
Abstract
Background
Osler’s nodes, Janeway lesions and splinter haemorrhages are cutaneous manifestations of infective endocarditis. They occur due to vascular occlusion by septic emboli and a resulting localized vasculitis. They are usually bilateral. We report a case of unilateral Osler’s nodes, Janeway lesions and splinter haemorrhages due to an ipsilateral surgical arterio-venous fistula infection.
Case presentation
A fifty-two-year-old Sri Lankan female with end stage kidney disease presented with fever for five days with blurred vision, pain and redness of the right eye. She had a left brachio-cephalic arterio-venous fistula (AVF) created one month back. She complained of a foul-smelling discharge from the surgical site for past three days. Redness of the right eye with a hypopyon was noted. AVF site over the left cubital fossa was infected with a purulent discharge. Osler’s nodes, Janeway lesions and splinter haemorrhages were noted in the distal fingers, thenar and hypothenar eminences of the left hand. Right hand and both feet were normal. No cardiac murmurs were heard. Blood cultures, vitreous sample cultures and pus cultures from the fistula site were all positive for methicillin sensitive Staphylococcus aureus. Infective endocarditis was excluded by a trans-oesophageal echocardiogram. She was treated with IV flucloxacillin and surgical excision of the AVF.
Conclusion
Infections of AVF can result in septic emboli formation which can have both anterograde arterial embolization and retrograde venous embolization. Arterial embolization can result in unilateral Osler’s nodes, Janeway lesions and splinter haemorrhages. Venous embolization can cause metastatic infections in the systemic and pulmonary circulations.
Similar content being viewed by others

Introduction
Osler’s nodes, Janeway lesions and splinter haemorrhages are cutaneous manifestations of infective endocarditis [1]. Osler’s nodes are tender violaceous cutaneous nodules that occur in the distal ends of fingers and over thenar and hypothenar eminences. It is hypothesized to occur due to vascular occlusion by septic micro-emboli causing localised vasculitis with or without micro-abscess formation [2]. Janeway lesions are non-tender, erythematous macules commonly found on palms and soles [3]. Splinter haemorrhages are red–brown to purple–black, thin longitudinal lines in the distal portion of nails which occur in diverse conditions including infective endocarditis [4]. The above cutaneous signs usually occur bilaterally. We describe a case of unilateral Osler’s nodes, Janeway lesions and splinter haemorrhages in the setting of an infected ipsilateral brachio-cephalic arterio-venous fistula (AVF).
Case presentation
A fifty-two-year-old Sri Lankan female with end stage kidney got admitted with five days of fever and a painful red right eye. She was receiving regular haemodialysis via a right subclavian tunnelled catheter. The chronic kidney disease was secondary to long standing, poorly controlled diabetes and hypertension. Her diabetes was complicated with proliferative retinopathy and right sided vitreous haemorrhage which occured 2 weeks ago. The visual acuity in the right eye following the haemorrhage was 20/70. Over the last five days the vision deteriorated to complete blindness. She had a left sided brachio-cephalic AVF created one month back. There was a purulent discharge from the surgical site over the past 3 days.
On examination she had a right sided red eye with a hypopyon, suggestive of endophthalmitis. The surgical site was dehiscent with foul smelling pus discharge. A thrill was felt at the fistula site. The left hand had Osler’s nodes, Janeway lesions and splinter haemorrhages (Fig. 1). The right hand and feet were normal. There were no cardiac murmurs.

Right hand (A) is normal while the left hand (B) has Osler’s nodes and Janeway lesions over the thenar and hypothenar eminences (arrow). The lesions over the thenar eminence are magnified in C which shows Osler’s nodes (arrow) and Janeway lesions (arrowhead). Splinter haemorrhages of the left nailbed (arrow) and the normal nails of the right hand are shown in D
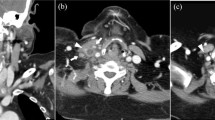
Three blood cultures from different sites, vitreous sample cultures and surgical site swab cultures were persistently positive for methicillin sensitive Staphylococcus aureus (MSSA). The in-vitro incubation periods were similar for blood cultures from the peripheral veins and the tunnelled catheter. The tunnelled catheter was removed, and the tip culture did not grow any organisms. No valvular vegetations, insufficiency or abscesses were noted in the trans-oesophageal echocardiogram. There was no evidence of a patent foramen ovale. A diagnosis of ‘left brachio-cephalic AVF surgical site infection and right endophthalmitis due to systemic embolization’ was arrived at. The relevant biochemical and haematological parameters on admission are given in Table 1.
She was treated with high dose IV flucloxacillin for 4 weeks and intra vitreous vancomycin. A temporary vascular catheter was inserted to the right internal jugular vein after 3 days of IV antibiotics, by which time the fever had settled; for haemodialysis every third day. The temporary catheter was changed every 6th day. The surgical site was explored, irrigated and the fistula was excised. The excised tissue did not grow any organisms; probably because the excision was done 1 week after the initiation of IV antibiotics. The infection was completely treated, but the patient continued to be blind in the right eye.
Discussion and conclusions
We report a case of unilateral Osler’s nodes, Janeway lesions and splinter haemorrhages secondary to AVF site infection. Arterio-venous fistulae are created for easy vascular access during haemodialysis in patients with end-stage kidney disease. A brachio-cephalic fistula is created by anastomosing the brachial artery and the cephalic vein at the cubital fossa [5]. In a mature brachio-cephalic fistula, most of the blood in the brachial artery flow into the cephalic vein while the rest, flow to the forearm and hand along the radial and ulnar arteries.
The incidence of arterio-venous fistulae infection is around 0.9% [6]. Despite the common occurrence, unilateral Osler’s nodes, Janeway lesions and Splinter haemorrhages are not recognised signs of AVF infections. Mousa et al. [7] have described a patient with a left brachio-axillary polytetrafluoroethylene (PTFE) vascular graft infection, who was found to have splinter haemorrhages and Janeway lesions on the left hand without similar findings in the right hand. This probably is the first reported case of unilateral Janeway lesions or splinter haemorrhages [7]. Despite an extensive search we could not find any other case describing the above phenomenon. We report the first case of direct surgical arterio-venous fistula (without a prosthetic graft) infection leading to unilateral Janeway lesions, Osler’s nodes and splinter haemorrhages.
Infection of the AVF can be either a peri-vascular cellulitis or infection of the vessels itself (endarteritis) [8]. We hypothesize that the infection of the brachio-cephalic fistula generated septic micro-thrombi which embolized both distally along the radial and ulnar arteries, and proximally along the arterialised cephalic vein. The fistula provided a means to bypass the capillary circulation which would otherwise filter the emboli, preventing it from reaching the venous circulation. Anterograde (distal), localised brachial arterial embolization resulted in Osler’s nodes, Janeway lesions and splinter haemorrhages in the ipsilateral hand whereas retrograde/venous embolization led to systemic (and potentially pulmonary) embolization. In the index patient, systemic embolization manifested as right side endophthalmitis. The pathways taken by arterial and venous emboli are depicted in Fig. 2.

Pathways taken by septic emboli in anterograde arterial embolization and retrograde venous embolization
Despite the fact that AVF site infection cause retrograde-venous embolization which reach the systemic circulation, Osler’s nodes and Janeway lesions were not noted on the right hand or feet in the index patient. Although there is a high blood flow from the brachial artery to the cephalic vein (due to the high-pressure gradient between the artery and the vein), we hypothesize that the retrograde septic emboli got filtered in the pulmonary circulation. Therefore, blood flowing to the contralateral (right) hand would have had a lesser concentration of emboli leading to a lesser density of embolic phenomena (or none), compared to anterograde brachial arterial embolization to the ipsilateral (left) hand. Furthermore, the venous emboli would have been diluted in a higher volume of blood at the cardiac chambers. This also would contribute to the difference in the number of Osler’s nodes and Janeway lesions between the two hands.
Therefore, we can postulate that; in brachio-cephalic AVF infections, the hand ipsilateral to the AVF (with anterograde arterial embolization) will have a higher density of embolic phenomena whereas the opposite hand and legs (embolization through systemic circulation) will have a comparably lower number of lesions; or none as in the index case.
In conclusion AVF infections can cause both arterial and venous embolization. Arterial embolization can manifest as unilateral (or differential) Osler’s nodes, Janeway lesions and splinter haemorrhages of the ipsilateral hand. Venous embolization can lead to metastatic infection in the systemic and pulmonary circulations.
Availability of data and materials
The clinical records of the patient are available from the corresponding author on reasonable request.
Abbreviations
- AVF:
-
Arterio-venous fistula
- ECG:
-
Electrocardiogram
- ESR:
-
Erythrocyte sedimentation rate
- MSSA:
-
Methicillin sensitive Staphylococcus aureus
- PTFE:
-
Polytetrafluoroethylene
References
Murdoch DR, Corey RG, Hoen B, Miró M, Fowler VG, Bayer AS, et al. Clinical presentation, etiology and outcome of infective endocarditis in the 21st century: the international collaboration on endocarditis-prospective cohort study. Arch Intern Med. 2009;169:463.
Marrie TJ. Osler’s nodes and Janeway lesions. Am J Med. 2008;121:105–6.
Pino Gil M, Velasco M, Botella R, Ballester JE, Pedro F, Aliaga A. Janeway lesions: differential diagnosis with Osler’s nodes. Int J Dermatol. 1993;32:673–4.
Haber R, Khoury R, Kechichian E, Tomb R. Splinter hemorrhages of the nails: a systematic review of clinical features and associated conditions. Int J Dermatol. 2016;55:1304–10.
Bunch C. Creation of brachiocephalic fistula BT - operative dictations in general and vascular surgery. In: Hoballah JJ, Scott-Conner CEH, Chong H Sen, editors. Cham: Springer International Publishing; 2017. p. 871–2.
Schild AF, Perez E, Gillaspie E, Seaver C, Livingstone J, Thibonnier A. Arteriovenous fistulae vs. arteriovenous grafts: a retrospective review of 1,700 consecutive vascular access cases. J Vasc Access. 2008;9:231–5.
Mousa M, Habte-Gabr E, Mueller W. Infected arteriovenous hemodialysis graft presenting as left and right infective endocarditis. Am J Nephrol. 1995;15:521–3.
MacRae JM, Dipchand C, Oliver M, Moist L, Yilmaz S, Lok C, et al. Arteriovenous access: infection, neuropathy, and other complications. Can J Kidney Heal Dis. 2016;3:2054358116669127.
Acknowledgements
None.
Funding
No funding involved.
Author information
Authors and Affiliations
Contributions
PR, HA and PK were involved in diagnosing and managing the patient. PR and HA drafted the manuscript while PW and PK critically revised it.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent will be provided to the Editor-in-Chief of this journal upon request.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ruwanpathirana, P., Athukorala, H., Weeratunga, P. et al. Unilateral Osler nodes, Janeway lesions and splinter haemorrhages associated with surgical arterio-venous fistula infection: a case report. BMC Infect Dis 23, 451 (2023). https://doi.org/10.1186/s12879-023-08439-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-023-08439-x