
Abstract
Background
Prolonged length of stay in post-anesthesia care unit (PLOS in PACU) is a combination of risk factors and complications that can compromise quality of care and operating room efficiency. Our study aimed to develop a nomogram to predict PLOS in PACU of patients undergoing elective surgery.
Methods
Data from 24017 patients were collected. Least absolute shrinkage and selection operator (LASSO) was used to screen variables. A logistic regression model was built on variables determined by a combined method of forward selection and backward elimination. Nomogram was designed with the model. The nomogram performance was evaluated with the area under the receiver operating characteristic curve (AUC) for discrimination, calibration plot for consistency between predictions and actuality, and decision curve analysis (DCA) for clinical application value.
Results
A nomogram was established based on the selected ten variables, including age, BMI < 21 kg/m2, American society of Anesthesiologists Physical Status (ASA), surgery type, chill, delirium, pain, naloxone, operation duration and blood transfusion. The C-index value was 0.773 [95% confidence interval (CI) = 0.765 - 0.781] in the development set and 0.757 (95% CI = 0.744-0.770) in the validation set. The AUC was > 0.75 for the prediction of PLOS in PACU. The calibration curves revealed high consistencies between the predicted and actual probability. The DCA showed that if the threshold probability is over 10% , using the models to predict PLOS in PACU and implement intervention adds more benefit.
Conclusions
This study presented a nomogram to facilitate individualized prediction of PLOS in PACU for patients undergoing elective surgery.
Similar content being viewed by others

Introduction
A post-anesthesia care unit (PACU) is a vital part of hospital surgical suites and ambulatory care centers. The responsibility of medical staff in PACU is to transfer patients who have undergone anesthesia to the ward after satisfactory recovery [1, 2]. Prolonged length of stay in PACU (PLOS in PACU) is a combination of multiple risk factors and complications. By targeting PLOS, identifying these risk factors and complications can improve patient safety and quality of anesthesia which is beneficial to implement the protocols of enhanced recovery after surgery (ERAS) [3]. In addition, shortening the length of stay in PACU can reduce the waiting time of patients in the operating room, the turnover efficiency of which could be improved. Therefore, it is necessary to find relevant risk factors and establish a nomogram to predict the probability of PLOS in PACU. Combined with the nomogram, individualized prevention and intervention can be implemented based on risk factors.
Several clinical predictive models for different populations have been reported. Rodney A Gabriel et al. analyzed data from 4151 outpatients and identified risk factors for PLOS in PACU, including morbid obesity, hypertension, surgical specialty, primary anesthesia type, and scheduled case duration [4]. Similarly, Eric M Jaryszak et al. analyzed risk factors in 190 tonsillectomy patients [5]. Cao et al. included 913 patients and established a model for PLOS in PACU after cholecystectomy [6]. In addition, some investigations were performed on pediatric patients [7, 8]. However, the population of these studies was limited to outpatients or patients with a certain type of surgery, and the sample size was small. Most studies only analyzed relevant risk factors for PLOS in PACU without establishing and validating a nomogram for predicting the outcome. Cao et al. established a nomogram for PLOS in PACU on patients undergoing cholecystectomy [6]. However, there are many different types of surgery, and it is clear that a nomogram on a specific type of surgery is not suitable for widespread clinical use. In addition, most of the predictive variables screened in these studies were patient general characteristics and underlying diseases. Even with high predictive power, it is difficult for clinicians to prevent and intervene these risk factors.
In the current study, a nomogram was constructed to predict the PLOS in PACU by collecting clinical data on general characteristics, perioperative complications, surgery, and anesthesia from 24017 patients covering various types of surgery. We aim to provide anesthesiologists and nurses in PACU with a convenient predictive tool for the individualized prevention and intervention of associated risk factors.
Materials and methods
Study population
The research was in accordance with the Ethical Principles for Medical Research Involving Human Subjects, outlined in the Helsinki Declaration of 1975 (revised 2013). This study was conducted at The First Affiliated Hospital, Zhejiang University School of Medicine, a tertiary hospital. The protocol was approved by the clinical research ethic committee of the hospital(IIT20230068A). Informed consent was waived by the institutional review board due to the retrospective nature of this study. The trial was registered prior to patient enrollment in the Chinese Clinical Trial Registry (ChiCTR2300069897, Principal investigator: Fuquan Fang, https://www.chictr.org.cn/showproj.html?proj=192900, Date: 29/03/2023). This manuscript adheres to the applicable STROBE guidelines.
There are 38 elective operating rooms and 22 recovery beds in our hospital. The medical staff at PACU consists of 2 attending physicians and 10 nurses. Confusion Assessment Method is a widely used delirium assessment tool [9] and we adopt the method. The diagnosis mainly depends on four characteristics: ① acute onset of mental status changes or a fluctuating course, ② inattention, ③ disordered thinking, and ④ altered level of consciousness. Delirium can be diagnosed by meeting both ① and ②, and by having either ③ or ④. The Critical-Care Pain Observation Tool (CPOT) [10] was used for postoperative pain assessment. CPOT consists of four behavioral items : ① facial expression, ② body movements, ③ compliance with the ventilator (intubated patients) or vocalization (non-intubated patients), and ④ muscle tension. Each behavior item is scored on a scale of 0 to 2. The total score ≥ 4 was defined as pain. Bedside Shivering Assessment Scale is a four-point scale, such as absent, mild, moderate, or severe [11]. A diagnosis of chills can be made if the symptoms are mild, such as trembling of the muscles in the neck or chest. Aldrete Recovery Score ≥ 8 is considered to discharge from PACU [12]. Scores are made up of five components: activity, awareness, breathing, oxygen saturation and circulation. Each category is scored between 0 and 2. The higher the score, the better the result. RS is the arithmetic sum of the five categories. These data are stored electronically after the nurses' routine monitoring records.
Data were collected from 24017 patients undergoing elective surgery between June 2019 and February 2021. The data set only included patients over 18 years of age who were admitted to PACU for resuscitation after elective surgery with tracheal intubation anesthesia. Patients were randomly divided (7: 3) into development (16753) and validation (7264) sets. Exclusion criteria were patients with emergency surgery, brain surgery, heart surgery, mental disease, missing data. Demographic data and clinical characteristics including sex, age, Body Mass Index (BMI), hypertension, diabetes, American Society of Anesthesiologists physical status classification (ASA), type of surgery, operation duration, temperature at admission to PACU, chill, delirium, pain, naloxone, neostigmine, transfusions of red blood cells, plasma, platelets, whole blood, and autologous blood were collected through the electronic medical record system. Continuous variables were converted into categorical variables such as age, BMI, temperature, and operation duration. To determine the diagnostic reliability of age and operation duration, summary statistics were calculated including sensitivity, specificity, positive predictive value, negative predictive value, Cohen’s Kappa coefficient and the area under the receiver operating characteristic (ROC) curve. On this basis, the cut-off values of age and operative duration were calculated to be 55 and 110, respectively. BMI and temperature were transformed into multinomial variables. Therefore, the first and third quartiles were chosen as the classification basis, which were 21 kg/m2, 25 kg/m2 and 36.2℃, 37.2℃, respectively. The type of surgery was divided into minor surgery, moderate surgery, and major surgery. Minor surgeries include skin surface masses, varicose veins, thyroid nodules, breast nodules, skin debridement and endoscopic procedures such as hysteroscopy, ureteroscopy, etc. Moderate surgeries include gallstones, hepatorenal cysts, thyroid cancer, breast cancer, lung wedge resection, joint replacement, etc. Major surgeries include liver cancer, gallbladder cancer, stomach cancer, intestinal cancer, pancreatic cancer, kidney cancer, lobectomy, segmental resection, spinal surgery, etc. PLOS was defined as greater than or equal to the third quartile of length of stay (≥ 80 min).
Statistical analysis
All statistical analyses were performed using R software (version 4.2.0). Categorical variables were described as percentages (%). whereas continuous variables were reported as medians and interquartile ranges (IQRs). The least absolute shrinkage and selection operator (LASSO) regression model was used to screen for statistically significant variables with the R package “glmnet”. These variables were then put into multivariate regression analysis with a combination method of forward selection and backward elimination based on the Akaike Information Criterion. Variables, satisfying a significance level of P < 0.05 were used to build predictive model. Student's t test was used to compare the area under the receiver operating characteristic curve (AUC) of model 10 and model 11.
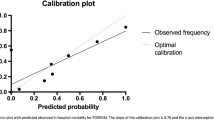
The performance of the nomogram was evaluated for both the development and validation sets using calibration and discrimination [13]. Calibration curves were used to assess the calibration ability of this predictive nomogram, while the Harrell's concordance index (C-index) and the area under the receiver operating characteristic (ROC) curve (AUC) were both used to evaluate the discrimination ability [14]. Furthermore, decision curve analysis (DCA) was utilized to evaluate the clinical applicability [15]. Statistical significance was set at 2-sided p < 0.05.
Results
Characteristics of patients
The data collection process was illustrated in Fig. 1. Data from the remaining 24017 cases were used for subsequent analysis. In the whole population, development, and validation sets, the median length of stay were 54 (IQR: 36-80), 54 (IQR: 36-80), and 54 (IQR: 36-80) minutes, respectively. PLOS was defined as length of stay greater than the third quartile interval. The demographic and clinical characteristics of the patients in both sets were listed in Table 1. The clinical characteristics of the total population in each variable for both the PLOS and non-PLOS groups were listed in Table 2.

The flowchart of our study. PACU, postoperative anesthesia care unit
Nomogram variable screening
A total of 19 variables were entered into LASSO regression analysis after setting dummy variables for unordered categorical variables such as BMI and temperature. The LASSO result was determined with development set. The lambda. min was 0.0003744695 and 17 variables are selected, while lambda. 1se = 0.01409854, and 11 variables were selected (Fig. 2). In the current study, the lambda.1se criteria was used for predictors selection [16], and the 11 predictors included age, BMI < 21 kg/m2, ASA, surgery type, chill, delirium, pain, naloxone, PLOD, blood transfusion and temperature < 36.2℃. After multiple logistic regression analysis, the above factors were still statistically significant (Table 3). However, the model with 11 variables (model 11) includes hypothermia and chills. To make the nomogram simple and convenient for clinical use, we kicked out hypothermia with relatively small regression coefficient and set up a model with 10 variables (model 10). The AUC of the two models were compared and no significant difference in predictive power between the simplified model 10 and model 11 was found (p = 0.12). In addition, chills are defined: during recovery from anesthesia, the brain's central response to cold is reduced, and the spinal cord's central response is restored to normal, resulting in rigidity or parochial muscle tremors as a result of an involuntary nervous reflex. In this study, when chills were recorded by nurse in PACU, patients were required to present rigidity or parochial muscle tremors. The record of chills was relatively objective.

LASSO regression analysis for factors selection. A selection of the tuning parameter (λ) by using 10-fold via minimum and 1-SE criteria. B Non-zero coefficients selection by using the 10-fold cross-validation. LASSO, least absolute shrinkage, and selection operator
Nomogram construction and validation
A static nomogram for PLOS in PACU was constructed according to the model 10 (Fig. 3). This is an example of using the nomogram to predict the PLOS probability of a patient from data set. The total score was calculated from each item, and the predicted probability is derived accordingly. Further, a dynamic nomogram based on the model 10 was developed and freely available online to make it easier for medical staff to calculate the risk of PLOS in PACU (https://ffq11051.shinyapps.io/DynNomapp/). The regression equations constructed on Model 10 can be seen in the summary model panel of the dynamic nomogram. The C-index value of the development set was 0.773 (95% CI = 0.765-0.781), and the verification set was 0.757 (95% CI = 0.744-0.770). In both sets, the AUC was > 0.75 (Fig. 4A, B), indicating that nomogram has valuable ability to discriminate. Calibration curves of the nomogram demonstrated a high agreement between predicted and actual probabilities in both the development and validation sets (Fig. 4C, D). To sum up, the nomogram for PLOS in PACU had considerable discriminative and calibrating abilities.

A static nomogram showing a patient's scoring process. To use the nomogram, the specific points (black dots) of individual patients are located on each variable axis. A patient's characteristics are identified by a red dot. Red dots are drawn upward to determine the score received by each variable; the sum (3.38) of these score is located on the Total score axis, and a line is drawn downward to the PLOS axes to determine the probability (41.3%) of PLOS in PACU. ASA, American society of Anesthesiologists Physical Status; BMI, body mass index; PLOD, Prolonged length of operation duration; PLOS, prolonged length of stay

AUC and calibration curves of the models. A, B AUC of the model10 and model11 to predict probability of PLOS in PACU in the development and validation sets. The black line (model11) represents AUC = 0.776. which is considered ideal. The red line (model10, based on which the nomogram was established) represents AUC = 0.773. AUC (model10) vs AUC (model11), p > 0.05. C, D Calibration curves of the nomogram for PLOS in the development and validation sets. The black dots calculated with nomogram are evenly distributed around the grey bold lines, showing perfect consistency. AUC, area under the receiver operating characteristic curve; DEV, development; ROC, receiver operating characteristic curve; PLOS, prolonged length of stay; VAD, validation
Clinical utility
The DCA for the models was presented, which showed the comparability of model 10 and model 11 in clinical use (Fig. 5). Additionally, the DCA showed that when the threshold probability was greater than 10%, using the models to predict PLOS in PACU and implement intervention adds more benefit than either the treat-all-patients scheme or the treat-none scheme. These results further confirmed that the nomogram established based on Model 10 has a favorable performance.

DCA of the nomogram. A PLOS benefit in the development set. B PLOS benefit in the validation set. The blue line represents model10 (based on which the nomogram was established. The red line represents model11. The results of the prediction models are the blue and red lines. The two other lines are “intervention for all” (grey line) and “intervention for none” (black line). DCA, decision curve analysis; DEV, development; PLOS, prolonged length of stay; VAD, validation
Discussion
A nomogram for predicting PLOS in PACU for patients undergoing elective surgery was developed and validated with excellent discrimination and calibration in the current study. Combined with the nomogram, individualized prevention and intervention based on the risk factors can be achieved, thereby improving operating room turnover, and implementing protocols of ERAS.
Patients with endotracheal tube into PACU were included in this study for the purpose of consistency in the start time of anesthesia recovery. Some patients may be delayed entering the PACU after extubation in the operating room due to a shortage of beds. However, these patients need only a short stay to meet the PACU discharge, which makes the stay time in PACU not an accurate reflection of recovery quality. Therefore, in order to analyze the recovery more accurately, patients with endotracheal tube were included in this study. There is no definition of "PLOS". Some studies defined it as length of stay > 2 hours [4] or > 60 minutes [17]. Rodney A Gabriel et al defined it as greater than the third quartile range [4]. Subsequent similar studies have also adopted this definition [6]. For consistency, this approach was employed in this study. Based on clinical experience or related research reports, the following risk factors statistically analyzed in this study may not be surprising, but these factors were quantified in this study to predict PLOS in PACU and were used to establish a nomogram.
Age and BMI were analyzed as risk factors. Rodney A et al. found that age ≥ 65 was not a risk factor for PLOS in PACU [4]. However, Cao et al found the opposite result in the gallbladder surgery population [6]. The reason for choosing 65 as the cutoff point was not explained in their study. In order to make the diagnosis more accurate, we determined the diagnostic reliability of an age cutoff point of 55 by calculating statistical data including sensitivity, specificity, positive predictive value, negative predictive value, Cohen’s Kappa coefficient and AUC. Age ≥ 55 was a risk factor in the study. Most studies only used dichotomies for BMI [4, 6, 18]. Therefore, low body weight had been ignored. So, we distributed body weight in quartiles, using 25% and 75% as cut-off points. This study showed that low body weight (< 21 kg/m2 ) was a statistically significant risk factor. Some studies had reported that BMI ≥ 40 kg/m2 was a risk factor for delayed postoperative recovery, mainly because morbid obesity increase the risk of sleep apnea especially in the setting of opioid utilization [4, 19]. The reason why our study did not reach a consistent conclusion may be due to the characteristics of the patient population included in this study. In this study, the number of patients with BMI ≥ 40 kg/m2 was 13, accounting for 0.05%, which may be caused by regional dietary and living habits. One of the five diagnostic criteria for frailty syndrome is weight loss. These patients have a poor tolerance to anesthesia and surgery, therefore requiring longer recovery time after surgery [20]. In addition, Cao et al. had reported that the lower the BMI, the longer the postoperative length of stay in PACU [6].
It is not surprising that ASA, major surgeries, and operation duration are risk factors for PLOS in PACU. Major surgeries have been thought to cause inflammatory induced postoperative cognitive decline [21], which is associated with poorer postoperative recovery, increased medical costs and higher mortality [22, 23]. Postoperative delirium increased PLOS in PACU occurrence in the study, which consisted with above. Preoperative fluid fasting for more than 6 hours was reported as an independent risk factor for delirium [24]. Incidence of cognitive decline in elderly patients under general anesthesia at bispectral index 55-65 was higher than at 40-50 [25]. Chernov and his colleagues conducted neuropsychological tests pre-operation and post-operation, which determined the association between regional cerebral blood flow reduction and poor cognitive performance [26]. For major surgery, regional nerve block combined with general anesthesia could effectively prevent cognitive decline [21], which decreased incidence of PLOS in PACU. Whether the risk of delirium differs between general anesthesia with inhalants and total intravenous anesthesia remains controversial [27]. Perioperative use of dexmedetomidine, paracetamol and Nonsteroidal Anti-inflammatory Drugs (NSAIDs) has been suggested to prevent postoperative delirium by directly alleviating neuroinflammation [28, 29]. The most relevant medications with the onset of delirium are benzodiazepines, gabapentin, and scopolamine [29]. Hypothermia is also associated with complications such as PLOS in PACU, delirium, pain, and chills [30]. Strengthening intraoperative temperature management is beneficial to improve postoperative recovery.
This study showed that pain and naloxone use were risk factors of PLOS in PACU. Anesthesiologists use different opioids depending on surgery and individual patient. By converting different opioids into morphine and then standardizing them according to the patient's weight and length of operation, this would make nomogram complicated and impractical. So, this study collected data on the use of naloxone, indirectly reflecting opioid overdose. Since both insufficient analgesia and opioid overdoses can lead to PLOS in PACU, it is necessary to explore better methods of monitoring analgesia. In recent years, various monitors have been invented for quantifying pain, such as analgesia nociception index, skin conductance, pupillometry, nociceptive flexion reflex threshold, surgical pleth index and qNOX [31]. The nociception level index, a multi-parameter artificial intelligence-driven index, can objectively guide opioid administration, potentially leading to more appropriate analgesic regimen [32]. Additionally, incorporating a multimodal analgesia approach and reducing opioid use are considered key strategy [33]. Some studies have shown that dexmedetomidine is more effective than other agents in perioperative analgesia [34,35,36]. However, Bhiken I Naik et al. found no such positive effect after multistage deformation-correcting spinal surgery [37]. In addition, intraoperative intravenous lidocaine (1.5 mg/kg induction followed by 2 mg/kg/h) can reduce postoperative pain and promote recovery [38]. Meta-analysis shows that NSAIDs is beneficial, such as lornoxicam, pregabalin, ibuprofen, gabapentin, and acetaminophen [39]. In a network meta-analysis of 52 trials involving 2112 subjects, the pre-emptive analgesic effect of gabapentin was evaluated as significantly reducing postoperative pain scores, opioid consumption, and the incidence of PLOS in PACU [40]. In addition to adjuvant analgesics, combined nerve block and intrathecal anesthesia are also effective [41].
This study found that intraoperative transfusion of blood products prolonged postoperative recovery. Disruption of physiological homeostasis is the main reason. In addition, transfusion of blood products had been reported to cause postoperative residual neuromuscular blockade and affect neuromuscular functional recovery in the PACU [42]. It remains unclear whether blood transfusion also affects the pharmacokinetics and pharmacodynamics of other anesthetics. Regarding blood transfusion, the "yes" and "no" were used as cut-points in the study. If a cut-point "> x units" was used as a predictor, this may improve the nomogram's predictive power. However, the variety of blood component types and quantities were collected in this study. Treating each blood component as an independent variable and counting their respective quantities would make the resulting nomogram complex and inconvenient for clinical use, especially in the environment of busy clinical anaesthetic work. In addition, this study found that neostigmine use was not a risk factor for PLOS in PACU, possibly because neostigmine does not accurately reflect neuromuscular blocker overdoses. The amount and type of neuromuscular blocker were not collected in this study, mainly to consider that if it is a risk factor, it should be standardized according to drug type, operation duration and patient weight before conducting nomogram score, which will make the nomogram complex and less useful.
The study has several limitations. First, some variables that may contribute to improving the predictive ability of the model were not included, such as cerebral apoplexy etc. Second, we did not collect detailed usage and types of opioids and neuromuscular blockers. Third, the nomogram was not verified externally. In future clinical work, we will further verify the feasibility of the model.
In summary, we have developed a predictive model with excellent differentiation and clinical utility that can help identify patients with a higher probability of PLOS in PACU. The screening of high risk factors and the establishment of nomogram are helpful to improve the quality of ERAS and the efficiency of the operating room.
Availability of data and materials
The data and materials in the present study can be available from the corresponding author on reasonable request. The emails of corresponding author: huzhiyong777@zju.edu.cn.
Abbreviations
- PLOS in PACU:
-
Prolonged length of stay in post-anesthesia care unit
- LASSO:
-
Least absolute shrinkage and selection operator
- AUC:
-
Area under the receiver operating characteristic curve
- DCA:
-
Decision curve analysis
- ASA:
-
American Society of Anesthesiologists Physical Status
- CI:
-
Confidence interval
- ERAS:
-
Enhanced recovery after surgery
- CPOT:
-
Critical-care pain observation tool
- BMI:
-
Body Mass Index
- IQRs:
-
Interquartile ranges
- C-index:
-
Concordance index
- NSAIDs:
-
Nonsteroidal anti-inflammatory drugs
- DEV:
-
Development
- VAD:
-
Validation
References
Ma H, Wachtendorf LJ, Santer P, et al. The effect of intraoperative dexmedetomidine administration on length of stay in the post-anesthesia care unit in ambulatory surgery: A hospital registry study. J Clin Anesth. 2021;72:110284. https://doi.org/10.1016/j.jclinane.2021.110284.
Fairley M, Scheinker D, Brandeau ML. Improving the efficiency of the operating room environment with an optimization and machine learning model. Health Care Manag Sci. 2019;22(4):756–67. https://doi.org/10.1007/s10729-018-9457-3.
Ehrenfeld JM, Dexter F, Rothman BS, et al. Lack of utility of a decision support system to mitigate delays in admission from the operating room to the postanesthesia care unit. Anesth Analg. 2013;117(6):1444–52. https://doi.org/10.1213/ANE.0b013e3182a8b0bd.
Gabriel RA, Waterman RS, Kim J, Ohno-Machado L. A Predictive Model for Extended Postanesthesia Care Unit Length of Stay in Outpatient Surgeries. Anesth Analg. 2017;124(5):1529–36. https://doi.org/10.1213/ANE.0000000000001827.
Jaryszak EM, Lander L, Patel AK, Choi SS, Shah RK. Prolonged recovery after out-patient pediatric adenotonsillectomy. Int J Pediatr Otorhinolaryngol. 2011;75(4):585–8. https://doi.org/10.1016/j.ijporl.2011.01.024.
Cao B, Li L, Su X, Zeng J, Guo W. Development and validation of a nomogram for determining patients requiring prolonged postanesthesia care unit length of stay after laparoscopic cholecystectomy. Ann Palliat Med. 2021;10(5):5128–36. https://doi.org/10.21037/apm-20-2182.
Anandan D, Zhao S, Whigham AS. Factors Affecting Post-Anesthesia Care Unit Length of Stay in Pediatric Patients after an Adenotonsillectomy. Ann Otol Rhinol Laryngol. 2020;129(11):1071–7. https://doi.org/10.1177/0003489420931557.
Walia H, Balaban O, Jacklen M, Tumin D, Raman V, Tobias JD. Pilot study comparing post-anesthesia care unit length of stay in moderately and severely obese children. J Anesth. 2017;31(4):510–6. https://doi.org/10.1007/s00540-017-2326-2.
Shenkin SD, Fox C, Godfrey M, et al. Delirium detection in older acute medical inpatients: a multicentre prospective comparative diagnostic test accuracy study of the 4AT and the confusion assessment method. BMC Med. 2019;17(1):138. https://doi.org/10.1186/s12916-019-1367-9.
Chen J, Hu F, Yang J, et al. Validation of a Chinese version critical-care pain observation tool in nonintubated and intubated critically ill patients: Two cross-sectional studies. J Clin Nurs. 2019;28(15–16):2824–32. https://doi.org/10.1111/jocn.14862.
Arnold JT, Hemsley Z, Hodder SG, Havenith G, Lloyd AB. Reliability and validity of methods in the assessment of cold-induced shivering thermogenesis. Eur J Appl Physiol. 2020;120(3):591–601. https://doi.org/10.1007/s00421-019-04288-2.
Shapses M, Tang L, Layne A, Beri A, Rotman Y. Fatty Liver Is an Independent Risk Factor for Delayed Recovery from Anesthesia. Hepatol Commun. 2021;5(11):1848–59. https://doi.org/10.1002/hep4.1772.
Balachandran VP, Gonen M, Smith JJ, DeMatteo RP. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015;16(4):e173-80. https://doi.org/10.1016/S1470-2045(14)71116-7.
Pencina MJ, D’Agostino RB. Overall C as a measure of discrimination in survival analysis: model specific population value and confidence interval estimation. Stat Med. 2004;23(13):2109–23. https://doi.org/10.1002/sim.1802.
Zhang Z, Rousson V, Lee WC, et al. Decision curve analysis: a technical note. Ann Transl Med. 2018;6(15):308. https://doi.org/10.21037/atm.2018.07.02.
Xuan Z, Yu Z, Tan G, et al. Development and validation of a novel nomogram for predicting systemic inflammatory response syndrome’s occurrence in patients undertaking flexible ureteroscopy. Transl Androl Urol. 2022;11(2):228–37. https://doi.org/10.21037/tau-22-34.
Brown I, Jellish WS, Kleinman B, et al. Use of postanesthesia discharge criteria to reduce discharge delays for inpatients in the postanesthesia care unit. J Clin Anesth. 2008;20(3):175–9. https://doi.org/10.1016/j.jclinane.2007.09.014.
Elsharydah A, Walters DR, Somasundaram A, et al. A preoperative predictive model for prolonged post-anaesthesia care unit stay after outpatient surgeries. J Perioper Pract. 2020;30(4):91–6. https://doi.org/10.1177/1750458919850377.
Mulier JP. Perioperative opioids aggravate obstructive breathing in sleep apnea syndrome: mechanisms and alternative anesthesia strategies. Curr Opin Anaesthesiol. 2016;29(1):129–33. https://doi.org/10.1097/ACO.0000000000000281.
Jin Z, Rismany J, Gidicsin C, Bergese SD. Frailty: the perioperative and anesthesia challenges of an emerging pandemic. J Anesth. 2023;37(4):624–40. https://doi.org/10.1007/s00540-023-03206-3.
Singh NP, Makkar JK, Borle A, Singh PM. Role of supplemental regional blocks on postoperative neurocognitive dysfunction after major non-cardiac surgeries: a systematic review and meta-analysis of randomized controlled trials. Reg Anesth Pain Med. 2022;https://doi.org/10.1136/rapm-2022-104095.
Liu Q, Sun YM, Huang H, et al. Sirtuin 3 protects against anesthesia/surgery-induced cognitive decline in aged mice by suppressing hippocampal neuroinflammation. J Neuroinflammation. 2021;18(1):41. https://doi.org/10.1186/s12974-021-02089-z.
Chan MT, Cheng BC, Lee TM, Gin T, Group CT. BIS-guided anesthesia decreases postoperative delirium and cognitive decline. J Neurosurg Anesthesiol. 2013;25(1):33–42. https://doi.org/10.1097/ANA.0b013e3182712fba.
Radtke FM, Franck M, MacGuill M, et al. Duration of fluid fasting and choice of analgesic are modifiable factors for early postoperative delirium. Eur J Anaesthesiol. 2010;27(5):411–6. https://doi.org/10.1097/EJA.0b013e3283335cee.
Hou R, Wang H, Chen L, Qiu Y, Li S. POCD in patients receiving total knee replacement under deep vs light anesthesia: A randomized controlled trial. Brain Behav. 2018;8(2):e00910. https://doi.org/10.1002/brb3.910.
Chernov VI, Efimova NY, Efimova IY, Akhmedov SD, Lishmanov YB. Short-term and long-term cognitive function and cerebral perfusion in off-pump and on-pump coronary artery bypass patients. Eur J Cardiothorac Surg. 2006;29(1):74–81. https://doi.org/10.1016/j.ejcts.2005.10.001.
Miller D, Lewis SR, Pritchard MW, et al. Intravenous versus inhalational maintenance of anaesthesia for postoperative cognitive outcomes in elderly people undergoing non-cardiac surgery. Cochrane Database Syst Rev. 2018;8(8):CD012317. https://doi.org/10.1002/14651858.CD012317.pub2.
Qin C, Jiang Y, Lin C, Li A, Liu J. Perioperative dexmedetomidine administration to prevent delirium in adults after non-cardiac surgery: A systematic review and meta-analysis. J Clin Anesth. 2021;73:110308. https://doi.org/10.1016/j.jclinane.2021.110308.
Jin Z, Hu J, Ma D. Postoperative delirium: perioperative assessment, risk reduction, and management. Br J Anaesth. 2020;125(4):492–504. https://doi.org/10.1016/j.bja.2020.06.063.
Khan ZH, Arab S, Emami B. Comparison of the effects of anesthesia with isoflurane and total intravenous anesthesia on the intensity of body temperature reduction during anesthesia and incidence of postoperative chills. Acta Med Iran. 2011;49(7):425–32.
Ledowski T. Objective monitoring of nociception: a review of current commercial solutions. Br J Anaesth. 2019;123(2):e312–21. https://doi.org/10.1016/j.bja.2019.03.024.
Meijer F, Honing M, Roor T, et al. Reduced postoperative pain using Nociception Level-guided fentanyl dosing during sevoflurane anaesthesia: a randomised controlled trial. Br J Anaesth. 2020;125(6):1070–8. https://doi.org/10.1016/j.bja.2020.07.057.
Helander EM, Billeaud CB, Kline RJ, et al. Multimodal Approaches to Analgesia in Enhanced Recovery After Surgery Pathways. Int Anesthesiol Clin Fall. 2017;55(4):51–69. https://doi.org/10.1097/AIA.0000000000000165.
Rajan S, Hutcherson MT, Sessler DI, et al. The Effects of Dexmedetomidine and Remifentanil on Hemodynamic Stability and Analgesic Requirement After Craniotomy: A Randomized Controlled Trial. J Neurosurg Anesthesiol. 2016;28(4):282–90. https://doi.org/10.1097/ANA.0000000000000221.
Hwang W, Lee J, Park J, Joo J. Dexmedetomidine versus remifentanil in postoperative pain control after spinal surgery: a randomized controlled study. BMC Anesthesiol. 2015;15:21. https://doi.org/10.1186/s12871-015-0004-1.
Abdallah FW, Brull R. Facilitatory effects of perineural dexmedetomidine on neuraxial and peripheral nerve block: a systematic review and meta-analysis. Br J Anaesth. 2013;110(6):915–25. https://doi.org/10.1093/bja/aet066.
Naik BI, Nemergut EC, Kazemi A, et al. The Effect of Dexmedetomidine on Postoperative Opioid Consumption and Pain After Major Spine Surgery. Anesth Analg. 2016;122(5):1646–53. https://doi.org/10.1213/ANE.0000000000001226.
Peng Y, Zhang W, Kass IS, Han R. Lidocaine Reduces Acute Postoperative Pain After Supratentorial Tumor Surgery in the PACU: A Secondary Finding From a Randomized Controlled Trial. J Neurosurg Anesthesiol. 2016;28(4):309–15. https://doi.org/10.1097/ANA.0000000000000230.
Michelet D, Andreu-Gallien J, Bensalah T, et al. A meta-analysis of the use of nonsteroidal antiinflammatory drugs for pediatric postoperative pain. Anesth Analg. 2012;114(2):393–406. https://doi.org/10.1213/ANE.0b013e31823d0b45.
Xuan C, Yan W, Wang D, et al. Efficacy of preemptive analgesia treatments for the management of postoperative pain: a network meta-analysis. Br J Anaesth. 2022;129(6):946–58. https://doi.org/10.1016/j.bja.2022.08.038.
Anger M, Valovska T, Beloeil H, et al. PROSPECT guideline for total hip arthroplasty: a systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2021;76(8):1082–97. https://doi.org/10.1111/anae.15498.
Wang G, Wang J, Zhou H, Zhao X, Wu X. Impairment of recovery of muscle function by residual rocuronium after re-transfusion of intraoperative salvaged blood. Chin Med J (Engl). 2014;127(5):821–4.
Acknowledgments
The authors thank Patrick M. McQuillan MD., Department of Anesthesiology, Penn State Hershey Medical Centre, Penn State College of Medicine, Hershey, PA, USA, for his critical comments during manuscript preparation.
Funding
This work was supported by the National Natural Science Foundation of China (No. 82171260; No. 81641042; No. 81471240) and the Natural Science Foundation of Zhejiang Province (No. LZ22H090002; No. 2014C33170).
Author information
Authors and Affiliations
Contributions
Fuquan Fang and Tiantian Liu conducted a literature review, participated in the study design, data collection, and wrote the first draft of the paper. Jun Li and Yanchang Yan assisted in statistical analysis and manuscript editing. Wenxin Hang assisted with ethical applications and clinical trial registration. Dandan and Sujuan Ye helped with statistical analysis and made significant contributions to manuscript revision. Pin Wu and Yuhan Hu prepared figures. Zhiyong Hu initiated the study and participated in study design, data interpretation and manuscript revision. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The protocol was approved by the clinical research ethic committee of the hospital (IIT20230068A). Informed consent was waived by Clinical Research Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine (Chairman: Prof. Youming LI M.D.) due to the retrospective nature of this study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fang, F., Liu, T., Li, J. et al. A novel nomogram for predicting the prolonged length of stay in post-anesthesia care unit after elective operation. BMC Anesthesiol 23, 404 (2023). https://doi.org/10.1186/s12871-023-02365-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-023-02365-w