
Abstract
Background
Improvements in the use of polypharmacy or potentially inappropriate medication (PIM) may reduce medication costs in Japan. We aimed to evaluate the impact of improvement in prescription on both overall health outcomes and medication costs in Japanese facilities for older people.
Methods
Residents in Japanese facilities for older people between March 2019 and March 2020 were included in this study. The following five indices were used to evaluate overall health outcomes: EuroQoL-5D-5L, Barthel Index, Mini Mental State Examination, Dementia Behaviour Disturbance Scale, and Vitality Index. The team, which consisted of one physician and several pharmacists, suggested improved prescriptions for the attending physicians of the participants. The impact of improvement in prescriptions on the health outcomes score, medication costs, and the number of medications were evaluated through two comparison groups: those whose number of medications decreased (decrement group, DG) and those whose medications did not (not decrement group, NDG); those prescribed PIMs in March 2019 and those not prescribed PIMs in March 2020 (improvement group, IG) and those prescribed PIMs both in March 2019 and March 2020 (not improvement group, NIG). In both comparison groups, propensity score matching was performed to balance demographics, and all health outcome scores, medication costs, and the number of medications in March 2020 were assessed using a t-test. Statistical significance was set at a p-value of < 0.05.
Results
Eight-hundred-and-ninety-one participants (75.5% women, 86.2 ± 7.9 years old) were enrolled. After matching, in the comparison between the DG (N = 232, 77.2%, 85.7 ± 8.5) and NDG (N = 232, 78.5%, 86.0 ± 3.1), changes in the health outcomes score were nonsignificant. However, the medication costs and the number of medications significantly decreased. After matching, in the comparison between IG (N = 141, 75.2%, 86.7 ± 8.1) and NIG (N = 273, 74.2%, 86.2 ± 8.3), changes in health outcome scores and medication costs were not significant. However, the number of medications significantly decreased.
Conclusions
Improvements in prescriptions did not adversely affect the overall health outcomes. However, it impacted medication costs and the number of medications. Improvement in prescriptions could decrease medication costs while maintaining overall health outcomes.
Similar content being viewed by others


Background
Polypharmacy and potentially inappropriate medication (PIM), which is induced by polypharmacy, are crucial issues for older people worldwide [1]. Polypharmacy is defined as the use of multiple drugs simultaneously and is often defined as the use of five or more drugs in combination per day [2]. PIM is a medication that has a higher risk than its anticipated benefits [3, 4]. In 2016, there were 14 different criteria for PIMs, such as the Beers criteria and the STOPP/START criteria, and 729 different medications/classes reported in all criteria. Most criteria for PIMs include the usage of benzodiazepines, NSAIDs, antihistamines and antipsychotics for older people [5]. Several studies reported that the use of polypharmacy or PIMs increased the risk of adverse events and hospitalization [6,7,8]. Older people often use polypharmacy or PIMs because they often suffer from a combination of diseases and have multiple physiological dysfunctions. Systematic reviews regarding the use of PIMs have reported that approximately 11.5–62.5% of older people used PIMs [9, 10].
The use of polypharmacy and PIMs are serious issues in Japan, one of the most aging societies in the world. The proportion of people aged 65 years or older is 28.7%in March 2020 and this is estimated to reach 30.0% by 2025 [11,12,13]. With rapid ageing, national medical care expenditure in Japan is increasing, and as of 2018, it was Japanese yen (JPY) 43.4 trillion, which is estimated to reach JYP 66.7–68.5 trillion in 2040 [14, 15]. Increasing the number of prescriptions or the number of days per prescription was one of the causes for the increase in national medical care expenditures [16]. Based on the data reported by Suzuki et al., 33.2% of people over 65 years in Japan are prescribed five or more medicines, and 22.9% are using PIMs [17]. Therefore, it is expected that improving the use of polypharmacy or PIMs will lead to a reduction in national medical care expenditures.
However, the value of appropriate use of medication should not only be considered in terms of costs. The fundamental concept of the cost-effectiveness of health care interventions is that both costs and health outcomes should be simultaneously analysed [18, 19].
A few studies on polypharmacy or PIMs have been conducted in Japan, and almost all of them take only single components, health outcomes or costs, into account. A study using the data of hospitalized older patients showed that people prescribed six or more medications were at a higher risk of adverse events than those who were prescribed five or fewer medications [20]. A study has been conducted in Japan to evaluate the impact of improving the appropriate use of polypharmacy or PIMs on quality of life (QoL) and activities of daily living (ADL) [21]. Previous studies also reported that medication costs decreased with improvements in prescriptions, and the amount was JPY 65.6–170.4 per day [22, 23].
The purpose of this study was to simultaneously evaluate the impacts of improvement in prescriptions on both overall health outcomes and medication costs and to ensure that this improvement would lead to decreased medication costs while maintaining overall health outcomes.
Methods
Study design
This was a prospective observational study. Participants enrolled in this study were admitted to nursing homes or residential facilities with health and caregiving services for older people under Life Company Limited, Tokyo, Japan, between March 2019 and March 2020 (47 facilities, N = 3461). A team of one physician and several pharmacists cooperating with Life Company Limited proposed optimized prescriptions for each resident to attending physicians. This proposal project had already started in June 2018 in one facility, and it expanded every 3 months to other facilities in sequence. This proposal was supervised by the author YT who is one of the co-authors of this paper and participated in developing the guidelines for the appropriate use of medications for older people [24].
The prescriptions that residents received were collected, and surveys were conducted in March 2019 and March 2020. Using their prescriptions, daily costs of medications and the number of medications were estimated. The price of each medication was derived from the “National drug tariff in Japan 2020” [25]. Overall health outcomes were assessed in March 2019 and March 2020 by staff working at the facilities using the following five measurements: EuroQoL-5D-5L-proxy (EQ-5D-5L), Barthel Index (BI), Mini-Mental State Examination (MMSE), Dementia Behaviour Disturbance Scale (DBD), and Vitality Index (VI). Demographics of participants, such as age and sex, were derived from the database managed by Life Company Limited.
All residents in the facilities whose informed consent was obtained participated in this study, and participants whose demographic data (age, sex, five health outcome indices and prescription) was obtained in March 2019 and whose data were still available 1 year later were included in the analysis.
Questionnaires
EuroQoL-5D-5L-proxy (EQ-5D-5L)
The EQ-5D-5L was used to evaluate health-related QoL. This consisted of the following five dimensions: “Mobility,” “Self-Care,” “Usual Activities,” “Pain/Discomfort,” and “Anxiety/Depression.” Answers for each dimension were merged and converted to the QoL score, in which 0.0 indicated death and 1.0 indicated perfect health. Negative QoL scores (below 0) were assigned to extremely bad health status [26, 27]. The Japanese tariff was used for the conversion from original answers to QoL scores [28].
Barthel index (BI)
BI was used to assess the ADL. Using BI, ADL were measured on a scale of 0 to 100, with higher scores indicating greater independence from physical assistance [29]. A score of 60 appeared to be a pivotal score where patients transitioned from dependency to assisted independence, and for those with a Barthel score below 40, it was found that none had independent mobility skills, and fewer than 50% were independent in very basic skills, such as feeding, grooming, and sphincter control [30].
Mini-mental state examination (MMSE)
The MMSE is one of the most popular questionnaires used to measure cognitive function [31]. It was also used to assess the severity of dementia. The maximum score that could be achieved in the MMSE was 30. By using the MMSE, patients with MMSE scores of 21–23, 11–20, and 0–10 were classified as suffering from mild, moderate, and severe Alzheimer’s disease, respectively [32, 33].
Dementia behaviour disturbance scale (DBD)
Behavioural disturbance is a common and distinctive feature of dementia. DBD was used to assess the severity of behavioural disturbance, and the severity of behavioural disturbance was measured on a scale of 0 to 112, with increases in DBD scores indicating more severe behavioural disturbance [34]. There were two types of DBD: one consisted of 28 questions, and the other consisted of 13 questions [35]. The former was used in this study.
Vitality index (VI)
VI was developed to measure vitality related to ADL in older patients with dementia. Using VI, vitality was measured on a scale of 0 to 10, with higher scores indicating more vitality related to ADL [36].
Comparisons
The following three comparisons were conducted in this study to compare health outcome scores (EQ-5D-5L, BI, MMSE, DBD, and VI), daily costs of medications, and the number of medications.
Comparison in terms of the facilities where suggestions for improving prescriptions were conducted
Participants were classified into two groups according to the timing of when proposals for improving prescriptions were started at the facilities they resided in. Those who were in facilities where the proposals were implemented by the end of March 2020 (31 facilities) were categorized into the implemented facilities group (IFG), and the rest were categorized into the not implemented facilities group (NIFG). It should be noted that this classification was based on facilities, not based on whether participants underwent a decrease in medications.
Comparison in terms of the number of decreased prescribed medications
Participants whose number of prescribed medications in March 2020 decreased compared to that in March 2019 were categorized into the decreased group (DG). Residents who had increased or no change in the number of prescribed medications were categorized into the not decreased group (NDG).
Comparison in terms of the improvement in the use of PIMs
According to the “Guidelines for medical treatment and its safety in older people 2015,” PIMs were referred to as cautiously administered medications being prescribed to older people with a high risk of adverse events [37]. Participants who were prescribed PIMs in March 2019 and not prescribed it in March 2020 were categorized into the improvement group (IG), and those who were prescribed PIMs both in March 2019 and March 2020 were categorized into the not improvement group (NIG).
Data analyses
To neglect the effects of extraordinarily high-priced anticancer drugs on the daily costs of medication, participants whose daily cost of medication was over ten thousand JPY were omitted as outliers. Fixed ratio propensity score matching was conducted in March 2019 to balance demographics such as age, sex, health outcomes score, daily costs of medications, and the number of medications [38, 39]. After matching, the health outcomes score, daily costs of medications, and the number of medications in March 2020 were assessed using a t-test [40]. Statistical significance was set at p-value < 0.05, and all analyses were performed using Python version 3.7.7.
Results
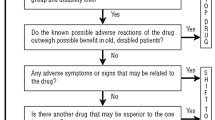
Both questionnaires and prescriptions were collected from 1260 participants in March 2019. Out of the 1260 participants, 891 participants (75.5% women, 86.2 ± 7.9 years old) who were still available 1 year later were included in the analysis. Other demographics, such as types of nursing care level, medications received, health outcomes score, daily costs of medications, and the number of medications, are shown in Table 1. The proportion of participants whose medications were reduced increased by 13.3 pts. (IFG: 47.1%, NIFG: 33.8%), and that of participants who stopped using PIMs increased by 15.7 pts. (IFG: 34.4%, NIFG: 18.7%) (Figs. 1 and 2). Decreased medications in the prescriptions in the DG group included magnesium oxide, rebamipide, and amlodipine besylate, while those in the IG group were magnesium oxide, furosemide, and spironolactone (Tables 2 and 3).

Distribution of the participants with a decrease in the number of medications. IFG (implemented facilities group), participants who were in facilities where proposals for improving inappropriate prescriptions were implemented by the end of March 2020 were classified into this group. NIFG (not implemented facilities group), participants who were not in facilities where proposals for improving inappropriate prescriptions were implemented by the end of March 2020 were classified into this group. *The number of people and their proportion are written in squares. **Summation of the number of people in the figure is not consistent with 889, which was the target population for analysis because there were participants with missing data in March 2020

Distribution of participants with an improvement in the use of PIMs. IFG (implemented facilities group), participants who were in facilities where proposals for improving inappropriate prescriptions were implemented by the end of March 2020 were classified into this group. NIFG (not implemented facilities group), participants who were not in facilities where proposals for improving inappropriate prescriptions were implemented by the end of March 2020 were classified into this group. *The number of people and their proportion are written in squares. **Summation of the number of people in the figure is not consistent with 889, which was the target population for analysis. This was because a few participants did not use PIMs or there were participants with missing data in March 2020
Comparison in terms of the facilities where suggestions for improving prescriptions were conducted (IFG vs. NIFG)
Before matching, the number of participants in the IFG was 604 and that in the NIFG was 273. After 1:2 matching, the number of participants in each group was 459 and 234, respectively. The demographics of each group are shown in Table 4. There were no significant changes in any health outcome score, daily costs of medications or the number of medications (Table 5).
Comparison in terms of the decrease in the number of medications (DG vs. NDG)
Before matching, the number of participants in the DG was 321 and that in the NDG was 416. After 1:1 matching, the numbers of participants in each group were 232 and 232, respectively. The demographics of each group are shown in Table 6. There were no statistically meaningful changes in health outcomes. However, the changes in the number of medications and the daily costs were statistically significant. The mean values of the number of medications for DG and NDG were 5.0 and 9.1, respectively. The daily costs for each group were 351.8 and 728.4, respectively (Table 7).
Comparison in terms of the improvement in the use of PIMs (IG vs. NIG)
Out of the 891 participants, 521 (58.4%) used PIMs in March 2019. Before matching, the number of patients in the IG was 153, and that of the NIG was 368. After 1:2 matching, the number of participants in each group was 141 and 275, respectively. The demographics of each group are shown in Table 8. There were no statistically significant changes in any health outcomes or daily costs of medications. However, the number of medications significantly decreased, and the mean values for IG and NIG were 6.0 and 7.9, respectively (Table 9).
Discussion
Few studies have assessed both medication costs and overall health outcomes in the same study. The results of our study showed that improving prescriptions would not adversely affect the overall health outcomes, and this contributed to a decrease in the number of medications and medication costs.
The reason why a decrease in medications was observed was partially due to the use of PIMs. Some medications that should be cautiously administered to older people (e.g., magnesium oxide, loxoprofen and ketoprofen) became less likely to be prescribed. However, the usage of other medications, such as levamipide and moisturizer (heparinoid), which were not classified into PIMs, was also decreased (Tables 2, 3). This could be interpreted as the avoidance of over-prescriptions.
Comparison with previous research
In previous studies, QoL and ADL were not impaired by reducing medications or improving PIMs [41, 42]. Moreover, cognitive function was not found to be impaired [43]. The results of our study were consistent with these results. In all comparisons in this study, none of the indices of health outcomes showed statistically meaningful changes (Tables 5, 7, and 9).
When comparing the IFG and NIFG, a decrease in medication costs was not observed (Tables 4 and 5). This result is inconsistent with previous research, which reported that medication costs decreased by JPY 65.6 per day. This could have occurred because more participants used PIMs in the previous research than the participants in this study. Ohshima et al. observed that 76.9% of the participants used PIMs [22]. This proportion was higher than that found in this study (58.4%).
In the comparison between the DG and NDG, the participants in whom the use of polypharmacy improved, medication costs significantly decreased (Table 7). In a previous study similar to this comparison (comparing whether the number of medications decreased or not), it was reported that medication costs decreased by JPY 170.4 per day, and this was consistent with the result of this study, which showed that medication costs decreased by JPY 241.3 per day (Tables 6 and 7) [23].
We could consider a hypothetical situation in which a proposal for improving prescriptions is implemented for the 710,000 older people in Japan who reside in facilities for older people as of 2018 [44]. In the IFG group, there was a 13.3% increase in the number of participants who had a decrease in the number of medications compared to the NIFG group, and daily medication costs were found to decrease by JPY 241.3 per day (Fig. 1, Tables 6 and 7). Given these results, for 710,000 older people, the number of medications may be reduced for 94,430 older people, and the annual medication costs may be reduced by JPY 8.3 billion.
Limitations
There are five main limitations of this study. The first limitation is representativeness. This study was conducted in private facilities for older people, where many older people who needed care lived due to illnesses or functional disorders. The participants in this study may be in a worse state of health than the general older people individuals in Japan. In addition, the difference between private and public facilities should be considered, as it affects representativeness. The admission criteria for public facilities tend to be stricter than those of private facilities, which means that residents in public facilities tend to have worse health statuses than those in private facilities. The out-of-pocket expenditure of public facilities is less than that of private facilities, which implies the possibility that the income of residents in private facilities is different from that of residents in public facilities. Moreover, in this study, the baseline data of 1260 out of 3461 (36.4%) participants were completely collected in March 2019. Nonresponse biases might have also occurred, even though propensity matching balanced the baseline between comparison groups.
The second limitation is that some residents who participated in this study in March 2019 moved out of the residential facilities by March 2020 due to hospitalizations or a change in their place of residence. The impact of improvements in prescriptions on overall health outcomes and medication costs might not have been evaluated precisely because some of the residents who were participants moved out.
The third limitation is that the improvement period was different after the development of the proposals because the proposals were launched sequentially at each facility every 3 months from June 2018. In particular, the study result of the comparison between the IFG and NIFG might be underestimated for the participants in the facilities where proposals had been conducted before the beginning of this study.
The fourth limitation is the lack of long-term efficacy data, laboratory data and subjective data. The long-term impact, such as over 1 year, was not assessed sufficiently, and it was difficult to evaluate the minor changes in laboratory data, such as HbA1C, and subjective components of a health state, such as pain.
The fifth limitation is that the demographics of participants, especially past medical history, were not sufficiently obtained, and it was difficult to determine the use of PIMs. Essentially, PIMs should be determined by considering not only the type of medication but also the history of the patient. Therefore, it is likely that the proportion of people using PIMs was overestimated and the impacts of improvement in the use of PIMs were underestimated because it was only classified by the type of medications.
The strength of our study is that it evaluates the impact of improving prescriptions on overall health outcomes and costs simultaneously. Improvement in prescriptions must not be promoted only to reduce medication costs, without considering its impact on overall health outcomes. There were some limitations, one of which was that this study was conducted in nursing home care facilities. Further studies that are conducted under other situations, such as public facilities or in-home-based care, are warranted. Despite some limitations, we believe that the results of this study have important implications for promoting improvement in prescriptions and could facilitate appropriate prescriptions while considering cost-effectiveness.
Conclusions
Modification of the use of polypharmacy and/or PIMs would decrease medication costs and the number of medications prescribed while maintaining one’s overall health outcomes. Further studies, which could facilitate appropriate prescriptions while considering cost-effectiveness, are warranted.
Availability of data and materials
The datasets generated and analysed during the current study are not publicly available due to informed consent documents but are available from the corresponding author on reasonable request.
Abbreviations
- PIM:
-
Potentially Inappropriate Medications
- QoL:
-
Quality of Life
- ADL:
-
Activities of Daily Living
- JPY:
-
Japanese Yen
- EQ-5D-5L:
-
Euro-QoL-5D-5L
- BI:
-
Barthel Index
- MMSE:
-
Mini-Mental State Examination
- DBD:
-
Dementia Behaviour Disturbance Scale
- VI:
-
Vitality Index
- IFG:
-
Implemented facilities group
- NIFG:
-
Not implemented facilities group
- DG:
-
Decreased Group
- NDG:
-
Not decrease group
- IG:
-
Improvement Group
- NIG:
-
Not Improvement Group
References
Dagli RJ, Sharma A. Polypharmacy: a global risk factor for elderly people. J Int Oral Health. 2014;6:i–ii.
Masnoon N, Shakib S, Kalisch-Ellett L, Caughey GE. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017;17:230. https://doi.org/10.1186/s12877-017-0621-2.
Mohamed MR, Ramsdale E, Loh KP, Arastu A, Xu H, Obrecht S, et al. Associations of polypharmacy and inappropriate medications with adverse outcomes in older adults with cancer: a systematic review and meta-analysis. Oncologist. 2020;25:e94–e108. https://doi.org/10.1634/theoncologist.2019-0406.
Sharma M, Loh KP, Nightingale G, Mohile SG, Holmes HM. Polypharmacy and potentially inappropriate medication use in geriatric oncology. J Geriatr Oncol. 2016;7:346–53. https://doi.org/10.1016/j.jgo.2016.07.010.
Lucchetti G, Lucchetti AL. Inappropriate prescribing in older persons: a systematic review of medications available in different criteria. Arch Gerontol Geriatr. 2017;68:55–61. https://doi.org/10.1016/j.archger.2016.09.003.
Aguiar JP, Brito AM, Martins AP, Leufkens HGM, Alves da Costa F. Potentially inappropriate medications with risk of cardiovascular adverse events in the elderly: a systematic review of tools addressing inappropriate prescribing. J Clin Pharm Ther. 2019;44:349–60. https://doi.org/10.1111/jcpt.12811.
Xing XX, Zhu C, Liang HY, Wang K, Chu YQ, Zhao LB, et al. Associations between potentially inappropriate medications and adverse health outcomes in the elderly: a systematic review and meta-analysis. Ann Pharmacother. 2019;53:1005–19. https://doi.org/10.1177/1060028019853069.
Albert SM, Colombi A, Hanlon J. Potentially inappropriate medications and risk of hospitalization in retirees: analysis of a US retiree health claims database. Drugs Aging. 2010;27:407–15. https://doi.org/10.2165/11315990-000000000-00000.
Guaraldo L, Cano FG, Damasceno GS, Rozenfeld S. Inappropriate medication use among the elderly: a systematic review of administrative databases. BMC Geriatr. 2011;11:79. https://doi.org/10.1186/1471-2318-11-79.
Motter FR, Fritzen JS, Hilmer SN, Paniz ÉV, Paniz VMV. Potentially inappropriate medication in the elderly: a systematic review of validated explicit criteria. Eur J Clin Pharmacol. 2018;74:679–700. https://doi.org/10.1007/s00228-018-2446-0.
Statistics Bureau of Japan. Population estimates in October 2020; 2020. https://www.stat.go.jp/data/jinsui/pdf/202010.pdf. Accessed 3 Feb 2021.
Statistics Bureau of Japan. Older people in international comparison; 2018. https://www.stat.go.jp/data/topics/topi1135.html. Accessed 3 Feb 2021.
Cabinet Office, Government of Japan. Annual report on the aging. Society. 2019;2019 https://www8.cao.go.jp/kourei/whitepaper/w-2019/html/zenbun/s1_1_1.html. Accessed 3 Feb 2021.
Ministry of Health, Labour and Welfare. Twenty eighth Council for Social security, 2040, supplementary material 2. The Future of Social Security-Looking to. https://www.mhlw.go.jp/stf/shingi2/0000072604_00001.html. Accessed 3 Feb 2021.
Ministry of Health, Labour and Welfare. Estimation of national medical care Expenditure 2018; 2020. https://www.mhlw.go.jp/toukei/saikin/hw/k-iryohi/18/index.html. Accessed 3 Feb 2021.
Cabinet Office, Government of Japan, Chapter 3. Economic growth and financial consolidation. In: Annual Report on the Japanese Economy and Public Finance 2014; 2014. https://www5.cao.go.jp/j-j/wp/wp-je14/index_pdf.html. Accessed 3 Feb 2021.
Suzuki Y, Sakakibara M, Shiraishi N, Hirose T, Akishita M, Kuzuya M. Prescription of potentially inappropriate medications to older adults. A nationwide survey at dispensing pharmacies in Japan. Arch Gerontol Geriatr. 2018;77:8–12. https://doi.org/10.1016/j.archger.2017.12.010.
Drummond MF, Sculpher MJ, Claxton K, Stoddart GL, Torrance GW. Methods for the economic evaluation of health care programmes. 4th ed. Oxford: Oxford University Press; 2015.
Neumann PJ, Sanders GD, Russell LB, Siegel JE, Ganiats TG. Costs-effectiveness in health and medicine. 2nd ed. New York: Oxford University Press; 2016.
Kojima T, Akishita M, Kameyama Y, Yamaguchi K, Yamamoto H, Eto M, et al. High risk of adverse drug reactions in elderly patients taking six or more drugs: analysis of inpatient database. Geriatr Gerontol Int. 2012;12:761–2. https://doi.org/10.1111/j.1447-0594.2012.00868.x.
Sakakibara M, Igarashi A, Takase Y, Kamei H, Nabeshima T. Effects of prescription drug reduction on quality of life in community-dwelling patients with dementia. J Pharm Pharm Sci. 2015;18:705–12. https://doi.org/10.18433/j37p5x.
Ohshima S, Hara A, Abe T, Akimoto H, Ohara K, Negishi A, et al. Deprescribing using the guidelines for medical treatment and its safety in the elderly and changes in patient QOL and activities of daily living. Yakugaku Zasshi. 2017;137:623–33. Japanese. https://doi.org/10.1248/yakushi.16-00263.
Ishimaru A, Watanabe F, Kanaka S. Efficacy of pharmacists’ intervention in preventing polypharmacy in hospitals for chronic care, 3. Japanese Society of Geriatric Pharmacy; 2020. p. 4–8.
Ministry of Health, Labour and Welfare. Guideline for the appropriate use of medications for the older people; 2019. https://www.mhlw.go.jp/content/11120000/000568037.pdf. Accessed 3 Oct 2021.
Ministry of Health, Labour and Welfare. National drug tariff in Japan 2020. https://www.mhlw.go.jp/topics/2020/04/tp20200401-01.html. Accessed 3 Feb 2021.
Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20:1727–36. https://doi.org/10.1007/s11136-011-9903-x.
Brooks R. EuroQol: the current state of play. Health Policy. 1996;37:53–72. https://doi.org/10.1016/0168-8510(96)00822-6.
Ikeda S, Shiroiwa T, Igarashi A, Noto S, Fukuda T, Saito S, et al. Developing a Japanese version of the EQ-5D-5L value set. J Natl Inst Public Health. 2015;64:47–55.
Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965;14:61–5.
Granger CV, Dewis LS, Peters NC, Sherwood CC, Barrett JE. Stroke rehabilitation: analysis of repeated Barthel index measures. Arch Phys Med Rehabil. 1979;60:14–7.
Folstein MF, Folstein SE, McHugh PR. Mini-mental state. J Psychiatr Res. 1975;12:189–98. https://doi.org/10.1016/0022-3956(75)90026-6.
Saxton J, Morrow L, Eschman A, Archer G, Luther J, Zuccolotto A. Computer assessment of mild cognitive impairment. Postgrad Med. 2009;121:177–85. https://doi.org/10.3810/pgm.2009.03.1990.
Perneczky R, Wagenpfeil S, Komossa K, Grimmer T, Diehl J, Kurz A. Mapping scores onto stages: mini-mental state examination and clinical dementia rating. Am J Geriatr Psychiatry. 2006;14:139–44. https://doi.org/10.1097/01.JGP.0000192478.82189.a8.
Baumgarten M, Becker R, Gauthier S. Validity and reliability of the dementia behavior disturbance scale. J Am Geriatr Soc. 1990;38:221–6. https://doi.org/10.1111/j.1532-5415.1990.tb03495.x.
Machida A. Estimation of the reliability and validity of the short version of the 28-item dementia behavior disturbance scale. Nihon Ronen Igakkai Zasshi. 2012;49:463–7. https://doi.org/10.3143/geriatrics.49.463.
Toba K, Nakai R, Akishita M, Iijima S, Nishinaga M, Mizoguchi T, et al. Vitality index as a useful tool to assess elderly with dementia. Geriatr Gerantol Int 2002;2:23–29. https://doi.org/https://doi.org/10.1046/j.1444-1586.2002.00016.x.
The Japan Geriatrics Society. Guidelines for medical treatment and its safety in the older people 2015; 2015. https://www.jpn-geriat-soc.or.jp/info/topics/pdf/20170808_01.pdf. Accessed 3 Feb 2021.
Stuart EA. Matching methods for causal inference: a review and a look forward. Stat Sci. 2010;25:1–21. https://doi.org/10.1214/09-STS313.
Rubin DB. Matching to remove bias in observational studies. In: Matched sampling for causal effects. Cambridge: Cambridge University Press; 2006. p. 62–80. https://doi.org/10.1017/CBO9780511810725.007.
Kim TK. T test as a parametric statistic. Korean J Anesthesiol. 2015;68:540–6. https://doi.org/10.4097/kjae.2015.68.6.540.
Pruskowski JA, Springer S, Thorpe CT, Klein-Fedyshin M, Handler SM. Does deprescribing improve quality of life? A systematic review of the literature. Drugs Aging. 2019;36:1097–110. https://doi.org/10.1007/s40266-019-00717-1.
Almutairi H, Stafford A, Etherton-Beer C, Flicker L. Optimisation of medications used in residential aged care facilities: a systematic review and meta-analysis of randomised controlled trials. BMC Geriatr. 2020;20:236. https://doi.org/10.1186/s12877-020-01634-4.
Kersten H, Molden E, Tolo IK, Skovlund E, Engedal K, Wyller TB. Cognitive effects of reducing anticholinergic drug burden in a frail elderly population: a randomized controlled trial. J Gerontol A Biol Sci Med Sci. 2013;68:271–8. https://doi.org/10.1093/gerona/gls176.
Ministry of Health, Labour and Welfare. Survey of social welfare. Institutions, vol. 2018. 2018. https://www.mhlw.go.jp/toukei/saikin/hw/fukushi/18/index.html. Accessed 3 Feb 2021.
Acknowledgements
We are grateful to the residents and caregivers of the facilities run by Life Company Limited who were included in this study. We are also grateful to Hiroshi Yoshihara, a researcher at the University of Tokyo, for his support in digitizing prescription data by developing an image recognition program.
Funding
This study did not receive any funding.
Author information
Authors and Affiliations
Contributions
TA analysed the data and was a major contributor in writing the manuscript. MS contributed to the interpretation of data and participated regularly in the writing process. AI mainly planned this study and provided advice in writing the manuscript. KT contributed to conducting this study by managing the staff related to all facilities. YT was responsible for proposals for improving prescriptions. SI provided constructive criticism for conducting the study. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved as a prospective observational study by the ethics committee of the Graduate School of Pharmaceutical Science, Faculty of Pharmaceutical Science, University of Tokyo. Informed consent was obtained from all participants when they decided to move to facilities for the older people run by Life Company Limited, and the residents and their families were informed about this study at the start. If individuals were not capable of providing consent (e.g., patients with severe dementia), informed consent was obtained from a proxy in their family. All methods were performed in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
TA:
Has no competing interests.
SM:
Employee:
Astellas Pharma Inc.
AI:
Research grants:
Taiho Pharmaceutical Co. Ltd., CSL Behring Japan Inc., Gilead Science K.K., Fuji Film K.K., Terumo corporation., Takeda Pharmaceutical Inc., Boston Scientific Japan Inc., DeSC Health care Inc., Otsuka Pharmaceutical KK., Varian Medical Systems Inc., and Intuitive Surgical G.K.
Consulting/lecture fees.
GSK Japan Inc., MSD Inc., Pfizer Japan Inc., Sanofi-Pasteur Inc., Novartis Pharma K.K., AbbVie GK, Astellas Pharma Inc., Chugai Pharmaceutical Co. Ltd., Asahi Kasei Pharma Inc., Novo Nordisk Pharma Inc., Eisai Inc., Beckton Dickinson and Company, Maruho Co. Ltd., Ono Pharmaceutical Inc., Sato Pharmaceutical Inc., Sumitomo Dainippon Pharma Inc., and Eli Lilly Japan K.K.
TK:
Has no competing interests.
YT:
Consulting fee:
Nichi-Iko Pharmaceutical Co., Ltd., Syakai-Hoken-Syuppan-Sya Co., Ltd., Benesse Senior Support Co., Ltd.
Speaker’s honourarium:
IQVIA Inc., Eisai Co., Ltd., Mylan EPD, Otsuka Pharmaceutical Co., Ltd., Daiichi Sankyo Espha Co., Ltd., Takeda Pharmaceutical Co., Ltd., Celgene Corporation, Novartis Pharma K.K., Shionogi & Co., Ltd. Janssen Pharmaceutical K.K., Ono Pharmaceutical Co., Ltd.,
SI:
Consulting fees.
Eisai Co. Ltd., Sanofi K.K.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ashizawa, T., Mishina, S., Igarashi, A. et al. Improvement in prescriptions while maintaining overall health outcomes: a prospective observational study conducted in Japanese facilities for older people. BMC Geriatr 22, 323 (2022). https://doi.org/10.1186/s12877-022-02872-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-022-02872-4