
Abstract
Background
Multicomponent physical exercise is the most recommended type of physical intervention in older adults. Experimental data suggest the relevance of the muscle-brain axis and the relationship between muscle contraction and release of brain-derived neurotrophic factor, however, the impact of this relationship on cognition remains unclear, especially in people with diagnosis of cognitive impairment. This study assesses the effect of multicomponent physical exercise on global cognition in people with mild cognitive impairment or dementia.
Methods
Randomized controlled trials published until January 2021 were searched across three electronic databases (PubMed, Scopus, and Cochrane Database). Data about exercises included in the multicomponent intervention (endurance, strength, balance, or flexibility), the inclusion of aerobic exercise, and the change in global cognition were extracted. The effect size was represented as a standardized mean difference. Risk of bias was assessed by the RoB2 tool.
Results
A total of 8 studies were included. The overall effect size suggested an effect of multicomponent exercise on global cognition. However, the subgroup analysis showed an effect only when aerobic exercise was included in the intervention. No effect when mild cognitive impairment and dementia were assessed separately was found.
Conclusion
This study suggests that multicomponent physical exercise could have an effect on global cognition in people with mild cognitive impairment or dementia only when aerobic exercise is included in the intervention. Our results support the inclusion of structured physical exercise programs in the management of people with cognitive impairment.
Similar content being viewed by others


Background
In recent decades we are living a paradox, we have experienced a steady increase in life expectancy, which has been accompanied by an increase in chronic conditions and associated with a high functional cost [1]. This functional cost not only brings health consequences, but also a huge socioeconomic impact. Few conditions exemplify this picture as cognitive impairment, a condition that affect almost fifty million people worldwide according to the latest World Health Organization (WHO) report [2]. This report highlights the importance of implementing an international plan for risk factors education, assessment and management early diagnosis, targeted treatment, caregiver assistance, and dementia-related research. Cognitive decline has been associated with an increase in the risk of functional decline, falls, need of long-term-care, care given burden, and an increase in the direct and indirect cost related with the attention, among others [3]. However, although most developed countries have designed and implemented national strategies to reduce the burden of dementia, their impact has been slightly modified [4, 5], which highlights the relevance of the implementation of any intervention that could reduce this burden.
Currently, there is not enough evidence available for disease-modifying pharmacological treatments [6], and the benefits of these treatments on cognition are limited [7, 8]. For this reason, non-pharmacological treatments to manage dementia and mild cognitive impairment (MCI) are currently a relevant research topic [9]. Research on physical activity and physical exercise, as part of non-pharmacological interventions, have been of interest not only for their effects on physical performance but also for their effects on cognitive function. Evidence provided by systematic reviews and meta-analyses suggests that physical exercise could improve global cognition in people with MCI or dementia [10,11,12]. A network meta-analysis that compared the effect of non-pharmacological interventions on cognition in people with Alzheimer´s disease or MCI, showed that physical exercise could produce a significant improvement compared with other interventions [13].
Among the effects of the different types of physical exercise on the cognition of people with cognitive impairment, some questions remain unanswered, such as the effect of multicomponent physical exercises. This type of exercise includes endurance, strength, balance, and flexibility training [14], and is the most recommended exercise for older people showing positive effects on functional decline during hospitalization [15], frailty [16], and sarcopenia [17]. From this perspective, the role of multicomponent physical exercise over cognition has aroused interest. Increase evidence suggests the existence of a muscle-brain axis that could explain the exercise-induced neuroprotection, which may be related to the improvement in mitochondrial function by exercise in skeletal muscle [18]. In addition, muscle contraction has been related to an increase in the expression of the brain-derived neurotrophic factor (BDNF) [19]. In general, physical exercise increases BDNF in neurodegenerative diseases regardless of the duration, or intensity of the intervention [20]. However, when the effect of strength exercise is assessed, no association was found [21].
The effects of multicomponent physical exercise on cognitive function, especially in people diagnosed with cognitive impairment, are still unclear. Therefore, the aim of this systematic review and meta-analysis is to estimate the effect of multicomponent physical exercise on global cognition in people with MCI or dementia.
Methods
Protocol and registration
The protocol of this systematic review was registered at the International Prospective Register of Systematic Reviews (PROSPERO), with the register identification CRD42020184660. In addition, the protocol was approved by the Ethics Committee of the Pontificia Universidad Javeriana and the Hospital Universitario San Ignacio.
Search strategy
A search was performed on MEDLINE (via PubMed), Scopus, and Cochrane Database up to January 2021. The search was aimed to identify published randomized controlled trials assessing the effect of multicomponent physical exercise on global cognition in people with dementia and MCI. Global cognition was considered the outcome because it is the best measurement of the cognitive function in patients with dementia and MCI and is the most common way to assess cognition in the included randomized controlled trials. We examined the reference list of eligible studies to expand the search. The complete MEDLINE search strategy is displayed in Supplementary material (Supplementary Table S1). The search was performed to identify any type of physical exercise that could be part of the multicomponent intervention according with the definition proposed by Cress et al [14]. Additionally, different types of cognitive impairment were included in the search strategy to try of encompass most of the etiologies.
Inclusion criteria
The studies included in this systematic review met the following inclusion criteria: (i) Participants: adult participants with dementia or MCI secondary to either. (ii) Intervention: multicomponent physical exercise defined as an exercise program including endurance, strength, balance, or flexibility [14]. We included studies developing any intervention program that included at least two of the above-mentioned exercises without other intervention (e.g., cognitive interventions), and regardless of the inclusion of aerobic exercise as part of the intervention. (iii) Outcome: global cognition measured by any validate neuropsychological test. (iv) Control: any control was accepted except those with a physical activity component. If the control intervention included a component of cognitive training or stimulation, both total and partially, the RCT was included in the analysis. (v) Type of study: randomized controlled trials. We only included in this review studies in English and Spanish. No exclusion criteria were considered.
Study identification and data extraction
After defining the search strategy, all records were imported into the reference management system (Mendeley, desktop version 1.19.4) to exclude duplicate records. Two authors (LVS and CAB) independently performed the search literature and data extraction, with the intervention of a third author in case of disagreement (ICR). The following data were extracted from the selected studies using an ad-hoc form: author, publication year, country, sample size, losses, female proportion, mean age in control and intervention group, type of cognitive impairment, types of physical exercises included in the intervention, length of the intervention (weeks), number of sessions per week, duration per session (minutes), type of control group, the intensity of the multicomponent exercise (as reported by each study), cognitive assessment tool and effect on global cognition.
Risk of bias
The risk of bias was assessed independently by two authors using the revised Cochrane risk-of-bias tool for randomized trials (RoB2) [22]. The RoB2 included assessment of six domains: randomization process, derivation for intended interventions, missing outcome data, measurement of the outcome, selection of the reported results, and overall results. Each domain was rated as low, moderate, and high risk of bias. To report on the risk of bias, a graphical representation was used.
Data analysis
The effect size (ES) and 95% confidence intervals (CIs) for the effect of physical exercise programs on global cognition were calculated using the Cohen’s d index. A pooled ES was estimated using a random-effects model based on the Der Simonian and Laird method [23]. We consider the ES classified as proposed by Cohen et al. [24]; small effect (0.2), moderate effect (0.5), and large effect (0.8). Inconsistence across studies was assessed using the I2 statistic [25], whose values were considered as follows: not important (0%–40%), moderate (30–60%), substantial (50–90%), and considerable (75–100%). Moreover, the corresponding p value were also considered. To determine the size and clinical relevance of heterogeneity, τ2 statistic was calculated and interpreted as low when τ2 was lower than 0.04, moderate when was from 0.04 to 0.14 and as substantial when it was from 0.14 to 0.40 [26]. In case of high heterogeneity, two subgroup analyses were developed: i) by type of cognitive impairment, distinguishing between patients with MCI and dementia, and ii) by the inclusion of aerobic exercise in the intervention. When global cognition was measured using more than one scale, a pooled ES was calculated. To define the effect of individual studies in the overall effect size a sensitive analysis was performed.
The small study effect was graphically assessed using a funnel plot, additionally, the Egger test was estimated. Finally, the trim-and-fill analysis was used to estimate the number of studies needed to remove publication bias, and to estimate the ES without publication bias. Stata/IC software, version 16.1 for Windows was used for statistical analysis.
Results
Study identification
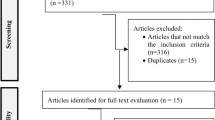
A total of 2789 records were found following the search strategy. After removing duplicates, and reviewing the title and abstract, 31 relevant papers were chosen for full reading. Finally, only 8 articles met the inclusion criteria (Fig. 1). The excluded articles and the reasons for exclusion are reported in the Supplementary Table S2.

Flow diagram for searching and selection of the included studies
Characteristics of included studies
Eight studies assessing the effect of multicomponent physical exercise on global cognition in people with dementia and MCI [27,28,29,30,31,32,33,34] were included in the review. The studies included 367 participants from seven countries: France [29, 31], Spain [27], Brazil [28], Croatia [30], Korea [32], United States [33], and Japan [34]. The mean age was between 77.7 and 77.9 years in the intervention and control group, respectively, and women accounted for 70.3%. Five studies [28, 29, 31,32,33] included only participants with dementia and three with MCI [27, 30, 34].
Regarding multicomponent physical exercise interventions, all studies included at least two types of exercise considered in the definition of multicomponent physical exercise [14]. All studies included balance exercises, four included flexibility exercises [27, 31,32,33] and one did not include strength training [31]. Aerobic exercise was part of the intervention in six studies [27, 29, 31,32,33,34]. The intensity of physical activity was considered low to moderate in three papers [27, 31, 34], moderate in two [29, 33], and low in one [32], additionally, two studies did not report on exercise intensity [28, 30]. The length of the intervention programs was 8 to 52 weeks, including 1 to 7 sessions per week, and 30 to 90 min per session.
The Mini-Mental State Examination [27,28,29, 32, 34] was the most widely used cognitive measurement tool, other tools included were Montreal Cognitive Assessment (MoCA) [30], Brief Cognitive Screening Battery (BCSB) [28], Rapid Evaluation of Cognitive Function (ERFC) [31], Boston Naming Test (BNT) [33], Hopkins Verbal Learning Test (HVLT) [33], and Alzheimer’s Disease Assessment Scale-Cognitive (ADAS-Cog) [34]. Table 1 summarizes the studies included in the review.
Risk of bias
The risk of bias was assessed using the revised Cochrane risk-of-bias tool for randomized trials (RoB2) [22]. Depending on the intervention effect of interest, the studies were divided into intention-to-treat effect [29, 30, 32,33,34] or per-protocol effect [27, 28, 31]. Overall bias was reported as low risk in 20% of studies with an intention-to-treat analysis and 33.3% in those with a per-protocol approach. Supplementary Figure S1.
Effect of physical activity on global cognition, subgroup analysis and sensitive analysis
The ES of multicomponent physical exercise on global cognition in MCI and dementia was 0.34 (95% IC: 0.08, 0.60). We found a moderate inconsistence (I2 = 41.21%). Between-trials heterogeneity was considered moderate (τ2 = 0.06).
For the subgroup analysis considering the type of cognitive impairment, the pooled ES was 0.34 (95% CI: -0.05, 0.74; I2 = 57.59%) for dementia and 0.34 (95% CI: 0.00, 0.69; I2 = 15.52%) for MCI. For the subgroup analysis by the inclusion of aerobic exercises in the exercises protocol, the ES was 0.32 (95% CI: 0.03, 0.61; I2 = 44.78%) for those multicomponent physical exercise including aerobic exercise and 0.44 (95% CI: -0.38, 1.25; I2 = 62.39%) for those not including aerobic exercise, respectively (Figs. 2 and 3).

Subgroup analysis by the type of cognitive impairment

Subgroup analysis of the inclusion or not of aerobic exercise
When sensitivity analysis was performed the two studies which omission showed a higher impact on the overall effect size were de Souto Barreto et al. (ES: 0.4; 95% CI: 0.11–0.7) and Kwak et al. (ES: 0.25; 95% CI: 0.02–0.48). Omitting the study of Kemoun et al., the only study that did not include strength exercises in the intervention, the effect size was 0.27 (95% CI: 0.02–0.52). (Fig. 4).

Sensitivity analysis
Small study effects
After visual inspection of the funnel plot and considering the Eger test, we found small study effects for the effect of multicomponent physical exercise on global cognition in MCI and dementia (p = 0.009). The trim-and-fill analysis showed that only one study was needed to remove the small study effects and that the ES of observed and imputed studies would be 0.274 (95% CI: -0.01, 0.56) (Supplementary Figure S2).
Discussion
This systematic review and meta-analysis provides evidence supporting the effectiveness of multicomponent physical exercise associated with aerobic exercise on global cognition in people with MCI or dementia. Furthermore, this meta-analysis shows that when exercises protocol did not include aerobic exercise this effect disappeared. Also, we did not find an effect when MCI and dementia were separately analyzed.
Our data suggest that multicomponent physical activity plus aerobic exercise produces positive effects on global cognition in patients with MCI and dementia. However, only two studies did not include aerobic exercise as part of the intervention and presented a high heterogeneity between them. Currently, multicomponent physical exercise is the one most frequently recommended for high-prevalent conditions in older adults such as frailty [35]. Although the relationship between this type of exercise and cognitive functions is unclear, the effectiveness of physical exercise in reducing frailty and improving cognition, emotions, and social networks has been reported among frail older adults [16], using multicomponent exercise and including aerobic exercise. This fact makes difficult to isolate the effect of the multicomponent exercise intervention approach, whose evidence on cognition remains inconclusive [36], as well as the most suitable combination of components, duration and dose [37]. Nevertheless and considering that physical activity is part of the intervention of the vast majority of conditions that affect older people, the inclusion of an individualized physical exercise in the management of the older patients should be part of the daily clinical practice [38].
The inclusion of aerobic exercise within the multicomponent physical exercise programs seems to be of importance in positively impacting cognitive function. The positive effect of aerobic exercise has been reported among cognitively healthy individuals [39], and appears to be stronger as age increases, suggesting a protective effect against age-related cognitive decline. Additionally, aerobic exercise has demonstrated to positively impact on the cognitive function, behavior, and mobility [40] of patients with dementia and the global cognitive ability of older adults with MCI [10], although some individual domains are not significantly improved (i.e. attention, verbal fluency, and visuospatial domains).
Some mechanisms have been proposed to explain the effects of multicomponent physical exercise on cognitive function. The association between multicomponent physical exercise (a composite strength and balance training program associated with a walking recommendation) and brain-derived neurotrophic factor (BDNF), a factor that promotes the growth and differentiation of neurons and supports the survival of existing neurons, was previously explored. It seems that blood levels of BDNF are not affected by the multicomponent physical exercise intervention [41]. This result is consistent with animal models in which strength exercise reduces aerobic exercise-induced adult hippocampal neurogenesis due to reduced BDNF and β-hydroxybutyrate [42], and with a study in young male participants that showed no effect of acute strength exercise on plasma levels of BDNF [43]. Similarly, a meta-analysis that assessed the effect of physical activity on BDNF did not find the effect of strength exercises on BDNF levels [21]. These results suggest that the multicomponent physical exercise, or at least the strength exercises, could have no effect on the neurogenesis processes mediated by BDNF. However, the BDNF is not the only cytokine with a role in the neurogenesis and neuroplasticity process. Ciliary neurotrophic factor (CNTF), leukaemia inhibitory factor (LIF), vascular endothelial growth factor (VEGF) family, and insulin-like growth factor I (IGF-I) are some cytokines that have been related to neuronal plasticity [44]. IGF-I level is related to neurotransmission, neuronal plasticity and neurotrophic potential, and the declined serum levels have been associated with age-related cognitive decline [45]. In addition, healthy levels of IGF-I are associated with an increase in hippocampal mass and verbal recall[44]. Related to physical activity, a contraction-induced muscle release of IGF-I has been shown, independently of the levels of Growth Hormone [46]. Moreover, muscle contraction and physical exercise have a relation to an improvement in mitochondrial function, that is related to a neuroprotective role through both brain plasticity and angio-neurogenesis ways [18]. Finally, resistance training showed a positive effect on spatial memory in animal models, although it has not an effect on the reduction in oxidative parameter levels [47]. This evidence suggests that the impact of multicomponent physical exercise in cognition implies different paths and supports the existence of a complex muscle-brain axis.
This study shows the importance of included a physical exercise intervention in the management of patients with cognitive decline including both aerobic and multicomponent exercise (i.e., endurance, strength, balance, or flexibility exercises), independently of the stage of cognitive impairment. As far as we know, this is the first systematic review and meta-analysis that explores the effect of multicomponent physical exercise intervention on cognition in patients with MCI and dementia, using the accepted definition of multicomponent physical exercise in the inclusion criteria. However, our study has some limitations. First, no information on independent cognitive domains was found, so only data on global cognition was reported. Second, few primary studies were found with a small sample size and therefore small study effects was found in the analysis. Third, only two studies did not include aerobic exercise as part of the intervention and presented a high heterogeneity between them. Finally, only published papers in English and Spanish were included, so no information on other languages was included.
Conclusion
This systematic review and meta-analysis suggests a positive effect of the multicomponent physical exercises on global cognition in people with MCI or dementia specially when aerobic exercise was included in the exercise protocol. However, due to the limitations of the included studies, these findings should be cautiously interpreted. Well-designed clinical trials comparing aerobic exercise to multicomponent exercise should be conducted to clarify the true effect on cognition. However, our results support the needed to include physical exercise in the cognitive rehabilitation protocols and cognitive impairment therapies.
Availability of data and materials
The datasets generated and/or analysed during the current study are available in file data_set_srma.dta of the repository bmc_g-data-set (https://github.com/lcvenegas/bmc_g-data-set).
References
Lee R, Mason A. Cost of Aging. Finance Dev. 2017;54(1):7–9 http://www.ncbi.nlm.nih.gov/pubmed/28835725.
WHO. Towards a Dementia Plan: A WHO Guide.; 2018. https://apps.who.int/iris/bitstream/handle/10665/272642/9789241514132-eng.pdf?ua=1 Accessed 18 Mar 2019.
Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020;396(10248):413–46. https://doi.org/10.1016/S0140-6736(20)30367-6.
Burns A, Robert P. Dementia care: International perspectives. Curr Opin Psychiatry. 2019;32(4):361–5. https://doi.org/10.1097/YCO.0000000000000511.
The Lancet Neurology. Response to the growing dementia burden must be faster. Lancet Neurol. 2018;17(8):651. https://doi.org/10.1016/S1474-4422(18)30256-4.
Tisher A, Salardini A. A Comprehensive Update on Treatment of Dementia. Semin Neurol. 2019;39(2):167–78. https://doi.org/10.1055/s-0039-1683408.
Sharma K. Cholinesterase inhibitors as Alzheimer’s therapeutics (Review). Mol Med Rep. 2019;20(2):1479–87. https://doi.org/10.3892/mmr.2019.10374.
Birks JS, Harvey RJ. Donepezil for dementia due to Alzheimer’s disease. Cochrane Database Syst Rev. 2018;2018(6). doi:https://doi.org/10.1002/14651858.CD001190.pub3
Shah H, Albanese E, Duggan C, et al. Research priorities to reduce the global burden of dementia by 2025. Lancet Neurol. 2016;15(12):1285–94. https://doi.org/10.1016/S1474-4422(16)30235-6.
Zheng G, Xia R, Zhou W, Tao J, Chen L. Aerobic exercise ameliorates cognitive function in older adults with mild cognitive impairment: a systematic review and meta-analysis of randomised controlled trials. Br J Sports Med. 2016;50(23):1443–50. https://doi.org/10.1136/bjsports-2015-095699.
Du Z, Li Y, Li J, Zhou C, Li F, Yang X. Physical activity can improve cognition in patients with Alzheimer’s disease: a systematic review and meta-analysis of randomized controlled trials. Clin Interv Aging. 2018;13:1593–603. https://doi.org/10.2147/CIA.S169565.
Song D, Yu DSF, Li PWC, Lei Y. The effectiveness of physical exercise on cognitive and psychological outcomes in individuals with mild cognitive impairment: a systematic review and meta-analysis. Int J Nurs Stud. 2018;79:155–64. https://doi.org/10.1016/j.ijnurstu.2018.01.002.
Liang J-H, Xu Y, Lin L, Jia R-X, Zhang H-B, Hang L. Comparison of multiple interventions for older adults with Alzheimer disease or mild cognitive impairment: a PRISMA-compliant network meta-analysis. Medicine (Baltimore). 2018;97(20): e10744. https://doi.org/10.1097/MD.0000000000010744.
Cress ME, Buchner DM, Prohaska T, et al. Best practices for physical activity programs and behavior counseling in older adult populations. Eur Rev Aging Phys Act. 2006;3(1):34–42. https://doi.org/10.1007/s11556-006-0003-9.
Izquierdo M, Martínez-Velilla N, Casas-Herrero A, et al. Effect of exercise intervention on functional decline in very elderly patients during acute hospitalization: a randomized clinical trial. JAMA Intern Med. 2019;179(1):28–36. https://doi.org/10.1001/jamainternmed.2018.4869.
Tarazona-Santabalbina FJ, Gómez-Cabrera MC, Pérez-Ros P, et al. A multicomponent exercise intervention that reverses frailty and improves cognition, emotion, and social networking in the community-dwelling frail elderly: a randomized clinical trial. J Am Med Dir Assoc. 2016;17(5):426–33. https://doi.org/10.1016/j.jamda.2016.01.019.
Phu S, Boersma D, Duque G. Exercise and SARCOPENIA. J Clin Densitom. 2015;18(4):488–92. https://doi.org/10.1016/j.jocd.2015.04.011.
Burtscher J, Millet GP, Place N, Kayser B, Zanou N. The Muscle-Brain Axis and Neurodegenerative Diseases: The Key Role of Mitochondria in Exercise-Induced Neuroprotection. Int J Mol Sci. 2021;22(12). doi:https://doi.org/10.3390/IJMS22126479
Wang R, Holsinger RMD. Exercise-induced brain-derived neurotrophic factor expression: therapeutic implications for Alzheimer’s dementia. Ageing Res Rev. 2018;48:109–21. https://doi.org/10.1016/j.arr.2018.10.002.
Ruiz-González D, Hernández-Martínez A, Valenzuela PL, Morales JS, Soriano-Maldonado A. Effects of physical exercise on plasma brain-derived neurotrophic factor in neurodegenerative disorders: a systematic review and meta-analysis of randomized controlled trials. Neurosci Biobehav Rev. 2021;128:394–405. https://doi.org/10.1016/j.neubiorev.2021.05.025.
Szuhany KL, Bugatti M, Otto MW. A meta-analytic review of the effects of exercise on brain-derived neurotrophic factor. J Psychiatr Res. 2015;2015(60):56–64. https://doi.org/10.1016/j.jpsychires.2014.10.003.
Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:1–8. https://doi.org/10.1136/bmj.l4898.
DerSimonian R, Laird N. Meta-analysis in clinical trials revisited. Contemp Clin Trials. 2015;45(Pt A):139–45. https://doi.org/10.1016/j.cct.2015.09.002.
Cohen J. Statistical Power Analysis for the Behavioral Sciences. Second: Lawrence Erlbaum Associates; 1988.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. Br Med J. 2003;327(7414):557–60. https://doi.org/10.1136/bmj.327.7414.557.
Stettler C, Allemann S, Wandel S, et al. Drug eluting and bare metal stents in people with and without diabetes: collaborative network meta-analysis. BMJ. 2008;337. doi:https://doi.org/10.1136/bmj.a1331
Bisbe M, Fuente-Vidal A, López E, et al. comparative cognitive effects of choreographed exercise and multimodal physical therapy in older adults with amnestic mild cognitive impairment: randomized clinical trial. J Alzheimers Dis. 2020;73(2):769–83. https://doi.org/10.3233/JAD-190552.
Christofoletti G, Oliani MM, Gobbi S, Stella F, Bucken Gobbi LT, Renato CP. A controlled clinical trial on the effects of motor intervention on balance and cognition in institutionalized elderly patients with dementia. Clin Rehabil. 2008;22(7):618–26. https://doi.org/10.1177/0269215507086239.
de Souto BP, Cesari M, Denormandie P, Armaingaud D, Vellas B, Rolland Y. Exercise or social intervention for nursing home residents with dementia: a pilot randomized. Controlled Trial J Am Geriatr Soc. 2017;65(9):E123–9. https://doi.org/10.1111/jgs.14947.
Greblo Jurakic Z, Krizanic V, Sarabon N, Markovic G. Effects of feedback-based balance and core resistance training vs. Pilates training on cognitive functions in older women with mild cognitive impairment: a pilot randomized controlled trial. Aging Clin Exp Res. 2017;29(6):1295–8. https://doi.org/10.1007/s40520-017-0740-9.
Kemoun G, Thibaud M, Roumagne N, et al. Effects of a physical training programme on cognitive function and walking efficiency in elderly persons with dementia. Dement Geriatr Cogn Disord. 2010;29(2):109–14. https://doi.org/10.1159/000272435.
Kwak Y-S, Um S-Y, Son T-G, Kim D-J. Effect of regular exercise on senile dementia patients. Int J Sports Med. 2008;29(6):471–4. https://doi.org/10.1055/s-2007-964853.
Steinberg M, Leoutsakos J-MS, Lyketsos CG. Evaluation of a home-based exercise program in the treatment of Alzheimer’s disease: the Maximizing Independence in Dementia (MIND) study. Int J Geriatr Psychiatry. 2009;24(7):680–5. https://doi.org/10.1002/gps.2175.
Suzuki T, Shimada H, Makizako H, et al. A Randomized Controlled Trial of Multicomponent Exercise in Older Adults with Mild Cognitive Impairment. Aleman A, ed. PLoS One. 2013;8(4):e61483. doi:https://doi.org/10.1371/journal.pone.0061483
Dent E, Morley JE, Cruz-Jentoft AJ, et al. Physical frailty: ICFSR international clinical practice guidelines for identification and management. J Nutr Heal Aging. 2019;23(9):771–87. https://doi.org/10.1007/s12603-019-1273-z.
de Oliveira Gonçalves I, Bandeira AN, Coelho-Júnior HJ, et al. Multicomponent exercise on physical function, cognition and hemodynamic parameters of community-dwelling older adults: a quasi-experimental study. Int J Environ Res Public Health. 2019;16(12):2184. https://doi.org/10.3390/ijerph16122184.
Venegas-Sanabria LC, Martínez-Vizcaino V, Cavero-Redondo I, Chavarro-Carvajal DA, Cano-Gutierrez CA, Álvarez-Bueno C. Effect of physical activity on cognitive domains in dementia and mild cognitive impairment: overview of systematic reviews and meta-analyses. Aging Ment Heal. 2020;0(0):1–9. https://doi.org/10.1080/13607863.2020.1839862.
Izquierdo M, Duque G, Morley JE. Physical activity guidelines for older people: knowledge gaps and future directions. Lancet Heal Longev. 2021;2(6):e380–3. https://doi.org/10.1016/S2666-7568(21)00079-9.
Stern Y, Mackay-Brandt A, Lee S, et al. Effect of aerobic exercise on cognition in younger adults: a randomized clinical trial. Neurology. 2019;92(9):E905–16. https://doi.org/10.1212/WNL.0000000000007003.
Cancela JM, Ayán C, Varela S, Seijo M. Effects of a long-term aerobic exercise intervention on institutionalized patients with dementia. J Sci Med Sport. 2016;19(4):293–8. https://doi.org/10.1016/j.jsams.2015.05.007.
Arrieta H, Rezola-Pardo C, Kortajarena M, et al. The impact of physical exercise on cognitive and affective functions and serum levels of brain-derived neurotrophic factor in nursing home residents: a randomized controlled trial. Maturitas. 2020;131:72–7. https://doi.org/10.1016/j.maturitas.2019.10.014.
Lan Y, Huang Z, Jiang Y, et al. Strength exercise weakens aerobic exerciseinduced cognitive improvements in rats. PLoS One. 2018;13(10). doi:https://doi.org/10.1371/journal.pone.0205562
Correia PR, Pansani A, MacHado F, et al. Acute strength exercise and the involvement of small or large muscle mass on plasma brain-derived neurotrophic factor levels. Clinics. 2010;65(11):1123–6. https://doi.org/10.1590/S1807-59322010001100012.
Duzel E, Van Praag H, Sendtner M. Can physical exercise in old age improve memory and hippocampal function? Brain. 2016;139(3):662–73. https://doi.org/10.1093/BRAIN/AWV407.
Aleman A, Torres-Alemán I. Circulating insulin-like growth factor I and cognitive function: neuromodulation throughout the lifespan. Prog Neurobiol. 2009;89(3):256–65. https://doi.org/10.1016/J.PNEUROBIO.2009.07.008.
Berg U, Bang P. Exercise and circulating insulin-like growth factor I. Horm Res Paediatr. 2004;62(Suppl. 1):50–8. https://doi.org/10.1159/000080759.
Feter N, Spanevello RM, Soares MSP, et al. How does physical activity and different models of exercise training affect oxidative parameters and memory? Physiol Behav. 2019;201:42–52. https://doi.org/10.1016/j.physbeh.2018.12.002.
Acknowledgements
Not applicable
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
LCV, CAB, and ICR designed the protocol, defined the search terms, extracted data, and assessed the risk of bias. LCV and CAB analyzed the data extracted. LCV, CAB, and ICR wrote the manuscript. CCG revised the manuscript. VMV revised and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This systematic review was approved by the Ethics and Research Comite at Pontificia Universidad Javeriana.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Table S1.
PubMed search strategy until January 2021. Analogous search strategies were used for Scopus, and Cochrane Database. Supplementary Table S2. Articles excluded. Supplementary Figure S1. Risk of bias using the Cochrane Collaboration´s tool for assessment of risk of bias (RoB2): A. Intention-to-treat effect; B. Per-protocol effect. Supplementary Figure S2. Publication bias.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Venegas-Sanabria, L.C., Cavero-Redondo, I., Martínez-Vizcaino, V. et al. Effect of multicomponent exercise in cognitive impairment: a systematic review and meta-analysis. BMC Geriatr 22, 617 (2022). https://doi.org/10.1186/s12877-022-03302-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-022-03302-1