
Abstract
Background
The triglyceride glucose (TyG) index has been regarded as an effective proxy of Insulin resistance (IR). Studies on the TyG index, obesity and the risk of prehypertension (PHT) in elderly people are not apparent currently. The study sought to investigate the predictive value of TyG index and the associations with PHT risk and obesity.
Methods
A community-based cross-sectional study was conducted in Bengbu City, Anhui province, China. Participants older than 65 years accepted questionnaire surveys, physical examinations and blood biochemistry tests. Based on the testing results, indicators including BMI (body mass index), WC (waist circumference), WHtR (waist-to-height-ratio), LAP(Lipid accumulation products) and TyG were calculated. Residents were classified into quartiles by their TyG indexes. Receiver operating characteristic curve (ROC) analysis was carried out to predict obesity indices for PHT. The three additive interaction indicators, RERI (relative excess risk due to interaction), AP (attributable proportion due to interaction) and S (synergy index) were used to assess the interaction impacts.
Results
Two thousand six hundred sixty-six eligible elderly people were included in study and the prevalence of PHT was 71.04% (n = 1894). With increasing TyG index quartile, PHT became more prevalent. After adjusting for confounding factors, the prevalence of PHT risk with TyG levels in the fourth quartile (Q4, male: 2.83, 95%CI: 1.77–4.54; female: 2.75, 95%CI:1.91–3.97) was greater than that in the first quartile (Q1:ref). TyG index (AUC: 0.626, 95%CI: 0.602 to 0.650) was superior than BMI (AUC: 0.609, 95%CI: 0.584 to 0.633) in predicting PHT among females. Eventually, there were significant interactions of TyG index with obesity in males (General obesity: AP = 0.87, 95%CI: 0.72 to 1.02, S = 10.48, 95%CI: 3.43 to 31.97; Abdominal obesity: AP = 0.60,95%CI: 0.38 to 0.83, S = 3.53, 95%CI: 1.99 to 6.26) and females (General obesity: AP = 0.89, 95%CI: 0.79 to 0.98, S = 12.46, 95%CI: 5.61 to 27.69; Abdominal obesity: AP = 0.66, 95%CI: 0.51 to 0.82, S = 3.89, 95%CI:2.54 to 5.98).
Conclusion
TyG index and PHT risk are tightly correlated. The risk of chronic disease in the elderly can be decreased by early detection of PHT utilizing the TyG index. In this research, the TyG index was more predictable than other indicators of obesity.
Similar content being viewed by others

Background
Hypertension (HTN), which as a typical chronic disease, is a significant risk factor for diseases such as kidney disease, microvascular problems and cardiovascular disease (CVD) [1]. HTN has gradually become one of the most serious public health problems recognized worldwide [2]. The risk of HTN is rising annually as a result of the aging population's increasing severity in recent years. According to the most recent epidemiology data, HTN affects more than 1.2 billion people worldwide [3]. In 2025, this number is predicted to increase to 1.56 billion [4]. HTN places a heavy strain on society and nations in terms of both financial and medical costs and it disproportionately affects residents of developing and low-income nations [5]. To lessen the likelihood of developing HTN, early identification of HTN risk factors and active intervention of those factors are crucial. The Seventh National Joint Committee of HTN (JNC 7) classified prehypertension (PHT) as a form of HTN in 2003 [6]. Research have indicated that those with PHT are much more prone than people with normal blood pressure to develop HTN and CVD [7, 8]. Therefore, people with PHT can be screened by blood pressure in the clinical setting. Early intervention is used to reduce the risk of PHT in the elderly and reduce the mortality rate of chronic diseases in people with HTN. Furthermore, numerous investigations [9, 10] have shown that the risk of PHT is associated with obesity and insulin resistance (IR). Obese individuals have a greater tendency to develop PHT.
The triglyceride glucose (TyG) index was a relatively simple and reliable alternative indicator for IR proposed by Simental-Mendia [11] in 2008. The TyG index has been extensively employed in the investigation of endocrine and CVD disorders in recent years. The correlation and predictive ability of TyG index with these diseases were confirmed by Zou Su [12], Li Minghui [13] and Zhang F [14].
The synergistic effect of HTN and diabetes on the risk of PHT needs to be taken considered. This cross-sectional study was carried out among the elderly non-diabetic and non-hypertensive population, to eliminate these confounding impacts. The main objective of this study was to explore the relationship between TyG index and the risk of PHT in the elderly population in Anhui Province, China. The second purpose was to compare the predictive ability of obesity indicators such as TyG index, LAP index, BMI, WC and WHtR on the risk of PHT in the elderly population. The final objective was to investigate any potential interaction between the TyG index and obesity on PHT risk.
Methods
Study population
This cross-sectional study called “Community-based Cardiovascular and Health Promotion Study” (COCHPS) was conducted in Bengbu City, Anhui Province, China. According to the results of a survey on HTN in China published in 2018 [15], the prevalence of PHT among people older than 65 years was about 30.5%. The allowable error is 3% and the confidence level was 1-ɑ = 0.95. PASS 11 software was used to calculate the sample size to be investigated as 936. Assuming that the non-response rate of the subjects was 10%, the sample size was required 1040 cases. Assuming that the qualified rate of the questionnaire is 90%, the total sample size was about 1156 cases. Finally,9139 community residents older than 65 years were selected in our study by a multistage random sampling. The inclusion criteria for this study were as follows: ①The participants did not have any mental illness or cognitive communication disorder; ②Participants lived in the communities for at least six months; ③Agreed to participate in the investigation; ④Elderly population. Exclusion criteria:①Unable or unwilling to complete the whole investigation; ②Residents with mental disorders; ③Subjects with diabetes or are taking hypoglycemic medications; ④Subjects with HTN or taking medication for high blood pressure. The data were screened in accordance with the requirements of the research. Figure 1 illustrates the eventual inclusion of 2666 participants. This study complied with the Declaration of Helsinki and had been approved by the Ethics Committee of Bengbu Medical College (No. BBMC-H-2021–098). All participants in the study provided written informed consent.

Flowchart of the selected participants in this study
Data collection
Questionnaire survey
A face-to-face questionnaire survey was conducted by qualified staffs. The following information were included in the questionnaire: ① Personal general information: name, sex, age, educational level (illiteracy/functionally illiterate, primary school, junior high school, high school graduate or higher), marital status (unmarried, married, single status); ② Life behaviors: current smoking (smoking continuously for more than a year and still smoking at least one cigarette each day in the past year), current drinking (drinking continuously for more than a year and still drinking 100 ml/d average in the past year), exercising (exercise for at least 20 min four or even more times a week is deemed adequate; otherwise, it is inadequate.) [16]; ③ dietary preference (meat preference, balanced diet, vegetarian preference): A 24-h recall method was used to assess the dietary preference, which was based on eight diverse food groups [17] (starchy staples, vitamin A rich vegetables and fruits, other vegetables and fruits, meat and poultry, fish and shrimp, eggs, legumes and nuts, milk and milk products). The dietary preference was counted the number of food groups that a resident consumed in the past 24 h. Any individual food item in each food group consumed by a resident earns one point for dietary preference, the meat preference was defined as more than three points intake of animal food, vegetarian preference was defined as more than three points intake of vegetable food, meanwhile, the balanced diet was considered as an equal amount intake of animal food and vegetable; ④Past medical history: HTN, diabetes and other medication histories.
Anthropometric measurements
An automatic height and weight measuring instrument (Heng Ding Technology DMH-301) was utilized by trained investigators to detect the height (cm) and weight (kg) of the research subjects. Participants were instructed to take their shoes and weights off and wear loose clothing. To determine the waist circumference of participants, the soft ruler was wrapped around a circle across the navel and measured at the end of exhalation. The measurement of waist circumference is in cm. Two decimal places were retained for these data.
Blood pressure measurement
Blood pressure was measured by an electronic sphygmomanometer (Omron HBP-1300) with an accuracy of 1 mmHg. To guarantee the accuracy of the value, participants should rest and sit for at least 10 min. The average of three times with blood pressure readings was measured for data analysis.
Laboratory examinations
Early in the morning, fasting blood samples (fasting for at least 8 h) were taken by medical practitioners. The measurement of fasting plasma glucose (FPG), triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C) and other indicators was performed using an automatic biochemical analyzer (Modular P800, Switzerland).
Definitions
The definitions of related chronic diseases
HTN: Systolic blood pressure (SBP) ≥ 140 mmHg and/or Diastolic blood pressure (DBP) ≥ 90 mmHg [6]; PHT: SBP 120-139 mmHg and/or DBP:80–89 mmHg [6]; diabetes: fasting plasma glucose (FPG) ≥ 7.0 mmol/L [16]; impaired fasting glucose(IFG): 6.1 ≤ FPG < 7 mmol/L [16]; hypercholesterolemia(HC):TC ≥ 6.22 mmol/L [18]. Metabolic syndrome (MetS): based on abdominal obesity (WC of males ≥ 90 cm, WC of females ≥ 80 cm) and combined two or more of the following(① TG ≥ 1.7 mmol/L; ② HDL-C of male < 1.03 mmol/L or HDL-C of female < 1.29 mmol/L; ③ SBP ≥ 130 mmHg or DBP ≥ 85 mmHg; ④ FPG ≥ 5.6 mmol/L) [19].
The definitions of the obesity index
General obesity was diagnosed with BMI, which calculated by weight (kg)/height (m2). lean: BMI < 18.5; normal: 18.5 ≤ BMI ≤ 23.9; overweight: BMI ≥ 24; obesity: BMI ≥ 28 [20]. Abdominal obesity was diagnosed with WC and WHtR. WC of males ≥ 90 cm or WC of females ≥ 85 cm [21]; WHtR = WC (cm)/height (cm); WHtR ≥ 0.5 was defined as abdominal obesity [21].
The definitions of the prediction index
The definitions of LAP were [WC (cm) -65] × [TG (mmol/L)] in males and [WC (cm) -58] × [TG (mmol/L)] in females [22]. The definition of TyG index is ln[TG(mg/dl) × FPG(mg/dl)/2] [11].
Statistical analysis
PASS 15.0 (NCSS, LLC, Kaysville, Utah, USA), IBM SPSS Statistics version 25 (IBM SPSS Inc., Chicago, USA), R 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria), MedCalc Version 18 (DEMO) software (MedCalc Software Ltd., Ostend, Belgium) and GraphPad Prism version 8.0.0 for Windows (GraphPad Software, San Diego, California USA) were used for statistical analysis of the survey data. The Kolmogorov–Smirnov test was utilized in this study to examine the normality of the data. The findings demonstrated that the normal distribution was not supported by P < 0.05. Kruskal–Wallis H Test and Mann–Whitney U test were employed to examine group differences, and continuity variables were specified by median and quartile spacing. Classification factors were presented as percentages of frequency (%), and the chi-square test was used to investigate differences across groups. For data analysis, the TyG index was separated into four groups according to quartiles (Q1, Q2, Q3, Q4). Multivariate logistic regression was used to study the relationship between PHT risk and TyG index in each group.
After adjusting confounding factors, Model 1 (Education level, Marital status, Physical activity, Dietary Preference, Current smoking, Current drinking were adjusted for the unadjusted model), Model 2 (The adjustment of IFG and HC were added on the basis of Model 1.) and Model 3 (The adjustment of FPG, TC, HDL and LDL were added on the basis of Model 2) were formed. ROC curve analysis was performed, sensitivity, specificity and Youden index were used to determine the differential ability of each index for PHT. By comparing the area under the curve (AUC), the prediction effect of different indicators on PHT risk was evaluated. Z test was used to test and analyze AUCs, and p values < 0.05, indicating statistical significance. Finally, the additive interaction indexes RERI, AP and SI were used to evaluate any potential additive interactions between obesity and the TyG index on PHT. All analyses were two-sided P value and P < 0.05 was considered statistically significant.
Results
Demographic and biochemical index of the study population
The profiles of participants with PHT and those with normal blood pressure are shown in Table 1. 2666 elderly subjects (1096 men and 1570 women) over the age of 65 years old met the criteria and included in this analysis. The prevalence of PHT was 837 (76.37%) in men and 1057 (67.32%) in women. In comparison to people with normotension, PHT participants exhibited significantly increased in weight, WC, TG, FPG, TyG index and LAP (P < 0.05). People with PHT or normotension had clearly differed from each other in terms of BMI level and the prevalence of metabolic syndrome (P < 0.05). Only among women were significant variations in dietary preference discovered (P < 0.05).
Characteristics of the study population by TyG index quartiles
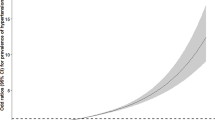
Figure 2 demonstrated that as the TyG index quartiles increased, so did the prevalence of PHT in general, with an upward tendency. The clinical characteristics of the study population according to the quartiles of the TyG index were shown in Table 2. Significant differences were discovered among the TyG index quartile groups of subjects for LDL-C, HDL-C, current drinking, abdominal obesity, BMI levels, blood pressure status, prevalence of IFG, and MetS (P < 0.05). WC, BMI, FPG, TG, TC and LAP rose progressively across the quartiles of the TyG index (all P < 0.05). In addition, the age of men and the education levels and dietary preference of women were also observed significant differences in TyG index quartiles (P < 0.05).

Prevalence of normotension and prehypertension in TyG index quartiles of different gender. a Prevalence of prehypertension in male TyG index quartiles. b Prevalence of prehypertension in female TyG index quartiles
Logistic regression analysis for risk factors of PHT
Figure 3 showed the results of the logistic regression model analysis for PHT risk factors. The findings demonstrated that the sex, dietary preference, TyG index quartiles, BMI levels, abdominal obesity and MetS were statistically significant in subjects with PHT and normotension. The TyG index in Q3 (1.876, 95%CI:1.465 to 2.402) and Q4(2.112, 95%CI: 1.610 to 2.769) group were statistically significant associated with PHT compared with Q1 group. Apart from that, participants with MetS was a risk factor for PHT (OR:2.364, 95%CI:1.663 to 3.359), but abdominal obesity was a protective factor for PHT(OR:0.661, 95%CI:0.533 to 0.820). The risk of PHT considerably increased as the BMI levels climbed (18.5–23.9: OR:1.636, 95%CI:1.037 to 2.581, ≥ 24: OR:2.817, 95%CI:1.733 to 4.581, ≥ 28: OR:4.141, 95%CI:2.273 to 7.542).

Binary logistic regression analysis of PHT
Relationship between TyG index and prevalence of PHT
The relationship between TyG index quartiles and the risk of PHT prevalence in men and women were shown in Table 3. In this regression model, the Q1 quartile of TyG index served as the reference value (OR = 1). The risk of PHT was significantly higher in the high quartile group Q3 and Q4 of TyG index than that in the low quartile group Q1 in both males (Q3:2.72, 95%CI:1.81–4.09; Q4: 2.76, 95%CI: 1.82–4.19) and females (Q3:2.46, 95%CI: 1.80–3.35; Q4: 3.02, 95%CI: 2.18–4.18). The TyG index and the risk of PHT were still correlation significantly after adjusting confounding variables in multivariable model (model 1, model 2, model 3).
Predictive value of TyG index and other common anthropometric indices/ratios of obesity on the risk of HTN
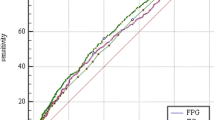
Table 4 and Fig. 4 showed the ROC curve analysis findings of PHT. The results comprised cut-off value, sensitivity, specificity, Youden index, and the AUC of TyG index and other obesity indicators. The AUC of these indexes were all greater than 50%, which was diagnostic significance for PHT. The cut-off value of TyG index was 8.29 for men and 8.50 for women. The TyG index of women has the greatest AUC value (0.626, 95%CI:0.602 to 0.650), followed by BMI(0.609, 95%CI:0.584 to 0.633). In contrast to women, the AUC of BMI (0.633, 95%CI:0.604 to 0.661) was higher in the participants of men than TyG (0.614, 95%CI:0.584 to 0.643) and LAP (0.611, 95%CI:0.581 to 0.640).

ROC curve of PHT in males and females. a Males. b Females
Interaction between TyG index and obesity situation on PHT
Table 5 showed the results from the analysis of the interaction. The interaction was analyzed by the critical value of TyG index and obesity status. The cut-off point of the ROC curve in men > 8.29 and women > 8.5 was used to designate the TyG index as positive ( +). BMI ≥ 28 was defined as general obesity positive ( +), while abdominal obesity positive( +) was defined as having a waist circumference over 85 cm for women and 90 cm for men. Regarding males, PHT risk was 5.34 times higher in subgroups with high TyG indexes and general obesity than it was in subgroups with low TyG indexes and non-obesity (aOR: 5.34, 95%CI:1.86 to 15.30). AP was 0.87 (95%CI:0.72 to 1.02), indicating that 87% of PHT was caused by the combined interaction of both risk factors. SI was10.48 (95%CI:3.43 to 31.97), suggesting that this subgroup was 10.48 times higher than that of participants exposed to a single risk factor. The same applies to women (aOR:6.87, 95%CI:3.24 to 14.55), AP:0.89(95%CI:0.79 to 0.98), SI:12.46 (95%CI:5.61 to 27.69). Contrary to general obesity, individuals with high TyG index and non-abdominal obesity were more susceptible to developing PHT in both men(aOR:2.36, 95%CI:1.63 to 3.40; AP:0.60, 95%CI:0.38 to 0.83; SI:3.53, 95%CI:1.99 to 6.26) and women(aOR:3.03, 95%CI: 2.04 to 4.49; AP: 0.66, 95%CI: 0.51 to 0.82; SI: 3.89, 95%CI: 2.54 to 5.98).
Discussion
Results of this cross-sectional study in relation to population research demonstrate that as the TyG index quartile group climbed, so increased the risk of PHT. The connection between PHT risk and TyG index remained significant after adjusting for confounding factors.
Insulin regulation and various bodily functions are both impacted by the IR mechanism of action. It is considered to be an unfavorable metabolic condition brought on by elevated triglyceride and insulin levels as a result of insulin insensitivity, one of the primary triggers to the dysfunction of lipid and glucose metabolism [23]. Under normal physiological circumstances, insulin widens blood vessels by boosting the synthesis of nitric oxide in vascular endothelial cells, facilitating the transfer of nutrients and controlling the dynamic balance of glucose in the body [24]. When the body is in a state of IR, the sensitivity of islets decreases, vasoconstrictor factors increase, pathological vascular sclerosis occurs and abnormal vasoconstriction takes place [25]. In addition, the renin–angiotensin–aldosterone system and sympathetic nervous system function are out of balance, which results in endothelial and smooth muscle cell appear hypertrophy, peripheral vascular resistance increases, water and sodium retention increased blood volume and ultimately elevated blood pressure [26, 27]. In cross-sectional studies, cohort studies and controlled trials, IR has been demonstrated to be one of the significant independent risk factors for various of chronic diseases [28,29,30]. The change in triglyceride level in the body is the another determining factor for the occurrence of IR [31]. Chronic oxidative stress creates greater challenges for liver and muscle tissue, when islet cells are exposed to an environment of high triglycerides [32]. In addition, the body is in a condition of obesity, excess free fatty acids in the liver or muscle tissue and other places appear abnormal accumulation. Obesity reduces the ability of adipose tissue to store fat and persistent proinflammatory response will be triggered that promotes IR develop [33]. IR worsens insulin sensitivity and promotes more lipid accumulation [34], toxic substances are created by ectopic fat accumulation and lipotoxicity damages organs [35].
IR can be effectively replaced by the TyG index, a biochemical index created by combining triglycerides and FPG [36]. A 2021 Korean cohort study showed a good causal relationship between TyG and IR [37]. Contrast with the hyperinsulinemic-euglycemic clamp (HIEC), the gold standard for IR diagnostics [38]. The operation of HIEC is intrusive and necessitates substantial financial and technical assistance, making it challenging to implement in clinical practice [39]. HOMA-IR is currently a popular alternative IR indication in clinical practice. Although the cost of measurement is less than that of HIEC, the collection of fasting plasma insulin data required for measurement has various issues, such as poor reuse rate and large error in the measurement process [40]. The results of Irace showed that TyG index is more strongly correlated with lipid Profile in the blood than homeostasis Model assessment of insulin resistance (HOMA-IR) [41]. According to Sarang Jeong's research findings in the Korean population, the TyG index is considered to be a more trustworthy indicator to replace IR than the HIEC and HOMA-IR [42]. TyG index is more suitable for extensive population investigation in the field of public health [43]. The TyG index has gained popularity in recent years for use in CVD prediction, including HTN. When the terms TyG index and CVD were searched on PubMed, the results revealed a total of 69 papers that were pertinent since 2014, including 12 in 2021, 30 in 2022, and 16 in 2023. Among them, there are 14 papers related to HTN. Those with PHT are more prone to develop HTN than those with normal blood pressure and they also have a greater prevalence of CVD [44, 45]. Yu Yan [46] and Zegui Huang [47] et al. published a study on the association between TyG index and HTN risk. The findings demonstrated that the increase in TyG index was independently correlated with the progression of arteriosclerosis and that a long-term increase in TyG index was linked to a higher chance of ischemic stroke. In addition, the prevalence of PHT was correlated with TyG index and increased with the increase of TyG index [14, 48]. In recent years, a large number of cohort studies have been conducted on the relationship between TyG index and hypertension and cardiovascular diseases, and the results show that there is a significant causal relationship between TyG index and hypertension, and the results of the measurement response relationship curve show that TyG index is positively correlated with the risk of hypertension [49, 50]. The difference is that the causal relationship between TyG and cardiovascular disease in people with prehypertension remains unclear. A prospective cohort study published in 2021 showed that TyG index was significantly correlated with the progression of arterial stiffness in people with hypertension. However, the causal relationship between TyG index and arterial stiffness in people with prehypertension cannot be fully confirmed [51].
The occurrence of HTN and diabetes has similar pathophysiological process and the synergistic effect exists between them [52]. People with one condition, high blood pressure or diabetes, are more likely to have the another [52]. Nearly two-thirds of diabetic individuals have HTN [53]. Therefore, the important influencing factors of PHT should be sought to predict its occurrence early. This is important for reducing the prevalence of HTN and diabetes, reducing the risk of CVD and cerebrovascular diseases, and reducing the global burden of disease.
In this study, elderly people with diabetes and HTN were excluded. To some extent, this can reduce the interaction and synergistic effect between HTN and diabetes. According to a report on the state of HTN in China that Zengwu Wang [15] published in 2018, PHT is more common than 55% among the elderly population 65 years of age and older and the prevalence grows with age. The health issues facing the elderly population are more pressing given the grim trend of global population aging.
ROC curve results of this cross-sectional study showed that TyG index was the best predictor of PHT in the elderly female population and its AUC value was the largest. Different from elderly women, the AUC of BMI in the ROC curve of elderly men was slightly greater than that of TyG. This results were matched thefinding of ZhenYu Zeng [54]. Through the analysis of the sensitivity and specificity of TyG index, among the male individuals, 65.25% of the participants may be accurately classified as being normotension (specificity = 65.25), while 54.36% of the participants can be classified correctly as PHT (sensitivity = 54.36). The Youden index of BMI in men was the best at identifying patients from non-patients. With a likelihood of 56.58% to identify actual patients (sensitivity = 56.58) and a probability of 68.81% to identify non-patients (specificity = 68.81), TyG had the highest Youden index among the female subjects. Additionally, TyG-BMI, TyG-WC, TyG-WHtR, and other Tyg-related indicators were developed and used in the study of metabolic syndrome by TaiwoHRaimi, MMirr, and other researchers [55, 56]. The findings of their study demonstrated that TyG-related indicators had a greater capacity to predict metabolic syndrome than the TyG index. A retrospective study was recently published in April 2023 to investigate the relationship between TyG correlation index (TyG-BMI) and hypertension and prehypertension. The results of this study showed that TyG-BMI was consistently positively correlated with hypertension and prehypertension. It is a reliable indicator to predict the occurrence of prehypertension and hypertension [57]. The application of the TyG-related index may help us to better predict the risk of PHT in future studies.
In addition, the study took into account the relationship between obesity and PHT. The results revealed that PHT risk and general obesity were positively correlated. This is in line with the findings of SA Isezuo, Abdellatif Moussouni, Hu L et al. [10, 58, 59]. Contrary to the results of other investigations, this study found a negative correlation between PHT risk and abdominal obesity as defined by waist circumference. The appearance may be affected by the selection of research objects. Those with diabetes and HTN were not included in this study because these conditions are known to have higher WC.
Some limitations in this study should be considered. First of all, this study is a cross-sectional one rather than a cohort study that takes into account the causal relationship between the risk of PHT and the TYG index.
In addition, a significant portion of elderly individuals with diabetes and HTN were excluded, which reduced the sample size. Finally, the relationship between WC and PHT is different from other studies and needs to be confirmed by further research. Notwithstanding these limitations, this study excluded two significant confounders, HTN and diabetes, which reduced their interactions and concerned the link between PHT and TyG index.
Conclusions
In conclusion, the results of this study demonstrated that substantial correlation between TyG index and the prevalence of PHT in the elderly people without diabetic and HTN. TyG index was proved to be an effective predictor of the risk of PHT. Although the interaction between PHT and general obesity is confirmed in this study, the relationship with abdominal obesity still needs to be discussed. Cohort studies can be employed in further research to elucidate the mechanism between TyG index and PHT risk. Moreover, TyG index can be further coupled with various anthropometric indicators to discover a more accurate predictor of PHT in clinical work. This can achieve the early prevention of PHT and lower the mortality from chronic diseases.
Availability of data and materials
The datasets analyzed during the current study are not publicly available due to the personal privacy but are available from the corresponding author on reasonable request.
Abbreviations
- PHT:
-
Prehypertension
- HTN:
-
Hypertension
- CVD:
-
Cardiovascular disease
- TyG index:
-
Triglyceride glucose index
- IR:
-
Insulin resistance
- WC:
-
Waist circumference
- FPG:
-
Fasting blood glucose
- TC:
-
Total cholesterol
- TG:
-
Triglycerides
- HDL-C:
-
High-density lipoprotein cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- BMI:
-
Body mass index
- HC:
-
Hypercholesterolemia
- IFG:
-
Impaired fasting glucose
- MetS:
-
Metabolic syndrome
- ROC:
-
Receiver operating characteristic
- AUC:
-
Area under the curve
- SD:
-
Standard deviation
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- HOMA-IR:
-
Model assessment of insulin resistance
- HIEC:
-
Hyperinsulinemic-euglycemic clamp
References
Mills KT, Bundy JD, Kelly TN, et al. Global Disparities of Hypertension Prevalence and Control: A Systematic Analysis of Population-Based Studies From 90 Countries. Circulation. 2016. https://doi.org/10.1161/CIRCULATIONAHA.115.018912.
Campbell NR, Lackland DT, Niebylski ML, World Hypertension League Committee, International Society of Hypertension Executive Committee. High blood pressure: why prevention and control are urgent and important: a 2014 fact sheet from the World Hypertension League and the International Society of Hypertension. J Clin Hypertens (Greenwich). 2014;16(8):551. https://doi.org/10.1111/jch.12372.
Rossier BC, Bochud M, Devuyst O. The Hypertension Pandemic: An Evolutionary Perspective. Physiology (Bethesda). 2017. https://doi.org/10.1152/physiol.00026.2016.
Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. Lancet. 2005. https://doi.org/10.1016/S0140-6736(05)17741-1.
Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020. https://doi.org/10.1038/s41581-019-0244-2.
Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC7 report. JAMA. 2003;289(19):2560–72.
Huang Y, Cai X, Li Y, et al. Prehypertension and the risk of stroke: a meta-analysis. Neurology. 2014;82(13):1153–61. https://doi.org/10.1212/WNL.0000000000000268.
Gupta AK, McGlone M, Greenway FL, Johnson WD. Prehypertension in disease-free adults: a marker for an adverse cardiometabolic risk profile. Hypertens Res. 2010;33(9):905–10. https://doi.org/10.1038/hr.2010.91.
Wakabayashi I. Stronger associations of obesity with prehypertension and hypertension in young women than in young men. J Hypertens. 2012;30(7):1423–9. https://doi.org/10.1097/HJH.0b013e3283544881.
Hu L, Huang X, You C, et al. Prevalence and Risk Factors of Prehypertension and Hypertension in Southern China. PLoS ONE. 2017;12(1):e0170238. https://doi.org/10.1371/journal.pone.0170238.
Simental-Mendía LE, Rodríguez-Morán M, Guerrero-Romero F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord. 2008;6(4):299–304. https://doi.org/10.1089/met.2008.0034.
Zou S, Yang C, Shen R, et al. Association between the triglyceride-glucose index and the incidence of diabetes in people with different phenotypes of obesity: a retrospective study. Front Endocrinol (Lausanne). 2021;12:784616. https://doi.org/10.3389/fendo.2021.784616.
Li M, Zhan A, Huang X, et al. Positive association between triglyceride glucose index and arterial stiffness in hypertensive patients: the China H-type hypertension registry study. Cardiovasc Diabetol. 2020;19:1–9. https://doi.org/10.1186/s12933-020-01124-2.
Zhang F, Zhang Y, Guo Z, et al. The association of triglyceride and glucose index, and triglyceride to high-density lipoprotein cholesterol ratio with prehypertension and hypertension in normoglycemic subjects: a large cross-sectional population study. J Clin Hypertens (Greenwich). 2021;23:1405–12. https://doi.org/10.1111/jch.14305.
Wang Z, Chen Z, Zhang L, et al. Status of hypertension in China: results from the China hypertension survey, 2012–2015. Circulation. 2018;137:2344–56. https://doi.org/10.1161/CIRCULATIONAHA.117.032380.
Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15:539–53.
Kennedy G, Ballard T, Dop M C. Guidelines for Measuring Household and Individual Dietary Diversity. Rome: FAO Publisher; 2011.
Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of The Third Report of The National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). JAMA. 2001;285(19):2486–97. https://doi.org/10.1001/jama.285.19.2486.
Alberti KG, Zimmet P, Shaw J, IDF Epidemiology Task Force Consensus Group. The metabolic syndrome: a new worldwide definition. Lancet. 2005;366:1059–62.
Chen C, Lu FC. Department of disease control ministry of health, PR China. The guidelines for prevention and control of overweight and obesity in Chinese adults. Biomed Environ Sci. 2004;17:1–36.
Health and Family Planning Commission of the People’s Republic of China. WS/T 428–2013. Health Industry Standards of the People’s Republic of China: Adult Weight Determination [in Chinese]. Beijing: China Standards Publishing House; 2013.
Kahn HS. The "lipid accumulation product" performs better than the body mass index for recognizing cardiovascular risk: a population-based comparison. BMC Cardiovasc Disord. 2005; https://doi.org/10.1186/1471-2261-5-26.
Ramdas Nayak VK, Satheesh P, Shenoy MT, Kalra S. Triglyceride Glucose (TyG) Index: a surrogate biomarker of insulin resistance. J Pak Med Assoc. 2022;72(5):986–8. https://doi.org/10.47391/JPMA.22-63.
Artunc F, Schleicher E, Weigert C, Fritsche A, Stefan N, Häring HU. The impact of insulin resistance on the kidney and vasculature. Nat Rev Nephrol. 2016;12(12):721–37. https://doi.org/10.1038/nrneph.2016.145.
Hill MA, Jaisser F, Sowers JR. Role of the vascular endothelial sodium channel activation in the genesis of pathologically increased cardiovascular stiffness. Cardiovasc Res. 2022;118(1):130–40. https://doi.org/10.1093/cvr/cvaa326.
Saitoh S. Insulin resistance and renin-angiotensin-aldosterone system. Nihon Rinsho. 2009;67:729–34.
Soleimani M. Insulin resistance and hypertension: new insights. Kidney Int. 2015;87(3):497–9. https://doi.org/10.1038/ki.2014.392.
Hill MA, Yang Y, Zhang L, et al. Insulin resistance, cardiovascular stiffening and cardiovascular disease. Metabolism. 2021;119:154766. https://doi.org/10.1016/j.metabol.2021.154766.
Arshi B, Tohidi M, Derakhshan A, Asgari S, Azizi F, Hadaegh F. Sex-specific relations between fasting insulin, insulin resistance and incident hypertension: 8.9 years follow-up in a Middle-Eastern population. J Hum Hypertens. 2015;29(4):260–7. https://doi.org/10.1038/jhh.2014.70.
Tagi VM, Mainieri F, Chiarelli F. Hypertension in patients with insulin resistance: etiopathogenesis and management in children. Int J Mol Sci. 2022;23(10):5814. https://doi.org/10.3390/ijms23105814.
Abbasi F, Kohli P, Reaven GM, Knowles JW. Hypertriglyceridemia: a simple approach to identify insulin resistance and enhanced cardio-metabolic risk in patients with prediabetes. Diabetes Res Clin Pract. 2016;120:156–61. https://doi.org/10.1016/j.diabres.2016.07.024.
Hegarty BD, Furler SM, Ye J, Cooney GJ, Kraegen EW. The role of intramuscular lipid in insulin resistance. Acta Physiol Scand. 2003;178(4):373–83. https://doi.org/10.1046/j.1365-201X.2003.01162.x.
Ertunc ME, Hotamisligil GS. Lipid signaling and lipotoxicity in metaflammation: indications for metabolic disease pathogenesis and treatment. J Lipid Res. 2016;57(12):2099–114. https://doi.org/10.1194/jlr.R066514.
Du T, Yuan G, Zhang M, Zhou X, Sun X, Yu X. Clinical usefulness of lipid ratios, visceral adiposity indicators, and the triglycerides and glucose index as risk markers of insulin resistance. Cardiovasc Diabetol. 2014;13:146. https://doi.org/10.1186/s12933-014-0146-3.
Ahmed B, Sultana R, Greene MW. Adipose tissue and insulin resistance in obese. Biomed Pharmacother. 2021;137:111315. https://doi.org/10.1016/j.biopha.2021.111315.
Sánchez-García A, Rodríguez-Gutiérrez R, Mancillas-Adame L, et al. Diagnostic accuracy of the triglyceride and glucose index for insulin resistance: a systematic review. Int J Endocrinol. 2020;2020:4678526. https://doi.org/10.1155/2020/4678526.
Park B, Lee HS, Lee YJ. Triglyceride glucose (TyG) index as a predictor of incident type 2 diabetes among nonobese adults: a 12-year longitudinal study of the Korean Genome and Epidemiology Study cohort. Transl Res. 2021;228:42–51. https://doi.org/10.1016/j.trsl.2020.08.003.
DeFronzo RA, Tobin JD, Andres R. Glucose clamp technique: a method for quantifying insulin secretion and resistance. Am J Physiol. 1979;237(3):E214-23. https://doi.org/10.1152/ajpendo.1979.237.3.E214.
Tam CS, Xie W, Johnson WD, Cefalu WT, Redman LM, Ravussin E. Defining insulin resistance from hyperinsulinemic-euglycemic clamps. Diabetes Care. 2012;35:1605–10. https://doi.org/10.2337/dc11-2339.
Manley SE, Stratton IM, Clark PM, Luzio SD. Comparison of 11 human insulin assays: implications for clinical investigation and research. Clin Chem. 2007;53:922–32. https://doi.org/10.1373/clinchem.2006.077784.
Irace C, Carallo C, Scavelli FB, et al. Markers of insulin resistance and carotid atherosclerosis. A comparison of the homeostasis model assessment and triglyceride glucose index. Int J Clin Pract. 2013;67(7):665–72. https://doi.org/10.1111/ijcp.12124.
Jeong S, Lee JH. The verification of the reliability of a triglyceride-glucose index and its availability as an advanced tool. Metabolomics. 2021;17(11):97. https://doi.org/10.1007/s11306-021-01837-9.
Mohd Nor NS, Lee S, Bacha F, Tfayli H, Arslanian S. Triglyceride glucose index as a surrogate measure of insulin sensitivity in obese adolescents with normoglycemia, prediabetes, and type 2 diabetes mellitus: comparison with the hyperinsulinemic-euglycemic clamp. Pediatr Diabetes. 2016;17(6):458–65. https://doi.org/10.1111/pedi.12303.
Huang Y, Wang S, Cai X, et al. Prehypertension and incidence of cardiovascular disease: a meta-analysis. BMC Med. 2013;11:177. https://doi.org/10.1186/1741-7015-11-177.
Xue H, Wang J, Hou J, et al. Prehypertension and chronic kidney disease in Chinese population: four-year follow-up study. PLoS ONE. 2015;10(12):e0144438. https://doi.org/10.1371/journal.pone.0144438.
Yan Y, Wang D, Sun Y, et al. Triglyceride-glucose index trajectory and arterial stiffness: results from Hanzhong Adolescent Hypertension Cohort Study. Cardiovasc Diabetol. 2022;21(1):33. https://doi.org/10.1186/s12933-022-01453-4.
Huang Z, Ding X, Yue Q, et al. Triglyceride-glucose index trajectory and stroke incidence in patients with hypertension: a prospective cohort study. Cardiovasc Diabetol. 2022;21(1):141. https://doi.org/10.1186/s12933-022-01577-7.
Simental-Mendía LE, Hernández-Ronquillo G, Gamboa-Gómez CI, Gómez-Díaz R, Rodríguez-Morán M, Guerrero-Romero F. The triglycerides and glucose index is associated with elevated blood pressure in apparently healthy children and adolescents. Eur J Pediatr. 2019;178(7):1069–74. https://doi.org/10.1007/s00431-019-03392-x.
Gao Q, Lin Y, Xu R, et al. Positive association of triglyceride-glucose index with new-onset hypertension among adults: a national cohort study in China. Cardiovasc Diabetol. 2023;22(1):58. https://doi.org/10.1186/s12933-023-01795-7.
Li H, Zuo Y, Qian F, et al. Triglyceride-glucose index variability and incident cardiovascular disease: a prospective cohort study. Cardiovasc Diabetol. 2022;21(1):105. https://doi.org/10.1186/s12933-022-01541-5.
Wu Z, Zhou D, Liu Y, et al. Association of TyG index and TG/HDL-C ratio with arterial stiffness progression in a non-normotensive population. Cardiovasc Diabetol. 2021;20(1):134. https://doi.org/10.1186/s12933-021-01330-6.
Sowers JR. Diabetes mellitus and vascular disease. Hypertension. 2013;61(5):943–7. https://doi.org/10.1161/HYPERTENSIONAHA.111.00612.
Ahmed AM, Hersi A, Mashhoud W, et al. Cardiovascular risk factors burden in Saudi Arabia: The Africa Middle East Cardiovascular Epidemiological (ACE) study. J Saudi Heart Assoc. 2017;29(4):235–43. https://doi.org/10.1016/j.jsha.2017.03.004.
Zeng ZY, Liu SX, Xu H, Xu X, Liu XZ, Zhao XX. Association of triglyceride glucose index and its combination of obesity indices with prehypertension in lean individuals: a cross-sectional study of Chinese adults. J Clin Hypertens (Greenwich). 2020;22(6):1025–32. https://doi.org/10.1111/jch.13878.
Raimi TH, Dele-Ojo BF, Dada SA, et al. Triglyceride-Glucose Index and Related Parameters Predicted Metabolic Syndrome in Nigerians. Metab Syndr Relat Disord. 2021;19(2):76–82. https://doi.org/10.1089/met.2020.0092.
Mirr M, Skrypnik D, Bogdański P, Owecki M. Newly proposed insulin resistance indexes called TyG-NC and TyG-NHtR show efficacy in diagnosing the metabolic syndrome. J Endocrinol Invest. 2021;44(12):2831–43. https://doi.org/10.1007/s40618-021-01608-2.
Chen L, He L, Zheng W, et al. High triglyceride glucose-body mass index correlates with prehypertension and hypertension in east Asian populations: A population-based retrospective study. Front Cardiovasc Med. 2023;10:1139842. https://doi.org/10.3389/fcvm.2023.1139842.
Isezuo SA, Sabir AA, Ohwovorilole AE, Fasanmade OA. Prevalence, associated factors and relationship between prehypertension and hypertension: a study of two ethnic African populations in Northern Nigeria. J Hum Hypertens. 2011;25(4):224–30. https://doi.org/10.1038/jhh.2010.56.
Moussouni A, Sidi-Yakhlef A, Hamdaoui H, Aouar A, Belkhatir D. Prevalence and risk factors of prehypertension and hypertension in Algeria. BMC Public Health. 2022;22(1):1571. https://doi.org/10.1186/s12889-022-13942-y.
Acknowledgements
We are grateful to all staff professionals and participants.
Funding
This study was financed by the National Science Foundation of China (number: 81703227), the “512” talent development program of Bengbu Medical College (number: by51202301), the Humanity and Social Science Research Project of Anhui Educational Committee (number: 2022AH051402), the Students Innovation Project of Bengbu Medical College (number: S202110367119).
Author information
Authors and Affiliations
Contributions
The study was designed by ZJY and SL. ZJY, JLL, ZTY and ZH participated in the methods section and collected the research data. ZJY and JLL analyzes and interprets the collected research data. ZJY drafted the manuscript. SL and ZJY critically revised the finished manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study adhered to the Declaration of Helsinki and was approved by the Ethics Committee (full name: Ethics Committee of Bengbu Medical College) (No. BBMC-H-2021–098). The authors declared that all methods were carried out in accordance with relevant guidelines and regulations. Written informed consent was obtained from all the participants.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, J., Jia, L., Zhu, T. et al. The relationship and interaction between triglyceride glucose index and obesity in the risk of prehypertension population: a cross-sectional study from a survey in Anhui, Eastern China. BMC Cardiovasc Disord 23, 336 (2023). https://doi.org/10.1186/s12872-023-03365-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-023-03365-x