
Abstract
Background
Coronary artery disease (CAD) is showing an increasing trend in young adults. Cigarette smoking has been shown to be a major cause of premature CAD. Previous studies have also shown that hyperuricemia (HUA) is associated with CAD; however, the interaction effect between HUA and smoking on CAD is uncertain. Therefore, this study was designed to determine the relationship and interactive effects of HUA and smoking on the risk of CAD in young adults ≤ 35 years of age.
Methods
In this observational study we consecutively included adults (18–35 years of age) with suspected CAD who underwent coronary angiography for the first time in our institution from January 2005 to December 2015. Patients with stenosis affecting ≥50% of the luminal diameter and acute myocardial infarction were considered to have CAD. A serum uric acid (SUA) level ≥ 7.0 mg / dl (420 mmol / L) in males and ≥ 6.0 mg / dl (357 mmol / L) in females was defined as hyperuricemia. We tested for an interaction between HUA and cigarrete smoking on CAD. The relationship between HUA, cigarrete smoking, and CAD was assessed by multivariate logistic regression analysis.
Results
A total of 1113 participants were included in this study; 771 participants were confirmed to have CAD. HUA was present in 34.8% of the participants. HUA was significantly higher in the CAD group (odds ratio [OR], 1.34; 95% confidence interval [CI], 1.02–1.76; p = 0.035). More smokers were in the CAD group (OR, 1.59; 95% CI, 1.22–2.07; p = 0.001). Based on multivariate regression analysis and after adjustment for age, BMI, high LDL-C level, low HDL-C level, hypercholesterolemia, hypertriglyceridemia, metabolic syndrome, diabetes mellitus, and hypertension, HUA was shown to be strongly associated with the presence of CAD in non-smokers (OR, 1.84; 95% CI, 1.03–3.29; p = 0.039). We further demonstrated that the interaction between HUA and cigarrete smoking achieved statistical significance for the presence of CAD (p = 0.008).
Conclusions
In the current study, HUA was shown to be associated with the presence of CAD in non-smokers ≤ 35 years of age.
Similar content being viewed by others


Background
Coronary artery disease (CAD) is relatively rare in patients < 40 years of age, occurring in 6–10% of all patients < 40 years of age; however, there has recently been an increase in incidence [1, 2]. A variety of risk factors are known to be involved in the onset and progression of CAD [3], the contributions of which vary in patients of different ages. Cigarette smoking has been shown to be a major cause of premature CAD. Several studies have described the relationship between hyperuricemia (HUA) and CAD in middle-aged and elderly populations [4, 5]. These studies have shown that HUA may play a role in CAD; however, due to the relatively low prevalence of CAD in young adults, the association between HUA and CAD in young adults has not elicited attention among the public.
Given the oxidative and inflammatory-induced properties of HUA and cigarrete smoking, along with the associations with risk for CAD, investigating the effect of the interaction between HUA and current smokers on premature CAD is warranted.
Thus, the current study was designed to determine the following: 1) association between HUA and CAD; 2) association between cigarette smoking and CAD; 3) interactive effect of both factors on the risk for CAD in young adults ≤ 35 years of age; and 4) the association between HUA and cigarrete smoking in the study participants.
Methods
Study population
In this observational study, young adults suspected to have CAD (18–35 years of age) who underwent coronary angiography for the first time at Anzhen Hospital between January 2005 and December 2015 were consecutively enrolled. Our study was approved by the Institutional Ethics Committee at Beijing Anzhen Hospital. Written informed consent was gained from all participants. The exclusion criteria were as follows: 1. gout, heart failure, renal impairment (an estimated glomerular filtration rate [eGFR] < 60 mL/minute per 1.73 m2), inflammatory diseases, autoimmune diseases (Takayasu’s arteritis, infective endocarditis, and rheumatic heart disease), and missing uric acid data; 2. medication history prior to admission, including diuretics or anti-hypertension drugs, losartan and hydrochlorothiazide tablets, compound amiloride hydrochloride tablets, irbesartan, and hydrochlorothiazide, which are known to affect the level of uric acid; 3. previous percutaneous coronary intervention or coronary artery bypass grafting in our institution; and 4. congenital heart disease, cardiomyopathy, and valvular heart disease.
Ascertainment of outcome
Coronary angiography was performed using a standardized technique. Coronary angiogram results were affirmed by two experienced cardiologists. Major epicardial coronary arteries, including the left main, left anterior descending, left circumflex, right coronary artery, and the vessels’ main branches, were evaluated, and a luminal diameter stenosis ≥50% in any of the vessels above was defined as CAD. Patients with a history of an acute myocardial infarction were also considered to have CAD.
Definition and collection of variables
Based on published clinical guidelines, HUA was defined as a serum uric acid (SUA) level ≥ 7.0 mg/dl (420 mmol / L) in males and ≥ 6.0 mg / dl (357 mmol/L) in females [6]. Hypertension was defined as a blood pressure ≥ 140/90 mmHg or using anti-hypertension medications [7]. Diabetes mellitus was defined according to the WHO diabetes diagnostic criteria in 1999. LDL-C ≥ 130 mg/dl (3.4 mmol / L) was considered to be a high LDL-C level, TG ≥ 150 mg/dl (1.7 mmol / L) was considered to be hypertriglyceridemia, HDL-C < 40 mg/dl (1.0 mmol / L) was considered to be a low HDL-C level, and TC ≥ 200 mg/dl (5.2 mmol / L) was considered to be hypercholesterolemia [8].
SUA was analyzed on a Beckmann AU54 automated biochemical analyzer (Beijing, China) using a uric acid commercial kit (uricase-peroxidase method).
Personal histories of hypertension, diabetes mellitus, a family history of CAD, cigarette smoking, and alcohol consumption were collected from electronic medical records.
Statistical analyses
Continuous variables are presented as the mean ± standard deviation and compared using an unpaired t-test for normally distributed data or as the median with interquartile range and compared using a Mann-Whitney U test for non-normally distributed data. Categorical variables are presented as frequencies or percentages and compared using a chi-square test. Univariate analysis was performed, then covariates with a p < 0.05 on the univariate analysis were analyzed for collinearity. The variables were then selected and added to a multivariable analysis. The relationship between HUA, cigarrete smoking, and the presence of CAD was evaluated with multivariate logistic regression analysis. A p value ≤0.05 (two-sided) was considered statistically significant. We tested for interactions between uric acid (HUA or normouricemia) and cigarrete smoking on the risk for CAD. A p-value for interaction was measured using the log likelihood ratio test to determine if there was a significant difference between the following two regression models: 1. a complex regression model including not only the exposure and confounding factors, but also the interaction terms of each of the factors with the effect modifier; and 2. a simple model without the interaction terms. With a p-value for interaction < 0.05, there was a significant difference between the two models, indicating that the complex model interpreted the data better. All analyses were performed with the statistical software package R and EmpowerStats (http://www.empowerstats.com; X&Y Solutions, Inc., Boston, MA, USA) [9].
Results
Patient demographics
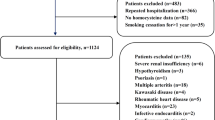
A total of 1113 participants fulfilling the criteria were enrolled in this observational study. The mean age was 31.8 years and 93.7% of the participants were male. Additional file 1: Figure S1 shows the flow chart of the study. The 771 participants with ≥50% major cardiac artery narrowing and a history of an acute myocardial infarction made up the CAD group, and the remaining 342 participants comprised the non-CAD group. The baseline characteristics are shown in Table 1. Current smokers and hypertriglyceridemia were more prevalent in the CAD group than the non-CAD group (68.2% vs. 57.4% and 60.6% vs. 47.8%, respectively; P<0.001). The CAD group also had a decreased level of HDL-C (P<0.001). Moreover, a greater percentage of patients with HUA were in the CAD group (p = 0.034). In the CAD group, 21.6% of patients were treated with drugs.
Univariate analysis of different CAD risk factors
Univariate analysis showed that the traditional CAD risk factors for cigarette smoking, BMI, family history of CAD, hypertriglyceridemia, low level of HDL-C, metabolic syndrome, and diabetes mellitus were significantly associated with the presence of CAD (P<0.05). In contrast, the risk factors for hypertension and hypercholesterolemia were not significantly related to CAD(Table 2). Within the entire patient group, univariate analysis revealed that HUA was significantly associated with the occurrence of CAD (OR, 1.34; 95% CI, 1.02–1.76; p = 0.035; Table 2).
Multivariate logistic regression analysis model of different traditional CAD risk factors
Logistic regression analysis further indicated that the traditional CAD risk factors, such as cigarette smoking, diabetes mellitus, and hypertriglyceridemia, had significant associations with the presence of CAD (P<0.05; Fig. 1).

Forest plot of Multi-variate logistic regression analysis model of different CAD risk factors. Logistic regression analysis indicated that cigarrete smoking, diabetes mellitus and hypertriglyceridemia had significant associations with the presence of CAD. Hyperuricemia, BMI, family history of CAD, high LDL-C level, low HDL-C level, hypercholesterolemia and hypertension were not associated with the occurrence of CAD. The factors that were related to the dependent variables mentioned in previous studies enter into the univariate analysis. Covariates with p < 0.05 in the univariate analysis were analyzed for collinearity. Afterwards, the variables selected finally were added to the full models. Abbreviations: HDL-C = high density lipoprotein cholesterol; LDL-C = low density lipoprotein cholesterol; BMI = body mass index; CAD = coronary artery disease
Multivariate logistic regression analysis of HUA on CAD
In addition, the association between HUA and the occurrence of CAD differed between groups. Multivariate logistic analysis showed that after adjusting for age, high LDL-C, low HDL-C, hypercholesterolemia, hypertriglyceridemia, metabolic syndrome, BMI, hypertension, diabetes mellitus, and a family history of CAD, HUA was significantly associated with the occurrence of CAD in the subgroup of non-smokers (OR, 1.84; 95% CI, 1.03–3.29), but the association did not exist in the current smokers sub-group (OR, 0.93; 95% CI, 0.64–1.35; Table 3). Figure 2 shows the logistic association between HUA and the presence of CAD in the non-smoker (p = 0.039) and current smoker groups (p = 0.69).

The association of hyperuricemia and the presence of CAD according to cigarrete smoking in Multi-variate logistic regression analysis. Abbreviations: CI = confidence interval; OR = odds ratio; CAD = coronary artery disease
Interaction effect of HUA and cigarrete smoking on the risk of CAD
We further found that the interaction between HUA and cigarrete smoking achieved statistical significance for the occurrence of CAD (p = 0.008; Additional file 1: Table S1).
Relationship between HUA and cigarrete smoking in the study population
Moreover, we found more subjects with HUA among the current smokers (p < 0.001), and the current smoker group had higher levels of plasma uric acid than the non-smoker group (p < 0.001), both in males (p = 0.009) and females (p = 0.019; Additional file 1: Table S2).
Discussion
HUA and CAD
In this observational study, we confirmed that HUA was significantly associated with incident CAD in non-smokers ≤ 35 years of age.
Previous studies have also reported a relationship between HUA and CAD [4, 10,11,12]. Some of the results confirmed a strong association between HUA and CAD; however, most of the results focused on the relationship between HUA and the risk of CAD in a middle-aged and elderly population [11, 13]. The reports did not focus on the relationship between HUA and CAD in young adults. A study involving a population with an average age of 40 ± 4 years suggested that SUA levels were independently related to coronary calcifications (indicators of sub-clinical coronary atherosclerosis). The recent study concerning on the relationship between HUA and CAD in patients ≤35 years of age (the 2015 CARDIA study) showed that after adjusting for demographic and lifestyle factors, the baseline SUA concentration was positively associated with the prevalence of CVD (HR, 1.21; 95% CI, 1.05–1.39; p = 0.005). This positive association was not significant in the full model due to the simultaneous effects of traditional risk factors (HR, 1.09; 95% CI, 0.94–1.27; p = 0.24) [14]. This conclusion was similar to our findings. Compared with the above studies, our study had access to a wide range of covariates and minimized the residual confounding, and still demonstrated a strong association.
Role of cigarette smoking
We stratified our patients into smokers versus non-smokers and found that the association between HUA and the presence of CAD existed in non-smokers only. In current smokers, we did not find a strong association between HUA and the presence of CAD, considering the stronger effect of cigarette smoking on young patients with CAD and the unbalanced gender ratio in the participants.
In addition, we identified more subjects with HUA among current smokers. The reasons for the increase in SUA levels in current smokers group may include the following: 1. Increasing SUA reabsorption. Studies have shown that smoking is positively correlated with the degree of insulin resistance, [15] and insulin resistance promotes sodium-hydrogen exchange in the renal proximal tubules [13]. With the increase in sodium-hydrogen exchange, anions, including uric acid, increase [16]. 2. Reducing the SUA excretion. Cigarettes contain a variety of harmful substances, including oxidants and free radicals that can result in a cytotoxic effect and lead to renal damage, thus eventually reducing the excretion of uric acid [17, 18]. A 2011 study of SUA and cigarette smoking among 300 volunteers 19.6–55.5 years of age showed a reduction in SUA levels in the smoking group [19]. These results were not consistent with our results, considering the differences in the age and the health status of the study participants, which need further study.
The current results can only explain the possible existence of the interaction between HUA and cigarette smoking on CAD, and the specific pathways need more in-depth research.
The clinical importance of this article is that for young adults, in addition to the main risk factors for premature CAD, such as cigarette smoking, non-traditional risk factors, such as HUA plays an important role in the occurrence of premature CAD. A young non-smoking population, from the perspective of coronary heart disease prevention, should pay more attention to the adverse effects of metabolic diseases, such as HUA and obesity, and improve eating habits to maintain a uric acid at normal levels.
Study limitations
There were several limitations to this study. First, the participants in the control group included some sub-health groups. If the participants in the control group were thoroughly healthy, the effect of HUA on CAD would be more prominent. Second, most of our participants were high-risk groups of cardiovascular disease. Thus, the positive rate of coronary angiography was high. These populations may not represent the general population. Third, the effect of anti-HUA drugs on the progression of CAD should be investigated further in large randomized trials, which may potentially provide new therapeutic approaches for the prevention and treatment of CAD.
Conclusions
In our study, HUA was shown to be significantly associated with the presence of CAD in non-smokers ≤ 35 years of age.
Abbreviations
- BMI:
-
Body mass index
- CAD:
-
Coronary artery disease
- CI:
-
Confidence interval
- HDL-C:
-
High density lipoprotein cholesterol
- LDL-C:
-
Low density lipoprotein cholesterol
- MS:
-
Metabolic syndrome
- NCEP ATP III:
-
The Adult Treatment Panel III (ATP III) of the National Cholesterol Education Program
- OR:
-
Odds ratio
- SUA:
-
Serum uric acid
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
References
Maroszynska-Dmoch EM, Wozakowska-Kaplon B. Clinical and angiographic characteristics of coronary artery disease in young adults: a single Centre study. Kardiol Pol. 2016;74(4):314–21.
Bhardwaj R, Kandoria A, Sharma R. Myocardial infarction in young adults-risk factors and pattern of coronary artery involvement. Niger Med J. 2014;55(1):44.
Alkhawam H, Zaiem F, Sogomonian R, et al. Coronary artery disease in young adults. Am J Med Sci. 2015;350(6):479–83.
Braga F, Pasqualetti S, Ferraro S, et al. Hyperuricemia as risk factor for coronary heart disease incidence and mortality in the general population: a systematic review and meta-analysis. Clin Chem Lab Med. 2016;54(1):7–15.
Wu AH, Gladden JD, Ahmed M, et al. Relation of serum uric acid to cardiovascular disease. Int J Cardiol. 2016;213:4–7.
Guo L-x. Interpretation of the Chinese expert consensus: recommendations for diagnosis and treatment of asymptomatic hyperuricemia complicated with cardiovascular diseases. J Transl Intern Med. 2014;2(2):93.
Liu LS. 2010 Chinese guidelines for the management of hypertension. Zhonghua Xin Xue Guan Bing Za Zhi. 2011;39(2):579–615.
Joint Commission on Revisions of Chinese Guideline for the Management of Dyslipidemia in Adults. [2016 Chinese guideline for the management of dyslipidemia in adults][J]. Zhonghua Xin Xue Guan Bing Za Zhi. 2016;44(10):833–853. https://doi.org/10.11909/j.issn.1671-5411.2018.01.011.
Liu J, Zuo SW, Li Y, et al. Hyperhomocysteinaemia is an independent risk factor of abdominal aortic aneurysm in a Chinese Han population. Scientific reports. 2016;6:17966.
Zuo T, Liu X, Jiang L, et al. Hyperuricemia and coronary heart disease mortality: a meta-analysis of prospective cohort studies. BMC Cardiovasc Disord. 2016;16(1):207.
Yang Y, Tian J, Zeng C, et al. Relationship between hyperuricemia and risk of coronary heart disease in a middle-aged and elderly Chinese population. J Int Med Res. 2017;45(1):254–60.
Chuang SY, Chen JH, Yeh WT, et al. Hyperuricemia and increased risk of ischemic heart disease in a large Chinese cohort. Int J Cardiol. 2012;154(3):316–21.
Qin L, Yang Z, Gu H, et al. Association between serum uric acid levels and cardiovascular disease in middle-aged and elderly Chinese individuals. BMC Cardiovasc Disord. 2014;14(1):26.
Wang H, Jacobs DR Jr, Gaffo AL, et al. Serum urate and incident cardiovascular disease: the coronary artery risk development in young adults (CARDIA) study. PLoS One. 2015;10(9):e0138067.
Neeland IJ, Patel RS, Eshtehardi P, et al. Coronary angiographic scoring systems: an evaluation of their equivalence and validity. Am Heart J. 2012;164(4):547–552.e541.
Mahnensmith RL, Aronson PS. The plasma membrane sodium-hydrogen exchanger and its role in physiological and pathophysiological processes. Circ Res. 1985;56(6):773–88.
Sinning C, Lillpopp L, Appelbaum S, et al. Angiographic score assessment improves cardiovascular risk prediction: the clinical value of SYNTAX and Gensini application. Clin Res Cardiol. 2013;102(7):495–503.
Duran M, Kalay N, Akpek M, et al. High levels of serum uric acid predict severity of coronary artery disease in patients with acute coronary syndrome. Angiology. 2012;63(6):448.
Haj Mouhamed D, Ezzaher A, Neffati F, et al. Effect of cigarette smoking on plasma uric acid concentrations. Environ Health Prev Med. 2011;16(5):307–12.
Acknowledgements
We hereby thank and acknowledge the assistance of Changzhong Chen and Xinglin Chen in the statistical analysis and precious advice of this work.
Availability of data and materials section
The data of this study will not be shared publically because they will be applied for further researches of this series. But authors do agree that the data can be shared individually if requested.
Funding
This work was supported by the Beijing Municipal Administration of Hospitals Clinical Medicine Development of Special Funding Support (code: ZYLX2903) and the National Key Clinical Specialty Construction Project (29–213) for study design, the “Beijing Municipal Administration of Hospitals” Ascent Plan (Code: DFL2170601) for data collection and analysis.
Author information
Authors and Affiliations
Contributions
All authors take responsibility for the integrity of the data, the accuracy of the data analysis and the revise of the manuscript. SL, WL and YL participated in the study design. XL and WL participated in the acquisition of data. SL drafted the manuscript. DS, YZ and YZ conceived of the study, participated in its design and coordination, revised the paper and obtained funding. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interest
The authors declare that they have no competing interests.
Ethics approval and consent to participate
The present study was approved by the Institutional Ethics Committee of Anzhen Hospital. Written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Table S1. Interaction effect of hyperuricemia and cigarrete smoking on CAD. Table S2. Relationship between hyperuricemia/uric acid and smoking in the special group. Figure S1. Flowchart of the study. (DOCX 546 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Lv, S., Liu, W., Zhou, Y. et al. Hyperuricemia and smoking in young adults suspected of coronary artery disease ≤ 35 years of age: a hospital-based observational study. BMC Cardiovasc Disord 18, 178 (2018). https://doi.org/10.1186/s12872-018-0910-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-018-0910-5