
Abstract
Background
Ischemic stroke, including transient ischemic attack (TIA) and acute-phase cerebral infarction (aCI), is a serious health problem in the aging society. Thus, this study aimed to identify TIA and aCI biomarkers.
Methods
In 19 patients with TIA, candidate antigens recognized by serum IgG autoantibodies were screened using a human aortic endothelial cell cDNA library. Through amplified luminescent proximity homogeneous assay-linked immunosorbent assay (AlphaLISA), serum antibody levels against the candidate antigens were examined in healthy donor (HD), TIA, and aCI cohorts (n = 285, 92, and 529). The plasma antibody levels in the Japan Public Health Center-based Prospective Cohort Study (1991–1993) were also examined.
Results
The candidate antigens were aldolase A (ALDOA) and fumarate hydratase (FH). In AlphaLISA, patients with TIA or aCI had higher anti-ALDOA antibody (ALDOA-Ab) and anti-FH antibody (FH-Ab) levels than the HDs (P < 0.05). In a multivariate logistic regression analysis, the ALDOA-Ab (odds ratio [OR]: 2.46, P = 0.0050) and FH-Ab (OR: 2.49, P = 0.0037) levels were independent predictors of TIA. According to the case–control study, the ALDOA-Ab (OR: 2.50, P < 0.01) and FH-Ab (OR: 2.60, P < 0.01) levels were associated with aCI risk. In a correlation analysis, both ALDOA-Abs and FH-Abs were well associated with hypertension, coronary heart disease, and habitual smoking. These antibody levels also correlated well with maximum intima–media thickness, which reflects atherosclerotic stenosis.
Conclusions
ALDOA-Abs and FH-Abs can be novel potential biomarkers for predicting atherosclerotic TIA and aCI.
Similar content being viewed by others

Background
Ischemic stroke, including transient ischemic attack (TIA) and cerebral infarction (CI), is the most globally known cerebrovascular disorder. In particular, TIA is a temporary episode of neurological dysfunction caused by focal brain, spinal cord, or retinal ischemia, without acute infarction [1]. Meanwhile, CI is an episode of neurological dysfunction caused by focal brain infarction, often resulting in fatality and disability [2]. Patients with TIA are at a high risk of CI. According to epidemiologic studies, the prevalence of prior TIA in patients with CI was 15–30%. Additionally, the risk of CI on the 7th, 30th, and 90th-day post-TIA was 2.0 to 8.0%, 8.0 to 13.5%, and 9.5 to 20.1%, respectively [3, 4]. TIA with progressive aggravation is an early-warning signal for CI. Therefore, early TIA diagnosis and CI onset prediction are the key steps to reduce ischemic stroke occurrence [5].
Presently, TIA and CI can be predicted early in the medical field through several ways, including modern imaging techniques (e.g., transcranial Doppler [6], computed tomography, magnetic resonance imaging [7], and cerebral angiography [8]), blood biochemical indicators (e.g., oxidatively modified low-density lipoprotein [9], homocysteine [10], lipoprotein-related phospholipase A2, C-reactive protein [11], and heat shock protein [12]), and comprehensive assessment of risk factors [13] (e.g., hypertension, hyperlipidemia, body mass index [BMI], obesity, smoking habits, and family history). However, these methods are frequently insufficient to represent standard approaches for early TIA diagnosis and CI onset prediction. Therefore, novel biomarkers that would largely improve the management and prognosis of TIA and CI must be identified [14].
Atherosclerosis is highly likely to be involved in the pathogenesis of ischemic stroke, and most incident ischemic strokes (i.e., TIA and CI) are based on atherosclerosis [15]. Atherosclerosis is not only a simple pathological process of lipid deposition in the vascular wall. It is also an inflammatory proliferative dynamic mechanism induced by an excessive autoimmune response following vascular endothelial and smooth muscle cell injuries [16]. Endogenous antigens cause autoimmune responses that significantly influence the development of atherosclerosis, ultimately leading to the stenosis or blockage of the offending artery [17]. These antigens induce autoantibodies that have been detected in the serum of patients with atherosclerosis-related diseases, such as CI, coronary heart disease (CHD), and diabetes mellitus (DM) [18].
The serological identification of antigens by recombinant cDNA expression cloning (SEREX) is an established method for identifying endogenous antigenic proteins, combining molecular cloning and serological typing by using phage expression libraries [19]. SEREX was originally developed to screen out tumor-associated antigens, and it has identified more than 2300 novel tumor antigens recorded in Cancer Immunome Database, a public access online database [20, 21]. Hence, it is one of the most effective methods for identifying antigenic targets on a genome scale [22,23,24,25,26,27,28,29,30]. Consequently, it has also been used for autoimmune diseases, such as systemic lupus erythematosus, Kawasaki disease, Behcet’s disease, and multiple sclerosis [22,23,24,25]. In earlier studies, we used SEREX for examining atherosclerosis-related diseases and for identifying antibodies against RPA2 [26], MMP1, CBX1, and CBX5 [27] in CI, and ATP2B4, BMP-1 [28], TUBB2C [29], and SH3BP5 [30] in other atherosclerosis-related diseases.
Both TIA and CI have the pathological basis of atherosclerosis [15], and through SEREX, we found that atherosclerosis causes the increase of serum autoantibody levels in the early stage of lesions [26,27,28,29,30]. Clearly, the identification of sensitive, specific, and novel biomarkers is crucial to early predict TIA and CI. Therefore, this study aimed to identify autoantibodies associated with TIA and CI via SEREX. These autoantibodies could be used as molecular predictive biomarkers to reflect disease status.
Methods
Serum of patients and healthy donors (HDs)
We collected serum samples from HDs and patients diagnosed with TIA or CI caused by the development of atherosclerotic vulnerable plaque [31, 32]. HDs were selected from individuals with no history of TIA or CI, including acute-phase cerebral infarction (aCI) or old (chronic-phase) cerebral infarction (oCI), and with medical checkups, including cerebral MRI. Conversely, subjects with autoimmune disease were excluded. Next, we randomly selected 19 TIA serum samples, which were previously used to search for other stroke markers [27], and used them for SEREX screening.
In comparing the serum antibody levels, we set up four independent groups, which included 621 patients and 285 HDs. Of the 621 patients, 92, 464, and 65 suffered from TIA, aCI, and oCI, respectively. Table 1 shows the baseline characteristics of participants.
Sera were extracted from the patients with TIA, aCI, and oCI in Chiba Prefectural Sawara Hospital, Chiba Rosai Hospital, and Chiba Aoba Municipal Hospital and from HDs in Chiba Prefectural Sawara Hospital, Higashi Funabashi Hospital, and Port Square Kashiwado Clinic. We centrifuged the samples at 3000 g for 10 min at room temperature and stored the supernatants at −80°C until use. Repeated thawing and freezing of samples were avoided.
Clinical data
Regarding the risk factors of atherosclerosis, we collected the following data from the patients’ clinical records: age, sex, HT, DM, hyperlipidemia, CHD, obesity, and smoking. In this study, hypertension was defined as a history of systolic blood pressure > 140 mmHg, diastolic blood pressure > 90 mmHg, or the use of antihypertensive agents. DM was defined as having previously diagnosed with DM, treated with DM medication, and/or a fasting blood glucose level ≥ 126 mg/dL. Hyperlipidemia was defined as a history of total cholesterol > 220 mg/dL, triglyceride > 150 mg/dL, or the use of lipid-lowering agents. CHD was defined as a history of myocardial infarction or angina pectoris. Patients were considered as smokers if they either smoked during the study period or had a history of smoking. Finally, obesity was defined as BMI ≥ 25 kg/m2. We also collected the participants’ serum routine examination results, including blood routine, serum biochemistry, and blood electrolytes.
Screening by expression cloning and identified antigens of sequence analysis
Clones that were immunoreactive against the serum of patients with TIA were screened using a commercially available human aortic endothelial cell cDNA library (Uni-ZAP XR Premade Library, Stratagene, La Jolla, CA). Escherichia coli (E. coli) XL1-Blue MRF′ was infected with Uni-ZAP XR phage. Further details were described in our previously published and improved version of the immunoscreening method [18, 26, 30, 33, 34].
The monoclonalized phage cDNA clones were converted into pBluescript phagemids by in vivo excision using ExAssist helper phage (Stratagene). Plasmid DNA was obtained from the E. coli SOLR strains transformed by the phagemids. We sequenced the inserted cDNAs, followed by homologous analysis using a public database provided by the National Center for Biotechnology Information (https://blast.ncbi.nlm.nih.gov/Blast.cgi).
Purification of recombinant candidate proteins
To construct the expression plasmids of glutathione-S-transferase (GST)-fused proteins, we recombined the cDNA sequences into pGEX-4 T vectors and transfected them into E. coli BL-21, as previously described [6, 17, 21, 33, 34].
Subsequently, we cultured transformed E. coli BL-21 cells containing pGEX-4 T-2 clones and centrifuged the cell lysates. The GST-fusion recombinant proteins recovered in the supernatant fraction were directly purified by glutathione-Sepharose affinity chromatography (GE Healthcare Life Sciences) according to the manufacturer’s and our previous instructions [26, 28, 30]. We dissolved the precipitates containing recombinant proteins in 8 M urea in TED buffer [50 mM Tris–HCl (pH 8.0), 1 mM EDTA, and 1 mM dithiothreitol]. Next, we dialyzed the samples stepwise against 4 and 2 M urea in TED buffer every hour and then against the TED buffer. Finally, the recombinant proteins recovered in the supernatant using glutathione-Sepharose were purified, as described above [26,27,28,29,30].
Western blotting
GST, GST–aldolase A (ALDOA), and GST–fumarate hydratase (FH) proteins (0.3 μg) were electrophoresed through SDS–polyacrylamide gel and analyzed by western blotting. To this end, we used anti-GST (goat) or 1:5000-diluted serum from patients with TIA or CI (#350 and #692). The proteins were then incubated with horseradish peroxidase-conjugated secondary antibody, as previously described [30, 33, 35, 36].
Amplified luminescent proximity homogeneous assay-linked immunosorbent assay (AlphaLISA) of antibody biomarkers
The serum antibodies against the purified proteins were quantitatively measured by AlphaLISA. After being prepared according to Perkin Elmer’s instructions (Waltham, MA) and our previous reports [27, 30, 33, 34], the samples mixture was incubated for 14 days at room temperature in the dark. The chemical emission was read using the EnSpire Alpha microplate reader (Perkin Elmer). Specific reactions were calculated by subtracting the alpha values (alpha-photon counts) of the GST control from those of GST-fusion proteins.
Nested case–control study
A nested case–control study was conducted using the antibody levels detected by AlphaLISA. This study was nested within the Japan Public Health Center (JPHC)-based Prospective Study [37, 38], which stored the plasma samples of approximately 30,000 Japanese individuals aged 40–69 years at a baseline period of 1990–1994. We used the samples of 202 incidental cases of acute ischemic stroke developed between the baseline and 2008 and those of 202 controls. The age (within 2 years), sex, blood sampling date (within 3 months), time since last meal (within 4 h), and study location (Public Health Center area) of these controls were matched with those of the cases. The odds ratios (ORs) and 95% confidence intervals (CIs) were estimated using a conditional logistic regression model. We informed the study participants of the objectives and methods of the study; those who answered the questionnaire and donated blood indicated that they gave informed consent to participate. The ethics committee of the National Cancer Center, Osaka University, and Tsukuba University approved this study.
Statistical analyses
We compared differences in the alpha values between two groups by using Student’s t-test and Mann–Whitney U test. Additionally, the correlation between the alpha values and clinical case data was determined by Spearman’s correlation analysis. Using univariate and multivariate logistic regression analyses, we identified the set of variables that could be used to classify participants according to positive history for ischemic stroke. Furthermore, the ORs of the antibody levels of ALDOA and FH (ALDOA-Ab and FH-Ab, respectively) for CI in the nested case–control study were estimated and compared using a conditional logistic regression model. Through a receiver operating characteristic (ROC) analysis, we assessed the predictive values of markers for TIA and CI. Additionally, the cutoff values were set to maximize the sum of sensitivity and specificity. All tests were two-tailed. We considered P < 0.05 as statistically significant. All statistical data were analyzed using either the SPSS 13.0 software (SPSS Inc., Chicago, IL) or GraphPad Prism 5 (GraphPad Software, La Jolla, CA).
Results
Identification of ALDOA and FH as antigens in the serum of patients with TIA
By expression cloning, two independent clones were identified in the serum of 19 patients with TIA (Fig. 1). Specifically, we found a sequence homology with ALDOA (Accession number: NM_184041) and FH (Accession number: NM_000143). The region between amino acids 70 and 469 of ALDOA and that between amino acids 1 and 185 of FH were obtained as pBluescript II clones; both were then recombined into pGEX-4 T-2 vectors individually. Recombinant ALDOA and FH proteins were expressed in E. coli as GST-fusion proteins and subsequently purified by glutathione-Sepharose affinity chromatography.

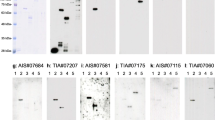
Immunoscreening of TIA antigens by SEREX. Bacterial proteins including phage cDNA products were blotted on nitrocellulose membranes and reacted with the sera of patients with TIA. The a, b, and c show the representative results of stained membranes (membrane diameter: 86 mm) after the second screening of SEREX. Arrows indicate positive phage clones
Presence of serum antibodies confirmed by western blotting
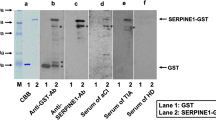
We aimed at confirming the presence of ALDOA-Abs and FH-Abs in the serum of patients with TIA or CI through western blotting. Using an anti-GST antibody, we recognized GST-ALDOA, GST-FH, and GST proteins as the reactions of 65-, 67-, and 28-kDa proteins, respectively (Fig. 2). Conversely, GST-ALDOA and/or GST-FH, but not GST, reacted with the serum antibodies of patients #350 and #692. Therefore, most, if not all, of the GST-fusion antigen proteins’ reactivity with serum antibodies may be caused by antigen proteins rather than the GST domain. Specific reactions against ALDOA or FH proteins were estimated by subtracting the antibody levels of GST from those of GST-tagged antigen proteins.

Presence of serum antibodies against ALDOA and FH antigenic proteins. The representative results of western blotting are shown. The latter showed the detection at the expected size of all the affinity-purified glutathione-S-transferase (GST)-fusion antigenic proteins (GST-ALDOA: 65 kDa; GST-FH: 67 kDa). GST and GST-fusion proteins were electrophoresed through SDS–polyacrylamide gels. They were subsequently stained with Coomassie Brilliant Blue or western blotting using anti-GST (αGST) or patient sera (#350 and #692). The specific reactions to GST-ALDOA and GST-FH are shown. The star represents degradation products after the electrophoresis. The left side of the figure shows the molecular weights
Increase of ALDOA-Ab and FH-Ab levels in patients with TIA or CI
As mentioned, the ALDOA-Ab and FH-Ab levels in the sera of HDs and patients with TIA, aCI, or oCI were quantitatively analyzed using AlphaLISA. The alpha counts represent the luminescent photon counts corresponding to the antibody levels. Both antibody levels were significantly higher in patients with TIA, aCI, and oCI than in HDs (P < 0.05) (Table 2). Furthermore, the alpha counts were not significantly different between the three patient groups (Fig. 3). Therefore, ALDOA-Ab and FH-Ab levels may be closely related to the three ischemic cerebrovascular diseases (i.e., TIA, aCI, and oCI), but not to the disease type.

Comparison of the serum ALDOA-Ab and FH-Ab levels between HDs and patients with TIA, aCI, or oCI. The antigens GST-ALDOA (a) and GST-FH (b) were used. After the subtraction of the levels of antibodies against control GST, the serum antibody levels were examined by AlphaLISA, shown using a box-whisker. The stars indicate P values vs. HD specimens. One star indicates P < 0.05, two stars indicate P < 0.01, and three stars indicate P < 0.001. Table 2 shows the averages, SDs, total numbers, and P values
The ability of the markers ALDOA-Abs and FH-Abs to detect TIA, aCI, and oCI was evaluated by the ROC analysis. The areas under the curve of ALDOA-Abs and FH-Abs were 0.63 (95% CIs: 0.56–0.69) (Fig. 4a) and 0.63 (95% CI: 0.56–0.70) (Fig. 4d) for TIA, 0.63 (95% CI: 0.60–0.67) (Fig. 4b) and 0.63 (95% CI: 0.59–0.67) (Fig. 4e) for aCI, and 0.62 (95% CI: 0.54–0.70) (Fig. 4c) and 0.67 (95% CI: 0.60–0.75) (Fig. 4f) for oCI, respectively. At a cutoff value of 14,869 for the ALDOA-Abs, the antibody level’s sensitivity and specificity for TIA diagnosis were 69.57 and 54.74%, respectively (Fig. 4a), similar to those for aCI diagnosis (69.40 and 51.58%, respectively) (Fig. 4b). The sensitivity and specificity for FH-Abs are shown in Fig. 4d, e, and f.

Receiver operating characteristic (ROC) analysis of ALDOA-Abs and FH-Abs as predictors of TIA, aCI, or oCI. Numbers in the figures indicate the cutoff values for marker levels. Numbers in parentheses indicate sensitivity (left) and specificity (right). Areas under the curve (AUC), 95% confidence intervals (95% CI), and P values are shown
Association between TIA and clinical parameters including ALDOA-Ab and FH-Ab levels
Table 3 summarizes the results of univariate and multivariate logistic regression analyses. Using the cutoff values of 14,869 and 2849, the univariate logistic regression analysis revealed that the elevated ALDOA-Ab (OR: 2.91, 95% CI: 1.76–4.83, P < 0.0001) and FH-Ab (OR: 2.88, 95% CI: 1.78–4.67, P < 0.0001) levels were associated with the increased risk for TIA, respectively. Those factors with P < 0.05 in the univariate analysis were used in the multivariate regression analysis. In this subsequent analysis, elevated ALDOA-Ab (OR: 2.46, 95% CI: 1.31–4.62, P = 0.0050) and FH-Ab (OR: 2.49, 95% CI: 1.35–4.63, P = 0.0037) levels were independent predictors of TIA. The predictive values of ALDOA-Abs and FH-Abs for TIA were similar to that of hypertension, which is a typical risk factor of TIA. Specifically, the risk factors of TIA were as follows: age (OR: 6.04, 95% CI: 3.15–11.58, P < 0.0001), hypertension (OR: 2.97, 95% CI: 1.61–5.45, P = 0.0005), and DM (OR: 5.31, 95% CI: 2.05–13.79, P = 0.0006).
Elevated positive predictive values (PPVs) by the combination of ALDOA-Abs, FH-Abs, and clinical risk factors
Next, we calculated the positive rates of 92 patients with TIA and 285 HDs, with the involvement of the conventional risk factors (i.e., age, HT, and DM). We used the cutoff values of 14,869 and 2849 for ALDOA-Abs and FH-Abs to detect TIA. The PPVs of age, HT, and DM were 48.0, 51.3, and 71.1%, respectively (Table 4). Conversely, the PPVs of ALDOA-Abs combined with age, HT, and DM increased to 63.1, 63.5, and 91.3%, whereas those of FH-Abs were 61.9, 56.9, and 94.1%, respectively, thereby similar. Furthermore, the PPVs of ALDOA-Abs combined with HT and DM, and those of FH-Abs combined with age and DM reached up to 100%.
JPHC cohort analysis
The abovementioned logistic regression analysis proved that ALDOA-Abs and FH-Abs are independent early-warning risk factors of TIA, which is one of prodromal stages of CI. To further validate their association with CI, we conducted a prospective case–control study nested within the JPHC-based Prospective Study (the interference of age, sex, and area was excluded). The ALDOA-Ab and FH-Ab levels were divided into quartiles. For the participants with the second and highest quartiles of the antibody level, the ORs (95% CIs) were 2.38 (1.24–4.55) and 2.50 (1.26–4.96), respectively, compared with that for those with the lowest quartile (Table 5). Additionally, the FH-Ab levels were positively associated with the risk for aCI. Specifically, the ORs (95% CIs) were 2.17 (1.20–3.92) and 2.60 (1.41–4.80) for those participants with the third and highest quartiles of the antibody level, respectively. Therefore, ALDOA-Abs and FH-Abs can predict the onset of aCI.
Association between the ALDOA-Ab and FH-Ab levels and the clinical parameters
We then examined whether the serum ALDOA-Ab and FH-Ab levels correlate with clinical parameters such as sex, other diseases, lifestyle, and obesity (Table 6). The ALDOA-Ab levels were well associated with blood pressure (P = 0.0022), CHD (P = 0.0400), and habitual smoking (P < 0.0001), but not with sex, DM, HL, alcohol intake, or obesity. The FH-Ab levels showed similar correlation with the ALDOA-Ab levels, except that the former significantly correlated with DM (P = 0.0183) and less correlated with smoking habit (P = 0.0566).
The correlation between the antibody levels and other clinical parameters was also examined by Spearman correlation analysis. The levels of both AODOA-Abs and FH-Abs significantly correlated with age, blood pressure, maximum intima–media thickness (max IMT), and blood sugar (Table 7). Considering that max IMT is one of indices of atherosclerosis, both ALDOA-Abs and FH-Abs could reflect the degree of atherosclerosis. Consistent with the results in Table 6, DM-related blood sugar was more closely related to FH-Abs than ALDOA-Abs. Meanwhile, the antibody levels inversely correlated with the albumin/globulin ratio, cholinesterase, total protein, albumin, total cholesterol, and red blood cell count.
Discussion
After the application of SEREX using the sera of patients with TIA, we found two antigens, namely, ALDOA and FH. Additionally, the presence of antibodies against ALDOA and FH in the patients’ sera was confirmed by western blotting (Fig. 2). We also evaluated the antibody levels through AlphaLISA, which allowed us to compare the levels between patients and HDs. Our results showed that compared with HDs, patients with TIA, aCI, or oCI had significantly elevated levels of ALDOA-Abs and FH-Abs (Fig. 3). We further found that these antibodies are independent predictors (the interference of age, sex, and area was excluded) of TIA by a clinical statistical analysis (Table 3). Of note, TIA tends to develop into aCI, thereby a clear risk factor of aCI [39]. As independent early-warning risk factors of TIA, the elevated ALDOA-Ab and FH-Ab levels may also be predictive markers of aCI. Therefore, we further confirmed it by the statistical analysis of prospective case–control studies nested in large community-based samples (Table 5).
ALDOA is one of the glycolytic enzymes that catalyze the reversible conversion of fructose-1,6-bisphosphate into glyceraldehyde-3-phosphate and dihydroxyacetone phosphate [40]. ALDOA is widely distributed in the entire body tissues. As a catalytic enzyme, ALDOA represents as one of the key enzymes in glycolysis. Of note, it participates in the hypoxic responses regulating both glucose and energy metabolisms and can be a hypoxia biomarker [41]. Ischemic stroke is a typical atherosclerosis-related disease, with local tissue hypoxia as its basic pathophysiological feature. ALDOA is also a hypoxia-inducible gene expression product [42]. When brain tissue undergoes ischemia or hypoxia, both glucose uptake and metabolism are stimulated to compensate for the reduced energy production by inducing ALDOA overexpression [43]. Hypoxia-inducible factor 1-alpha (HIF-1α), which is a transcription factor that is sensitive to hypoxia-inducible genes, upregulates ALDOA expression in hypoxic cells [44], thereby enhancing its glycolysis metabolism. Chang et al. proved that ALDOA overexpression upregulates the expression of matrix metalloproteinase (MMP) 9 via HIF-1α [45]. These results are in line with our previous study [27] wherein anti-MMP1 antibodies demonstrated increased specificity in the serum of patients with TIA. MMPs can degrade the main components of the vascular extracellular matrix and is an important factor responsible for the induction of atherosclerosis. A close relationship between ALDOA and MMPs suggests that ALDOA overexpression may not only be a sequential pathological process in TIA development; it may also be related to the initiation and deterioration of TIA. Moreover, the present study revealed the ALDOA-Ab levels were well associated with HT, CHD, and habitual smoking, but not with sex, DM, HL, alcohol abuse, and obesity (Table 6). ALDOA-Abs were also associated with max IMT, metabolic disturbance (e.g., blood sugar, total cholesterol, and total protein), and inflammation (e.g., white blood cell count and C-reactive protein) (Table 7). Thus, the serum ALDOA-Ab marker can discriminate HT-induced atherosclerotic TIA and aCI.
Meanwhile, FH is a key enzyme involved in the tricarboxylic acid (TCA) cycle. It can reversibly catalyze the conversion of fumaric acid into L-malate in the cells [46]. The TCA cycle mainly functions by oxidizing pyruvate supplied by the glycolytic pathway, with the goal of producing energy. Aside from its classical metabolic functions, FH has other nonmetabolic functions under cellular stimulation [47]. FH has been reported to be associated with tumorigenesis, specifically by altering the gene expression and configuration of tumor cells [48]. Xiao et al. found that FH could antagonize α-ketoglutarate-dependent demethylase through its metabolite fumarate, thereby affecting histone methylation [49]. In addition, Wang et al. showed that in the absence of glucose or hypoxia, which inhibits histone demethylation by lysine-specific demethylase 2A, FH exhibits adenosine monophosphate–activated protein kinase–mediated phosphorylation [50]. FH inhibits histone methylation by reducing the physiological activity of vascular endothelial growth factor (VEGF) [51]. This outcome, in turn, affects the repair and remodeling of the vascular endothelium after atherosclerosis. Of note, abnormal histone methylation is responsible for significant changes in the expression of genes, including VEGF. FH regulates the occurrence and development of atherosclerosis [52], consistent with our finding that the FH-Ab levels in patients with TIA and ischemic stroke are significantly higher than those in HDs (Fig. 3).
Hyperlipidemia contains the following three criteria: total cholesterol > 220 mg/dL, triglyceride > 150 mg/dL, or regular use of lipid-lowering agents; in addition, it is one of the risk factors for atherosclerosis [53]. However, the atherosclerosis markers ALDOA-Ab and FH-Ab were not associated with hyperlipidemia, but with hypertension (Tables 6 and 7). Atherosclerosis is a multifactorial disease [54], and the upstream atherosclerosis-inducing mechanism via hyperlipidemia could be different from that via hypertension, of which the latter pathway might be accompanied with the elevated expression of ALDOA and FH.
Given that TIA is one of the prodromal stages of aCI, ALDOA-Abs and FH-Abs could be used as risk predictors of TIA and aCI. To examine this hypothesis, we conducted a case–control study nested within the JPHC-based Prospective Study. The ALDOA-Ab and FH-Ab levels were measured in 202 cases of incident CI documented between the baseline and 2008, and in 202 controls with matching age, sex, and area. Subsequently, the ALDOA-Ab and FH-Ab levels for aCI (associated with atherosclerosis) were estimated using a conditional logistic regression model. Our results showed that both the antibody levels were positively and strongly associated with the risk for aCI (Table 5). Therefore, such antibody markers can be applied to predictive diagnosis rather than simple risk evaluation.
Although the PPVs of ALDOA-Abs and FH-Abs for TIA were 69.57% and 55.43%, respectively (Fig. 4), they increased when combined with conventional risk factors such as age, HT, and DM (Table 4). Especially, 100% of PPV was attained by combining ALDOA-Abs with HT and DM or combining FH-Abs with age and DM. Thus, antibody markers combined with clinical risk factors improve the ability to predict TIA, suggesting that this combination is also applicable to the early prediction of aCI. The ALDOA-Ab and FH-Ab levels correlated with CHD, HT, habitual smoking (ALDOA-Ab), DM (FH-DM) (Table 6), age, max IMT, C-reactive protein, and blood sugar (Table 7). Max IMT is one of typical indices of atherosclerosis, and CHD and DM are atherosclerosis-related diseases. Furthermore, HT, habitual smoking, age, C-reactive protein, and blood sugar are risk factors of atherosclerosis. Therefore, ALDOA-Abs and FH-Abs are biomarkers for atherosclerotic ischemic stroke. The large-scale JPHC cohort analysis also showed that these antibody markers were useful predictors of aCI onset.
Conclusion
The levels of antibodies against ALDOA and FH were significantly higher in patients with TIA or aCI than in HDs. These antibody markers can be novel predictors of TIA and pre-onset aCI, which are induced by atherosclerosis.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- TIA:
-
Transient ischemic attack
- aCI:
-
Acute cerebral infarction
- HD:
-
Healthy donor
- oCI:
-
Old cerebral infarction
- HT:
-
Hypertension
- DM:
-
Diabetes mellitus
- CHD:
-
Coronary heart disease
- BMI:
-
Body mass index
- SEREX:
-
Serological identification of antigens by recombinant cDNA expression cloning
- E. coli :
-
Escherichia coli
- GST:
-
Glutathione-S-transferase
- AlphaLISA:
-
Amplified luminescent proximity homogeneous assay-linked immunosorbent assay
- JPHC:
-
The Japan Public Health Center-based Prospective Study
- OR:
-
Odds ratio
- ROC:
-
Receiver operating characteristic
- ALDOA:
-
Aldolase A, fructose-bisphosphate
- ALDOA-Ab:
-
Anti-ALDOA antibody
- FH:
-
Fumarate hydratase
- FH-Ab:
-
Anti-FH antibody
- 95% CI:
-
95% Confidence interval
- PPV:
-
Positive predictive value
- max IMT:
-
Maximum intima-media thickness
- HIF-1α:
-
Hypoxia-inducible factor 1α
- MMP:
-
Matrix metalloproteinase
- VEGF:
-
Vascular endothelial growth factor
References
Easton JD, Saver JL, Albers GW, Alberts MJ, Chaturvedi S, Feldmann E, et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke. 2009;40(6):2276–93. https://doi.org/10.1161/STROKEAHA.108.192218.
Sacco RL, Kasner SE, Broderick JP, Caplan LR, Connors J, Culebras A, et al. An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44(7):2064–89. https://doi.org/10.1161/STR.0b013e318296aeca.
Lisabeth LD, Ireland JK, Risser JM, Brown DL, Smith MA, Garcia NM, Morgenstern LB. Stroke risk after transient ischemic attack in a population-based setting. Stroke. 2004;35(8):1842–6. https://doi.org/10.1161/01.STR.0000134416.89389.9d.
Kleindorfer D, Panagos P, Pancioli A, Khoury J, Kissela B, Woo D, et al. Incidence and short-term prognosis of transient ischemic attack in a population-based study. Stroke. 2005;36(4):720–3. https://doi.org/10.1161/01.STR.0000158917.59233.b7.
Kernan WN, Ovbiagele B, Black HR, Bravata DM, Chimowitz MI, Ezekowitz MD, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(7):2160–236. https://doi.org/10.1161/STR.0000000000000024.
Bonow RH, Witt CE, Mosher BP, Mossa-Basha M, Vavilala MS, Rivara FP, et al. Transcranial Doppler microemboli monitoring for stroke risk stratification in blunt cerebrovascular injury. Crit Care Med. 2017;45(10):e1011–7. https://doi.org/10.1097/CCM.0000000000002549.
Coutts SB, Modi J, Patel SK, Demchuk AM, Goyal M, Hill MD, et al. CT/CT angiography and MRI findings predict recurrent stroke after transient ischemic attack and minor stroke: results of the prospective CATCH study. Stroke. 2012;43(4):1013–7. https://doi.org/10.1161/STROKEAHA.111.637421.
Wolpert S, Caplan LR. Current role of cerebral angiography in the diagnosis of cerebrovascular diseases. AJR Am J Roentgenol. 1992;159(1):191–7. https://doi.org/10.2214/ajr.159.1.1609697.
Stemme S, Faber B, Holm J, Wiklund O, Witztum JL, Hansson GK. T lymphocytes from human atherosclerotic plaques recognize oxidized low density lipoprotein. Proc Natl Acad Sci USA. 1995;92(9):3893–7. https://doi.org/10.1073/pnas.92.9.3893.
Homocysteine Studies Collaboration. Homocysteine and risk of ischemic heart disease and stroke: a meta-analysis. JAMA. 2002;288(16):2015–22. https://doi.org/10.1001/jama.288.16.2015.
Nambi V, Hoogeveen RC, Chambless L, Hu Y, Bang H, Coresh J, et al. Lipoprotein-associated phospholipase A2 and high-sensitivity C-reactive protein improve the stratification of ischemic stroke risk in the atherosclerosis risk in communities (ARIC) study. Stroke. 2009;40(2):376–81. https://doi.org/10.1161/STROKEAHA.107.513259.
Kramer J, Harcos P, Prohászka Z, Horváth L, Karádi I, Singh M, et al. Frequencies of certain complement protein alleles and serum levels of anti-heat-shock protein antibodies in cerebrovascular diseases. Stroke. 2000;31(11):2648–52. https://doi.org/10.1161/01.str.31.11.2648.
O’Donnell MJ, Xavier D, Liu L, Zhang H, Chin SL, Rao-Melacini P, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet. 2010;376(9735):112–23. https://doi.org/10.1016/S0140-6736(10)60834-3.
Dolmans LS, Rutten FH, El Bartelink ML, Seppenwoolde G, van Delft S, Kappelle LJ, Hoes AW. Serum biomarkers for the early diagnosis of TIA: The MIND-TIA study protocol. BMC Neurol. 2015;15:119. https://doi.org/10.1186/s12883-015-0388-z.
Amarenco P, Cohen A, Tzourio C, Bertrand B, Hommel M, Besson G, et al. Atherosclerotic disease of the aortic arch and the risk of ischemic stroke. New Engl J Med. 1994;331(22):1474–9. https://doi.org/10.1056/NEJM199412013312202.
Matsuura E, Atzeni F, Sarzi-Puttini P, Turiel M, Lopez LR, Nurmohamed MT. Is atherosclerosis an autoimmune disease? BMC Med. 2014;12:47. https://doi.org/10.1186/1741-7015-12-47.
Matsuura E, Kobayashi K, Lopez LR. Atherosclerosis in autoimmune diseases. Curr Rheumatol Rep. 2009;11(1):61–9. https://doi.org/10.1007/s11926-009-0009-1.
Hiwasa T, Zhang XM, Kimura R, Ohno M, Chen PM, Nishi E, et al. Elevated adiponectin antibody levels in serum of patients with atherosclerosis-related coronary artery disease, cerebral infarction and diabetes mellitus. J Circ Biomark. 2016;5:8. https://doi.org/10.5772/63218.
Sahin U, Türeci O, Schmitt H, Cochlovius B, Johannes T, Schmits R, et al. Human neoplasms elicit multiple specific immune responses in the autologous host. Proc Natl Acad Sci USA. 1995;92(25):11810–3. https://doi.org/10.1073/pnas.92.25.11810.
Türeci O, Usener D, Schneider S, Sahin U. Identification of tumor-associated autoantigens with SEREX. Methods Mol Med. 2005;109:137–54. https://doi.org/10.1385/1-59259-862-5:137.
Scanlan MJ. Identification of human tumor antigens by serological analysis of recombinant cDNA expression libraries (SEREX). Curr Protoc Immunol. 2005;Chapter 20:Unit 20.7. https://doi.org/10.1002/0471142735.im2007s65.
Lim Y, Lee DY, Lee S, Park SY, Kim J, Cho B, et al. Identification of autoantibodies associated with systemic lupus erythematosus. Biochem Biophys Res Commun. 2002;295(1):119–24. https://doi.org/10.1016/s0006-291x(02)00637-x.
Kaneko M, Ono T, Matsubara T, Yamamoto Y, Ikeda H, Yoshiki T, et al. Serological identification of endothelial antigens predominantly recognized in Kawasaki disease patients by recombinant expression cloning. Microbio Immunol. 2004;48(9):703–11. https://doi.org/10.1111/j.1348-0421.2004.tb03472.x.
Lu Y, Ye P, Chen SL, Tan EM, Chan EK. Identification of kinectin as a novel Behçet’s disease autoantigen. Arthritis Res Ther. 2005;7(5):R1133–9. https://doi.org/10.1186/ar1798.
Muto M, Mori M, Hiwasa T, Takiguchi M, Iwadate Y, Uzawa A, et al. Novel serum autoantibodies against talin1 in multiple sclerosis: possible pathogenetic roles of the antibodies. J Neuroimmunol. 2015;284:30–6. https://doi.org/10.1016/j.jneuroim.2015.05.005.
Machida T, Kubota M, Kobayashi E, Iwadate Y, Saeki N, Yamaura A, et al. Identification of stroke-associated-antigens via screening of recombinant proteins from the human expression cDNA library (SEREX). J Transl Med. 2015;13(1):71. https://doi.org/10.1186/s12967-015-0393-4.
Wang H, Zhang XM, Tomiyoshi G, Nakamura R, Shinmen N, Kuroda H, et al. Association of serum levels of antibodies against MMP1, CBX1, and CBX5 with transient ischemic attack and cerebral infarction. Oncotarget. 2017;9(5):5600–13. https://doi.org/10.18632/oncotarget.23789.
Hiwasa T, Machida T, Zhang XM, Kimura R, Wang H, Iwase K, et al. Elevated levels of autoantibodies against ATP2B4 and BMP-1 in sera of patients with atherosclerosis-related diseases. Immunome Res. 2015;11(2):097. https://doi.org/10.4172/17457580.1000097.
Hiwasa T, Zhang XM, Kimura R, Machida T, Kitamura K, Yamazoe R, et al. Association of serum antibody levels against TUBB2C with diabetes and cerebral infarction. Gratis J Biomed Sci. 2015;1(2):49–63. https://doi.org/10.18314/gjbs.v1i2.27.
Hiwasa T, Tomiyoshi G, Nakamura R, Shinmen N, Kuroda H, Kunimatsu M, et al. Serum SH3BP5-specific antibody level is a biomarker of atherosclerosis. Immunome Res. 2017;13(2):132. https://doi.org/10.4172/1745-7580.1000132.
Naghavi M, Libby P, Falk E, Casscells SW, Litovsky S, Rumberger J, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: Part I. Circulation. 2003;108(14):1664–72. https://doi.org/10.1161/01.CIR.0000087480.94275.97.
Adams HP Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in acute stroke treatment. Stroke. 1993;24(1):35–41. https://doi.org/10.1161/01.str.24.1.35.
Yoshida Y, Zhang XM, Wang H, Machida T, Mine S, Kobayashi E, et al. Elevated levels of autoantibodies against DNAJC2 in sera of patients with atherosclerotic diseases. Heliyon. 2020;6(8): e04661. https://doi.org/10.1016/j.heliyon.2020.e04661.
Zhang XM, Wang H, Mine S, Takemoto M, Yokote K, Kitamura K, et al. Association of serum anti-prolylcarboxypeptidase antibody marker with atherosclerotic diseases accompanied by hypertension. J Mol Biomark Diagn. 2017;8(5):361. https://doi.org/10.4172/2155-9929.1000361.
Nakashima K, Shimada H, Ochiai T, Kuboshima M, Kuroiwa N, Okazumi S, et al. Serological identification of TROP2 by recombinant cDNA expression cloning using sera of patients with esophageal squamous cell carcinoma. Int J Cancer. 2004;112(6):1029–35. https://doi.org/10.1002/ijc.20517.
Adachi-Hayama M, Adachi A, Shinozaki N, Matsutani T, Hiwasa T, Takiguchi M, et al. Circulating anti-filamin C autoantibody as a potential serum biomarker for low-grade gliomas. BMC Cancer. 2014;14(1):452. https://doi.org/10.1186/1471-2407-14-452.
Tsugane S, Sawada N. The JPHC study: design and some findings on the typical Japanese diet. Jpn J Clin Oncol. 2014;44(9):777–82. https://doi.org/10.1093/jjco/hyu096.
Yamagishi K, Iso H, Kokubo Y, Saito I, Yatsuya H, Ishihara J, et al. Dietary intake of saturated fatty acids and incident stroke and coronary heart disease in Japanese communities: the JPHC Study. Eur Heart J. 2013;34(16):1225–32. https://doi.org/10.1093/eurheartj/eht043.
Wu CM, McLaughlin K, Lorenzetti DL, Hill MD, Manns BJ, Ghali WA. Early risk of stroke after transient ischemic attack: a systematic review and meta-analysis. Arch Intern Med. 2007;167(22):2417–22. https://doi.org/10.1001/archinte.167.22.2417.
Rottmann WH, Tolan DR, Penhoet EE. Complete amino acid sequence for human aldolase B derived from cDNA and genomic clones. Proc Natl Acad Sci USA. 1984;81(9):2738–42. https://doi.org/10.1073/pnas.81.9.2738.
Zeng Y, Lv Y, Tao L, Ma J, Zhang H, Xu H, et al. G6PC3, ALDOA and CS induction accompanies mir-122 down-regulation in the mechanical asphyxia and can serve as hypoxia biomarkers. Oncotarget. 2016;7(46):74526–36. https://doi.org/10.18632/oncotarget.12931.
Kawai K, Uemura M, Munakata K, Takahashi H, Haraguchi N, Nishimura J, et al. Fructose-bisphosphate aldolase A is a key regulator of hypoxic adaptation in colorectal cancer cells and involved in treatment resistance and poor prognosis. Int J Oncol. 2017;50(2):525–34. https://doi.org/10.3892/ijo.2016.3814.
Semenza GL, Roth PH, Fang HM, Wang GL. Transcriptional regulation of genes encoding glycolytic enzymes by hypoxia-inducible factor 1. J Biol Chem. 1994;269(38):23757–63. https://doi.org/10.1016/0092-8674(94)90283-6.
Grandjean G, De Jong PR, James BP, Koh MY, Lemos R, Kingston J, et al. Definition of a novel feed-forward mechanism for glycolysis-HIF1α signaling in hypoxic tumors highlights aldolase A as a therapeutic target. Cancer Res. 2016;76(14):4259–69. https://doi.org/10.1158/0008-5472.CAN-16-0401.
Chang YC, Chan YC, Chang WM, Lin YF, Yang CJ, Su CY, et al. Feedback regulation of ALDOA activates the HIF-1α/MMP9 axis to promote lung cancer progression. Cancer Lett. 2017;403:28–36. https://doi.org/10.1016/j.canlet.2017.06.001.
Yogev O, Yogev O, Singer E, Shaulian E, Goldberg M, Fox TD, Pines O. Fumarase: a mitochondrial metabolic enzyme and a cytosolic/nuclear component of the DNA damage response. PLoS Biol. 2010;8(3): e1000328. https://doi.org/10.1371/journal.pbio.1000328.
Yang W, Xia Y, Hawke D, Li X, Liang J, Xing D, et al. PKM2 phosphorylates histone H3 and promotes gene transcription and tumorigenesis. Cell. 2012;150(4):685–96. https://doi.org/10.1016/j.cell.2012.07.018.
Yang M, Soga T, Pollard PJ, Adam J. The emerging role of fumarate as an oncometabolite. Front Oncol. 2012;2:85. https://doi.org/10.3389/fonc.2012.00085.
Xiao M, Yang H, Xu W, Ma S, Lin H, Zhu H, et al. Inhibition of α-KG-dependent histone and DNA demethylases by fumarate and succinate that are accumulated in mutations of FH and SDH tumor suppressors. Gene Dev. 2012;26(12):1326–38. https://doi.org/10.1101/gad.191056.112.
Wang T, Yu Q, Li J, Hu B, Zhao Q, Ma C, et al. O-GlcNAcylation of fumarase maintains tumour growth under glucose deficiency. Nat Cell Biol. 2017;19(7):833–43. https://doi.org/10.1038/ncb3562.
Huang T, Yuan GF, Zhang ZG, Zou ZQ, Li D. Cardiovascular pathogenesis in hyperhomocysteinemia. Asia Pac J Clin Nutr. 2008;17(1):8–16. https://doi.org/10.6133/apjcn.2008.17.1.02.
Kim YR, Kim CS, Naqvi A, Kumar A, Kumar S, Hoffman TA, Irani K. Epigenetic upregulation of p66shc mediates low-density lipoprotein cholesterol-induced endothelial cell dysfunction. Am J Physiol Heart Circ Physiol. 2012;303(2):H189–96. https://doi.org/10.1152/ajpheart.01218.2011.
Chen T, Wu Y, Gu W, Xu Q. Response of vascular mesenchymal stem/progenitor cells to hyperlipidemia. Cell Mol Life Sci. 2018;75(22):4079–91. https://doi.org/10.1007/s00018-018-2859-z.
Valanti EK, Dalakoura-Karagkouni K, Siasos G, Kardassis D, Eliopoulos AG, Sanoudou D. Advances in biological therapies for dyslipidemias and atherosclerosis. Metabolism. 2021;116: 154461. https://doi.org/10.1016/j.metabol.2020.154461.
Acknowledgements
The authors would like to thank Prof. Masaki Takiguchi (Department of Biochemistry and Genetics, Graduate School of Medicine, Chiba University) for valuable discussion and suggestion.
Funding
The design of this study was supported in part by a research grant from the Japan Agency for Medical Research and Development (AMED) of Japan (Practical Research Project for Life-Style related Diseases including Cardiovascular Diseases and Diabetes Mellitus). Sample collection, preparation, analysis, and interpretation of data were supported by JSPS KAKENHI (Grant Number: 20K17953, 19K09451, 17K19810, and 17K16626). International collaborative research was supported by Natural Science Foundation of Guangdong Province, China (Grant NO: 2018A0303131003), Science and Technology Program of Guangzhou, China (Grant NO: 201707010449), and Toka-Donghua Educational and Cultural Exchange Foundation, and Setsuro Fujii Memorial of Medical Sciences and The Osaka Foundation for Promotion of Fundamental Medical Research. JPHC Study was supported by National Cancer Center Research and Development Fund (since 2011) and a Grant-in-Aid for Cancer Research from the Ministry of Health, Labour and Welfare of Japan (from 1989 to 2010).
Author information
Authors and Affiliations
Contributions
HW, EK, YI, KG, AX, and TH conceived and designed the experiments; HW, XMZ, YY, KS, GT, and RN performed the experiments; HW, HL, HI, MS, KY, NS1, ST, AA1, TM1, and TM2 analyzed and interpreted the data; SM, IK, TW, AA2, HT, KK, HS, NS2, and HK contributed reagents, materials, analysis tools or data; HW, HL, EK, YI, KY, NSa, and TH wrote the paper. The author(s) read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Our study conformed to the ethical standards of the 1964 Declaration of Helsinki and its later amendments. This study was approved by the Ethics Committee of the Graduate School of Medicine, Chiba University (No. 2012–438, No. 2014–44, No. 2016–86, No. 2017–251, No. 2018–320, No. 2020–1129), including the cooperating Chiba Prefectural Sawara Hospital, Chiba Rosai Hospital, Chiba Aoba Municipal Hospital, and Port Square Kashiwado Clinic. All participating studies, except the JPHC study, obtained written informed consent from all participants according to the protocols approved by their institutional ethical committees. The JPHC study was launched in 1990 before the enactment of ethical guidelines in Japan (2002); thus, obtaining written informed consent for blood sample collection (1990–1994) was not mandatory. After being provided with a written or verbal explanation, the participants were asked to provide blood for this study, and their informed consent was obtained in writing or verbally. Their verbal consent was recorded in the list during blood collection. Additionally, in accordance with the ethical guidelines enacted after blood collection, a research summary was published on the homepage, which guarantees the participants the opportunity to refuse participation (https://epi.ncc.go.jp/jphc/764/3701.html). The institutional ethical committees in National Cancer Center approved this study (Approved No. 2003–054).
Consent for publication
Not applicable.
Competing interests
This work was performed in collaboration with Fujikura Kasei Co., Ltd. Go Tomiyoshi, Rika Nakamura, Natsuko Shinmen, and Hideyuki Kuroda are employees of Fujikura Kasei Co., Ltd.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, H., Lu, H., Zhang, XM. et al. Association of serum levels of antibodies against ALDOA and FH4 with transient ischemic attack and cerebral infarction. BMC Neurol 21, 274 (2021). https://doi.org/10.1186/s12883-021-02301-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-021-02301-w