
Abstract
Background
Maternal obesity is the most common medical condition among women of reproductive age worldwide. The pre-pregnancy body mass index and gestational weight gain have been suggested to be associated with maternal mental disorders. This study aimed to investigate the effects of the pre-pregnancy body mass index and gestational weight gain on antenatal depression, stress, and anxiety.
Methods
In total, 4,890 pregnant women were enrolled in the present study, which is based on an ongoing prospective cohort study. We used self-reported pre-pregnancy weights and the last weights measured prior to delivery (using professional instruments) to calculate the pre-pregnancy body mass index and gestational weight gain. The questionnaires used included the Center for Epidemiologic Studies Depression Scale (CES-D), Self-Rating Anxiety Scale (SAS), and 10-item version of the Perceived Stress Scale (PSS-10). We used Pearson product-moment correlation and multivariable logistic regression models to examine the impact of the pre-pregnancy body mass index and gestational weight gain on different maternal mental disorders.
Results
After adjusting for conception, annual household income, occupation, education, smoking status, and drinking status, excessive gestational weight gain during pregnancy was associated with a greater chance of anxiety symptoms in the entire sample (adjusted model: odds ratio = 1.479, 95% confidence interval = 1.128, 1.938) and especially in women with a normal body mass index (adjusted model: odds ratio = 1.668, 95% confidence interval = 1.209, 2.302). However, the relationship between the maternal pre-pregnancy body mass index and mental health was not significant.
Conclusion
Pregnant women with a normal pre-pregnancy body mass index had a greater chance of experiencing anxiety symptoms before delivery if gestational weight gain was excessive; however, its effects on depression or stress symptoms were not observed. The maternal pre-pregnancy body mass index may not be independently associated with maternal mental disorders.
Similar content being viewed by others


Background
Pregnancy is a period of significant neurobiological and psychological changes brought about by physiological hormones, and is usually accompanied by an increase in various negative emotions [1]. Approximately one in five women experience antenatal mental disorders, such as depression and anxiety [2]. Perinatal depression (period prevalence: 18% for prenatal depression and 14% for postpartum depression) is one of the most common psychological problems in pregnant women [3]; its prevalence may be even higher in Asian populations (24.3%) [4]. Perinatal anxiety and stress affect approximately 17% and up to 84% of all women, respectively [5]. A Chinese study revealed that more than 50% of pregnant women have symptoms of anxiety and stress, especially in the late pregnancy and postpartum periods [6].Poor dietary intake and social support, an increased risk of preeclampsia, and pregnancy and labour complications are some harmful consequences of anxiety, depression, and stress during the antenatal period [7]. Furthermore, maternal mental disorders are associated with several adverse foetal and neonatal outcomes, such as low birth weights, preterm births, high rates of diarrhoea, poor breastfeeding practices, infectious illnesses, and poor cognitive development [8].
Maternal obesity is a growing public health concern; in fact, it is the most common medical condition in women of reproductive age worldwide [9].Women who are overweight or obese are more likely to experience excessive gestational weight gain (GWG) and postpartum weight retention [10]. The prevalence of obesity during pregnancy differs according to diverse guidelines [11]. Studies in population-based cohorts have shown that significant ethnic differences in the genetic background, living environment, and lifestyle lead to population-level differences in the body mass index (BMI) and GWG [12]. For instance, according to traditional Chinese customs, pregnant women are frequently required to overeat certain foods and reduce exercise during pregnancy [13]; however, overnutrition and a lack of exercise in mothers may lead to excessive GWG, postpartum weight retention, and macrosomia [14].
Evidence suggests that pre-pregnancy obesity and excessive GWG may increase the risk of adverse mental health outcomes in pregnant women [15,16,17]. Moreover, these factors may also negatively impact a woman’s self-image and self-esteem [18]. Ertel et al. found that pre-pregnancy obesity was associated with elevated depressive symptoms during the postpartum period [19]. A systematic review and meta-analysis also suggested that pre-pregnancy obesity was associated with an increased risk of maternal depressive symptoms and anxiety during pregnancy and in the postpartum period [17]. Kominiarek et al. conducted a survey to evaluate the association between prenatal stress and GWG; their findings suggested that the lowest stress scores were associated with adequate GWG [20]. However, all of these studies have considered a single symptom to measure the mental health of pregnant mothers and have ignored the multiple negative emotions experienced by these women. Stress, anxiety, and depressive symptoms are intercorrelated; their active assessment and management is required in the perinatal period [6].
Understanding the risk factors of perinatal emotion disorders, especially those that can be modified, can improve our ability to identify women at risk and provide additional ways for possible prevention and intervention. To the best of our knowledge, there are few studies (especially those considering racial factors) on the effects of pre-pregnancy BMI and GWG on antenatal mental disorders. In the present study, we aimed to assess the prevalence of pre-pregnancy BMI and GWG in and the sociodemographic characteristics of pregnant Chinese women. We hypothesized that the pre-pregnancy BMI and GWG would predict depression, stress, and/or anxiety symptoms during pregnancy.
Methods
Design and participants
This prospective cohort study was performed as part of the ongoing China National Birth Cohort Study from March 2017 to May 2020. The study design was approved by the Ethics Committee of the International Peace Maternity and Child Health Hospital (affiliated with the Shanghai Jiao Tong University School of Medicine; approval no.: GKLW2016-21).Study participation was voluntary; the patients declared their willingness to participate only after examining the objectives and procedures of the study. All enrolled patients provided written informed consent.
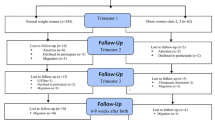
The inclusion criteria were as follows: (i) women planning to seek prenatal care and deliver at the study hospital, (ii) women whose maternity files were established in the hospital, (iii) women with singleton pregnancies, (iv) women who could complete online questionnaires in Chinese, and (v) women willing to sign the consent form. The exclusion criteria were as follows: (i) women aged < 20 years; (ii) women with mental disorders, including depression or anxiety before pregnancy; (iii) women with mental disorders in the first and second trimesters of pregnancy; and (iv) women with serious underlying conditions. After enrolment, structured questionnaires were administered to pregnant women hospitalised for childbirth or before delivery. Thereafter, women with preterm births (i.e., delivery before 37 completed weeks of gestation); those who transferred to another hospital; those with insufficient pre-pregnancy BMI, weight, and height data; and those with other missing data were excluded. The final study sample comprised 4,890 women.
Measurements
BMI and GWG
BMI is a statistical index that is computed using a person’s weight and height; it provides an estimate of the body fat in men and women of any age. Pre-pregnancy BMI was calculated by dividing the participants’ pre-pregnancy weight (in kg) by their height (in m2). Based on the adult BMI classification standards for the Chinese population [21], we categorized our participants into the following four groups using their BMI: underweight (BMI < 18.5 kg/m2), normal weight (18.5 kg/m2 ≤ BMI < 24 kg/m2), overweight (24 kg/m2 ≤ BMI < 28 kg/m2), and obese (BMI ≥ 28 kg/m2).
GWG data were obtained by computing the difference between the last weight measured using professional instruments before delivery in the hospital and the self-reported pre-pregnancy weight. However, there are no official guidelines on GWG for the Chinese population. In the current study, maternal GWG was defined as excessive, adequate, and insufficient. We adopted the Institute of Medicine’s (IOM) recommendation for GWG and defined adequate GWG as being 12.5–18.0 kg, 11.5–16.0 kg, 7.0–11.50 kg, and 5.0–9.0 kg in underweight women, women with normal weight, overweight women, and obese women, respectively [22].
Measurement of depressive symptoms
The Center for Epidemiologic Studies Depression Scale (CES-D) was used to measure the level of depressive symptoms in the enrolled women. The CES-D is a 20-item tool, with each item rated on a 4-point scoring system; the total score ranges from 0 to 60. Higher scores indicated a higher probability of an individual experiencing depression. A cut-off score of 16 was used to determine non-depression/depression in pregnant women and postpartum mothers [23]. The Chinese version of the scale has been reported to have good reliability and validity [24]. The Cronbach’s α was 0.924 in the current study.
Measurement of anxiety symptoms
Anxiety symptoms were assessed using the Self-Rating Anxiety Scale (SAS), which was developed in 1971. It is primarily used to evaluate the severity of an individual’s anxiety. It is a 20-item scale, with each item rated using a 4-level score [25]. Higher scores indicate more severe anxiety symptoms.SAS has been reported to have good reliability and validity in China, and a standardised score of 50 is the upper limit for normative populations [26]. The Cronbach’s α was 0.894 in the current study.
Measurement of perceived stress
Perceived stress was assessed using the 10-item Perceived Stress Scale (PSS-10). Each item was scored on a 5-point scale, with the total score ranging from 0 to 40 [27]. Higher scores indicate higher levels of perceived stress, and scores of 14 or above are indicative of moderate-to-high levels of perceived stress [28]. The Chinese version of this scale has demonstrated good reliability and validity [29]. The Cronbach’s α was 0.833 in the current study.
Assessment of covariates
Several variables were assessed, including age, gestational age at delivery, method of conception, education, occupation, annual household income, parity, place of residence, ethnicity, drinking status, and smoking status. Sociodemographic data were assessed using an interviewer-administered questionnaire before delivery. If the gestational week differed from the delivery gestational week, the researcher manually modified it according to medical records.
Statistical analysis
Descriptive statistics were used to summarise the participants’ characteristics. Continuous variables are expressed as means ± standard deviations, whereas categorical variables are expressed as percentages. An analysis of variance was performed to analyse the differences among the groups. The Chi-square and Fisher exact tests were performed to examine the association between two categorical variables. A Pearson’s correlation coefficient analysis was undertaken as an exploratory analysis to explore the relationship among the pre-pregnancy BMI, GWG, CES-D score, and SAS score. A binary logistic regression was performed to calculate the odds ratios (ORs) and 95% confidence intervals (CIs) for the relationships among the pre-pregnancy BMI, GWG, and risk of exceeding scale thresholds (CES-D, SAS, and PSS-10 scores) in the entire sample. All statistical analyses were two-sided and performed using R version 4.0.5 (R Foundation for Statistical Computing, Vienna, Austria); p < 0.05 indicated statistical significance.
Results
Among 4,890 participants, 999 (20.4%), 2,059 (42.1%), and 1,832 (37.7%) had insufficient, adequate, and excessive GWG, respectively. Furthermore, 53.5% and 43.4% of the participants with an underweight and a normal BMI before pregnancy, respectively, had adequate GWG; conversely, 64.0% and 73.2% of the participants with an overweight and obese BMI before pregnancy had excessive GWG, respectively. Table 1 presents the participants’ demographic data according to the pre-pregnancy BMI categories. No significant differences were observed among the four groups in terms of the place of residence, occupation, ethnicity, smoking status, and drinking status (p > 0.05 for all). Women with pre-pregnancy obesity tended to be younger and had a higher proportion of excessive GWG (all p < 0.05). Significant intergroup differences were observed in terms of conception, annual household income, education, and parity: most women who conceived naturally and were underweight were more likely to have relatively a higher income and education level, and most were nulliparous before this pregnancy.
Table 2 shows a comparison of the scale scores (CES-D, SAS, and PSS-10 scores) among different GWG subgroups according to the total sample and the pre-pregnancy BMI categories. In the total sample and among normal-weight women, the SAS scores were higher in those with excessive GWG than in those with insufficient or adequate GWG (p < 0.001). No such differences were observed among the GWG subgroups for the other pre-pregnancy BMI categories. Furthermore, 7.8% and 7.2% of the patients with normal pre-pregnancy BMI and in the total sample, respectively, had SAS scores ≥ 50. Among women with a normal BMI, the PSS-10 score was higher in those with excessive GWG than in those with insufficient and adequate GWG. No such differences were observed among the GWG subgroups for the other pre-pregnancy BMI categories. Furthermore, the likelihood of the PSS-10 score being ≥ 14 was higher in both the total sample and in women with a normal BMI than in the women from the other BMI categories. Conversely, the CES-D score did not differ significantly among the GWG subgroups in all the pre-pregnancy BMI categories (all p > 0.05).
Low correlations were observed among the pre-pregnancy BMI, GWG, and the three scale scores. No significant association was found among the PSS-10 score, SAS score, and pre-pregnancy BMI (all p > 0.05). However, a strong correlation was found between the CES-D and SAS scores (rho = 0.77, p < 0.05), CES-D and PSS-10 scores (rho = 0.74, p < 0.05), and SAS and PSS-10 scores (rho = 0.63, p < 0.05).This indicates that the three scale scores were positively correlated with each other (See Fig. 1 for details).

Correlation heat map of pre-pregnancy BMI, GWG, and the three scale scores
A logistic regression analysis was performed to explore the relationship between GWG and maternal mental disorders (Table 3). Excessive GWG was found to be associated with exceeding the SAS score threshold in the entire sample (OR = 1.535; 95% CI = 1.173, 2.008). After adjusting for potential confounders, excessive GWG was also found to be associated with a greater chance of anxiety symptoms in the entire sample (OR = 1.479; 95% CI = 1.128, 1.938).
Another logistic regression analysis was performed to explore the relationship between GWG and depression, anxiety, and stress according to the pre-pregnancy BMI. Excessive GWG significantly increased the possibilities of anxiety in both the unadjusted and adjusted models (unadjusted model: OR = 1.767, 95% CI = 1.284, 2.431; adjusted model: OR = 1.668, 95% CI = 1.209, 2.302). Conversely, excessive GWG was significantly associated with the chance of exceeding the PSS-10 score thresholds in the unadjusted model (OR = 1.227; 95% CI = 1.033, 1.459) but not in the adjusted model (OR = 1.151; 95% CI = 0.966, 1.372).
Discussion
The main purpose of our study was to explore the impact of pre-pregnancy BMI and GWG on the psychological state of women. The most important finding of this study is that excessive GWG is strongly associated with greater chances of exceeding the SAS score thresholds in pregnant Chinese women with a normal pre-pregnancy BMI, while in no other category were the results significant.No effects of GWG on depression or stress symptoms were observed. In other words, pregnant women with normal weight before pregnancy are more likely to have anxiety symptoms if they gain too much weight during pregnancy. We did not find a strong association between the pre-pregnancy BMI and the perinatal psychological status. These findings suggest that avoiding excessive GWG can reduce the incidence of anxiety in pregnant women with a normal pre-pregnancy weight.
In the present study, excessive GWG did not affect the women’s stress and depression during pregnancy but aggravated their anxiety. Currently, the conclusions of various relevant studies are not consistent, which indicates that the relationship between GWG and prenatal anxiety, depression, and stress is complex and variable. Ertel et al. did not observe an association between GWG and prenatal depressive symptoms [19]. A study of 505 pregnant women showed that excessive gestational weight gain independently predicted greater postpartum depressive symptoms [16]. In a study focusing on the relationship between stress and GWG, the researchers believed that there might be evidence of an association between stress and maternal body weight and weight gain [30]. Eichler et al. found that GWG was significantly positively linked to stress only during the second trimester [31].The inconsistency in the reported findings can be explained by the following: (1) most of the evidence is based on self-reported body weight and height, which is associated with a higher potential for misclassification (when compared with prospective measurement of maternal BMI) [32] and (2) as a limitation of most studies, the analysed women underestimated their pre-pregnancy weight and overestimated their GWG [33].
Nevertheless, in our study, the negative effect of excessive GWG on perinatal anxiety could not be ignored. We found that women with normal pre-pregnancy weight in our study were at a greater chance of experiencing anxiety symptoms due to excessive GWG. The number of studies on anxiety and weight gain is rather small; however, the findings of some studies are consistent with our findings. Systematic literature suggests that obese pregnant women are at a higher risk of developing comorbid anxiety disorders [34]. Zanardo et al. indicate that women who experienced excessive GWG have a higher risk of developing anxiety [35]. In our study, the finding relates only to women who had normal pre-pregnancy nutritional status. A possible explanation is that women with normal weight before pregnancy receive less relevant education than women with substandard pre-pregnancy weight do; adequate health consultation can positively impact the lifestyle and dietary structure of pregnant women [36]. As healthcare providers tend to focus more on women with obesity [37], women with a normal pre-pregnancy weight may not be able to control their weight correctly in the absence of proper guidance. It is conceivable that women entering pregnancy at an underweight or normal-weight BMI may find the associated changes in body shape more difficult to accept [38]. Studies showed body dissatisfaction might have negative outcomes, including anxiety or feeling stressed, poor self-esteem, isolation, and social anxiety [39, 40]. Another explanation of how GWG affects maternal mental health is inflammatory markers. The study indicated that excessive GWG was associated with higher concentrations of inflammatory factors [41], and inflammation has been implicated in anxiety [42]. Thus, while paying attention to obese or overweight pregnant women, we should also provide adequate advice and health guidance to women with normal pre-pregnancy weights.
At the same time, it should be noted that the incidence of perinatal anxiety was relatively low in our study as compared to in previous studies; these previous studies have revealed that 15–30% of pregnant women have clinically significant levels of anxiety [43, 44]. With an SAS score of 50 as the cut-off, only 5.9% of the women were diagnosed with anxiety. Furthermore, 7.8% of women with a normal pre-pregnancy weight and excessive GWG were diagnosed with anxiety symptoms. The large difference in the incidence may also explain the inconsistencies in the reported effects of GWG on prenatal anxiety among different studies.
Our hypothesis that pre-pregnancy BMI was associated with depression, stress, and/or anxiety symptoms during pregnancy was not supported by our data; this is consistent with the findings of other studies. McPhie et al. reported that pre-pregnancy BMI could not predict depressive or anxiety symptoms [45]. However, there are conflicting findings regarding pre-pregnancy and antenatal mental disorders. A systematic review and meta-analysis of the impact of pre-pregnancy BMI on maternal depressive and anxiety symptoms revealed positive associations between pre-pregnancy weight and depression and anxiety [17]. Another study evaluating the prevalence and risk of antenatal mental disorders among obese and overweight women claimed that women who were obese when they became pregnant were more likely to experience elevated antenatal mental health problems [46].
To date, existing findings on the relationship between BMI and mental disorders during pregnancy are inconsistent, and the causal direction of the relationship between obesity and mental health problems in pregnant women is unclear. This inconsistency may be related to the differences in the methodologies adopted (including evaluation instruments and definitions) [47] and to the differences in the adjustments for confounding factors across the studies. In our study, the method of conception, annual household income, occupation, parity, and education were important confounding factors; 68.5% of the participants’ families had a higher annual income, 75.8% of the participants had a bachelor’s degree at the very least, and only 10.5% of the participants were unemployed. In a similar study from Australia, only 61.3% of the women had a Bachelor’s or Master’s degree [47], while Cheng et al. reported that 25% of their participants were unemployed [6]. A community-based cross-sectional study in Aligarh also found that the prevalence of maternal mental disorders was significantly higher among mothers who were part of a higher age group, who belonged to a low socioeconomic class, who had no educational background or had a lower level of education, who were housewives, and who had higher parity [48]. Moreover, social and cultural factors may also affect the body image, weight satisfaction, and weight-gain attitudes of the women [19].
In the present study, only 41.93% of the women met the IOM recommendations and gained an adequate gestational weight; however, as the pre-pregnancy BMI increased, this proportion decreased gradually and the proportion of excessive GWG increased gradually. It is particularly concerning that current evidence shows that up to 64% of overweight women and 73.2% of obese women have GWG that exceeds the GWG currently recommended by IOM; this is consistent with our findings [49, 50]. Healthcare providers should calculate the pre-pregnancy BMI of pregnant women at their first prenatal visit, so that they can provide optimal diet and exercise counselling for achieving the IOM-recommended GWG.
We also noticed positive correlations among the perceptions of depression, anxiety, and stress. Previous studies have proposed that perceived stress, anxiety, and depression are strongly correlated with pregnancy [51, 52]. Several comorbidities may exist among maternal mental disorders. Dindo et al. found high rates of co-occurrence of anxiety and stress disorders in women with depression [53]. Because of this increasing emphasis on screening for comorbidities during pregnancy, it is necessary to further study depression, stress, and anxiety as comorbidities as well.
To the best of our knowledge, this study included the largest sample to date to explore the relationship among the pre-pregnancy BMI, GWG, and maternal mental health in the Chinese population. However, our study has some limitations. First,although the weight during pregnancy was measured using professional measuring machines, the pre-pregnancy weight was self-reported; this may have led to some potential misclassification. Second, some major complications, such as gestational diabetes mellitus, hypertension disorders, and thyroid dysfunction, were not evaluated in our study, even though these are important confounders in the evaluation of maternal mental disorders. Finally, assessments of mental health were derived from self-reported questionnaires, which may be susceptible to measurement bias.
Conclusion
This large prospective cohort study demonstrated that women with normal weight before pregnancy are more likely to have anxiety symptoms if they gain too much weight during pregnancy. However, our findings did not indicate a strong association between the pre-pregnancy BMI and the perinatal psychological status. Instead, our findings suggest that excessive GWG is associated with antenatal anxiety,in women with a normal pre-pregnancy weight. Thus, such women should receive sufficient attention and health guidance, because poor weight control during pregnancy might aggravate their anxiety symptoms. More than 50% of the women in our study did not meet the IOM standards for adequate GWG. In the future, larger longitudinal studies are needed to explore the biological mechanisms linking GWG with maternal mental health. Screening and interventions should be performed to identify women at a high risk of excess GWG relatively early in pregnancy to prevent the occurrence of mental disorders.
Data Availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
Body mass index
- CES-D:
-
Center for Epidemiologic Studies Depression Scale
- CI:
-
Confidence interval
- GWG:
-
Gestational weight gain
- HPA:
-
Hypothalamic pituitary adrenal
- IOM:
-
Institute of Medicine
- OR:
-
Odds ratio
- PSS-10:
-
10-item version of the Perceived Stress Scale
- SAS:
-
Self-Rating Anxiety Scale
- SD:
-
Standard deviation
References
Penner F, Rutherford HJV. Emotion regulation during pregnancy: a call to action for increased research, screening, and intervention. Arch Womens Ment Health. 2022;25(2):527–31.
Simpson KR. Maternal Mental Health. MCN: The American Journal of Maternal/Child Nursing. 2022;47(1):59.
Gavin NI, Lohr KN, Meltzer-Brody, Gartlehner S, Swinson G, Lohr K et al. perinatal depression: a systematic review of prevalence and incidence rti author awards series. 2019.
Mahendran R, Puthussery S, Amalan M. Prevalence of antenatal depression in South Asia: a systematic review and meta-analysis.Journal of Epidemiology & Community Health. 2019.
McCarthy M, Houghton C, Matvienko-Sikar K. Women’s experiences and perceptions of anxiety and stress during the perinatal period: a systematic review and qualitative evidence synthesis. BMC Pregnancy Childbirth. 2021;21(1):811.
Cheng CY, Chou YH, Chang CH, Liou SR. Trends of Perinatal Stress, Anxiety, and Depression and Their Prediction on Postpartum Depression.Int J Environ Res Public Health. 2021;18(17).
Nisar A, Yin J, Waqas A, Bai X, Wang D, Rahman A, et al. Prevalence of perinatal depression and its determinants in Mainland China: a systematic review and meta-analysis. J Affect Disord. 2020;277:1022–37.
Montagnoli C, Zanconato G, Cinelli G, Tozzi AE, Bovo C, Bortolus R, et al. Maternal mental health and reproductive outcomes: a scoping review of the current literature. Arch Gynecol Obstet. 2020;302(4):801–19.
Davis AM. Collateral damage: maternal obesity during pregnancy continues to rise. Obstet Gynecol Surv. 2020;75(1):39–49.
Campbell EE, Dworatzek PD, Penava D, de Vrijer B, Gilliland J, Matthews JI, et al. Factors that influence excessive gestational weight gain: moving beyond assessment and counselling. J Matern Fetal Neonatal Med. 2016;29(21):3527–31.
Vitner D, Harris K, Maxwell C, Farine D. Obesity in pregnancy: a comparison of four national guidelines. J Matern Fetal Neonatal Med. 2019;32(15):2580–90.
Walter S, Mejía-Guevara I, Estrada K, Liu SY, Glymour MM. Association of a genetic risk score with body Mass Index Across different birth cohorts. JAMA. 2016;316(1):63–9.
Withers M, Kharazmi N, Lim E. Traditional beliefs and practices in pregnancy, childbirth and postpartum: a review of the evidence from asian countries. Midwifery. 2018;56:158–70.
Poston L, Caleyachetty R, Cnattingius S, Corvalán C, Uauy R, Herring S, et al. Preconceptional and maternal obesity: epidemiology and health consequences. Lancet Diabetes Endocrinol. 2016;4(12):1025–36.
Bodnar LM, Wisner KL, Moses-Kolko E, Sit DKY, Hanusa BH. Prepregnancy Body Mass Index, Gestational Weight Gain, and the likelihood of major depressive disorder during pregnancy. J Clin Psychiatry. 2009;70(9):1290–6.
Cunningham SD, Mokshagundam S, Chai H, Lewis JB, Levine J, Tobin JN, et al. Postpartum depressive symptoms: Gestational Weight Gain as a risk factor for adolescents who are overweight or obese. J Midwifery Women’s Health. 2018;63(2):178–84.
Dachew BA, Ayano G, Betts K, Alati R. The impact of pre-pregnancy BMI on maternal depressive and anxiety symptoms during pregnancy and the postpartum period: a systematic review and meta-analysis. J Affect Disord. 2021;281:321–30.
Silveira ML, Ertel KA, Dole N, Chasan-Taber L. The role of body image in prenatal and postpartum depression: a critical review of the literature. Arch Womens Ment Health. 2015;18(3):409–21.
Ertel KA, Huang T, Rifas-Shiman SL, Kleinman K, Rich-Edwards J, Oken E, et al. Perinatal weight and risk of prenatal and postpartum depressive symptoms. Ann Epidemiol. 2017;27(11):695–700e1.
Kominiarek MA, Grobman W, Adam E, Buss C, Culhane J, Entringer S, et al. Stress during pregnancy and gestational weight gain. J Perinatol. 2018;38(5):462–7.
Bei-Fan Z, Cooperative Meta Anal Grp W. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in chinese adults: study on optimal cut-off points of body mass index and waist circumference in chinese adults. Asia Pac J Clin Nutr. 2002;11:685–S93.
Institute of M, National Research Council Committee to Reexamine IOMPWG. The National Academies Collection: Reports funded by National Institutes of Health. In: Rasmussen KM, Yaktine AL, editors. Weight Gain During Pregnancy: Reexamining the Guidelines. Washington (DC): National Academies Press (US) Copyright © 2009, National Academy of Sciences.; 2009.
Radloff LS, The CES-D, Scale. A self-report Depression Scale for Research in the General Population. Appl Psychol Meas. 1977;1(3):385–401.
Yang L, Jia CX, Qin P. Reliability and validity of the Center for epidemiologic Studies Depression Scale (CES-D) among suicide attempters and comparison residents in rural China. BMC Psychiatry. 2015;15:76.
Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–9.
Huang Z, Hao J, Su P, Huang K, Xing X, Cheng D, et al. The impact of prior abortion on anxiety and depression symptoms during a subsequent pregnancy: data from a Population-Based Cohort Study in China. Klinik Psikofarmakoloji Bülteni-Bulletin of Clinical Psychopharmacology. 2016;22(1):51–8.
Cohen S, United States. Perceived stress in a probability sample of the. The social psychology of health. The Claremont Symposium on Applied Social Psychology. Thousand Oaks, CA, US: Sage Publications, Inc; 1988. p. 31–67.
Alharbi H, Alshehry A. Perceived stress and coping strategies among ICU nurses in government tertiary hospitals in Saudi Arabia: a cross-sectional study. Ann Saudi Med. 2019;39(1):48–55.
Mao Q, Zhu L-x. Su X-y. A comparison of postnatal depression and related factors between chinese new mothers and fathers. J Clin Nurs. 2011;20(5–6):645–52.
Braig S, Logan CA, Reister F, Rothenbacher D, Genuneit J. Psychosocial stress and longitudinally measured gestational weight gain throughout pregnancy: the Ulm SPATZ Health Study. Sci Rep. 2020;10(1):1996.
Eichler J, Schmidt R, Hiemisch A, Kiess W, Hilbert A. Gestational weight gain, physical activity, sleep problems, substance use, and food intake as proximal risk factors of stress and depressive symptoms during pregnancy. BMC Pregnancy Childbirth. 2019;19(1):175.
Hartley E, McPhie S, Skouteris H, Fuller-Tyszkiewicz M, Hill B. Psychosocial risk factors for excessive gestational weight gain: a systematic review. Women Birth. 2015;28(4):e99–e109.
Headen I, Cohen AK, Mujahid M, Abrams B. The accuracy of self-reported pregnancy-related weight: a systematic review. Obes Rev. 2017;18(3):350–69.
Nagl M, Linde K, Stepan H, Kersting A. Obesity and anxiety during pregnancy and postpartum: a systematic review. J Affect Disord. 2015;186:293–305.
Zanardo V, Giliberti L, Giliberti E, Grassi A, Perin V, Parotto M, et al. The role of gestational weight gain disorders in symptoms of maternal postpartum depression. Int J Gynaecol Obstet. 2021;153(2):234–8.
Vinturache A, Winn A, Mannion C, Tough S. Women’s recall of health care provider counselling on gestational weight gain (GWG): a prospective, population-based study. BMC Pregnancy Childbirth. 2019;19(1):136.
Weeks A, Liu RH, Ferraro ZM, Deonandan R, Adamo KB. Inconsistent weight communication among prenatal Healthcare Providers and Patients: a narrative review. Obstet Gynecol Surv. 2018;73(8):423–32.
Andrews B, Hill B, Skouteris H. The relationship between antenatal body attitudes, pre-pregnancy body mass index, and gestational weight gain. Midwifery. 2018;56:142–51.
Shoraka H, Amirkafi A, Garrusi B. Review of body image and some of contributing factors in Iranian Population. Int J Prev Med. 2019;10:19.
Alleva JM, Sheeran P, Webb TL, Martijn C, Miles E. A Meta-Analytic review of stand-alone interventions to improve body image. PLoS ONE. 2015;10(9):e0139177.
Hrolfsdottir L, Schalkwijk CG, Birgisdottir BE, Gunnarsdottir I, Maslova E, Granstrom C, et al. Maternal diet, gestational weight gain, and inflammatory markers during pregnancy. Obes (Silver Spring). 2016;24(10):2133–9.
Peirce JM, Alvina K. The role of inflammation and the gut microbiome in depression and anxiety. J Neurosci Res. 2019;97(10):1223–41.
Dennis CL, Falah-Hassani K, Shiri R. Prevalence of antenatal and postnatal anxiety: systematic review and meta-analysis. Br J Psychiatry. 2017;210(5):315–23.
Yatziv T, Vancor EA, Bunderson M, Rutherford HJV. Maternal perinatal anxiety and neural responding to infant affective signals: insights, challenges, and a road map for neuroimaging research. Neurosci Biobehav Rev. 2021;131:387–99.
McPhie S, Skouteris H, Fuller-Tyszkiewicz M, Hill B, Jacka F, O’Neil A. Relationships between mental health symptoms and body mass index in women with and without excessive weight gain during pregnancy. Midwifery. 2015;31(1):138–46.
Molyneaux E, Poston L, Ashurst-Williams S, Howard LM. Pre-pregnancy obesity and mental disorders during pregnancy and postpartum: a systematic review and meta-analysis. Pregnancy Hypertens. 2014;4(3):236.
Holton S, Fisher J, Nguyen H, Brown WJ, Tran T. Pre-pregnancy body mass index and the risk of antenatal depression and anxiety. Women Birth. 2019;32(6):e508–e14.
Naaz N, Mehnaz S, Ansari MA, Amir A. Maternal mental health and its determinants - a community-based cross-sectional study in Aligarh, Uttar Pradesh. Indian J Public Health. 2021;65(1):16–21.
Faucher MA, Barger MK. Gestational weight gain in obese women by class of obesity and select maternal/newborn outcomes: a systematic review. Women Birth. 2015;28(3):e70–9.
Gavard JA, Artal R. The association of gestational weight gain with birth weight in obese pregnant women by obesity class and diabetic status: a population-based historical cohort study. Matern Child Health J. 2014;18(4):1038–47.
Ahmed A, Feng C, Bowen A, Muhajarine N. Latent trajectory groups of perinatal depressive and anxiety symptoms from pregnancy to early postpartum and their antenatal risk factors. Arch Womens Ment Health. 2018;21(6):689–98.
Razurel C, Kaiser B, Antonietti JP, Epiney M, Sellenet C. Relationship between perceived perinatal stress and depressive symptoms, anxiety, and parental self-efficacy in primiparous mothers and the role of social support. Women Health. 2017;57(2):154–72.
Dindo L, Elmore A, O’Hara M, Stuart S. The comorbidity of Axis I disorders in depressed pregnant women. Arch Womens Ment Health. 2017;20(6):757–64.
Acknowledgements
We would like to express our gratitude to all participants, doctors, and staff who participated in the China National Birth Cohort Study. We would like to thank Editage (www.editage.cn) for English language editing.
Funding
This work was supported by The National Key Research and Development Program of China. Grant number: 2016YFC1000203; Shanghai Jiao Tong University School of Medicine: Nursing Development Program. The funding bodies had no role in the collection, analysis, or interpretation of the data, the study design, or the writing of the manuscript.
Author information
Authors and Affiliations
Contributions
XZ collected and analysed the data and contributed to the writing of the report. LR conducted the program and conceptualized and developed the study. DJY contributed to data analysis. TW contributed to the writing of the report. HL designed the study, investigated existing literature, and reviewed the writing of the manuscript. ZWL conducted the validation, provided supervision, and acquired funding. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study design was approved by the Ethics Committee of the International Peace Maternity and Child Health Hospital (affiliated with the Shanghai Jiao Tong University School of Medicine; approval no.: GKLW2016-21). All the experiments in our study were conducted with accordance to the Declaration of Helsinki. The participants declared their willingness with participate only after examining the objectives and procedures of the study; all enrolled patients provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: LZ reports financial support was provided by The National Key Research and Development Program of China. ZX reports financial support was provided by Shanghai Jiao Tong University School of Medicine.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhou, X., Rao, L., Yang, D. et al. Effects of maternal pre-pregnancy body mass index and gestational weight gain on antenatal mental disorders in China: a prospective study. BMC Pregnancy Childbirth 23, 188 (2023). https://doi.org/10.1186/s12884-023-05502-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-023-05502-y