
Abstract
Background
Low birth weight (LBW) is associated with infant mortality and postpartum health complications. In previous studies, overall LBW has been found to be significantly associated with several sociodemographic factors, including ethnicity, maternal age, and family income. Few studies have evaluated the association between environmental risk factors and LBW rates. This study investigated the effect of pre-birth water, sanitation, and hygiene (WASH) and housing conditions on self-reported low birth weight.
Methods
The Ethiopian Demographic and Health Survey, which covered all administrative regions of Ethiopia from January to June 2016, provided data for this study. STATA version 16 was used to analyze 12,125 participants across weighted samples. Multivariable multilevel mixed-effect logistic regression analysis was conducted to determine the effects of each factor on the outcome while accounting for data clustering. The adjusted odds ratios and corresponding 95% confidence intervals were used to determine the statistical significance of the independent variables.
Results
One thousand five hundred and seventeen newborns, or 12.59% [95% CI (10.2- 15.3)], had low birth weights. When other factors were taken into account, the following factors were significantly associated with low birth weight: not using small-scale water treatment technology before using water [AOR (95% CI) 1.36 (1.08–2.23)], burning solid fuels for energy [AOR (95% CI) 1.99 (1.60–2.21)], living in homes with natural wall coverings [AOR (95% CI) 1.81 (1.47–2.21)], using a shared latrine within a woman's housing complex or compound [AOR (95% CI) 1.63(1.06–2.25)], and living in peripheral, isolated regions [AOR (95% CI) 1.38 (1.06–2.21)].
Conclusion
A little more than one out of every ten deliveries in Ethiopia was under normal (recommended) weight. This study shows that poor housing conditions and lack of household WASH infrastructure are independent predictors of poor birth outcomes among Ethiopian women, adding to the limited evidence that environmental factors within the domicile contribute to low birth weight. Interventions to address these issues may help lower the prevalence of LBW.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
According to the World Health Organization (WHO), low birth weight (LBW) is defined as a weight of < 2500 g at birth. LBW is also a major cause of death among children under the age of five [1]. The long-term effects of LBW on postnatal development may include an increased risk of respiratory distress, infection, hypoglycemia, polycythemia, intellectual difficulties, cerebellar palsy, vision and hearing loss, and feeding and digestion issues [2,3,4].
It is well established that socioeconomic, demographic, and genetic factors affect LBW. In previous studies, race, maternal age and health, and family socioeconomic status were individual-level variables associated with LBW incidence [5,6,7]. It has also been recognized that several environmental factors increase the incidence of LBW. These elements include exposure to toxins in the air, water, and pesticides, as well as the proximity of the parent’s home to other environmental dangers including motorways and gas drilling sites [8, 9].
Nevertheless, the majority of prior studies on the environmental influences of LBW rates mostly concentrate on commonly observed air pollutants, such as gases (NOx, SO2, CO, and O3) and particulate matter (PM10 and PM2.5) [2, 10, 11]. Goal three of the Sustainable Development Goals (SDGs) states that "preventable deaths of infants and children under the age of five must end and maternal mortality must be reduced by 75 percent by 2030 [12]. Frameworks that have gained traction for reducing feto-maternal mortality, such as the "Three Delays" and "Continuum of Care" models, almost entirely concentrate on increasing access to and the quality of maternal health services, with little attention paid to broader environmental influences [13, 14].
Between sixty and eighty percent of communicable infections in Ethiopia are caused by poor hygiene, a lack of access to clean water, and other problems. Additionally, it's estimated that environmental conditions including overcrowding, a lack of access to water sources, and unsanitary facilities are responsible for 50% of the effects of undernutrition [15]. Only 17% of people in a given community practice improved hygiene, 65% of families had access to improved water sources, and 6.3% had improved sanitation [16]. The above-mentioned direct and indirect effects of WASH on health can be used to infer the plausibility of this effect on child health, but there is a lack of methodical mapping and evaluation of these numerous, complicated, and frequently overlapping pathways. Anecdotal evidence and observational studies make up the majority of the evidence for these pathways, which is generally weak.
According to previous studies, a person's health cannot be entirely explained by factors at the individual level; therefore, a novel methodology is needed to understand the community-level causal pathways of public health outcomes [17]. In the current study, we propose that examinations of these multi-level domiciliary conditions, which can have a significant impact on embryo-fetal development, should be conducted to better understand how the environment affects human reproduction.
Thus, the goal of this study was to present epidemiologic data on the potential effects of the various environmental risk factors in the home on the weight of newborns in Ethiopia. Determining whether household environment-related stress—both physical and psychosocial—affects birth outcomes for women in low-income countries is critical for understanding whether the global prevalence of LBW could be reduced by improving the environmental conditions in which pregnant women seek clean water and improved sanitation. Moreover, estimating the contribution of these risk factors to poor health could serve as the foundation for identifying and utilizing policy, advocacy, and programming synergies that will result in more effective, efficient, and equitable investments in both reproductive and environmental health sectors. Our objective was to address these research gaps, which would increase policy coherence and result in more effective interventions.
Methods
Study design and area
The 2016 Ethiopian Demography and Health Survey (EDHS) provided secondary data that were analyzed. Amhara, Benishangul-Gumuz, Gambella, Harari, Oromia, Somali, and the Southern Nations, Nationalities, and People's Region (SNNPR), together with two administrative cities (Addis Ababa and Dire-Dawa), participated in the Demographic and Health Survey. There are currently 115,114,480 people living in Ethiopia, according to the latest available United Nations statistics [18].
Data source and study period
The data for this investigation were obtained from the official database of the Demography Health Survey (DHS) program; www.measuredhs.com after permission was requested. The Demographic and Health Survey in Ethiopia was conducted between 18 January and 27 June 2016.
Sampling procedure, study population, and sample size
The 2007 Population and Housing Census, which used a stratified two-stage cluster sampling technique, served as the sampling frame for EDHS 2016. In the first stage, 645 enumeration areas (EAs) were carefully selected using a probability proportional to the size of the EA and an independent selection in each sampling stratum (202 in urban areas and 443 in rural areas). The second step involved the systematic selection of 28 households. The EDHS 2016 report includes a publication on the sampling methodology [19].
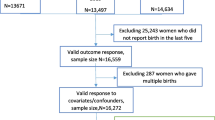
In this survey, mothers were asked to provide information on the birth weight of any child delivered within the previous five years. In addition, data on housing characteristics were gathered from the de jure population. A weighted sample of 19,318 women revealed that at least one birth had occurred in the five years before the study. The analysis was subsequently discontinued for 4828 mothers whose infants had not been weighed. A total of 699 mothers were excluded because they did not know the birth weights of their children. The final sample was a weighted sample of 12,125 participants.
Study variables
Outcome variables
Low birth weight, defined as the weight of a newborn less than 2.5 kg at birth regardless of gestational age, was the study's outcome variable. All mothers who were interviewed between the ages of 15 and 49 who had given birth and whose children had been weighed and recalled were included. Newborns were classified into non-LBW birth weight ≥ 2,500 g = 0 and birth weight < 2,500 g = 1.
Independent variables
Potential risk factors of LBW were extracted from the data set after examining recent literature. The extracted variables were categorized as individual, household, and community-level variables because the 2016 EDHS data are hierarchical. Maternal factors that were unique to each woman were classified as individual-level variables (Table 1).
On the other hand, household-level variables included characteristics that apply to all mothers residing in the same household (Table 2). The variables at the community level were those that applied to all women living in the same community (cluster), such as place of residence, region, community (cluster) poverty, and community women's education (Table 3). Individual factors within the cluster were aggregated to produce variables, such as community women's education and community poverty. Based on the national median values of the created variables, the generated variables were further divided into low and high categories.
Data management and statistical analysis
Before the analysis, the variables were sorted, cleaned, and recorded using STATA version 14. Households whose outcome variables were missing or were marked as unavailable because their values could not be used were excluded. These data were recorded into the database under a special code designated "na" that either indicated responses that were judged to be inconsistent with other responses on the questionnaire and thought to be likely errors or answers with the value "Don't know."
Multilevel analysis
Analytical and descriptive statistics including frequencies and proportions were computed. A weighted analysis was carried out to account for the uneven likelihood of selection between the strata caused by the non-proportional distribution of samples to different regions, residences, and study participants' non-response rates. Multilevel (three-level) regression was utilized because of the hierarchical structure of the 2016 EDHS data, where individuals nested within households and households nested within clusters. Biased parameter and standard error estimations could emerge from using single-level analysis while ignoring the hierarchical character of the data. Furthermore, hierarchical data do not support the normal logistic regression assumption of independent observations. By simultaneously analyzing the impacts of explanatory factors at various levels, multilevel analysis overcomes these constraints.
Variables with a p-value of less than 0.25 were included in the multivariable analysis following the bi-variable multilevel logistic regression analysis. The adjusted odds ratio was calculated with a matching 95% confidence level to show the strength of the association. The dependent variable was judged to be significantly associated with variables with a p-value ≤ 0.05. Using a Variance Inflation Factor (VIF) of < 10, multicollinearity between the individual- and community-level variables was examined.
Random effects
Five random intercept models were fitted (Models 1, 2, 3, 4, and 5).
Model one (null model)—This model has only the intercept and no other independent variables. The intra-class correlation coefficient (ICC) and median odds ratio (MOR) statistics were calculated for the measures of variation (random effects). While MOR can measure unexplained cluster variability, ICC can explain cluster variability (heterogeneity). The ICC was 17%, indicating that variations in the prevalence of LBW were caused by variations at the cluster level. Significant group-level variance is shown by an ICC of at least 2%, which is a requirement for a multilevel study design. Additionally, intra-household clustering was suggestive of employing a three-level model as opposed to a two-level model that overlooks heterogeneity at the household level (controlling for intra-household and intra-cluster variability). Individual-, household-, and community-level variables were taken into account in Models 2, 3, and 4, respectively.
Model five was adjusted for the individual-, household-, and community-level factors. This model demonstrated that unobserved community- and household-level factors might account for 17.3% of the unexplained variation. The fifth model with the lowest deviance was selected as the best-fit model after comparison. The goodness of fit was also tested using Schwarz's Bayesian Information Criterion (BIC) and Akaike's information criterion (AIC). The lowest AIC or BIC values were deemed a better explanatory model.
Result
Socio-demographic characteristics
Mothers between the ages of 25 and 34 made up 77.1% of the study subjects. Similarly, more than half (63.7%) of the households had four to seven members. One-third (29%) of the mothers in the study had no formal schooling. Concerning household wealth, 17.89% of households were in the two lower quintiles. In terms of the participants' community-level characteristics, half (50.4%) of the participants lived in rural areas. Moreover, three fourth (78%) of the homes were located in large central areas. More impoverished households were observed in the majority (84.51%) of clusters compared to the national median proportion (Table 4).
Water, sanitation, and hygiene related characteristics of households
The majority of the households (71.85%) used improved water sources, whereas 66.9% had improved sanitation facilities. A large majority (97.36%) of households used water sources that were not in their own homes. Toilets were shared with another home in 44.09% of the surveyed households. Adult females collected water in three-quarters of the homes. Eighteen percent of the households had to travel for more than 30 min to collect water. A mobile handwashing station was present in 62% of the households. Soap or detergents were only present in places where individuals cleansed their hands in 33% of households.
Similarly, only 14.13% of homes treated their water at the point of use. A total of 61.96% of the households reported water service continuity lasting a full day or more in the 14 days before the survey. Concerning child feces, only 1.08% of the homes in the survey flushed child feces into the toilet (Table 5).
Household fuel and housing material-related characteristics of households
In the current study, 82% of the households used solid fuels to meet their energy needs, and slightly more than half (56.5%) of the households cooked meals in a different building from where they slept and lived. Regarding the construction materials used in homes, the survey found that natural flooring materials were used in 55.7% of the homes and that rudimentary finishing was used on the majority of the walls (81.94%). For roofs, 78.63% of the homes used improved materials (Table 6).
Prevalence of low birth weight
A total of 1517 infants, [(12.59%, 95% CI (10.2- 15.3)], were born underweight in the five years before the survey.
Factors associated with LBW
The measure of association (fixed effects)
Utilizing solid fuels, having unimproved wall covering, and not using point-of-use water treatment were found to be strongly associated with LBW when considering household-level factors. As per community-level characteristics, LBW was found to be significantly associated with living in small peripheral states in the multilevel multivariable mixed effects logistic regression analysis. When other factors were taken into account, households that did not employ small-scale water treatment technology before using water had a 1.3 times higher likelihood of having babies who were underweight at birth [AOR (95% CI) 1.36 (1.08–2.23)].
The likelihood of neonates having low birth weight was also significantly associated with families using solid fuels for energy [AOR (95% CI) 1.99 (1.60–2.21)]. Infants with low birth weight were 1.8 times more likely to be delivered in dwellings where the walls were coated with natural materials [AOR (95% CI) 1.81 (1.47–2.21)]. Using a shared sanitary facility within a woman's domicile or compound was also associated with a greater risk of low birth weight [AOR (95% CI) 1.63(1.06–2.25)]. Compared to metro inhabitants, those who lived in small peripheral regions were 1.3 times more likely to give birth to neonates who were below normal weight [AOR (95% CI) 1.38 (1.06–2.21)] (Table 7).
Measures of variations (random effects)
The ICC in the empty model demonstrated that the variation in the prevalence of LBW across clusters accounted for 17% of the overall variation. Furthermore, when choosing two places at random, the odds ratio between the highest risk area and the lowest risk area was 1.60 (95% CI: 1.26, 1.93). Nine percent of the national variation observed in the empty model was explained by individual, household, and community-level variables (PCV = 9%). When compared to the empty model, individual-, household-, and community-only models, and then again to the entire model, the values of AIC, BIC, and Deviance all indicated a continuous decrease. This demonstrates that the final model developed during the analysis had acceptable goodness of fit (Table 8).
Discussion
The WHO estimates that poor WASH and housing conditions account for over ten percent of the world's illness burden when multiple health consequences are taken into account. However, the impact of inadequate housing and WASH on prenatal birth weight has not yet been quantified [24]. According to the latest available WHO statistics, Ethiopia experienced 28,020 LBW fatalities in 2020, accounting for 4.97% of all deaths. The country is ranked 37th in the world for LBW mortality, with an age-adjusted death rate of 9.52 per 100,000 people [25]. As a result, many argue that frameworks that have been popular for lowering feto-maternal mortality have missed opportunities for potential synergies between newborn and environmental health.
The major objective of this study was to identify multilevel characteristics associated with LBW in Ethiopia. Accordingly, the analysis found that factors evolving from individual, household, and community (cluster) levels had an impact on weight at birth. The likelihood of LBW varied significantly between households and clusters. Because of this heterogeneity, it was inferred that individual-level factors might not account for the entire variation. The results revealed that in the five years before the survey, 12.59% [95%CI (10.2- 15.3)] of newborns were delivered with low birth weight. This implies that Ethiopia still struggles with preventable events that might be averted by integrating prenatal health with housing and WASH interventions.
There is a growing body of evidence, supported by biological plausibility, which indicates that poor water quality affects fetal and neonatal outcomes in a variety of ways [26, 27]. Water contamination by microbiological pathogens, chemicals, and radiation is a problem that affects the health of a significant segment of the population [20, 28]. This study has provided quantifiable measures of association by identifying that households that did not employ point-of-use water treatment before using water had a 36% higher likelihood of having babies who were underweight at birth.
Household water treatment (HWT), also known as point-of-use water treatment, offers a technique to reduce risk levels by treating water that has been contaminated at the source and by domestic handling in communities without consistent access to safe drinking water [29]. Although it has been demonstrated that the opportunity and financial costs of acquiring and treating water consume a sizable portion of the resources of poor families [20], little is known about how and why some people modify their behavior concerning water treatment while others do not. Future studies must gain a deeper understanding of the factors driving water treatment decisions.
Ninety-four percent of Ethiopian families use solid fuels like wood, kerosene, and charcoal for cooking or heating [21]. Traditional domestic energy practices have a significant impact on socioeconomic development, the environment, and human health [30]. The total burden of disease is five times greater than that caused by outdoor air pollution. Women are disproportionately exposed to pollution from cooking fuels because they are typically in charge of childcare and cooking [30].
According to earlier studies, exposure to home air pollution during pregnancy can endanger both the mother and the unborn child. Carbon monoxide, the primary component of incomplete combustion, reacts with hemoglobin to generate carboxyhemoglobin, resulting in a diminished ability to carry oxygen to tissues and the growing fetus [31]. As a result, increased prenatal fatalities occur and newborns have low birth weights. The rates of electrification in urban and rural areas in Ethiopia are drastically different. Clean cooking fuel is primarily used by urbanized households with highly educated household heads [32]. In order to strengthen their capacity to motivate community members across a wide variety of user types or levels of readiness to use clean fuels and to provide social support for such behaviors, future interventions should consider these factors.
Historical data from the United States and Europe support the theory that housing modifications have an impact on feto-maternal outcomes [33, 34]. Regarding long-term health metrics, those who live in completed homes, with brick or plaster walls, and a tiled roof perform much better than people who live in the least desirable type of housing [35]. Poor housing quality is linked to a higher risk of developing many illnesses, most notably respiratory and infectious diseases, but also blood pressure and cardiovascular disease [36].
In the present study, infants with low birth weights were more likely to be born in homes covered in natural cover than in those with finished walls. Given the rapid development currently occurring in sub-Saharan Africa, a full understanding of the protective efficacy of housing modifications is required to calculate the potential reductions in fetal morbidity and death. As a result, the Ethiopian government will need to work with the private sector to encourage housing development by increasing access to and upgrading the quality of the available stock, while also making it simpler for people to access land and housing finance.
Research has shown that public toilets are a vital component of building sustainable, open, and inclusive communities. However, human feces is a major source of transmission for many common diseases, as well as many vaginal and urinary infections, which makes it crucial to offer hygienic public toilets [37]. Today’s modern public health discourse, however, questions whether public toilets act as a conduit for pathogen transmission and physical disability or as a facilitator of health [38]. In many parts of the developing world, women are forced to navigate difficult—and perhaps personally dangerous—social and environmental public conditions to locate a safe, private area to defecate and bathe, which creates psychosocial stress [39]. Additionally, the absence of household WASH infrastructure exposes women to criminality and harassment, which have previously been identified as important predictors of women's vulnerability to LBW [28].
Few studies have specifically examined the influence of shared toilets on adverse pregnancy outcomes. Those that did, report that using a shared toilet was more likely to result in low birth weight than using a private family restroom [37, 40]. This was further illustrated in the current study, which found that mothers who reported sharing toilets with other households had a 63% higher likelihood of giving birth to underweight newborns. Interventions that introduce gender-sensitive sanitation — including clean, safe, and separate toilets, and access to water—may thus serve to ensure gender-equitable living conditions that address the needs of all people, including pregnant women in Ethiopia.
People who lived in small peripheral regions were more likely to give birth to neonates who were below normal weight than metro residents. The Ethiopian government has recognized the small peripheral regions Afar, Somalia, Benishangul, and Gambella as developing regional states because of the high prevalence of poverty and social metrics that trail far below national averages [41]. While variations in socio-demographic variables may account for regional variations in prevalence, it is known that deficiencies, inconsistent service delivery, inequity, and inefficiency are some of the key fetal health challenges. Thus, for such regions to deliver the goods and services that the native population desires with a comparative or absolute advantage, more work must be done to ensure the development of the human and social capital of the regions.
This study reveals that a lack of household WASH infrastructure is a risk factor for poor birth outcomes in women in low-income countries, adding to the scant evidence about environmental causes of LBW. To the best of our knowledge, this study is the first to quantify the proportional contributions of the individual-, family-, and community-level environmental factors that impact birth weight in Ethiopia. Despite the aforementioned benefits, this study has some limitations. Because the data were cross-sectional, they were inadequate for determining causal correlations. The lack of temporal data is unlikely to introduce any bias; however, major changes in housing standards and WASH services are unlikely to occur over such short periods. Another potential limitation of this study is the lack of information on housing features other than the building materials used to construct floors, walls, and roofs in the survey data. There is no information available about a home's interiors, such as whether the eaves are open or whether any windows or doors have screens. Finally, a recall bias may be introduced when measuring historical events.
Conclusion
The intricate interactions between access to water, sanitation, and hygiene as well as housing conditions and birth outcomes among Ethiopian women were examined in this study. The study also provides opportunities for further research and insights that may have policy- and program-related implications for environmental and child-health programs. Important risk factors for LBW include households without a private source of drinking water, living in small peripheral regions, using solid fuels as the main source of energy, and households in which women handle their sanitary needs in shared or public spaces. Because of the multiple pathways through which poor access to water, sanitation, and hygiene may negatively impact newborn health outcomes, it is necessary to integrate WASH and housing considerations to support efforts within the newborn and child healthcare program in Ethiopia and vice versa to leverage greater progress in reducing neonatal mortality and morbidity.
Availability of data and materials
The datasets generated during and analyzed during the current study are not publicly available but are available from the corresponding author Aiggan Tamene via apublic22@gmail.com on reasonable request.
References
Negrato CA, Gomes MB. Low birth weight: causes and consequences. Diabetol Metab Syndr. 2013;5(1):1–8.
Kwinta P, Klimek M, Drozdz D, Grudzień A, Jagła M, Zasada M, et al. Assessment of long-term renal complications in extremely low birth weight children. Pediatr Nephrol. 2011;26(7):1095–103.
Singer D, Thiede LP, Perez A. Adults born preterm: long-term health risks of former very low birth weight infants. Dtsch Arztebl Int. 2021;118(31–32):521.
Valcamonico A, Accorsi P, Sanzeni C, Martelli P, La Boria P, Cavazza A, et al. Mid-and long-term outcome of extremely low birth weight (ELBW) infants: an analysis of prognostic factors. J Matern Fetal Neonatal Med. 2007;20(6):465–71.
Gete DG, Waller M, Mishra GD. Effects of maternal diets on preterm birth and low birth weight: a systematic review. Br J Nutr. 2020;123(4):446–61.
Kc A, Basel PL, Singh S. Low birth weight and its associated risk factors: health facility-based case-control study. PLoS One. 2020;15(6): e0234907.
Getaneh T, Negesse A, Dessie G, Desta M. The impact of pregnancy-induced hypertension on low birth weight in Ethiopia: systematic review and meta-analysis. Ital J Pediatr. 2020;46(1):1–11.
Lu C, Zhang W, Zheng X, Sun J, Chen L, Deng Q. Combined effects of ambient air pollution and home environmental factors on low birth weight. Chemosphere. 2020;240: 124836.
Li C, Yang M, Zhu Z, Sun S, Zhang Q, Cao J, et al. Maternal exposure to air pollution and the risk of low birth weight: a meta-analysis of cohort studies. Environ Res. 2020;190: 109970.
Bekkar B, Pacheco S, Basu R, DeNicola N. Association of air pollution and heat exposure with preterm birth, low birth weight, and stillbirth in the US: a systematic review. JAMA Network Open. 2020;3(6):e208243-e.
Chersich MF, Pham MD, Areal A, Haghighi MM, Manyuchi A, Swift CP, et al. Associations between high temperatures in pregnancy and risk of preterm birth, low birth weight, and stillbirths: systematic review and meta-analysis. BMJ. 2020;371:m3811.
Nabyonga-Orem J. Monitoring Sustainable Development Goal 3: how ready are the health information systems in low-income and middle-income countries? BMJ Glob Health. 2017;2(4): e000433.
Yunus S, Kauser S, Ali S. Three ‘delays’ as a framework for critical analysis of maternal near miss and maternal mortality. J South Asian Feder Obst Gynae. 2013;5:57–9.
Graham WJ, Varghese B. Quality, quality, quality: gaps in the continuum of care. Lancet. 2012;379(9811):e5–6.
Morgan C, Bowling M, Bartram J, Kayser GL. Water, sanitation, and hygiene in schools: status and implications of low coverage in Ethiopia, Kenya, Mozambique, Rwanda, Uganda, and Zambia. Int J Hyg Environ Health. 2017;220(6):950–9.
Tamene A, Afework A. Exploring barriers to the adoption and utilization of improved latrine facilities in rural Ethiopia: an Integrated Behavioral Model for Water, Sanitation and Hygiene (IBM-WASH) approach. PLoS One. 2021;16(1): e0245289.
Roux AVD, Schwartz S, Susser E. Ecological variables, ecological studies, and multilevel studies in public health research. Oxford Textbook of Global Public Health. 2017:411:493–507.
Bekele A, Lakew Y. Projecting Ethiopian demographics from 2012–2050 using the spectrum suite of models. Ethiop Public Health Assoc. 2014;4.
Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia, and Rockville: CSA and ICF; 2016.
Tamene A. A qualitative analysis of factors influencing household water treatment practices among consumers of self-supplied water in rural Ethiopia. Risk Manag Healthc Policy. 2021;14:1129.
Endalew M, Belay DG, Tsega NT, Aragaw FM, Gashaw M, Asratie MH. Household solid fuel use and associated factors in Ethiopia: a multilevel analysis of data from 2016 Ethiopian Demographic and Health Survey. Environ Health Insights. 2022;16:11786302221095032.
Florey L, Cameron T. Using household survey data to explore the effects of improved housing conditions on malaria infection in children in sub-Saharan Africa. DHS Analytical Studies No. 61. Rockville: ICF International; 2016.
Admasu Y, Alkire S, Scharlin-Pettee S. Multidimensional poverty, gender, and forced displacement: A multi-country, intrahousehold analysis in Sub-Saharan Africa. OPHI Working Papers No. 139. Oxford: Oxford Poverty and Human Development Initiative (OPHI); 2022. p. 1–33. ISSN:2040-8188. ISBN:978-1-912291-30-4.
Mackinnon E, Ayah R, Taylor R, Owor M, Ssempebwa J, Olago LD, et al. 21st-century research in urban WASH and health in sub-Saharan Africa: methods and outcomes in transition. Int J Environ Health Res. 2019;29(4):457–78.
Endalamaw A, Engeda EH, Ekubagewargies DT, Belay GM, Tefera MA. Low birth weight and its associated factors in Ethiopia: a systematic review and meta-analysis. Ital J Pediatr. 2018;44(1):1–12.
Ricciardi C, Guastadisegni C. Environmental inequities and low birth weight. Ann Ist Super Sanita. 2003;39(2):229–34.
Svechkina A, Dubnov J, Portnov BA. Environmental risk factors associated with low birth weight: the case study of the Haifa Bay Area in Israel. Environ Res. 2018;165:337–48.
Campbell OM, Benova L, Gon G, Afsana K, Cumming O. Getting the basic rights–the role of water, sanitation, and hygiene in maternal and reproductive health: a conceptual framework. Tropical Med Int Health. 2015;20(3):252–67.
Tamene A, Habte A, Woldeyohannes D, Tamrat H, Endale F, Eajo T, et al. Water treatment at the point-of-use and treatment preferences among households in Ethiopia: a contemporaneous systematic review and meta-analysis. PLoS One. 2022;17(10): e0276186.
Weber E, Adu-Bonsaffoh K, Vermeulen R, Klipstein-Grobusch K, Grobbee DE, Browne JL, et al. Household fuel use and adverse pregnancy outcomes in a Ghanaian cohort study. Reprod Health. 2020;17(1):1–8.
Demelash H, Motbainor A, Nigatu D, Gashaw K, Melese A. Risk factors for low birth weight in Bale zone hospitals, South-East Ethiopia: a case–control study. BMC Pregnancy Childbirth. 2015;15(1):1–10.
Sanbata H, Asfaw A, Kumie A. Indoor air pollution in slum neighborhoods of Addis Ababa. Ethiopia Atmospheric Environ. 2014;89:230–4.
Tanya Nagahawatte N, Goldenberg RL. Poverty, maternal health, and adverse pregnancy outcomes. Ann N Y Acad Sci. 2008;1136(1):80–5.
Suglia SF, Duarte CS, Sandel MT. Housing quality, housing instability, and maternal mental health. J Urban Health. 2011;88(6):1105–16.
Reddy UM, Davis JM, Ren Z, Greene MF. Opioid use in pregnancy, neonatal abstinence syndrome, and childhood outcomes: executive summary of a joint workshop by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, American Congress of Obstetricians and Gynecologists, American Academy of Pediatrics, Society for Maternal-Fetal Medicine, Centers for Disease Control and Prevention, and the March of Dimes Foundation. Obstet Gynecol. 2017;130(1):10.
Grjibovski A, Bygren LO, Svartbo B, Magnus P. Housing conditions, perceived stress, smoking, and alcohol: determinants of fetal growth in Northwest Russia. Acta Obstet Gynecol Scand. 2004;83(12):1159–66.
Patel R, Gupta A, Chauhan S, Bansod DW. Effects of sanitation practices on adverse pregnancy outcomes in India: a conducive finding from recent Indian demographic health survey. BMC Pregnancy Childbirth. 2019;19(1):1–12.
Greed C. The role of the public toilet: pathogen transmitter or health facilitator? Build Serv Eng Res Technol. 2006;27(2):127–39.
Baker KK, Story WT, Walser-Kuntz E, Zimmerman MB. Impact of social capital, harassment of women and girls, and water and sanitation access on premature birth and low infant birth weight in India. PLoS One. 2018;13(10): e0205345.
Padhi BK, Baker KK, Dutta A, Cumming O, Freeman MC, Satpathy R, et al. Risk of adverse pregnancy outcomes among women practicing poor sanitation in rural India: a population-based prospective cohort study. PLoS Med. 2015;12(7): e1001851.
Aychiluhm SB, Tadesse AW, Mare KU, Abdu M, Ketema A. A multilevel analysis of short birth interval and its determinants among reproductive age women in developing regions of Ethiopia. PLoS One. 2020;15(8): e0237602.
Oljira T, Hailu M. Integrated functional adult education program and its contributions to livelihoods in Ethiopia. Heliyon. 2021;7(8): e07718.
Acknowledgements
We would like to acknowledge the Demographic Health Survey program office for allowing us to access all the relevant DHS data for this study.
Funding
Not Applicable.
Author information
Authors and Affiliations
Contributions
A.T. conceptualized the study and created the initial analytical design, led the interpretation of data, drafting of the manuscript, and led the revision of the intellectual content. A.H. led the literature review, contributed to the design, analysis, and interpretation of data, drafting of the manuscript, and supported the intellectual review of the document. M.T. contributed to the design, analysis, and interpretation of the data, drafting of the manuscript, and supporting revision of the intellectual content. Z.W.S. led the acquisition of data, provided inputs to the methodology, and conducted data analysis. A.A. participated in the drafting of the “Methods” section of the manuscript and review of the versions. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
All methods and procedures were carried out per the relevant guidelines and regulations of the Declaration of Helsinki. The DHS survey report did not include an ethical approval ID, but the authors received written permission from ICF International (DHS office) to access this dataset upon registration with possible justification. The DHS also declared that informed consent was obtained from all subjects and/or their legal guardian during the primary data collection. The retrieved data were only used for the registered research, and data were not shared with anyone other than the co-authors. All data collected by DHS are Institutional Review Board (IRB) certified and this secondary analysis received further IRB approval from the Wachemo University College of Medicine and Health Science Research Determination Committee.
Consent for publication
Not applicable.
Competing interests
We stated that there are no conflicts of interest with any people or groups that might improperly influence or skew the paper's content.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tamene, A., Habte, A., Tagesse, M. et al. Using household survey data to explore the effects of the domiciliary environment on weight at birth: a multilevel mixed-effects analysis of the 2016 Ethiopian Demographic Health Survey. BMC Pregnancy Childbirth 23, 194 (2023). https://doi.org/10.1186/s12884-023-05521-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-023-05521-9