
Abstract
Background
The heart rate method, based on the linear relation between heart rate and oxygen uptake, is potentially valuable to monitor intensity levels of physical activities. However, this depends not least on its reproducibility under standard conditions. This study aims, therefore, to evaluate the reproducibility of the heart rate method in the laboratory using a range of heart rates associated with walking commuting.
Methods
On two different days, heart rate and oxygen uptake measurements were made during three submaximal (model 1) and a maximal exercise intensity (model 2) on a cycle ergometer in the laboratory. 14 habitual walking commuters participated. The reproducibility, based on the regression equations from test and retest and using three levels of heart rate from the walking commuting, was analyzed. Differences between the two models were also analyzed.
Results
For both models, there were no significant differences between test and retest in the constituents of the regression equations (y intercept, slope and r value). Neither were there any systematic differences in estimated absolute levels of VO2 between test and retest for either model. However, some rather large individual differences were seen in both models. Furthermore, no significant differences were seen between the two models in slopes, intercepts and r values of the regression equations or in the estimated VO2.
Conclusion
The heart rate method shows good reproducibility on the group level in estimating oxygen consumption from heart rate–oxygen uptake relations in the laboratory, and based on three levels of heart rate which are representative for walking commuting.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
To monitor metabolic demands and physiological work intensities of physical activities in free-living field conditions is of great value in both physical and health education, promotion, surveillance and research. For that purpose a number of small, lightweight and portable instruments for indirect calorimetric measurements have been developed. However, they are costly, technically complicated, and can be sensitive to ambient conditions (MacFarlane 2017; Salier Eriksson et al. 2012; Schantz et al. 2018), which makes them difficult to use in a large scale in research as well as in educational contexts. Furthermore, relevant methodological evaluations of them in laboratory (cf. Rosdahl et al. 2010) or in field conditions (Salier Eriksson et al. 2012; Schantz et al. 2018) are rare.
This motivates a renewed interest in the heart rate method (HR method). It is based on a linear relationship between heart rate (HR) and work rate/oxygen uptake (VO2) during exercise, as described during the first half of the twentieth century (Boothby 1915; Krogh and Lindhard 1917; Hohwü Christensen 1931; Berggren and Hohwü Christensen 1950). HR recordings from various physical activities have since then been used in numerous studies as a basis for interpreting energy requirements and exercise intensities in humans (e.g., Bradfield 1971; Åstrand 1971; cf. Montoye et al. 1996; Achten and Jeukendrup 2003; Shephard and Aoyagi 2012) as well as in animals (cf. Green 2011). The value of such measurements is greater if individual HR–VO2 relations are established (cf. Montoye et al. 1996, p. 103), which today is facilitated by portable heart rate recorders and automatized stationary metabolic measurement devices. Furthermore, the relation between standardized work rates on ergometer cycles and VO2 can, due to a small interindividual variability in mechanical efficiency (for 2/3 of both male and female subjects within 6%, according to Åstrand and Rhyming 1954), be used as a substitute for measuring VO2 (cf. Åstrand and Ryhming 1954; Åstrand 1960, 1971), if taking into account that body weight affects these energy demands at standardized work rates (Åstrand et al. 1960; Berry et al. 1993; Lafortuna et al. 2008; Björkman 2017). That enables the heart rate method to also be used for purposes such as health education and promotion in which the exact levels of VO2 are not necessary to establish. In that way, different physical activities can be related on an individual basis in terms of, e.g., energy demands (kilocalories/-joules) and intensity levels (metabolic equivalents of task), and interpreted in relation to dose of physical activity and effects on, e.g., health outcomes (cf. Paffenbarger et al. 1986; Hu et al. 1999).
However, the mentioned practice of using a method is one thing, validity and reproducibility is another. Already Berggren and Hohwü Christensen (1950) stated that the HR method must be used “with great care” since the HR “can vary independent of metabolic rate.” There are a number of issues related to validity of the HR method, e.g., the external validity of the HR–VO2 relations from laboratory to field settings, and to various types of physical activities, as well as with different durations and ambient conditions that need to be studied in their own rights. Here we instead focus on the fundamental need of evaluating the reproducibility of the HR method under controlled laboratory conditions and to, in relation to previous studies, further the methodological approaches used.
Studies have indicated that the HR response to a repeated standardized cycle ergometer work rate may sometimes be stable and sometimes vary (cf. Montoye et al. 1996, p. 101). One reason for non-stability is a habituation effect of varying magnitude, but leading to a lower pulse rate at a given submaximal work rate. To our knowledge, this is described for the first time by Per-Olof Åstrand in his doctoral thesis (Åstrand 1952, p. 20), and the direction of this effect was later clarified by him in an interview (Eriksson and Larsson 2001). As a consequence, Åstrand did not make use of his first test results for the thesis, and neither was the Åstrand–Ryhming ergometer cycle test (Åstrand and Ryhming 1954) based on the first tests, but on the result of the second test (Eriksson and Larsson 2001, p. 17). The habituation effect has later been stated by Åstrand (1976), and noted by Ekblom-Bak et al. (2014). Another reason for instability in the HR response is a non-systematic day to day variability (Berggren and Hohwü Christensen 1950; cf. Montoye et al. 1996; Achten and Jeukendrup 2003). Whereas habituation effects can be handled through pretest trials, a day to day variability is more difficult to circumvent, and can jeopardize the reproducibility of the HR–VO2 relation under controlled laboratory conditions. In such case, the extent to which we can rely on measurements in the laboratory for interpretation in field condition will indeed also be hampered.
HR–VO2 relations during physical activity in the laboratory can be established through multiple submaximal and maximal work rates, and the pairs of HR and VO2 data used to calculate a linear regression equation. It is thereby relevant to evaluate the reproducibility of the HR–VO2 method on the basis of the equations, as well as the outcomes of them using different levels of HR to estimate VO2. Surprisingly enough, such evaluations in humans, have, to our knowledge, only been the focus of two studies (Christensen et al. 1983; McCrory et al. 1997). Both of them used a single HR level for their evaluations of the outcomes. One of the studies was dominated by patients with different clinical disorders (Christensen et al. 1983). In it, the HR–VO2 relation was established from rest to low and intermediate work rates of walking and ergometer cycling. A great variability in the outcomes, based on rather low heart rate values from a 24-h registration, led the authors to conclude that the “applied procedure seems unsuitable for metabolic studies in individual patients who engage in ordinary daily activities with low energy expenditure” (Christensen et al. 1983). McCrory et al. (1997) studied the reproducibility in healthy subjects. Two different HR–VO2 relations were established based on measurements from resting to walking. Their single-point HR evaluation was also based on HR recordings from a normal day (ca. 15 h). In the HR–VO2 relation which was based on solely walking, a good reproducibility was noted on the group level, whereas a certain variability was noted in the individual levels.
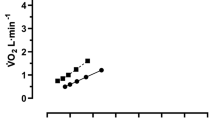
The conflicting results, and evaluations based on only one, and rather low levels of HR, together with the paucity of critical evaluations of the HR–VO2 method, prompted us to scrutinize these matters further. Methodological issues that need to be addressed relate to the degree of reproducibility possibly varying within one and the same study depending on the levels of HR being used for the evaluations (Fig. 1). If, for example, regression equation slopes from test and retest cross each other, an excellent reproducibility will be attained at that point. However, on both sides of it, the absolute differences in estimated VO2 will increase, but in different directions. A great number of other potential interrelations between dual regression slopes and y intercepts can produce a substantial variation in the test–retest variability. The magnitude of those differences may, however, be of no importance if they occur outside of the range of HR of interest. The reproducibility of VO2 estimations, based on HR–VO2 relations, needs, therefore, to be studied at several levels of HR that are distributed along a relevant range of HR.

An illustration of how a variability in HR–VO2 relations at test and retest can affect measures of reproducibility. Linear relations from regression equations, based on values from three submaximal work rates at test and retest, are illustrated as unbroken lines. Based on different HR and the regression equations, the estimated levels of VO2 can be higher, equal or lower at test compared to retest (see broken lines)
Another factor that is likely to determine the degree of reproducibility is the number and span of work rates that are used to establish the HR–VO2 relations. To enable systematic studies of these matters, it is, therefore, important to specify the levels of HR used in terms of both absolute levels and percentages of maximal heart rate (Londeree and Ames 1976) as well as the heart rate reserve (HRR) (Karvonen et al. 1957; Swain and Leutholtz 1997). The corresponding levels of VO2 and their percentage of the maximal oxygen uptake are also of value to describe (Fig. 1).
Walking commuting has been stated to occur at lower heart rates and relative exercise intensities than cycling (Oja et al. 1991) which, given the background above, may affect the reproducibility of the heart rate method. The aim of this study was, therefore, to evaluate day-to-day reproducibility of HR–VO2 regression equations and the estimated oxygen uptakes based on three levels of heart rates representative for everyday walking commuting. Two HR–VO2 relations were established and compared, one with three levels of submaximal exercise (model 1), and another which also included a maximal exercise (model 2). Model 2 has previously been used in research studies (e.g., Åstrand 1971; Schantz 1980; Schantz et al. 1983). Model 1 has been extensively used in health education at our university college, and has the advantage of not including a maximal exercise test. The HR–VO2 relations were attained on an ergometer cycle in the laboratory in healthy and physically active middle-aged male and female walking commuters.
Methods
Participants
Approval to conduct the study was obtained from the Ethics Committee North of the Karolinska Institute at the Karolinska Hospital (Dnr 03-637), Stockholm, Sweden.
Recruitment of participants
The process of selecting participants was divided into several steps. It started with recruitment through advertisements in two large morning newspapers in Stockholm in May and June of requesting participants. The inclusion criteria required being at least 20 years old; living in the county of Stockholm (excluding the municipality of Norrtälje); walking or cycling the whole way, any distance, between home and to one’s work or place of study, and actively commuting in that fashion at least once a year. Answers could be sent in cost-free by post, fax, e-mail or by phone. These advertisements resulted in 2148 people volunteering to take part.
A questionnaire (The Physically Active Commuting in Greater Stockholm Questionnaire 1; PACS Q1) was sent home to these volunteers; 2010 were returned after three reminders. The questionnaire consisted of 35 questions, but only the questions relevant to selecting our population were used in this study. These included gender, age, how physically strenuous their professional jobs were, commuting frequencies per week for each month of the year and commuting duration. The commuting distance of each individual was also used for selecting the study group. These were measured on routes drawn in maps by each respondent. The mapped route distance measuring method is described in detail in Schantz and Stigell (2009). From the answers from PACS Q1, the respondents were divided into categories based on their reported mode of either cycling or walking, or combining both modes.
Our sample was selected from the pedestrian category, i.e., those subjects who only walked to work. Other criteria were that they had ages and route distances close to the median values of the male and female pedestrians, respectively (cf. Stigell and Schantz 2015). They also rated their daily professional jobs as light or very light physically. Letters describing the physiological studies and test procedures were sent to the male and female pedestrians who fulfilled the criteria.
The recipients of the letter were first asked if their previously drawn route was still valid, or of a comparable distance time wise (comparably defined as plus/min 5–10 min). They then answered a health declaration concerning (1) medication and for which kind of illness, (2) if they had any palpitations, chest pain or abnormally heavy breathing during exercise, (3) if they had high blood pressure, and (4) if they had recently avoided or discontinued exercise for reasons of injury or health. The letter emphasized the right to terminate the tests at any time and without having to stipulate a reason. A signed informed consent of participation was returned.
Based on this information, individuals with invalid route distances as well as with high blood pressure or on medication that could affect normal heart rate were excluded. Anyone on medication with risks for strong side effects was also excluded. We contacted the remaining pedestrians by telephone to answer any potential questions, and to book test times. Telephone contacts continued until we had seven men and seven women who fulfilled the criteria and were willing to participate (Table 1).
Equipment and preparation
Stationary metabolic gas analysis system
A stationary metabolic gas analysis system, the Oxycon Pro® (Carefusion GmbH, Hoechberg, Germany) was used in the mixing chamber mode for all metabolic measurements in the laboratory. The software used was JLAB 4.53. In this system, the concentration of oxygen is measured by a paramagnetic analyzer and the carbon dioxide concentration by an infra-red analyzer. The expired air is sampled continuously from the mixing chamber through a Nafion tubing on the outside of the equipment that connects to a Nafion tubing on the inside of the equipment and that terminates at the analyzer inlets. Ventilation is measured through a digital volume transducer which is attached to the outlet of the mixing chamber. The equipment was switched on 30 min before data collection and calibrated before and after each test using the built-in automated procedures and according to the manufacturer’s recommendations. The ambient conditions were first recorded, followed by calibration of the volume sensor and the gas analyzers. A high-precision gas of 15.00% O2 and 6.00% CO2 (accuracy O2 ± 0.04% rel. and CO2 ± 0.1% rel. Air Liquide AB, Kungsängen, Sweden) was used for calibration.
A face mask with non-rebreathing air inlet valves (Combitox, Dräger Safety, Lübeck, Germany) was used. It was carefully fitted on the subject and checked for air leakage immediately prior to the measurements by the investigator and adjusted until no leakage occurred. For several subjects, a rubber insert was taped inside the top of the mask to prevent air leakage from the bridge of the nose. A tube (inner diameter of 35 mm) attached to the mask led the expired air into the mixing chamber. The measured variables were exported to Excel for further processing.
Ergometer cycle
A manually braked pendulum ergometer cycle (828E Monark Exercise AB, Vansbro, Sweden) was used. Before each experiment, the scale was zeroed while each subject sat on the saddle with his or her feet resting on the frame between the pedals, and hands resting on the handle bars. The saddle height was adjusted so that the participant’s knees were slightly flexed when the feet were on the pedals in their lowest position. The handle bars were adjusted to allow the participants to sit in an upright position. A digital metronome (DM70 Seiko S-Yard Co. Ltd, Tokyo, Japan) helped the subjects maintain the correct cadence while cycling. The work rate was controlled every minute by checking the cadence of the participant and the braking force as indicated on the pendulum scale.
Heart rate
During the resting period and the exercise protocol, HR was measured using a Polar Electro S610i Heart Rate Monitor, with a Polar Wearlink 31 transmitter (Polar Electro Oy, Kempele, Finland).
Measurements
Laboratory tests, standardization procedures and rest conditions
The walking commuters were tested in the laboratory at rest, and submaximal as well as maximal work rates on two different occasions, which were completed within an average of 8.0 ± 4.7 days. Two trained investigators carried out the laboratory tests, each participant having the same investigator for each test. The participants were not able to drink during any of the tests.
The pedestrians were asked to follow the same standard procedures before each test occasion. These were (1) not to engage in any vigorous exercise for 24 h beforehand, (2) not to cycle to the laboratory, (3) to refrain from eating, drinking, smoking and taking snuff (smokeless tobacco) for at least 1 h before arrival at the laboratory, (4) not to eat a large meal at least 3 h before the tests, (5) to avoid stress and (6) to cancel the test if they had fever, an infection or a cold. The time of the day that the tests were undertaken was not standardized since it does not affect the HR–VO2 relation during physical activity (McCrory et al. 1997). The participants wore light clothes, such as T-shirts, shorts and training shoes, so as to diminish any effect of the energy liberation from the submaximal exercises on sweating and body temperature.
On arrival at the laboratory, the participants were weighed and measured, and a check list was ticked off to determine if they had followed the standard procedures named above. A Polar heart rate monitor and a Wearlink were then placed on a wrist and around the chest, respectively. The participants rested quietly for 10 min on a treatment table. Resting heart rate, calculated from the time period between every single heart rate, was determined from the average of the 5 min between the 6th and 10th min.
Cycle ergometer exercise protocol
The participants cycled at three different work rates: 50, 100 and 150 W for the women, and 100, 150 and 200 W for the men. A cadence of 50 revolutions per minute was chosen (Åstrand 1952, p. 19). At each work rate, the participant cycled until steady state (approximately 6 min), after which the resistance was increased. The third work rate was increased to only 125 W or 175 W for women and men, respectively, if, after the second work rate, the subject’s HR was higher than 150 beats per minute and their perceived rate of exertion exceeded 15 for both legs and breathing (Borg 1998, p. 30). The HR from the Polar heart rate monitor, with the HR averaged for every 15 s, and RPE was noted in the protocol after every minute.
Between the second and third work rates, the test person continued cycling for 1 min at a self-chosen low cadence with a resistance of 5 N. The subject was then instructed to resume the cadence of 50 rpm while the investigator slowly increased the work rate until, after 1 min, the third work rate was reached. For that purpose, resistance was increased to 50 W during the first 15 s, to 100 W the second 15 s and successively to the required work rate during the last 30 s. After the third submaximal test, the subject continued cycling for 2 min at a self-chosen low cadence at 5 N.
During the maximal exercise phase, the subjects cycled at a cadence of 80 rpm (Foss and Hallén 2004). For the first three minutes, the work rates were 60, 100, and 120 or 140 W for 1 min each. The latter alternatives depended on which third work rate the subjects had during the submaximal work: 120 W if the third submaximal work rate had been 125 W or 175 W for women and men, respectively; 140 W if it had been 150 W or 200 W for women and men, respectively. The work rate increased thereafter by 20 W every 60 s. The test continued until exhaustion. HR was noted before each increase of the resistance and also at the moment when the participant terminated the test because of exhaustion.
To assess the rating of perceived exertion (RPE), the Borg scale, as mentioned before, was used (Borg 1998, p.30). The subjects were instructed on how to use the scale before commencing the tests. They were asked to point to a number on the scale that corresponded to their feeling of exertion for breathing and in their legs, respectively, before every increase of resistance during the submaximal test and directly after the maximal test. During the maximal phase they continued until exhaustion. To ensure that each subject achieved maximal exertion, at least two of the following three criteria were met by each subject: (1) a plateau in VO2 despite increasing exercise intensity (defined as a VO2 increment of less than 150 ml), (2) a respiratory exchange ratio of ≥ 1.1, and (3) a rating of RPE of ≥ 17 on the Borg scale (Borg 1970; Howley et al. 1995; Midgley et al. 2007).
The laboratory tests were completed within an average of 18.9 ± 17.7 days (23.7 ± 21.5 days for men; 14.1 ± 12.2 days for women).
Measurements of heart rate during commuter walking
The participants commuted either to or from their workplace choosing themselves which time was most convenient. 18 of the pedestrians (nine men; nine women) were tested in the morning (start times between 07:26 h and 10:15 h) and the remaining two women were tested after work (start times 16:47 h and 16:48 h). The field trips took place in the inner urban and suburban–rural areas of Stockholm, Sweden. A detailed description of these areas can be found in Wahlgren and Schantz (2011). The majority of the pedestrians walked at least partly within the inner urban area (cf. Table 1). They were met at the designated address by one of the investigators, who checked that the pretest standardization procedures, as described above, had been followed. The participants were instructed to walk at their normal pace. HR was measured using the Polar electro heart rate recorder and the HR was averaged for every 15 s. The starting time of the walking trip was synchronized with the second investigator waiting at the destination. The participants were not able to drink during their walk commute.
On arrival at the destination, the total trip time was noted and the walker was asked to rate his perceived rate of exertion for both breathing and legs. They were asked how many stops that were made at traffic lights as well as other stops, and marked them on maps with their routes. The participants were also asked to confirm whether that route had been taken the whole way, and if not, any deviation from the originally marked route was added to the map.
Analytical approach and statistical analyses
For determining the resting HR, the values are based on each single time period between the heart beats, which were transformed into heart rates per minute and averaged for a 5-min period.
For the submaximal tests in the laboratory, the mean of the four 15-s values for VO2 and HR for the last minute of each load was used for analysis. The values for the maximal tests were calculated by averaging the highest four 15-s consecutive values for VO2 and HR at maximal exercise, i.e., a collection period of 60 s (Howley et al. 1995). The same corresponding values were used for both VO2 and HR.
The reproducibility of the paired individual data for VO2 and HR between test and retest in the laboratory was calculated as absolute and relative differences, and analyzed with Wilcoxon’s signed rank test and Student’s paired t test as well as coefficient of variation (CV). The CV was calculated by dividing the standard deviation of the difference between the test–retest values by √2. This value (typical error) was then divided with the average of the test–retest values and multiplied by 100 (Hopkins 2000). With regard to significance, the same results were obtained with the non-parametric Wilcoxon’s signed rank test and the parametric Student’s paired t test. In the further statements with regard to analyses undertaken, and in “Results”, we do, however, only report the values obtained from the Student’s paired t test.
The HR–VO2 relations based on each individual´s paired VO2 and HR from three submaximal work rates (model 1) plus a maximal work rate (model 2) at test and retest were described by linear regression analyses and correlation coefficients (r values). The absolute differences in y intercepts, slopes and r values between test and retest were evaluated with paired Student’s t test for each model. The absolute values for the y intercepts, slopes and r values at test and retest were also compared between models 1 and 2 with paired Student’s t test, and the 95% confidence intervals for the mean values were also calculated.
The reproducibility of the estimated VO2, based on the regression equations from test and retest, and calculated on the basis of three levels of HR from each individual’s cycle commuting, was calculated as absolute and relative differences. They were analyzed for all individuals with Student’s paired t test, the 95% confidence intervals for the mean values and coefficient of variation (CV).
Whether the levels of estimated VO2 at test and retest, as well as the differences between test and retest, were altered between models 1 and 2 was also evaluated with Student’s paired t test and 95% confidence intervals for the mean values. Bland–Altman plots with 95% limits of agreement in individual absolute values of estimated VO2 were graphically displayed (Bland and Altman 1986).
Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS, 17.0, Chicago, IL, USA). The Bland–Altman plots were created with Graph-Pad Prism® 4 software package (Graph-Pad Software Inc., San Diego, CA, USA). Values are presented as mean ± SD unless otherwise stated. The significance level was set at p < 0.05 when data were used only once, and when data were used twice, a Bonferroni correction of the level of significance was done resulting in p < 0.025.
Results
Reproducibility of repeated single measurements
There were no systematic absolute or relative differences in VO2 and HR between the first and second measurement occasions in the laboratory (Table 2).
Positioning work rates for the HR–VO2 relations in the laboratory
The three submaximal work rates, used in both models of HR–VO2 regression equations, induced mean levels of HR ranging from on average 117 ± 15 to 157 ± 11 beats per minute for the males, and from 98 ± 9 to 154 ± 7 for the females (Table 2). For maximal HR and other descriptive aspects of the work rates used, see Tables 2 and 3.
Positioning the HR from the commuter walking used for estimating levels of VO2
The mean values of the lowest, middle and highest fifth of heart rates during each participants’ walking commute were used to estimate the corresponding level of VO2 based on the HR–VO2 regression equations. These heart rate segments were determined through ordering all heart rates from the lowest to the highest, and then dividing them into segments of 1/5 of all heart rates. It is the segments with the 20% lowest, intermediate and highest heart rates that are described in Table 4. The range of mean HR levels was between 104 ± 17 and 124 ± 20 beats per minute for the males, and from 103 ± 8 to 128 ± 10 for the females. For further details on the responses to the work rates used, see Table 4.
Reproducibility of HR–VO2 regression equations and estimated levels of VO2 (model 1)
The test and retest HR–VO2 regression equations and estimated levels of oxygen uptake from three levels of HR are presented in Tables 5 and 6. There were no indications of differences in y intercept, slope or r value in the regression equations at the retest compared to the test (Table 5). Based on calculations of all subjects, there were no systematic differences in estimated absolute levels of VO2 between test and retest (Table 6). The relative differences between test and retest were 1.91 ± 11.1, 1.71 ± 8.36 and 1.57 ± 7.34% (all n.s.) based on estimations from the lowest to the highest levels of HR. The 95% limits of agreement for the individual variations in the differences in estimated VO2 between test and retest varied between − 0.2775 and 0.2518 (L min−1) for the low HR, − 0.2436 and 0.2122 for the middle HR, and − 0.2352 and 0.2008 for the high HR (Fig. 2).

Individual levels of differences and the 95% limits of agreement between estimations of VO2 (L · min−1) calculated from fixed levels of low, middle and high HR from commuter walking as well as from repeated measurements of VO2–HR relations based on three submaximal work rates (Model 1). The y axes show absolute differences in VO2 against the mean values of the estimations from the repeated measurements on the x axes
Reproducibility of HR–VO2 regression equations and estimated levels of VO2 (model 2)
The test and retest HR–VO2 regression equations and estimated levels of VO2 from three levels of HR are presented in Tables 7 and 8. There were no significant differences between test and retest in the constituents of the regression equations (y intercept, slope and r value) (Table 7). Based on calculations of all subjects, there were no systematic differences in estimated absolute levels of VO2 between test and retest. The relative differences between test and retest, based on estimations from three different levels of HR, were 3.12 ± 8.25, 3.13 ± 7.60 and 2.81 ± 7.47% (all n.s.) (Table 8). The 95% limits of agreement for the individual variations in the differences in estimated VO2 between test and retest varied between − 0.1940 and 0.1428) (L · min−1) for the low HR, − 0.2163 and 0.1478 for the middle HR, and − 0.2437 and 0.1737 for the high HR (Fig. 3).

Individual levels of differences and the 95% limits of agreement between estimations of VO2 (L · min−1) calculated from fixed levels of low, middle and high HR from commuter walking as well as from repeated measurements of VO2–HR relations based on three submaximal work rates (Model 2). The y axes show absolute differences in VO2 against the mean values of the estimations from the repeated measurements on the x axes
Comparisons of regression equations and estimated VO2 between the HR–VO2 relations in models 1 and 2
The differences between the two HR–VO2 models in the y intercept, slope, r value as well as in the three levels of estimated VO2 at test and retest were compared for all subjects. All differences between the models were small and non-significant. The mean absolute and relative differences varied from 0.01 ± 0.08 to 0.02 ± 0.05 L/min (all n.s.) and 0.21 ± 6.89 to 1.42 ± 3.91% (all n.s.), respectively (Tables 9 and 10).
Discussion
An important feature of this study is that we have developed a transparent framework for analyses of the reproducibility of the HR method in laboratory conditions. It is characterized by positioning all HR values used in relation to both resting and maximal HR. This relates to both the HR–VO2 relations that were established in the laboratory, and the evaluation of them with three relevant HR levels that were obtained from walking commuting in field conditions. In this way, the relative localization of the measurement points of HRs used is clarified in a way that can be reproduced, and compared with future studies of these matters.
The main finding of this study is that there were no significant differences between test and retest in the constituents of the regression equations (y intercept, slope and r value) in model 1 and model 2. In line with that, there were no systematic differences in estimated absolute mean levels of VO2 between test and retest for either model. The relative differences between test and retest, based on estimations from three different levels of HR, were 1.91 ± 11.1, 1.71 ± 8.36 and 1.57 ± 7.34% (all n.s.) in model 1, and 3.12 ± 8.25, 3.13 ± 7.60 and 2.81 ± 7.47% (all n.s.) in model 2. However, some large individual differences were seen in both models, as indicated by the range of standard deviations for the relative differences (7.34–11.1%). Consequently, the 95% confidence intervals for the mean values of all subjects indicate variations of between about 8 and 14% for the three different estimations of relative differences in VO2 between test and retest. This spreading is further illustrated in the individual differences between test and retest, and the given 95% limits of agreements which are also illustrated in Figs. 2 and 3.
Another important finding was that there were no significant differences between models 1 and 2 in the constituents of the regression equations (y intercept, slope and r value) or in any of the outcome variables (estimated levels of oxygen uptake, or in the absolute or relative differences between test and retest).
An overall pattern of stability was discerned on the group levels between test and retest in VO2 and HR, which permits the present test–retest analyses of the outcomes of the HR–VO2 regression equations. The fact that we started the measurements with 15 min of rest in a supine position, and that all subjects were very physically active (cf. Table 1) can be relevant for this outcome. It should, at the same time, be kept in mind that habituation effects in HR with repeated measurements have been noted in studies of samples from the general population (Åstrand 1952; Åstrand 1976; Ekblom Bak et al. 2014). As a safeguard, a habituating pretest, as was applied by McCrory et al. (1997), is, therefore, recommended as a standard procedure.
A non-systematic test–retest variability in HR was also noted by McCrory et al. (1997). They even controlled for sex and some individual factors, such as being an emotional person, without being able to see any such relations. Berggren and Hohwü Christensen (1950) studied the HR–VO2 relation repeatedly in one person and found a variability in the heart rate of the same order of absolute magnitude in work rates demanding between 1 and 4 L of VO2. Thus, it is possible that this variability stands for an intrinsic feature of repeated HR–VO2 spot measures. And in many ways, this is reasonable since VO2, according to the Fick principle, is the product of heart rate, stroke volume and the difference between arterial and mixed venous oxygen content. Thus, levels of four different variables can, in principle, vary in response to a work rate, and still the resulting VO2 can be the same. From that perspective, it is not surprising that the HR may vary from time to time at a given exercise-induced VO2. It indicates that the biological steering mechanisms for these variables are not strictly controlled.
In individual cases, linearity between HR and VO2 has been indicated to sometimes end at near to maximal VO2 levels, with greater increases in VO2max than in HR (Hohwü Christensen 1931; Davies 1968; Åstrand and Rodahl 1970, p 352, 414). Given that, it could be questionable to include values on maximal HR and VO2, as has been done in model 2 in our study, and thus it could be anticipated that the regression equations and outcomes of models 1 and 2 might differ. Including maximal HR and VO2 could, on the other hand, serve as an anchor, stabilizing effects of day to day variability of the regression equations that otherwise could come into play. One reason for such a role for HR values from maximal work rate is its low CV (Table 2) in comparison with those at the submaximal work rates. The fact that we did not see any significant differences between the outcomes in models 1 and 2 indicates the potential value of educational models that do not include measurements from maximal work rates. Furthermore, it indicates that research models for establishing the HR–VO2 relation may be adequate without maximal measurements. To include more submaximal measurements than the three that we have used, might, however, be a beneficial way to create even greater day to day stability in models based on only submaximal work rates, and deserve future studies.
One reason for the good reproducibility on the group level for model 1, despite only making use of three submaximal work rates, can be the span of the HR attained between work rates 1 and 3 (in average 37–56 beats per minute for males and females, respectively). It is important that the utilized range of HR from walking commuting is within the range of the HR attained from the three submaximal ergometer cycle work rates in the laboratory, which is the case for the females (cf. Tables 2 and 4). If instead VO2 were to be estimated from higher or lower HR than established from the submaximal work rates in the laboratory, it is possible that greater test–retest differences would have been observed (cf. Figure 1).
A comment on the field heart rates used is that the walking commuting HR were monitored in the morning and evening at slightly varying times. Given that the standardization criteria were followed, these times of HR collections are representative for walking commuting since the HR–VO2 relation during physical activity is not affected by the time of the day (McCrory et al. 1997).
Another comment favoring a stability in the measurement conditions is that the mean values for the positions of per cent HRmax used to establish the HR–VO2 relations related well to the expected VO2 relative to VO2max in both sexes (Table 3) (Londoree and Ames 1976).
Our results are in line with those of McCrory et al. (1997), and considerably more favorable in relation to using the HR–VO2 method than those indicated by Christensen et al. (1983). There are several explanations for that. The measures used by Christensen et al. (1983) for establishing HR–VO2 regression equations were resting and sitting, as well as three low to intermediate exercise rates on an ergometer cycle (8–100 W) and three exercise rates on a treadmill, thus altogether eight measurement points. For both the slope and the y intercept of the regression equations, the measurements at low levels of HR are, under those circumstances, more influential. At the same time, it is well known that the HR–VO2 ratios at rest and sitting are quite unstable, resulting in variations in regression equations (Booyens and Hervey 1960; Montoye et al. 1996, p. 103; McCrory et al. 1997). Between very low intensities of exercise and rest, the slope of the HR–VO2 linear relationship will have a different angle compared to higher intensities (Achten and Jeukendrup 2003; Booyens and Harvey 1960; Luke et al. 1997; Spurr et al. 1988), which could be another reason for the results of Christensen et al. (1983). Furthermore, mixing the work forms on cycle ergometer and treadmill as the bases for the HR–VO2 measures is in itself problematic since HR response for a given VO2 differs in these different forms of movement (Lafortuna et al. 2008). This creates a greater risk for non-stability in the regression equations with repeated measurements. Finally, the measures of 24 h HR by Christensen et al. (1983) resulted in a mean value of 86 beats per minute. In line with the reasoning in the Introduction (cf. Fig. 1), a HR close to the endpoint of the spectrum of measurement points forming the regression equation will with greater plausibility lead to a lower reproducibility. Another potential explanation for their results relates to their use of a heterogeneous sample of predominantly patients and large variations in age, whereas we studied a sample of healthy and physically active middle-aged individuals. Having stated that, one has to keep in mind that the external validity of our findings in relation to other types of participants is uncertain. Thus, to forward the general knowledge in these respects, there is indeed a need for further studies of these matters.
As stated in “Introduction”, the studied models 1 and 2 mimic those that have been used at our research and educational setting. In our mind, it would be of great value to further the understanding of if the HR method can be optimized through using more submaximal measuring points when establishing HR–VO2 relation in laboratory. Berggren and Hohwü-Christensen (1950) undertook a number of HR and VO2 measurements on one individual, and their results indicate a variation in oxygen pulse for a given oxygen uptake. However, we do not know if such variations occur “within a day”, or are the result of “between-day variations”. Independent of the cause for them, using, e.g., five or seven submaximal measurements points might stabilize the day to day variation, as compared to using only three points, and systematic studies of this deserve to be undertaken.
In approaching the end of this discussion, it is reasonable to also point at the fact that we do not know anything about the external validity of the HR method in the laboratory in relation to field conditions such as during walking commuting. Two studies have looked at the intensity of walking commuting using different HR methods (Kokkonen-Harjula et al. 1988; Oja et al. 1991). However, none of these studies considered that, for reasons such as cardiovascular drift with prolonged work durations (Achten and Jeukendrup 2003; Coyle and Gonzalez-Alonso 2001; Saltin and Stenberg 1964) or stress due to traffic conditions (Carroll et al. 2009; Lambiase et al. 2012), the relationship measured in the laboratory may differ when being in a walking commuting environment, and that consequently the indicated intensity of walking commuting might be incorrect. This will be the focus in our further studies.
We have, as pointed out in the beginning of “Discussion”, developed a framework for studying these matters in terms of relating all HRs used to the maximal HR (%maxHR) and the relative position of the HR in between the resting and the max HR (%HRR). In future studies, we do also suggest that the body temperature is monitored since this factor influences the metabolism and may affect the blood flow distribution and thereby also the constituents of the Fick principle, with possible effects on HR–VO2 relations.
In conclusion, the present study demonstrates good reproducibility on the group level of HR–VO2 relations established through cycle ergometer exercise with healthy and physically active middle-aged walking commuters as participants in laboratory conditions, and evaluated at three levels of heart rates from walking commuting that represent moderate exercise intensities.
Abbreviations
- CI:
-
Confidence interval
- CV:
-
Coefficient of variation
- PACS Q1:
-
Physically active commuting in Greater Stockholm, Questionnaire 1
- HR:
-
Heart rate
- N:
-
Newton
- RPE:
-
Rated perceived exertion
- SD:
-
Standard deviation
- VO2 :
-
Volume of oxygen uptake
- W:
-
Watt
References
Achten J, Jeukendrup AE (2003) Heart rate monitoring: applications and limitations. Sports Med 33:517–538
Åstrand P-O (1952) Experimental studies of physical working capacity in relation to sex and age. Ejnar Munksgaard, Copenhagen
Åstrand I (1960) Aerobic work capacity in men and women with special reference to age. Acta Physiol Scand Suppl 49(169):1–92
Åstrand I (1971) Estimating the energy expenditure of housekeeping activities. Am J Clin Nutr 24(12):1471–1475
Åstrand P-O (1976) Quantification of exercise capability and evaluation of physical capacity in man. Prog Cardiovasc Dis 19(1):51–67
Åstrand P-O, Rodahl K (1970) Textbook of work physiology. Physiological bases of exercise, 1st edn. McGraw-Hill, New York
Åstrand P-O, Ryhming I (1954) A nomogram for calculation of aerobic capacity (physical fitness) from pulse rate during sub-maximal work. J Appl Physiol 7:218–221
Åstrand I, Åstrand P-O, Stunkard A (1960) Oxygen intake of obese individuals during work on a bicycle ergometer. Acta Physiol Scand 50:294–299
Berggren G, Hohwü Christensen E (1950) Heart rate and body temperature as indices of metabolic rate during work. Eur J Appl Physiol Occup Physiol 14:255–260
Berry MJ, Storsteen JA, Woodard CM (1993) Effects of body mass on exercise efficiency and VO2 during steady-state cycling. Med Sci Sports Exerc 25:1031–1037
Björkman F (2017) Validity and reliability of a submaximal cycle ergometer test for estimation of maximal oxygen uptake. Doctoral thesis no 11 at The Swedish School of Sport and Health Sciences, GIH. Stockholm: The Swedish School of Sport and Health Sciences, p. 87.
Bland JM, Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1(8476):307–310
Boothby WM (1915) A determination of the circulation rate in man at rest and at work: the regulation of the circulation. Am J Physiol 37:383–417
Booyens J, Hervey GR (1960) The pulse rate as a means of measuring metabolic rate in man. Can J Biochem Physiol 38(11):1301–1309
Borg G (1970) Perceived exertion as an indicator of somatic stress. Scand J Rehab Med 2:92–98
Borg G (1998) Borg's perceived exertion and pain scales. Human Kinetics Publishers, Champaign, IL
Bradfield RB (1971) A technique for determination of usual daily energy expenditure in the field. Am J Clin Nutr 24(9):1148–1154
Carroll D, Phillips AC, Balanos GM (2009) Metabolically exaggerated cardiac reactions to acute psychological stress revisited. Psychophysiology 46:270–275
Christensen CC, Frey HM, Foenstelien E, Aadland E, Refsum HE (1983) A critical evaluation of energy expenditure estimates based on individual O2 consumption/heart rate curves and average daily heart rate. Am J Clin Nutr 37(3):468–472
Coyle EF, Gonzalez-Alonso J (2001) Cardiovascular drift during prolonged exercise: new perspectives. Exerc Sport Sci Rev 29:88–92
Davies CT (1968) Limitations to the prediction of maximum oxygen intake from cardiac frequency measurements. J Appl Physiol 24(5):700–706
Ekblom-Bak E, Björkman F, Hellenius ML, Ekblom B (2014) A new submaximal cycle ergometer test for prediction of VO2 max. Scand J Med Sci Sports 24(2):319–326
Eriksson M, Larsson B (2001) Ergometri – konditionstest på cykel: En undersökjning av hur Åstrandtestet utvecklades och används idag. (eng. Ergometry – fitness test on cycle. An investigation about how the Åstrand test was developed and is used today). Examensarbete 27:2001. Stockholm: Idrottshögskolan i Stockholm.
Foss O, Hallén J (2004) The most economical cadence increases with increasing workload. Eur J Appl Physiol 92:443–451
Green JA (2011) The heart rate method for estimating metabolic rate: review and recommendations. Comp Biochem Physiol A Mol Integr Physiol 158(3):287–304
Hohwü Christensen E (1931) Die Pulsfrequenz während und unmittelbar nach schwerer körperlicher Arbeit. Arbeitsphysiologie 6:453–469
Hopkins WG (2000) Measures of reliability in sports medicine and science. Sports Med 30(1):1–15
Howley ET, Bassett DR Jr, Welch HG (1995) Criteria for maximal oxygen uptake: review and commentary. Med Sci Sports Exerc 27:1292–1301
Hu FB, Sigal RJ, Rich-Edwards JW, Colditz GA, Solomon CG, Willett WC, Speizer FE, Manson JE (1999) Walking compared with vigorous physical activity and risk of type 2 diabetes in women: a prospective study. JAMA 282(15):1433–1439
Karvonen MJ, Kentala E, Mustala O (1957) The effects of training on heart rate; a longitudinal study. Ann Med Exp Biol Fenn 35(3):307–315
Krogh A, Lindhard J (1917) A comparison between voluntary and electrically induced muscular work in man. J Physiol 51(3):182–201
Kukkonen-Harjula K, Oja P, Laukkanen R, Tyry T (1988) Kävellen tai pyöräillen kuljetun työmatkan fysiologinen kuormittavuus. (Finnish) (In English: The physiological strain during walking or cycling to work). Liikunta Ja Tiede 25:82–85
Lafortuna CL, Agosti F, Galli R, Busti C, Lazzer S, Sartorio A (2008) The energetic and cardiovascular response to treadmill walking and cycle ergometer exercise in obese women. Eur J Appl Physiol 103:707–717
Lambiase MJ, Dorn J, Chernega NJ, McCarthy TF, Roemmich JN (2012) Excess heart rate and systolic blood pressure during psychological stress in relation to metabolic demand in adolescents. Biol Psychol 91:42–47
Londeree BR, Ames SA (1976) Trend analysis of the % VO2 max-HR regression. Med Sci Sports 8(2):123–125
Luke A, Maki KC, Barkey N, Cooper R, McGee D (1997) Simultaneous monitoring of heart rate and motion to assess energy expenditure. Med Sci Sports Exerc 29:144–148
Macfarlane DJ (2017) Open-circuit respirometry: a historical review of portable gas analysis systems. Eur J Appl Physiol 117(12):2369–2386
McCrory MA, Molé PA, Nommsen-Rivers LA, Dewey KG (1997) Between-day and within-day variability in the relation between heart rate and oxygen consumption: effect on the estimation of energy expenditure by heart-rate monitoring. Am J Clin Nutr 66(1):18–25
Midgley AW, McNaughton LR, Polman R, Marchant D (2007) Criteria for determination of maximal oxygen uptake: a brief critique and recommendations for future research. Sports Med 37:1019–1028
Montoye HJ, Kemper HCG, Saris WHM, Washburn RA (1996) Measuring physical activity and energy expenditure. Human Kinetics, Champaign
Oja P, Mänttäri A, Heinonen A, Kukkonen-Harjula K, Laukkanen R, Pasanen M, Vuori I (1991) Physiological effects of walking and cycling to work. Scand J Med Sci Sports 1:151–157
Paffenbarger RS Jr, Hyde RT, Wing AL, Hsieh CC (1986) Physical activity, all-cause mortality, and longevity of college alumni. N Engl J Med 314(10):605–613
Rosdahl H, Gullstrand L, Salier-Eriksson J, Johansson P, Schantz P (2010) Evaluation of the Oxycon Mobile metabolic system against the Douglas bag method. Eur J Appl Physiol 109(2):159–171
Salier Eriksson J, Rosdahl H, Schantz P (2012) Validity of the Oxycon Mobile metabolic system under field measuring conditions. Eur J Appl Physiol 112(1):345–355
Saltin B, Stenberg J (1964) Circulatory response to prolonged severe exercise. J Appl Physiol 19:833–838
Schantz P (1980) Långtur: om 150 mil turåkning längs svenska fjällkedjan. (Swedish) (in English: Long ski trip: about 1500 km of ski touring along the Swedish mountain range). Idrottsfysiologi: Rapport nr 19, Trygg-Hansa: Stockholm.
Schantz P, Stigell E (2009) A criterion method for measuring route distance in physically active commuting. Med Sci Sports Exerc 41:472–478
Schantz P, Henriksson J, Jansson E (1983) Adaptation of human skeletal muscle to endurance training of long duration. Clin Physiol 3:141–151
Schantz P, Salier Eriksson J, Rosdahl H (2018) An overview, description and synthesis of methodological issues in studying oxygen consumption during walking and cycling commuting using a portable metabolic system (Oxycon Mobile). Appendix I in: Jane Salier Eriksson. 2018. The heart rate method for estimating oxygen uptake in walking and cycle commuting. Evaluations based on reproducibility and validity studies of the heart rate method and a portable metabolic system. Doctoral thesis 13, The Swedish School of Sport and Health Sciences, GIH, Stockholm, Sweden.
Shephard RJ, Aoyagi Y (2012) Measurement of human energy expenditure, with particular reference to field studies: an historical perspective. Eur J Appl Physiol 112(8):2785–2815
Spurr GB, Prentice AM, Murgatroyd PR, Goldberg GR, Reina JC, Christman NT (1988) Energy expenditure from minute-by-minute heart-rate recording: comparison with indirect calorimetry. Am J Clin Nutr 48:552–559
Stigell E, Schantz P (2015) Active commuting behaviors in a Nordic metropolitan setting in relation to modality, gender, and health recommendations. Int J Environ Res Public Health 12:15626–15648
Swain DP, Leutholtz BC (1997) Heart rate reserve is equivalent to % VO2 reserve, not to % VO2 max. Med Sci Sports Exerc 29(3):410–414
Wahlgren L, Schantz P (2011) Bikeability and methodological issues using the active commuting route environment scale (ACRES) in a metropolitan setting. BMC Med Res Methodol 11:6
Acknowledgements
Open access funding provided by The Swedish School of Sport and Health Sciences, GIH. We are grateful to the volunteers for participating in the study, and for the technical assistance of Erik Stigell, Cecilia Schantz-Eyre, Golam Sajid, Per Brink, and Phoung Pihlträd.
Funding
This work was supported by funding from the Public Health Funds of the Stockholm County Council (LS0401-0158), the Research Funds of the Swedish Transport Administration (TRV:2017/63917-6522), and The Swedish School of Sport and Health Sciences, GIH.
Author information
Authors and Affiliations
Contributions
PS conceived the overall aim of the study, and designed the study. JSE, PS and HR were responsible for collecting and analyzing the data. HR was responsible for the quality of the measurement devices in the laboratory. PS and JSE drafted the manuscript. All authors read, commented and accepted the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Communicated by Peter Krustrup.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Schantz, P., Salier Eriksson, J. & Rosdahl, H. The heart rate method for estimating oxygen uptake: analyses of reproducibility using a range of heart rates from commuter walking. Eur J Appl Physiol 119, 2655–2671 (2019). https://doi.org/10.1007/s00421-019-04236-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-019-04236-0