
Abstract
Background
Previous research is inconclusive on the effects of mode of delivery on maternal health-related quality-of-life (HRQoL). We conducted a systematic review and meta-analysis to assess the current evidence for associations between mode of delivery and postpartum health-related quality-of-life.
Methods
Electronic databases MEDLINE ALL (OVID), Web of Science, The Cochrane Library, CINAHL and EMBASE (OVID) were searched for English written articles investigating the relationship between mode of delivery and quality-of-life published form inception to 15th October 2020. Two reviewers independently screened titles and abstracts, assessed full texts, and extracted data. Meta-analysis was conducted where possible.
Results
Twenty-one studies, including 19,879 women, met the inclusion criteria. A meta-analysis of 18 studies found HRQoL scores were significantly higher for women after vaginal delivery in comparison to caesarean (emergency and elective combined) (Effect Size (ES) 0.17, 95% CI 0.01–0.25, n = 7665) with highest scores after assisted vaginal delivery (ES 0.21, 95% CI 0.13–0.30, n = 2547). Physical functioning (ES 11.18, 95% CI = 2.29–20.06, n = 1746), physical role (ES 13.10, 95% CI = 1.16–25.05, n = 1471), vitality (ES 6.31, 95% CI = 1.14–10.29, n = 1746) and social functioning (ES 5.69, 95% CI = 1.26–10.11, n = 1746) were significantly higher after vaginal delivery compared to caesarean.
Conclusions
Health-related quality-of-life scores were higher for women after vaginal delivery in comparison to caesarean section. Consequently, women should be encouraged to deliver vaginally where possible. The findings of this research should be available to the relevant population to help support informed choice.
Similar content being viewed by others

Background
Childbirth is a major event in a woman’s life, that for many, brings significant health problems. Following birth she must recover from these whilst learning to feed and care for her newborn [1]. Whilst puerperal changes are expected to be complete within the first 6 weeks after childbirth [2] many women experience postnatal morbidities for extended periods [3,4,5]. Furthermore, many of these morbidities can go undetected and untreated [4, 5]. The journey to recovery is important as it impacts on the mother’s health-related quality-of-life (HRQoL) and the health of the baby [4, 5].
HRQoL is a multidimensional measure of health from the individual’s perspective. It focuses on the physical, emotional and social impact that diseases have on individuals and accounts for their goals, expectations, standards and concerns [5,6,7,8]. HRQoL has increasing importance within healthcare for its ability to estimate well-being, the impact of disease and the cost-effectiveness of interventions [5, 7, 9]. Evidence shows HRQoL is a valid measure of maternal health [5, 10].
Mode of delivery is an influential factor on postpartum HRQoL [11, 12]. Caesarean section (CS) rates are increasing with more women requesting an elective caesarean for personal and societal reasons, yet whether such perceived benefits continue after birth is debated [13,14,15]. Two recent reviews have explored the effects of delivery modes on HRQoL though their findings contradict [16, 17]. One study reported that HRQoL was higher in women with vaginal delivery (VD) than CS [16], whilst another found no significant difference in HRQoL between the delivery types [17]. Methodological differences between the studies may explain the contradictory findings. To our knowledge there is no paper that reviews the effects of delivery mode on HRQoL to include non-Asian populations in any period of time. This review aims to close this literature gap by systematically reviewing published literature on the association between HRQoL in postpartum women and mode of delivery.
Methods
The protocol for this review is registered on PROSPERO (CRD42020145090).
Search strategy
A systematic search of the electronic databases MEDLINE ALL (OVID) (which covers the main Medline database, Medline Daily and Medline EPub Ahead of Print, In Process, In Data Reviews and Other Non-Indexed Citations, PubMed-not-Medline), Web of Science (SCI-EXPANDED, SSCI and ESCI), The Cochrane Library (Cochrane reviews and Cochrane Central Register of Controlled Trials), CINAHL and EMBASE (OVID) was conducted on 10th November 2019 and updated on 15th October 2020. No date limit was applied, and filters excluded non-English language studies as translation resources were unavailable. The search strategy included full, truncated, and MeSH terms pertaining to mode of delivery (vaginal and caesarean), childbirth, HRQoL and QoL measures (Additional file 8). Reference lists of systematic reviews and included studies were also screened for potential studies. A specialist librarian (SJ) supported the search strategy.
Eligibility criteria
Eligible studies included full text journal articles that reported overall HRQoL scores as a primary outcome, and that specified and stratified by mode of delivery. Observational studies of any design were considered appropriate for inclusion. Validated Quality of Life (QoL) tools must have been evidenced. The eligible population included women of reproductive age (15–49 years) who had experienced vaginal or caesarean delivery, including those with other health conditions (e.g., diabetes, gestational diabetes). Studies in restricted populations (e.g., critically ill (a life-threatening process that can result in mortality or significant morbidity [18])) were excluded as they are not representative of the general population.
Study selection and data extraction
Titles and abstracts were independently reviewed by two authors (KE, HF/OO). All abstracts identified were retained for full-text assessment. Reasons were noted for exclusion. Any disagreements during study selection were resolved by referral to a third author (LAK). References of selected articles were reviewed to identify any other eligible studies. Two reviewers (KE, HF/ OO) independently extracted data from included studies using a piloted electronic data abstraction form (Additional file 9). Extracted data pertained to study location, study design, population, delivery mode, HRQoL tool, mean HRQoL scores, and follow-up.
Quality appraisal
Two reviewers (KE, HF/ OO) independently undertook quality appraisal, resolving disagreements through discussion or referral to an independent reviewer (LAK). The Cochrane Risk of Bias In Non-Randomized Studies-of Interventions (ROBINS-I) tool was used to assess the quality of all studies [19]. Studies were assessed for sources of potential bias including method of recruiting participants, sample size, validated outcome measures, confounders, loss to follow-up and type of analysis.
Data summary, synthesis and statistical analysis
Studies included were assessed using the Robin’s tool which includes seven domains using a high, low or unclear scale [19]. Random-effects meta-analyses were conducted using STATA SE Version 16.1 to calculate the standardised mean difference of overall HRQoL scores. Consistent measurement tools across studies for explanatory outcomes (component and dimension scores) allowed a mean difference analysis. Findings were presented using a forest plot. Due to lack of studies in the spontaneous vaginal delivery (SVD) group, SVD and assisted/ instrumental vaginal delivery (AVD/ IVD) were clustered into a single ‘vaginal delivery (VD)’ group. The weighted mean and normal distribution were used to produce the standard deviation of outcome measurements as if the combined group had never been divided into two [20]. Analysis of caesarean section included both elective and emergency caesarean sections resultant of the study data available. This review intended to pool data across measurement tools. However, the tools constructs were too divergent, so data were pooled according to individual tool type. Hedges g test was conducted to measure the effect size (ES) where measurement tools were different. Mean difference (unstandardized) was used to measure the effect size where measurement tools were the same. Effect sizes greater than 0 were considered to indicate greater HRQoL improvement in vaginal delivery than caesarean section. Egger’s test was used to assess publication bias. Meta-regression was used to explore heterogeneity and investigate the relationship between effect size of sample size (small study bias), study design, year of study (trend analysis) and location. Results were summarized using bubble plots. The cut-off date for assigning studies to ‘earlier’ and ‘recent’ groups for the study year subgroup analyses was 2016. This date was chosen to capture any recent effects not measured by previous reviews [16, 17]. Heterogeneity was assessed using the I2 statistic and considered low, moderate, and high at values of 25, 50, and 75% respectively [21].
Studies that were statistically incomparable were narratively summarized.
Results
Searching, sifting, and sorting
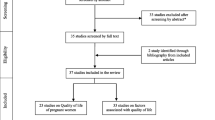
The search of five databases identified 2501 unique records on 10th November 2019. An updated search on 15th October 2020 yielded 557 unique records. Following title and abstract sifting 146 articles were assessed for eligibility and 21 were eligible for inclusion. The main reason for exclusion was irrelevant outcomes (i.e., delivery modes not compared or QoL not reported by birth mode). Authors were contacted where information was unclear. Unavailable full text articles were excluded. The PRISMA diagram (Fig. 1) provides details of exclusions at each stage and reasons for full text exclusions can be found in Additional file 1.

PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers, and other sources [22]
Characteristics of included studies
Twenty-one studies met the inclusion criteria and were included within the review. The studies were conducted between 2007 and 2019 across 39 countries with no particular geographical pattern. The most common locations were Bangladesh, China, Germany, Italy, India, Iran, Ireland, Spain, Turkey, and the United Kingdom (UK). Two studies were multi-country studies of which one study was conducted across 25 locations [23]. The sample size of included studies was 19,879 women. Study samples ranged from 130 to 2990 (median = 400). Timepoints for assessment of outcomes ranged between 12 h and 10 years (median = 2 months) postpartum, with diverse study durations (narrowest 12–24 h [24], widest ≤1 yr- ≥ 10 yrs. [25]). The youngest maternal age was 15 and the oldest 49 years [26, 27]. Birth modes were grouped differently. Vaginal were categorised as spontaneous (SVD, n = 10), assisted (AVD, n = 5) and vaginal (VD, n = 2). Caesarean sections were mostly reported as a whole group (CS, n = 11) although two studies reported elective (ElCS) and emergency caesarean section (EmCS) separately [24, 28]. HRQoL tools included the Medical Outcome Short Form (SF-6D,12&36, n = 11), European Quality of Life Five Dimension Scale (EQ-5D, n = 3) and World Health Organization Quality of Life (WHOQOL-BREF, n = 3). One study used a disease-specific measure: The Mother-Generated Index (MGI) [29]. Where authors specified validation of QoL the tools were considered accepted validated measures in this review.
Eighteen studies were meta-analysed, of which eleven provided overall HRQoL scores, four reported SF-36 summary scores: Physical Component Summary (PCS) and Mental Component Summary (MCS), and eight reported SF-36 dimensions. Three studies were narratively synthesised following due to their unique tool [30], or incomparable dimensions [27, 31]. Full characteristics are shown in Additional file 2.
Risk of bias assessment
The main limitation, effecting 67% of studies, was inadequate confirmation or a lack of consideration of confounding variables potentially leading to selection bias (Fig. 2). This is particularly an issue for studies with small sample sizes spread across multiple settings, like Kavosi et al. [32]. Studies were checked for control of the following variables: parity, labor induction, analgesics, hospital setting, preterm birth, birth weight and gestational age. Three studies adjusted for confounders outside this scope including age, education, and employment status [23, 25, 33]. One study adjusted for some, but not all, of the specified confounders listed in their analyses. Full details of the risk of bias assessment are provided in Additional file 3.

Risk of Bias criteria assessment according to the Robins tool [19]
Overall HRQoL
Statistical analysis of overall HRQoL scores between vaginal delivery and caesarean section
Twelve studies were initially statistically analysed comparing overall HRQoL scores between vaginal delivery and caesarean section groups. Pooled analysis found vaginal delivery had statistically higher HRQoL than caesarean section (ES 0.26, 95% CI = 0.04–0.48, n = 10,040, 12 studies) (Fig. 3) [11, 26, 29, 31, 34,35,36,37,38,39,40]. However, the vaginal delivery group had high heterogeneity (I2 = 99.39%). This was caused by one study [37], whose means were considerably higher than the other studies pooled. This outlying study was removed, leaving one study remaining in the VD group thus unable to be pooled (Fig. 3) [31]. Consequently, both studies were analysed narratively [31, 37]. Ten studies were subsequently meta-analysed reporting the estimated overall standardized mean difference was statistically significant (ES 0.17, 95% CI 0.01–0.25, n = 7665, 10 studies) showing HRQoL was higher for VD than CS (Fig. 4) [11, 26, 29, 34,35,36, 38,39,40]. There was medium heterogeneity (60.1%) due to variation between studies rather than within-study sampling (Q = 32.27, p = 0.00).

Forest plot of random effects meta-analysis of studies assessing overall HRQoL score stratifying by delivery type, outliers included

Forest plot of random effects meta-analysis of studies assessing overall HRQoL score stratifying by delivery type, outliers removed
Statistical analysis of overall HRQoL scores and vaginal delivery
Both vaginal subgroups, SVD and AVD, reported significantly higher HRQoL comparted to CS (ES 0.15, 95% CI = 0.04–0.26, n = 5118, 10 studies vs ES 0.21, 95% CI 0.13–0.30, n = 2547, 5 studies respectively) (Fig. 4) [11, 26, 29, 34,35,36, 38,39,40]. Variation between SVD studies was high (I2 = 72.85%) whereas AVD studies were harmonious (I2 = 0.00%). A meta-regression showed SVD had a negative non-significant relationship with AVD, therefore no stratified analysis was conducted (− 0.76, 95% CI = -0.24–0.09).
Subgroup analysis
To investigate heterogeneity subgroup analyses on study year, sample size, design and location was conducted. Results showed a significant association between delivery mode and HRQoL from 2016 onwards (ES 0.23, 95% CI = 0.17–0.30, n = 5274, 6 studies) [11, 34, 36, 38, 39, 41], but not prior (ES 0.06, 95% CI = -0.06–0.19, n = 3291, 4 studies) [26, 29, 35, 40] (Fig. 5). Meta-regression confirmed a small increase in effect in recent studies (0.02, p = 0.01). Chronological analysis revealed study results have been consistent since 2009, almost identical since 2018 showing that HRQoL has been significantly higher for women who delivered vaginally for over a decade (Fig. 6).

Forest plot of random effects meta-analysis of studies assessing overall HRQoL score stratified by earlier and recent studies

Forest plot studies assessing overall HRQoL score reporting effect size stratified by date of study
Sample size had no direct impact on effect size (0.00, p = 0.66) evidencing results were not inflated and there was evidence of publication bias (0.55, p = 0.67).
Study design
The effect size was higher in prospective studies (ES 0.21, 95% CI = 0.08–0.34, n = 1649, 4 studies) [11, 28, 39, 42] than cross-sectional studies (ES 0.15, 95% CI = 0.05–0.25, n = 6016, 6 studies) [26, 29, 35, 36, 38, 41] (Fig. 7), with medium heterogeneity present in both design types (I2 = 46.03% and I2 = 68.76% respectively). Study design did not significantly change the effect size (0.054, p = 0.519).

Meta-analysis forest plot of overall HRQoL total score showing subgroup analysis by study design
Study location
In all locations, HRQoL was higher after VD. The association was significant in Germany, Ireland and Italy (ES 0.35, 95% CI = 0.19–0.49, n = 275, 1 study) [28], Spain (ES 0.22, 95% CI = 0.14–0.30, n = 3346, 1 study) [38], and the UK (ES 0.20, 95% CI = 0.04–0.35, n = 970, 1 study) [38] (Fig. 8). Between study heterogeneity was medium (52.3%). Most locations had a negative, insignificant, meta-regression coefficient (p < 0.11) showing no influence on effect size. Germany, Ireland, and Italy had a positive, non-significant coefficient (0.016, p = 0.924, 95% CI = -0.30–0.33) suggestive of a positive impact on the effect size. Iran had a significantly negative coefficient (− 0.33, p = 0.04, 95% CI -0.65- -0.02) indicating a negative influence on the effect size. However, both statistics lack power and further research is required to confirm these results. Due to the small number of studies for all locations these results are for visual representation and should be interpreted with caution.

Meta-analysis forest plot of overall HRQoL score showing subgroup analysis by study location
Mental (MSC) and Physical Component Scores (PCS)
Statistical analysis of component scores (MCS and PCS) and HRQoL
Four studies reporting MSC and PCS scores were statistically analysed. For both components, HRQoL was found to be higher after VD than after CS, yet the association was only significant for PCS (ES 0.24, 95% CI = 0.01, 0.48, n = 1122, 4 studies and ES 0.04, 95% CI = -0.04, 0.1, n = 1122, 4 studies respectively) [23, 24, 32, 41] (Fig. 9). Overall, there was a small significant effect size between the birth modes and HRQoL (ES 0.12, 95% CI = 0.01, 0.23, n = 2244, 4 studies) [23, 24, 32, 41]. Heterogeneity was medium between all studies reporting component scores (I2 = 60.98%) and between studies reporting PCS (77.40%). This was resultant of within-study sampling error (15.76, p = 0.03). The variation in MCS can be explained by chance (I2 = 0.00%) therefore no stratified analysis was conducted.

Forest plot of random effects meta-analysis of studies assessing overall HRQoL score stratified by MCS and PCS
Subgroup analysis
Findings were consistent for all studies eligible in this study regardless of date of study. Study findings have been constant since 2007, except for one PCS result in 2007 [24]. These consistent findings highlight that HRQoL has been consistently significantly higher for women who delivered vaginally for nearly 15 years (Fig. 10). The effect has marginally decreased in more recent studies (− 0.04, p0.003).

Meta-analysis forest plot showing component scores showing subgroup analysis by year of study
Sample size showed no significant effect on heterogeneity (− 0.00, p0.42) and publication bias was not present (1.16, p = 0.18).
Study design
Effect size was higher, but non-significant, in RCTs (ES 0.22, 95% CI = -0.02–0.45, n = 1832, 2 studies) [23, 24] (Fig. 11). Meta-regression confirmed study design had no influence on effect size (0.134, p = 0.32, 95% CI = -0.131–0.40) (Fig. 11). Unexpectedly heterogeneity was highest among RCTs studies (I2 = 90.97%), potentially caused by bias in one outlying study [24]. Subgroup analysis by location was not possible as very few studies reported location(s).

Meta-analysis forest plot showing component scores, stratified by study design
Study location
Subgroup analyses by location were not possible as too few studies shared locations.
HRQoL dimensions
Statistical analysis of SF-36 dimensions and HRQoL
Eight studies reporting SF-36 dimensions scores were included in a statistical analysis. Vaginal delivery was associated with significantly higher physical functioning (Mean difference (MD) 11.29, 95% CI = 2.25–20.33, n = 1746 8 studies) [23, 24, 28, 32, 37, 42, 43], physical role (MD 13.26, 95% CI = 1.10–25.41, n = 1471, 7 studies) [23, 24, 32, 37, 42, 43], vitality (MD 6.43, 95% CI = 1.13–11.72, n = 1746, 8 studies) [23, 24, 28, 32, 33, 37, 42, 43], and social functioning (MD 5.81, 95% CI = 1.31–10.32, n = 1746, 8 studies) [23, 24, 28, 32, 33, 37, 42, 43] scores than caesarean section (Additional file 4). Bodily pain, emotion role, mental health and general health had higher scores after VD, though this did not reach statistical significance. Heterogeneity was high on all dimensions (95–99%) therefore subgroup analyses were conducted to identify the cause.
Subgroup analysis of SF-36 dimensions and HRQoL
Study year
Study results were found consistent since 2015 (Additional file 5). HRQoL was significantly higher after VD than after CS regardless of date of study conducted (MD 7.65, 95% CI = 4.77–10.53, n = 3636, 6 studies) [23, 24, 32, 33, 37, 40] (Additional file 6). This may be explained by the higher heterogeneity being found between the earlier studies (I2 = 99.52%). Meta-regression confirmed study year was not a significant cause of heterogeneity (− 0.42, p = 0.35).
Sample size had a small significant negative effect (− 0.004, p = 0.00) indicating smaller studies may overestimate mean differences. Publication bias was not evident (− 0.44, p = 0.52).
Study design had a significant impact on mean differences for cohort studies (MD 25.47, 95% CI 15.38–35.56, n = 2378, 2 studies) [37, 44], cross-sectional studies (MD 3.93, 95% CI 1.77–6.09, n = 334, 4 studies) [32, 33, 42, 43], and prospective studies (MD 7.35, 95% CI 3.98–10.73, n = 346, 2 studies) [24, 28] (Additional file 7). This was confirmed by meta-regression (0.97, p = 0.00). No statistical difference was found between the groups (VD and CS) in randomised control trial’s (MD 0.41, 95% CI -0.02,0.84, n = 864, 1 study), however data was only taken from one study and therefore more data is needed to substantiate these findings.
Study location
Subgroup analysis by location was only possible in Iran where there were multiple studies. Results found a significant impact on effect size only for physical role (MD 19.55, 95% CS 0.26–38.83, n = 2359, 4 studies) [32, 37, 42, 43] (Fig. 12). This was confirmed by meta-regression (0.23, p = 0.05).

Meta-analysis forest plot showing subgroup analysis of physical role SF-36-dimension scores of Iranian studies
Narrative analysis
Three studies were narratively analysed. Two Iranian studies reported conflicting findings [37] [31]. HRQoL was significantly higher after VD in a retrospective cohort of 2100 women [37], whereas a cross-sectional study of 410 women found no significant differences between delivery modes (p = 0.43) [31]. This may be explained by the different timepoints observed (1 year, 6 months respectively), variation of QoL measures (SF-36, WHOQoL-BREF respectively), and small sample sizes. One Canadian study found global WHOQOL-BREF dimension scores were higher 8 weeks after vaginal delivery than after caesarean section (n = 181) [27]. These studies were of good quality and low bias. However, more studies are needed to substantiate these results particularly considering the small sample size.
This review was not able to conduct analyses on ethnicity and health condition, as proposed in the protocol, due to lack of information provided by the authors.
Discussion
The global rate of caesarean sections has risen 21% in 15 years (2000–2015) [45]. More women are requesting caesarean sections for personal reasons such as fear of labor or negative vaginal delivery experiences accounting for up to 42% of all caesarean sections [46, 47]. Literature shows the impact delivery has on postpartum HRQoL varies between the different modes of delivery [11, 12, 16, 17, 48]. However, there is no unanimity in the direction of these associations as demonstrated by two reviews on the topic that had conflicting findings [16, 17]. Furthermore, these reviews were subject to selection bias caused by limiting searches by study date and language. Consequently, the included population was largely from Iran thus the findings may not generalise to non-Asian populations. The aim of this systematic review was to examine the relationship between mode of delivery and postpartum HRQoL though a systematic review of published evidence. To our knowledge this is the largest and most recent review investigating this association. The findings are expected to increase health professional’s awareness to support women’s quality-of-life after childbirth.
The results showed women who delivered vaginally had a significantly higher postpartum HRQoL than those that delivered via caesarean section. These findings are consistent with primary studies that found QoL was better after vaginal delivery in early postpartum months and 5 years later [43, 44]. They also support the findings of a related review where, up to 2015, caesarean section was negatively associated with HRQoL [16]. The current review provides new evidence that the association continues into the present. Yet not all research agrees, some found caesarean section was not a contributing factor to reduced QoL and others found no statistically significant difference between delivery types [17, 49, 50]. The discordance between literature may be explained by the diverse study methodologies observed by this review, including QoL measurement tools, HRQoL dimensions, and study location.
This review showed the strength of association varied between spontaneous vaginal delivery and assisted vaginal delivery. Both had significantly higher HRQoL scores than those who delivered by caesarean section, though there was no statistically significant relationship between the vaginal delivery types. The effect was strongest for AVD and findings harmonious. However, when interpretating these results it should be considered AVD sample size was half that of SVD.
This study revealed physical HRQoL was also better after vaginal delivery. Significant relationships were found between delivery modes and physical component, functioning, and role, with the latter two having the strongest associations of all dimensions. Furthermore, bodily pain, general health, and environmental scores were also higher after VD but non-significantly. This strengthens previous evidence that physical recovery is slower after caesarean [51]. Mental HRQoL was also found higher after VD on all dimensions with a significant association for vitality and social functioning, but non-significant for mental component, emotional role, or mental health.
This review highlights that HRQoL has been found higher after vaginal delivery, than caesarean, for over a decade. Consequently, this study provides evidence useful for the counselling of patients in obstetric practices. Health authorities are urged to disseminate this information to policy makers, clinicians and women planning a birth to ensure evidence-based decisions are fostered, providing interventions or training where necessary. Public health programmes, such as antenatal classes could be used to effectively translate this knowledge.
Policy implications
The findings of this review have implications for obstetric practitioners and health professionals in health centers. Understanding how delivery modes effect postpartum QoL can lead to more informed choices and postpartum care, thus improving QoL. Traditional physical postpartum checks should be supplemented with QoL assessment to identify the full range of needs required for recovery after birth enabling women to reach and maintain optimum health for themselves, and their babies. Therefore findings of this study should also be used by health authorities to implement effective health programs, stratagies and policies.
This study is timely with the rise in CS rates and has implications for healthcare policy makers. The results are consistent with studies reporting that CS leads to slower recovery, prolonged hospital stays, and increased health service costs [51]. For these economic reasons policies should be reviewed to encourage women to give birth vaginally in the absence of medical indications.
Strengths and limitations
There are several caveats in this study which can be attributed to a lack of specification of the study population. For instance, most of the delivery mode subgroups (SVD, AVD, VD, EmCS, ElCS) were analysed according to their overarching groups (VD and CS). Analysing subgroups in this combined manner induces interpretation bias. The included studies observed deliveries in hospitals and health centres. Other settings such as home births were not reported resulting in subject bias. Predominantly the studies did not adequately adjust for confounders therefore the exploration of additional factors as intended in the protocol (CRD42020145090) was restricted. Finally, data were typically collected within 6 months postpartum limiting the reviews’ ability to make longitudinal conclusions.
Review methodology limitations (first) include the exclusion criteria. Papers not presented in the English language were excluded, thus the generalizability of results is limited. Secondly qualitative studies were excluded as they did not measure HRQoL however further qualitative work would help give greater detail about women’s perceptions of their postpartum mental and physical health. Moreover, the included HRQoL tools measure different constructs thus the subscales were too different to harmonize and study results were pooled individually by tool rather than together as originally intended. However, most included studies used the SF-36 tool providing a consistent basis to this study. The SF-36 is reportedly the most suitable tool for measuring HRQoL providing the findings of this review with credibility [30, 52]. Finally, due to the different timepoints observed between studies the latest time-points were used for analysis in this study. Thus, observations of changes in QoL over time could not be made. Medium-high heterogeneity was present, and location and study design showed a small effect on dimension scores. Further research is required to substantiate these indications.
The strengths of this review include following Cochrane methods and a comprehensive search of the literature. All aspects of the reviewing process were conducted by two independent reviewers thus the likelihood of reviewing bias is low. This is an up-to-date review including the largest sample and worldwide, high-quality studies. The included QoL tools were validated and comprised of generic and disease-specifics measures. Study results were found constant since 2007 and 2014 for component and dimensions scores respectively. Meta regressions were conducted to account for heterogeneities and control for follow-up showing heterogeneity was not consequential of publication bias, study design, or year.
Conclusion
This review showed that for all mental and physical aspects women had higher HRQoL scores after vaginal delivery after caesarean section. The association was statistically significant for physical component, physical functioning, physical role, vitality and social functioning. It is therefore recommended that pregnant women should be encouraged to deliver vaginally in the absence of medical indications.
References
ACOG. Ob-Gyns Stress the Importance of Postpartum Care: The Fourth Trimester 2016. Available from: https://www.acog.org/About-ACOG/News-Room/News-Releases/2016/Ob-Gyns-Stress-the-Importance-of-Postpartum-Care-The-Fourth-Trimester?IsMobileSet=false [updated 23 May 2016].
Technical Working Group WHO. Postpartum Care of the Mother and Newborn: A Practical Guide. 1999;26(4):255–8.
Cheng C-Y, Li Q. Integrative review of research on general health status and prevalence of common physical health conditions of women after childbirth. Womens Health Issues. 2008;18(4):267–80.
Symon A, McGreavey J, Picken C. Postnatal quality of life assessment: validation of the mother-generated index. Bjog. 2003;110(9):865–8.
Van der Woude DAA, Pijnenborg JMA, de Vries J. Health status and quality of life in postpartum women: a systematic review of associated factors. Eur J Obstet Gynecol Reprod Biol. 2015;185:45–52.
World Health Organization. WHOQOL: Measuring Quality of Life. Geneva: World Health Organization; 2019. Available from: https://www.who.int/healthinfo/survey/whoqol-qualityoflife/en/
Hamming JF, De Vries J. Measuring quality of life. Br J Surg. 2007;94(8):923–4.
Janodia M. Health related quality of life (HRQOL) measures in healthcare delivery system: Indian perspective. J Young Pharm. 2016;8:164–7.
World Health Organization. WHO recommendations non-clinical interventions to reduce unnecessary caesarean sections. Geneva: World Health Organization; 2019. p. 2.
Darcy JM, Grzywacz JG, Stephens RL, Leng I, Clinch CR, Arcury TA. Maternal depressive symptomatology: 16-month follow-up of infant and maternal health-related quality of life. J Am Board Fam Med. 2011;24(3):249–57.
Petrou S, Kim SW, McParland P, Boyle EM. Mode of delivery and long-term health-related quality-of-life outcomes: a prospective population-based study. Birth. 2017;44(2):110–9.
Prick BW, Bijlenga D, Jansen AJG, Boers KE, Scherjon SA, Koopmans CM, et al. Determinants of health-related quality of life in the postpartum period after obstetric complications. Eur J Obstet Gynecol Reprod Biol. 2015;185:88–95.
Edwards J, N.J. D. Elective caesarean section - the patient's choice? J Obstet Gynaecol. 2001;21(2):128–9.
McCourt C, Weaver J, Statham H, Beake S, Gamble J, Creedy DK. Elective cesarean section and decision making: a critical review of the literature. Birth (Berkeley, Calif). 2007;34(1):65–79.
Minkoff H, Chervenak FA. Elective primary cesarean delivery. N Engl J Med. 2003;348(10):946–50.
Rezaei N, Tavalaee Z, Sayehmiri K, Sharifi N, Daliri S. The relationship between quality of life and methods of delivery: a systematic review and meta-analysis. Electron Physician. 2018;10(4):6596–607.
Rezaei S, Salimi Y, Zahirian Moghadam T, Mirzarahimi T, Mehrtak M, Zandiyan H. Quality of life after vaginal and cesarean deliveries: a systematic review and meta-analysis. Int J Hum Rights Healthc. 2018;11:165–75.
Robertson LC, Al-Haddad M. Recognizing the critically ill patient. Anaesthes Intens Care Med. 2013;14(1):11–4.
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomized studies of interventions. BMJ. 2016;355:i4919.
Collaboration TC. Combining groups 2011 [5.1.0:[Available from: https://handbook-5-1.cochrane.org/chapter_7/7_7_3_8_combining_groups.htm.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Hutton EK, Hannah ME, Ross S, Joseph KS, Ohlsson A, Asztalos EV, et al. Maternal outcomes at 3 months after planned caesarean section versus planned vaginal birth for twin pregnancies in the twin birth study: a randomised controlled trial. BJOG. 2015;122(12):1653–62.
Jansen AJ, Essink-Bot ML, Duvekot JJ, van Rhenen DJ. Psychometric evaluation of health-related quality of life measures in women after different types of delivery. J Psychosom Res. 2007;63(3):275–81.
Sidebotham P, Fraser J, Covington T, Freemantle J, Petrou S, Pulikottil-Jacob R, et al. Understanding why children die in high-income countries. Lancet (London, England). 2014;384(9946):915–27.
Akyn B, Ege E, Kocodlu D, Demiroren N, Yylmaz S. Quality of life and related factors in women, aged 15-49 in the 12-month post-partum period in Turkey. J Obstet Gynaecol Res. 2009;35(1):86–93.
Mousavi SA, Mortazavi F, Chaman R, Khosravi A. Quality of life after cesarean and vaginal delivery. Oman Med J. 2013;28(4):245–51.
Fobelets M, Beeckman K, Buyl R, Daly D, Sinclair M, Healy P, et al. Mode of birth and postnatal health-related quality of life after one previous cesarean in three European countries. Birth (Berkeley, Calif). 2018;45(2):137–47.
Bodhare TN, Sethi P, Bele SD, Gayatri D, Vivekanand A. Postnatal quality of life, depressive symptoms, and social support among women in southern India. Women Health. 2015;55(3):353–65.
Baghirzada L, Downey KN, Macarthur AJ. Assessment of quality of life indicators in the postpartum period. Int J Obstet Anesthes. 2013;22(3):209–16.
Zaheri F, Nasab LH, Ranaei F, Shahoei R. The relationship between quality of life after childbirth and the childbirth method in nulliparous women referred to healthcare centers in Sanandaj, Iran. Electron Physician. 2017;9(12):5985–90.
Kavosi Z, Keshtkaran A, Setoodehzadeh F, Kasraeian M, Khammarnia M, Eslahi M. A comparison of Mothers' quality of life after Normal vaginal, cesarean, and water birth deliveries. Int J Commun Based Nurs Midw. 2015;3(3):198–204.
AlShehri NMAA, Alanazi MQ, Alanazi WQ, Alanazi JQ, et al. Relationship between health related quality of life determinants and type ofDelivery in Saudi women. Fam Med Med Sci Res. 2015;4(1):1–4.
Fobelets M, Beeckman K, Buyl R, Healy P, Grylka-Baeschlin S, Nicoletti J, et al. Preference of birth mode and postnatal health related quality of life after one previous caesarean section in three European countries. Midwifery. 2019;79:102536.
Li W-Y, Liabsuetrakul T, Stray-Pedersen B, Li Y-J, Guo L-J, Qin W-Z. The effects of mode of delivery and time since birth on chronic pelvic pain and health-related quality of life. Int J Gynecol Obstet. 2014;124(2):139–42.
Mahumud RA, Ali N, Sheikh N, Akram R, Alam K, Gow J, et al. Measuring perinatal and postpartum quality of life of women and associated factors in semi-urban Bangladesh. Qual Life Res. 2019;28(11):2989–3004.
Majzoobi MR, Majzoobi M, Nazari-Pouya F, Biglari M, Poorolajal J. Comparing Quality of Life in Women after Vaginal Delivery and Cesarean. J Midwifery Reprod Health. 2014;2(4):207–14.
Martinez-Galiano JM, Hernandez-Martinez A, Rodriguez-Almagro J, Delgado-Rodriguez M. Quality of life of women after giving birth: associated factors related with the birth process. J Clin Med. 2019;8(3):324.
Ozdemir F, Ozturk A, Karabulutlu O, Tezel A. Determination of the life quality and self-care ability of the mothers in post-partum period. JPMA J Pak Med Assoc. 2018;68(2):210–5.
Sadat Z, Abedzadeh-Kalahroudi M, Atrian MK, Karimian Z, Sooki Z. The impact of postpartum depression on quality of life in women after Child's birth. Iran Red Crescent Med J. 2014;16(2).
Rezaei N, Azadi A, Zargousi R, Sadoughi Z, Tavalaee Z, Rezayati M. Maternal health-related quality of life and its predicting factors in the postpartum period in Iran. Scientifica. 2016;2016:8542147. https://doi.org/10.1155/2016/8542147. Epub 2016 Feb 28. PMID: 27022506; PMCID: PMC4789062.
Sadat Z, Taebi M, Saberi F, Kalarhoudi MA. The relationship between mode of delivery and postpartum physical and mental health related quality of life. Iran J Nurs Midwifery Res. 2013;18(6):499–504.
Torkan B, Parsay S, Lamyian M, Kazemnejad A, Montazeri A. Postnatal quality of life in women after normal vaginal delivery and caesarean section. BMC Pregnancy Childbirth. 2009;9:4.
Angelini CR, Pacagnella RC, Parpinelli MA, Silveira C, Andreucci CB, Ferreira EC, et al. Quality of life after an episode of severe maternal morbidity: evidence from a cohort study in Brazil. Biomed Res Int. 2018;2018:9348647.
Wise J. Alarming global rise in caesarean births, figures show. BMJ. 2018;363:k4319.
Begum T, Saif-Ur-Rahman K, Yaqoot F, Stekelenburg J, Anuradha S, Biswas T, et al. Global incidence of caesarean deliveries on maternal request: a systematic review and meta-regression. BJOG Int J Obstet Gynaecol. 2021;128(5):798–806.
NHS. Overview Caesarean section 2019 Available from: https://www.nhs.uk/conditions/caesarean-section/.
Kohler S, Annerstedt KS, Diwan V, Lindholm L, Randive B, Vora K, et al. Postpartum quality of life in Indian women after vaginal birth and cesarean section: a pilot study using the EQ-5D-5L descriptive system. BMC Pregnancy Childbirth. 2018;18:1–3.
Hoedjes M, Vogel I, Berks D, Franx A, Duvekot JJ, Habbema JDF, et al. Poor health-related quality of life after severe preeclampsia. Pregnancy Hypertens. 2010;1:S32.
Triviño-Juárez J-M, Romero-Ayuso D, Nieto-Pereda B, Forjaz M-J, Criado-Álvarez J-J, Arruti-Sevilla B, et al. Health related quality of life of women at the sixth week and sixth month postpartum by mode of birth. Women Birth. 2017;30(1):29–39.
Jansen AJ, Duvekot JJ, Hop WC, Essink-Bot ML, Beckers EA, Karsdorp VH, et al. New insights into fatigue and health-related quality of life after delivery. Acta Obstet Gynecol Scand. 2007;86(5):579–84.
Huang IC, Wu AW, Frangakis C. Do the SF-36 and WHOQOL-BREF measure the same constructs? Evidence from the Taiwan population*. Qual Life Res. 2006;15(1):15–24.
Acknowledgements
The views expressed in this publication are not necessarily those of the University of Warwick or of the NIHR.
Funding
KE was funded by Warwick Evidence (NIHR). LAK was funded by Warwick Evidence (NIHR) and Applied Research Collaboration West Midlands (NIHR). HF was funded by Warwick Evidence (NIHR). SJ was funded by University of Warwick Library. OO was funded by Warwick Evidence (NIHR) and Johnson & Johnson Inc.
Author information
Authors and Affiliations
Contributions
All aspects of the review were conducted and written up by the primary reviewer (KE). Secondary reviewers (HF/OO) sifted title/abstracts and full texts and undertook data extraction and quality appraisal on all included studies. SJ helped develop the search strategy. OU provided support for the statistical analysis. LAK advised on protocol, methodology and reviewed and the manuscript. All authors critically reviewed the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplemenaty Table T1.
Excluded studies after full text data extraction and reasons.
Additional file 2: Supplementary Table T2.
Characteristics of Included Studies.
Additional file 3: Supplementary Table T3.
Risk of Bias assessment score of included studies.
Additional file 4: Supplementary Figure F1.
Forest plot of random effects meta-analysis of studies assessing overall HRQoL score, stratified by SF-36 dimensions.
Additional file 5: Supplementary Figure 2.
Meta-analysis forest plot showing component scores showing subgroup analysis by year of study and SF-36 dimension.
Additional file 6: Supplementary Figure 3.
Forest plot of random effects meta-analysis of studies assessing HRQoL by SF-36 dimension score, stratified by earlier and recent studies.
Additional file 7: Supplementary Figure 4.
Meta-analysis forest plot of SF-36 dimension score, stratified by study design.
Additional file 8.
MEDLINE Search Strategy.
Additional file 9.
Data Extraction Form Template.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Evans, K., Fraser, H., Uthman, O. et al. The effect of mode of delivery on health-related quality-of-life in mothers: a systematic review and meta-analysis. BMC Pregnancy Childbirth 22, 149 (2022). https://doi.org/10.1186/s12884-022-04473-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-022-04473-w