
Abstract
Background
Solid fuels are still widely used for cooking in rural China, leading to various health implications. Yet, studies on household air pollution and its impact on depression remain scarce. Using baseline data from the China Kadoorie Biobank (CKB) study, we aimed to investigate the relationship between solid fuel use for cooking and depression among adults in rural China.
Methods
Data on exposure to household air pollution from cooking with solid fuels were collected and the Chinese version of the World Health Organization Composite International Diagnostic Interview short-form (CIDI-SF) was used to evaluate the status of major depressive episode. Logistic regression analysis was performed to investigate the association between solid fuel use for cooking and depression.
Results
Amongst 283,170 participants, 68% of them used solid fuels for cooking. A total of 2,171 (0.8%) participants reported of having a major depressive episode in the past 12 months. Adjusted analysis showed that participants who had exposure to solid fuels used for cooking for up to 20 years, more than 20 to 35 years, and more than 35 years were 1.09 (95% CI: 0.94–1.27), 1.18 (95% CI: 1.01–1.38), and 1.19 (95% CI: 1.01–1.40) times greater odds of having a major depressive episode, respectively, compared with those who had no previous exposure to solid fuels used for cooking.
Conclusion
The findings highlight that longer exposure to solid fuels used for cooking would be associated with increased odds of major depressive episode. In spite of the uncertainty of causal relationship between them, using solid fuels for cooking can lead to undesirable household air pollution. Reducing the use of solid fuels for cooking by promoting the use of clean energy should be encouraged.
Similar content being viewed by others


Background
Depression is one of the most common mental health disorders, affecting more than 280 million people globally [1]. A recent systematic review and meta-analysis revealed that the 12-month and lifetime prevalence rates of major depressive disorder in China were 1.6% and 1.8%, respectively, and the percentages had been increasing over time [2]. If the population in China is estimated to be 1.426 billion in 2023 [3], the 12-month prevalence of major depressive disorder may reach over 22.8 million of individuals. A longitudinal population study in Australia suggested that the severity of depression is a major predictor for suicidal ideation and suicidal attempt [4]. Based on a recent meta-analysis on 15 studies, the prevalence of suicidal attempt in a lifetime among individuals with major depressive disorder was 3.45 times higher than those without major depressive disorder [5]. A study conducted in mainland China reported that the prevalence of suicidal ideation was 16.7% among 1,916 patients (18–70 years old) with major depressive disorder [6]. Symptoms of major depressive disorder, such as low mood, anhedonia and impaired cognition, are one of the key contributors to functional impairment [7], which could cause a great economic burden to the society. A study by Rayner et al. [8] reported that there was a significant correlation between total healthcare costs (i.e., accident and emergency department visits, hospitalizations, and visits to doctor) and depression. In addition, patients with multimorbidity and depression had more than twice the inpatient costs compared with those without depression [9]. The estimated health burden from depression has been continuously increasing over the years. More recently, a systematic review reported that major depressive disorder was accounted for 49 million disability-adjusted life-years in 2020 [10].
Approximately 2.4 billion people still use solid fuels such as animal dung, wood, and coal for cooking globally [11]. To date, solid fuels are extensively used in China, especially in rural households. There are half a billion people (40% of total population) in mainland China living in rural areas [12], with more than three-fourths of these rural households using solid fuels for cooking [13]. Incomplete combustion of solid fuels produces compounds such as carbon monoxide, sulphur dioxide, black carbon and PM2.5(fine particulate matter with a diameter of less or equal to 2.5 μm) [14]. Concentrations of PM2.5 from household air pollution due to cooking with solid fuels can be substantially high, causing up to 40% higher PM2.5exposure compared with the indoor and outdoor environments [15]. Previous studies have confirmed that the exposure to solid fuel use contributes to adverse health effects such as sleep disturbance [16], chronic bronchitis and obstructive pulmonary disease [17], hypertension [18] and an increased risk of cardiovascular disease hospitalization and stroke among rural population [19]. A nationwide prospective cohort study also reported significant association between using solid fuels for cooking and cardiovascular mortality in China [20].
A longitudinal study conducted in the United States reported that individuals with previous 30-day exposure to ambient fine PM were 1.2 times more likely to have moderate to severe depressive symptoms [21]. Based on a national longitudinal survey in China, cooking with solid fuels was associated with a higher risk of depressive symptoms among individuals aged 60 years and above [22]. Similarly, a cohort study also reported positive association between solid fuel use and depression [21]. However, the study conducted by Pun et al. [21] in the urban areas of the United States did not focus specifically on household use of solid fuels as the source of air pollution. Meanwhile, the studies conducted by Li et al. [22] and Shao et al. [23] were restricted to middle-aged and older Chinese population living in urban or rural areas.
Air pollutant emissions from solid fuels are associated with adverse health effects. In recent decades, improved cookstoves and combustion technologies have been implemented but a large number of individuals remain using solid fuels for cooking. Despite the important role of solid fuels in producing energy, its potential detrimental impact on mental health demands urgent attention. There is a lack of studies focusing on the use of epidemiological data to investigate the association between solid fuel use and depression in developing countries; concerns arise as China is the second most populous country where 40% of the population are living in rural areas and actively using solid fuels for cooking. It is crucial to investigate the relationship between these two variables specifically in rural China with a large-scale study. Therefore, this current study aimed to investigate the association between using solid fuels for cooking and depression in rural China.
Methods
Study design and population
This study employed a secondary data analysis using the baseline data from the China Kadoorie Biobank (CKB) study. The original CKB study was conducted between 2004 and 2008, which recruited over 0.5 million adults from 10 regions across mainland China. After providing informed written consent, each participant attended a face-to-face interview and a physical examination. A total of 512,681 adults aged between 30 and 79 years (without any major disability) with permanent residence were included in this baseline survey. A standardized electronic questionnaire was used to collect participant information including sociodemographic characteristics, lifestyle habits, exposure to passive smoking and domestic indoor air pollution, medical history, physical activity, and mental health status. The questionnaire used can be accessed via the official website of CKB (https://www.ckbiobank.org/study-resources/survey-data). Each participant’s resting blood pressure (BP) was measured using the A&D digital BP monitor (Model No.: UA-779). A body composition analyzer (Model No.: TBF-300GS) was used to measure body mass index (BMI), while a standing height measuring instrument was used to measure weight and height. BMI is calculated by using this formula: the participant’s weight in kilograms (kg) divided by the square of height (H) in meters (m), (BMI = kg/ H2) [24]. BMI at 28 kg / m2is recommended as the cut-off point for obesity for the Chinese people [25, 26]. More detailed information about the original CKB study has been previously reported [27,28,29]. Ethics approvals for the CKB study were obtained from the Chinese Center for Disease Control and Prevention (Approval Notice 005/2004) and the Oxford Tropical Research Ethics Committee (OxTREC Ref: 025–04) of the University of Oxford. The study was conducted in line with the principles outlined in the Declaration of Helsinki.
Measurements
Exposure to household use of solid fuels
The approach of Yu et al. [20] was followed to calculate the durations of exposure to solid fuels used for cooking and heating separately. Participants were asked to provide detailed information about their exposure to household use of solid fuels for cooking and heating, including related information such as the duration (in years) they lived in their three most recent residences, frequency of cooking in each residence, types of fuels used for cooking and heating, and availability of cookstove ventilation (chimney or extractor). Participants who reported that they cooked less often than once a month in a residence were considered as noncooking and regarded as having no exposure to solid fuel used for cooking. Participants who reported that they cooked at least once a month were then asked to provide additional information related to the types of primary fuels they used. There are two categories of primary fuels, namely “clean fuels” such as gas and electricity, and “solid fuels” such as wood and coal [30]. The total duration (in years) of household use of solid fuels for cooking was calculated by summing up the duration of using solid fuels as the primary cooking fuel in each residence. Likewise, participants who used solid fuels for heating in winter were asked further questions about the types of primary fuels they used, and the total duration (in years) of household use of solid fuels for heating was calculated by summing up the corresponding duration in each residence. The level of exposure to solid fuels used for heating was estimated by multiplying a weight coefficient to years of solid fuels used for heating, of which the weight coefficient was calculated based on the average portion of years with temperature less than 8 degree Celsius in each of the residences from 1999 to 2013, ranging from 0.18 to 0.42, as detailed in Yu et al. [20].
Depression
In this study, major depressive episode was evaluated by the Chinese version of the World Health Organization Composite International Diagnostic Interview short-form (CIDI-SF) [31]. As there is no gold standard for assessing mental disorders in the CIDI-SF, this version was calibrated rather than validated and produced similar population estimates of major depressive episode to the Structured Clinical Interview for DSM-IV, which is a state-of-the-art clinical research diagnostic interview tool for mental disorders [32]. Participants were first asked whether they had any of the following symptoms lasting for ≥ 2 weeks in the past 12 months: a) feeling much saddened, or depressed than usual; b) loss of interest in most things like hobbies or activities that usually gave you pleasure; c) feeling so hopeless and loss of appetite even for your favorite food; d) feeling worthless and useless, everything that went wrong was your fault, and life was very difficult with no way out. If participants answered “yes” to any of the above-mentioned situations, they were further assessed for major depression using CIDI-SF through a face-to-face interview by trained health professionals. Participants who reported at least 3 out of 7 depression symptoms (i.e., 1) weight change, 2) difficulty in sleeping, 3) losing interest in things, 4) feeling tired or low on energy, 5) trouble concentrating, 6) feeling worthless, or 7) thoughts about death) in the CIDI-SF questionnaire were considered likely to have major depression [33].
Covariates
Adjustment for covariates was performed in this analysis, including sociodemographic characteristics (i.e., age, gender, marital status, education level and annual household income), lifestyle habits (i.e., smoking status, alcohol assumption, and physical activity), health status (i.e., BMI and blood pressure), stressful life events in the past two years, passive smoking, cookstove ventilation, and exposure to solid fuels used for heating. Smoking status was classified into four categories: 1) never smoke, 2) quitted, 3) occasional smoker, and 4) current smoker. Participants were classified as a “regular alcohol drinker” if they reported that they drank alcohol “usually at least once a week.” Otherwise, they were classified as a “non-regular drinker.” Physical activity was estimated as metabolic equivalent task hours per day spent on activities related to occupation, commuting, housework, and non-sedentary leisure-time activities. Exposure to stressful life events (Yes/No) was defined as the occurrence of common major life events in the past two years, such as death of a spouse, marital separation/divorce, traffic accident and major natural disaster. Exposure to passive smoking was assessed by self-report responses to the question related to frequency of secondhand smoking exposure. The variable was categorized into 4 levels (none, > 0 to 2 h/week, > 2 to 12 h/week, > 12 h/week). The cut-off points were conventionally selected based on the tertile points among those who had exposure to passive smoking, with the three exposure categories being anticipated to reflect low, middle and high levels of exposure to passive smoking.
Statistical analysis
All statistical analyses were conducted using the IBM SPSS 25.0 (IBM Corp., Armonk, NY). Data were summarized descriptively using statistics including means, standard deviations, frequencies and percentages. For continuous variables, skewness statistics and normality probability plots were used to assess normality. In this study, the outcome of interest was status of major depressive episode in the past year (Yes/No). The primary exposure of interest was duration of solid fuels used for cooking which was categorized into four levels. Specifically, those participants who had no previous exposure to solid fuels used for cooking or always used clean fuels were categorized as the reference group. The remaining participants were conventionally stratified into three tertiles to characterize low, middle and high levels of exposure with totally four levels for the exposure factor: (i) none, (ii) > 0 to 20 years, (iii) > 20 to ≤ 35 years, (iv) > 35 years. Likewise, the exposure to solid fuels used for heating was categorized into four levels: (i) none, (ii) > 0 to 8.2 years, (iii) > 8.2 to ≤ 13.5 years, (iv) > 13.5 years. The association between major depression in the past year and exposure to solid fuels used for cooking was examined by logistic regression analysis. Unadjusted and adjusted logistic regression analyses were conducted with adjustment for the covariates of sociodemographic characteristics and lifestyle habits, presence of stressful life events in the past two years, presence of cookstove ventilation, exposure to passive smoking, and level of exposure to solid fuels used for heating. As the time scope of the outcome of major depressive episode was the past 12 months from the time of survey, it was possible that some participants might have a major depressive episode prior to exposure to solid fuel usage. A sensitivity analysis was therefore conducted by excluding those participants who had no more than one year of solid fuel usage before the survey. All tests involved were 2-sided at 5% level of significance.
A total of 283,170 participants were included in this secondary data analysis study. Among them, 2,171 participants were classified as having major depressive episode in the past year, and there were totally 91,611 participants without exposure to solid fuels used for cooking and 61,873 to 65,612 participants with different levels of exposure to solid fuels used for cooking. Such a sample size is adequate to detect an odds ratio of having major depressive episode of as small as 1.17 when comparing anyone of the exposure groups with the non-exposure group with over 80% power at 2-sided 5% level of significance.
Results
Characteristics of the study population
Amongst 283,170 participants who were included in the baseline survey of the CKB study, the average age was 51.4 (SD = 10.5) years, and 58.2% of them were female. About 68% of them used solid fuels for cooking, with a 27-year median. More than half of the study sample (67%) had at least some cookstove ventilation. Nearly 23% participants had exposure to passive smoking for more than 12 h per week. A total of 2,171 (0.8%) participants reported major depressive episode in the past year. Characteristics of the study population stratified by levels of exposure to solid fuels used for cooking are shown in Table 1.
Association between household use of solid fuels for cooking and major depressive episode
Based on their duration of exposure to solid fuels used for cooking, participants were categorized into four levels: (i) none, (ii) > 0 to 20 years, (iii) > 20 to ≤ 35 years, (iv) > 35 years. Those participants who had no previous exposure to solid fuels used for cooking or always used clean fuels for cooking were categorized as the reference group (none exposure). The remaining participants were conventionally stratified into three tertiles to characterize low, middle and high levels of exposure. Unadjusted logistic regression analysis showed that an increased level of exposure to solid fuels used for cooking was associated with an increased odds of having a major depressive episode (unadjusted model in Table 2). After adjusting for sociodemographic characteristics, obesity and lifestyle habits, presence of stressful life events, presence of cookstove ventilation, passive smoking exposure, and level of exposure to solid fuels used for heating, the pattern of association between an increased odds of having a major depressive episode and an increased level of exposure was also noted. Participants who had exposure to solid fuels used for cooking for up to 20 years, more than 20 to 35 years, and more than 35 years were 1.09 (95% CI 0.94–1.27), 1.18 (95% CI: 1.01–1.38) and 1.19 (95% CI: 1.01–1.40) times greater odds of having a major depressive episode, respectively, compared with those who had no previous exposure to solid fuel used for cooking or always used clean fuels for cooking (adjusted model 1 in Table 2). A sensitivity analysis was conducted by excluding those participants who had no more than one year of solid fuel usage before the survey, the results were similar to the primary analysis one (adjusted model 2 in Table 2).
Discussion
Approximately 46% of the population in China used solid fuels as a household energy source, leading to household air pollution; and the proportion was substantially higher in rural areas [13, 23]. In fact, the present study found that 68% of rural residents used solid fuels for cooking. To the best of our knowledge, this is the largest national study to explore the relationship between solid fuel use and depression in rural China. The results revealed an association between household use of solid fuels for cooking and major depression, particularly for those who had used solid fuels for more than 20 years, after controlling for potential confounding covariates, including sociodemographic characteristics, lifestyle habits, health status, presence of stressful life events, presence of cookstove ventilation, passive smoking exposure, and exposure to solid fuels used for heating. Although participants with longer exposure generally associated with an increased odds of having a major depressive episode, the odds ratio of the longest exposure group (> 35 years, OR = 1.19) was unexpectedly similar to the second longest exposure group (> 20 to 35 years, OR = 1.18). A possible explanation may be owing to the fact that people with longer exposure were more likely subject to a competing risk of death, which may diminish the strength of association, particularly in the longest exposure group.
There is a growing body of evidence that solid fuel use is associated with a high risk of depression [22, 23], which is consistent with the current findings. Individuals (N= 8637) with exposure to solid fuel combustion for over 4 years had 1.12 times greater odds of having depressive symptoms [23]. Supported by the following longitudinal survey (N= 7005) [22], individuals using solid fuels in cooking for more than 7 years had 1.36 times greater odds of depression risk than those who always used clean fuels.
This study, together with the aforementioned previous studies, provides evidence on the association between the exposure to solid fuels and the prevalence of depression. However, only limited evidence exists on the mechanisms linking the use of solid fuels for cooking with depression. The incomplete combustion of solid fuels generates various air pollutants including PM, carbon monoxide, sulfur oxides, and polycyclic aromatic hydrocarbons [34, 35]. One possible explanation may be that inhalation of air pollutants can trigger associated oxidative stress, cerebrovascular damage, neuroinflammation, and neurodegenerative pathology, which all might cause or exacerbate the risk of depression [36,37,38]. Animal experience revealed that PM might cause neurotoxicity by inducing microglia activation characterized by the release of TNFα, which damages the olfactory bulb and increases depression risk [39]. Moreover, studies indicated that PM causes elevated levels of cortisol [40], which has been related to the development of depression [41]. Furthermore, domestic cooking with solid fuels could increase the risk of chronic diseases, such as cancer and cardiorespiratory diseases [19, 42], which are strongly associated with depression [43, 44].
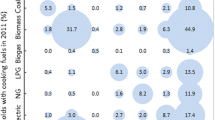
In rural China, solid fuels are reported to be the dominant cooking fuel, with biomass and coal accounting for 47.6% [45] and 13.5% [46], respectively. Our study gives valuable insights into the potential hazardous effects of using solid fuels for cooking on mental health. It indicates household solid fuels used for cooking is a critical public health issue and that policy makers must take responsibility to make the needed policy changes. It is necessary to encourage people to switch to cleaner fuels and technologies when cooking to reduce exposure to household air pollution. Moreover, in this study, depressive episode was more prevalent in those without cookstove ventilation. This result is in line with those of the previous studies [22, 47], showing that cooking ventilation may weaken the relationship of cooking with solid fuel and long duration cooking with depressive symptoms, suggesting that improvements in cooking ventilation should be strongly encouraged.
As a remark, although people with longer exposure to solid fuels used for cooking generally associated with an increased odds of having a major depression episode, the odds ratio of the longest exposure group (> 35 years, OR = 1.19) was unexpectedly similar to the second longest exposure group (> 20 to 35 years, OR = 1.18). A possible explanation may be owing to the fact that people with longer exposure were more likely subject to a competing risk of death, which may diminish the strength of association, particularly in the longest exposure group.
Despite the significance of the findings, there are several limitations in this study that may impact the generalisability of this study. First, the cross-sectional study design assesses both outcome of interest and exposure simultaneously. Therefore, it may not be able to establish a cause-and-effect relationship between household solid fuels used for cooking and depression. In addition, self-reported information is prone to recall bias when participants fail to accurately remember an event in the past. Nonetheless, the overestimation or underestimation of association between cause and effect may be resolved through a longitudinal cohort study in which an event may be observed first, followed by the effects. On the other hand, different cooking practices and chemical properties of fuel such as density, volatility and thermal capacity which could affect the indoor air pollution were not examined in the CKB study. Hence, this could result in imprecision of actual exposure to solid fuels used for cooking. Although this study had controlled for potential confounders (e.g., sociodemographic characteristics, obesity status and lifestyle habits, presence of stressful life events, presence of cookstove ventilation and passive smoking exposure), the results might be confounded by other unmeasured covariates. This is because our study was a secondary data analysis where the adjusted analysis was only able to be performed based on existing available variables.
Conclusion
This study demonstrates the significant association between the use of household solid fuels for cooking and the prevalence of depression in rural China; and the longer duration of exposure, the higher odds of having a depressive episode. Further studies are warranted to examine if there is a causal relationship between them. Nevertheless, reducing the use of solid fuels for cooking by promoting the use of clean energy should be encouraged.
Availability of data and materials
The datasets used and analyzed during this current study are available from the corresponding author on reasonable request.
References
World Health Organization. Depression. 2021. https://www.who.int/news-room/fact-sheets/detail/depression. Accessed 20 Nov 2022.
Zhao YJ, Jin Y, Rao WW, et al. Prevalence of major depressive disorder among adults in China: a systematic review and meta-analysis. Front Psychiatry. 2021;12:659470. https://doi.org/10.3389/fpsyt.2021.659470.
United Nations. India overtakes China as the world’s most populous country. 2023. https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/undesa_pd_2023_policy-brief-153.pdf . Accessed 3 May 2023.
Handley T, Rich J, Davies K, Lewin T, Kelly B. The challenges of predicting suicidal thoughts and behaviours in a sample of rural Australians with depression. Int J Environ Res Public Health. 2018;15(5):928. https://doi.org/10.3390/ijerph15050928.
Cai H, Xie XM, Zhang Q, Cui X, Lin JX, Sim K, Ungvari GS, Zhang L, Xiang YT. Prevalence of suicidality in major depressive disorder: a systematic review and meta-analysis of comparative studies. Front Psychiatry. 2021;12:690130. https://doi.org/10.3389/fpsyt.2021.690130.
Ge F, Jiang J, Wang Y, Yuan C, Zhang W. Identifying suicidal ideation among Chinese patients with major depressive disorder: evidence from a real-world hospital-based study in China. Neuropsychiatr Dis Treat. 2020;16:665–72. https://doi.org/10.2147/NDT.S238286.
Chow TK, Bowie CR, Morton M, Lalovic A, McInerney SJ, Rizvi SJ. Contributors of functional impairment in major depressive disorder: a biopsychosocial approach. Curr Behav Neurosci Rep. 2022;9:59–72. https://doi.org/10.1007/s40473-022-00247-y.
Rayner L, Hotopf M, Petkova H, Matcham F, Simpson A, McCracken LM. Depression in patients with chronic pain attending a specialised pain treatment centre: prevalence and impact on health care costs. Pain. 2016;157(7):1472–9. https://doi.org/10.1097/j.pain.0000000000000542.
Bock JO, Luppa M, Brettschneider C, et al. Impact of depression on health care utilization and costs among multimorbid patients–from the MultiCare Cohort Study. PLoS One. 2014;9(3):e91973. https://doi.org/10.1371/journal.pone.0091973.
COVID-19 Mental Disorders Collaborators. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet (London, England). 2021;398:1700–12. https://doi.org/10.1016/S0140-6736(21)02143-7.
World Health Organization. Household air pollution: key facts. 2022. https://www.who.int/news-room/fact-sheets/detail/household-air-pollution-and-health#:~:text=Worldwide%2C%20around%202.4%20billion%20people,and%20i . Accessed 22 Jan 2023.
NBSC. China statistical yearbook-2019. Beijing: China Statistics Press; 2019.
Tang X, Liao H. Energy poverty and solid fuels use in rural China: analysis based on national population census. Energy Sustain Dev. 2014;23:122–9. https://doi.org/10.1016/J.ESD.2014.08.006.
Shen G, Xing R, Zhou Y, et al. Revisiting the proportion of clean household energy users in rural China by accounting for energy stacking. Sustainable Horizons. 2022;1:100010. https://doi.org/10.1016/j.horiz.2022.100010.
Xu H, Li Y, Guinot B, et al. Personal exposure of PM2. 5 emitted from solid fuels combustion for household heating and cooking in rural Guanzhong Plain, northwestern China. Atmos Environ. 2018;185:196–206. https://doi.org/10.1016/j.atmosenv.2018.05.018.
Chair SY, Choi KC, Cao X, et al. Association between household solid fuel use for cooking and sleep disturbance in rural China: findings from the China Kadoorie Biobank data. Sleep Med. 2021;83:13–20. https://doi.org/10.1016/J.SLEEP.2021.04.029.
Po JY, FitzGerald JM, Carlsten C. Respiratory disease associated with solid biomass fuel exposure in rural women and children: systematic review and meta-analysis. Thorax. 2011;66:232–9. https://doi.org/10.1136/THX.2010.147884.
Yan Z, Liu Y, Yin Q, et al. Impact of household solid fuel use on blood pressure and hypertension among adults in China. Air Qual Atmos Health. 2016;9:931–40. https://doi.org/10.1007/S11869-016-0395-2/TABLES/5.
Hystad P, Duong M, Brauer M, et al. Health effects of household solid fuel use: Findings from 11 Countries within the prospective urban and rural epidemiology study. Environ Health Perspect. 2019;127(5):57003. https://doi.org/10.1289/EHP3915.
Yu K, Qiu G, Chan KH, et al. Association of solid fuel use with risk of cardiovascular and all-cause mortality in rural China. JAMA. 2018;319(13):1351–61. https://doi.org/10.1001/jama.2018.2151.
Pun VC, Manjourides J, Suh H. Association of ambient air pollution with depressive and anxiety symptoms in older adults: Results from the NSHAP study. Environ Health Perspect. 2017;125(3):342–8. https://doi.org/10.1289/EHP494.
Li C, Zhou Y, Ding L. Effects of long-term household air pollution exposure from solid fuel use on depression: evidence from national longitudinal surveys from 2011 to 2018. Environ Pollut. 2021;283:117350. https://doi.org/10.1016/j.envpol.2021.117350.
Shao J, Ge T, Liu Y, Zhao Z, Xia Y. Longitudinal associations between household solid fuel use and depression in middle-aged and older Chinese population: a cohort study. Ecotoxicol Environ Saf. 2021;209:111833. https://doi.org/10.1016/j.ecoenv.2020.111833.
Lemmens HJ, Brodsky JB, Bernstein DP. Estimating ideal body weight–a new formula. Obes Surg. 2005;15(7):1082–3.
Xu W, Zhang H, Paillard-Borg S, Zhu H, Qi X, Rizzuto D. Prevalence of overweight and obesity among Chinese adults: role of adiposity indicators and age. Obes Facts. 2016;9(1):17–28. https://doi.org/10.1159/000443003.
Zhou B, Coorperative Meta-Analysis Group of China Obesity Task Force. Predictive values of body mass index and waist circumference to risk factors of related diseases in Chinese adult population. Zhonghua Liu Xing Bing Xue Za Zhi. 2002;23(1):5–10.
Chen Z, Lee L, Chen J, et al. Cohort profile: the Kadoorie Study of Chronic Disease in China (KSCDC). Int J Epidemiol. 2005;34(6):1243–9. https://doi.org/10.1093/ije/dyi174.
Chen Z, Chen J, Collins R, et al. China Kadoorie Biobank of 0.5 million people: survey methods, baseline characteristics and long-term follow-up. Int J Epidemiol. 2011;40(6):1652–66. https://doi.org/10.1093/ije/dyr120.
Li LM, Lv J, Guo Y, et al. The China Kadoorie Biobank: Related methodology and baseline characteristics of the participants. Zhonghua Liu Xing Bing Xue Za Zhi. 2012;33(3):249–55.
Wang S, Luo K. Life expectancy impacts due to heating energy utilization in China: Distribution, relations, and policy implications. Sci Total Environ. 2018;610–611:1047–56. https://doi.org/10.1016/j.scitotenv.2017.08.195.
Kessler RC, Andrews G, Mroczek D, et al. The World Health Organization Composite International Diagnostic Interview short-form (CIDI-SF). Int J of Methods Psychiatr Res. 1998;7:171–85. https://doi.org/10.1002/MPR.47.
Sun X, Zheng B, Lv J, Guo Y, Bian Z, Yang L, Chen Y, Fu Z, Guo H, Liang P, Chen Z, Chen J, Li L, Yu C, China Kadoorie Biobank (CKB) Collaborative Group. Sleep behavior and depression: findings from the China Kadoorie Biobank of 0.5 million Chinese adults. J Affect Disord. 2018;229:120–4. https://doi.org/10.1016/j.jad.2017.12.058.
Meng R, Yu C, Liu N, et al. Association of depression with all-cause and cardiovascular disease mortality among adults in China. JAMA Netw Open. 2020;3(2):e1921043. https://doi.org/10.1001/jamanetworkopen.2019.21043. Published 2020 Feb 5.
Shen G, Chen Y, Du W, et al. Exposure and size distribution of nitrated and oxygenated polycyclic aromatic hydrocarbons among the population using different household fuels. Environ Pollut. 2016;216:935–42. https://doi.org/10.1016/j.envpol.2016.07.002.
Zhang H, Zhu T, Wang S, et al. Indoor emissions of carbonaceous aerosol and other air pollutants from household fuel burning in Southwest China. Aerosol Air Qual Res. 2014;14:1779–88. https://doi.org/10.4209/aaqr.2013.10.0305.
Bhatt S, Nagappa AN, Patil CR. Role of oxidative stress in depression. Drug Discov Today. 2020;25(7):1270–6. https://doi.org/10.1016/j.drudis.2020.05.001.
Calderón-Garcidueñas L, Calderón-Garcidueñas A, Torres-Jardón R, Avila-Ramírez J, Kulesza RJ, Angiulli AD. Air pollution and your brain: what do you need to know right now. Prim Health Care Res Dev. 2015;16(4):329–45. https://doi.org/10.1017/S146342361400036X.
Hurley LL, Tizabi Y. Neuroinflammation, neurodegeneration, and depression. Neurotox Res. 2013;23(2):131–44. https://doi.org/10.1007/s12640-012-9348-1.
Ji X, Liu R, Guo J, et al. Olfactory bulb microglia activation mediated neuronal death in real-ambient particulate matter exposure mice with depression-like behaviors. Sci Total Environ. 2022;821:153456. https://doi.org/10.1016/j.scitotenv.2022.153456.
Li H, Cai J, Chen R, et al. Particulate matter exposure and stress hormone levels: a randomized, double-blind, crossover trial of air purification [published correction appears in Circulation. 2017 Sep 12;136(11):e199]. Circulation. 2017;136(7):618–27. https://doi.org/10.1161/CIRCULATIONAHA.116.026796.
Stetler C, Miller GE. Depression and hypothalamic-pituitary-adrenal activation: a quantitative summary of four decades of research. Psychosom Med. 2011;73(2):114–26. https://doi.org/10.1097/PSY.0b013e31820ad12b.
Balmes JR. Household air pollution from domestic combustion of solid fuels and health. J Allergy Clin Immunol. 2019;143(6):1979–87. https://doi.org/10.1016/j.jaci.2019.04.016.
Carnevali L, Montano N, Statello R, Sgoifo A. Rodent models of depression-cardiovascular comorbidity: bridging the known to the new. Neurosci Biobehav Rev. 2017;76(Pt A):144–53. https://doi.org/10.1016/j.neubiorev.2016.11.006.
Carvalho AF, Hyphantis T, Sales PM, et al. Major depressive disorder in breast cancer: a critical systematic review of pharmacological and psychotherapeutic clinical trials. Cancer Treat Rev. 2014;40(3):349–55. https://doi.org/10.1016/j.ctrv.2013.09.009.
Hou B, Liao H, Huang J. Household cooking fuel choice and economic poverty: Evidence from a nationwide survey in China. Energy and Buil. 2018;166:319–29. https://doi.org/10.1016/j.enbuild.2018.02.012.
Duan X, Jiang Y, Wang B, et al. Household fuel use for cooking and heating in China: results from the first Chinese Environmental Exposure-Related Human Activity Patterns Survey (CEERHAPS). Appl Energy. 2014;136:692–703. https://doi.org/10.1016/j.apenergy.2014.09.066.
Liao W, Liu X, Kang N, et al. Effect modification of kitchen ventilation on the associations of solid fuel use and long-duration cooking with the increased prevalence of depressive and anxiety symptoms: the Henan Rural Cohort Study. Indoor Air. 2022;32(3):e13016. https://doi.org/10.1111/ina.13016.
Acknowledgements
Not applicable.
Funding
This study was funded by grants from the National Key Research and Development Program of China (2016YFC0900500, 2016YFC0900501, 2016YFC0900504), the Kadoorie Charitable Foundation in Hong Kong, and Wellcome Trust (088158/Z/09/Z, 104085/Z/14/Z, 104085/Z/14/Z) in the UK.
Author information
Authors and Affiliations
Contributions
Sek Ying Chair contributed to the conceptualization of the manuscript, writing of the original draft, reviewing and editing the manuscript. Kai Chow Choi contributed to the formal analysis, data curation, writing, reviewing and editing the manuscript. Mei Sin Chong contributed to writing, reviewing and editing the manuscript. Ting Liu contributed to writing, reviewing and editing the manuscript. Wai Tong Chien contributed to writing, reviewing and editing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The CKB study was conducted in line with the principles outlined in the Declaration of Helsinki; ethics approvals were obtained from the Chinese Center for Disease Control and Prevention and the Oxford Tropical Research Ethics Committee of the University of Oxford; and an informed consent was obtained from each participant [26].
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chair, S.Y., Choi, K.C., Chong, M.S. et al. Household air pollution from solid fuel use and depression among adults in rural China: evidence from the China Kadoorie Biobank data. BMC Public Health 23, 1081 (2023). https://doi.org/10.1186/s12889-023-16038-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-16038-3