
Abstract
Background
Sarcopenic Obesity (SO) is characterized by low lean and high fat mass; i.e. from a functional aspect a disproportion between engine (muscle) and mass to be moved (fat). At present, most research focuses on the engine, but the close “cross talk” between age-associated adipose and skeletal muscle tissue inflammation calls for comprehensive interventions that affect both components alike. Protein and exercise are likely candidates, however with respect to the latter, the enthusiasm for intense and frequent exercise is rather low, especially in functionally limited older people. The aim of this study was therefore to evaluate the effect of whole-body electromyostimulation (WB-EMS), a time-efficient, joint-friendly and highly customizable exercise technology, on obesity parameters and cardiometabolic risk in men with SO.
Methods
One-hundred community-dwelling (cdw) Bavarian men ≥70 years with SO were randomly assigned to either (a) whey protein supplementation (WPS), (b) WB-EMS and protein supplementation (WB-EMS&P) or (c) non-intervention control (CG). Protein supplementation contributed to an intake of 1.7–1.8 g/kg/body mass/d, WB-EMS consisted of 1.5 × 20 min/week (85 Hz, 350 μs, 4 s of strain–4 s of rest) with moderate-high intensity. Using an intention to treat approach with multiple imputation, the primary study endpoint was total body fat mass (TBF), secondary endpoints were trunk fat mass (TF), waist circumference (WC) and total-cholesterol/HDL-cholesterol ratio (TC/HDL-C).
Results
After 16 weeks of intervention, TBF was reduced significantly in the WPS (− 3.6 ± 7.2%; p = 0.005) and WB-EMS&P (− 6.7 ± 6.2%; p < 0.001), but not in the CG (+ 1.6 ± 7.1%; p = 0.191). Changes in the WB-EMS&P (p < 0.001) and the WPS group (p = 0.011) differ significantly from the CG. TF decreased in the WB-EMS&P (p < 0.001) and WPS (p = .117) and increased in the CG (p = .159); WC decreased significantly in the treatment groups and was maintained in the CG. Lastly, the TC/HDL-C ratio improved significantly in the WB-EMS&P and WPS group and was maintained in the CG. Significant differences between WB-EMS&P and WPS were determined for waist circumference only (p = 0.015; TBF: p = 0.073; TF: p = 0.087; TC/HDL-C: p = .773).
Conclusion
Moderate-high dosed whey protein supplementation, especially when combined with WB-EMS, may be a feasible choice to address obesity and cardiometabolic risk in older cdw men with SO unable or unmotivated to exercise conventionally.
Trial registration number
ClinicalTrials.gov NCT02857660; registration date: 05/01/2017.
Similar content being viewed by others

Background
Sarcopenic obesity (SO) is characterized by the redistribution of muscle and fat mass at increased age [1]. Most researchers focus on the functional aspect of this “geriatric syndrome” [2], however, its severe cardiometabolic implications [3] - highly relevant for morbidity and mortality of older people [1, 4] - are undisputed. Although there is an ongoing debate as to which of the two parameters, sarcopenia or obesity, dominates the molecular process related to the pro-inflammatory status of SO [5], i.e. which is the cause and which is the effect [5], the optimum therapies for both conditions are still exercise and nutrition [6]. With respect to the latter, a considerable amount of research (review in [7,8,9,10,11,12] concentrates on an optimum protein and amino acid intake in the elderly, predominately under the aspect of maintenance of muscle mass (and function). In contrast, to our best knowledge no study has determined the isolated effect of protein/amino acids on obesity and cardiometabolic risk factors in people with prevalent SO. Nevertheless, a beneficial effect of (whey) protein [13] on total and abdominal fat reduction and (other) cardiometabolic risk factors [13, 14] in overweight and obese people has been previously reported. In parallel, apart from its beneficial effect on sarcopenia, resistance exercise training (RT) favorably affects obesity and cardiometabolic risk factors in middle-aged and older adults [15,16,17,18]. However, it is unrealistic to assume that people with SO will achieve the intensity and frequency of exercise recommended for positively impacting disabling conditions or obesity [19]. In this context, whole-body electromyostimulation (WB-EMS), an effective, time-efficient, joint-friendly and highly customized further development of the recognized local EMS application predominately applied in therapy [16, 20,21,22,23,24,25,26,27], may be a good choice for older subjects at risk for sarcopenic obesity (SO).
The aim of this contribution was to determine the effect of isolated whey protein supplementation (WPS) and a combined WB-EMS and whey protein protocol on SO under particular consideration of the obesity and cardiometabolic aspect of SO in community dwelling men 70 years+ and older with SO.
Our primary hypothesis was that WB-EMS&P but not isolated WPS significantly affected obesity, compared with a non-training, non-protein-supplemented control.
Our secondary hypothesis was that WB-EMS&P but not isolated WPS significantly affected cardiometabolic risk factors compared with a non-training, non-protein-supplemented control.
Methods
The Franconian Sarcopenic Obesity (FranSO) study is a randomized controlled trial in a parallel groups design with three balanced study arms: (a) WB-EMS and protein supplementation (b) protein supplementation (c) non-intervention control. The present contribution focuses on the “obesity” aspect of the study and (related) cardiometabolic risk factors. The corresponding “sarcopenia” aspect was specifically addressed in a recently published article [21].
The Institute of Medical Physics (IMP), Friedrich-Alexander University Erlangen-Nürnberg (FAU) conducted the study between February and December 2016. FranSO was approved by the ethics committee of the FAU (Ethikantrag 67_15b)Footnote 1 and fully complied with the Helsinki Declaration “Ethical Principles for Medical Research Involving Human Subjects“. All study participants gave their written informed consent. The FranSO-study was fully registered under ClinicalTrials.gov: NCT2857660.
Participants
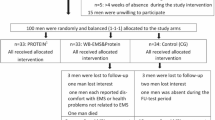
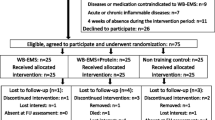
After extensive screening [28], 100 community dwelling, Caucasian males 70 years and older with the eligibility criteria listed below were randomly allocated to the three study arms (Fig. 1). Inclusion criteria apart from sex, age and status (see above) were (a) skeletal muscle mass index (SMI) < 0.789Footnote 2 as suggested by the Foundation for the National Institutes of Health (FNIH) [29] for the sarcopenia aspect of SO. (b) A percentage body fat ratio of > 27% (PBF) representing obesity, as recommended by Baumgartner [30]. Exclusion criteria were (a) present medication or diseases affecting body composition or preventing WB-EMS application (e.g. cardiac pacemaker), (b) any type of RT conducted for > 45 min/week, (c) absence during the intervention period, (d) regular alcohol consumption > 80 g/d on 5 days/week or (e) unwillingness to accept the randomization procedure. Fig. 1 shows participant flow through the study.

Diagram of participant flow through the different study phases
Intervention
Whole-body Electromyostimulation (WB-EMS)
Although WB-EMS has been frequently described (e.g. [20, 22, 23, 25, 26, 31,32,33,34]), a brief introduction of this predominately resistance type exercise will be given. WB-EMS is based on the recognized local electromyostimulation predominately applied in the treatment of muscular injuries. The main benefit of EMS might be that it can be applied independent of voluntary muscle activation up to supra-maximum level. A drawback of EMS frequently addressed is the restricted impact on functional parameters, at least when applied in a static mode (review in [35]). Unlike local EMS, current WB-EMS equipment enables the simultaneous activation of up to 10 regions or 14 muscle groups. The total stimulated area, up to 2600–2800 cm2, can be simultaneously activated, with selectable intensity for each region. In the present study, we applied our video-guided WB-EMS standard protocol (bipolar, 85 Hz, impulse-width: 350 μs) in a standing position 1.5 × 20 minFootnote 3 per week for 16 weeks. We used an interval approach with 4 s of EMS stimulation with an immediate impulse burst and an impulse pause of 4 s. During the impulse phases, different low intensity exercises were conducted [25, 26] in order to overcome the frequently reported limited impact of static EMS application on neuromuscular coordination and functional parameters. In detail, we conducted two sets of 8 different movements (Table. 1) with 6–12 repetitions. However, intensity and amplitude of the exercises/movements given in Table 1 were kept very low to ensure that the effect of the voluntary exercise per se did no impact our primary and secondary outcomes (Table. 1).
After 4 weeks of conditioning, we progressively increased the duration of the session from 14 min up to 20 min. Of importance, the WB-application was applied in a highly customized personal training setting with one instructor responsible for two participants. This procedure is crucial for the proper regulation of (impulse) intensity, because we have to use a rate of perceived exertion (RPE) to generate a sufficient but tolerable intensity of the EMS application. Indeed, due to the variations in current sensitivity in the various muscle groups and differences in pain sensation of the individuals an objective prescription of (impulse) intensity is not adequate. Thus, we prescribed an RPE of “6–7” (i.e. “hard+” to “very hard”) on the Borg CR10 Scale. We individually adapted this intensity during the second session and after 4, 8 and 12 weeks for each body region in close interaction between participant and instructor. Instructors started the WB-EMS application with this saved initial setting and increased the (impulse) intensity slightly every 3 min to achieve the prescribed RPE during the WB-EMS application. This procedure was conducted in very close cooperation with the participants in order to generate optimum exercise intensity.
Protein supplementation
Dependent on their habitual dietary intake, we gave participants of the WPS and WB-EMS&P group with whey protein powder supplements (Inkospor Active, INKO, Roth, Germany) in order to realize a total daily protein amount of 1.7–1.8 g/kg/bodymass. The supplement contained 2.8% of fat, 6.4% of carbohydrates CHO) and 80% of (whey) protein. Including a high amino acid (57%), and L-Leucine (9%) component, the chemical score of this product is 159.Footnote 4 The protein powder was ingested with water; doses larger than 40 g were split into two lower quantities. We did not prescribe intake at a specific time of the day. All the participants were carefully instructed on how to apply the protein supplementation. They were also contacted every second week and interviewed about their proper protein (and Vitamin D) supplementation; in parallel all participants were asked to maintain their dietary habits including dietary protein intake during the intervention.
Vitamin D supplementation
We provided participants of all study arms with cholecalciferol (Taxofit, Cologne, Germany). Subjects were instructed to take a dose of 800 IU/d.
Outcomes
Primary study outcome
-
Changes in total body fat mass (TBF) from baseline to 16 week follow-up
Secondary study outcome
-
Changes in trunk fat mass (TF) from baseline to 16 week follow-up
-
Changes in waist circumference from baseline to 16 week follow-up
-
Changes in total cholesterol/HDL-Cholesterol ratio from baseline to 16 week follow-up
-
Changes in triglycerides (TAG) from baseline to 16 week follow-up
Experimental study outcome
-
Changes in total visceral fat area (VFA) from baseline to 16 week follow-up
Assessment
All tests were performed by the same method and researcher at a similar time of day (±1 h) immediately before and after 16 weeks of intervention. Great emphasis was placed on the standardization of the tests including consistent verbal test prescription. Participants were requested to avoid severe physical activity and refrain from food/beverages 24 h and 3 h respectively prior to the assessment.
Anthropometric data
All parameters were determined with calibrated devices. Waist circumference was determined as the minimum circumference between the distal end of the rib cage and the top of the iliac crest along the midaxillary line. Body height was assessed using a Harpender stadiometer (Crosswell, Crymych, UK), body mass and composition were determined via direct-segmental, multi-frequency Bio-Impedance Analysis (DSM-BIA, InBody 770, Seoul, Korea). Using a tetrapolar eight-point tactile electrode system that applies six frequencies (1, 5, 50, 250, 500 and 1000 kHz), this device enables the body composition of the trunk, arms and legs to be determined separately. Appendicular skeletal muscle mass (ASMM) was calculated adding the mass for upper and lower limbs. Following the sarcopenia definition of the FNIH [29], we calculated skeletal muscle mass index (SMI) as ASMM/BMI. Reliability of the DSM-BIA device to determine TBF was checked by a test-retest protocol in two studies with 2 × 25 male participants 30–50 [36] and 70+ years old [21]. Whilst refraining from food, beverages and physical activity participants were assessed twice within one hour. Resulting ICC was 0.89 (95%-CI: .88–.93) and 0.88 (95%-CI: .85–.91) in the cohort 70 + .
Blood sampling
Blood was drawn on a different date three days before the main assessment. After an overnight fast, blood was consistently sampled between 7:00 and 9:00 in the morning in a sitting position from an antecubital vein. Serum samples were centrifuged for 20 min at 3000 RPM and analyzed by the “Zentrallabor” of the Medical Department, FAU. Glucose, total cholesterol, HDL and LDL cholesterol and triglycerides (Olympus Diagnostica GmbH, Hamburg, Germany) were determined.
Questionnaires
To adequately assess baseline characteristics of the participants, a questionnaire asked for various aspects including (a) demographic parameters, (b) diseases, (c) medication, (d) operations (e) physical limitations, low-traumatic fractures, injuries or falls within the last year, (f) pain frequency and intensity at different regions (f) lifestyle, including physical activity, exercise [37] and (g) nutrition. The abridged version of the Late Life Function and Disability Instrument (LLFDI) was used to determine the self-rated physical performance of the participants [38]. After 16 weeks of intervention, all participants conducted a comparable questionnaire in order to detect changes that may affect our study endpoints. All questionnaires were carefully checked for completeness and accuracy in close cooperation between research assistants and participants.
Dietary protocols
In order to determine habitual dietary intake, 4-day dietary protocols were conducted by all the participants immediately before and after the trial. Participants were carefully briefed and instructed on how to keep the protocols. The consumed food was analyzed by a certified nutritionist using the Freiburger Nutrition Protocol (nutri-science, Hausach, Germany). Doubtful results, e.g. energy consumption below 1000 or higher than 3500 kcal/d, were checked together with the participant. In all cases, the men provided a second dietary protocol that was based on days more representative for their usual nutrition. Compliance with the protein and/or vitamin-D supplementation was monitored by the same nutritionist biweekly (see above).
Changes in trial outcomes after trial commencement
No changes in trial outcomes were made after trial commencement.
Obesity definition
We diagnosed obesity using the body-fat rate (i.e. percent body fat; TBF%) as determined by the DSM-BIA (DSM-BIA, InBody 770, Seoul, Korea) assessment and applying a cut-off point of > 27% body fat (PBF) according to the suggestion of Baumgartner [30] for SO.
Sample size calculation
The sample size calculation of the FranSO study was based on the Sarcopenia aspect of the project.Footnote 5 With respect to the present primary hypothesis that addresses “total body fat” (TBF), a recent study with men 65+ [26] reported a mean difference between WB-EMS (− 1.3 ± 0.9 kg) and control condition (− 0.3 ± 0.9 kg) of 1.0 ± 1.0 kg. Applying a similar, slightly more conservative approach with a mean difference of 1.0 ± 1.25 kg the sample size of 33 participants per group generates a 90% power to detect differences of TBF between the WB-EMS&P and the CG (α = .05; t-test based sample size calculation).
Randomization procedures
One hundred participants were randomly assigned to three study arms (WB-EMS&P vs. WPS vs. CG) using strata of 5 years and a uniform allocation rate of 1:1:1 (Fig. 1). For the group allocation, lots enclosed in opaque plastic shells (“kinder egg”, Ferrero, Italy) were drawn from a bowl by the participants themselves, albeit under supervision of the primary investigator responsible for the randomization procedure (WK). Neither participants nor researchers knew the allocation beforehand. After the group allocation, WK enrolled participants and carefully instructed them about dos and don’ts.
Blinding
The blinding strategy refer to the assessments of the study outcomes. Research assistants/outcome assessors did not know the group allocation of the participants (WB-EMS&P, WPS or CG) and were requested not to ask either.
Biometry and statistical analysis
All participants who were randomly allocated to the three study arms at baseline were included in the intention to treat (ITT) analysis. ITT analysis and imputation of missing (follow-up) data were conducted using R statistics software with multiple imputation performed by the Amelia II program [39]. Imputation was repeated 100 times. Multiple imputation worked well in all cases. We used graphical (QQ- and box-plots) and statistical (Shapiro-Wilkes-Test) tests to validate the normal distribution of the outcomes presented here. Based on a normal distribution of the data we applied paired-samples t-test to compute intra-group changes. Differences between the groups were determined using one-way analysis of variance (ANOVA). The approach of Allison [40] was used to combine the outcomes of the imputation. Relevant differences in analysis of variance results (i.e. p < .100) were further addressed by pairwise t-test comparisons for multiple imputation with pooled standard deviation. We adjusted “p”-values for multiple testing by the method suggested by Holm [41]. Tests were all applied 2-sided. The accepted level of significance was 5%.
Results
Baseline characteristics of the FranSO participants listed in Table 2 did not differ relevantly between the study arms. Apart from the still non-significant between group differences for baseline protein intake, baseline data reported in Table 2 is very homogeneous between the groups. Apart from the eligibility criteria-induced low SMI and high PBF, most of the parameters were representative for cdw German men 70 years+ [42, 43]. This includes measures of functional sarcopenia that had been expected to be less favorable in this cohort.
Participant flow through the study was shown in Fig. 1. Altogether eight subjects were lost to follow-up; dropout rates per group averaged < 10%. We observed an overall attendance rate for the WB-EMS sessions of 91 ± 7% (i.e. ≈22 of 24 sessions). Adherence to the WB-EMS protocol was determined using the subjects’ average RPEs that were recorded by the instructors after 5, 10, 15 and 20 min. RPE averaged 6.8 ± 0.3 (7 = “very hard”) with no relevant changes after the 4th week. The proper intake of the recommended dose of protein powder was assessed by checking our protein supplementation lists and records and by a follow-up compliance questionnaire. In summary, both treatment groups took a lower dose of protein powder than prescribed (WB-EMS&P: -4.2 ± 5.2 g/d; p = 0.119; WPS: -7.3 ± 4.8 g/d, p = 0.001). This was completely compensated by the increased dietary protein intake in both groups, however. Thus, total protein intake (1.78 ± 0.09 g/kg body mass/d) did not differ during the intervention period and was at the upper end of our intended total intake. In detail, all but two participants of the WB-EMS&P group (1.59 and 1.65 g/kg/d) achieved the prescribed total protein dose of 1.7–1.8 g/kg body mass/d. One participant quit the study due to uneasiness during WB-EMS application; another participant cited antipathy to consume high (whey) protein doses for its dropout. No further adverse effects were reported by the participants.
Study outcomes
Baseline results and changes for total body fat (TBF) was listed in Table 3. Based on similar baseline values (p = .995), TBF was reduced significantly by 3.6 ± 7.2% in the WPS (p = 0.005) and 6.7 ± 6.2% in the combined WB-EMS and whey protein supplement group (p < 0.001). A non-significant increase of 1.6 ± 7.1% (p = 0.191) was determined in the control group that differed significantly from the WB-EMS&P (p < 0.001) and the WPS group (p = 0.011). No significant differences were observed between both intervention groups (p = 0.073). Correspondingly, we reject our main hypothesis that only the combined treatment group but not the WPS group significantly reduced TBF compared with a control group without protein supplementation or WB-EMS application.
The results for the secondary study endpoints are listed in Table 4. Again, no significant group differences were observed at baseline (p ≥ 0.407).
Trunk body fat decreased significantly in the WB-EMS&P (p < 0.001) and non-significantly in the WPS group (p = 0.117), and increased non-significantly in the CG (p = 0.159). Significant group differences were determined between WB-EMS&P and the CG only (p < 0.001; WPS vs. CG: p = 0.068; WB-EMS&P vs. WPS: p = 0.087). In parallel, based on comparable baseline data (WB-EMS&P: 119 ± 34 vs. WPS: 117 ± 30 vs. CG: 121 ± 33 cm2), “total visceral fat area” (VFA) did not change in the CG (0.4 ± 7.7%, p = .614) and decreased significantly in the WPS (− 3.1 ± 8.4%; p = .017) and WB-EMS&P groups (− 4.6 ± 8.7%; p = .002). Again, a significant difference was determined between the WB-EMS&P and the control group (p = .034).
Waist circumference decreased significantly (p ≤ 0.001) in both treatment groups, and was maintained in the CG (p = .714). Significant group differences were observed between the treatment groups and the CG (WB-EMS&P: p = 0.001; WPS: p = 0.033) and between the WB-EMS&P and WPS group (p = 0.015).
The ratio of total cholesterol to HDL-cholesterol changed favorably in both treatment groups (p < .001) and was maintained in the CG (p = .365). Both treatment groups differ significantly from the CG (p = .039 and p = .020) with no relevant differences between WB-EMS&P and WPS (p = 0.773). Looking behind the covariates, corresponding intragroup changes and group differences were predominately based on significant reductions of total cholesterol in the treatment groups (WB-EMS&P:-8.7 ± 18.9, p ≤ .009; WPS: -10.2 ± 17.7 mg/dl) and a non-significant increase in the CG (3.8 ± 16.0 mg/dl, p = .220). HDL-C levels increased in all groups (1.7 to 2.0 mg/dl). However, changes were significant (p = 0.046 and p = 0.048) in the CG and WPS group only (WB-EMS&P: p = .072).
In parallel, more favorable effects in both treatment groups vs control, albeit without reaching significance (p > 0.10 to 0.15), were observed for the ratio of LDL-C to HDL-C. In contrast, triglycerides were not significantly affected by WB-EMS application or protein supplementation. Further, no group differences were observed (Table. 4). The same is true for resting glucose, with baseline values predominately in the normal range and intragroup changes far from being significant (p > 0.40).
Thus, in summary we had to reject hypothesis 2 that WB-EMS&P but not isolated protein supplementation will significantly affect cardiometabolic risk factors compared with a non-training, non-protein-supplemented control.
Confounders
Follow-up questionnaires and structured interviews in close interaction with the participants did not indicate relevant changes of lifestyle, diseases and medication during the study period. In parallel, none of the participants reported operations or injuries for longer than one week.
Energy intake, CHO, fat and alcohol intake as assessed by 4-day dietary protocols did not change significantly within (p ≥ .270) or vary between the study groups (p ≥ 0.606). However, as mentioned above, dietary protein intake increased significantly in the WPS (9 ± 12 g/d, p = .001), increased slightly in the WB-EMS&P (3 ± 16 g/d; p = 0.316) and was maintained in the CG (− 1 ± 16 g/d; p = 0.671). Corresponding group differences were non-significant (p ≥ 0.056).
Discussion
The key result of the study was that both WB-EMS&Protein and isolated WPS significantly affect total and abdominal obesity and other important cardiometabolic risk factors in community dwelling men 70+ with Sarcopenic Obesity. This result could not have been necessarily expected. The FORMOsA study [22, 44], which determined the effect WB-EMS&P in cdw women 70+ with SO, generally confirmed the favorable positive effects on cardiometabolic risk factors; FORMOsA failed to generate any significant reduction of total and abdominal body fat, however. Two main reasons may contribute to this result: (a) the low frequency and intensity of the WB-EMS application and (2) the low-moderate dose of WPS (0.3 g/kg/d) supplied in FORMOsA. Thus, in order to generate a more striking effect, we applied a more challenging WB-EMS protocol and provided higher doses of whey protein. The present results confirmed this strategy. Summarizing the favorable effects on body fat and cardiometabolic risk, FranSO ranged in the upper region of combined RT/protein supplement approaches in older adults (e.g. ([45,46,47,48,49,50]).
In contrast to the recognized effect of combined resistance type & protein approaches, the clinical effectiveness of isolated protein and/or amino acid supplementation on body fat and cardiometabolic risk factors in older (sarcopenic) obese people has not yet been clearly determined. However, there is significant evidence that high-protein diets generate favorable effects on parameters closely related to obesity parameters. This includes specific effects on appetite, hunger and satiety hormones [51, 52], significant enhancement of fat oxidation and increased thermogenesis [53, 54]. Further, isolated WPS augments muscle mass under isoenergetic conditions [21], preserves muscle mass under energy deficiency and induces more fat loss during energy restrictive diets in obese older adults [55, 56]. However, studies that assessed the effects of whey protein on fat reduction under isoenergetic conditions are rare and inconsistent. After 23 weeks of 56 g/d of WPS in overweight-obese adults, Baer et al. [13] reported a significant reduction of 2.3 kg in fat mass and 2.4 cm in waist circumference (WC) compared with an isoenergetic CHO supplementation. Tahavorgar et al. [57], who compared the effects of 12 weeks of whey versus soy protein preloads (65 or 60 g/d, 30 min before the largest meal of the day) in overweight to obese Persian males, 30–65 years old, described significant reductions of PBF and WC in both protein groups. However WPS resulted in much more pronounced reductions of PBF (− 9.1% vs. -3.1%), WC (− 9.7 vs. -2.3 cm) and appetite compared to soy protein. In contrast, after 12 weeks of intervention, Pal et al. [58] did not observe significant effects of WPS (54 g/d) on fat mass and distribution compared with an isoenergetic control group in a comparable cohort of overweight to obese adults. With respect to other markers of cardiometabolic health, a recent review [59] summarized predominately favorable effects on total cholesterol, LDL-C, HDL-C and TAG after 4–12 weeks of WPS using different doses. Likewise, the authors [59] reported positive effects of WPS on glucose control, inflammation/oxidative stress and blood pressure, however, the present literature summarized in this review is less consistent.
It was not our intention to address the aspect of whether protein supplementation increases the effect of WB-EMS on body composition, physical functioning and cardiometabolic indices. Rather, we aimed to determine (a) whether a recognized WB-EMS application [16, 21,22,23,24,25,26,27, 44] combined with a moderate to high dosed WPS intervention may positively impact cardiometabolic indices including body fat in men with SO, and (b) whether the (very) low threshold intervention “isolated WPS” may be sufficient to realize this aim.
Not perfectly addressed within the present research design, but based on the rather consistent effects of WB-EMS [16, 20,21,22,23,24,25,26,27, 44] on body composition provided by the literature, we think it is legitimate to discuss the effect of an additional WPS on recognized WB-EMS protocols with respect to body fat and cardiometabolic indices in older adults. The only study that focuses on people with SO, however, did not observe significant corresponding differences between WB-EMS with and without protein supplementation ([22, 44]. Enlarging the research area to the related RT literature, there is again limited evidence for the superiority of combined RT&Protein protocols (vs. isolated RT) on cardiometabolic risk and body fat indices. Several studies (e.g. [46,47,48,49,50, 60,61,62,63,64,65]) focus on this issue in middle-aged to older adults; however, based on a predominately positive effect on body fat and cardiometabolic risk factors in both groups [46, 48,49,50, 61,62,63,64,65], we were unable to locate any study that determined significant differences between the conditions. Of importance, however, studies vary considerably as to the protein source (whey/casein supplements, milk/red meat or combined egg/meat/milk diets) and dose (0.17 to 1.00 g/kg body mass/d) and frequently feature an insufficient sample size. Conversely, a recent study [65] with sufficient power that applied most of the recommendations given for optimum protein supplementation [7, 8, 66] did not report differences for body fat changes or cardiometabolic indices for their overweight to obese cohort 35–65 years old.
On the other hand, it is debatable whether the similar or predominately non-significantly more favorable results of the combined group compared to the easy feasible and very low threshold “protein-only” approach justify an additional WB-EMS (or RT) application; at least under the premise of significant effects on muscle mass in both treatment groups [21]. However, comparable to the reduction of fat parameters, the hypertrophic response of the WB-EMS&P was about twice as highFootnote 6 as among the WPS group. Even more relevant for frail cohorts,Footnote 7 functional parameters (i.e. grip-strength, gait speed) were not relevantly affected by the protein supplementation, while the combined protocol caused highly significant and clinically relevant effects. Thus, we strongly recommend a combined resistance type and protein intervention. Comparing WB-EMS with other resistance type exercises, its joint-friendly, time effective and highly customized mode of application predestines WB-EMS as a good option for older people either unable or unwilling to exercise conventionally.
Some limitations and features may decrease the scientific evidence of the FranSO study and our corresponding recommendations. (a) In contrast to present definitions [29, 67,68,69], subjects diagnosed as sarcopenic fulfilled only the morphological aspect of Sarcopenia (i.e. SMI < 0.789 kg/(kg/m2). (b) Following Baumgartner et al. [30], we selected a cut-off point of > 27% PBF for obesity. However, the average PBF in 2986 Caucasian males of Swiss origin 74–98 years old was reported to be 25.4 ± 5.1% (MV ± SD), corresponding to a BMI of 25.2 ± 3.0 kg/m2 [70]. Further, applying a T-Score based criterion (i.e. PBF-MV + 2 SD), based on our Northern Bavarian database of 1189 Caucasian men 18–35 years old [28], the corresponding cut-off point ranged around 31% PBF (24.5% for MV-1SD). (c) An additional isolated WB-EMS training group might have provided deeper insights. However, in fact, cdw men with sarcopenic obesity are rare [28]. Even though we weakened our inclusion criteria (see above), we are unable to generate another subgroup with sufficient statistical power. Since we determined the effects of an isolated WB-EMS group in a previous trial [22, 44], we opted to focus on the effect of isolated WPS on musculoskeletal and cardiometabolic risk factors in this study. (d) We used DSM-BIA to determine body composition. There are still some general concerns about this technology, at least when applied on adults with severe obesity [71] and when summarizing the results of different devices and equipment. We determined excellent agreements for PBF (Intra Class Correlation for PBF: 0.86 to 0.92 with consistently narrow limits of agreement) for lean-overweight cohorts of different ages between the DSM-BIA InBody 770 (Korea Seoul) used in this study and our DXA scanner (Hologic 4500a, Boston, USA), however. This observation was confirmed by Ling et al. [72] for the previous DSM-BIA version InBody 720 (Seoul, Korea) and an identical DXA scanner. (e) Due to unavailable validation data for the InBody 770, we considered “total visceral fat area”, as determined by DSM-BIA as an experimental endpoint. Nonetheless, using a small sample of the FranSO cohort demonstrated a good agreement between Magnet Resonance Imaging (MAGNETOM Skyrafit, Siemens Healthcare GmbH, Erlangen, Germany) and DSM-BIA (InBody 770; Seoul, Korea). However, this finding has to be confirmed with an adequate sample size. (f) We did not focus on “isoenergetic conditions” and hence did not supply the CG with a similar amount of non-protein derived energy (e.g. 50–60 g/d CHO for the CG in compensation for 51 and 59 g/d protein-supplementation in the treatment groups). Due to the specific assignment of protein for anabolic processes, the impact on thermoregulation, hunger and satiety along with its minor impact on energy metabolism during energy balance [73] and decreased energy efficiency [74], we think a corresponding approach might produce a more pronounced bias compared with an only theoretical computed difference for energy uptake. Of importance however, even when considering the 200–250 “extra kcal” of the protein supplementation, we did not detect a significant increase of energy uptake in the treatment groups (< 90 kcal/d). We attribute this finding to the frequently reported whey protein effects on appetite, hunger and satiety [51, 52, 57]. (g) The WB-EMS setting of the present study can be considered as personal training with one instructor and two users. This approach is also applied in the majority of commercial settings and ensures a high level of safety and effectivity [75]. However, a relevant part of the WB-EMS results can be contributed to the close interaction and may be independent of the training tool.
The generalization of our results to other cohorts may be problematic. Considering factors related to SO (e.g. inflammation [5], mitochondrial abnormalities [76], oxidative stress [77]) muscle response to exercise and/or protein may differ from healthy older people. On the other hand, WB-EMS trials with other cohorts but similar WB-EMS application demonstrated comparable results on obesity and cardiometabolic parameters [16, 23].
Conclusion
FranSO is the first study to demonstrate the positive effect of whey protein supplementation, and to a more favorable extent, WB-EMS&Protein on obesity and cardiometabolic risk in cwd people 70+ with SO. The importance of this finding is obvious: Even in older men within the range of recent protein recommendations [7], higher whey protein doses not only affected muscle mass [21] but also reduced obesity and cardiometabolic indices. Adding exercise to this easy feasible approach significantly increases the effect on obesity (but not cardiometabolic) parameters. In this context, the joint-friendly, time effective and highly customized and personalized WB-EMS training technology that mitigate barriers and concerns about conventional resistance exercise may be a reasonable and safe option for older, functionally limited and frail people to fight obesity and sarcopenia.
Notes
Ethikkommission der Friedrich-Alexander-Universität Erlangen-Nürnberg, Krankenhausstraße 12, 91,054 Erlangen, Germany; phone + 49 9131 85–22,270; e-mail: ethikkommission@fau.de
Appendicular skeletal muscle mass (ASMM)/ body mass index (BMI)
E.g. WB-EMS training every Monday/Tuesday and every second Thursday/Friday
Briefly, the chemical score indicates the “quality” of the protein source. The chemical score is calculated from the content of the amino acid with the lowest occurrence in the protein to be tested.The reference used is egg protein (100%).
Primary endpoint: Changes of Sarcopenia Z-Score [22] from baseline to 16 week follow-up
However, differences between WB-EMS&P versus WPS were also not significant (p = 0.055) for SMI
However, we did not consider our cdw cohort as “frail”
Ethikkommission der Friedrich-Alexander-Universität Erlangen-Nürnberg, Krankenhausstraße 12, 91,054 Erlangen, Germany; phone + 49 9131 85–22,270; e-mail: ethikkommission@fau.de
Abbreviations
- ASMM:
-
Appendicular skeletal muscle mass
- cdw:
-
Community dwelling
- CG:
-
Control group
- CI:
-
Confidence interval
- DSM-BIA:
-
Direct-segmental, multi-frequency Bio-Impedance Analysis
- FNIH:
-
Foundation for the National Institutes of Health
- FORMOsA:
-
“Forschungsverbund Muskelschwund (Sarkopenie) und Osteoporose – Folgen eingeschränkter Regeneration im Alter”
- FranSO:
-
Franconian sarcopenic obesity (study)
- HDL-C:
-
High density lipoprotein cholesterol
- ITT:
-
Intention to treat
- LDL-C:
-
Low density lipoprotein cholesterol
- LLFDI:
-
Late life function disability instrument
- MV:
-
Mean value
- n.s.:
-
Non-significant
- PBF:
-
Percent body fat
- RPE:
-
Rate of perceived exertion
- RT:
-
Resistance exercise training
- SD:
-
Standard deviation
- SMI:
-
Skeletal muscle mass index
- SO:
-
Sarcopenic obesity
- TBF:
-
Total body fat mass
- TC/HDL-C:
-
Total-cholesterol/HDL-cholesterol ratio
- TF:
-
Trunk fat mass
- WB-EMS:
-
Whole-body electromyostimulation
- WB-EMS&P:
-
Combined whole-body electromyo-stimulation and protein supplement group
- WC:
-
Waist circumference
- WK:
-
Wolfgang Kemmler
- WPS:
-
whey protein supplementation
References
Stenholm S, Harris TB, Rantanen T, Visser M, Kritchevsky SB, Ferrucci L. Sarcopenic obesity: definition, cause and consequences. Curr Opin Clin Nutr Metab Care. 2008;11(6):693–700.
Cruz-Jentoft AJ, Landi F, Topinkova E, Michel JP. Understanding sarcopenia as a geriatric syndrome. Curr Opin Clin Nutr Metab Care. 2010;13(1):1–7.
Malafarina V, Uriz-Otano F, Iniesta R, Gil-Guerrero L. Sarcopenia in the elderly: diagnosis, physiopathology and treatment. Maturitas. 2012;71(2):109–14.
Zamboni M, Mazzali G, Fantin F, Rossi A, Di Francesco V. Sarcopenic obesity: a new category of obesity in the elderly. Nutr Metab Cardiovasc Dis. 2008;18(5):388–95.
Kalinkovich A, Livshits G. Sarcopenic obesity or obese sarcopenia: a cross talk between age-associated adipose tissue and skeletal muscle inflammation as a main mechanism of the pathogenesis. Ageing Res Rev. 2017;35:200–21.
Goisser S, Kemmler W, Porzel S, Volkert D, Sieber CC, Bollheimer LC, Freiberger E. Sarcopenic obesity and complex interventions with nutrition and exercise in community-dwelling older persons--a narrative review. Clin Interv Aging. 2015;10:1267–82.
Bauer J, Biolo G, Cederholm T, Cesari M, Cruz-Jentoft AJ, Morley JE, Phillips S, Sieber C, Stehle P, Teta D, et al. Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE study group. J Am Med Dir Assoc. 2013;14(8):542–59.
Baum JI, Kim IY, Wolfe RR. Protein Consumption and the elderly: what is the optimal level of intake? Nutrients. 2016;8(6)
Komar B, Schwingshackl L, Hoffmann G. Effects of leucine-rich protein supplements on anthropometric parameter and muscle strength in the elderly: a systematic review and meta-analysis. J Nutr Health Aging. 2015;19(4):437–46.
Lancha AH Jr, Zanella R Jr, Tanabe SG, Andriamihaja M, Blachier F. Dietary protein supplementation in the elderly for limiting muscle mass loss. Amino Acids. 2017;49(1):33–47.
Malafarina V, Uriz-Otano F, Iniesta R, Gil-Guerrero L. Effectiveness of nutritional supplementation on muscle mass in treatment of sarcopenia in old age: a systematic review. J Am Med Dir Assoc. 2013;14(1):10–7.
Xu ZR, Tan ZJ, Zhang Q, Gui QF, Yang YM. The effectiveness of leucine on muscle protein synthesis, lean body mass and leg lean mass accretion in older people: a systematic review and meta-analysis. Br J Nutr. 2015;113(1):25–34.
Baer DJ, Stote KS, Paul DR, Harris GK, Rumpler WV, Clevidence BA. Whey protein but not soy protein supplementation alters body weight and composition in free-living overweight and obese adults. J Nutr. 2011;141(8):1489–94.
Pal S, Radavelli-Bagatini S. The effects of whey protein on cardiometabolic risk factors. Obes Rev. 2013;14(4):324–43.
Cornelissen VA, Fagard RH, Coeckelberghs E, Vanhees L. Impact of resistance training on blood pressure and other cardiovascular risk factors: a meta-analysis of randomized, controlled trials. Hypertension. 2011;58(5):950–8.
Kemmler W, Teschler M, Weissenfels A, Bebenek M, Frohlich M, Kohl M, von Stengel S. Effects of whole-body Electromyostimulation versus high-intensity resistance exercise on body composition and strength: a randomized controlled study. Evid Based Complement Alternat Med. 2016;2016:9236809.
Strasser B, Arvandi M, Siebert U. Resistance training, visceral obesity and inflammatory response: a review of the evidence. Obes Rev. 2012;13(7):578–91.
Strasser B, Schobersberger W. Evidence for resistance training as a treatment therapy in obesity. J Obes. 2011;2011 https://doi.org/10.1155/2011/482564
Chodzko-Zajko WJ, Proctor DN, Fiatarone Singh MA, Minson CT, Nigg CR, Salem GJ, Skinner JS. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med Sci Sports Exerc. 2009;41(7):1510–30.
Fritzsche D, Fruend A, Schenk S, Mellwig K, Keinöder H, Gummert J, Horstkotte D. Elektromyostimulation (EMS) bei kardiologischen Patienten. Wird das EMS-Training bedeutsam für die Sekundärprävention? Herz. 2010;35(1):34–40.
Kemmler W, Weissenfels A, Teschler M, Willert S, Bebenek M, Shojaa M, Kohl M, Freiberger E, Sieber C, von Stengel S. Whole-body Electromyostimulation and protein supplementation favorably affect Sarcopenic obesity in community-dwelling older men at risk. The randomized controlled FranSO study. Clin Interv Aging. 2017;12:1503–13.
Kemmler W, Teschler M, Weissenfels A, Bebenek M, von Stengel S, Kohl M, Freiberger E, Goisser S, Jakob F, Sieber C, et al. Whole-body Electromyostimulation to fight Sarcopenic obesity in community-dwelling older women at risk. Results of the randomized controlled FORMOsA-Sarcopenic obesity study. Osteo Int. 2016;27(10):3261–70.
Kemmler W, Kohl M, VS S. Effects of high intensity resistance training versus whole-body Electromyostimulation on cardiometabolic risk factors in untrained middle aged males. A randomized controlled trial. J Sports Res. 2016;3(2):44–55.
Kemmler W, von Stengel S. Whole-body electromyostimulation as a means to impact muscle mass and abdominal body fat in lean, sedentary, older female adults: subanalysis of the TEST-III trial. Clin Interv Aging. 2013;8:1353–64.
Kemmler W, Schliffka R, Mayhew JL, von Stengel S. Effects of whole-body-Electromyostimulation on resting metabolic rate, anthropometric and neuromuscular parameters in the elderly. The training and ElectroStimulation trial (TEST). J Strength Cond Res. 2010;24(7):1880–1886.
Kemmler W, Birlauf A, von Stengel S. Einfluss von Ganzkörper-Elektromyostimulation auf das Metabolische Syndrom bei älteren Männern mit metabolischem Syndrom. Dtsch Z Sportmed. 2010;61(5):117–23.
van Buuren F, Mellwig KP, Prinz C, Korber B, Frund A, Fritzsche D, Faber L, Kottmann T, Bogunovic N, Dahm J, et al. Electrical myostimulation improves left ventricular function and peak oxygen consumption in patients with chronic heart failure: results from the exEMS study comparing different stimulation strategies. Clin Res Cardiol. 2013;102(7):523–34.
Kemmler W, Teschler M, Weissenfels A, Sieber C, Freiberger E, von Stengel S. Prevalence of sarcopenia and Sarcopenic obesity in community-dwelling German men 70+ using various established definitions. Osteo Int. 2017;28(6):1881–1889.
Studenski SA, Peters KW, Alley DE, Cawthon PM, McLean RR, Harris TB, Ferrucci L, Guralnik JM, Fragala MS, Kenny AM, et al. The FNIH sarcopenia project: rationale, study description, conference recommendations, and final estimates. J Gerontol A Biol Sci Med Sci. 2014;69(5):547–58.
Baumgartner RN. Body composition in healthy aging. Ann N Y Acad Sci. 2000;904:437–48.
Kemmler W, Bebenek M, Engelke K, von Stengel S. Impact of whole-body electromyostimulation on body composition in elderly women at risk for sarcopenia: the training and ElectroStimulation trial (TEST-III). Age (Dordr). 2014;36(1):395–406.
von Stengel S, Bebenek M, Engelke K, Kemmler W. Whole-Body Electromyostimulation to Fight Osteopenia in Elderly Females: The Randomized Controlled Training and Electrostimulation Trial (TEST-III). J Osteoporos. 2015;Volume 2015:Article ID 643520.
Wahl P, Hein M, Achtzehn S, Bloch W, Mester J. Acute effects of superimposed electromyostimulation during cycling on myokines and markers of muscle damage. J Musculoskelet Neuronal Interact. 2015;15(1):53–9.
Wirtz N, Zinner C, Doermann U, Kleinoeder H, Mester J. Effects of loaded squat exercise with and without application of superimposed EMS on physical performance. J Sports Sci Med. 2016;15(1):26–33.
Filipovic A, Kleinoder H, Dormann U, Mester J. Electromyostimulation--a systematic review of the influence of training regimens and stimulation parameters on effectiveness in electromyostimulation training of selected strength parameters. J Strength Cond Res. 2011;25(11):3218–38.
Kemmler W, Wittke A, Bebenek M, Fröhlich M, von Stengel S. High intensity resistance training methods with and without protein supplementation to fight cardiometabolic risk in middle-aged males a randomized controlled trial. Biomed Res Int. 2016; https://doi.org/10.1155/2016/9705287.
Kemmler W, Weineck J, Kalender WA, Engelke K. The effect of habitual physical activity, non-athletic exercise, muscle strength, and VO2max on bone mineral density is rather low in early postmenopausal osteopenic women. J Musculoskelet Neuronal Interact. 2004;4(3):325–34.
McAuley E, Konopack JF, Motl RW, Rosengren K, Morris KS. Measuring disability and function in older women: psychometric properties of the late-life function and disability instrument. J Gerontol A Biol Sci Med Sci. 2005;60(7):901–9.
Honaker J, King G. Blackwell M. Amelia II: A program for missing data JSS. 2011;45(7):1–47.
Alison P. Missing data. Thousand Oaks: Sage Publication; 2002.
Holm S. A Simple sequentially rejective multiple test procedure. Scand J Stat. 1979;6(1):65–70.
DESTATIS. Statistisches Jahrbuch 2015 [Statistical yearbook 2015]. Wiesbaden, Germany: Statistisches Bundesamt; 2015.
Robert-Koch-Institut: Daten und Fakten: Ergebnisse der Studie »Gesundheit in Deutschland aktuell 2012«. In: Beiträge zur Gesundheitsberichterstattung des Bundes. Edited by RKI. Berlin; 2014.
Wittmann K, Sieber C, von Stengel S, Kohl M, Freiberger E, Jakob F, Lell M, Engelke K, Kemmler W. Impact of whole body electromyostimulation on cardiometabolic risk factors in older women with sarcopenic obesity: the randomized controlled FORMOsA-sarcopenic obesity study. Clin Interv Aging. 2016;11:1697–706.
Bunout B, Barrera G, de la Maza P, Avendano M, Gattas V, Petermann M, Hirsh S. Effects of nutritional supplementation and resistance training on muscle strength in free living elders. Results of one year follow. J Nutr Health Aging. 2004;8(2):68–75.
Daly RM, O'Connell SL, Mundell NL, Grimes CA, Dunstan DW, Nowson CA. Protein-enriched diet, with the use of lean red meat, combined with progressive resistance training enhances lean tissue mass and muscle strength and reduces circulating IL-6 concentrations in elderly women: a cluster randomized controlled trial. Am J Clin Nutr. 2014;99(4):899–910.
Cermak NM, Res PT, de Groot LC, Saris WH, van Loon LJ. Protein supplementation augments the adaptive response of skeletal muscle to resistance-type exercise training: a meta-analysis. Am J Clin Nutr. 2012;96(6):1454–64.
Chale A, Cloutier GJ, Hau C, Phillips EM, Dallal GE, Fielding RA. Efficacy of whey protein supplementation on resistance exercise-induced changes in lean mass, muscle strength, and physical function in mobility-limited older adults. J Gerontol A Biol Sci Med Sci. 2013;68(6):682–90.
Kukuljan S, Nowson CA, Sanders K, Daly RM. Effects of resistance exercise and fortified milk on skeletal muscle mass, muscle size, and functional performance in middle-aged and older men: an 18-mo randomized controlled trial. J Appl Physiol. 2009;107(6):1864–73.
Verdijk LB, Jonkers RA, Gleeson BG, Beelen M, Meijer K, Savelberg HH, Wodzig WK, Dendale P, van Loon LJ. Protein supplementation before and after exercise does not further augment skeletal muscle hypertrophy after resistance training in elderly men. Am J Clin Nutr. 2009;89(2):608–16.
Bendtsen LQ, Lorenzen JK, Bendsen NT, Rasmussen C, Astrup A. Effect of dairy proteins on appetite, energy expenditure, body weight, and composition: a review of the evidence from controlled clinical trials. Adv Nutr. 2013;4(4):418–38.
Chungchunlam SM, Henare SJ, Ganesh S, Moughan PJ. Dietary whey protein influences plasma satiety-related hormones and plasma amino acids in normal-weight adult women. Eur J Clin Nutr. 2015;69(2):179–86.
Acheson KJ, Blondel-Lubrano A, Oguey-Araymon S, Beaumont M, Emady-Azar S, Ammon-Zufferey C, Monnard I, Pinaud S, Nielsen-Moennoz C, Bovetto L. Protein choices targeting thermogenesis and metabolism. Am J Clin Nutr. 2011;93(3):525–34.
Gentile CL, Ward E, Holst JJ, Astrup A, Ormsbee MJ, Connelly S, Arciero PJ. Resistant starch and protein intake enhances fat oxidation and feelings of fullness in lean and overweight/obese women. Nutr J. 2015;14:113.
Coker RH, Miller S, Schutzler S, Deutz N, Wolfe RR. Whey protein and essential amino acids promote the reduction of adipose tissue and increased muscle protein synthesis during caloric restriction-induced weight loss in elderly, obese individuals. Nutr J. 2012;11:105.
Kim JE, O'Connor LE, Sands LP, Slebodnik MB, Campbell WW. Effects of dietary protein intake on body composition changes after weight loss in older adults: a systematic review and meta-analysis. Nutr Rev. 2016;74(3):210–24.
Tahavorgar A, Vafa M, Shidfar F, Gohari M, Heydari I. Whey protein preloads are more beneficial than soy protein preloads in regulating appetite, calorie intake, anthropometry, and body composition of overweight and obese men. Nutr Res. 2014;34(10):856–61.
Pal S, Ellis V, Dhaliwal S. Effects of whey protein isolate on body composition, lipids, insulin and glucose in overweight and obese individuals. Br J Nutr. 2010;104(5):716–23.
Fekete AA, Givens DI, Lovegrove JA. Can milk proteins be a useful tool in the management of cardiometabolic health? An updated review of human intervention trials. Proc Nutr Soc. 2016;75(3):328–41.
Bemben MG, Witten MS, Carter JM, Eliot KA, Knehans AW, Bemben DA. The effects of supplementation with creatine and protein on muscle strength following a traditional resistance training program in middle-aged and older men. J Nutr Health Aging. 2010;14(2):155–9.
Bunout D, Barrera G, de la Maza P, Avendano M, Gattas V, Petermann M, Hirsch S. The impact of nutritional supplementation and resistance training on the health functioning of free-living Chilean elders: results of 18 months of follow-up. J Nutr. 2001;131(9):2441S–6S.
Campbell WW, Crim MC, Young VR, Joseph LJ, Evans WJ. Effects of resistance training and dietary protein intake on protein metabolism in older adults. Am J Phys. 1995;268(6 Pt 1):E1143–53.
Eliot KA, Knehans AW, Bemben DA, Witten MS, Carter J, Bemben MG. The effects of creatine and whey protein supplementation on body composition in men aged 48 to 72 years during resistance training. J Nutr Health Aging. 2008;12(3):208–12.
Iglay HB, Apolzan JW, Gerrard DE, Eash JK, Anderson JC, Campbell WW. Moderately increased protein intake predominately from egg sources does not influence whole body, regional, or muscle composition responses to resistance training in older people. J Nutr Health Aging. 2009;13(2):108–14.
Weinheimer EM, Conley TB, Kobza VM, Sands LP, Lim E, Janle EM, Campbell WW. Whey protein supplementation does not affect exercise training-induced changes in body composition and indices of metabolic syndrome in middle-aged overweight and obese adults. J Nutr. 2012;142(8):1532–9.
Nowson C, O'Connell S. Protein requirements and recommendations for older people: a review. Nutrients. 2015;7(8):6874–99.
Chen LK, Liu LK, Woo J, Assantachai P, Auyeung TW, Bahyah KS, Chou MY, Chen LY, Hsu PS, Krairit O, et al. Sarcopenia in Asia: consensus report of the Asian working Group for Sarcopenia. J Am Med Dir Assoc. 2014;15(2):95–101.
Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, Martin FC, Michel JP, Rolland Y, Schneider SM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European working group on sarcopenia in older people. Age Ageing. 2010;39(4):412–23.
Fielding RA, Vellas B, Evans WJ, Bhasin S, Morley JE, Newman AB, Abellan van Kan G, Andrieu S, Bauer J, Breuille D, et al. Sarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. International working group on sarcopenia. J Am Med Dir Assoc. 2011;12(4):249–56.
Schutz Y, Kyle UU, Pichard C. Fat-free mass index and fat mass index percentiles in Caucasians aged 18-98 y. Int J Obes Relat Metab Disord. 2002;26(7):953–60.
Johnson Stoklossa CA, Forhan M, Padwal RS, Gonzalez MC, Prado CM. Practical considerations for body composition assessment of adults with class II/III obesity using bioelectrical impedance analysis or dual-energy X-ray absorptiometry. Curr Obes Rep. 2016;5(4):389–96.
Ling CH, de Craen AJ, Slagboom PE, Gunn DA, Stokkel MP, Westendorp RG, Maier AB. Accuracy of direct segmental multi-frequency bioimpedance analysis in the assessment of total body and segmental body composition in middle-aged adult population. Clin Nutr. 2011;30(5):610–5.
Melzer K. Carbohydrate and fat utilization during rest and physical activity. ESPEN. 2011;6:e45–52.
Westerterp-Plantenga MS. Protein intake and energy balance. Regul Pept 2008;149(1–3):67–69.
Kemmler W, Froehlich M, von Stengel S, Kleinöder H. Whole-body Electromyostimulation – the need for common sense! Rationale and guideline for a safe and effective training. Dtsch Z Sportmed. 2016;67(9):218–21.
Calvani R, Joseph AM, Adhihetty PJ, Miccheli A, Bossola M, Leeuwenburgh C, Bernabei R, Marzetti E. Mitochondrial pathways in sarcopenia of aging and disuse muscle atrophy. Biol Chem. 2013;394(3):393–414.
Sullivan-Gunn MJ, Lewandowski PA. Elevated hydrogen peroxide and decreased catalase and glutathione peroxidase protection are associated with aging sarcopenia. BMC Geriatr. 2013;13:104.
Schafer I, von Leitner EC, Schon G, Koller D, Hansen H, Kolonko T, Kaduszkiewicz H, Wegscheider K, Glaeske G, van den Bussche H. Multimorbidity patterns in the elderly: a new approach of disease clustering identifies complex interrelations between chronic conditions. PLoS One. 2010;5(12):e15941.
Acknowledgements
The authors would like to express their thanks for the support from the non-profit organization and health sport club “Netzwerk Knochengesundheit e.V.”.
Funding
The paper presented independent research and was partially funded by the non-profit organization and health sport club “Netzwerk Knochengesundheit e.V.”. The funding body played no role in this study and had no influence on the study design, data collection, analysis and interpretation of the data, and in writing the manuscript.
Availability of data and materials
The datasets used and analyzed during the present study are available from the corresponding author (WK) on reasonable request.
Author information
Authors and Affiliations
Contributions
All authors (WK, MK, EF, CS, SvS) contributed substantially to the conception and design of the study, participated in drafting and revising the article and gave final approval of the submitted version. WK, MK and SvS also helped in the acquisition, analysis and interpretation of the data.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the ethics committee of the FAU Erlangen-Nürnberg (Ethikantrag 67_15b)Footnote 8 and complied with the Helsinki Declaration “Ethical Principles for Medical Research Involving Human Subjects“. After detailed information, all study participants gave their written informed consent. The FranSO-trial was fully registered in ClinicalTrials.gov, trial registration number: NCT02857660; registration date: 05/01/2017; registered title: Effect of Whole Body Electromyostimulation and/or Protein Supplementation on Sarcopenic Obesity in 70+ (FRANSO).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kemmler, W., Kohl, M., Freiberger, E. et al. Effect of whole-body electromyostimulation and / or protein supplementation on obesity and cardiometabolic risk in older men with sarcopenic obesity: the randomized controlled FranSO trial. BMC Geriatr 18, 70 (2018). https://doi.org/10.1186/s12877-018-0759-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-018-0759-6