a longer follow-up period will become available. In addition, although we used the smallest available census unit, some of the IRIS in Guadeloupe are relatively large, and then probably heterogeneous. Despite these limitations, our study provided for the first time an extensive description of geographical disparities in cancer incidence, in a region where socioeconomic and environmental issues are major concerns. Although the identification of explanatory factors was out of the scope of the present study, we nevertheless highlighted areas of special interest and put forward some hypotheses that warrant to be further investigated in more in-depth analyses. Etiological studies are planned for some cancer sites. Furthermore, a mapping of the use of pesticides, which take into account the diversity of pollutants and their historical use is in progress, and will allow ecological studies. Taking together, these findings will inform health policies in the territory.
Availability of data and materials
The datasets analyzed for the current study are available from the corresponding author on reasonable request
Abbreviations
- AHC:
-
Ascendant Hierarchical Clustering
- BYM:
-
Besag York and Mollié
- ICD-O3:
-
International Classification of Diseases for Oncology 3
- IRIS:
-
Ilots regroupés pour l’information statistique
- SIR:
-
Standardized Incidence Ratio
References
Ferlay J, Ervik M, Colombet M, Mery L, Piñeros M, Znaor A, et al. Global Cancer observatory. 2020. Available from: https://gco.iarc.fr/. Accessed 25 Nov 2021.
Cassetti T, La Rosa F, Rossi L, D’Alò D, Stracci F. Cancer incidence in men: a cluster analysis of spatial patterns. BMC Cancer. 2008;8:344.
Richard J-B, Pitot S, Cornely V, Pradines N, Beck F. Premiers résultats du Baromètre santé DOM 2014 Guadeloupe. Baromètre santé: Sante Publique France; 2014.
Auguste A, Dugas J, Menvielle G, Barul C, Richard J-B, Luce D. Social distribution of tobacco smoking, alcohol drinking and obesity in the French West Indies. BMC Public Health. 2019;19:1424.
Calderini Y, Blanc S, Tantin MM. La population active continue de baisser en Guadeloupe - Insee Analyses Guadeloupe - 36. INSEE. 2019. Available from: https://www.insee.fr/fr/statistiques/3975584; .
Cadelis G, Tourres R, Molinie J. Short-term effects of the particulate pollutants contained in Saharan dust on the visits of children to the emergency department due to asthmatic conditions in Guadeloupe (French archipelago of the Caribbean). PLoS One. 2014;9:e91136.
Boisnoir A, Pascal P-Y, Cordonnier S, Lemée R. Spatio-temporal dynamics and biotic substrate preferences of benthic dinoflagellates in the Lesser Antilles. Caribbean sea Harmful Algae. 2019;81:18–29.
Dereumeaux C, Saoudi A, Guldner L, Pecheux M, Chesneau J, Thomé J-P, et al. Chlordecone and organochlorine compound levels in the French West Indies population in 2013-2014. Environ Sci Pollut Res Int. 2020;27:41033–45.
Besag J, York J, Mollie A. Bayesian image restoration, with two applications in spatial statistics. Ann Inst Stat Math. 1991;43:1–20.
Bivand R, Pebesma EJ, Gómez-Rubio V. Applied spatial data analysis with R. Second edition. New York: Springer; 2013.
R Core Team. R: A. Language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2013.
Multigner L, Ndong JR, Giusti A, Romana M, Delacroix-Maillard H, Cordier S, et al. Chlordecone exposure and risk of prostate cancer. J Clin Oncol. 2010;28:3457–62.
Wei EK, Giovannucci E, Wu K, Rosner B, Fuchs CS, Willett WC, et al. Comparison of risk factors for colon and rectal cancer. Int J Cancer. 2004;108:433–42.
Luce D, Michel S, Dugas J, Bhakkan B, Menvielle G, Joachim C, et al. Disparities in cancer incidence by area-level socioeconomic status in the French West Indies. Cancer Causes Control. 2017;28:1305–12.
Chuang S-C, Lee Y-CA, Wu G-J, Straif K, Hashibe M. Alcohol consumption and liver cancer risk: a meta-analysis. Cancer Causes Control. 2015;26:1205–31.
Quach P, El Sherif R, Gomes J, Krewksi D. A systematic review of the risk factors associated with the onset and progression of primary brain tumours. NeuroToxicology. 2017;61:214–32.
Moss JL, Liu B, Feuer EJ. Urban/rural differences in breast and cervical Cancer incidence: the mediating roles of socioeconomic status and provider density. Womens Health Issues. 2017;27:683–91.
Mahmood S, MacInnis RJ, English DR, Karahalios A, Lynch BM. Domain-specific physical activity and sedentary behaviour in relation to colon and rectal cancer risk: a systematic review and meta-analysis. Int J Epidemiol. 2017;46:1797–813.
Auguste A, Gaëte S, Herrmann-Storck C, Michineau L, Joachim C, Deloumeaux J, et al. Prevalence of oral HPV infection among healthy individuals and head and neck cancer cases in the French West Indies. Cancer Causes Control. 2017;28:1333–40.
Castellsagué X. Natural history and epidemiology of HPV infection and cervical cancer. Gynecol Oncol. 2008;110(3 Suppl 2):S4–7.
Sharma T, Banerjee BD, Thakur GK, Guleria K, Mazumdar D. Polymorphism of xenobiotic metabolizing gene and susceptibility of epithelial ovarian cancer with reference to organochlorine pesticides exposure. Exp Biol Med (Maywood). 2019;244:1446–53.
Davis Lynn BC, Rosenberg PS, Anderson WF, Gierach GL. Black-white breast Cancer incidence trends: effects of ethnicity. J Natl Cancer Inst. 2018;110:1270–2.
Armstrong BK, Cust AE. Sun exposure and skin cancer, and the puzzle of cutaneous melanoma: a perspective on fears et al. mathematical models of age and ultraviolet effects on the incidence of skin cancer among whites in the United States. American journal of epidemiology 1977; 105: 420-427. Cancer Epidemiol. 2017;48:147–56.
Acknowledgements
Not applicable
Funding
This study is part of the project GESSICa – “Risk factors associated with cancer in Guadeloupe: Environment, Socioeconomic context”, co-financed by the European Union in the framework of the Operational Program FEDER-FSE Guadeloupe Regional Council 2014–2020 / European Fund for Regional development (GP0024692).
The cancer registry of Guadeloupe is co-supported by grants from the ‘French National Institute of Cancer (INCa) and Santé Publique France,
The content is solely the responsibility of the authors. The funders are not responsible for any use that may be made of the information contained herein.
Author information
Authors and Affiliations
Contributions
BB analyzed the data and drafted the manuscript. DL and JD managed the study and revised the manuscript. All authors contribute to the conception of the study and to data interpretation, and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The cancer registry of Guadeloupe is authorized by the French Data Protection Authority, Commission National Informatique et Liberté (CNIL), authorization N° 909113 of June 29, 2009. Given their public health mandate, French cancer registries are authorized by the French Data Protection Authority “Commission National Informatique et Liberté” (CNIL), to collect data on cancer cases with a waiver for written informed consent (CNIL deliberation n°03–053 of November 27, 2003). Patients’ information is given by notices displayed in health care facilities, their attending physician or specialist. General information is also available on the National Cancer Institute website: http://lesdonnees.e-cancer.fr/Informations/Sources/Notice-d-information-generale.
This study obtained ethics approval from the local research ethic committee of the university hospital of Guadeloupe “Comité éthique CHUPPA” under the registration number A77_14_02_2022_ANSPACAGU. The privacy impact assessment was vetted by the data protection officer of the University hospital of Guadeloup (dpo@chu-guadeloupe.fr) in accordance to the General Data Protection Regulation (GDPR). The study was performed in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bhakkan-Mambir, B., Deloumeaux, J. & Luce, D. Geographical variations of cancer incidence in Guadeloupe, French West Indies. BMC Cancer 22, 783 (2022). https://doi.org/10.1186/s12885-022-09886-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-022-09886-6