
Abstract
Background
Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) can induce a stronger regenerative ability than traditional 2-stage hepatectomy (TSH). ALPPS has become popular for achieving fast hypertrophy in patients with an insufficient future liver remnant (FLR). However, ALPPS is associated with high morbidity and mortality. Partial ALPPS is a variation that may decrease the morbidity and mortality. The purpose of this study was to perform a meta-analysis comparing outcomes of ALLPS and partial ALLPS.
Methods
PubMed, Embase, and Cochrane Library databases were searched for studies comparing partial ALPPS and complete ALPPS up to April 2019. Included studies were assessed by the Newcastle-Ottawa Scale (NOS). Weighted mean difference (WMD)/standard mean difference (SMD) and odds ratios (OR) with 95% confidence intervals (CIs) were calculated to compare FLR, time interval between stages, postoperative complications, and mortality between partial and complete ALPPS.
Results
Four studies including 124 patients were included. FLR hypertrophy of partial ALPPS was comparable to complete ALPPS (p = 0.09). The time interval between stages was not different between the 2 procedures (p = 0.57). The postoperative complications rate of partial ALPPS was significantly lower than that of complete ALPPS (OR = 0.38; p = 0.03). The mortality rate of partial ALLPS (4.9%) was lower than that of complete ALLPS (18.9%), but the difference was not significant (OR = 0.37; p = 0.12).
Conclusions
Partial ALLPS is associated with similar FLR hypertrophy and time interval between stages as complete ALLPS, and a lower complication rate. Further studies are needed to examine patient selection and outcomes of the 2 procedures.
Similar content being viewed by others


Background
Hepatectomy is the most effective treatment for large and/or multiple liver tumors [1]. However, an extensive hepatectomy cannot be performed if there will be an insufficient future liver remnant (FLR) because it may lead to post-hepatectomy liver failure (PHLF). To minimized PHLF, 20 to 25% of liver is needed in healthy livers while 30–35% in diseased livers [2]. In traditional 2-stage hepatectomy, liver hypertrophy can be induced after stage 1 by portal vein embolization (PVE) or portal vein ligation (PVL), and thus the FLR can meet the size requirement for the second stage procedure [3]. However, liver regeneration is slow making the time interval between the 2 stages long [4].
In 2007, Schlitt et al. performed the first “in-situ split” procedure [5], which was then named “Associating Liver Partition and Portal vein ligation for Staged hepatectomy” (ALPPS) by Clavien. ALPPS was performed by separating the future liver remnant and the diseased hemi-liver in the first stage with an in-situ split, in combination with PVL. Schnitzbauer et al. reported that ALPPS could induce rapid hypertrophy of the FLR (median FLR hypertrophy of 74% in 9 days) [5]. However, a serious complication (Clavien-Dindo > grade 3) rate of 44% and a mortality rate of 12% has limited the application of ALPPS [5].
Since the creation of the ALPPS Registry and the adoption of more stringent patient selection criteria, the overall mortality rate has dropped to 9% and serious complication rate to 27% [6]. Patients younger than 60 years old and those with colorectal cancer liver metastases (CRLM) have lower morbidity and mortality rates when they undergo ALPPS, while the prognosis for patients with gallbladder cancer or cholangiocarcinoma is poor. Technical modifications of ALPPS, such as partial ALPPS, tourniquet ALPPS, radiofrequency and microwave ALPPS, and mini-ALPPS have also been shown to be associated with reduced morbidity and mortality [7]. Partial ALPPS was described by Alvarez et al. [8], and consists of dividing the portal vein of the diseased hemi-liver up to middle hepatic vein. Compared with complete ALPPS, partial ALPPS induces comparable FLR hypertrophy with a lower morbidity rate and near zero mortality rate [8, 9]. However, Chan et al. have argued that complete ALPPS induces more rapid FLR hypertrophy than partial ALPPS, while not affecting the perioperative risk in chronic liver diseases [10]. As such, it is difficult to draw a firm conclusion due to the limited power of individual studies.
Thus, the purpose of this study was to conduct a meta-analysis comparing partial ALPPS with complete ALPPS with respect to FLR hypertrophy, the time interval between stages, postoperative complications, and mortality.
Methods
Study design and search strategy
PubMed, Embase, and Cochrane Library databases were searched up to April 2019, using the terms: “partial ALPPS” OR “p-ALPPS” OR “partial associating liver partition and portal vein ligation for staged hepatectomy”. We included studies without language or year restrictions, and the reference lists of all relevant studies were reviewed for additional potentially relevant studies.
Inclusion and exclusion criteria
Studies were included when they met the following criteria: (1) Described the complete or partial ALPPS technique; (2) Were aimed at comparing FLR hypertrophy, time interval between stages, postoperative complication, and/or mortality. The excluded criteria were: (1) Studies using an animal model; (2) Non-comparative studies, review articles, letters, case reports, or journal editorials.
Data extraction
Information extracted from the studies included author names, year of publication, number of patients, patient demographic data, indications for surgery, amount of parenchymal transection, FLR hypertrophy, time interval between stages, postoperative complications, and mortality rate. Two investigators extracted the data independently. A third investigator participated in when disagreements existed. We attempted to contact the study authors to obtain original data that could not be extracted from an article, but did not receive any reply.
Quality assessment and statistical analysis
The modified Newcastle-Ottawa Scale was used to assess the quality of included studies. Data were collected following the Quality of Reporting of Meta-Analyses statement. Publication bias was assessed by the construction and visual inspection of funnel plots. Statistical analysis was performed according to instructions in the Cochrane Reviewer’s Handbook.
Weighted mean difference (WMD)/standard mean difference (SMD) and odds ratio (OR) and 95% confidence interval (CI) and a fixed-effects model was used to compare continuous and dichotomous variables. Values of P < 0.05 were considered to indicate a statistically significant difference. When the mean and standard deviation (SD) were not reported, median and range values were used to calculate the mean and SD with the formulas reported by Wan et al. [11] and Luo et al. [12]. All statistical analyses were performed using Review Manager version 5.2 for Windows (Cochrane Collaboration, Oxford, UK). Statistical heterogeneity was evaluated with a forest plot, chi-square test. and I2 statistic. If heterogeneity was observed, a random-effects model of analysis was used; otherwise a fixed-effects model was employed.
Results
Literature search
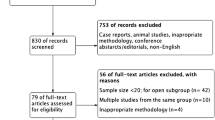
A flow diagram of the literature search results, including the reasons for excluding studies, is shown in Fig. 1. Ninety-two publications were identified from the database searches, and no relevant publications were identified by examining the study reference lists. Twenty-nine publications were excluded on account of duplication, and 44 were excluded after screening the titles and abstracts. Finally, 19 full-text articles were reviewed. Of those articles, 2 reviews, 2 commentaries, 1 case report, and 3 abstract only were excluded. Three articles about other variations of ALPPS (1 about mini-ALPPS, and 2 about ALPTIPS) and 3 articles with no comparison group were excluded. Another article was excluded because of data duplication. Finally, 4 clinical studies containing 124 patients were included in the meta-analysis.

Flow diagram of study selection
Characteristics of the included studies
In the 4 included studies [8,9,10, 13], 62 patients received partial ALPPS and 62 patients received complete ALPPS. In the study by Alvarez et al. 1 patient underwent both stages of ALPPS by a pure laparoscopic technique. All of the other patients in the 4 studies had ALPPS performed by the open approach. The basic characteristics of the included studies are summarized in Table 1. All studies were designed to compare the outcomes between partial ALPPS and complete ALPPS, and all studies were retrospective studies. Assessed by the NOS, all studies received a score of > 5 stars (Table 2).
FLR hypertrophy
Because the study by Petrowsky et al. [9] reported no significant difference in FLR hypertrophy between partial and complete ALPPS (60% vs. 61%) without any other relevant information, only the other 3 studies were summarized in Fig. 2. SMD was used for comparison because different indexes of measurement were used in these studies. Moderate heterogeneity was observed between the studies (chi-square = 6.48; df = 2; p = 0.04; I2 = 69%). The results indicated that FLR hypertrophy in the partial ALPPS group and complete ALPPS group was comparable (SMD = − 0.49; 95% CI: − 1.26-0.28; p = 0.21).

Forest plot and meta-analysis of future liver remnant regeneration
Time interval between stages
The study by Alvarez et al. [8] only reported a total median time interval of 7 days, without range, for both groups. Thus, we only summarized the other 3 studies in Fig. 3. Moderate heterogeneity was observed between the studies (chi-square = 6.50; df = 2; p = 0.04; I2 = 69%). Analysis indicated there was no difference in the time interval between stages between the complete ALPPS and partial ALPPS groups (WMD = − 1.66; 95% CI: − 8.58-5.26; p = 0.64).

Forest plot and meta-analysis of the time interval between stages
Postoperative complications
All 4 studies were included in the analysis of postoperative complications (Fig. 4). Moderate heterogeneity was observed between the studies (chi-square = 7.58; df = 3; p = 0.06; I2 = 60%). In partial ALPPS group, 43.5% of patients experienced postoperative complications, which was significantly lower than the 56.5% observed in the complete ALPPS group (OR = 0.38; 95% CI: 0.16–0.90; p = 0.03).

Forest plot and meta-analysis of postoperative complications
Mortality rate
The study by Alvarez et al. [8] only reported a total mortality rate of 6.60% for both groups. Thus, only the other 3 studies were included in the analysis (Fig. 5). Moderate heterogeneity was observed between the studies (chi-square = 4.88; df = 3; p = 0.09; I2 = 59%). The analysis showed a 4.9% mortality rate in the partial ALPPS group, and a 18.9% mortality rate in the complete ALPPS group; however, the difference was not statistically significant (OR = 0.37; 95% CI: 0.11–1.29; p = 0.12).

Forest plot and meta-analysis of mortality after stage 2 operation
Discussion
The results of this meta-analysis indicated that FLR hypertrophy and time between stages were not different between partial ALPPS and complete ALPPS. However, the postoperative complications rate in the partial ALPPS group was significantly lower than that in the complete ALPPS group, and while the mortality rate in the partial ALPPS group was markedly lower than in the complete ALPPS group the difference did not reach statistical significance.
Although ALPPS has become very popular for achieving fast hypertrophy of the FLR, the high morbidity and mortality of the procedure are important obstacles for its use. Mortality rates of 15–20% have been reported, even by experienced centers [14,15,16,17]. Alvarez et al. suggested that partial parenchymal transection could reduce morbidity without negatively impacting FLR hypertrophy [8]. Petrowsky et al. reported that partial ALPPS was associated with a zero postoperative mortality rate, and lower morbidity than complete ALLPS [9]. Based on clinical and experimental evidence, Linecker et al. reported that at least 50% of the liver needed to be transected in partial ALPPS to trigger equal volume hypertrophy as observed in complete ALPPS [13]. In the articles included in the current meta-analysis, partial ALPPS induced comparable FLR hypertrophy with a lower postoperative complications rate, consistent with prior reports. However, in 2017 Chan et al. reported an opposite result; complete ALPPS induced more rapid FLR hypertrophy than partial ALPPS while not affecting the perioperative risk [10]. Since this study was the only one that included patients with hepatocellular carcinoma (HCC), more studies are required to establish outcomes of ALLPS in patients with HCC.
The mechanism by which ALPPS induces rapid FLR hypertrophy is not clear. There are 2 main hypotheses that have been put forward to account for this phenomenon. One is that the redistribution of portal vein flow causes hypertrophy, which is based on the hypertrophy observed in patients with increased blood flow due to a portal vein embolization (PVE) [18]. Another hypothesis is that growth factors released in response to tissue injury trigger liver regeneration. Experiments using animal models strongly support the hypothesis of growth factors. Injection of plasma from ALPPS animals has been shown to induce rapid liver regeneration in animals that have not undergone ALPPS [19]. In addition, levels of interleukin (IL)-6 and tumor necrosis factor α (TNFα) are elevated after stage 1 hepatectomy in animal models and humans [19]. An interesting study by Langiewicz et al. found a clinical relevance between the Indian hedgehog (Ihh) pathway and ALPPS: liver regeneration was achieved through the hedgehog signaling pathway after both chemical injury and resection. Rapid regeneration, similar to that seen with ALPPS, was observed after administration of recombinant Ihh after PVL, while this phenomenon was blocked by neutralization of Ihh [20]. This suggests that ALPPS activates liver regeneration via the Ihh pathway.
The reason partial ALPPS is safer than complete ALLPS is likely because it is less invasive [21, 22]. Similarly, laparoscopy-assisted ALPPS [23, 24], mini ALPPS [25], and portal vein embolization ALPPS adopt less invasive operative strategies to split the diseased hemi-liver in stage 1, which enhances the tolerability of the stage 2 operation. It is important to understand that the degree of liver partitioning affects FLR hypertrophy, and determines the timing and operative strategy of stage 2. As shown in Table 1, at least 50% liver transection is needed to induce a degree of liver regeneration comparable to complete ALPPS. Time interval between the 2 stages is generally accepted as a factor that determines the surgical difficulty of stage 2; a longer time interval between stages increases the difficulty of the second stage due to greater adhesions [10].
In spite of the potential benefits, a complete ALPPS may not be applied due to difficulty of parenchymal transection in some cases. For example, when a large tumor stretching the middle hepatic vein in right anterior section, it may cause severe venous bleeding during complete ALPPS. A tumor located close to the IVC or caudate also is not feasible for complete ALPPS. In these situations, a p-ALPPS may be preferred and our study may provide essential information.
There are limitations to this study. The included studies were retrospective, and lack the powerful evidence of randomized controlled trials (RCTs), which are still absent with respect to this topic. The indications for ALLPS varied among the studies. In addition, the scarcity of available literature comparing partial and complete ALPPS and the exiguous number of patients hampered the quality of the results.
Conclusion
The results of this meta-analysis indicated that FLR hypertrophy and time between stages were not different between partial ALPPS and complete ALPPS. However, the postoperative complications rate in the partial ALPPS group was significantly lower than that in the complete ALPPS group, and while the mortality rate in the partial ALPPS group was markedly lower than in the complete ALPPS group the difference did not reach statistical significance. More studies are needed to confirm the benefits of partial ALLPS, and indications for the procedure.
Availability of data and materials
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Abbreviations
- ALPPS:
-
associating liver partition and portal vein ligation for staged hepatectomy
- CRLM:
-
colorectal liver metastases
- FLR:
-
future liver remnant
- HCC:
-
Hepatocellular Carcinoma
- Ihh :
-
Indian hedgehog
- NOS:
-
Newcastle-Ottawa Scale
- OR:
-
odds ratio
- PHLF:
-
posthepatectomy liver failure
- PVE:
-
portal vein embolization
- PVL:
-
portal vein ligation
- RCT:
-
randomized controlled trials
- SMD:
-
standard mean difference
- TSH:
-
two-stage hepatectomy
- WMD:
-
Weighted mean difference
References
Agrawal S, Belghiti J. Oncologic resection for malignant tumors of the liver. Ann Surg. 2011;253:656–65.
Clavien PA, Petrowsky H, DeOliveira ML, Graf R. Strategies for safer liver surgery and partial liver transplantation. N Engl J Med. 2007;356:1545–59.
Jaeck D, Oussoultzoglou E, Rosso E, Greget M, Weber JC, Bachellier P. A two-stage hepatectomy procedure combined with portal vein embolization to achieve curative resection for initially unresectable multiple and bilobar colorectal liver metastases. Ann Surg. 2004;240:1037–49 1049-1051.
Abulkhir A, Limongelli P, Healey AJ, Damrah O, Tait P, Jackson J, et al. Preoperative portal vein embolization for major liver resection: a meta-analysis. Ann Surg. 2008;247:49–57.
Schnitzbauer AA, Lang SA, Goessmann H, Nadalin S, Baumgart J, Farkas SA, et al. Right portal vein ligation combined with in situ splitting induces rapid left lateral liver lobe hypertrophy enabling 2-staged extended right hepatic resection in small-for-size settings. Ann Surg. 2012;255:405–14.
Schadde E, Ardiles V, Robles-Campos R, Malago M, Machado M, Hernandez-Alejandro R, et al. Early survival and safety of ALPPS: first report of the international ALPPS registry. Ann Surg. 2014;260:829–36 836-838.
Lang H, de Santibanes E, Schlitt HJ, Malago M, van Gulik T, Machado MA, et al. 10th anniversary of ALPPS-lessons learned and quo Vadis. Ann Surg. 2019;269:114–9.
Alvarez FA, Ardiles V, de Santibanes M, Pekolj J, de Santibanes E. Associating liver partition and portal vein ligation for staged hepatectomy offers high oncological feasibility with adequate patient safety: a prospective study at a single center. Ann Surg. 2015;261:723–32.
Petrowsky H, Gyori G, de Oliveira M, Lesurtel M, Clavien PA. Is partial-ALPPS safer than ALPPS? A single-center experience. Ann Surg. 2015;261:e90–2.
Chan A, Chok K, Dai J, Lo CM. Impact of split completeness on future liver remnant hypertrophy in associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) in hepatocellular carcinoma: complete-ALPPS versus partial-ALPPS. Surgery. 2017;161:357–64.
Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:135.
Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27:1785–805.
Linecker M, Kambakamba P, Reiner CS, Linh NT, Stavrou GA, Jenner RM, et al. How much liver needs to be transected in ALPPS? A translational study investigating the concept of less invasiveness. Surgery. 2017;161:453–64.
Li J, Girotti P, Konigsrainer I, Ladurner R, Konigsrainer A, Nadalin S. ALPPS in right trisectionectomy: a safe procedure to avoid postoperative liver failure? J Gastrointest Surg. 2013;17:956–61.
Schadde E, Ardiles V, Slankamenac K, Tschuor C, Sergeant G, Amacker N, et al. ALPPS offers a better chance of complete resection in patients with primarily unresectable liver tumors compared with conventional-staged hepatectomies: results of a multicenter analysis. World J Surg. 2014;38:1510–9.
Nadalin S, Capobianco I, Li J, Girotti P, Konigsrainer I, Konigsrainer A. Indications and limits for associating liver partition and portal vein ligation for staged hepatectomy (ALPPS). Lessons learned from 15 cases at a single Centre. Z Gastroenterol. 2014;52:35–42.
Kremer M, Manzini G, Hristov B, Polychronidis G, Mokry T, Sommer CM, et al. Impact of Neoadjuvant chemotherapy on hypertrophy of the future liver remnant after associating liver partition and portal vein ligation for staged hepatectomy. J Am Coll Surg. 2015;221:717–28.
Goto Y, Nagino M, Nimura Y. Doppler estimation of portal blood flow after percutaneous transhepatic portal vein embolization. Ann Surg. 1998;228:209–13.
Schlegel A, Lesurtel M, Melloul E, Limani P, Tschuor C, Graf R, et al. ALPPS: from human to mice highlighting accelerated and novel mechanisms of liver regeneration. Ann Surg. 2014;260:839–46 846-847.
Langiewicz M, Schlegel A, Saponara E, Linecker M, Borger P, Graf R, et al. Hedgehog pathway mediates early acceleration of liver regeneration induced by a novel two-staged hepatectomy in mice. J Hepatol. 2017;66:560–70.
Linecker M, Kron P, Lang H, de Santibanes E, Clavien PA. Too many languages in the ALPPS: preventing another tower of babel? Ann Surg. 2016;263:837–8.
Edmondson MJ, Sodergren MH, Pucher PH, Darzi A, Li J, Petrowsky H, et al. Variations and adaptations of associated liver partition and portal vein ligation for staged hepatectomy (ALPPS): many routes to the summit. Surgery. 2016;159:1058–72.
Schelotto PB, Gondolesi G. Laparoscopy in ALPPS procedure: when we can do it? Ann Surg. 2017;265:e30–1.
Machado MA, Makdissi FF, Surjan RC. Totally laparoscopic ALPPS is feasible and may be worthwhile. Ann Surg. 2012;256(e13):e16–9.
de Santibanes E, Alvarez FA, Ardiles V, Pekolj J, de Santibanes M. Inverting the ALPPS paradigm by minimizing first stage impact: the mini-ALPPS technique. Langenbeck's Arch Surg. 2016;401:557–63.
Acknowledgements
Not applicable.
Funding
This work was supported by National Natural Science Foundation of China, China [81873591, and 81670591]; National undergraduate innovation training programs [201801132, and 201701099]; Guangdong undergraduate innovation training programs [201801290]; Guangdong Natural Science Foundation, China [2016A030311028]; The Science and Technology Planning Project of Guangdong Province, China (2018A050506030); and Science and Technology Program of Guangzhou, China [201704020073]. The fundings supported the data collection used in this study and the English-language editing service. The fundings has no role in the design of the study and analysis and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
Conceptualization: XW, YM; Investigation and Statistical analysis: XW, JR, XZ; Writing original manuscript: XW; Writing review & editing: XW, RD; Funding acquisition: YM. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Wu, X., Rao, J., Zhou, X. et al. Partial ALPPS versus complete ALPPS for staged hepatectomy. BMC Gastroenterol 19, 170 (2019). https://doi.org/10.1186/s12876-019-1090-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-019-1090-1