
Abstract
Background
Micronutrients are minerals and vitamins and they are essential for normal physiological activities. The objectives of the study were to describe the progress and determinants of micronutrient levels and to assess the effects of micronutrients in the treatment outcome of kalazar.
Methods
A prospective cohort study design was used. The data were collected using patient interviews, measuring anthropometric indicators, and collecting laboratory samples. The blood samples were collected at five different periods during the leishmaniasis treatments: before starting anti-leishmaniasis treatments, in the first week, in the second week, in the third week, and in the 4th week of anti-leishmaniasis treatments. Descriptive statistics were used to describe the profile of patients and to compare the treatment success rate. The generalized estimating equation was used to identify the determinants of serum micronutrients.
Results
The mean age of the patients were 32.88 years [SD (standard deviation) ±15.95]. Male constitute 62.3% of the patients and problematic alcohol use was present in 11.5% of the patients. The serum zinc level of visceral leishmaniasis patients was affected by alcohol (B − 2.7 [95% CI: − 4.01 - -1.5]), DDS (B 9.75 [95% CI: 7.71–11.79]), family size (B -1.63 [95% CI: − 2.68 - -0.58]), HIV (B -2.95 [95% CI: − 4.97 - -0.92]), and sex (B − 1.28 [95% CI: − 2.5 - -0.07]). The serum iron level of visceral leishmaniasis patients was affected by alcohol (B 7.6 [95% CI: 5.86–9.35]), family size (B -5.14 [95% CI: − 7.01 - -3.28]), malaria (B -12.69 [95% CI: − 14.53 - -10.87]), Hookworm (− 4.48 [− 6.82 - -2.14]), chronic diseases (B -7.44 [95% CI: − 9.75 - -5.13]), and HIV (B -5.51 [95% CI: − 8.23 - -2.78]). The serum selenium level of visceral leishmaniasis patient was affected by HIV (B -18.1 [95% CI: − 20.63 - -15.58]) and family size (B -11.36 [95% CI: − 13.02 - -9.7]). The iodine level of visceral leishmaniasis patient was affected by HIV (B -38.02 [95% CI: − 41.98 - -34.06]), DDS (B 25 .84 [95% CI: 22.57–29.1]), smoking (B -12.34 [95% CI: − 15.98 - -8.7]), chronic illness (B -5.14 [95% CI: − 7.82 - -2.46]), and regular physical exercise (B 5.82 [95% CI: 0.39–11.26]). The serum vitamin D level of visceral leishmaniasis patient was affected by HIV (B -9.43 [95% CI: − 10.92 - -7.94]), DDS (B 16.24 [95% CI: 14.89–17.58]), malaria (B -0.61 [95% CI: − 3.37 - -3.37]), and family size (B -1.15 [95% CI: − 2.03 - -0.28]). The serum vitamin A level of visceral leishmaniasis patient was affected by residence (B 0.81 [95% CI: 0.08–1.54]), BMI (B 1.52 [95% CI: 0.42–2.6]), DDS (B 1.62 [95% CI: 0.36–2.88]), family size (B -5.03 [95% CI: − 5.83 - -4.22]), HIV (B -2.89 [95% CI: − 4.44 - -1.34]),MUAC (B 0.86 [95% CI: 0.52–1.21]), and age (B 0.09 [95% CI: 0.07–0.12]).
Conclusion
The micronutrient levels of visceral leishmaniasis patients were significantly lower. The anti-leishmaniasis treatment did not increase the serum micronutrient level of the patients.
Similar content being viewed by others
Background
Leishmaniasis is a group of vector born disease caused by the leishmania species. The three forms of leishmaniasis are cutaneous leishmaniasis, mucocutaneous leishmaniasis, and visceral leishmaniasis [1]. The severest form of the disease is visceral leishmaniasis and every year, it affects around 90, 000 people globally [2, 3]. It was reported from Bangladesh, Brazil, Ethiopia, India, South Sudan, and Sudan [4,5,6]. In the Amhara region, 5000 visceral leishmaniasis patients were reported annually [7, 8].
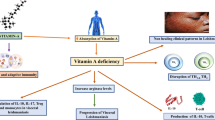
Micronutrients are minerals and vitamins that are required in a small amount, and they are essential for normal physiological activities. They serve as co-factors for many important metabolic enzymes. They enhance the function of the immune system and regulate gene transcription [9]. Disease conditions, especially inflammatory disease decrease the micronutrient levels [10]. Visceral leishmaniasis is among the disease condition that decrease the patient’s micronutrient level [11, 12]. The serum micronutrient concentration can be affected by chronic diseases, BMI, smoking, DDS (dietary diversification score), physical activity, intestinal parasites, MUAC (mid-upper arm circumference), HIV, and ethnicity [13,14,15,16,17,18,19,20,21,22,23,24,25,26].
The impacts of visceral leishmaniasis and micronutrient deficiency were not limited to the patients and their families; it also affects the socio-economic development of the nations [27,28,29]. Evidence on micronutrient level of visceral leishmaniasis patient was scarce and this research work conducted to answer the following objectives during visceral leishmaniasis treatment
-
Describe the progress of micronutrient levels during visceral leishmaniasis treatment.
-
Identify the determinants of micronutrient levels.
-
To assess the effects of micronutrient levels on the treatment outcome.
Methods
Study design
A prospective cohort study design was used.
Settings
The study was conducted among visceral leishmaniasis patients taking their treatment in the Amhara national regional state leishmaniasis treatment centers. The five leishmaniasis treatment centers of the region are Felegehiwote referral hospital, Gondar University hospital, Metema hospital, Addis Zemen health center, and Abderafi health center. From these treatment centers, more than 5000 incident visceral leishmaniasis patients was reported annually [7, 8]. The data were collected from August 2016–May 2019.
Participants
The target population for this study was adult visceral leishmaniasis patients receiving their treatment from the five treatment centers of the regional state. Visceral leishmaniasis patients fulfilling the world health organization case definition that means, a person with chronic fever, splenomegaly, and weight loss with parasitologically confirmed results were included. Visceral leishmaniasis patients with incomplete records were excluded from the study.
Variables
The stool sample was collected to adjust for hookworm, which significantly affects the serum iron level. From each visceral leishmaniasis patient, one gram stool sample was collected in 10 ml SAF (sodium acetate-acetic acid-formalin solution). To see the presence of intestinal parasitic infection using concentration technique [30]. The blood samples were collected at five repeated times in a month: before starting anti-leishmaniasis treatments, in the first week, in the second week, in the third week, and in the 4th week of anti-leishmaniasis treatments. At each spot, five-milliliter blood sample was collected from each visceral leishmaniasis patient following standard operating procedures to measure the serum zinc, iron, vitamin A, vitamin D, and selenium level. Urine samples were collected simultaneously with blood samples to measure their iodine levels. High-performance liquid chromatography was used to measure the serum vitamin A level of the patient [31], atomic absorption spectrophotometer was used to measure the serum zinc and selenium levels [32, 33], serum iron level was measured using Cobas 6000 (Roche kits German) instruments (Set 2015; analytics 2014), mini Vitek Immune Diagnostic Assay System (VIDAS) machine was used to measure the serum vitamin D level and urine iodine level was measured using the Sandell Kolthoff reaction. Vitamin A, Iron, and Zinc were measured using micrograms per deciliter (mcg/dl); Iodine was measured using micrograms per liter (mcg/l); Selenium and Vitamin D were measured using Nanograms per milliliter (ng/ml). Strict quality control measures were implemented during each laboratory procedure. CAGE tool was used to detect problematic alcohol use [34], Dietary diversification score (DDS) was measured using the world health organization (WHO) recommendations [35]. An International physical activity questionnaire (IPAQ) was used to measure regular physical activity [36]. Treatment success was declared if the patients become symptom-free and the absence of leishmania parasites in microscopy.
Data source
The data were collected using patient interview, measuring anthropometric indicators, collecting blood, urine, and stool samples. The interview and anthropometric indicators were collected by clinical nurses.
Bias
Probability sampling was used to select the study participants that decrease the selection bias. To decrease information bias: Training was given for data collectors and supervisors, the whole data collection procedures were closely supervised, data were cleaned and cheeked for errors before data entry.
Study size
The sample size was calculated using Epi-info software with the assumption of a 95% confidence interval, 90% power, HIV positive visceral leishmaniasis patients to HIV negative visceral leishmaniasis patients proportion of 1:2, risk ratio of 1.2 (HIV decreases the micronutrient level by 20%) and 15% loss to follow up rate; finally giving 465 HIV positive visceral leishmaniasis patients and 930 HIV negative visceral leishmaniasis patients. A systematic random sampling technique was used to select both HIV positive and HIV negative visceral leishmaniasis patients.
Quantitative variables
Quantitative variables were checked for the outlier. Their measures of central tendency and measure of dispersion were reported after checking the correct assumption.
Statistical methods
Data were entered into the computer using Epi-info software [37] and transported to SPSS for the analysis [38]. Descriptive statistics were used to describe the profile of patients and to compare the treatment success rate of visceral leishmaniasis patients. Generalized estimating equations (GEE, Autoregressive correlation matrix) were used to identify the determinants of serum micronutrients [39].
Ethical clearance was obtained from Bahir Dar University College of Medicine and Health Sciences ethical review committee. Permission was obtained from the Amhara national regional state health bureau and each treatment center. Written informed consent was obtained from each leishmaniasis patient before recruitment. Visceral leishmaniasis patients with abnormal laboratory findings were referred to the curative care segment of the hospital. The confidentiality of the data was kept at each level. Study participant’s right to withdraw from the research was respected at any point.
Results
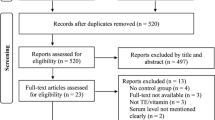
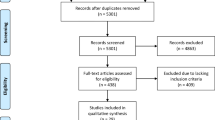
Totally, 1309 visceral leishmaniasis patients were followed, giving for a response rate of 94%; 32 patients did not volunteer to participate, the medical records of 31 VL (visceral leishmaniasis) patients were incomplete and 23 patients have died. Most of the study participants were included from Gondar university hospital (305), followed by Felegehiwote referral hospital (298), Metema hospital (268), Addis zemen health center (224), and Abderafi health center (214). The mean age of study participants was 32.88 years [SD ±15.95 years]. Male constitute 62.3% of study participants and problematic alcohol use was observed in 11.5% of the patients (Table 1).
Interpretations
Problematic alcohol use decreases the serum zinc level by 2.7 micrograms per deciliter (mcg/dl). Female kalazar patients had 1.28 mcg/dl less zinc level than males. High dietary diversification increases the serum zinc level by 9.75 mcg/dl. High family size decreases the serum zinc level by 1.63 mcg/dl. The serum zinc level of HIV positive visceral leishmaniasis patients was 2.95 mcg/dl less than HIV negative visceral leishmaniasis patients. The anti-leishmaniasis treatment did not increase the serum zinc level of the patients.
Problematic alcohol use increases the serum iron level of the patients by 7.6 mcg/dl. Chronic illness decreases the serum iron level of the patients by 7.44 mcg/dl. Malaria co-infection decreases the serum iron level of the patients by 12.69 mcg/dl. Hookworm infection decreases the serum iron level of visceral leishmaniasis patients by 4.48 mcg/dl. High family size decreases the serum iron level of the patients by 5.14 mcg/dl. HIV infection decreases the serum iron level of the patients by 5.54 mcg/dl. The serum iron level of patient increase by 0.11mcq/dl per a year increase in the patient age. The serum iron level of the patient increase by 0.75 mcq/dl per a centimeter increase in the MUAC of the patient. The anti-leishmaniasis treatment increases the serum iron level of the patient by 0.67 mcg/dl.
HIV positive visceral leishmaniasis patient had 18.1 ng/ml less serum selenium level than HIV negative visceral leishmaniasis patients. High family size decreases the serum selenium level of the patients by 11.36 ng/ml. The anti-leishmaniasis treatment increases the serum selenium level by 3.04 ng/ml.
Malaria decreases the iodine level of visceral leishmaniasis patients by 3.78 mcg/l. High DDS increases the iodine level of the patients by 25.84 mcg/l. Smoking decreases the iodine level of the patients by 12.34 mcg/l. HIV decreases the iodine level of visceral leishmaniasis patients by 38.02 mcg/l. Chronic illness decreases the iodine level of visceral leishmaniasis patients by 5.14 mcg/l. The anti-leishmaniasis treatment increases the iodine level of patients by 13.67 mcg/l.
Problematic alcohol use decreases the serum vitamin A level of visceral leishmaniasis patients by 1.09 mcg/dl. Chronic illness decreases the serum vitamin A level of the patients by 2.56 mcg/dl. Urban residence increases the serum vitamin A level of the patient by 0.81 mcq/dl. High DDS increases the serum vitamin A level of the patient by 1.62 mcg/dl. Malaria co-infection decreases the serum vitamin A level of the patient by 4.8 mcg/dl. High family size decreases the serum vitamin A level of visceral leishmaniasis patients by 5.03 mcg/dl. HIV infection decreases the serum vitamin A level of the patients by 2.89 mcg/dl. A centimeter increase in the MUAC of visceral leishmaniasis patients increases the serum vitamin A level by 0.86 mcg/dl. The anti-leishmaniasis treatment did not increase the serum vitamin A level of the patient.
A unit increase in the BMI of visceral leishmaniasis patients increases the serum vitamin D level by 1.52 ng/ml. High DDS increases the serum vitamin D level of the patients by 16.24 ng/ml. Malaria decreases the serum vitamin D level of the patients by 0.61 ng/ml. In the presence of hookworm infection, the serum vitamin D level of visceral leishmaniasis patients decreased by 3.94 ng/ml. High family size decreases the serum vitamin D level of the patients by 1.15 ng/ml. HIV co-infection decreases the serum vitamin D level of the patient by 9.43 ng/ml. The anti-leishmaniasis treatment did not increase the serum vitamin D level of visceral leishmaniasis patients (Table 2).
The micronutrient level directly affects treatment outcome of visceral leishmaniasis; especially the treatment outcome was not successful if the serum zinc, iron, vitamin A and vitamin D levels were lower than the first quartile. The overall treatment success rate of visceral leishmaniasis treatment was 84.7% [95% CI: 82.77 - 86.67%] (Tables 3, 4).
Discussion
Problematic alcohol use decreases the serum zinc level by 2.7 mcg/dl, and the serum vitamin A level by 1.09 mcg/dl. This finding was in line with previous research outputs [40, 41]. This is because alcohol interferes with the absorption and metabolism of zinc [42]. However, alcohol increases the serum iron level of visceral leishmaniasis patients by 7.6 mcg/dl. This is because alcohol increases the absorption of iron from the intestine [43].
A high dietary diversification score increases the serum zinc level of leishmaniasis patients by 9.75 mcg/dl, the iodine level by 25.84 mcg/l, the serum vitamin D level by 16.24 ng/ml, and the serum vitamin A level by 1.62 mcg/dl. This finding agrees with previous work [44]. This is because high dietary diversification score increases access to enough quality and quantity of micronutrients [45].
A high family size decreases the serum zinc level of the patients by 1.63 mcg/dl, the serum iron level by 5.14 mcg/dl, the serum zinc level by 11.36 ng/dl, the serum vitamin A level by 5.03 mcg/dl, the serum vitamin D level of the patients by 1.15 ng/ml. This finding was in line with previous researches work [41, 46, 47]. This is due to the sharing of the limited micronutrient-rich foods to the unbalanced household family members [48].
The serum zinc level of HIV positive visceral leishmaniasis patient was 2.95 mcg/dl less than HIV negative visceral leishmaniasis patients, HIV positive visceral leishmaniasis patients had 5.54 mcg/dl less serum iron level than HIV negative visceral leishmaniasis patients, HIV positive visceral leishmaniasis patient had 18.1 ng/dl less serum selenium level than HIV negative visceral leishmaniasis patients, HIV decreases the iodine level of visceral leishmaniasis patients by 38.02 mcg/l, the serum vitamin A level of visceral leishmaniasis patients by 2.89 mcg/dl, the serum vitamin D level by 9.43 ng/ml. This finding agrees with previous research findings [21, 49]. This is due to the reason that HIV infection reduced the intake of food and absorption and increased utilization and loss of micronutrients [50].
Chronic illness decreases the serum iron level of visceral leishmaniasis patients by 7.44 mcg/dl, the iodine level by 5.14 mcg/l, and the serum vitamin A level by 2.56 mcg/dl. This finding agrees with the 2019 published research work [51]. This is because the homeostasis of micronutrients, especially iron will be disturbed by chronic illnesses [52].
Malaria co-infection decreases the serum iron level of visceral leishmaniasis patients by 12.69 mcg/dl, the iodine level by 3.78 mcg/l, the serum vitamin A level by 4.8 mcg/dl and the serum vitamin D level by 0.61 ng/ml. This finding was in line with previously published works [53,54,55]. This is due to the ingestion of the nutrients by the parasites, decreases the intake from the host (anorexia), and increases the execration of the nutrients [56,57,58].
Hookworm infection decreases the serum iron level of visceral leishmaniasis patients by 4.48 mcg/dl; the serum vitamin D level by 3.94 ng/ml. This finding agrees with previous research outputs [59]. This is due to ingestion of nutrients by the parasites [60].
Per a year increase in the age of the patient, the serum iron level increases by 0.11 mcg/dl. This finding agrees with other’s scholars work [61]. This is due to the fact that serum iron decreasing factors like chronic diseases and other unhealthy lifestyles were prevalent in the older age [62].
Per a centimeter increase in the MUAC of the patient, the serum iron level increases by 0.75 mcg/dl and the serum vitamin A level by 0.86 mcg/dl. This finding was in line with previously published work [63]. This is due to the reason that, higher MUAC groups have good nutritional support [64].
Smoking decreases the iodine level of visceral leishmaniasis patients by 12.34 mcg/l. This finding agrees with previous scholar’s work [65]. This is due to the effect of smoking in disturbing the iodine metabolism [66, 67].
Leishmaniasis patients in the urban area had 0.81 mcg/dl higher serum vitamin A level than the rural patients. This finding agrees with finding from Nepal [68]. This is because of the higher awareness of the urban population about vitamin A [69].
A unit increase in the BMI of visceral leishmaniasis patients increases the serum vitamin D level by 1.52 ng/ml. This finding disagrees with finding from Norway [70]. This might be due to the cultural difference between the two populations.
The serum zinc level of females was 1.28 mcg/dl less than male. This finding agrees with previous literature [71]. This is because women lose their serum zinc level during their pregnancy and menstruation [72].
The anti-leishmaniasis treatment did not increase the serum zinc, vitamin A, vitamin D, or iron level of the patients. It increases the serum selenium level by 3.04 ng/ml and the iodine level by 13.67 mcg/l.
The overall treatment success rate of visceral leishmaniasis treatment was 84.7% [95% CI: 82.77 - 86.67%]. A systematic review and meta-analysis estimate also supports this finding [73].
Low serum zinc level decreases the treatment outcome of visceral leishmaniasis. This finding was in line with finding from India [12]. This is due to the effects of zinc in the immune system of the patients [74].
Higher patient iron level increases the treatment success rate of visceral leishmaniasis. This finding supports the results of previously published work [75]. This is due to the crucial role of iron in red blood cell production that is used to transport essential substances, including the anti-leishmaniasis drugs [76].
Higher serum vitamin A and Vitamin D level favors good treatment outcome in visceral leishmaniasis. This finding agrees with previous researchers outputs [77,78,79]. This indicates that administering the anti-leishmaniasis treatment alone will not yield a favorable treatment outcome in visceral leishmaniasis patients.
Possible limitation of this study was a failure to address all the vitamins and minerals status of visceral leishmaniasis patients, but since practically it is very difficult to address all of them this study gives the baseline evidence on main vitamins and mineral levels.
Conclusion
The serum micronutrient levels of visceral leishmaniasis patients were low. Problematic alcohol use affects the serum zinc, iron, vitamin A levels. DDS affects the serum zinc, iodine, vitamin A, and vitamin D level. Family size affects the serum zinc, iron, selenium, vitamin A, and vitamin D levels. HIV infection affects the serum zinc, iron, selenium, iodine, vitamin A, and vitamin D levels. Anti-leishmaniasis drug slightly increases the serum iodine and selenium levels, but it doesn’t increase the serum iron, zinc, vitamin A, and vitamin D levels. The serum levels of zinc, iron, vitamin A, and vitamin D significantly affect the treatment outcomes of visceral leishmaniasis.
Recommendation
The visceral leishmaniasis treatment guideline should incorporate supplementing the micronutrients as part of anti-leishmaniasis intervention.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- B:
-
Beta coefficient
- BMI:
-
Body mass index
- CI:
-
Confidence interval
- DDS:
-
Dietary diversification score
- GEE:
-
Generalized estimating eqs.
- HIV:
-
Human immune deficiency virus
- MCG/DL:
-
Micrograms per deciliter
- Mg/dl:
-
Milligram per deciliter
- MUAC:
-
Mid upper arm circumference
- Ng/dl:
-
Nanogram per deciliter
- SD:
-
Standard deviation
- VL:
-
Visceral leishmaniasis
- WHO:
-
World health organization
References
Torres-Guerrero E, Quintanilla-Cedillo MR, Ruiz-Esmenjaud J, Arenas R. Leishmaniasis: a review. F1000Res. 2017;6.
WHO: Key facts on leishmaniasis. In: WHO, editor. Leishmanisis fact sheets, vol. 1. Geneva: World health organization; 2019..
Kolaczinski JH, Hope A, Ruiz JA, Rumunu J, Richer M, Seaman J. Kala-azar epidemiology and control, southern Sudan. Emerg Infect Dis. 2008;14(4):664–6..
Thakur CP. Is elimination of kala-azar feasible by 2017? Indian J Med Res. 2016;144(6):799–802.
Nampoothiri RV, Sreedharanunni S, Chhabria BA, Jain S. Visceral Leishmaniasis: Kala-azar. QJM. 2016;109(5):347–8.
Sunyoto T, Adam GK, Atia AM, Hamid Y, Babiker RA, Abdelrahman N, Vander Kelen C, Ritmeijer K, Alcoba G, den Boer M, et al. "Kala-Azar is a dishonest disease": community perspectives on access barriers to visceral Leishmaniasis (Kala-Azar) diagnosis and Care in Southern Gadarif, Sudan. Am J Trop Med hyg. 2018;98(4):1091–101.
FDREMH. visceral Lithuanians diagnosis and treatment guideline for health workers in Ethiopia. Addis Ababa: disease prevention and controle departement; 2006. p. 1–35.
Deribe K, Meribo K, Gebre T, Hailu A, Ali A, Aseffa A, Davey G. The burden of neglected tropical diseases in Ethiopia, and opportunities for integrated control and elimination. Parasit Vectors. 2012;5:240.
Shenkin A. Micronutrients in health and disease. Postgrad Med J. 2006;82(971):559–67.
Dao DT, Anez-Bustillos L, Cho BS, Li Z, Puder M, Gura KM. Assessment of micronutrient status in critically ill children: challenges and opportunities. Nutrients. 2017;9(11):1185.
Paul UK, Chakraborty PK, Hoque MR, Jafrin W, Sarkar S, Akhter S, Roy AS. Serum iron status among visceral leishmaniasis patients. Mymensingh Med J. 2014;23(4):654–7.
Lal CS, Kumar S, Ranjan A, Rabidas VN, Verma N, Pandey K, Verma RB, Das S, Singh D, Das P. Comparative analysis of serum zinc, copper, magnesium, calcium and iron level in acute and chronic patients of visceral leishmaniasis. J Trace Elem Med Biol. 2013;27(2):98–102.
Li J, Wu N, Li Y, Ye K, He M, Hu R. Cross-sectional analysis of serum calcium levels for associations with left ventricular hypertrophy in normocalcemia individuals with type 2 diabetes. Cardiovasc Diabetol. 2015;14:43.
Pirpamer L, Hofer E, Gesierich B, De Guio F, Freudenberger P, Seiler S, Duering M, Jouvent E, Duchesnay E, Dichgans M, et al. Determinants of iron accumulation in the normal aging brain. Neurobiol Aging. 2016;43:149–55.
Ryan JD, Armitage AE, Cobbold JF, Banerjee R, Borsani O, Dongiovanni P, Neubauer S, Morovat R, Wang LM, Pasricha SR, et al. Hepatic iron is the major determinant of serum ferritin in NAFLD patients. Liver Int. 2018;38(1):164–73.
Filippini T, Michalke B, Grill P, Malagoli C, Malavolti M, Vescovi L, Sieri S, Krogh V, Cherubini A, Maffeis G, et al. Determinants of serum manganese levels in an Italian population. Mol Med Rep. 2017;15(5):3340–9.
Bener A, Khattab AO, Bhugra D, Hoffmann GF. Iron and vitamin D levels among autism spectrum disorders children. Ann Afr Med. 2017;16(4):186–91.
Thomas D, Chandra J, Sharma S, Jain A, Pemde HK. Determinants of nutritional Anemia in adolescents. Indian Pediatr. 2015;52(10):867–9.
McNally JD, Menon K, Chakraborty P, Fisher L, Williams KA, Al-Dirbashi OY, Doherty DR. The association of vitamin D status with pediatric critical illness. Pediatrics. 2012;130(3):429–36.
Chen J, Peng H, Zhang K, Xiao L, Yuan Z, Chen J, Wang Z, Wang J, Huang H. The insufficiency intake of dietary micronutrients associated with malnutrition-inflammation score in hemodialysis population. PLoS One. 2013;8(6):e66841.
Anyabolu HC, Adejuyigbe EA, Adeodu OO. Serum Micronutrient Status of Haart-Naïve, HIV Infected Children in South Western Nigeria: A Case Controlled Study. AIDS Res Treat. 2014;2014:8.
Alberg AJ, Chen JC, Zhao H, Hoffman SC, Comstock GW, Helzlsouer KJ. Household exposure to passive cigarette smoking and serum micronutrient concentrations. Am J Clin Nutr. 2000;72(6):1576–82.
Kant AK, Graubard BI. Ethnicity is an independent correlate of biomarkers of micronutrient intake and status in American adults. J Nutr. 2007;137(11):2456–63.
Foo LH, Khor GL, Tee ES, Dhanaraj P. Determinants of iron status in Malaysian adolescents from a rural community. Int J Food Sci Nutr. 2004;55(6):517–25.
Goodman GE, Thornquist M, Kestin M, Metch B, Anderson G, Omenn GS. The association between participant characteristics and serum concentrations of beta-carotene, retinol, retinyl palmitate, and alpha-tocopherol among participants in the Carotene and Retinol Efficacy Trial (CARET) for prevention of lung cancer. Cancer Epidemiol Biomark Prev. 1996;5(10):815.
Kimmons JE, Blanck HM, Tohill BC, Zhang J, Khan LK. Associations between body mass index and the prevalence of low micronutrient levels among US adults. MedGenMed. 2006;8(4):59.
Beard J. Recent evidence from human and animal studies regarding iron status and infant development. J Nutr. 2007;137(2):524s–30s.
Marx JJ. Iron and infection: competition between host and microbes for a precious element. Best Pract Res Clin Haematol. 2002;15(2):411–26.
Bailey RL, West KP Jr, Black RE. The Epidemiology of Global Micronutrient Deficiencies. Ann Nutr Metab. 2015;66(Suppl. 2):22–33.
Institute S: Methods in Parasitology. Sodium acetate-acetic acid-formalin solution method for stool specimen. Basel: Swiss TPH: Swiss Tropical Institute; 2005. p. 1–18.
Catignani G, Bieri J. Simultaneous determination of retinol and alpha-tocopherol in serum or plasma by liquid chromatography. Clin Chem. 1983;29(4):708–12.
Smith J, Butrimovitz G, Purdy W. Direct measurement of zinc in plasma by atomic absorption spectroscopy. Clin Chem. 1979;25(8):1487–91.
Lewis S, Hardison N, Veillon C. Comparison of isotope dilution mass spectrometry and graphite furnace atomic absorption spectrometry with Zeeman background correction for the determination of plasma selenium. Anal Chem. 1986;58(6):1272–3.
Bush B, Shaw S, Cleary P, Delbanco TL, Aronson MD. Screening for alcohol abuse using the CAGE questionnaire. Am J Med. 1987;82(2):231–5.
Swindale A, Bilinsky P. Food and Nutrition Technical Assistance (FANTA). Household dietary diversity score (HDDS) for measurement of household food access: indicator guide. Version 2; 2006.
Sjostrom M, Ainsworth B, Bauman A, Bull F, Hamilton-Craig C, Sallis J. Guidelines for data processing analysis of the international physical activity questionnaire (IPAQ)-short and long forms; 2005.
Dean AG. Epi info and Epi map: current status and plans for Epi info 2000. J Public Health Manage Pract. 1999;5(4):54–7.
SPSS. IBM SPSS statistics for windows, version 25. Armonk, NY: Corp IS; 2017.
Hardin JW. Generalized estimating equations (GEE). Encyclopedia of statistics in behavioral science; 2005.
Gloria L, Cravo M, Camilo M, Resende M, Cardoso JN, Oliveira AG, Leitão CN, Mira FC. Nutritional deficiencies in chronic alcoholics: relation to dietary intake and alcohol consumption. Am J Gastroenterol. 1997;92(3).
Feleke BE, Feleke TE, Mekonnen D, Beyene MB. Micronutrient levels of tuberculosis patients during the intensive phase, a prospective cohort study. Clin Nutr ESPEN. 2019;31:56–60.
Livingstone C. Zinc: physiology, deficiency, and parenteral nutrition. Nutr Clin Pract. 2015;30(3):371–82.
DUANE P, RAJA KB, SIMPSON RJ, PETERS TJ. INTESTINAL IRON ABSORPTION IN CHRONIC ALCOHOLICS. Alcohol Alcohol. 1992;27(5):539–44.
Yeneabat T, Adugna H, Asmamaw T, Wubetu M, Admas M, Hailu G, Bedaso A, Amare T. Maternal dietary diversity and micronutrient adequacy during pregnancy and related factors in east Gojjam zone, Northwest Ethiopia, 2016. BMC Pregnancy Childbirth. 2019;19(1):173.
Nair MK, Augustine LF, Konapur A. Food-based interventions to modify diet quality and diversity to address multiple micronutrient deficiency. Front Public Health. 2016;3:277.
Feleke BE. Nutritional status and intestinal parasite in school age children: a comparative cross-sectional study. Int J Pediatr. 2016;2016:1962128.
Batool F, Kausar S, Khan S, Ghani M, Margrate M. NUTRITIONAL STATUS. Prof Med J. 2019;26(03).
Lamidi EO. Household composition and experiences of food insecurity in Nigeria: the role of social capital, education, and time use. Food Security. 2019:1–18.
Feleke BE. Maternal HIV status affects the infant hemoglobin level: a comparative cross-sectional study. Medicine (Baltimore). 2016;95(31):e4372.
Graham VA. Effects of micronutrients on the status of HIV-infected African American women; 2018.
Means RT. The Anemia of Inflammation/Chronic Disease and the Unexplained Anemia of the Elderly. In: Anemia in the Young and Old: Springer; 2019. p. 157–66.
Osterholm EA, Georgieff MK. Chronic inflammation and iron metabolism. J Pediatr. 2015;166(6):1351–1357.e1351.
White NJ. Anaemia and malaria. Malar J. 2018;17(1):371.
Bivona G, Agnello L, Lo Sasso B, Scazzone C, Butera D, Gambino CM, Iacolino G, Bellia C, Ciaccio M. Vitamin D in malaria: more hypotheses than clues. Heliyon. 2019;5(2):e01183.
Bendabenda J, Patson N, Hallamaa L, Mbotwa J, Mangani C, Phuka J, Prado EL, Cheung YB, Ashorn U, Dewey KG, et al. The association of malaria morbidity with linear growth, hemoglobin, iron status, and development in young Malawian children: a prospective cohort study. BMC Pediatr. 2018;18(1):396.
Elsworth B, Keroack CD, Duraisingh MT. Elucidating host cell uptake by malaria parasites. Trends Parasitol. 2019;35(5):333–5.
Vidyullatha A, Reddy VS, Madhulika CL. A study of clinical profile of malaria and its acute complications caused by different species of plasmodium in children. J Evol Med Dent Sci. 2019;8(9):604–10.
Ahamed AM, Hobiel HA, Modawe GA, Elsammani MS. Hematological changes in Sudanese patients with falciparum malaria attending Elnihoud teaching hospital. Sudan J Med Sci (SJMS). 2019:24–30.
Elfu Feleke B. Epidemiology of hookworm infection in the school-age children: a comparative cross-sectional study. Iran J Parasitol. 2018;13(4):560–6.
Clark TN, Gilman RH. Hookworm and Strongyloides Infections. In: Hunter's Tropical Medicine and Emerging Infectious Diseases: Elsevier; 2020. p. 845–50.
Lee EA, Shin DW, Yoo JH, Ko HY, Jeong SM. Anemia and Risk of Fractures in Older Korean Adults: A Nationwide Population-Based Study. J Bone Miner Res. 2019:e3675.
Flynn MG, Markofski MM, Carrillo AE. Elevated inflammatory status and increased risk of chronic disease in chronological aging: Inflamm-aging or Inflamm-inactivity? Aging Dis. 2019;10(1):147.
Feleke BE, Feleke TE. Pregnant mothers are more anemic than lactating mothers, a comparative cross-sectional study, Bahir Dar, Ethiopia. BMC Hematol. 2018;18:2–2.
Briend A, Mwangome MK, Berkley JA. Using mid-upper arm circumference to detect high-risk malnourished patients in need of treatment. In: Handbook of Famine, Starvation, and Nutrient Deprivation: From Biology to Policy; 2019. p. 705–21.
Wang D, Yu S, Yin Y, Xie S, Cheng Q, Li H, Cheng X, Qiu L. Iodine status of euthyroid adults: A cross-sectional, multicenter study. J Clin Lab Anal. 2019:e22837.
S-j K, Kim MJ, Yoon SG, Myong JP, Yu HW, Chai YJ, Choi JY, Lee KE. Impact of smoking on thyroid gland: dose-related effect of urinary cotinine levels on thyroid function and thyroid autoimmunity. Sci Rep. 2019;9(1):4213.
Jia M, Shi X, Gu X, Guan H, Teng X, Teng D, Fan C, Li Y, Shan Z, Teng W. Smoking is positively associated with Antithyroperoxidase antibodies and Antithyroglobulin antibodies in populations with mildly deficient iodine intake. Biol Trace Elem Res. 2019;187(2):383–91.
Katz J, Khatry SK, West KP, Humphrey JH, Leclerq SC, Pradhan EK, Pohkrel R, Sommer A. Night blindness is prevalent during pregnancy and lactation in rural Nepal. J Nutr. 1995;125(8):2122–7.
Beletew B. knowledge, attitude and practice on key essential nutrition action messages and associated factors among mothers of children birth-24 month in Wereilu wereda, South Wollo Zone, Amhara, Northeast Ethiopia, 2018: Addis Ababa Universty; 2018.
Konradsen S, Ag H, Lindberg F, Hexeberg S, Jorde R. Serum 1, 25-dihydroxy vitamin D is inversely associated with body mass index. Eur J Nutr. 2008;47(2):87–91.
Kandhro GA, Kazi TG, Afridi HI, Kazi N, Baig JA, Arain MB, Shah AQ, Sarfraz RA, Jamali MK, Syed N. Effect of zinc supplementation on the zinc level in serum and urine and their relation to thyroid hormone profile in male and female goitrous patients. Clin Nutr. 2009;28(2):162–8.
Swanson CA, King JC. Zinc utilization in pregnant and nonpregnant women fed controlled diets providing the zinc RDA. J Nutr. 1982;112(4):697–707.
Gebreyohannes EA, Bhagvathula AS, Abegaz TM, Seid MA. Treatment outcomes of visceral leishmaniasis in Ethiopia from 2001 to 2017: a systematic review and meta-analysis. Infect Dis Poverty. 2018;7(1):108.
Van Weyenbergh J, Santana G, D'Oliveira A, Santos AF, Costa CH, Carvalho EM, Barral A, Barral-Netto M. Zinc/copper imbalance reflects immune dysfunction in human leishmaniasis: an ex vivo and in vitro study. BMC Infect Dis. 2004;4(1):50.
Singh B, Singh SS, Sundar S. Hepcidin mediated iron homoeostasis as immune regulator in visceral leishmaniasis patients. Parasite Immunol. 2019;41(1):e12601.
Bogdanova A, Kaestner L, Simionato G, Wickrema A, Makhro A. Heterogeneity of red blood cells: causes and consequences. Front Physiol. 2020;11.
Whitcomb JP, DeAgostino M, Ballentine M, Fu J, Tenniswood M, Welsh J, Cantorna M, McDowell MA. The role of vitamin D and vitamin D receptor in immunity to <i>Leishmania major</i> infection. J Parasitol Res. 2012;2012:134645.
Lima Maciel BL, Valverde JG, Rodrigues-Neto JF, Freire-Neto F, Keesen TSL, Jeronimo SMB. Dual immune modulatory effect of vitamin a in human visceral Leishmaniasis. PLoS One. 2014;9(9):e107564.
Mashayekhi Goyonlo V, Norouzy A, Nemati M, Layegh P, Akhlaghi S, Taheri AR, Kiafar B. Nutritional intake and chronicity associated with the Old World cutaneous Leishmaniasis: role of vitamin a. Iran J Public Health. 2020;49(1):167–72.
Acknowledgments
Our heartfelt appreciation goes to Amhara national regional state health bureau for their unreserved effort during the fieldwork. Our acknowledgment also extends to all organizations and individuals that had inputs for this research work.
Funding
This research work was financially supported by federal democratic republic of Ethiopia ministry of health and Bahir Dar University. The funder has no role in design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
BEF conceived the experiment; BEF and TEF performed the experiment, plan the data collection process, analyzed and interpreted the data. BEF and TEF wrote the manuscript and approved the final draft for publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical clearance was obtained from Bahir Dar University College of medicine and health sciences ethical review committee. Permission was obtained from the Amhara national regional state health bureau and each treatment center. Written informed consent was obtained from each leishmaniasis patient before recruitment. Visceral leishmaniasis patients with abnormal laboratory findings were referred to the curative care segment of the hospital. The confidentiality of the data was kept at each level. Study participant right to withdraw from the research was respected at any point.
Consent for publication
Not applicable.
Competing interests
The authors declares that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Feleke, B.E., Feleke, T.E. Micronutrient levels and their effects on the prognosis of visceral leishmaniasis treatment, a prospective cohort study. BMC Infect Dis 20, 867 (2020). https://doi.org/10.1186/s12879-020-05615-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-020-05615-1