
Abstract
Background
Exposure to indoor air pollution from solid cooking fuel use may increase mental disorders risk through pathways such as oroxidative stress, neuroinflammation, or cerebrovascular damage. However, few studies have explored the underlying mechanism between solid cooking fuel use and psychological distress. The present study aims to investigate the mediating role of sleep quality on the relationship between solid cooking fuel use and psychological distress among older adults in rural Shandong, China.
Methods
This study used the cross-sectional data from the second follow-up survey of the Shandong Rural Elderly Health Cohort (SREHC). A total of 3,240 rural older adults were included in the analysis. Logistic regression and the Karlson, Holm, and Breen (KHB) mediation analyses were performed to investigate the relationship between solid cooking fuel use and psychological distress, as well as the mediating role of sleep quality in this association.
Results
This study found that solid cooking fuel use was significantly and positively associated with psychological distress among older adults in rural Shandong, China (OR = 1.38, 95% CI: 1.12,1.70). Mediation analysis revealed that sleep quality mediated the association between solid cooking fuel use and psychological distress among older adults (β = 0.06, P = 0.011). The mediation effect accounted for 16.18% of the total effect.
Conclusions
Our study showed that solid cooking fuel use was associated with psychological distress among rural older adults, and sleep quality mediated this association. Interventions should focus on addressing cooking fuel types and poor sleep quality to reduce psychological distress. In the future, more aggressive environmental protection policies would be needed to lessen the adverse effects of indoor air pollution on the health of older adults in rural China.
Similar content being viewed by others

Introduction
Globally, psychological distress is a major public health issue. Psychological distress is defined as a state of emotional suffering, characterized by depression and anxiety symptoms [1]. The risk of psychological distress has increased dramatically as people get older. More than one-third of Chinese older adults are at high risk of severe psychological distress symptoms [2]. Previous studies found that older adults with psychological distress have a higher risk of cognitive impairment, functional decline, poor quality of life, and mortality [3, 4]. Furthermore, the prevalence of psychological distress among rural older adults in China is significantly higher than in urban areas [5]. Preventing psychological distress among rural older adults has become a public health priority. Exploring risk factors and interventions for psychological distress is crucial to improving the mental health of rural older adults, preventing adverse health outcomes, and achieving healthy aging.
Indoor air pollution from solid cooking fuel use has captured extensive attention due to its serious threat to human health, which is particularly pressing in developing countries [6]. China has been facing significant health threats caused by indoor cooking fuel pollution, especially in rural areas [7]. Solid cooking fuel use emits significant amounts of hazardous pollutants into the environment, increasing the burden of disease and mortality [7]. Emerging literature has provided conclusive evidence for the relationship between solid cooking fuel use and mental health among older adults [8,9,10]. Solid fuels burning generates substantially higher levels of various gaseous pollutants than clean fuel, including particulate matter (PM), nitric oxide (NO), nitrogen dioxide (NO2), and carbon monoxide (CO) [11, 12]. Exposure to indoor air pollution from solid cooking fuel use may increase mental disorders risk like depression through pathways such as cerebrovascular damage, oxidative stress, neurodegeneration, or neuroinflammation [10, 11, 13, 14]. Moreover, several toxicological studies are confirming that particulate matter emitted from solid fuels enters the central nervous system through the alveolar epithelium, triggering inflammation and accelerating the progression of depression symptoms [15, 16]. Therefore, it may be hypothesized that there is an association between solid cooking fuel use and psychological distress, and that the underlying mechanism of this relationship remains unclear.
Sleep quality is an essential indicator of health and well-being among older adults [17]. Growing evidence has shown that poor sleep quality is linked to an increased risk of psychological distress among rural older adults in China [18, 19]. Other studies also observed an association between indoor air pollution from solid cooking fuel use and poor sleep quality among older adults [20,21,22]. Indoor air pollutants from solid cooking fuels may cause systemic inflammation through the respiratory tract or central nervous system. Excessive inflammation may lead to changes in the expression of genes that have protein products involved in the production and regulation of circadian rhythms (e.g., clock genes), resulting in reduced sleep quality [22]. Besides, previous studies have found that sleep quality plays a mediating role in the relationship between physical disorders and psychological distress [2, 19]. A recent research of rural older adults in China showed that the relationship between chronic conditions and psychological distress was mediated by sleep quality [2]. The use of solid cooking fuels increases the risk of various chronic diseases in older people, particularly chronic obstructive pulmonary disease and cardiovascular disease, which may reduce sleep quality [23]. Poor sleep quality impairs carbohydrate metabolism and endocrine function, activating inflammatory processes [24], and directly increases the risk of mental disorders such as psychological distress. Thus, sleep quality may act as a mediator between solid cooking fuel use and psychological distress.
Based on the abovementioned empirical research, this study aims at investigating the relationship between solid cooking fuel use and psychological distress, as well as the mediating role of sleep quality in this association among older adults in rural China. We proposed the following hypotheses: (1) older adults with solid cooking fuel use have a higher risk of psychological distress in rural Shandong, China; and (2) sleep quality is a mediator between solid cooking fuel use and psychological distress among rural older adults. The proposed mediation model in this study is depicted in Fig. 1.

Framework of mediation analysis
Methods
Data source and participants
This study used the cross-sectional data from the second follow-up survey of the Shandong Rural Elderly Health Cohort (SREHC), which was performed in Shandong Province from July to August 2022, including 3468 respondents aged 60 years and older. SREHC is an ongoing longitudinal study of the behavior and health of older adults in rural Shandong, China [25]. Shandong, located in eastern China, has the largest older population in China, with 20.9% of the population aged 60 and older in 2020 [26]. We used a multi-stage stratified cluster sampling method to select participants. First, the counties in Shandong Province were divided into three groups based on GDP per capita in 2018, and each group randomly selected one county as a sample county [27]. Three counties (Rushan, Qufu, and Laolin) were selected as the study sites, representing high, medium, and low economic levels, respectively. Second, five sample townships were randomly selected from each sampled county. Finally, four sample villages were randomly selected from each sample township. Older adults aged 60 years or older who were randomly selected from each sample village as survey respondents.
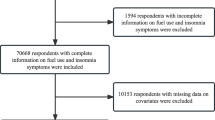
To assure quality, all respondents were interviewed face-to-face by trained interviewers using structured questionnaires. Inclusion criteria were (1) permanent residents aged 60 years and older who lived in the village for more than six months in the past year, and (2) clearly informed and voluntary participants who were able to complete the interview tasks independently. Exclusion criteria were (1) participants who were unwilling to cooperate with the interviewer, (2) participants with diagnosed mental or psychiatric illnesses (e.g., dementia, etc.) who were unable to answer independently. Moreover, to obtain complete and accurate data, we excluded missing data for the main variables. Finally, 3,240 older adults were included in this study. Figure S1 shows a flowchart of this study sample.
Measures
Psychological distress
The Chinese version of the Kessler 10 (K10) scale was employed to assess the psychological distress of older adults. The K10 was a commonly used tool for assessing mental health among older adults in China, which has been confirmed to have high reliability and validity [28]. The scale assessed the psychological distress of the respondents over the past 30 days, including depression, anxiety, tension, despair, restlessness, and worthlessness. The K10 scale contained 10 items, each of which was scored from 1 to 5, representing none of the time, occasionally, some of the time, most of the time, and all of the time. The total score ranged from 10 to 50 points, with higher scores indicating higher levels of psychological distress. Based on previous research, a threshold of 21 points was established in this study [29], and individuals who scored above 21 points were classified as groups with psychological distress. In this study, the scale was tested to have good reliability and validity (Cronbach’s α = 0.908, KMO value = 0.921).
Solid cooking fuel use
This study collected information on cooking fuel types by asking: “What kind of fuel does your household use primarily?” Participants’ primary choices for cooking fuels, which included coal, wood or straw, natural gas, liquefied gas, and electricity, were asked. Cooking fuel types were categorized as clean fuel (including electricity, natural gas, and liquefied gas) and solid fuel (including coal, wood/straw, or other) based on the definition of previous studies [7]. When mixed fuels were used for cooking, they were classified according to the primary fuel.
Sleep quality
The Pittsburgh Sleep Quality Index (PSQI), a Chinese version with high reliability and validity, was used to measure the sleep quality of older adults in the past 30 days [30]. This scale was the most widely used self-assessment questionnaire for assessing individuals’ sleep quality [31]. The PSQI scale consisted of 19 items, divided into seven dimensions: subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. Each dimension was scored from 0 to 3. The total PSQI score ranged from 0 to 21, with higher scores indicating poorer sleep quality among study participants [32]. In this study, the scale was tested to have good reliability and validity (Cronbach’s α = 0.756, KMO value = 0.806).
Covariates
Potential confounders for this study included sociodemographic characteristics, health behaviors, and physical health status. (1) Sociodemographic characteristics: self-made demographic questionnaires were used, which included age (years), gender (men, women), marital status [single (unmarried, divorced, widowed), married], highest level of education (illiterate, primary school, and middle school or above), residence status (live alone, non-living alone), and annual household income (four types based on percentiles, with Q1 being the poorest and Q4 being the richest, the mean were 7166.92, 14895.70, 28560.80, and 81132.70 yuan, respectively). (2) Health behaviors: including smoking (yes, no), drinking (yes, no), frequency of drinking tea (rarely or never, occasionally, and almost every day), physical activity (four types based on percentiles, with Q1 being the lowest and Q4 being the highest), and kitchen ventilation (yes, no). Physical activity was measured using the International Physical Activity Questionnaire Short Form (IPAQ-S). The scale included seven questions that synthesized three types of physical activity: walking, moderate-intensity, and high-intensity [33]. Different intensities of physical activity correspond to different Metabolism Equivalent (MET), and the respondents’ physical activity over the past seven days was assessed by combining the corresponding MET values of physical activity × weekly frequency (in days) × daily activity time (in minutes) [33]. The total physical activity level was calculated by summing the three intensities of physical activity. Kitchen ventilation included open windows, a chimney, an exhaust hood, and partial openings. (3) Physical health status: including chronic health conditions and functional limitations. There were three categories of chronic health conditions: no chronic condition, one chronic condition, and multimorbidity. The Activities of Daily Living (ADL) Scale was used to assess the functional limitations of older adults. The scale had 14 items with a score range from 14 to 56 points, with higher scores indicating worse activities of daily living [34]. In this study, the ADL scale was tested to have good reliability and validity (Cronbach’s α = 0.836, KMO value = 0.919).
Statistical analyses
All data were statistically analyzed using Stata 17.0 (Stata Corp, College Station, TX, USA) and SPSS 25.0 (IBM Corp, Armonk, NY, USA). First, all variables were performed with descriptive analyses. To examine the group differences, chi-square tests (for categorical variables) and t-tests (for continuous variables) were used. Second, the Harman one-way test was used to test the data for common method bias. Third, binary logistic regression was employed to investigate the relationship between solid cooking fuel use and psychological distress among older adults. Model 1 was unadjusted; Model 2 was a fully adjusted model controlling for age, gender, education, marriage status, residence status, household income, smoking, drinking, frequency of drinking tea, physical activity, kitchen ventilation, sleep quality, chronic health conditions, and activities of daily living; and Model 3 was performed using the LR stepwise forward method. Finally, the Karlson, Holm, and Breen (KHB) method, which was the most widely used in testing mediation effects in nonlinear probability models, was employed to estimate direct and indirect effects [35]. Given that the dependent variable in this study, psychological distress, was a dichotomous variable, a logit model of the KHB method was employed to evaluate the potential mediation effect of sleep quality on the association between solid cooking fuel use and psychological distress [36]. Furthermore, the mediation pathway model diagram with coefficients was used to visualize the mediating role of sleep quality in the relationship between solid cooking fuel use and psychological distress. The reported confidence intervals (CIs) were calculated to the 95% level. All tests were two-sided, and a P-value < 0.05 was considered statistically significant.
Results
Characteristics of participants
Table 1 presents the characteristics of the participants according to psychological distress. Of the 3,240 respondents, with a mean age of 72.43 years (SD = 5.91), 60.00% were female, 38.49% were illiterate, and 77.10% were married. The prevalence of psychological distress was 17.81%. Compared with participants without psychological distress, those who did were more likely to be female (P < 0.001), married (P < 0.001), had less education (P < 0.001), live alone (P = 0.007), had lower household income (P = 0.006), rarely or never drinking tea (P < 0.001), and had a lower level of physical activity (P < 0.001). Furthermore, there was a significant difference in solid cooking fuel use between respondents with and without psychological distress (t = 7.36, P = 0.007). Regarding sleep quality, those with psychological distress had worse sleep quality (t = -19.04, P < 0.001).
Common method bias analysis
Common method bias is prevalent in questionnaire studies [37]. In this study, the Harman one-way test was used to determine whether the data were affected by common method bias. The results of the study showed that the explained variance of the unrotated first factor was 17.75% (less than 40%), which indicates that there is no problem of common method bias in this study [37].
Associations between solid cooking fuel use and psychological distress
As shown in Table 2, a positive correlation was observed between solid cooking fuel use and psychological distress in the binary logistic regression models. In the unadjusted model (model 1), participants who primarily used solid fuels for cooking had a higher risk of psychological distress (OR = 1.24, 95% CI: 1.02, 1.51). The results in both the full adjusted (model 2) and adjusted using the LR stepwise forward method (model 3) models were consistent with model 1. Compared with clean cooking fuel users, the higher risk of psychological distress still significantly existed among solid cooking fuel users (Model 2: OR = 1.37, 95% CI: 1.11,1.69; Model 3: OR = 1.38, 95% CI: 1.12,1.70).
Mediating effect analyses
Table 3 shows the mediating effect of sleep quality on the relationship between solid cooking fuel use and psychological distress. After controlling for potential covariates using the LR stepwise forward method, KHB mediation analysis revealed that solid cooking fuel use was significantly associated with an elevated risk of psychological distress among older adults, mediated by sleep quality. The total effect (β = 0.38, P < 0.001), direct effect (β = 0.33, P = 0.002), and indirect effect (β = 0.06, P = 0.011) of solid cooking fuel use on psychological distress mediated by sleep quality were statistically significant. Sleep quality accounted for 16.18% of the total effect of solid cooking fuel use on psychological distress. The mediation pathway model with coefficients for solid cooking fuel use, sleep quality, and psychological distress is illustrated in Fig. 2.

Path diagram of the association between solid cooking fuel use and psychological distress with sleep quality as a mediator. Notes: ** p < 0.05, *** p < 0.001. 95% CIs in the parentheses are shown. Models control for age, gender, education, marriage status and household income, smoking, drinking, kitchen ventilation, chronic health conditions, and activities of daily living
Discussion
To our knowledge, this is the first study to investigate the mediating role of sleep quality in the relationship between solid cooking fuel use and psychological distress among older adults in rural Shandong, China. Our findings revealed that older people who use solid cooking fuels have a higher risk of psychological distress, and the mediating effect of sleep quality on this specific association. This study provides scientific guidance for the prevention of psychological distress among older adults, as well as an important theoretical basis for environmental health policy.
The present study indicated that solid cooking fuel use was significantly and positively associated with psychological distress among older adults in rural Shandong, China. Consistent with previous studies, we observed that exposure to air pollution from solid cooking fuels was associated with a higher risk of psychological distress among older adults [8, 9, 13]. One possible explanation is that using solid cooking fuels generates substantial health-harming pollutants, such as PM and CO [38]. These chemical pollutants emitted by solid cooking fuel use may increase levels of oxidative stress (OS) and neuroinflammatory cytokines in the human body, which have a close relationship with the pathogenesis of psychological distress [16, 39]. Another explanation for this finding is that household air pollution from solid cooking fuel use can cause or aggravate chronic diseases such as cardiovascular damage and cancer [7, 38], increasing disease burden, which affects psychological health potentially among older adults [40]. Besides, metabolic alterations caused by various gaseous pollutants from solid cooking fuels can cause psychological distress. Older adults chronically exposed to air pollutants have impaired metabolic function and elevated levels of triglycerides, free fatty acids, and glucose concentrations [41, 42]. Studies have shown that elevated levels of these indicators are associated with an increased risk of psychological disorders such as depression [43, 44].
Few studies have focused on the mechanisms underlying the relationship between solid cooking fuel use and psychological distress. Our mediation model revealed that sleep quality mediated the association between solid cooking fuel use and psychological distress among older adults. This finding suggested that rural older adults with solid cooking fuel use are more likely to suffer from psychological distress through poor sleep quality. Several possible explanations for this finding are as follows. First, using solid cooking fuels has a deleterious impact on the physiology of the respiratory system [15, 20]. Exposure to air pollutants from solid cooking fuel use can cause mucosal inflammation or edema, leading to sleep disorders through decreased pulmonary function and increased respiratory symptoms [20, 22]. Previous studies have pointed out that poor sleep quality can lead to a decline in physical status and various cognitive functions, including illnesses, pain, attention, and memory [7, 45]. Older adults with poor sleep quality have weakened planning and problem-solving abilities, which may make it difficult for them to cope with the challenges of daily life and ultimately cause psychological distress [46]. Second, long-term exposure to air pollutants in solid cooking fuel smoke is associated with a low level of serotonin [8]. Serotonin is a neurotransmitter that helps regulate wakefulness and circadian rhythms. Low serotonin levels may cause daytime sleepiness and normal nighttime sleep disturbance [47]. According to the cognitive model of insomnia [48], older adults with poor sleep quality exhibit more paranoid and worried attitudes towards sleep, such as overthinking about getting adequate sleep, which may further exacerbate emotional issues like anxiety [49]. Third, chemical pollutants from solid cooking fuel combustion can cause brain damage such as alterations of the blood-brain barrier and degenerating cortical neurons, which may have an impact on sleep quality [50]. Studies have shown that sleep disorders like short sleep duration and insomnia may lead to dysregulation of stress systems (e.g., hyperactivation of the hypothalamic-pituitary-adrenal (HPA) axis) [51], sensitizing older adults to stress-related disorders, including mood disorders, thereby contributing to the development of psychological distress [51, 52].
These findings have significant public health implications for improving the prevention strategies of psychological distress among older adults. First, primary care should pay more attention to and monitor the level of psychological distress characterized by depression and anxiety among rural older adults, especially solid cooking fuel users. Second, policymakers should increase financial investment to promote infrastructure for clean energy supply, especially in rural areas. Improving the accessibility of clean cooking fuels and advocating the preferential use of clean cooking fuels can help reduce the risk of psychological distress among older adults using solid cooking fuels. Finally, grassroots communities should conduct appropriate health education and healthy sleep promotion activities. Actively educate rural older adults about the hazards of solid fuels and remind them of kitchen ventilation, while strengthening the monitoring and assessment of sleep quality among rural older adults using solid cooking fuels.
There were several limitations of this study. First, this was a population-based cross-sectional study, and determining the causal relationship and the association direction between variables was difficult. More longitudinal design and experimental research are needed to confirm causality in the future. Second, the primary variable in this study was based on self-reported data, which may lead to recall bias, particularly in older adults. In the future, indoor air pollution levels from cooking fuels could be directly measured. Third, while we collected data on cooking fuel types, we ignored other indoor pollution information such as individual cooking duration of older adults, specific types and amounts of solid fuels used, seasonal variability, smoking, and heating, which may lead to under- or over-estimate the results. Fourth, this study excluded a subset of participants to obtain complete and accurate data, which could lead to potential bias with implications for the predictability and external validity of the results. Finally, this study validated only one mediating variable, and more potential mechanisms associated with solid cooking fuel use and psychological distress among older adults should be explored in the future.
Conclusions
The current study found that solid cooking fuel use was associated with an increased risk of psychological distress among older adults, with a mediating effect on sleep quality in this association. These findings suggested that substituting solid fuels for cooking with clean fuel may play an important role in reducing psychological distress among older solid cooking fuel users. In addition, there is an urgent need to prevent and improve sleep quality to reduce the potential risk of psychological distress among older adults who use solid cooking fuels.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- PM:
-
Particulate matter
- NO:
-
Nitric oxide
- NO2 :
-
Nitrogen dioxide
- CO:
-
Carbon monoxide
- SREHC:
-
Shandong Rural Elderly Health Cohort
- K10:
-
Kessler 10
- PSQI:
-
Pittsburgh Sleep Quality Index
- ADL:
-
Activities of daily living
- KHB:
-
Karlson, Holm, and Breen
- OS:
-
Oxidative stress
- HPA:
-
Hypothalamic-pituitary-adrenal
- IPAQ-S:
-
International Physical Activity Questionnaire Short Form
- MET:
-
Metabolism Equivalent
References
Jing Z, Li J, Fu PP, Wang Y, Yuan Y, Zhao D, Hao W, Yu C, Zhou C. Physical multimorbidity and lifetime suicidal ideation and plans among rural older adults: the mediating role of psychological distress. BMC Psychiatry. 2021;21(1):78. https://doi.org/10.1186/s12888-021-03087-4
Yang S, Li J, Zhao D, Wang Y, Li W, Li J, Li Z, Wei Z, Yan C, Gui Z, Zhou C. Chronic conditions, persistent pain, and psychological distress among the rural older adults: a path analysis in Shandong, China. Front Med (Lausanne). 2021;8:770914. https://doi.org/10.3389/fmed.2021.770914
Freire ACC, Pondé MP, Liu A, Caron J. Anxiety and depression as longitudinal predictors of mild cognitive impairment in older adults. Can J Psychiatry. 2017;62(5):343–50. https://doi.org/10.1177/0706743717699175
Atkins J, Naismith SL, Luscombe GM, Hickie IB. Psychological distress and quality of life in older persons: relative contributions of fixed and modifiable risk factors. BMC Psychiatry. 2013;13:249. https://doi.org/10.1186/1471-244X-13-249
Sun J, Lyu S. Social participation and urban-rural disparity in mental health among older adults in China. J Affect Disord. 2020;274:399–404. https://doi.org/10.1016/j.jad.2020.05.091
Gordon SB, Bruce NG, Grigg J, Hibberd PL, Kurmi OP, Lam KB, Mortimer K, Asante KP, Balakrishnan K, Balmes J, Bar-Zeev N, Bates MN, Breysse PN, Buist S, Chen Z, Havens D, Jack D, Jindal S, Kan H, Mehta S, Moschovis P, Naeher L, Patel A, Perez-Padilla R, Pope D, Rylance J, Semple S. Martin WJ 2nd. Respiratory risks from household air pollution in low and middle income countries. Lancet Respir Med. 2014;2(10):823–60. https://doi.org/10.1016/S2213-2600(14)70168-7
Yu K, Qiu G, Chan KH, Lam KH, Kurmi OP, Bennett DA, Yu C, Pan A, Lv J, Guo Y, Bian Z, Yang L, Chen Y, Hu FB, Chen Z, Li L, Wu T. Association of solid fuel use with risk of cardiovascular and all-cause mortality in rural China. JAMA. 2018;319(13):1351–61. https://doi.org/10.1001/jama.2018.2151
Banerjee M, Siddique S, Dutta A, Mukherjee B, Ranjan Ray M. Cooking with biomass increases the risk of depression in pre-menopausal women in India. Soc Sci Med. 2012;75(3):565–72. https://doi.org/10.1016/j.socscimed.2012.03.021
Li X, Guo Y, Xiao J, Liu T, Zeng W, Hu J, He G, Rong Z, Zhu Z, Wu F, Ma W. The effect of polluting cooking fuels on depression among older adults in six low- and middle-income countries. Sci Total Environ. 2022;838(Pt 2):155690. https://doi.org/10.1016/j.scitotenv.2022.155690
Li C, Zhou Y, Ding L. Effects of long-term household air pollution exposure from solid fuel use on depression: evidence from national longitudinal surveys from 2011 to 2018. Environ Pollut. 2021;283:117350. https://doi.org/10.1016/j.envpol.2021.117350
Block ML, Calderon-Garciduenas L. Air pollution: mechanisms of neuroinflammation and CNS disease. Trends Neurosci. 2009;32(9):506–16. https://doi.org/10.1016/j.tins.2009.05.009
MohanKumar SMJ, Campbell A, Block M, Veronesi B. Particulate matter, oxidative stress and neurotoxicity. Neurotoxicology. 2008;29(3):479–88. https://doi.org/10.1016/j.neuro.2007.12.004
Shao J, Ge T, Liu Y, Zhao Z, Xia Y. Longitudinal associations between household solid fuel use and depression in middle-aged and older Chinese population: a cohort study. Ecotoxicol Environ Saf. 2021;209:111833. https://doi.org/10.1016/j.ecoenv.2020.111833
Liu Y, Chen X, Yan Z. Depression in the house: the effects of household air pollution from solid fuel use among the middle-aged and older population in China. Sci Total Environ. 2020;703:134706. https://doi.org/10.1016/j.scitotenv.2019.134706
Sutunkova MP, Katsnelson BA, Privalova LI, Gurvich VB, Konysheva LK, Shur VY, Shishkina EV, Minigalieva IA, Solovjeva SN, Grebenkina SV, Zubarev IV. On the contribution of the phagocytosis and the solubilization to the iron oxide nanoparticles retention in and elimination from lungs under long-term inhalation exposure. Toxicology. 2016;363–364:19–28. https://doi.org/10.1016/j.tox.2016.07.006
Bhatt S, Nagappa AN, Patil CR. Role of oxidative stress in depression. Drug Discov Today. 2020;25(7):1270–6. https://doi.org/10.1016/j.drudis.2020.05.001
Czeisler CA. Duration, timing and quality of sleep are each vital for health, performance and safety. Sleep Health. 2015;1(1):5–8. https://doi.org/10.1016/j.sleh.2014.12.008
Wang P, Song L, Wang K, Han X, Cong L, Wang Y, Zhang L, Yan Z, Tang S, Du Y. Prevalence and associated factors of poor sleep quality among Chinese older adults living in a rural area: a population-based study. Aging Clin Exp Res. 2020;32(1):125–31. https://doi.org/10.1007/s40520-019-01171-0
Zhao D, Li J, Hao W, Yuan Y, Yu C, Jing Z, Wang Y, Fu P, Zhou C. The relationship between activities of daily living and suicidal ideation among Chinese rural older adults: a multiple mediation model through sleep quality and psychological distress. Aging. 2020;12(22):22614–25. https://doi.org/10.18632/aging.103857
Chen C, Liu GG, Sun Y, Gu D, Zhang H, Yang H, Lu L, Zhao Y, Yao Y. Association between household fuel use and sleep quality in the oldest-old: evidence from a propensity-score matched case-control study in Hainan, China. Environ Res. 2020;191:110229. https://doi.org/10.1016/j.envres.2020.110229
Liao W, Liu X, Kang N, Song Y, Wang L, Yuchi Y, Huo W, Mao Z, Hou J, Wang C. Associations of cooking fuel types and daily cooking duration with sleep quality in rural adults: effect modification of kitchen ventilation. Sci Total Environ. 2023;854:158827. https://doi.org/10.1016/j.scitotenv.2022.158827
Shumake KL, Sacks JD, Lee JS, Johns DO. Susceptibility of older adults to health effects induced by ambient air pollutants regulated by the European Union and the United States. Aging Clin Exp Res. 2013;25(1):3–8. https://doi.org/10.1007/s40520-013-0001-5
Li J, Qin C, Lv J, Guo Y, Bian Z, Zhou W, Hu J, Zhang Y, Chen J, Cao W, Yu C, Li L. Solid fuel use and incident COPD in Chinese adults: findings from the China Kadoorie Biobank. Environ Health Perspect. 2019;127(5):57008. https://doi.org/10.1289/EHP2856
Meier-Ewert HK, Ridker PM, Rifai N, Regan MM, Price NJ, Dinges DF, Mullington JM. Effect of sleep loss on C-reactive protein, an inflammatory marker of cardiovascular risk. J Am Coll Cardiol. 2004;43(4):678–83. https://doi.org/10.1016/j.jacc.2003.07.050
Wang Y, Fu P, Li J, Jing Z, Wang Q, Zhao D, Zhou C. Changes in psychological distress before and during the COVID-19 pandemic among older adults: the contribution of frailty transitions and multimorbidity. Age Ageing. 2021;50(4):1011–8. https://doi.org/10.1093/ageing/afab061
Zhao D, Li J, Gao T, Sun J, Wang Y, Wang Q, Zhou C. Do older adults with multimorbidity prefer institutional care than those without multimorbidity? The role of functional limitation. BMC Geriatr. 2022;22(1):126. https://doi.org/10.1186/s12877-022-02812-2
Jing Z, Li J, Wang Y, Ding L, Tang X, Feng Y, Zhou C. The mediating effect of psychological distress on cognitive function and physical frailty among the elderly: evidence from rural Shandong, China. J Affect Disord. 2020;268:88–94. https://doi.org/10.1016/j.jad.2020.03.012
Zhou C, Chu J, Wang T, Peng Q, Heng J, Zheng W, Liu D, Wang X, Ma H, Xu L. Reliability and validity of 10-item Kessler scale (K10) Chinese version in evaluation of mental health status of Chinese population. Chin J Clin Psychol. 2008;16:627–9.
Nakamura K, Watanabe Y, Kitamura K, Kabasawa K, Someya T. Psychological distress as a risk factor for dementia after the 2004 Niigata-Chuetsu earthquake in Japan. J Affect Disord. 2019;259:121–7. https://doi.org/10.1016/j.jad.2019.08.041
Liu X, Tang M, Hu L, Wu A, Wu H, Zhao G, Gao C, Li W. Reliability and validity of the Pittsburgh sleep quality index. Chin J Psychiatry. 1996;29:103–7.
Mollayeva T, Thurairajah P, Burton K, Mollayeva S, Shapiro CM, Colantonio A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: a systematic review and meta-analysis. Sleep Med Rev. 2016;25:52–73. https://doi.org/10.1016/j.smrv.2015.01.009
Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. https://doi.org/10.1016/0165-1781(89)90047-4
Macfarlane DJ, Lee CC, Ho EY, Chan KL, Chan DT. Reliability and validity of the Chinese version of IPAQ (short, last 7 days). J Sci Med Sport. 2007;10(1):45–51. https://doi.org/10.1016/j.jsams.2006.05.003
Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185:914–9. https://doi.org/10.1001/jama.1963.03060120024016
Breen R, Karlson KB, Holm A. Total, direct, and indirect effects in logit and probit models. Sociol Methods Res. 2013;42(2):164–91.
Kohler U, Karlson KB, Holm A. Comparing coefficients of nested nonlinear probability models. Stata J. 2011;11(3):420–38.
Zhou H, Long L. Statistical remedies for common method biases. Adv Psychol Sci. 2004;(06):942–50.
Lee KK, Bing R, Kiang J, Bashir S, Spath N, Stelzle D, Mortimer K, Bularga A, Doudesis D, Joshi SS, Strachan F, Gumy S, Adair-Rohani H, Attia EF, Chung MH, Miller MR, Newby DE, Mills NL, McAllister DA, Shah ASV. Adverse health effects associated with household air pollution: a systematic review, meta-analysis, and burden estimation study. Lancet Glob Health. 2020;8(11):e1427–34. https://doi.org/10.1016/S2214-109X(20)30343-0
Li W, Dorans KS, Wilker EH, Rice MB, Ljungman PL, Schwartz JD, Coull BA, Koutrakis P, Gold DR, Keaney JF Jr, Vasan RS, Benjamin EJ, Mittleman MA. Short-term exposure to ambient air pollution and biomarkers of systemic inflammation: the Framingham Heart Study. Arterioscler Thromb Vasc Biol. 2017;37(9):1793–800. https://doi.org/10.1161/ATVBAHA.117.309799
Pruchno RA, Wilson-Genderson M, Heid AR. Multiple chronic condition combinations and depression in community-dwelling older adults. J Gerontol Biol Sci Med Sci. 2016;71(7):910–5. https://doi.org/10.1093/gerona/glw025
Yang S, Chen R, Zhang L, Sun Q, Li R, Gu W, Zhong M, Liu Y, Chen LC, Sun Q, Liu C. Lipid metabolic adaption to long-term ambient PM2.5 exposure in mice. Environ Pollut. 2021;269:116193. https://doi.org/10.1016/j.envpol.2020.116193
Rajagopalan S, Park B, Palanivel R, Vinayachandran V, Deiuliis JA, Gangwar RS, Das L, Yin J, Choi Y, Al-Kindi S, Jain MK, Hansen KD, Biswal S. Metabolic effects of air pollution exposure and reversibility. J Clin Invest. 2020;130(11):6034–40. https://doi.org/10.1172/JCI137315
Zhang M, Chen J, Yin Z, Wang L, Peng L. The association between depression and metabolic syndrome and its components: a bidirectional two-sample mendelian randomization study. Transl Psychiatry. 2021;11(1):633. https://doi.org/10.1038/s41398-021-01759-z
Ernst J, Hock A, Henning A, Seifritz E, Boeker H, Grimm S. Increased pregenual anterior cingulate glucose and lactate concentrations in major depressive disorder. Mol Psychiatry. 2017;22(1):113–9. https://doi.org/10.1038/mp.2016.73
Miyata S, Noda A, Iwamoto K, Kawano N, Okuda M, Ozaki N. Poor sleep quality impairs cognitive performance in older adults. J Sleep Res. 2013;22(5):535–41. https://doi.org/10.1111/jsr.12054
Tempesta D, Couyoumdjian A, Curcio G, Moroni F, Marzano C, De Gennaro L, Ferrara M. Lack of sleep affects the evaluation of emotional stimuli. Brain Res Bull. 2010;82(1–2):104–8. https://doi.org/10.1016/j.brainresbull.2010.01.014
Wang Y, Mao Z, Chen G, Tu R, Abdulai T, Qiao D, Liu X, Dong X, Luo Z, Wang Y, Li R, Huo W, Yu S, Guo Y, Li S, Wang C. Association between long-term exposure to ambient air pollutants and excessive daytime sleepiness in Chinese rural population: the Henan Rural Cohort Study. Chemosphere. 2020;248:126103. https://doi.org/10.1016/j.chemosphere.2020.126103
Harvey AG. A cognitive model of insomnia. Behav Res Ther. 2002;40(8):869–93.
Palmer CA, Alfano CA. Sleep and emotion regulation: an organizing, integrative review. Sleep Med Rev. 2017;31:6–16. https://doi.org/10.1016/j.smrv.2015.12.006
Balmes JR. Household air pollution from domestic combustion of solid fuels and health. J Allergy Clin Immunol. 2019;143(6):1979–87. https://doi.org/10.1016/j.jaci.2019.04.016
Meerlo P, Sgoifo A, Suchecki D. Restricted and disrupted sleep: effects on autonomic function, neuroendocrine stress systems and stress responsivity. Sleep Med Rev. 2008;12(3):197–210. https://doi.org/10.1016/j.smrv.2007.07.007
Doolin K, Farrell C, Tozzi L, Harkin A, Frodl T, O’Keane V. Diurnal hypothalamic-pituitary-adrenal axis measures and inflammatory marker correlates in major depressive disorder. Int J Mol Sci. 2017;18(10):2226. https://doi.org/10.3390/ijms18102226
Acknowledgements
We thank the officials of health agencies, all participants and staffs at the study sites for their cooperation.
Funding
This work was supported by the National Natural Science Foundation of China (grant numbers 72274109, 71974117, 71774104). The funders had no role in study design, data collection, analysis, decision to publish, or manuscript preparation.
Author information
Authors and Affiliations
Contributions
CCZ designed the study; JJL and DZ conducted the data acquisition; JJL and TTG performed the statistical analyses and interpreted the data; JJL drafted the manuscript; XHW and XQW engaged in the development of the study framework, interpretation of the results; SJC and JYL contributed to the revisions of successive drafts of the manuscript; CCZ, TTG and DZ critically reviewed and revised the manuscript; All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was reviewed and approved by the Ethics Committee of Shandong University. Before the survey, written informed consent was obtained from each participant, clarifying the purposes, significance, methods, and potential risks of the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Luo, J., Zhao, D., Gao, T. et al. The mediating effect of sleep quality on solid cooking fuel use and psychological distress among rural older adults: evidence from Shandong, China. BMC Geriatr 24, 750 (2024). https://doi.org/10.1186/s12877-024-05327-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-024-05327-0