
Abstract
Background
People with a severe mental illness (SMI) have shorter life expectancy and poorer quality of life compared to the general population. Most years lost are due to cardiovascular disease, respiratory disease, and various types of cancer. We co-designed an intervention to mitigate this health problem with key stakeholders in the area, which centred on an extended consultations for people with SMI in general practice. This study aimed to1) investigate general practitioners’ (GPs) experience of the feasibility of introducing extended consultations for patients with SMI, 2) assess the clinical content of extended consultations and how these were experienced by patients, and 3) investigate the feasibility of identification, eligibility screening, and recruitment of patients with SMI.
Methods
The study was a one-armed feasibility study. We planned that seven general practices in northern Denmark would introduce extended consultations with their patients with SMI for 6 months. Patients with SMI were identified using practice medical records and screened for eligibility by the patients’ GP. Data were collected using case report forms filled out by practice personnel and via qualitative methods, including observations of consultations, individual semi-structured interviews, a focus group with GPs, and informal conversations with patients and general practice staff.
Results
Five general practices employing seven GPs participated in the study, which was terminated 3 ½ month ahead of schedule due to the COVID-19 pandemic. General practices attempted to contact 57 patients with SMI. Of these, 38 patients (67%) attended an extended consultation, which led to changes in the somatic health care plan for 82% of patients. Conduct of the extended consultations varied between GPs and diverged from the intended conduct. Nonetheless, GPs found the extended consultations feasible and, in most cases, beneficial for the patient group. In interviews, most patients recounted the extended consultation as beneficial.
Discussion
Our findings suggest that it is feasible to introduce extended consultations for patients with SMI in general practice, which were also found to be well-suited for eliciting patients’ values and preferences. Larger studies with a longer follow-up period could help to assess the long-term effects and the best implementation strategies of these consultations.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
People with a severe mental illness (SMI), defined as psychotic disorders, bipolar disorders, and severe degree of depressive disorder, have a 10 to 20-year shorter life expectancy than the general population [1,2,3,4,5,6,7]. Most years lost are due to cardiovascular disease, respiratory disease, and various types of cancer [4, 8,9,10,11].
Several interventions have tried to address this disparity on multiple levels, i.e. interventions addressing individual, institutional, and socio-environmental risk factors [12], yet they have proved unsuccessful [12, 13]. Contrary to former interventions in the area, the SOFIA project ascribes a pivotal role to primary healthcare in improving the somatic health and quality of life of people with SMI [14]. This project is distinct from earlier attempts to develop interventions for this population group due to its effort in co-designing the intervention with patients, caretakers, and general practitioners (GPs) [15].
The SOFIA project began in 2017 with a 2-year co-design phase that co-developed the intervention in collaboration with relevant stakeholders aiming to align its design with the needs and challenges of patients, general practice, and other stakeholders [15]. The following themes became apparent from the co-design phase: GPs were concerned with the lack of time allocated for addressing what mattered to patients with SMI, and they needed tools to strengthen the patient-doctor relationship with this particular patient group (Jønsson ABR, Svanholm SL, Brodersen JB, Reventlow S, Brostrøm M: General practitioners’ experiences of providing somatic care for patients with severe mental illness: a qualitative study, forthcoming). Further, patients with SMI felt they were not always taken seriously when presenting somatic symptoms in general practice. Often, they were not physically examined and felt misunderstood by health care professionals [16].
Developing the preliminary SOFIA intervention
Based on findings from the co-design phase, the SOFIA project group developed a preliminary intervention that centred on GPs providing an extended consultation for patients with SMI (up to 45 min). Additionally, GPs received information on relevant collaborative care initiatives and an introductory meeting on conducting the extended consultation using the SOFIA scheme [14] (Table 1).
The extended consultation should be conducted by a GP and was fully reimbursed financially. The extended consultation aimed to ensure patient-centeredness and shared-decision making in planning care, e.g. ending the extended consultation with a shared care plan. It also included a focused health examination and medication review by the GP.
In developing this intervention, we adopted a patient-centred care approach. Patient-centred care can be defined as care that elicits individuals’ values and preferences. Once expressed, it allows this to guide all aspects of the individual’s healthcare, supporting their realistic health and life goals [17, 18]. German philosopher Martin Buber propagated in the 1920s the need for doctors to approach patients in a patient-centred manner. Buber called for a shift in focus from the disease to, first and foremost, attending to patients as human beings [19]. In general practice, we find patient-centred care to be the practice of caring for patients in ways that are meaningful and valuable to the individual patient [20]. Patient-centred care relies on the GPs’ clinical expertise in examination, diagnostics, and treatment decisions and on the GPs’ ability to involve the patients’ narrative, i.e. personal preferences and values in the consultation [21, 22]. In Denmark, general practice is known for continuity- and patient-centred care [23]. However, many find patient-centred consultations challenging to conduct with patients with SMI (Jønsson ABR, Svanholm SL, Brodersen JB, Reventlow S, Brostrøm M: General practitioners’ experiences of providing somatic care for patients with severe mental illness: a qualitative study, forthcoming).
Need for feasibility testing of the preliminary intervention
When presented with the SOFIA intervention design, several GPs, researchers, and stakeholders voiced concerns that general practice would not have the time and personnel to introduce extended consultations into routine care. It was also unclear how patients would experience being invited to an extended consultation on the GP’s initiative and how they would experience the consultation. Furthermore, many trial-related aspects concerning the feasibility of conducting a trial in general practice were unknown, including how to identify, eligibility screen, and recruit patients.
Therefore, we wanted to study these key uncertainties related to the feasibility of introducing an extended consultation in general practice to patient with SMI. Thus, the aims of the feasibility study were threefold: 1) to investigate how GPs experienced the feasibility of introducing an extended consultation for patients with SMI, 2) to assess the clinical content of extended consultations and how these were experienced by patients with SMI, and 3) to investigate the feasibility of identification, eligibility screening, and recruitment of patients with SMI.
Methods
Design
This study was a single-arm intervention study. In keeping with other studies, we use the term feasibility study as an umbrella term for any study that aims to support the development of a future study [24,25,26]. Since we primarily used qualitative methods to assess the study aims, we report its methods and findings using relevant items from the CONSORT extension for Pilot and Feasibility Trials [27] and the COREQ criteria for qualitative research [28] (Additional file 1).
The study in the context of other complex intervention phases of the SOFIA project
The study was planned to last 6 months from mid-January 2020. However, the study was terminated ahead of schedule by the end of March due to the Covid-19 pandemic. We could conclude from the preliminary data collected during the study that a more rigorous and comprehensive pilot study was needed. We found that many aspects concerning the feasibility of the intervention, and its implementation in general practice, were suboptimal or needed more extensive investigation, e.g. how to ensure fidelity to the preferred delivery of the intervention. Using the evidence obtained in this feasibility study, we planned the design of a subsequent pilot study [14].
The context of general practice in Denmark
In Denmark, GPs are organized within local groups (Danish: klynger) that collaborate on supervision, courses, and small-scale local quality improvement projects relevant to their everyday clinical practice [29, 30]. One group of GPs from the northern part of Jutland approached the SOFIA project group for advice about a local quality improvement project they were planning to improve care for patients with complex multimorbidity [31]. The GPs and the SOFIA project group agreed to collaborate on patients with SMI as an exemplary case for caring for patients with complex multimorbidity in general practice. The GPs received support for improving their quality of care for patients with SMI by participating in the SOFIA feasibility study, i.e. agreeing to participate in interviews, following formal eligibility screening criteria and other trial-related tasks.
Setting and participants
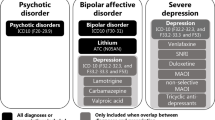
Patients with SMI were identified from patient records using the diagnostic system International Classification of Primary Care version 2 corresponding to psychotic disorders, bipolar disorder or severe depression (Fig. 1). In each general practice, the GP screened the patient record for eligible patients using the eligibility criteria (Fig. 1). Subsequently, practice personnel contacted eligible patients by phone and invited them to a 10-min conversation in the general practice. Here, practice personnel informed them about the study, and informed consent was obtained if the patient was eligible.

Patient eligibility and selection of patients according to their main SMI diagnosis
The intervention
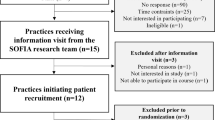
GPs attended a 3-h introductory course, defining the start of the study. Here, the intended conduct of the extended consultation was discussed with GPs to promote fidelity. The GPs also received guidance on carrying out study-related tasks, i.e. identifying, eligibility screening, and recruiting patients, and documenting these tasks and the clinical outcomes of the extended consultation. GPs received written materials to ensure correct documentation and guidance during the consultation. Following the introductory meeting, the staff at each general practice made a list of potentially eligible patients (see inclusion criteria in Fig. 1), which GPs subsequently screened for eligibility (see Fig. 2). Patients agreeing to participate in the study were asked to fill out one survey concerning the generic quality of life (the EQ5D5L survey [32]) and one survey on needs and preferences relating to life quality [33], which, if permitted by the patient, could be discussed during the consultation with the GP.

Patient flow chart in general practices
The extended consultation
The consultation was to comprise up to 45 min and follow the SOFIA scheme (Table 1) inspired by the patient-centred consultation model [34], divided into a patient part, a practitioner part, and a shared part. This consultation model intended to permit time for the patient to express their illness experiences, preferences and values, a dialogue about the patient’s quality of life, and a focused physical examination personalized to the patient’s medical history and complaints alongside a medication review. The consultation concluded with a dialogue between the GP and the patient about further potential diagnostic follow-up and, if relevant, changes to current treatment or referral to specialists or services in the municipality, i.e. shared decision-making. GPs were to schedule follow-up appointments as needed.
Data collection
The study evaluated the feasibility and content of the extended consultation from qualitative and quantitative data. In each general practice, three types of case report forms were filled out. Practice personnel filled out the first and second case report forms, which contained information about the number of patients recruited for the study and the characteristics of study participants, respectively. The GPs filled out the third case report form, which contained information about changes to the care plan following the extended consultation (Table 2).
A medical anthropologist (MS) observed the recruitment process in general practices and conducted interviews and informal conversations with GPs and staff. Extended consultations were observed and field notes made by MS following the provision of consent by both GP and patient, and whenever possible, given that several extended consultations took place simultaneously across general practices. In total, 20 (53%) extended consultations were observed. Additionally, 98 h of observation were conducted in general practice during the study period. This part of data collection focused on the clinic’s organization and everyday work life and how extended consultations were made to fit into this setting.
All participating GPs were interviewed following a semi-structured interview guide, and patients were additionally informally interviewed concerning their experiences with the extended consultation. Repeat interviews were carried out as needed. All interviews lasted between 9 and 25 min. Additionally, a 2-h focus group was conducted, entailing the use of the fishbowl technique [35] and plenum discussion. Here, all participating GPs and junior general medicine doctors participated, and AJ, JBB, MS and FM facilitated the focus group.
Interviews were audio-recorded, and observations were documented via field notes. Both were structured via an interview and observation guide, respectively. These covered four main themes concerning the intervention: (1) Experiences and perceptions of the extended consultation; (2) Challenges arising when conducting the extended consultation; (3) Content of the consultation; (4) Relevant changes in treatment or care planning following the extended consultation and four themes concerning feasibility of conducting the trial: (1) General information about the practice, (2) Recruitment and the patients included in the project, (3) Patient access to the practice, and (4) Introduction to the study and data collection. The guides (Additional file 2) were adapted and adjusted pragmatically to fit the particular context and GPs or patients involved, i.e. regarding practicalities or themes arising during the study.
Analysis
MS and a student worker transcribed all interviews. Transcripts were not returned to GPs or patients for comment or correction. MS and AJ analyzed transcripts and field notes following an interpretative phenomenological analysis (IPA) [36] allowing for a detailed examination of the main questions in the study. The IPA method is particularly valuable in this setting as it enables the micro-level reading of participants’ experiences [36]. IPA allows for detailed analysis of formal interviews, informal talks, and field notes before moving to more general claims, ensuring that all participants are equally heard. Transcripts were coded by MS and subsequently grouped under three main themes: Experiences with extended consultations, challenges related to conducting the extended consultations, and content of the extended consultation. We intended to provide participants the opportunity to give feedback on the findings. However, due to early termination because of the COVID-19 pandemic, this was not possible. AJ translated the informants’ quotes into English. NVivo12 software was used to manage the data.
Results
Before the study commenced, seven general practices expressed interest in participating. Two general practices withdrew participation, one due to time constraints and one due to illness among practice staff. The five remaining general practices employed seven GPs (Table 3).
Feasibility of introducing extended consultations for people with SMI in general practice
We identified 478 patients with SMI. Of these, 73 (15%) were diagnosed with a psychotic disorder, 61 (13%) had bipolar disorder, and 344 (72%) had depression. Across the three diagnostic groups, 141 (45%) patients met the inclusion criteria. Due to the early termination of the study caused by the COVID-19 pandemic, only 57 (40%) of the 141 eligible patients were contacted. Of these, 41 (72%) agreed to participate, but one patient did not show up, and two cancelled their appointment. Thus, of those contacted, 38 (67%) attended an extended consultation (Table 4).
Nine patients could not be reached, and seven declined participation (Fig. 2).
Experiences with extended consultations
In informal conversations before the study commenced, GPs expressed feeling overwhelmed by the amount of information provided during the introductory meeting. In addition, GPs expressed concerns that 45 min allocated to a single consultation would prove too long for patients. Moreover, since consultations in general practice usually last 10 to 15 min, the GPs anticipated that introducing the extended consultation into practice would give rise to logistical problems. In practice, all GPs found it possible to introduce extended consultations into routine care, although opinions diverged concerning possible disadvantages to other patients. Here, some GPs voiced concerns that spending additional time on a few selected patients came at the cost of other patients at the clinic due to the limited time available to GPs.
The GPs’ initial concern about whether patients with SMI would be capable of enduring an extended consultation proved unfounded. Instead, extended consultations with GPs appeared to elicit patients’ interest:
Well, I found it quite easy just to call them [patients] (…) the majority just said yes (…) so it’s been going really well (…) and it is the possibility of seeing the doctor for a longer consultation that has been attracting the patients (Resident in general medicine, focus group)
From conversations with patients, it was clear that patients found that the extended consultation was beneficial, noting that it indicated that the healthcare system was prioritizing their concerns, which the participating patients recounted that they had rarely experienced. One patient used the extended consultation as an opportunity to hand the GP a plastic bag containing books and notes that he felt the GP ought to see to understand him, which was important to him (Field note, March 2020). In informal conversations, patients expressed that it made a positive difference in their healthcare that they were a) invited to come and thus did not feel that they were taking up unnecessary time and b) that they could address more problems in the extended consultation as opposed to regular consultations. Patients also expressed an interest in participating in research, given the possibility of improving their health and helping other patients with SMI. Two patients (5%) described a negative experience with the extended consultation, experiencing that their GP was unwilling to address their concerns, strengthening their belief in the futility of consulting their GP when they had health problems.
Challenges related to conducting extended consultations
Conducting extended consultations presented challenges. Despite instructions shared at the introductory meeting and in the study pamphlet, in observed consultations, GPs faced difficulties adhering to the SOFIA scheme:
“Because we just do as we’re used to, right? Well, you get this antipsychotic and then we do this and this. And then I would be like, and how are things? I mean, you always pose these questions (…) but this is different” (GP7)
Also, the instructions in the SOFIA scheme were met with some reluctance:
“I don’t think it makes any sense that I have to use the stethoscope (…) It [the stethoscope] has little to no sensitivity and specificity, it’s more of a symbolic act that we do. So well, I’d rather write [in the SOFIA scheme] that it’s an option, not a requirement” (GP1)
Practical challenges also arose in the conduct of extended consultations. Critical tasks in general practices meant that extended consultations were often interrupted with questions or comments by staff or medical residents. This was perceived as frustrating by both GPs and patients.
Cancellations and patient no-shows likewise proved challenging. Two consultations were cancelled, and one patient did not attend a planned consultation (See Fig. 2). One patient cancelled the appointment for the extended consultation at the last minute leading to frustration from the GP about the concept of an extended consultation due to the “loss of” 45 min in the context of a tight schedule. Two GPs managed the risk of non-attendance by planning extended consultations either at the end of the day, when a no-show would be less inconvenient or during morning hours, when non-attendance would leave room for acute patients. Management of non-attendance resulted in overall greater satisfaction with the intervention among these GPs. However, placing an extended consultation, during which GPs and patients often discussed quite complex issues, at the end of the day also proved difficult for a GP on one occasion, leading to the GP ending the consultation before time as she had difficulty discussing complex issues that late in the day.
Content of the extended consultation
All GPs agreed that the duration of the extended consultation both enabled patients to set the agenda and led to a discussion of complex challenges faced by patients formerly unknown to the GP:
“It has been four very different consultations, with different themes. It could be loneliness, it could be work-related issues, and then one of them [patients] just needed to talk. And talk and talk and talk. And from that arose physical challenges or complaints. So there’s been more than enough to discuss, and I’ve also had the feeling that they [patients] have been very happy that they felt time had been allocated to them contrary to a usual consultation which lasts maybe 10 min, right?” (GP6, focus group)
Another GP expressed how the allocation of additional time allowed for further elaboration of the individual aspects of patients’ challenges:
“In my experience, so many of these conversations with patients are about being lonely or not being able to be there for one’s loved ones. That’s usually what bothers them the most (…) and then we try to locate the roots of that feeling. Sometimes it’s just regular physical challenges that we just never have discussed. For instance, one is incontinent and wearing a diaper. So she is reluctant to see other people, and [GP realizes] ‘we never made that gynaecological exam’ (…) or another one having severe trembling making her fall on the street, and she feels so sad because it prevents her from going to dances, which is her only hobby. She’s 70 (…) so I decide to get that checked, is it side effects of her meds or is it her Parkinson’s disease which is developing fast?” (GP5)
Hence, the structure of the SOFIA scheme allowed for discussion of whatever was experienced by the patient as a symptom, sensation, or challenge. Elicitation of patient preferences and values took up most of the agenda for the extended consultation. For example, one consultation included a discussion of family dynamics, identity, and blood pressure (P11), another focused on alcohol treatment (P1), and yet another consultation centred around ways of engaging in exercise while also revealing that the patient wished for increased continuity of interaction with the GP (P13).
Notwithstanding what the GPs perceived to be benefits of the extended consultation, they found it challenging to adhere to the SOFIA scheme, especially regarding allowing the patient to set the agenda for the conversation. In as many as eight consultations (21%), it was observed that the GP struggled with the task of allowing patients’ values and needs to guide the consultation. Instead, many GPs set the focus of the conversation in line with their perceptions of what mattered most. For instance, one GP dismissed a patient’s complaint concerning conflict with social workers as out of their hands (P20). In another example, a patient’s primary concern related to a physical ailment that the GP deemed benign and temporary, steering the conversation towards other issues, causing great frustration for the patient (Field note, February 2020).
During observed consultations, most GPs did not perform focused physical examinations of the patients as intended. Instead, prefilled surveys about patients’ quality of life unintendedly became the centrepiece of the consultation in place of somatic symptoms and concerns. Based on observations, none of the GPs used the recommended algorithm for medication review nor materials to support adherence to the SOFIA scheme, i.e. guiding material on how to structure and conduct the extended consultation.
Changes to the care plan after extended consultations
Overall, 31 of the 38 patients attending the extended consultation (82%) experienced at least one change in their treatment or care as a direct result of the extended consultation (Table 5).
Changes to healthcare provision included scheduling blood samples or other diagnostic procedures for somatic health concerns, follow-up visits concerning mental health problems, recommendations concerning lifestyle changes, and help reducing substance use. 26% of patients were referred to other specialist health care providers or social care. Reasons for referral included assessing lung function at a pulmonologist, medication or diagnostic assessment at a psychiatrist, and requesting more support for the patient from the municipality.
Discussion
Summary of main findings
We found that extended consultations were feasible to plan and execute with acceptable procedures for identification, eligibility screening and recruitment of patients and relatively high participation from patients, except for a few occasions when patients did not attend the consultation. This finding contradicted concerns initially expressed by GPs relating to the practicalities of time constraints in-clinic and patients’ capacity to endure such long consultations. All GPs agreed that extended consultations on several occasions demonstrated the possibility of enabling increased consideration of patients’ individual preferences and values. In 82% of consultations, patients had a change in their health care plan. These changes were primarily scheduling follow-up visits and referrals to other specialists or care in the municipality. The effects of these changes on the care of the health of study participants require studies with a longer follow-up time. Regrettably, we could not assess whether the feasibility or conduct of extended consultations would change over time, e.g. potential improvements in fidelity due to training, due to the early termination of the study because of the COVID-19 pandemic.
Introducing extended consultations in general practice was not without logistical challenges. For example, three patients (8%) either cancelled or did not attend the extended consultation. General practitioners and patients were frustrated when consultations were interrupted due to other patients with acute health problems, which required the GP’s immediate attention. Another concern for GPs was whether extended consultations might come at the cost of other patients, something we could not assess in this study. Regarding adherence to the SOFIA scheme, it appeared from observations of extended consultations that most often, GPs did not perform a physical examination as intended, nor did they use the recommended algorithm for medication review and materials to support adherence to the SOFIA scheme. Following this, and that GPs had felt overwhelmed by information on the introductory seminar, we see a need for a full-day course before GPs execute this intervention. Despite the low fidelity to the SOFIA scheme, both GPs and patients found that the consultations were beneficial. Despite the co-design phase, our data show the need for feasibility studies. This owes to the limitations of co-design as being discussed with selected participants in workshops, whereas this feasibility study have tested the intervention in real-life settings in general practice.
Strengths and limitations
The study has several strengths. First, the study’s rationale and design are well-grounded in theory and based on a 2-year co-design process involving patients and key stakeholders [37, 38]. Second, as the intervention was tested in everyday general practice settings, findings likely indicate those to be encountered should the intervention be introduced into routine general practice. Third, the study was conducted in line with the recommendation of the Medical Research Council [26], advocating for a stepped approach to trials of complex interventions. Fourth, we used multiple data sources, i.e. field notes, interviews with both GPs and patients and a focus group with GPs, which strengthens our information power for the interpretations drawn in this publication [39].
The study’s main limitation was its premature termination due to the COVID19 pandemic, limiting the number of patients included and shortening the follow-up time after patients’ extended consultation. This premature termination of the study hindered the assessment of potential changes regarding the feasibility of introducing extended consultations in general practice and potential improvement in fidelity to conduct of the consultations, i.e. adherence to the SOFIA scheme. Secondly, the premature termination of the study limited the time that general practices had to adopt the intervention and adapt it to their local usual-care practices. More time would possibly have led to the improved conduct of extended consultations, i.e., fidelity to the SOFIA scheme. More time would also have allowed for investigating whether the GPs’ and the patients’ views about extended consultations would change over time.
Furthermore, general practices had to cancel in-person follow-up consultations after the initial extended consultation due to the pandemic and resulting lockdown. This arguably had a negative influence on the introduction of extended consultations into routine care, both in terms of adaptation to the new work routines around the consultations and concerning the patients’ experiences of the value of the consultations. Thirdly, our study was based on supporting GPs in their local quality improvement project, simultaneously getting insight into how extended consultations would be implemented into routine care by simply introducing the concept and providing information about the recommended conduct of such consultations. As the GPs and practices who participated in the feasibility study also needed instruction on how to report data to the research team, a substantial amount of the instructional meeting was spent on how to accurately report data. We believe this contributed to the low fidelity to the intervention, as more detailed information on the SOFIA model was then only distributed in a written format, which most of the GPs likely did not find time to read. We would argue that a more detailed and rigorous implementation strategy, e.g., hosting training courses, providing videos or other examples of preferred conduct, having supervision practices set up and the like, would have increased fidelity to the extended consultation since GPs did find that intervention acceptable and meaningful for patients. In effect, changes to healthcare demonstrated in our study are likely conservative in terms of the true potential effects of these consultations. Fourthly and to the contrary, the GPs recruited for the trial represents a selected sample of GPs that were interested in the topic and on their own initiative had made contact to the SOFIA research group, which arguably reduces the generalizability of findings, and perhaps could lead to issues with reproducing the acceptability of the intervention in future studies.
Possibilities for patient-centred care in extended consultations
Results show that extended consultations provide a suitable setting for attending to patients’ individual preferences and values, both in terms of the content and conduct of the extended consultation and regarding the shared care plan following the discussion. It also allows GPs to accommodate multiple problems in parallel, and GPs may receive adequate guidance on conducting extended consultations, e.g. proper dialogue with GPs about how to ensure fidelity to the SOFIA scheme [14]. Here, we understand values as referring to a moral and cultural orientation and preferences as personal feelings towards different treatment options for mental and somatic illnesses [40]. As shown, the extended consultation allowed patients’ various concerns to be addressed, even when the concern was more social than medical, as a starting point for the consultation. In contrast with regular consultations, the extended time frame allowed attention to somatic, mental, and social concerns.
One of the most articulated dimensions of patient-centred care is the therapeutic relationship [20], which builds on a constructive relationship, prioritizing respectful communication between patient and physician [41]. We saw such therapeutic relationships enacted in several extended consultations when GPs followed instructions, allowing patients’ perspectives to guide the plan.
Our data underline the importance of eliciting patients’ individual preferences and values, given that life circumstances influence patients’ experiences of their illness and treatment [42, 43]. Our data showed large variation in what mattered to patients and thus the importance of allowing patients to set the agenda, which allowed patients to bring their life stories and circumstances into the conversation to determine what matters most to the individual patient and investigate sensations and symptoms that might indicate underdiagnosed or undertreated somatic illnesses. Most patients with SMI are managed poorly with usual primary care arrangements due to their significant and complex social and health challenges [44, 45] and a general unequal provision of care, emphasizing the importance of patient-centred care [46, 47]. This calls for a patient-centred approach encompassing life circumstances and patient perspectives reflected in a constructive therapeutic relationship. Another important dimension of patient-centred care is the biopsychosocial holistic approach [20], in which care is thought to encompass all domains of health, i.e. biophysical, cognitive, emotional, behavioural, and social domains [41].
Last, it should be noted, that while the extended consultation in the SOFIA scheme must be done by a GP owing to the possible need for diagnosing new conditions, follow-up consultations and yearly controls could be executed by other healthcare professionals, e.g. some practices have well-functioning relations between patients with SMI and the practice nurse, and the nurse already perform some of these consultations for already known co-morbidities in the patient.
Implications for practice
This feasibility study demonstrates that conducting extended health consultations for patients with SMI in the general practice setting is feasible. However, we also offer several suggestions for improved future implementation. A core premise for conducting extended consultations in general practice is allocating sufficient time. One worry is the current scarcity of GPs in Denmark, already burdened by a large patient load [48, 49]. Based on the above mentioned results and discussions, we hypothesise that extended consultations with patients in marginalized or vulnerable positions may in the long run release time as complications from undertreated and underdiagnosed conditions can be avoided. Extended consultations may also mitigate the inverse care law, by giving more time to those most in need [50]. This hypothesis require further investigation. In addition, time is also necessary for patient-centred care and a well-functioning patient-GP relationship [51, 52]. Yet, time constraints are typical for general practice care. Introducing extended consultations into general practice, therefore, does also require a cultural change in regards to the time allocated to individual patients. Importantly, such changes also require sufficient reimbursement for the resources required in the collective efforts related to introducing extended consultations into general practice, e.g. identifying patients, screening potentially eligible patients, contacting eligible patients, and conducting extended consultations and resulting follow-up measures.
Our findings also highlight the importance of ensuring that various implementation strategies are used to ensure fidelity to the intervention, e.g., providing clear instructions and engaging GPs in a dialogue about the intended conduct of the extended consultation, i.e., using the SOFIA scheme. Thus, for future extended consultations and future studies, it is recommended to host a comprehensive introductory course to ensure fidelity to the intended conduct of the extended consultation, i.e., fidelity to the SOFIA scheme (Table 1). This point relates to the generally well-accepted value of involving a diverse range of stakeholders when co-designing complex interventions [53].
It has been suggested that physical exams should be performed as a routine component of extended consultations for patients with SMI [54]. This group is less likely to be offered medical investigations, tests, or referrals for further check-ups [55,56,57]. We found that many GPs did not perform physical exams during extended consultations, although this was the intent of the SOFIA scheme (Table 1). This suggests that implementation strategies are needed to promote this change in usual care. However, it will be important to find the right balance between allowing GPs to make and act upon clinical judgment while ensuring fidelity to the essential elements of the extended consultation, e.g., physical examination, commonly referred to as promoting fidelity in function while allowing variance in the form of the intervention [58].
It is paramount for the feasibility of introducing extended consultations in general practice that patients are willing to participate, and that practice personnel can contact and recruit them for the intervention. Our findings regarding acceptable procedures for identification, eligibility screening and recruitment of patients and the relatively high participation rate of patients that can be hard to reach, and few cancellations and “no-shows”, suggests an acceptable clinical feasibility of implementing our patient recruitment strategy in general practice.
Future research
Due to the small size of this study and its premature termination, we cannot conclude whether we have succeeded in recruiting “the right patients”, i.e. those patients who will benefit from the intervention. This question will be further investigated in future trials [14]. Future research should investigate the direct and indirect costs of introducing extended consultations for selected “high-risk patient groups”, e.g. people that are marginalized, vulnerable, and often have complex care needs, as the provision of more time for some patients might come at the expense of other patients. Additionally, we found that most, but not all, patients appreciated being contacted and taking part in the study. Hence, future research should investigate the potentially negative effects of contacting vulnerable patients and how these can be mitigated. Building on the findings from this feasibility study, other aspects related to the feasibility of the SOFIA intervention will be pilot tested in a cluster-randomized two-arm pilot trial [14].
Conclusion
The findings of this study show that it is feasible to introduce extended consultations for patients with SMI in general practice, as evidenced by high participation rates, with the majority of contacted patients agreeing to participate in the study and only three patients not attending the extended consultation. General practices and patients with SMI additionally found this type of intervention acceptable. Although extended consultations were described as well-suited to eliciting patients’ values and preferences, challenges were identified related to the GPs’ adherence to the SOFIA scheme for the conduct of the extended consultations, marking the importance of proper guidance for GPs. Finally, we conclude that general practices require financial reimbursement for the time allocated, and also in the case of patient non-attendance, to make extended consultations financially feasible for general practitioners.
Availability of data and materials
The dataset(s) supporting the conclusions of this article are included within the article, following guidance on preparing raw clinical data for publication [59].
Abbreviations
- CONSORT:
-
Consolidated Standards of Reporting Trials
- COREQ:
-
Consolidated criteria for reporting qualitative research
- EQ5D5L:
-
EuroQol 5 Dimension 5 Level survey
- GP:
-
General practitioner
- IPA:
-
Interpretative phenomenological analysis
- KEU:
-
An acronym in Danish for “Kvalitets- og EfterUddannelsesudvalget”, directly translated it means the Committee for Quality and Continued Education
- N:
-
Number
- P:
-
Patient
- SMI:
-
Severe mental illness
- SOFIA:
-
An acronym in Danish for”Sammen Om Fysisk og psykisk helbred IAlmen praksis, directly translated it means (working) Together for Physical and Mental Health in General Practice
References
De Hert M, et al. Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry. 2011;10(1):52–77.
World Health O. Helping people with severe mental disorders live longer and healthier lives: policy brief. Geneva: World Health Organization; 2017.
Wahlbeck K, et al. Outcomes of Nordic mental health systems: life expectancy of patients with mental disorders. Br J Psychiatry. 2011;199(6):453–8.
Lawrence D, Hancock KJ, Kisely S. The gap in life expectancy from preventable physical illness in psychiatric patients in Western Australia: retrospective analysis of population based registers. BMJ. 2013;346:f2539.
Chang CK, et al. Life expectancy at birth for people with serious mental illness and other major disorders from a secondary mental health care case register in London. PLoS One. 2011;6(5):e19590.
Hiroeh U, et al. Death by homicide, suicide, and other unnatural causes in people with mental illness: a population-based study. Lancet. 2001;358(9299):2110–2.
Harris EC, Barraclough B. Suicide as an outcome for mental disorders. A meta-analysis. Br J Psychiatry. 1997;170:205–28.
Laursen TM, Munk-Olsen T, Gasse C. Chronic somatic comorbidity and excess mortality due to natural causes in persons with schizophrenia or bipolar affective disorder. PLoS One. 2011;6(9):e24597.
Crump C, et al. Comorbidities and mortality in persons with schizophrenia: a Swedish national cohort study. Am J Psychiatry. 2013;170(3):324–33.
Kugathasan P, et al. Coronary artery calcification and mortality risk in patients with severe mental illness. Circ Cardiovasc Imaging. 2019;12(3):e008236.
Kugathasan P, et al. Association of physical health multimorbidity with mortality in people with schizophrenia spectrum disorders: using a novel semantic search system that captures physical diseases in electronic patient records. Schizophr Res. 2019;75(12):1234–40.
Liu NH, et al. Excess mortality in persons with severe mental disorders: a multilevel intervention framework and priorities for clinical practice, policy and research agendas. World Psychiatry. 2017;16(1):30–40.
Speyer H, et al. The CHANGE trial: no superiority of lifestyle coaching plus care coordination plus treatment as usual compared to treatment as usual alone in reducing risk of cardiovascular disease in adults with schizophrenia spectrum disorders and abdominal obesity. World Psychiatry. 2016;15(2):155–65.
Rozing MP, et al. The SOFIA pilot trial: a cluster-randomized trial of coordinated, co-produced care to reduce mortality and improve quality of life in people with severe mental illness in the general practice setting. Pilot Feasibility Stud. 2021;7(1):168.
Reventlow S, Jønsson AB, Møller MCR, Davidsen AS, Olsen L. Co-producing healthcare interventions: transforming transdisciplinary research to develop healthcare services to meet the needs of patients with complex problems. In: Sturmberg J, editor. Embracing complexity in health: the transformation of science, practice, and policy. Springer International Publishing; 2019. https://link.springer.com/book/10.1007/978-3-030-10940-0.
Christensen I, Risør M, Grøn L, Reventlow S. Senses of touch the absence and presence of touch in health care encounters of patients with mental illness. Cult Med Psychiatry. 2023. Accepted for publication.
Paparella G. Person-centred care in Europe: a cross-country comparison of health system performance, strategies and structures. Oxford: Picker Institute; 2016.
CoulouridesKogan A, Wilber K, Mosqueda L. Moving toward implementation of person-centered care for older adults in community-based medical and social service settings: “You only get things done when working in concert with clients.” J Am Geriatr Soc. 2016;64(1):e8-14.
Buber M. I and Thou. New York: Howard Books; 2008.
Langberg EM, Dyhr L, Davidsen AS. Development of the concept of patient-centredness - a systematic review. Patient Educ Couns. 2019;102(7):1228–36.
Hvas L. Retten til at være rask i en diagnosekultur. In: Brinkmand APS, editor. Diagnoser. Perspektiver, kritik og diskussion. Klim; 2015. p. 319–340.
Schlesinger M, et al. Taking patients’ narratives about clinicians from anecdote to science. N Engl J Med. 2015;373(7):675–9.
Haggerty JL, et al. Continuity of care: a multidisciplinary review. BMJ. 2003;327(7425):1219–21.
Eldridge SM, et al. Defining feasibility and pilot studies in preparation for randomised controlled trials: development of a conceptual framework. PLoS One. 2016;11(3):e0150205.
Whitehead AL, Sully BGO, Campbell MJ. Pilot and feasibility studies: Is there a difference from each other and from a randomised controlled trial? Contemp Clin Trials. 2014;38(1):130–3.
Council TMR. Developing and evaluating complex interventions. In: Council TMR, editor. 2006.
Eldridge SM, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ (Clinical research ed). 2016;355:i5239–i5239.
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–57.
Larsen AT, Klausen MB, Højgaard B. Primary health care in the Nordic countries – comparative analysis and identification of challenges. Denmark: VIVE The Danish Center for Social Science Research; 2020.
Bundgaard M, et al. Quality clusters in general practice: associations between cluster organization and general practitioners’ self-reported benefits. Fam Pract. 2022;39(5):852–9.
Harrison C, et al. Examining different measures of multimorbidity, using a large prospective cross-sectional study in Australian general practice. BMJ Open. 2014;4(7):e004694.
Feng Y-S, et al. Psychometric properties of the EQ-5D-5L: a systematic review of the literature. Qual Life Res. 2021;30(3):647–73.
Bissenbakker KH, Møller A, Brodersen J, Jønsson AR. PROMs og livskvalitet: Hvordan måles livskvalitet hos mennesker med multisygdom? Tidsskrift for Forskning I Sygdom Og Samfund. 2020;17(32). https://tidsskrift.dk/sygdomogsamfund/article/view/120975.
Nystrup J, Larsen J-H, Risør O. Developing communication skills for the general practice consultation process. Sultan Qaboos Univ Med J. 2010;10:318–25.
Sutherland R, et al. Teaching a fishbowl tutorial: sink or swim? Clin Teach. 2012;9(2):80–4.
Tindall L, Smith JA, Flower P, Larkin M. Interpretative phenomenological analysis: theory, method and research. Qual Res Psychol. 2009;6(4):346–7.
Reventlow S, et al. Co-producing healthcare interventions: transforming transdisciplinary research to develop healthcare services to meet the needs of patients with complex problems. In: Sturmberg JP, editor., et al., Embracing complexity in health: the transformation of science, practice, and policy. Cham: Springer International Publishing; 2019. p. 169–83.
Davidsen AS, et al. Experiences of barriers to trans-sectoral treatment of patients with severe mental illness. A qualitative study. Int J Ment Health Syst. 2020;14(1):87.
Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26(13):1753–60.
Bastemeijer CM, et al. What do patient values and preferences mean? A taxonomy based on a systematic review of qualitative papers. Patient Educ Couns. 2017;100(5):871–81.
Sidani S, Fox M. Patient-centered care: clarification of its specific elements to facilitate interprofessional care. J Interprof Care. 2014;28(2):134–41.
Hudon C, et al. Measuring patients’ perceptions of patient-centered care: a systematic review of tools for family medicine. Ann Fam Med. 2011;9(2):155–64.
Ishikawa H, Hashimoto H, Kiuchi T. The evolving concept of “patient-centeredness” in patient-physician communication research. Soc Sci Med. 2013;96:147–53.
Gerrity M, Zoller E, Pinson N, Pettinari C, King V. Integrating primary care into behavioral health settings: what works for individuals with serious mental illness. New York: Milbank Memorial Fund; 2014.
Domino ME, et al. Through the looking glass: estimating effects of medical homes for people with severe mental illness. Health Serv Res. 2017;52(5):1858–80.
Hamm JA, Buck KD, Gonzalvo JD. Clinical application of patient-centered diabetes care for people with serious mental illness. Clin Diabetes. 2017;35(5):313.
Rudnick A, Roe D. Foundations and ethics of person-centered approaches to individuals with serious mental illness. In: Rudnick A, Roe D, editors. Serious mental illness: person-centered approaches. New York: Radcliffe Publishing; 2011. p. 8–18.
OECD. Primary care in Denmark. 2017.
Kristensen M, Thorsen T. [Increasing shortage of general practitioners in social deprived Danish communities.]. Ugeskr Læger. 2014;176:V08130497.
Tudor Hart J. The inverse care law. Lancet. 1971;297(7696):405–12.
Damarell RA, Morgan DD, Tieman JJ. General practitioner strategies for managing patients with multimorbidity: a systematic review and thematic synthesis of qualitative research. BMC Fam Pract. 2020;21(1):131.
Davis K, Schoenbaum SC, Audet A-M. A 2020 vision of patient-centered primary care. J Gen Intern Med. 2005;20(10):953–7.
Skivington K, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ. 2021;374:n2061.
UK N. Community mental health services. 2022. Available from: https://www.england.nhs.uk/mental-health/adults/cmhs/.
Dixon LB, et al. A comparison of type 2 diabetes outcomes among persons with and without severe mental illnesses. Psychiatr Serv. 2004;55(8):892–900.
Scott D, Platania-Phung C, Happell B. Quality of care for cardiovascular disease and diabetes amongst individuals with serious mental illness and those using antipsychotic medications. J Healthc Qual. 2012;34(5):15–21.
Mitchell AJ, Delaffon V, Lord O. Let’s get physical: improving the medical care of people with severe mental illness. Adv Psychiatr Treat. 2012;18(3):216–25.
Perez Jolles M, Lengnick-Hall R, Mittman BS. Core functions and forms of complex health interventions: a patient-centered medical home illustration. J Gen Intern Med. 2019;34(6):1032–8.
Hrynaszkiewicz I, et al. Preparing raw clinical data for publication: guidance for journal editors, authors, and peer reviewers. Trials. 2010;11(1):9.
World Medical A. World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. Bull World Health Organ. 2001;79(4):373–4.
Acknowledgements
The SOFIA study group wishes to thank all participating patients, general practitioners, practice staff and others involved. Particularly we would like to express our gratitude to Bolette Friderichsen, general practitioner and president of the Danish College of General Practitioners, for taking the initiative in this collaboration.
Access to patient medical records
According to the Danish Health Care Act, paragraph 42d, section 2, number 1-3, healthcare personnel are authorized to access patients’ medical records and to collect patient information for the purpose of quality improvement without the patients’ informed consent. All participants were anonymized, identifiers altered, and data derived from patients’ medical journals were encrypted. Data were stored and processed per the requirements of European General Data Protection Regulation.
Funding
Open access funding provided by Royal Library, Copenhagen University Library KEU Region North funded this sub-study of the SOFIA project, which is supported by the Novo Nordisk Foundation research grant (NNF16OC0022038) and the Copenhagen Center for Health Technology. None of the funding bodies had any role in the design of the study, the collection, analysis, and interpretation of data, nor in the writing of the manuscript.
Author information
Authors and Affiliations
Contributions
Abbreviations for authors: Jønsson ABR (AJ), Martiny FHJ (FM), Søndergaard MK (MS), Brodersen JB (JBB), Due TD (TD), Nielsen MH (MN), Bakkedal C (CB), Bardram JE (JEB), Bissenbakker K (KB), Christensen I (IC), Doherty K (KD), Kjellberg P (PK), Mercer S (SM), Reventlow S (SR), Rozing MP (MR), Møller A (AM)AJ, FM, SR and MR conceived the original idea; AJ, FM, JBB, SM, SR, MN, KD, TD and MR designed the study; AJ, FM, MS, SR, AM, KD and MR wrote the initial manuscript; JEB, TD, CB, KB, IC, PK, SM and AM provided critical feedback throughout the study and substantial revisions of the manuscript; all authors contributed to the final manuscript, and all authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We applied for ethical approval of the study to the National Committee on Health Research Ethics in Denmark, which decided that the current study was to be considered a quality improvement project (cf. journal number H-20003281). According to the Danish legislation, “komitéloven” (https://www.retsinformation.dk/eli/lta/2017/1083), quality improvement projects do not require ethical approval. Still, the study was conducted in compliance with the Helsinki Declaration in its latest form and good clinical practice guidelines and followed the rules for informed consent [60]. Informed consent was obtained from all study participants after they had been identified in the general practices’ patient medical records and prior to their participation. All study participants, including clinical staff, general practitioners, and patients, were informed about the study before participation via written material and oral explanation. The written material was tailored to the medical personnel and patients with SMI to ensure it was understandable and relevant. The information material was designed using study information and consent form templates from the National Committee on Health Research Ethics in Denmark, supplemented with guidance from the University of Copenhagen. We collected written consent forms from all study participants.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 2.
Interview and observation guide.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jønsson, A.B.R., Martiny, F.H.J., Søndergaard, M.K. et al. Introducing extended consultations for patients with severe mental illness in general practice: Results from the SOFIA feasibility study. BMC Prim. Care 24, 206 (2023). https://doi.org/10.1186/s12875-023-02152-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12875-023-02152-z