
Abstract
Purpose
We aim to compare the psychometric properties of the EQ-5D-5L questionnaire with the EQ-5D-3L version and EQ VAS, based on a survey conducted in a sample representing the general adult population of Poland.
Methods
The survey comprised health-related quality of life (HRQoL) questionnaires: EQ-5D-5L, EQ VAS, SF-12 and EQ-5D-3L, together with demographic and socio-economic characteristics items. The EQ-5D index values were estimated based on a directly measured value set for Poland. The following psychometric properties were analysed: feasibility, distribution of responses, redistribution from EQ-5D-3L to EQ-5D-5L, inconsistencies, ceiling effects, informativity power and construct validity. We proposed a novel approach to the construct validity assessment, based on the use of a machine learning technique known as the random forest algorithm.
Results
From March to June 2014, 3978 subjects (aged 18–87, 53.2% female) were surveyed. The EQ-5D-5L questionnaire had a lower ceiling effect compared to EQ-5D-3L (38.0% vs 46.6%). Redistribution from EQ-5D-3L to EQ-5D-5L was similar for each dimension, and the mean inconsistency did not exceed 5%. The results of known-groups validation confirmed the hypothesis concerning the relationship between the EQ-5D index values and age, sex and occurrence of diabetes.
Conclusions
The EQ-5D-5L, in comparison with its EQ-5D-3L equivalent, showed similar or better psychometric properties within the general population of a country. We assessed the construct validity of the questionnaire with a novel approach that was based on a machine learning technique known as the random forest algorithm.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Assessment of the health-related quality of life (HRQoL) is an essential step in the process of inferring the cost-effectiveness of medical technology. To ensure the correctness of pharmacoeconomic inference, the HRQoL estimates should tend to the true value. However, this is difficult because the HRQoL is a latent variable and cannot be measured and interpreted directly. The assessment of psychometric properties, i.e. validation, includes determining if there are grounds to believe that the questionnaire used to assess HRQoL measures what is intended [1]. Therefore, before the questionnaire is included in a study, it should be validated. It means checking to what extent, in a given clinical situation and a specific population, the results of the questionnaire can be correctly interpreted.
The most commonly assessed and pointed in the COSMIN checklist (COnsensus-based Standards for the selection of health status Measurement INstruments) psychometric properties comprise validity, reliability and sensitivity [2]. Validity determines whether the questionnaire measures what is intended to measure and that it is useful for its intended purpose. Reliability assesses whether the results of the questionnaire specifying the same feature will be repeatable for subsequent measurements. Sensitivity is the ability to measure differences in the HRQoL among patients or patient groups [1, 3].
The EQ-5D is one of the most commonly used HRQoL questionnaires in clinical and economic evaluations of health care [4, 5]. It was developed by the EuroQol group in 1990 [6]. The EQ-5D is a generic instrument: a non-specific questionnaire, which has no restrictions on the characteristics of the population for its use. This makes it possible to compare the HRQoL results of assessment within different populations. Each EQ-5D instrument comprises a descriptive system and a visual analogue scale (EQ VAS). The EQ VAS is a typical, thermometer-like, 20-cm-long scale, grading from 0 (representing “The worst health you can imagine”) to 100 (representing “The best health you can imagine”). The descriptive system consists of five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. The patient uses it to assess their health with a three-level or five-level scale (EQ-5D-3L and EQ-5D-5L, respectively) [6, 7]. The best health state is determined by a pattern of 11111. A single summary score (EQ-5D index value) may be calculated for the results of the descriptive system (health states profiles). It represents the utility related to the described health state. The utilities are determined based on social preference weights. The EQ-5D index values of health states are then used in economic analyses as part of health technology assessment [8].
In the beginning, the EQ-5D-3L provided the assessment of 243 (i.e. 35) possible health states. Many studies have shown the validity and reliability of the EQ-5D-3L, both in disease-specific (cardiovascular disease [9], schizophrenia [10], rheumatic disease [11], paediatric population [12], cervical cancer [13], diabetes [14]) and general populations [15, 16]. When the use of the EQ-5D questionnaire became more widespread, it was noted that it is necessary to improve its discriminatory power and reduce the ceiling effect (i.e. an unexpectedly increased frequency of the best (“no problem”) health status). This issue was of particular importance in the general population studies [17,18,19,20,21,22]. Hence, the EuroQol group decided to develop a new version of the questionnaire (EQ-5D-5L), which could cover 3125 (i.e. 55) possible health states [7, 23, 24].
Numerous literature references indicate better, or at least comparable, properties of the EQ-5D-5L version of the questionnaire in comparison to the EQ-5D-3L one [25,26,27,28]. As indicated by Buchholz et al. [27], most of the study populations are disease specific: inpatient rehabilitation [29], orthopaedics [30, 31], stroke [32, 33], liver disease [34,35,36], cancer [37], lung cancer [38], diabetes [39, 40], dermatology [41], psoriasis [42] and mixed population [43]. Recently published studies comparing EQ-5D-3L and EQ-5D-5L also refer to the disease-specific subpopulations: cataract [44], Crohns disease [45] and hip replacement surgery [46]. However, disease-specific populations characterise by predictively worse health and resulting HRQoL, so the distribution of assessed health states in these groups is shifted compared to the distribution in the general population. It shows that it is difficult to transfer the results of a validation study in the disease-specific population to the general one.
In this study, we aim to assess the psychometric properties of the EQ-5D-5L questionnaire in relation to the results of the EQ-5D-3L, and along with the EQ VAS results, based on a survey conducted in a sample representing the general adult population of Poland.
Methods
Population and study setting
To obtain a representative sample of the adult population, the administrative area of Poland was divided into 65 strata (16 voivodeships [counties] with 3–9 smaller areas based on the number of inhabitants in each). The previously defined size of the target population of the study was split proportionally into strata. The first stage of random stratified sampling was to take the samples from cities and villages, and then from randomly selected smaller areas (one or several adjacent streets) in previously selected locations. Finally, based on personal identification numbers (PESEL), samples of 8 people with different addresses from each stratum were selected. The maximum error in estimating the frequency of a given category in the sample was 1.55%.
The surveys were conducted with the support of the market research company—Centre for Public Opinion Research (CBOS)—from March to June 2014. The interviewers had to make at least three attempts to contact the respondent. No substitutes were permitted. As part of the survey, respondents answered questions about demographic characteristics and socio-economic status (computer-assisted personal interview, CAPI) and completed by themselves paper-and-pencil polish versions of HRQoL questionnaires in the following fixed order: EQ-5D-5L, EQ VAS, SF-12 and EQ-5D-3L. We also introduced in the survey the additional question about diabetes (the results of the planned substudy will be described elsewhere). A total of 10% of interviews underwent quality control. The Bioethics Committee at the Medical University of Warsaw approval was obtained for the survey (AkBE/34/17).
Data analysis
The validation of the EQ-5D-5L questionnaire consisted of an analysis of the following psychometric properties: feasibility, distribution of responses, redistribution from EQ-5D-3L to EQ-5D-5L, inconsistencies, ceiling effect, informativity power and construct validity.
We assessed feasibility by calculating the proportion of missing values for the results of the EQ-5D-3L and EQ-5D-5L questionnaires. We tabulated the responses from the descriptive system of EQ-5D-3L and EQ-5D-5L and compared the redistribution. We defined the inconsistency according to Janssen [25] as the proportion of response pairs (from EQ-5D-3L to EQ-5D-5L, all 15 pairs) which does not comply with the scheme: 3L1 to 5L1 or 5L2, 3L2 to 5L2, 5L3 or 5L4 and 3L3 to 5L4 or 5L5 (level 1 from EQ-5D-3L to level 1 from EQ-5D-5L, and so on)—the remaining subgroups are considered inconsistent. The consistent responses pairs are in Table 2. We estimated the EQ-5D index values for both versions of questionnaires based on directly measured value sets for Poland [47, 48].
The ceiling effect is defined as the proportion of respondents with either a “no problem” answer for a dimension or with the best health state (11111) [49]. We hypothesise that the ceiling effect for the EQ-5D-3L version will be higher than for EQ-5D-5L. In the general population, in which the expected percentage of patients with the best health will be higher than in the disease-specific population, it is essential to use a questionnaire as resistant to the ceiling effect as possible.
Informativity power determines the degree of uniform distribution of responses in each dimension. The more evenly the answers are distributed, the more useful the questionnaire is. As a measure of informativity power, we calculated the Shannon index (‘H’) and the Shannon Evenness index (‘J’) [50]. The Shannon index (‘H’) is defined as:
where L is the number of response levels (3 or 5 in EQ-5D) and pi = ni/N is the proportion of observations in the ith level. ‘H’ represents the absolute amount of informativity. The value of ‘H’ ranges from 0 (the weakest discriminatory power) to ‘H’max for a uniform distribution equal to log2L. ‘H’max is different for EQ-5D-3L (1.58; L = 3) and EQ-5D-5L (2.32; L = 5). The 95% confidence intervals for ‘H’ were calculated based on the variance of the Shannon index [51]:
Since the range of values for ‘H’ depends on the levels of possible answers, the parameter which can objectively determine the relative informativity power, the Shannon Evenness index (‘J’), is defined as:
where ‘J’ = 0 signifies the weakest discriminatory power, when all results are clustered around one answer, and ‘J’ = 1 signifies the highest discriminatory power when results are evenly distributed among all the levels of an answer.
Construct validity was analysed in two ways. In the first instance, we analysed it using the method of known-groups validation. For this purpose, we have implemented the analysis of variance model (ANOVA) to explore statistically significant relationships between the EQ-5D index values and age groups (18–29, 30–39, 40–49, 50–59, 60–69, 70+), sex and declared diagnosis of diabetes. We hypothesised that lower values of HRQoL would be more common among older respondents, females and patients having declared diabetes, as reported in studies [52,53,54]. We used linear regression models, for both sexes, to determine the relationship between age and the EQ-5D index values. We also calculated the Spearman coefficients to estimate the correlation between the domains of EQ-5D-3L and EQ-5D-5L, and with the results of EQ VAS and the first question from the SF-12 questionnaire (SF-1: “Is your health: excellent, very good, good, fair, or poor?”) [55].
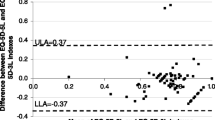
We developed the construct validity assessment by building a theoretical model of the hypothesised relationship between the characteristics of the respondent and the EQ-5D-5L index values, and then comparing the results of the EQ-5D-5L questionnaire with the prediction of the theoretical model. We designed an input–output model that receives a set of five input parameters (age group, sex, level of education, economic status and occurrence of diabetes) and can assign them the expected EQ-5D-5L index value. This model is based on a machine learning algorithm known as random forest [56, 57], commonly used in recent years in biomedical engineering [58,59,60]. The algorithm works by randomly selecting a subset of input data from the training set and learning a single regression tree, which forms the so-called random forest. This scheme is repeated as many times as there are trees in the random forest. The final prediction of the model is the average of the results from an individual tree. To teach the model, we used 60% of the data obtained from the interview database. The model consists of 300 trees, which is a compromise between the expected accuracy of prediction and the complexity of the algorithm. The remaining 40% of the interviews (test data set) is used to determine the convergence of the EQ-5D-5L index values from the survey with the results from the previously built model. For this purpose, we calculated the root-mean-square error measure (RMSEval). We also calculated RMSE for the training data set, based on which the model was built, thus determining the internal error of the theoretical model itself (RMSEint). Then, we compared the internal error distribution for the model itself, along with the RMSE results for the test data (Fig. 1). In our opinion, the convergence of both errors can infer the construct validity of the EQ-5D-5L questionnaire.

The scheme of the novel approach for construct validity assessment as based on the theoretical model
Statistical analysis
We estimated descriptive statistics to characterise the study population. Pearson’s chi-square test statistic was used to determine statistical significance at ceiling effect levels between EQ-5D-3L and EQ-5D-5L. One-way ANOVA was implemented for all of the parameters under consideration. The linear regression model used the least-squares method. Microsoft Excel (Microsoft® Office 365) and R software (3.6.2) [61] (with external packages [62,63,64,65]) were used for the analysis.
Results
The study was conducted on a representative sample of the adult general population of Poland (N = 3978; aged 18–87, 53.2% female; Table 1) [66, 67]. The socio-economic and demographic characteristics of the study population seems to be consistent with the characteristic of the Polish adult population from 2014. Diagnosis of diabetes was declared by 6.8% of respondents. Missing values were found in 0.4%, 0.9% and 0.1% of EQ-5D-5L, EQ-5D-3L and EQ VAS questionnaires, respectively.
The level 1 responses from EQ-5D-3L (3L1) were mostly (92.3%; here and later—on average) replaced by level 1 from EQ-5D-5L (5L1, Table 2). The 3L2 were distributed into 5L2 (49.2%), 5L3 (35.7%) and 5L4 (15.1%). The most uniform distribution of transitions from 3L2 to 5L2, 5L3 and 5L4 was observed for the mobility dimension. The 3L3 responses were distributed into 5L4 (64.5%) and 5L5 (35.5%). The highest proportion of transitions from 3L3 to 5L4 was observed for the pain/discomfort dimension (87.5%). Only for the mobility domain did the proportion of redistribution 3L3 to 5L5 prevailed (62.5%). According to the definition of Janssen [25], the average percentage of inconsistent transitions of results from EQ-5D-3L to EQ-5D-5L was 4.4% (Table 2).
The best health state (“11111”) was reported by 38.0% and 46.6% of the respondents, when answering the EQ-5D-5L and EQ-5D-3L questionnaires, respectively (p < 0.01, Table 3). The highest ceiling effect was observed for the self-care dimension, both for EQ-5D-3L and EQ-5D-5L. The estimated ceiling effects for individual dimensions of EQ-5D-5L and EQ-5D-3L were not statistically different.
Shannon’s index was largest for the pain/discomfort dimension, and smallest for the dimension of self-care, both for the EQ-5D-3L and EQ-5D-5L questionnaires (Table 4). For the EQ-5D-5L questionnaire, an increase in relative informativity power was observed for the dimensions of anxiety/depression, pain/discomfort and mobility and to a greater degree, a decrease in relative informativity power (17.9% and 19.3%) was observed for the dimensions of usual activities and self-care, respectively.
The results of the known-groups validity for the EQ-5D-5L and EQ-5D-3L questionnaires are summarised in Table 5. The analysis of variance indicates statistically significant differences in the results of the EQ-5D index values for six age groups, sex (lower utility score in women) and declared diagnosis of diabetes (lower utility score in diagnosed diabetes), both for EQ-5D-5L and EQ-5D-3L, which confirms the previous hypothesis. A reduction of EQ-5D-5L index value with age was observed, and this tendency was noted by the negative linear trend in the regression models:
In Table 6, we collected the results of the convergent validity assessment between the EQ-5D-5L questionnaire and EQ VAS, EQ-5D-3L and SF-1. In most cases, we observed a moderate correlation. The results for the same dimensions from EQ-5D-5L and EQ-5D-3L were convergent (italic in Table 6). Mobility and pain/discomfort are the dimensions most correlated with EQ VAS and SF-1.
The random forest algorithm for construct validity
The theoretical model which can predict what the HRQoL of a patient with a specific characteristic will look like, was constructed on the basis of the random forest algorithm, which is widely used in machine learning. For the assessment of construct validity, we wanted to compare the results of prediction HRQoL from the model with the results from the survey. The internal error of the theoretical model (RMSEint for the training data set) was 0.095 in utility units. This means that the model, using the same data set from which it was taught, makes an average prediction error of < 0.1 utility units. The RMSEval measure was equal to 0.121. This was calculated for the difference between the prediction of the theoretical model and the testing data set. In Fig. 2, we present the comparison of the theoretical model error distribution with the error distribution for the test data set. It can be seen that these distributions overlap almost completely. The estimations in Table 7 indicate that 85.6% of the errors for the test data set were lower than the 95th quantile of the theoretical model error distribution. On this basis, we can state that the results obtained from the EQ-5D-5L questionnaire (EQ-5D-5L index value) are consistent with the theory (developed from the model), which suggests a positive assessment of the construct validity of the EQ-5D-5L questionnaire.

The comparison of the model internal error (red) and testing data set prediction error (grey) distributions. (Color figure online)
Discussion
According to our best knowledge, this is the first study reporting the validity of the EQ-5D-5L in comparison to EQ-5D-3L, measured on the same sample of the general population coming from a European country. A novel approach for construct validity assessment was proposed, based on the machine learning algorithm known as the random forest.
We identified other studies from Greece [72] and Spain [51], in which authors compared the EQ-5D-5L and EQ-5D-3L in the same sample, but they include limitations. The Greek study population was from Athens and in age over 40, so this not constitute the general population of a country. In the Spanish study, the sample was from Catalonia. Both analyses used the mapping methods for calculation of the country value sets. In our study, for an estimate of both the EQ-5D-5L and EQ-5D-3L index values, we used directly measured country-specific value sets.
The results of the analysis show that the EQ-5D-5L questionnaire has a lower ceiling effect compared to the EQ-5D-3L version. Redistribution from EQ-5D-3L to EQ-5D-5L was similar for each dimension (i.e. transfer responses from 3L1 to 5L1 are more common than from 3L1 to 5L2 [about 90% vs 10%], transfer responses from 3L2 to 5L2 and 3L2 to 5L3 are more common than from 3L2 to 5L4, and transfer responses from 3L3 to 5L4 are more common than from 3L3 to 5L5 [about 70% vs 30%]). The mean inconsistency did not exceed 5%. In terms of Shannon's relative informativity power, the discrepancy of the results between each domain does not allow to draw clear conclusions about the advantage of one version of the questionnaire. The results of known-groups validation confirmed the hypothesis about the relationship between the EQ-5D index value and age group, sex and occurrence of diabetes. Individual dimensions of EQ-5D-5L correlate with the assessment of health on the EQ VAS scale, with the domains from EQ-5D-3L and SF-1. The results imply that EQ-5D-5L is a valid instrument for use in the Polish adult population.
The strength of this study lies in the fact that both the EQ-5D-5L and EQ-5D-3L questionnaire and EQ VAS results came from the same study iteration, and all are evaluated on the same occasion in the same group. Often, in studies comparing the properties of EQ-5D-3L and EQ-5D-5L in the general population, the samples for both versions of questionnaires were separate [68, 69]. The recently published study by Thompson et al. is also a kind of “indirect study”. Still, authors used the matching method to join individuals completing the EQ-5D-3L with those completing the EQ-5D-5L, and thus increasing the sample size [70].
We conducted our study on a representative sample of the general adult population of Poland. Therefore, validation of the EQ-5D-5L questionnaire takes into account a wide spectrum of a population characteristic. In the literature, a comparison of EQ-5D-3L and EQ-5D-5L questionnaire properties were often carried out in smaller populations that did not apply to the whole country [51, 69, 71,72,73]. The exceptions were studies performed in England, Germany, Spain, USA, South Korea, Japan and Malaysia [68, 74,75,76,77,78,79]. The psychometric properties may also be assessed in studies of value sets for individual countries, although they are often limited to the distribution of responses or the ceiling/floor effects [80, 81]. In our study, we used the directly measured country-specific EQ-5D index value sets for Poland, developed for both versions of the EQ-5D questionnaire (time trade-off (TTO)-based for EQ-5D-3L and TTO/discrete choice experiment (DCE)-based for EQ-5D-5L [47, 48]). This increased the reliability of the presented HRQoL assessment. In other studies, the interim scoring value sets for EQ-5D-5L were used [51, 72, 75, 77] or the EQ-5D index values were not estimated [69, 73, 74, 76, 79]. The directly measured country-specific value sets were used only in one study from Japan [78].
As a part of the construct validity assessment, we proposed a novel approach based on the theoretical model for HRQoL assessment in the Polish population, designed using the random forest algorithm for regression. Developing the model based on data obtained from a representative sample of the general population represents an attempt to create a reference for the HRQoL results that depends on the parameters describing the population characteristics. Relating the results of the questionnaire to the HRQoL predicted by the model, and comparing the accuracy of such an assessment with the accuracy of the model itself, allows us to conclude that the questionnaire is convergent with the predicted theory.
One of the limitations of this study may be the inability to assess reliability and responsiveness (similar results in the same study sample for a repeated protocol). Another potential limitation is the lack of construct validity assessment (through known-groups validation) related to multimorbidity. Further, the diagnoses of diabetes in our study are not the result of clinical assessment but were based on self-reporting. The fixed order of presented questionnaires in the survey could pose some limitations (i.e. introduce ordering effect). However, the introduction of the SF-12 questionnaire between the EQ-5D-5L and the EQ-5D-3L questionnaires may somehow eliminate the potential response memory effect.
Similarly to our study, a significant reduction in the ceiling effect for EQ-5D-5L in comparison to EQ-5D-3L was observed in other general population studies [28, 51, 68, 69, 71,72,73, 76, 77, 79] (Table 8). It is also worth noting that the ceiling effect at the level of 38% for EQ-5D-5L is much lower than the results obtained in other countries, which may be influenced by the characteristics of the studied populations themselves [51, 79]. The higher percentage of missing answers for EQ-5D-3L could be explained by the sequence of questionnaires in the survey (EQ-5D-3L was always the last one to be completed). As expected, an increase in Shannon informativity power was observed for the EQ-5D-5L questionnaire [28, 51, 72, 79]. However, the relative informativity power was often similar or lower than in the EQ-5D-3L questionnaire, which prevents us from claiming that EQ-5D-5L has greater informativity power than EQ-5D-3L, as has been reported in other studies [51, 68, 79]. The results of the study indicated a relatively large percentage of inconsistencies (4.4%), while in other studies it rarely exceeded 2% on average [71, 77]. In Janssen et al. [25], where the definition of inconsistency came from, it was 1.1% with 5912 observations. The results from our survey seem to be quite different from this (4.4% in 3978 observations), which may mean that the respondents to the EQ-5D-3L and EQ-5D-5L questionnaires were not entirely consistent. Perhaps it was related to the fact that the EQ-5D-3L questionnaire was not completed first and not immediately after EQ-5D-5L (EQ VAS and SF-12 were completed in between). Our results for the known-groups validation are convergent with other analyses [71, 72, 77], in particular, with respect to age and gender. No data were found analysing the convergence of the EQ-5D index values with declared diabetes in the general population.
In Henry et al. [82] authors estimated the minimally important difference (MID) for EQ-5D-5L scoring algorithms, including that from the Polish population. The mean result was 0.080 (0.030). The range of MID averages for different countries was from 0.072 (Malaysia) to 0.101 (Taiwan). In Coretti et al. [83] the minimally (clinically) important difference (MCID) for EQ-5D index value ranged from 0.03 to 0.54, with the raw average across 18 studies of 0.18. However, Coretti et al. review was about disease-specific populations. In our construct validity assessment based on the theoretical model the RMSEval (0.121) measure appears to be close to one SD difference above from the average value for the Polish algorithm and within the range described by Coretti et al. Due to the large scatter of the estimated MID it is still difficult to say if RMSEval is large or small. However, in our approach to the construct validity assessment, the most critical aspect is the convergence between the RMSEval and RMSEint rather than the utility results, and in this case, we observed that the errors distributions overlap almost completely (Fig. 2).
In Poland, we found only one validation study of a generic questionnaire (SF-36v2) for the general population of a country [84], and one assessment of the reliability of the generic questionnaire (WHOQOL-BREF) within a local community (Silesian agglomeration [85]). The fact that the EQ-5D validation study has not been available constituted essential unmet research need, as EQ-5D is commonly used among Polish patients and is recommended by the guidelines (Polish Agency for Health Technology Assessment [86]). Our study would support the credibility of the questionnaire and the correct interpretation of its results. Moreover, this study may also support its validity in countries with similar socio-economic characteristics in Central and Eastern Europe.
In the future, it would be worth assessing the reliability and responsiveness of the EQ-5D-5L questionnaire and extending the validity assessment with other parameters of the population characteristics, including multimorbidity.
Conclusions
In this study, the validity of the EQ-5D-5L questionnaire was assessed in a sample of the general adult population of Poland and, in comparison with EQ-5D-3L, showed similar (informativity power, known-groups validation) or better (ceiling effect) psychometric properties for this population. A novel approach to the assessment of construct validity was proposed, based on the use of the machine learning technique known as the random forest algorithm. The comparison of the model predictions and the results of the interviews provided a basis for the positive assessment of the construct validity. EQ-5D-5L is a commonly used instrument in HRQoL assessment, and this study will support the correct interpretation of its results in studies performed among the Polish population.
Data availability
Data are available from the author on a reasonable request.
Code availability
Not applicable.
References
Fayers, P. M., & Machin, D. (2007). Scores and measurements: Validity, reliability, sensitivity. In P.M. Fayers & D. Machin (Eds.), Quality of life. The assessment, analysis and interpretation of patient-reported outcomes (2nd ed., pp. 77–108). Chichester: Wiley.
Mokkink, L., Prinsen, C., Patrick, D., et al. (2019). COSMIN Study Design checklist for Patient-reported outcome measurement instruments. COnsensus-based Standards for the selection of health Measurement INstruments, Ver. July 2019. https://www.cosmin.nl/wp-content/uploads/COSMIN-study-designing-checklist_final.pdf. Accessed 15 July 2020.
Młyńczak, K., & Golicki, D. (2016). The review of psychometric properties of health related quality of life (HRQoL) instruments. Polish Review of Health Sciences, 4(49), 415–421.
Devlin, N. J., & Brooks, R. (2017). EQ-5D and the EuroQol group: Past, present and future. Applied Health Economics and Health Policy, 15(2), 127–137.
Brooks, R. (1996). EuroQol: The current state of play. Health Policy, 37(1), 53–72.
The EuroQol Group. (1990). EuroQol—A new facility for the measurement of health-related quality of life. Health Policy, 16(3), 199–208.
EQ-5D. https://www.euroqol.org. Accessed 04 January 2020.
Szende, A., Oppe, M., & Devlin, N. (2007). EQ-5D value sets: Inventory, comparative review and user guide. In A. Szende, M. Oppe, & N. Devlin (Eds.), EuroQol group monographs. Dordrecht: Springer.
Dyer, M. T. D., Goldsmith, K. A., Sharples, L. S., & Buxton, M. J. (2010). A review of health utilities using the EQ-5D in studies of cardiovascular disease. Health and Quality of Life Outcomes, 8, 13.
Prieto, L., Novick, D., Sacristan, J. A., Edgell, E. T., Alonso, J., & on behalf of the SOHO Study Group. (2003). A Rasch model analysis to test the cross-cultural validity of the EuroQoL-5D in the Schizophrenia Outpatient Health Outcomes Study. Acta Psychiatrica Scandinavica, 107(Suppl. 416), 24–29.
Luo, N., Chew, L. H., Fong, K. Y., Koh, D. R., Ng, S. C., Yoon, K. H., et al. (2003). Validity and reliability of the EQ-5D self- report questionnaire in English-speaking Asian patients with rheumatic diseases in Singapore. Quality of Life Research, 12(1), 87–92.
Brussoni, M., Kruse, S., & Walker, K. (2013). Validity and reliability of the EQ-5D-3LTM among a paediatric injury population. Health and Quality of Life Outcomes, 11, 157.
Lang, H. C., Chuang, L., Shun, S. C., Hsieh, C. L., & Lan, C. F. (2010). Validation of EQ-5D in patients with cervical cancer in Taiwan. Supportive Care in Cancer, 18(10), 1279–1286.
Janssen, M. F., Lubetkin, E. I., Sekhobo, J. P., & Pickard, A. S. (2011). The use of the EQ-5D preference-based health status measure in adults with Type 2 diabetes mellitus. Diabetic Medicine, 28(4), 395–413.
Aburuz, S., Bulatova, N., Twalbeh, M., & Gazawi, M. (2009). The validity and reliability of the Arabic version of the EQ-5D: A study from Jordan. Annals of Saudi Medicine, 29(4), 304–308.
Kontodimopoulos, N., Pappa, E., Niakas, D., Yfantopoulos, J., Dimitrakaki, C., & Tountas, Y. (2008). Validity of the EuroQoL (EQ-5D) instrument in a Greek general population. Value in Health, 11(7), 1162–1169.
Johnson, J. A., & Pickard, A. S. (2000). Comparison of the EQ- 5D and SF-12 health surveys in a general population survey in Alberta, Canada. Medicinal Care, 38(1), 115–121.
Burstrom, K., Johannesson, M., & Diderichsen, F. (2001). Health-related quality of life by disease and socio-economic group in the general population in Sweden. Health Policy, 55(1), 51–69.
Johnson, J. A., & Coons, S. J. (1998). Comparison of the EQ-5D and SF-12 in an adult US sample. Quality of Life Research, 7(2), 155–166.
Badia, X., Schiaffino, A., Alonso, J., & Herdman, M. (1998). Using the EuroQol 5-D in the Catalan general population: Feasibility and construct validity. Quality of Life Research, 7, 311–322.
Lubetkin, E., Jia, H., & Gold, M. R. (2004). Construct validity of the EQ-5D in low-income Chinese American primary care patients. Quality of Life Research, 13(8), 1459–1468.
Payakachat, N., Ali, M. M., & Tilford, J. M. (2015). Can the EQ-5D detect meaningful change? A systematic review. Pharmacoeconomics, 33(11), 1137–1154.
Herdman, M., Gudex, C., Lloyd, A., Janssen, M., Kind, P., Parkin, D., et al. (2011). Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Quality of Life Research, 20(10), 1727–1736.
Van Reenen, M., & Janssen, B. (2015). EQ-5D-5L User Guide. Basic Information on how to use the EQ-5D-5L instrument. Version 2.1. EuroQol Research Foundation.
Janssen, M. F., Birnie, E., Haagsma, J. A., & Bonsel, G. J. (2008). Comparing the standard EQ-5D three-level system with a five-level version. Value in Health, 11(2), 275–284.
Lloyd, A. (2018). EQ-5D: Moving from three levels to five. Editorial. Value in Health, 21(1), 57–58.
Buchholz, I., Janssen, M. F., Kohlmann, T., & Feng, Y. S. (2018). A systematic review of studies comparing the measurement properties of the three-level and five-level versions of the EQ-5D. Pharmacoeconomics, 36(6), 645–661.
Janssen, M. F., Bonsel, G. J., & Luo, N. (2018). Is EQ-5D-5L better than EQ-5D-3L? A head-to-head comparison of descriptive systems and value sets from seven countries. Pharmacoeconomics, 36(6), 675–697.
Buchholz, I., Thielker, K., Feng, Y. S., Kupatz, P., & Kohlmann, T. (2015). Measuring changes in health over time using the EQ-5D 3L and 5L: A head-to-head comparison of measurement properties and sensitivity to change in a German inpatient rehabilitation sample. Quality of Life Research, 24(4), 829–835.
Conner-Spady, B. L., Marshall, D. A., Bohm, E., Dunbar, M. J., Loucks, L., Al, K. A., et al. (2015). Reliability and validity of the EQ-5D-5L compared to the EQ-5D-3L in patients with osteoarthritis referred for hip and knee replacement. Quality of Life Research, 24(7), 1775–1784.
Greene, M. E., Rader, K. A., Garellick, G., Malchau, H., Freiberg, A. A., & Rolfson, O. (2015). The EQ-5D-5L improves on the EQ-5D-3L for health-related quality-of-life assessment in patients undergoing total hip arthroplasty. Clinical Orthopaedics and Related Research, 473(11), 3383–3390.
Golicki, D., Niewada, M., Buczek, J., Karlińska, A., Kobayashi, A., Janssen, M. F., et al. (2015). Validity of EQ-5D-5L in stroke. Quality of Life Research, 24(4), 845–850.
Golicki, D., Niewada, M., Karlińska, A., Buczek, J., Kobayashi, A., Janssen, M. F., et al. (2015). Comparing responsiveness of the EQ-5D-5L, EQ-5D-3L and EQ VAS in stroke patients. Quality of Life Research, 24(6), 1555–1563.
Jia, Y. X., Cui, F. Q., Li, L., Zhang, D. L., Zhang, G. M., Wang, F. Z., et al. (2014). Comparison between the EQ-5D-5L and the EQ-5D-3L in patients with hepatitis B. Quality of Life Research, 23(8), 2355–2363.
Scalone, L., Ciampichini, R., Fagiuoli, S., Gardini, I., Fusco, F., Gaeta, L., et al. (2013). Comparing the performance of the standard EQ-5D 3L with the new version EQ-5D 5L in patients with chronic hepatic diseases. Quality of Life Research, 22(7), 1707–1716.
Scalone, L. (2011). Comparing the standard EQ-5D-3L versus 5L version for the assessment of health of patients with live diseases. EuroQol Proceedings, 16, 213–239.
Kim, S. H., Kim, H. J., Lee, S. I., & Jo, M. W. (2012). Comparing the psychometric properties of the EQ-5D-3L and EQ-5D-5L in cancer patients in Korea. Quality of Life Research, 21(6), 1065–1073.
Khan, I., Morris, S., Pashayan, N., Matata, B., Bashir, Z., & Maguirre, J. (2016). Comparing the mapping between EQ-5D-5L, EQ-5D-3L and the EORTC-QLQ-C30 in non-small cell lung cancer patients. Health and Quality of Life Outcomes, 14, 60.
Pan, C. W., Sun, H. P., Wang, X., Ma, Q., Xu, Y., Luo, N., et al. (2015). The EQ-5D-5L index score is more discriminative than the EQ-5D-3L index score in diabetes patients. Quality of Life Research, 24(7), 1767–1774.
Pattanaphesaj, J., & Thavorncharoensap, M. (2015). Measurement properties of the EQ-5D-5L compared to EQ-5D-3L in the Thai diabetes patients. Health and Quality of Life Outcomes, 13, 14.
Poór, A. K., Rencz, F., Brodszky, V., Gulácsi, L., Beretzky, Z., Hidvégi, B., et al. (2017). Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L in psoriasis patients. Quality of Life Research, 26, 3409–3419.
Yfantopoulos, J., Chantzaras, A., & Kontodimas, S. (2017). Assessment of the psychometric properties of the EQ-5D-3L and EQ-5D-5L instruments in psoriasis. Archives of Dermatological Research, 309, 357–370.
Janssen, M. F., Pickard, A. S., Golicki, D., Gudex, C., Niewada, M., Scalone, L., et al. (2013). Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: A multi-country study. Quality of Life Research, 22(7), 1717–1727.
Gandhi, M., Ang, M., Teo, K., et al. (2019). EQ-5D-5L is more responsive than EQ-5D-3L to treatment benefit of cataract surgery. The Patient-Patient-Centered Outcomes Research, 12(4), 383–392.
Rencz, F., Lakatos, P. L., Gulácsi, L., et al. (2019). Validity of the EQ-5D-5L and EQ-5D-3L in patients with Crohn’s disease. Quality of Life Research, 28(1), 141–152.
Eneqvist, T., Nemes, S., Kärrholm, J., et al. (2020). How do EQ-5D-3L and EQ-5D-5L compare in a Swedish total hip replacement population? Acta Orthopaedica, 91(3), 272–278.
Golicki, D., & Niewada, M. (2015). General population reference values for 3-level EQ-5D (EQ-5D-3L) questionnaire in Poland. Polskie Archiwum Medycyny Wewnetrznej, 125(1–2), 18–26.
Golicki, D., Jakubczyk, M., Graczyk, K., & Niewada, M. (2019). Valuation of EQ-5D-5L health states in Poland: The first EQ-VT-based study in Central and Eastern Europe. Pharmacoeconomics, 37(9), 1165–1176.
Terwee, C. B., Bot, S. D., de Boer, M. R., van der Windt, D. A., Knol, D. L., Dekker, J., et al. (2007). Quality criteria were proposed for measurement properties of health status questionnaires. Journal of Clinical Epidemiology, 60(1), 34–42.
Shannon, C. E. (1997). The mathematical theory of communication. 1963. MD Computing, 14, 306–317.
Martí-Pastor, M., Pont, A., Ávila, M., Garin, O., Vilagut, G., Forero, C. G., et al. (2018). Head-to-head comparison between the EQ-5D-5L and the EQ-5D-3L in general population health surveys. Population Health Metrics, 16(1), 14.
Golicki, D., & Niewada, M. (2017). EQ-5D-5L Polish population norms. Polskie Archiwum Medycyny Wewnetrznej, 13(1), 191–200.
Sun, S., Chen, J., Johannesson, M., et al. (2011). Population health status in China: EQ-5D results, by age, sex and socio-economic status, from the National Health Services Survey 2008. Quality of Life Research, 20(3), 309–320.
Ferreira, L. N., Ferreira, P. L., Pereira, L. N., et al. (2014). EQ-5D Portuguese population norms. Quality of Life Research, 23(2), 425–430.
Ware, J. E., Kosinski, M., & Keller, S. D. (1996). A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Medical Care, 34, 220–233.
Ho, T. K. (1995). Random decision forests. Proceedings of 3rd International Conference on Document Analysis and Recognition (Vol. 1, pp. 278–282).
Breiman, L. (2001). Random forests. Machine Learning, 45(1), 5–32.
Shaikhina, T., Lowe, D., Daga, S., Briggs, D., Higgins, R., & Khovanova, N. (2019). Decision tree and random forest models for outcome prediction in antibody incompatible kidney transplantation. Biomedical Signal Processing and Control, 52, 456–462.
Alam, M. Z., Rahman, M. S., & Rahman, M. S. (2019). A Random Forest based predictor for medical data classification using feature ranking. Informatics in Medicine Unlocked, 15, 1–12.
Mohapatra, S. K., & Mohanty, M. N. (2020). Big data analysis and classification of biomedical signal using random forest algorithm. In S. Patnaik, A. Ip, M. Tavana, & V. Jain (Eds.), New paradigm in decision science and management. Advances in intelligent systems and computing (Vol. 1005, pp. 217–224). Singapore: Springer.
R Core Team. (2019). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/.
Kuhn, M. (2020). caret: Classification and regression training. R package version 6.0-85. https://CRAN.R-project.org/package=caret.
Liaw, A., & Wiener, M. (2002). Classification and regression by randomForest. R News, 2(3), 18–22.
Wickham, H., & Bryan, J. (2019). readxl: Read Excel Files. R package version 1.3.1. https://CRAN.R-project.org/package=readxl.
Wickham, H. (2016). ggplot2: Elegant graphics for data analysis. New York: Springer.
Central Statistical Office of Poland. (2014). Demographic Yearbook of Poland 2013. Warsaw.
Central Statistical Office of Poland. (2014). Statistical Yearbook of Poland 2013. Warsaw.
Feng, Y., Devlin, N., & Herdman, M. (2015). Assessing the health of the general population in England: How do the three- and five-level versions of EQ-5D compare? Health and Quality of Life Outcomes, 13, 171.
Agborsangaya, C. B., Lahtinen, M., Cooke, T., & Johnson, J. A. (2014). Comparing the EQ-5D 3L and 5L: Measurement properties and association with chronic conditions and multimorbidity in the general population. Health and Quality of Life Outcomes, 12, 74.
Thompson, A. J., & Turner, A. J. (2020). A comparison of the EQ-5D-3L and EQ-5D-5L. PharmacoEconomics, 38, 575–591.
Ferreira, L. N., Ferreira, P. L., Ribeiro, F. P., & Pereira, L. N. (2016). Comparing the performance of the EQ-5D-3L and the EQ-5D-5L in young Portuguese adults. Health and Quality of Life Outcomes, 14, 89.
Yfantopoulos, J. N., & Chantzaras, A. E. (2017). Validation and comparison of the psychometric properties of the EQ-5D-3L and EQ-5D-5L instruments in Greece. The European Journal of Health Economics, 18(4), 519–531.
Scalone, L., Cortesi, P. A., Ciampichini, R., Cesana, G., & Mantovani, L. G. (2015). Health Related Quality of Life norm data of the general population in Italy: Results using the EQ-5D-3L and EQ-5D-5L instruments. Epidemiology Biostatistics and Public Health, 12(3), 1–15.
Hinz, A., Kohlmann, T., Stöbel-Richter, Y., Zenger, M., & Brähler, E. (2014). The quality of life questionnaire EQ-5D-5L: Psychometric properties and normative values for the general German population. Quality of Life Research, 23(2), 443–447.
Hernandez, G., Garin, O., Pardo, Y., Vilagut, G., Pont, À., Suárez, M., et al. (2018). Validity of the EQ-5D-5L and reference norms for the Spanish population. Quality of Life Research, 27(9), 2337–2348.
Craig, B. M., Pickard, A. S., & Lubetkin, E. I. (2014). Health problems are more common, but less severe when measured using newer EQ-5D versions. Journal of Clinical Epidemiology, 67(1), 93–99.
Kim, T. H., Jo, M. W., Lee, S. I., Kim, S. H., & Chung, S. M. (2013). Psychometric properties of the EQ-5D-5L in the general population of South Korea. Quality of Life Research, 22(8), 2245–2253.
Shiroiwa, T., Fukuda, T., Ikeda, S., Igarashi, A., Noto, S., Saito, S., et al. (2016). Japanese population norms for preference-based measures: EQ-5D-3L, EQ-5D-5L, and SF-6D. Quality of Life Research, 25(3), 707–719.
Shafie, A. A., Vasan Thakumar, A., Lim, C. J., & Luo, N. (2019). Psychometric performance assessment of Malay and Malaysian English version of EQ-5D-5L in the Malaysian population. Quality of Life Research, 28(1), 153–162.
Law, E. H., Pickard, A. S., Xie, F., Walton, S. M., Lee, T. A., & Schwartz, A. (2018). Parallel valuation: A direct comparison of EQ-5D-3L and EQ-5D-5L societal value sets. Medical Decision Making, 38(8), 968–982.
Mulhern, B., Feng, Y., Shah, K., et al. (2018). Comparing the UK EQ-5D-3L and English EQ-5D-5L value sets. Pharmacoeconomics, 36(6), 699–713.
Henry, E. B., Barry, L. E., Hobbins, A. P., McClure, N. S., & O’Neill, C. (2020). Estimation of an instrument-defined minimally important difference in EQ-5D-5L Index Scores based on scoring algorithms derived using the EQ-VT version 2 valuation protocols. Value in Health, 23(7), 936–944.
Coretti, S., Ruggeri, M., & McNamee, P. (2014). The minimum clinically important difference for EQ-5D index: A critical review. Expert Review of Pharmacoeconomics & Outcomes Research, 14(2), 221–233.
Żołnierczyk-Zreda, D. (2010). The Polish version of the SF-36v2 questionnaire for the quality of life assessment. Przeglad Lekarski, 67(12), 1302–1307.
Kowalska, M., Skrzypek, M., Danso, F., & Humeniuk, M. (2012). Assessment of reliability of the whoqol-bref questionnaire in a study of quality of life among adults, the economically active population of the Silesian agglomeration. Przegla̧d epidemiologiczny, 66, 531–537.
The Polish Agency for Health Technology Assessment and Tariff System. Health Technology Assessment Guidelines. Version 3.0. Warsaw, August 2016. https://www.aotm.gov.pl/www/wp-content/uploads/wytyczne_hta/2016/20161104_HTA_Guidelines_AOTMiT.pdf. Accessed 04 February 2020.
Acknowledgements
We would like to thank Marcin Hermann from the CBOS market research company and Maciej Niewada from HealthQuest for coordinating the survey.
Funding
HealthQuest sp. z o.o., sp. kom. (Warsaw, Poland) and EuroQol Group (Rotterdam, Netherlands) funded the collection of data.
Author information
Authors and Affiliations
Contributions
KM contributed to study design, preparation and critical interpretation of the analyses, statistical analysis, literature search and manuscript draft. DG contributed to study design, data acquisition, critical interpretation of the analyses and manuscript draft. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
KM is an employee of HealthQuest sp. z o.o., sp. kom. (Warsaw, Poland). DG is a member of the EuroQol Group, a not-for-profit organization that develops and distributes instruments that assess and value health. DG is also a shareholder of HealthQuest. All authors did not receive funding for performing this study.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (The Bioethics Committee of the Medical University of Warsaw (AkBE/34/17)) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Consent for publication
Data collected in the study were anonymity and do not allow to identify the person.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Młyńczak, K., Golicki, D. Validity of the EQ-5D-5L questionnaire among the general population of Poland. Qual Life Res 30, 817–829 (2021). https://doi.org/10.1007/s11136-020-02667-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-020-02667-3