
Abstract
Background
Heart failure (HF) is considered one of the main causes of morbidity and death among chronic diseases worldwide. Patients have increasingly reported chronic pain in long-standing heart failure as a disturbing symptom. Its unknown etiology and mechanism, in addition to its insidious progressive nature, made both the doctor and the patient not notice it until it affects the quality of life (QoL) and general health status. The primary objective of this study is to find the prevalence of pain in chronic heart failure patients and its impact on their QoL. The secondary objective is to determine the predictors of QoL in HF patients.
Methods
A multicenter cross-sectional design was used. The European Quality of Life scale five dimensions scale and the Brief Pain Inventory were adopted to evaluate QoL and pain, respectively. The Statistical Package for the Social Sciences version 25 was applied to present the data. The Mann-Whitney U, Kruskal-Wallis, and Cronbach alpha tests were used.
Results
The final study had a total of 142 individuals. The prevalence of pain among HF patients was 84.5%. Knee pain was the main complaint among patients. Our patients' median pain severity score was 18 [5.00–25.00], while the median pain interference score was 39 [24.75–53.00]. They had a median EQ-5D score of 0.34 [0.0–0.6] and an EQ-VAS score of 50 [30–70]. Pain severity (p = 0.004 and p < 0.001, respectively) and pain interference (p < 0.001 and p = 0.001, respectively) were found to significantly associated with both QoL scores; the visual analogue scale (EQ-VAS) and EQ-5D-5L. In multivariate analysis, monthly income was the only variable significantly correlated with EQ-VAS and EQ-5D-5L, along with pain variables.
Conclusions
Pain is a common symptom among patients with HF and is significantly associated with their QoL. Low income is also highly associated with poor QoL. Definitive guidelines should be achieved to increase awareness and understanding of the importance of pain management, reaching a higher QoL level, less pain, and good adherence to HF medications.
Similar content being viewed by others

Background
Heart failure (HF) is a group of signs and symptoms caused by a weakened heart, resulting in decreased longevity [1]. Typical symptoms describe it (that is, breathlessness) and signs (that is, peripheral edema) caused by a functional and/or structural heart abnormality [2]. When these symptoms progress, affecting the patient’s long-term quality of life (QoL), then it is called chronic heart failure (CHF) [3]. HF is a common disease, with approximately 37.7 million people living worldwide [4]. Consequently, HF is one of the most common causes of morbidity and death in chronic diseases worldwide [5].
According to the International Association for the Study of Pain (IASP), the updated and recent definition of pain is an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage [6].
Quality of life is a term that aims to describe a population's or individual's entire well-being throughout their life at a specific point in time, incorporating both positive and negative aspects. For example, personal health (physical, mental, and spiritual), relationships, education level, work environment, social standing, money, and a sense of security are all important parts of QoL [7]. However, Health-related quality of life (HRQoL) is how well an individual functions in their life and their perceived well-being in mental, physical, and social aspects of health [8].
HF disease progression is characterized mainly by the decline in daily patient activities and its effect on the QoL [9]. However, it turned out that even in the asymptomatic periods of the disease [5, 10], these changes include a wide variety of deteriorations and limitations in performing basic activities, in addition to daytime and nighttime sleep [11], anxiety, and depression. This impact is not directly related to fatigue and dyspnea, which are the main symptoms of HF, but rather to the unrecognized pain by patients and clinicians [10, 12, 13]. Furthermore, it is rare for patients with HF to present with only one symptom. Instead, they mostly present with multiple symptoms together, and pain is one of them [13, 14]. This under-recognition of pain was attributed to the fact that this pain is insidious and, therefore, could not be noticed immediately [5].
Chronic pain appears to be prevalent, between 23 and 85% among patients [5]. However, this pain is not uniformly described by them. Its nature is not well understood and varies in intensity from patient to patient, but some patients describe their pain as localized or generalized [12]. From another perspective, chronic HF pain is suggested to be of different origins but can be classified into classes according to the mechanism, such as neuropathic, inflammatory, and ischemic pain [5].
Regardless of the nature of pain, the etiology is still vague and controversial. Several factors play a major role in pain severity, including age, comorbidities, mental health status, and even a history of cancer [5]. However, an essential factor found to have the greatest role in the severity of pain is the ejection fraction. The lower the ejection fraction, the more severe the pain [12, 15].
Heart failure symptoms were approved to be associated QoL [16, 17]. Nevertheless, pain is influenced by several factors, and cause and effect is a complex matter. In addition, it is quite difficult to relate a symptom directly to heart failure, as these patients have symptom clusters and the correlation depends on the symptom characteristics studied and the prevalence of these symptoms [18].
As a result of a previous review article, the prevalence of pain in HF patients ranges between 23 and 85% [5]. A wide-range prevalence like this cannot be neglected to improve treatment, and this improvement starts by considering pain as a significant symptom of HF. In addition, some studies have discovered that several symptoms are associated with lower QoL in HF patients. Pain, anxiety, and depression, for example, were all associated with a lower QoL [19]. Although recent evidence suggests that a high proportion of people with HF experience pain and correlate with a lower QoL [20], we do not know how pain affects QoL.
Furthermore, there is strong evidence that there is a correlation between hidden and unrecognized pain and decreased QoL in HF patients [13]. This study provides good insight into the factors related to QoL. Therefore, this study aims to look for the pain to determine its prevalence and severity in HF patients from a developing country and better understand its association with QoL. It also aims to show the contributions between these areas to establish medical management composed of a multidisciplinary team to control this essential symptom.
Methods
Study design
A multicenter cross-sectional design was used, including samples from the cardiology department at Al-Watani Hospital, An-Najah National University Hospital, and the Ministry of Health Clinics in Nablus, Palestine, from November 2020 to March 2021. Due to the coronavirus disease 2019 (COVID-19) crisis, many patients stopped visiting hospitals and clinics as they used to do before, so we visited them at their houses to complete the sample.
Sample size and sampling procedure
6th-year medical students carried out data collection via face-to-face interviews. A convenience sample of 142 patients met the criteria and took part in the analysis. Frequent check-ups have been performed to reassure the sampling environment, clear definitions, and criteria correspondence.
Inclusion criteria
We included patients 18 years old or more, who had chronic HF for more than 3 months, were stable on the treatment regimen, having a left ventricular ejection fraction of < 40% determined by echocardiography or ventriculography, with the mental and physical capacity to speak with the interviewer and the ability to collect all clinical and demographic data. Those who refused to give their consent, those who were unstable. And patients with documented lacking cognitive ability to respond to the data collection procedures were also excluded. We also excluded patients who had missing items on the BPI scale.
Data collection instrument
Data were obtained through multiple questionnaires. The main variables used were: (i) Sociodemographic data: including age, gender, body mass index (BMI), residency, education status, monthly income, social status, and job status (ii) Clinical data related to HF, including duration of HF disease, comorbid diseases, and chronic medications obtained from the medical record, (iii) HRQoL of HF patients, and (iv) Pain-related data. The data collection form was built based on previous studies' information [5, 9, 10, 12].
HRQoL measurement
The 5-dimensional European Quality of Life scale (EQ5D) is used to assess the HRQoL of the patient. It is a general instrument that allows the comparison of the HRQoL evaluation findings between different populations. The EQ5D instrument includes a descriptive system and a visual analogue one. The EQ5D5L system is the descriptive one. Mobility, pain/discomfort, self-care, anxiety/depression, and typical activities are the dimensions of this system. Each component has five levels: no issues, minor issues, moderate issues, severe issues, and extreme issues. The patient should provide the most appropriate answer in each of the five components to reflect his or her health status. This option yields a one-digit number indicating the level chosen for that dimension. Then the five-dimensional numbers can be merged to form a five-digit number that indicates the patient's health status. The visual analogue scale (EQ-VAS) is a thermometer-like scale that asks patients to rate their health status on the day of questionnaire completion. Zero denotes the worst health and 100 represents the best health [20]. Cohen’s k values for EQ-5D mobility, self-care, usual activities, pain/discomfort, and anxiety/depression items were 0.66, 1.0, 0.48, 0.66, and 0.48, respectively (p ≤ 0.001 for all dimensions). Moreover, Cronbach’s alpha was 0.75 for the Arabic version of the EQ-5D. The intra-class correlation coefficient for the EQ-VAS was 0.78 [21]. The Euro-QoL Research Foundation allowed us to utilize the Arabic form of the EQ-5D (registered ID: 41,390).
Measurement of pain
We define the prevalence of pain by the yes/no question [22]. The Brief Pain Inventory (BPI) in the Arabic version is the tool that was applied to evaluate the patient's severity of pain and the extent to which pain interferes with his ability to function in daily life. The BPI has two categories: Pain Interference and Pain Intensity. The two components of pain interference help uncover several issues that must be addressed to treat the patient accurately. Activity interference and affective interference are the two dimensions in question. The term "activity interference" refers to any type of activity, including more physical activities like walking. Affective interference is concerned with internal or emotional components of daily living (for example, happiness). Pain interference is divided into seven: mood, walking, working, general activity, sleeping, relationships, and enjoying life [23]. Each of them received a score ranging from 0 to 10, and a pain interference score was calculated by summing up the marks earned on the seven questions, the resultant score was between 0 and 70 [22]. Patients with a total 10-point score of ≤ 5 were considered ‘low interference’, while those who have a score of > 5 were marked as ‘high interference’ [24].
However, the following issues are evaluated in the items on pain severity: The worst pain experienced in the previous 24 h, the least pain experienced in the previous 24 h, the average pain experienced in the previous 24 h, and the pain experienced at the time of evaluation. Participants received a score ranging from zero to ten for each of the statements mentioned above. After summing up, the resultant pain severity scores ranged from 0 and 40 [22]. Specifically, the total score ranges between 0 and 40, which was converted into a 10-point scale. A score of ≤ 4 was considered mild, > 4–6 was moderate, and > 6 was severe [24]. In addition, a picture of the human body is shown, which allows the patient to point to pain sites that he complains of. We presented the sites of pain according to the BPI scale. The scale also asks about the patient's pain management and effectiveness. Cronbach alpha for the interference items 0.92 and 0.82 for the severity. Correlations between the severity and interference items ranged between 0.25 and 0.57 (P < 0.05) [25]. We were granted permission to use the MD Anderson Cancer Center's Arabic BPI-Short Form version, which had already been translated and verified [25, 26].
Before the interviewer, we explained to patients that all questions were related to heart failure, and they had to answer accordingly.
Confidentiality
Written informed consent was obtained from all patients and informed that all data are confidential and will be used only for clinical research and publication.
Statistical analysis
We used version 25 of the Statistical Package for the Social Sciences (SPSS) (IBM SPSS Statistics for Windows, IBM Corporation, Armonk, NY) for analysis. Sociodemographic and clinical factors were described using descriptive analysis. The normality of the data was checked using the Kolmogorov-Smirnov test. Their frequencies and percentages represented categorical variables. Continuous variables were described by means and standard deviations and/or medians and interquartile range. The connections between these characteristics and the QoL scores were then checked using the Mann-Whitney U and Kruskal-Wallis tests. The internal consistency was checked using the Cronbach alpha test. Eventually, regression analysis was used to separate the variables that exhibited a significant link to QoL in bivariate testing. The EQ-5D-5L crosswalk index value calculator (http://www.euroqol.org/about-eq-5d/valuation-of-eq-5d/eq-5d-5l-value-sets.html, accessed 7 May 2021) was used to calculate the EQ-5D-5L score by using values from patients with chronic heart failure. A statistically significant p-value was established at < 0.05.
Results
Characteristics of the sample
The participants had a mean age of 64.50 ± 10, and 47.2% of them were under the age of 65. Male patients account for around 57% of the overall number of patients, 78.2% are married, and 59.2% live in the city. Most of the patients (82.4%) are unemployed. Additionally, 79.6% of participants earn fewer than 2000 new Israeli Shekels monthly. Most patients receive primary and middle school education with 24.6% and 28.9%, respectively. It should be mentioned that 57% of patients are obese according to their BMI (Table 1).
Presence and site of pain
One hundred and forty-two patients with CHF were included in the analysis. 120 (84.5%) of these participants reported chronic pain. Table 2 contains detailed numbers showing the pain sites and presence. Knee pain was the main complaint among patients, with the right predominating (n = 62, 43.7%).
Management of pain
Eighty patients (66.7%) tried medications to relieve pain for patients who had pain, while others relied only on nonpharmacological methods, such as relaxation. About 50% of the participants with pain used acetaminophen. The levels of relief of the subjects differed, with 5% reporting no relief and 12.5% reporting complete relief. Table 3 summarizes the findings on pain management methods.
Brief invitatory pain
The mean ± SD pain severity score of our patients was 16.5 ± 11.28, while our patients' mean pain interference score was 38.0 with a standard deviation of 18.37. Their medians [Q1–Q3] for both scores were 18 [5.00–25.00] and 39 [24.75–53.00], respectively. The Cronbach alpha test was utilized to calculate the reliability of pain severity and pain interference scores, and the results were 0.886 and 0.836, respectively.
EQ-VAS and EQ-5D-5L scores
The median EQ-5D score in this cohort of patients was 0.34, with an interquartile range of [0.00–0.65], while the mean ± SD was 0.3 ± 0.36. The reliability of the items tested was 0.75. However, the median EQ-VAS score was 50 [30–70], while the mean ± SD score was 50.8 ± 21.33.
Univariate and multivariate analysis
Education level (p = 0.033) and monthly income (p = 0.001) showed a statistically significant association with EQ-VAS scores. Furthermore, it showed a significant association between the EQ-VAS scores and the severity category (p = 0.026), with the lowest median 30 (20–52.5) for the severe pain group and with the interference category (p < 0.001), the median [Q1–Q3] for low pain interference was 60 (43.75–70) compared to 30 (20–50) for high pain interference.
The other factors were not substantially related to this score (Table 4).
The results of the relationships with the EQ-5D-5L are shown in Table 5. There was a statistically significant relationship between education level (p = 0.007), gender (p = 0.005), social status (p = 0.028), occupation status (p = 0.002), and income (p < 0.001). It also shows a substantial link between EQ-5D-5L and the pain interference (p < 0.001) and pain severity (p = 0.001) categories. Medians [Q1–Q3] of EQ-5D-5L score for pain severity groups were as follows: 0.74 [0.62–0.84] for no pain, 0.36 [0.02–0.55] for mild pain, 0.18 [− 0.05–0.46] for moderate pain, and 0.04 [− 0.17–0.19] for severe pain. In addition, the median was lower for high pain interference 0.04 [− 0.15–0.15] than low pain interference 0.39 [0.04–0.70].
The other variables were not significantly related to this score.
The findings of the linear regression analysis revealed significant positive differences (p = 0.02) in EQ-VAS scores related to monthly income. These findings are detailed in Table 6. Both the pain interference score (p < 0.001) and the pain severity score (p = 0.004) had significant negative associations with the EQ-VAS score.
According to regression analysis, having a lower income level was substantially associated with having a lower EQ-5D score (p = 0.044). We discovered a significant negative relationship between the EQ-5D score and both pain interference (p = 0.001) and pain intensity (p < 0.001) (Table 7).
Discussion
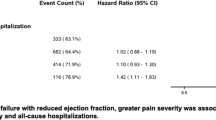
The current work found a high prevalence (84.5%) of pain among Palestinian HF patients. The important findings were significant and negative correlations between pain interference and QoL on the one hand and between pain severity and QoL on the other. Patients with CHF suffer from many symptoms, such as pain. There is a significant relationship between hidden pain and decreased quality of QoL in CHF patients [13]. Several studies have found a variety of symptoms, such as depression and anxiety, that decrease QoL in patients with HF [16, 19, 27,28,29]. In addition, a large number of publications conducted locally and globally have found a significant correlation between pain and poor QoL in HF patients and other populations [22, 28, 30,31,32,33,34,35,36]. As a result, greater attention to this topic is warranted. Importantly, a previous study with a large number of patients with HF from 40 countries revealed that HRQoL was a significant determinant of hospital admissions and all-cause mortality [37]. In addition to emerging evidence, it suggests that a large percentage of people with HF experience pain [28]. Therefore, we adopted the current research to determine the prevalence and sites of pain among patients with HF, their QoL, and the effect of pain and other variables on QoL.
Similar to a previous study, the prevalence of pain among HF patients was 85%, but the percentage of patients who had severe/very severe pain was 42.5%, which was higher than what we found (18.3%) [28]. However, another study on the same topic reported that 48% of HF patients had pain and that pain was not associated with QoL [27]. Differences in findings are probably due to a different instrument being used. Another work revealed a prevalence of 57%, with symptoms like pain associated with lowered performance status [38].
It was reported that 39.5% of HF patients complained of pain from more than one site [39]. Patients complaining of moderate to severe pain have higher adverse cardiac events [40]. When looking at stages, it can be found that 57% had pain in class III compared to 32% in class II. Therefore, pain is a complex issue and its severity and consequences on the patient’s health and life might be overlapped, as there are many factors associated with pain and its severity, such as physical harms, psychological problems, elderly, health literacy, community support, comorbid diseases, religions, and spiritual beliefs [5]. Further research should be conducted to figure out an appropriate way to control pain in chronic HF patients [5].
The current work conducted a detailed assessment of QoL in CHF in Palestine. The BPI scale was used to assess chronic pain symptoms, the EQ-5D scale and its EQ-VAS component were used to evaluate QoL. In our analysis, the median scores for EQ-5D and EQ-VAS were 0.34 and 50, respectively. HF patients were documented to have lower QoL compared with other patients with comorbid conditions and the general public [41]. A large analysis of multiple studies found moderate to high QoL in HF patients in relation to the mental aspect and moderate to poor QoL in the physical aspect [42]. A variety of demographic and clinical variables can have an impact on QoL. Certain demographic variables were associated with a worse QoL during this study, like the female sex. This result is similar to a previous study of 2709 HF patients [43]. But it was different in a study with a smaller sample size [28]. The patient’s age and disease duration were not associated with QoL. However, recent findings revered associations between these factors and QoL [44, 45].
Unemployment and low income were other variables significantly associated with poor QoL. Perhaps this result is because chronic illnesses have many complications, limitations, and acute problems that need a good socioeconomic status to control them [46]. Furthermore, most elderly might have been retired and their access to healthcare could be impaired specifically in a developing country, in addition to handling HF symptoms, which may affect the identifying and management of pain. Another study showed that higher-income people had better knowledge of their condition, healthier habits, preventive measures, and easy access to developed medical centers [47]. Furthermore, we found that single, divorced, or widowed patients had lower QoL than married ones. A previous study confirmed that marriage is associated with higher QoL in anxiety, self-care, cognition, social, sexual domains, and life satisfaction [48]. Furthermore, married patients are less at risk of depression than single or widowed patients [49]. Furthermore, according to our findings, patients with a lower level of education had a poorer QoL than those with a greater level of education. This could be related to differences in understanding the nature of the disease and how it affects QoL [50, 51]. Other publications have revealed that lack of education could contribute to people believing erroneous things about pain, leading them to apply maladaptive coping practices and improper access to pain relief options [52, 53].
The current study will help spread awareness about the importance of pain management in this population in developing countries. Additionally, understanding and managing the effect of chronic pain on the patient's mental health increases the patient's adherence to prescribed HF medications.
Strengths and limitations
This study has advantages, including the fact that it applied validated questionnaires to examine the prevalence of pain among HF patients and its influence on QoL in a developing country. Furthermore, face-to-face interviews were used to collect data, which may have enhanced the data's reliability. However, there were certain limitations, such as the spread of COVID-19 and the imposition of quarantine, which reduced the sample size and the doctors' strike in government facilities. Furthermore, elderly patients and patients who cannot walk and reach health facilities to receive their medicines and send a family member to replace them made it difficult to contact them. In addition, the most important limitation lies in the fact that its cross-sectional design makes it impossible to build causal links between exposure and outcome variables. Furthermore, the convenience sampling technique may have lowered the study's generalizability to additional HF patients. Importantly, certain clinical and objective variables, such as ejection fraction and treatment of HF were not collected or analyzed, in addition to lacking of detailed information on comorbidities, which certainly have an impact on the occurrence of pain complaints.
Conclusions
Chronic pain was prevalent among a wide range of patients with stable CHF. The subgroups with the lowest QoL are female gender, low education, low income, and unemployed. Additionally, we found that patients with more pain severity and pain interference had significantly lower QoL than others. Our results will provide policymakers and clinicians with reliable information about the impact of chronic pain on QoL, consider changing policies and taking new steps toward pain management, restrict it in current patients, and prevent its progression in future patients. Definitive guidelines should be established to increase awareness and understanding of the importance of pain management, with special guidelines organizing follow-up visits among those patients to reach a higher QoL level, less pain, and good adherence to HF medication.
Availability of data and materials
All data from the current work are obtainable from the corresponding author upon request (saedzyoud@yahoo.com).
Abbreviations
- HF:
-
Heart failure
- QoL:
-
Quality of life
- EQ5D:
-
The European Quality of Life scale 5 dimensions
- BPI:
-
The brief pain inventory
- SPSS:
-
The statistical package for the social sciences
- VAS:
-
The visual analogue scale
- CHF:
-
Chronic heart failure
- IASP:
-
The International Association for the study of pain
- NYHA:
-
The New York Heart Association
- COVID-19:
-
Coronavirus disease 2019
- BMI:
-
Body mass index
- HRQoL:
-
Health-related quality of life
- IRB:
-
Institutional review board
References
Mosterd A, Hoes AW. Clinical epidemiology of heart failure. Heart. 2007;93(9):1137–46.
McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, Burri H, Butler J, Čelutkienė J, Chioncel O, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–726.
Ramani GV, Uber PA, Mehra MR. Chronic heart failure: contemporary diagnosis and management. Mayo Clin Proc. 2010;85(2):180–95.
Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, Shibuya K, Salomon JA, Abdalla S, Aboyans V, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163–96.
Alemzadeh-Ansari MJ, Ansari-Ramandi MM, Naderi N. Chronic pain in chronic heart failure: a review article. J Tehran Heart Cent. 2017;12(2):49–56.
Raja SN, Carr DB, Cohen M, Finnerup NB, Flor H, Gibson S, Keefe FJ, Mogil JS, Ringkamp M, Sluka KA, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–82.
Teoli D, Bhardwaj A. Quality of life. In: StatPearls, edn. Treasure Island (FL): StatPearls Publishing Copyright © 2021, StatPearls Publishing LLC.; 2021.
Hays R, Reeve BB. Measurement and modeling of health-related quality of life. In: Heggenhougen K, Waltham QS, editors. International encyclopedia of public health. MA: Academic Press; 2008. p. 241–52.
Heo S, Lennie TA, Okoli C, Moser DK. Quality of life in patients with heart failure: ask the patients. Heart Lung. 2009;38(2):100–8.
de Leon CF, Grady KL, Eaton C, Rucker-Whitaker C, Janssen I, Calvin J, Powell LH. Quality of life in a diverse population of patients with heart failure: baseline findings from the heart failure adherence and retention trial (HART). J Cardiopulm Rehabil Prev. 2009;29(3):171–8.
Conley S, Feder SL, Jeon S, Redeker NS. Daytime and nighttime sleep characteristics and pain among adults with stable heart failure. J Cardiovasc Nurs. 2019;34(5):390–8.
Udeoji DU, Shah AB, Bharadwaj P, Katsiyiannis P, Schwarz ER. Evaluation of the prevalence and severity of pain in patients with stable chronic heart failure. World J Cardiol. 2012;4(8):250–5.
Goebel JR, Doering LV, Shugarman LR, Asch SM, Sherbourne CD, Lanto AB, Evangelista LS, Nyamathi AM, Maliski SL, Lorenz KA. Heart failure: the hidden problem of pain. J Pain Symptom Manag. 2009;38(5):698–707.
Godfrey C, Harrison MB, Medves J, Tranmer JE. The symptom of pain with heart failure: a systematic review. J Card Fail. 2006;12(4):307–13.
Shah AB, Udeoji DU, Baraghoush A, Bharadwaj P, Yennurajalingam S, Schwarz ER. An evaluation of the prevalence and severity of pain and other symptoms in acute decompensated heart failure. J Palliat Med. 2013;16(1):87–90.
Bekelman DB, Havranek EP, Becker DM, Kutner JS, Peterson PN, Wittstein IS, Gottlieb SH, Yamashita TE, Fairclough DL, Dy SM. Symptoms, depression, and quality of life in patients with heart failure. J Card Fail. 2007;13(8):643–8.
Blinderman CD, Homel P, Billings JA, Portenoy RK, Tennstedt SL. Symptom distress and quality of life in patients with advanced congestive heart failure. J Pain Symptom Manage. 2008;35(6):594–603.
Herr JK, Salyer J, Lyon DE, Goodloe L, Schubert C, Clement DG. Heart failure symptom relationships: a systematic review. J Cardiovasc Nurs. 2014;29(5):416–22.
Domenichiello AF, Ramsden CE. The silent epidemic of chronic pain in older adults. Prog Neuropsychopharmacol Biol Psychiatry. 2019;93:284–90.
Młyńczak K, Golicki D. Validity of the EQ-5D-5L questionnaire among the general population of Poland. Qual Life Res. 2021;30(3):817–29.
Aburuz S, Bulatova N, Twalbeh M, Gazawi M. The validity and reliability of the Arabic version of the EQ-5D: a study from Jordan. Ann Saudi Med. 2009;29(4):304–8.
Samoudi AF, Marzouq MK, Samara AM, Zyoud SH, Al-Jabi SW. The impact of pain on the quality of life of patients with end-stage renal disease undergoing hemodialysis: a multicenter cross-sectional study from Palestine. Health Qual Life Outcomes. 2021;19(1):39.
Poquet N, Lin C. The brief pain inventory (BPI). J Physiother. 2016;62(1):52.
Shalhoub M, Anaya M, Deek S, Zaben AH, Abdalla MA, Jaber MM, Koni AA, Zyoud SH. The impact of pain on quality of life in patients with osteoarthritis: a cross-sectional study from Palestine. BMC Musculoskelet Disord. 2022;23(1):248.
Ballout S, Noureddine S, Huijer HA, Kanazi G. Psychometric evaluation of the arabic brief pain inventory in a sample of Lebanese cancer patients. J Pain Symptom Manag. 2011;42(1):147–54.
Bonafé FSS, de Campos LA, Marôco J, Campos J. Brief Pain Inventory: a proposal to extend its clinical application. Eur J Pain. 2019;23(3):565–76.
Pantilat SZ, O’Riordan DL, Rathfon MA, Dracup KA, De Marco T. Etiology of pain and its association with quality of life among patients with heart failure. J Palliat Med. 2016;19(12):1254–9.
Rustoen T, Stubhaug A, Eidsmo I, Westheim A, Paul SM, Miaskowski C. Pain and quality of life in hospitalized patients with heart failure. J Pain Symptom Manag. 2008;36(5):497–504.
Gott M, Barnes S, Parker C, Payne S, Seamark D, Gariballa S, Small N. Predictors of the quality of life of older people with heart failure recruited from primary care. Age Ageing. 2006;35(2):172–7.
Hadi MA, McHugh GA, Closs SJ. Impact of chronic pain on patients’ quality of life: a comparative mixed-methods study. J Patient Exp. 2019;6(2):133–41.
Ataoğlu E, Tiftik T, Kara M, Tunç H, Ersöz M, Akkuş S. Effects of chronic pain on quality of life and depression in patients with spinal cord injury. Spinal Cord. 2013;51(1):23–6.
Costa WA, Monteiro MN, Queiroz JF, Gonçalves AK. Pain and quality of life in breast cancer patients. Clinics (Sao Paulo, Brazil). 2017;72(12):758–63.
Rostad HM, Puts MTE, Cvancarova Smastuen M, Grov EK, Utne I, Halvorsrud L. Associations between pain and quality of life in severe dementia: A Norwegian cross-sectional study. Dement Geriatr Cogn Dis Extra. 2017;7(1):109–21.
Conaghan PG, Alten R, Deodhar A, Sullivan E, Blackburn S, Tian H, Gandhi K, Jugl SM, Strand V. Relationship of pain and fatigue with health-related quality of life and work in patients with psoriatic arthritis on TNFi: results of a multi-national real-world study. RMD Open. 2020;6(2):e001240.
Abu Farha NH, Khatib MT, Salameh H, Zyoud SH. Cancer-related post-treatment pain and its impact on health-related quality of life in breast cancer patients: a cross sectional study in Palestine. Asia Pac Fam Med. 2017;16:7.
Matsuda M, Takemura H, Yamashita A, Matsuoka Y, Sawa T, Amaya F. Post-surgical chronic pain and quality of life in children operated for congenital heart disease. Acta Anaesthesiol Scand. 2019;63(6):745–50.
Johansson I, Joseph P, Balasubramanian K, McMurray JJV, Lund LH, Ezekowitz JA, Kamath D, Alhabib K, Bayes-Genis A, Budaj A, et al. Health-related quality of life and mortality in heart failure: the global congestive heart failure study of 23 000 patients from 40 Countries. Circulation. 2021;143(22):2129–42.
Conley S, Feder S, Redeker NS. The relationship between pain, fatigue, depression and functional performance in stable heart failure. Heart Lung. 2015;44(2):107–12.
Goodlin SJ, Wingate S, Albert NM, Pressler SJ, Houser J, Kwon J, Chiong J, Storey CP, Quill T, Teerlink JR. Investigating pain in heart failure patients: the pain assessment, incidence, and nature in heart failure (PAIN-HF) study. J Card Fail. 2012;18(10):776–83.
Gan Q, Zhang FR, Zhou QF, Dai LY, Liu YH, Chai XC, Wu F, Shen WF. Clinical significance of pain in patients with chronic heart failure. Chin Med J (Engl). 2012;125(18):3223–7.
Comín-Colet J, Anguita M, Formiga F, Almenar L, Crespo-Leiro MG, Manzano L, Muñiz J, Chaves J, de Frutos T, Enjuanes C. Health-related quality of life of patients with chronic systolic heart failure in Spain: results of the VIDA-IC study. Rev Esp Cardiol (Engl Ed). 2016;69(3):256–71.
Moradi M, Daneshi F, Behzadmehr R, Rafiemanesh H, Bouya S, Raeisi M. Quality of life of chronic heart failure patients: a systematic review and meta-analysis. Heart Fail Rev. 2020;25(6):993–1006.
Lewis EF, Lamas GA, O’Meara E, Granger CB, Dunlap ME, McKelvie RS, Probstfield JL, Young JB, Michelson EL, Halling K, et al. Characterization of health-related quality of life in heart failure patients with preserved versus low ejection fraction in CHARM. Eur J Heart Fail. 2007;9(1):83–91.
Molla S, Yitayal M, Amare G. Health-related quality of life and associated factors among adult patients with heart failure in Wolaita Zone Governmental hospitals, Southern Ethiopia. Risk Manag Healthc Policy. 2021;14:263–71.
Polikandrioti M, Panoutsopoulos G, Tsami A, Gerogianni G, Saroglou S, Thomai E, Leventzonis I. Assessment of quality of life and anxiety in heart failure outpatients. Arch Med Sci Atheroscler Dis. 2019;4:e38–46.
Wan Puteh SE, Siwar C, Zaidi MAS, Abdul Kadir H. Health related quality of life (HRQOL) among low socioeconomic population in Malaysia. BMC Public Health. 2019;19(Suppl 4):551.
Alexandre Tda S, Cordeiro RC, Ramos LR. Factors associated to quality of life in active elderly. Rev Saude Publica. 2009;43(4):613–21.
Moudi A, Shahinfar S, Razmara MR, Salehiniya H. Is the quality of life different in single and remarried elderly? J Educ Health Promot. 2020;9:44.
Yan XY, Huang SM, Huang CQ, Wu WH, Qin Y. Marital status and risk for late life depression: a meta-analysis of the published literature. J Int Med Res. 2011;39(4):1142–54.
Zyoud SH, Al-Jabi SW, Sweileh WM, Arandi DA, Dabeek SA, Esawi HH, Atyeh RH, Abu-Ali HA, Sleet YI, Abd-Alfatah BM, et al. Relationship of treatment satisfaction to health-related quality of life among Palestinian patients with type 2 diabetes mellitus: findings from a cross-sectional study. J Clin Transl Endocrinol. 2015;2(2):66–71.
Javanbakht M, Abolhasani F, Mashayekhi A, Baradaran HR, Jahangiri Noudeh Y. Health related quality of life in patients with type 2 diabetes mellitus in Iran: a national survey. PLoS ONE. 2012;7(8):e44526.
Cano A, Mayo A, Ventimiglia M. Coping, pain severity, interference, and disability: the potential mediating and moderating roles of race and education. J Pain. 2006;7(7):459–68.
Leclerc A, Gourmelen J, Chastang JF, Plouvier S, Niedhammer I, Lanoë JL. Level of education and back pain in France: the role of demographic, lifestyle and physical work factors. Int Arch Occup Environ Health. 2009;82(5):643–52.
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
DM, HN, and JA reviewed the literature, collected data, performed data analysis, and drafted the manuscript. MAA, YI, YD, and MMJ participated in study design, evaluated patients for eligibility criteria, reviewed the literature, and provided critical revisions. AAK and MA wrote the draft manuscript, took charge of the integrity of the data, and critically reviewed the research for the enhancement of intellectual content. SHZ formed the idea of the study, conceived and designed the research, supervised, coordinated, and analyzed the data, made a critical review of the explanation of the results, and assisted in the final writing of the manuscript. Then, all authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Institutional Review Board (IRB) of An-Najah National University and administrator of An-Najah National University Hospital both gave their approval for this study. Before the initiation of the investigation, consent was obtained. The IRB office at An-Najah National University granted approval in November 2020. All methods used in the study were carried out in accordance with relevant guidelines and regulations. Before the start of the interview, patients were asked to give their informed permission. All patients consented to the use of their clinical data for research purposes anonymously. Written informed consent was obtained from all patients and informed that all data are confidential and will be used only for clinical research and publication.
Consent for published
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mhesin, D., Nazzal, H., Amerah, J. et al. Prevalence of pain and its association with quality of life of patients with heart failure in a developing country: findings from a multicenter cross-sectional study. BMC Cardiovasc Disord 22, 426 (2022). https://doi.org/10.1186/s12872-022-02864-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-022-02864-7