
Abstract
Background
The heart rate (HR) method enables estimating oxygen uptake (V̇O2) in physical activities. However, there is a paucity in knowledge about the interchangeability of this method when applied to cycling, walking and running. Furthermore, with the aim of optimization, there is a need to compare different models for establishing HR-V̇O2 relationships.
Methods
Twenty-four physically active individuals (12 males and 12 females) participated. For each participant, two models of HR-V̇O2 relationships were individually established in ergometer cycling, level treadmill walking and running. Model 1 consisted of five submaximal workloads, whereas model 2 included also a maximal workload. Linear regression equations were used to estimate V̇O2 at seven intensity levels ranging between 25 and 85% of heart rate reserve (HRR). The estimated V̇O2 levels were compared between the exercise modalities and models, as well as with data from a previous study.
Results
A high level of resemblance in estimated V̇O2 was noted between running and cycling as well as between running and walking, with both model 1 and model 2. When comparing walking and cycling, the V̇O2 levels for given intensities of %HRR were frequently slightly higher in walking with both models (range of significant differences: 5–12%). The variations of the estimated individual V̇O2 values were reduced when using model 2 compared to model 1, both between and within the exercise modalities.
Conclusion
The HR method is optimized by more workloads and wider ranges. This leads to overall high levels of interchangeability when HR methods are applied in ergometer cycling, level treadmill walking and running.
Similar content being viewed by others
Background
Applying the heart rate (HR) method for interpreting oxygen uptake (V̇O2) in human physical activities can be beneficial for educational purposes, health promotion and disease prevention as well as from research perspectives. This is since our understanding of physical activities’ effects on morbidity, premature mortality and weight control as well as physical performance is largely related to intensities relative to the maximal oxygen uptake (e.g. [1, 2]), energy expenditure (e.g. [3, 4]) and MET hours (e.g. [5]).
The HR method is based on the linear relationship between HR and V̇O2 with increasing workload under steady state conditions, which was established already in the early twentieth century [6, 7]. Since the HR-V̇O2 relationships differ between individuals, especially depending on sex, age, body weight and fitness level (e.g. [8,9,10]), the relationships need to be determined individually. In that way, individual levels of V̇O2 can, in principle, be estimated by HR monitoring for a wide range of intensities (with individual exceptions at very low and very high intensities [11,12,13]). Given the estimated V̇O2 levels, the energy costs can then be calculated based on caloric coefficients ([14], p. 104).
A number of studies have used the HR method for estimating oxygen uptake in both humans [13, 15] and animals [16]. However, in order for the HR method to be used for the purposes mentioned above, it needs to be well methodologically developed. Issues of importance for enhancing this approach are: (1) reproducibility, (2) methods for establishing HR-V̇O2 relationships, (3) validity under various applied conditions during both prolonged constant and intermittent exercise, (4) external validity in terms of interchangeability between different dynamic exercise modalities, and (5) external validity in various groups of individuals.
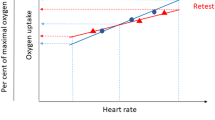
It is only recently that the reproducibility of the HR method has been systematically studied. These examinations, evaluating sedentary activities and treadmill walking [17] as well as ergometer cycling [18, 19], have demonstrated a good reproducibility with minor relative mean differences between test and retest. However, at the individual level, there is a variation that prompts stabilizing the establishment of HR-V̇O2 relationships. This requires further investigations. Possibilities in this respect may include more workloads and wider ranges when establishing the HR-V̇O2 relationships.
With regard to the interchangeability of the HR method between different forms of physical exercise, it has long been known that dynamic exercise using smaller muscle groups, compared to larger, induce a higher heart rate at a given level of V̇O2 [20,21,22]. If instead focusing on various dynamic exercises with only large muscle groups involved, the question of interchangeability is still a rather unexplored research area.
For various reasons, ergometer cycling is a valuable point of departure in this respect. This is because different workloads of ergometer cycling induce known mean levels of V̇O2 at steady state [23,24,25]. This enables the HR method to be used in education as well as in health promotion and disease prevention when a high level of accuracy is not critical. Furthermore, regardless of whether the HR-V̇O2 relationships are established through measurements or estimations of V̇O2, application of the HR method in field conditions is helpful for studies using larger groups of participants. This is since mobile metabolic measurement systems are both costly and technically complicated to use, and can be sensitive to ambient conditions [26, 27].
Given this background, it would be particularly valuable if the HR method, based on ergometer cycling, is interchangeable with other common forms of dynamic exercise that involve large muscle groups, such as walking and running. To our knowledge, Olsson, Salier Eriksson [28], is the only study that has systematically examined this in relation to level walking on treadmill. Although there was a general concordance in estimated mean levels of V̇O2 for given percentages of heart rate reserve (%HRR), there were indications of a reduced individual variation when a maximal workload was added to three submaximal levels of exercise. Indeed, this indicated that varying the ways of establishing HR-V̇O2 relationships can lead to different degrees of methodological optimization. In the present study, we have therefore developed the HR method to include more submaximal workloads (five vs three), and in combination with maximal workloads and wider measurement ranges. The potential optimizing effects will be evaluated through comparisons within the results of the present study as well as with Olsson, Salier Eriksson [28]. Finally, we extend the question about interchangeability through also examining level running on treadmill.
Methods
Participants
Twenty-four healthy and physically active individuals (12 men and 12 women) participated in the study. Most of them were recruited among the students at the Swedish School of Sport and Health Sciences, GIH, Stockholm, Sweden. Others were recruited through various training groups of recreational runners. The inclusion criteria were: man or woman between 20 and 45 years, healthy and injury free, familiar to cycling, walking and running, and performing endurance training regularly, at least 30 min twice a week, during at least the year prior to the study. Anthropometric characteristics and resting HR values for the participants are given in Table 1. Prior to the study, they were informed about the research project and their rights as participants. This information, as well as a health declaration, were sent to them before their start in the study. At the first occasion, a written informed consent of participation was signed of all participants, and they certified themselves to be healthy for participation. An ethical approval to conduct the study was obtained from the Ethics Committee North of the Karolinska Institute at the Karolinska Hospital (Dnr 03–637), Stockholm, Sweden.
Study design, standardization and experimental procedures
The experimental procedures consisted of four different test occasions on the equal amount of days. The first occasion, always conducted in the morning, was a pre-test and included measurements of the resting HR and the resting metabolism (data not used). HR was collected continuously while the subject rested in supine position on a treatment table for 30 min. After this measurement, a familiarization of trying out the equipment followed through performing submaximal exercise in ergometer cycling, level treadmill walking and running. During the three subsequent occasions, the various exercise modalities were performed in a randomized order. The cycling and running occasions, included both submaximal and maximal workloads, while the walking included only submaximal workloads. In most cases, the time of the day when these three sessions were performed varied within two hours for each participant. All four test occasions were initially scheduled at 5–7 day intervals. However, due to illness for some participants, this interval became 8 ± 5 days (mean ± SD). All measurements took place in a laboratory with well-controlled ambient conditions (room temperature 18–21 °C).
The participants were instructed to keep the following standardization procedures prior to the measurements. Before all occasions, they were asked to refrain from vigorous exercise 24 h preceding the tests. They were also asked to avoid stress, to travel to the laboratory in a manner that was not physically strenuous and to cancel the tests if they had either fever, an infection or a cold. Before the first occasion, they were instructed to be fasting in the morning (only water allowed) and refrain from eating at least 8 hours before the test. Prior to the subsequent occasions, instructions were to refrain from eating, consuming coffee, tea and energy drinks, smoking and taking snuff during 1 hour before the tests. Ingestions of heavier meals were allowed at least 3 hours before the tests.
All four occasions started with measurements of body weight (without shoes, but typically with shorts and t-shirts), while the body height was only measured at the first occasion. The measurements from the first occasion were used as baseline values (Table 1). The other measurements of weight were used to describe V̇O2 in relation to body weight when performing the various exercise modalities (Additional file 1: Table S1-S3). At the last three occasions, a measurement of the resting HR followed in a standardized procedure, while the participant rested in supine position on a treatment table for ten minutes. The HR values during the last 5 minutes were averaged. In this way, each occasion was initiated in the same manner, and the individual day-to-day variation could been observed. These intra-individual HR variations were mainly small (absolute median difference: 3.9 beats·min− 1). However, for six individuals their largest differences were between 10.0–15.8 beats·min− 1. This variation was regarded as acceptable.
The submaximal workloads for the three various exercise modalities, were performed with continuous measurements of HR and V̇O2, and continued until steady state had been reached for two consecutive minutes. This was normally attained after 5 minutes. The criterion for steady state was that HR was within 2–3 beats·min− 1. Rating of perceived exertion (RPE), according to Borg’s RPE scale 6–20 [29], was assessed separately for legs and breathing, at the end of each submaximal workload. The maximal cycle ergometer and treadmill tests were performed until voluntary exhaustion occurred. HR and V̇O2 were measured continuously, while RPE for both legs and breathing, respectively, were assessed directly after the tests. In order to ensure that the maximal tests attained their purposes, at least two of the following three criteria were met by each participant: 1) a plateau in V̇O2 despite increasing exercise intensity (defined as a V̇O2 increment of < 150 ml·min− 1), 2) a respiratory exchange ratio of ≥1.10, and 3) a RPE rating of ≥17 [30,31,32].
Ergometer cycling
The cycle exercise included 5–6 uninterrupted submaximal workloads and a maximal test. For all participants, the first five submaximal workloads were: 50, 75, 100, 125 and 150 W. Only these five submaximal workloads have been used in the present study. However, some participants continued and finished a 6th workload, at either 175 or 200 W. The decision on whether the last workload would be 150, 175 or 200 W, was primarily due to HR and RPE at 150 W. If HR was ≥170 beats·min− 1 or if RPE, either legs or breathing, was ≥17, the submaximal phase was ended after 150 W. When HR was between 150 and 169 beats·min− 1 or that RPE, either legs or breathing, was between 15 and 16, 175 W was in general chosen as the last workload. If HR was < 150 beats·min− 1 and RPE, both legs and breathing, was < 15, then 200 W was in all cases chosen as the final workload. Throughout all submaximal workloads, the participants sat in an upright position with their hands laying relaxed on the handlebars, while using a cycling cadence of 50 revolutions per minute (rpm) in accordance with earlier studies [23,24,25]. After the submaximal exercise, approximately 10 min of rest followed before the maximal test. During the last 2 minutes of this period, the participant started to cycle at a light resistance (about 7.4 N) using a self-chosen cadence.
The maximal cycling test was carried out through three different protocols, all using a cadence of 80 rpm. Protocols 1, 2 or 3 were used if the last submaximal workload had been 150, 175 or 200 W, respectively. The starting level was 60 W in all protocols, but during the first minute, each protocol used a varying schedule. Protocol 1 kept constant resistance. The 2nd protocol increased by 40 W after the first 20 s and then by 20 W after the next 20 s. The 3rd protocol increased by 40, 20 and 40 W after each period of 15 s. After the first minute, all protocols increased by 40 W, thereafter the resistance increased by 20 W every continued minute until exhaustion ended the test.
Treadmill walking
Five submaximal workloads of uninterrupted level (inclination 0.0°) walking were used at the following speeds: 3, 4, 5, 6, and 7 km·h− 1.
Treadmill running
Six submaximal workloads of uninterrupted level running and a maximal test were performed. The submaximal speeds were set at: 6, 7, 8, 10, 12 and 13 or 14 km·h− 1. However, only the first five submaximal workloads have been used in the present study. After the submaximal workloads, about 10 min of rest followed before the maximal test. During the last few minutes of this period, the participant walked at a slow pace (about 4 km·h− 1) on the treadmill.
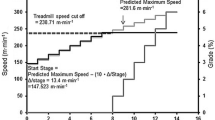
The maximal running test was performed through constant speed and successive increments of inclination every full minute. During the first minute, the inclination was set to 0.0°, after 1 minute it was increased to 1.0°, and then by 0.5° every minute until the test was ended. The constant running speed (12.7 ± 0.9 km·h− 1) was individually selected for each participant. The selection of speed was based on the participants’ general perceived exertion during the submaximal exercise. In agreement with each participant, an individual speed corresponding to approximately 15 on the RPE scale was chosen.
Equipment and preparations
Cycle ergometer and treadmill
The cycle exercise was performed on a manually braked Monark pendulum cycle ergometer 828E (Monark Exercise AB, Vansbro, Sweden). Prior to the study, service and calibration procedures were undertaken according to the manufacturer’s advice. Immediately before each phase of submaximal as well as maximal exercise, the scale was zeroed while the participant sat on the saddle with the feet resting on the surface between the pedals. A digital metronome (DM70 Seiko S-Yard Co. Ltd., Tokyo, Japan) was used to maintain correct cycling cadence. At regular intervals of 1 minute, the work rate was controlled by checking the cadence and the braking force as indicated by the pendulum position. The treadmill exercises were carried out on a RL2500E treadmill (Rodby Innovation AB, Vänge, Hagby, Sweden). Preceding the study, both the speed and the inclination were carefully controlled.
Stationary metabolic system
A stationary metabolic gas analysis system with a mixing chamber, Jaeger Oxycon Pro® (Carefusion GmbH, Hoechberg, Germany), was used during all metabolic measurements. This system has been shown to be valid and reliable [27, 33]. It was switched on around 30 min preceding data collection and calibrations were made prior to each individual test occasion, according to the manufacturer’s recommendations. A high precision gas, composed of 15.00% O2 and 6.00% CO2 (accuracy: O2 ± 0.04% and CO2 ± 0.1%) (Air Liquid AB, Kungsängen, Sweden), was used for calibration. In all tests, the participants wore a face mask, ORO-NASAL (Hans Rudolph Inc., Kansas City, MO, USA) with a lightweight non-rebreathing 3-way valve (Innovision A/S, Odense, Denmark). The valve was connected to a lightweight tube, 1.8 m long, (Innovision A/S, Odense, Denmark) for leading the exhaled air into the mixing chamber.
Heart rate monitor
The HR measurement was performed using a Polar RS400 monitor and the associated Polar WearLink transmitter (Polar Electro, Kempele, Finland).
Data processing and statistical analyses
All HR and V̇O2 values were saved in mean values of 15 s for data processing. For determination of the resting HR, the average of the last 5 minutes from the rest measurement at the first occasion was used. For all submaximal workloads, paired HR and V̇O2 values in the last, of the two consecutive minutes at steady state, have been used. In accordance with Howley, Bassett [31], the maximal HR and V̇O2 values were calculated by averaging the minute with highest continuous paired values. In the calculation of percentages of heart rate reserve (%HRR) during exercise, both the resting and maximal values were used in the equation; ((“exercise HR” - HRrest) · (HRmax - HRrest)− 1) · 100. Furthermore, the calculated relative exercise intensities for ergometer cycling, in terms of HRmax, HRR and V̇O2max, have been based on the maximal cycling values. Conversely, the values from the maximal treadmill test were used to describe the relative intensities for both walking and running.
For application of the HR method, two different models of HR-V̇O2 relationships were individually established for each of the three exercise modalities. These relationships were based on paired HR and V̇O2 values from five submaximal workloads (model 1), plus one maximal workload (model 2), and were calculated as linear regression equations. The HR-V̇O2 relationship in model 2 for cycling, was based on the maximal cycling values, while the HR-V̇O2 relationships for walking and running, respectively, were based on the values from the maximal treadmill test. The individual regression equations were then applied as parts of HR methods for estimating V̇O2 using individually derived HR values based on seven levels of %HRR according to the American College of Sports Medicine (ACSM) classification of exercise intensity [34]. The intensity levels, 25 and 35%HRR (very light to light), 45 and 55%HRR (moderate), and 65, 75 and 85%HRR (vigorous), were selected to cover a wide and commonly used intensity range for physical activity. For this determination of individual HR values, in terms of %HRR, the maximal HR values from the treadmill test were always used.
Exercise mode differences were calculated in both absolute and relative terms for the constituents of regression equations (y-intercept, slope and r2) and the V̇O2 estimations in both model 1 and model 2. Confidence intervals (CI) of 95% were calculated for all these differences as well as the absolute values. In the calculations of the relative differences, cycling was used as the reference value in the comparisons with walking and running, while walking was used as the basis when comparing with running. The absolute and relative exercise mode differences were evaluated jointly for all participants with the one-sample t-test, since no systematic variations were seen between the sexes when analysed with an independent t-test. A Bonferroni post-hoc test ([35], p. 377) was applied since all values in the exercise mode comparisons were analysed twice. Instead of dividing the level of significance with the number of comparisons, the P-values obtained were multiplied by two. This allowed P < 0.05 to be used as the significance level.
Linear regression lines, based on all participants individually estimated V̇O2 values between 25 and 85%HRR, were used to illustrate mean V̇O2 for all exercise modalities in both models. The corresponding regression equations were calculated. All participants’ individually estimated V̇O2 values were also graphically pairwise compared between all exercise modalities and models in scatter plots, and with linear regressions equations. The statistical analyses have been performed using the Statistical Package for the Social Sciences (IBM SPSS Statistics, 25 and 26, Chicago, IL, USA). Figures were created in GraphPad Prism® 8 software package (GraphPad Software Inc., San Diego, CA, USA). Values are given as mean ± SD, unless otherwise stated.
Results
Measurement positions for the establishments of HR-V̇O2 relationships
The measurement positions from the submaximal and maximal workloads that were used to establish the individual HR-V̇O2 relationships for ergometer cycling, treadmill walking and running are illustrated in Fig. 1 as mean values for males and females, separately. For further details on the workloads performed, such as relative exercise intensities of HR and V̇O2 as well as RPE levels, see Additional file 1 (Table S1-S3).

Average measurement positions for the establishments of individual HR-V̇O2 relationships. Five submaximal positions (symbols with connected lines) were used to establish the HR-V̇O2 relationships for both model 1 and model 2, whereas maximal positions (separated symbols) were used only for model 2. The figure is based on the individual values of all males (n = 12) and all females (n = 12), separately. a Cycling, b walking, and c running
Regression equations
For application of the HR method, individual linear regression equations were created for both model 1 (based on only submaximal workloads) and model 2 (based on both submaximal and maximal workloads) for each of the three exercise modalities. When studying the absolute and relative exercise mode differences of all participants with both models, there were only three exercise mode differences in y-intercepts and slopes. With regard to the r2-coefficients, no mode differences were noted in model 1, while in model 2 all differences were significant, but of a minor degree. Both the absolute values of the regression coefficients as well as the modality comparisons can be found in Additional file 2 (Table S4 and S5).
Application of HR methods
Interchangeability between the exercise modalities
The estimated mean V̇O2 levels, when applying the HR method at 25–85%HRR for ergometer cycling, treadmill walking and running are presented for model 1 in Table 2 and for model 2 in Table 3. Absolute and relative V̇O2 differences between the exercise modalities are given in pairwise comparisons as measures of the interchangeability.
In the comparison of walking vs cycling, the V̇O2 levels were frequently slightly higher for walking in both models. Significant relative differences of 6.3–7.5% were noted at 45–75%HRR in model 1 (Table 2), whereas differences of 4.6–11.8% were noted between 35 and 85%HRR in model 2 (Table 3).
Fewer, and mostly minor, but significant differences were noted in the comparisons of running vs cycling as well as of running vs walking. The V̇O2 levels were 5.4–15.0% higher for running as compared to cycling at 25–45%HRR in model 1 (Table 2). In model 2, the V̇O2 levels were 2.6–3.2% lower for running compared to walking at 65–85%HRR (Table 3).
Illustrations of these estimated mean V̇O2 levels at 25–85%HRR are given in linear regression lines in Fig. 2, and are further described through regression equations (Table 4).

Linear regression lines for the estimated V̇O2. The figure is based on the individual V̇O2 values of all participants (n = 24) and the seven intensity levels between 25 and 85%HRR. (a) Model 1 and (b) model 2. For regression equations and r2-coefficients, see Table 4
Optimization of interchangeability between the exercise modalities
Pairwise exercise mode comparisons of the estimated individual V̇O2 values are illustrated in Fig. 3, and described with linear regression equations (Table 5). In all three modality comparisons, the visually observed spreading of values was smaller in model 2 compared to model 1 (Fig. 3). Furthermore, numerically; (1) higher r2-coefficients, (2) y-intercepts closer to y = 0, (3) slopes closer to the lines of identity, and (4) narrower 95% CI for both y-intercepts and slopes, were noted in model 2 compared to model 1 (Table 5).

Exercise mode comparisons for the estimated individual V̇O2 values. The figure is based on the individual V̇O2 values of all participants (n = 24), ranging between 25 and 85%HRR. Line of identity = solid line and the linear regression = dashed line. Walking vs cycling; (a) model 1 and (b) model 2, running vs cycling; (c) model 1 and (d) model 2, and running vs walking; (e) model 1 and (f) model 2. For regression equations and r2-coefficients, see Table 5
Optimization within each exercise modality
When comparing the two models within each of the three exercise modalities, it is notable that the r2-coefficients of the linear relationships between %HRR and V̇O2 were somewhat numerically higher for all modalities in model 2 compared to model 1 (Table 4). At the same time, the model comparisons of individual V̇O2 values within each exercise modality, separately, illustrate overall minor individual variations (Fig. 4). This is also indicated by the corresponding r2-coefficients (range: 0.937–0.993) as well as by the y-intercepts and slopes with their 95% CI, which included or were close to the lines of identity (Table 6).

Model comparisons for the estimated individual V̇O2 values. The figure is based on the individual V̇O2 values of all participants (n = 24), ranging between 25 and 85%HRR. Line of identity = solid line and the linear regression = dashed line. (a) Cycling, (b) walking, and (c) running. For regression equations and r2-coefficients, see Table 6
Discussion
The studied interchangeability of HR methods when estimating oxygen uptake for ergometer cycling, level treadmill walking and running was undertaken at submaximal levels between 25 and 85% of HRR, according to the ACSM classification of exercise intensities [34]. An overall good interchangeability of the HR methods was noted between the various exercise modalities, although the V̇O2 levels for walking were frequently slightly higher (5–12%) compared to cycling.
Another part of this study evaluated if various forms of establishing HR-V̇O2 relationships can optimize HR methods. For this purpose, two different models of HR-V̇O2 relationships were constructed. Model 1 used five submaximal workloads, whereas model 2 also included a maximal workload. With this aim of optimization, systematic comparisons have also been made between the present study and Olsson, Salier Eriksson [28] that used only three submaximal workloads to establish the HR-V̇O2 relationships (for more details, see Additional file 3). The overall results from these analyses indicate that the inclusions of more workloads (both submaximal and maximal), and in combination with wider measurement ranges, reduce the individual variations when using HR methods. This increased stability in the HR-V̇O2 relationships makes the HR methods more accurate. Note, however, that these analyses of optimization strategies are based on pairwise numerical comparisons. Due to the low number (two or three) of possible comparisons, there has been no basis for statistical analyses. Moreover, it cannot be ruled out that the differences observed between the two studies (cf. Additional file 3) may, at least partly, be due to that various groups of participants have been used. Therefore, it would be valuable to also evaluate issues of optimization through intra-individual comparisons.
Interchangeability between the exercise modalities
The interchangeability between running and cycling as well as running and walking was essentially good in both models. This is in line with our interpretations ([28], S1 Discussion) of earlier studies [36, 37]. Although, the comparison of running and cycling in model 1 demonstrated three rather high relative differences (range: 5.4–15.0%), they were located at low exercise intensities (25–45%HRR) (Table 2), and are therefore of no practical importance as they refer to abnormally used intensities for running. However, since the HR method also enables estimations from running to cycling, caution should be considered at the lower intensities.
In the comparisons of walking and cycling, slightly higher mean V̇O2 levels were frequently noted for walking in both models (model 1: 6.3–7.5%; model 2: 4.6–11.8%) (Tables 2 and 3). Therefore, these differences can be compensated in an application of HR methods. In our previous study, only two small differences were noted (3.7 and 4.4%) [28]. The different outcomes are probably mainly due to the reduction of individual variations within the HR methods of this study (see Additional file 3). Support for the present results comes from linear regression analyses, performed by us, of mean HR and V̇O2 data in an earlier study by Grimby and Söderholm [38]. In general, higher V̇O2 estimations (on average 8%) for level treadmill walking compared to ergometer cycling were noted when HR methods were applied at four fixed HR values between 100 and 145 beats·min− 1. These overall results contradict our previous interpretations ([28], S1 Discussion) which indicated that only HR methods based on treadmill exercise using inclination overestimate V̇O2 compared to ergometer cycling. Instead, this might also be the case for level treadmill walking.
Possible reasons for the deviations in oxygen pulse (V̇O2/HR) for level treadmill walking compared to ergometer cycling could be a slightly modified arteriovenous oxygen difference or a modified stroke volume due to a different peripheral resistance or end-diastolic volume. A tentative explanation for why it is walking that these deviations are observed for, can be related to differences in exercise intensity levels. This is since it has long been known that the stroke volume increases gradually from low intensities up to about 40–50% of V̇O2max during exercise [39], and in some cases it continues to increase slightly over the full range up to maximal intensity [40, 41]. When studying the present submaximal intensity ranges in relation to V̇O2max for all participants, it is interesting to note that the average range for walking (16–37%) never exceeds 40% of V̇O2max, and it is of a clearly lower intensity spectrum compared to both cycling (27–62%) and running (42–75%) (Additional file 1: Table S1-S3). This indicates that the different intensity ranges may play a role in the deviations in oxygen pulse for walking. On the other hand, the arteriovenous oxygen difference has also been shown to increase more rapidly between low intensities and up to about 40% of V̇O2max than compared to higher relative intensities [39, 42]. This means that the increase in arteriovenous oxygen difference, combined with the increased stroke volume, may lead to similar increases in oxygen pulse at lower and higher exercise intensities. Still, minor differences in these relations might remain, and might thereby explain the small differences noted between walking and cycling.
Optimization of interchangeability between the exercise modalities
In all exercise mode comparisons of individual V̇O2 values, a reduced individual variation was observed when the submaximal HR-V̇O2 relationships (model 1) were extended with a maximal workload (model 2) (Table 5; Fig. 3). These indications of stabilization, from model 1 to model 2, were also noted in Olsson, Salier Eriksson [28].
A reduction of individual V̇O2 variation was also observed when comparing the use of three submaximal workloads in Olsson, Salier Eriksson [28] with the present use of five submaximal points and a wider range for walking (Additional file 3: Table S6; Fig. S2 and S3). Thus, it seems that an extension of the measurement ranges, through inclusion of additional submaximal and/or a maximal point, reduces the individual variations. This in turn optimizes the HR method by becoming more accurate when evaluating results at the group level, and as a likely consequence, more significant exercise mode differences were detected between walking and cycling in the present study compared to Olsson, Salier Eriksson [28].
Optimization within each exercise modality
The HR method can also be optimized within each exercise modality. This was mirrored in the linear relationships between %HRR and V̇O2 through somewhat numerically higher r2-coefficients in model 2 compared to model 1 (Table 4). The spreadings and the regression coefficients of the model comparisons of the individual V̇O2 values within each exercise modality (Table 6; Fig. 4), confirm that there are only small variations between the two models. From that perspective, the submaximal relationships (model 1) are sufficient when using HR methods within the same form of exercise as they are established.
When comparing the present results of the model comparisons of individual V̇O2 values in walking with Olsson, Salier Eriksson [28], that used fewer submaximal workloads and a narrower range, the individual variation was clearly reduced (Additional file 3: Table S7; Fig. S4b and S5b). The corresponding analyses for cycling showed already a low degree of individual variation in the previous study [28], and it did not become further reduced in the present study (Additional file 3: Table S7; Fig. S4a and S5a). We interpret that the different outcomes in cycling and walking, respectively, are primarily dependent on the differences in widths of the measurement ranges (see Additional file 3: Fig. S1).
External validity
The present results need to be viewed from a perspective of external validity. First of all, the participants examined were mostly students in physical education and health, and trained aerobically (V̇O2max running: 59.1 and 50.4 mL · min− 1 · kg− 1 in males and females, respectively) (Additional file 1: Table S3). Whether the present results are applicable to other groups of participants (e.g. older or less trained individuals) need to be evaluated. However, notably, the findings in our previous study [28], based on a group of middle-aged active commuters, are in several ways similar to the present study. This indicates that the findings might be reproducible in physically active individuals with different ages.
Furthermore, all data collection was conducted under standardized conditions in a laboratory. A natural consequential question is therefore whether the present results can be applied under field conditions. Indications that this is possible are demonstrated in a recently published study [43]. It showed that HR methods, based on ergometer cycling in a laboratory, can be valid at a group level for estimating intensity spectrums of V̇O2 during cycle commuting in field. On the other hand, it is currently unexplored whether HR methods’ interchangeability between different exercise modalities in laboratory conditions are applicable in field exercises. For future application of the HR method, further studies of these issues of external validity are therefore suggested.
Practical application
Although further studies on the external validity are recommended, the results of the present study should be interpreted as a basis for future research in exercise physiology. The new added values of interchangeability and methodological optimization strategies make an already well-established method more adaptable and accurate, and therefore, a powerful alternative to other tools for measuring physical responses of human activities. In addition, the present results facilitate applications of HR methods in contexts of health education and promotion as well as disease prevention. This is since our findings allow HR methods to be individually established on a cycle ergometer, and then applied through estimating V̇O2 during different physical activities in field with only HR measurements.
A final aspect that is worth recalling is that the present HR methods were applied to estimate V̇O2 at a wide range of exercise intensity levels (25–85% of HRR). It is important to note that the V̇O2 values obtained are based on calculations from measured values, but, theoretically estimated for the three different exercise modalities. This means that estimations of V̇O2 levels, in the cases of walking and running, have been made that are not practically applicable, i.e. at high and low V̇O2 levels, respectively. However, with regard to the present aim of interchangeability, these results are still valuable since the HR method can be applied from both directions, e.g. from walking to running, and vice versa.
Conclusion
This study has demonstrated an overall good interchangeability of HR methods when estimating V̇O2 for ergometer cycling, level treadmill walking and running, at mean levels ranging between 25 and 85% of HRR. However, the V̇O2 levels for walking were frequently slightly higher (about 5–12%) as compared to cycling, which can be compensated for as a part of the HR method. Finally, both the use of additional submaximal workloads (five vs three) over wider ranges as well as the inclusion of maximal workloads, generally indicated a stabilizing effect on the HR-V̇O2 relationships, thereby increasing the interchangeability, and optimizing the HR methods.
Availability of data and materials
The datasets used and/or analysed during the current study, and the supplementary materials, are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
Body mass index
- CO2 :
-
Carbon dioxide
- HR:
-
Heart rate
- HRR:
-
Heart rate reserve
- MET:
-
Metabolic equivalent of task
- O2 :
-
Oxygen
- RPE:
-
Rated perceived exertion
- RPM:
-
Revolutions per minute
- V̇O2 :
-
Volume of oxygen uptake per minute
- V̇O2/HR:
-
Oxygen pulse
References
Wenger HA, Bell GJ. The interactions of intensity, frequency and duration of exercise training in altering cardiorespiratory fitness. Sports Med. 1986;3(5):346–56.
Montero D, Lundby C. Refuting the myth of non-response to exercise training: 'non-responders' do respond to higher dose of training. J Physiol. 2017;595(11):3377–87.
Paffenbarger RS Jr, Hyde RT, Wing AL, Hsieh CC. Physical activity, all-cause mortality, and longevity of college alumni. N Engl J Med. 1986;314(10):605–13.
Ross R, Janssen I. Physical activity, total and regional obesity: dose-response considerations. Med Sci Sports Exerc. 2001;33(6 Suppl):S521–7 discussion S8-9.
Hu FB, Sigal RJ, Rich-Edwards JW, Colditz GA, Solomon CG, Willett WC, et al. Walking compared with vigorous physical activity and risk of type 2 diabetes in women: a prospective study. Jama. 1999;282(15):1433–9.
Boothby WM. A determination of the circulation rate in man at rest and at work. Am J Physiol-Legacy Cont. 1915;37(2):383–417.
Krogh A, Lindhard J. A comparison between voluntary and electrically induced muscular work in man. J Physiol. 1917;51(3):182–201.
Fairbarn MS, Blackie SP, McElvaney NG, Wiggs BR, Pare PD, Pardy RL. Prediction of heart rate and oxygen uptake during incremental and maximal exercise in healthy adults. Chest. 1994;105(5):1365–9.
Ekelund U, Poortvliet E, Yngve A, Hurtig-Wennlöv A, Nilsson A, Sjöstrom M. Heart rate as an indicator of the intensity of physical activity in human adolescents. Eur J Appl Physiol. 2001;85(3–4):244–9.
Lafortuna CL, Agosti F, Galli R, Busti C, Lazzer S, Sartorio A. The energetic and cardiovascular response to treadmill walking and cycle ergometer exercise in obese women. Eur J Appl Physiol. 2008;103(6):707–17.
Booyens J, Hervey G. The pulse rate as a mean of measuring metabolic rate in man. Can J Biochem Physiol. 1960;38:1301–9.
Davies CT. Limitations to the prediction of maximum oxygen intake from cardiac frequency measurements. J Appl Physiol. 1968;24(5):700–6.
Achten J, Jeukendrup AE. Heart rate monitoring: applications and limitations. Sports Med. 2003;33(7):517–38.
Carpenter TM. Tables, factors, and formulas for computing respiratory exchange and biological transformations of energy. 4th. ed. Washington DC: Carnegie Instituton of Washington Publication; 1964.
Shephard RJ, Aoyagi Y. Measurement of human energy expenditure, with particular reference to field studies: an historical perspective. Eur J Appl Physiol. 2012;112(8):2785–815.
Green JA. The heart rate method for estimating metabolic rate: review and recommendations. Comp Biochem Physiol A Mol Integr Physiol. 2011;158(3):287–304.
McCrory MA, Mole PA, Nommsen-Rivers LA, Dewey KG. Between-day and within-day variability in the relation between heart rate and oxygen consumption: effect on the estimation of energy expenditure by heart-rate monitoring. Am J Clin Nutr. 1997;66(1):18–25.
Schantz P, Salier Eriksson J, Rosdahl H. The heart rate method for estimating oxygen uptake: analyses of reproducibility using a range of heart rates from commuter walking. Eur J Appl Physiol. 2019;119(11–12):2655–71.
Schantz P, Salier Eriksson J, Rosdahl H. The heart rate method for estimating oxygen uptake: analyses of reproducibility using a range of heart rates from cycle commuting. PLoS One. 2019;14(7):e0219741.
Vokac Z, Bell H, Bautz-Holter E, Rodahl K. Oxygen uptake/heart rate relationship in leg and arm exercise, sitting and standing. J Appl Physiol. 1975;39(1):54–9.
Åstrand P-O. Quantification of exercise capability and evaluation of physical capacity in man. Prog Cardiovasc Dis. 1976;19(1):51–67.
Eston RG, Brodie DA. Responses to arm and leg ergometry. Br J Sports Med. 1986;20(1):4–6.
Åstrand P-O. Experimental studies of physical working capacity in relation to sex and age. Doctoral thesis. Copenhagen: Ejnar Munksgaard; 1952. Available from: http://urn.kb.se/resolve?urn=urn:nbn:se:gih:diva-5581
Ryhming I. A modified Harvard step test for the evaluation of physical fitness. Arbeitsphysiologie. 1953;15(3):235–50.
Åstrand P-O, Ryhming I. A nomogram for calculation of aerobic capacity (physical fitness) from pulse rate during sub-maximal work. J Appl Physiol. 1954;7(2):218–21.
Salier Eriksson J, Rosdahl H, Schantz P. Validity of the Oxycon Mobile metabolic system under field measuring conditions. Eur J Appl Physiol. 2012;112(1):345–55.
Schantz P, Salier Eriksson J, Rosdahl H. An overview, description and synthesis of methodological issues in studying oxygen consumption during walking and cycling commuting using a portable metabolic system (Oxycon Mobile). Appendix I. In: Eriksson JS. The heart rate method for estimating oxygen uptake in walking and cycle commuting. Evaluations based on reproducibility and validity studies of the heart rate method and a portable metabolic system. Doctoral thesis 13. Stockholm: The Swedish School of Sport and Health Sciences, GIH; 2018. Available from: http://urn.kb.se/resolve?urn=urn%3Anbn%3Ase%3Agih%3Adiva-5413.
Olsson K, Salier Eriksson J, Rosdahl H, Schantz P. Are heart rate methods based on ergometer cycling and level treadmill walking interchangeable? PLoS One. 2020;15(8):e0237388.
Borg G. Psychophysical scaling with applications in physical work and the perception of exertion. Scand J Work Environ Health. 1990;16(Suppl 1):55–8.
Borg G. Perceived exertion as an indicator of somatic stress. Scand J Rehabil Med. 1970;2(2):92–8.
Howley ET, Bassett DR Jr, Welch HG. Criteria for maximal oxygen uptake: review and commentary. Med Sci Sports Exerc. 1995;27(9):1292–301.
Midgley AW, McNaughton LR, Polman R, Marchant D. Criteria for determination of maximal oxygen uptake: a brief critique and recommendations for future research. Sports Med. 2007;37(12):1019–28.
Foss O, Hallén J. Validity and stability of a computerized metabolic system with mixing chamber. Int J Sports Med. 2005;26(7):569–75.
Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, et al. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43(7):1334–59.
Howell DC. Statistical methods for psychology. 7th ed. Belmont: Wadsworth; 2010.
Berggren G, Hohwü CE. Heart rate and body temperature as indices of metabolic rate during work. Arbeitsphysiologie. 1950;14(3):255–60.
Abrantes C, Sampaio J, Reis V, Sousa N, Duarte J. Physiological responses to treadmill and cycle exercise. Int J Sports Med. 2012;33(1):26–30.
Grimby G, Söderholm B. Energy expenditure of men in different age groups during level walking and bicycle ergometry. Scand J Clin Lab Invest. 1962;14:321–8.
Åstrand PO, Cuddy TE, Saltin B, Stenberg J. Cardiac output during submaximal and maximal work. J Appl Physiol. 1964;19:268–74.
Hermansen L, Ekblom B, Saltin B. Cardiac output during submaximal and maximal treadmill and bicycle exercise. J Appl Physiol. 1970;29(1):82–6.
Åstrand PO, Rodahl K, Dahl HA, Strømme SB. Textbook of work physiology. 4th ed. Champaign: Human Kinetics; 2003.
Gmada N, Al-Hadabi B, Haj Sassi R, Abdel Samia B, Bouhlel E. Relationship between oxygen pulse and arteriovenous oxygen difference in healthy subjects: effect of exercise intensity. Sci Sports. 2019;34(6):e297–306.
Salier Eriksson J, Olsson KSE, Rosdahl H, Schantz P. Heart rate methods can be valid for estimating intensity spectrums of oxygen uptake in field exercise. Front Physiol. 2021;12:687566.
Acknowledgements
We are grateful to the volunteers for participating in this study, and for constructive comments by the reviewers.
Funding
This work was funded by The Research Funds of the Swedish Transport Administration (TRV:2017/63917–6522) (to PS) and the Swedish School of Sport and Health Sciences, GIH (to PS and HR). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Conceptualization: KO, PS. Data curation: KO. Formal analysis: KO, PS. Funding acquisition: PS. Investigation: KO. Methodology: KO, HR, PS. Project administration: KO, PS. Supervision: PS. Validation: HR. Visualization: KO. Writing – original draft: KO, PS. Writing – review & editing: KO, HR, PS. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
An ethical approval to conduct the study was obtained from the Ethics Committee North of the Karolinska Institute at the Karolinska Hospital (Dnr 03–637), Stockholm, Sweden. A written informed consent of participation was signed by all participants before their start in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1
Measured V̇O2, HR, V̇O2/HR and RPE for submaximal and maximal ergometer cycling. Table S2 Measured V̇O2, HR, V̇O2/HR and RPE for submaximal treadmill walking. Table S3 Measured V̇O2, HR, V̇O2/HR and RPE for submaximal and maximal treadmill running.
Additional file 2: Table S4
Regression equations of model 1 and exercise mode comparisons. Table S5 Regression equations of model 2 and exercise mode comparisons.
Additional file 3:
A comparative analysis with the aim of optimizing the HR method: Table S6 Linear regression equations for the exercise mode comparisons of the estimated individual V̇O2 values in Olsson, Salier Eriksson (1) and the present study. Table S7 Linear regression equations for the model comparisons of the estimated individual V̇O2 values in Olsson, Salier Eriksson (1) and the present study. Figure S1. The average HR-V̇O2 measurement ranges in Olsson, Salier Eriksson (1) and the present study. Figure S2. Exercise mode comparisons for the estimated individual V̇O2 values in Olsson, Salier Eriksson (1). Figure S3. Exercise mode comparisons for the estimated individual V̇O2 values in the present study. Figure S4. Model comparisons for the estimated individual V̇O2 values in Olsson, Salier Eriksson (1). Figure S5. Model comparisons for the estimated individual V̇O2 values in the present study.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Olsson, K.S.E., Rosdahl, H. & Schantz, P. Interchangeability and optimization of heart rate methods for estimating oxygen uptake in ergometer cycling, level treadmill walking and running. BMC Med Res Methodol 22, 55 (2022). https://doi.org/10.1186/s12874-022-01524-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12874-022-01524-w