
Abstract
Background
National guidelines for rational opioid prescribing for acute postoperative pain are needed to optimise postoperative pain control and function whilst minimising opioid-related harm.
Objectives
This overview of systematic reviews aims to summarise and critically assess the quality of systematic reviews related to the 20 recommendations from two previously published consensus guideline papers (ten relevant at patient and prescriber levels and ten at a system / Public Health level). It also aims to identify gaps in research that require further efforts to fill these in order to augment the evidence behind creating national guidelines for rational opioid prescribing for acute postoperative pain.
Methods
A systematic database search using PubMed/MEDLINE and Cochrane was conducted in November 2022. Furthermore, reference lists were reviewed. All identified systematic reviews were assessed for eligibility. Data from each study was extracted using a pre-standardised data extraction form. The methodological quality of the included reviews was assessed by two independent reviewers using the AMSTAR 2 checklist. Descriptive synthesis of the results was performed.
Results
A total of 12 papers were eligible for analysis. Only eight out of the total 20 prioritised recommendations had systematic reviews that provided evidence related to them. These systematic reviews were most commonly of critically low quality.
Conclusion
The consensus papers provide guidance and recommendations based on the consensus of expert opinion that is based on the best available evidence. However, there is a lack of evidence supporting many of these consensus statements. Efforts to further analyse interventions that aim to reduce the rates of opioid prescribing and their adverse effects should therefore continue.
Similar content being viewed by others


Introduction
Background
Between the years of 1998 and 2018, opioid prescribing has more than doubled in England [1]. Liberal prescribing of opioids for postoperative pain relief increases the risk of persistent postoperative opioid use and adverse outcomes, which has reached epidemic proportions in certain countries. These adverse outcomes include dependence, addiction, opioid use disorders, opioid-induced ventilatory impairment and overdose-related deaths [2]. A study by Gomes et al. assessed the burden of opioid-related deaths in the USA and found that the percentage of all deaths attributable to opioids increased by an alarming 292% (from 0.4% to 1.5%) between 2001 and 2016 [3]. Prescribers may unwittingly be playing a major part in this epidemic. A cohort study in 2019 found that 76.2% of surgical patients in the USA filled an opioid prescription within the first 7 days after a surgical procedure compared to 11.1% of surgical patients in Sweden [4]. An iatrogenic driving factor to the overprescribing of opioids was the unrestricted titration of opioids to numerical pain scores, such as the ‘Pain as the 5th Vital Sign’ campaign, which has now been discredited [5].
To solve this problem, guidelines have been proposed in different countries, as well as consensus documents to implement their content, but also to consider aspects that have not included. In the United Kingdom (UK), the Faculty of Pain Medicine released recommendations composed by a multi-organisational and multidisciplinary collaboration, setting out guiding principles for preoperative, perioperative, postoperative and post discharge opioid management. The aim of these recommendations is to reduce postoperative opioid use and the adverse effects caused by them. In summary, the Best Practice document gives the following recommendations on aspects of postoperative opioid management: 1) pain relief should be optimised; 2) pain assessment should involve functional assessment; 3) immediate-release opioids are preferred; 4) give advice on medicine self-administration on discharge; 5) local protocols for the prescription of discharge medications after surgery should be developed; 6) hospital discharge letter must explicitly state the recommended opioid dose, amount supplied and planned duration of use; 7) identify patients for de-escalation of opioids; 8) guidance should be given about necessary medicine review post-discharge [6].
But guidelines are necessary but not enough, and local guidance should consider local aspects and include educational programme, as recently considered as the highest priority in the context of multimodal, opioid-sparing, analgesia [7]. Accordingly, there have been two consensus statements published in the UK since 2020, not only relevant at patient and prescriber levels, but also at system and Public Health levels, aiming at facilitating local implementation and education. The first consensus paper, by Levy et al., was an international multidisciplinary consensus statement, which aimed to provide guidance in order to “assist healthcare professionals and hospitals across the world to implement effective opioid stewardship practices that achieve a balance between the administration of sufficient opioid analgesia to facilitate recovery and restoration of function, while concurrently minimising the risk of opioid-related harms” [8]. Levy et al. provides ten priority recommendations based on best evidence and, in the absence of such, expert opinion. The second statement was by Forget et al., which aimed to propose a consensus, not only on the prescribing of opioids, but also on policies for system-level interventions. Their ten recommendations were approved by a panel of experts in the field, along with healthcare representatives from different related medical disciplines and patient representatives from around the world. Therefore, the research reflects the view of a multi-stakeholder panel and represents a breadth of perspectives [2].
Although both papers provide valuable recommendations for opioid prescribing practices, they are based on expert opinion. Expert opinion is often sought during the development of governance and regulatory policies when there is insufficient empirical evidence to implement a policy or change [9], but it is essential now, in the context of evidence-based medicine, centred around the incorporation of knowledge gained through clinical trials, systematic reviews (SRs) and meta-analyses [10] to reappraise the quality of the underlying evidence and to identify knowledge gaps.
Aims
The primary aim of this overview of SRs is to summarise the evidence and critically assess the quality of SRs that are relevant to the ten priorities of each of the Levy et al. [8] and Forget et al [2] consensus statement papers. By doing so, this overview will assess the quality of evidence supporting these two consensuses. The secondary aim is to identify gaps in research that require further efforts to fill these in order to augment the evidence behind the creation of a consensus statement for rational opioid prescribing for acute postoperative pain.
Methods
Review design
This overview of reviews was conducted in accordance with the Cochrane Handbook for the Systematic Review of Interventions and reported following the Reporting guideline for overviews of healthcare interventions: the Preferred Reporting Items for Overviews of Reviews (PRIOR) statement [11, 12].
Due to the nature of this literature-based project, no ethics approval was required. However, each of the SRs included state the ethics considerations and approval that they required.
Eligibility criteria
The inclusion and exclusion criteria are shown in Table 1.
Search strategy
The search strategy involved looking at the SRs cited in reference lists of the consensus statements by Levy et al. [8] and Forget et al. [2] in addition to an electronic literature search, which was conducted during November 2022 using PubMed/MEDLINE. Various search strategies were used to identify SRs relating to the ten priorities of the Levy et al. (2020) consensus and the ten priorities of the Forget et al. consensus [2]. The complete search strategies are reported at the end of this paper under “Search Terms for Database Search”. A search limit of ‘systematic review’ and ‘meta-analysis’ was added. Papers were retrieved through additional sources, such as hand-searching the reference list of the Acute Pain Management document [13] and consulting an expert in the field for relevant papers. Backward snowballing was also used to identify relevant papers missed through the database search strategy.
Study selection
All identified citations were collated and uploaded to RefWorks 2 and duplicates were removed. Two independent reviewers (CM, RT) screened the titles and abstracts of identified articles to assess relevancy. Irrelevant articles were removed at this stage. Subsequently, full texts of selected articles were accessed and further screened by the same two reviewers (CM, RT) by applying the inclusion and exclusion criteria to assess eligibility. Articles that did not meet the eligibility criteria were removed. Any queries or uncertainties were discussed and resolved through discussion and consensus between the two reviewers (CM, RT) and a supervisor (PF).
Date extraction
A standardised data extraction form was predefined to portray the study characteristics of included articles. The following data was extracted from each article into this data extraction form by a single author (CM): author, title, year of publication, country, search period, number of primary studies included, total number of participants, effect size, intervention, outcome measures, study methods, quality evaluation method, degree of certainty, meta-analysis (yes/no) and main findings.
Quality assessment
The methodological quality of the included SRs was assessed by two independent reviewers (CM, RG) using the Assessment of Multiple Systematic Reviews 2 (AMSTAR 2) checklist [14]. The AMSTAR 2 checklist consists of ten items, including seven critical items. AMSTAR 2 does not generate an overall ‘score’, but rather it categorises the quality of the assessed article as one of the following: high (≤ 1 non-critical item weakness); moderate (> 1 non-critical item weakness); low (1 critical item weakness, with or without non-critical weaknesses); critically low (> 1 critical item weakness, with or without non-critical weaknesses). Each reviewer entered their score for each item of the checklist for each SR into an Excel document. Any discrepancies were discussed between the reviewers until consensus was reached.
Data synthesis
A quantitative meta-analytic synthesis of the included SRs was not performed due to great heterogeneity across the reviews arising from differences in sample characteristics, as well as differences between methods and outcome measures. Therefore, the data was grouped to the relevant ten priorities of the Levy consensus and the ten priorities of the Forget consensus and descriptive synthesis of the results was performed [2, 8].
Results
Search outcomes
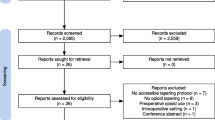
In total, 1,063 studies were identified. 276 duplicate records were removed, leaving 787 studies to be screened. After title and abstract analysis, a further 771 papers were excluded based on inclusion and exclusion criteria. The full texts of 16 studies were sought for retrieval. One study could not be fully retrieved, therefore 15 full texts were retrieved and assessed. 12 studies met the inclusion and exclusion criteria and were used in this overview (Fig. 1). The list of studies excluded after full-text analysis and reasons are shown at the end of this paper.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram (2020). This diagram illustrates the selection process of studies included in this systematic review and is based on the 2020 PRISMA flow diagram [15]
Study characteristics
A summary of the detailed characteristics of the included SRs is presented in Table 2 and their findings are summarised in Table 3. All 12 included SRs were published between 2016 and 2022. The included authors are from the USA (n = 5) [16,17,18,19,20], UK (n = 2) [21, 22], Australia (n = 1) [23], Canada (n = 1) [24], France (n = 1) [25], Poland (n = 1) [26] and Switzerland (n = 1) [27]. Three reviews included only randomised controlled trials (RCTs) [22, 25, 27]; three other reviews included only non-randomised studies of intervention (NRSIs) [19, 23, 24]; five reviews included both RCTs and NRSIs [16,17,18, 20, 21]; and one review did not specify the type of studies it included [26]. The number of studies in the SRs ranged from 6 to 135 with a mean of 41.33, and the total number of participants in these studies ranged from 810 to 1,922,743 with a mean of 220,197.58. However, one study did not report the total number of participants [17]. Only four out of the 12 included SRs were meta-analysed [19, 22, 26, 27].
There was heterogeneity with regards to quality evaluation methods used in the included SRs. Three SRs used the Newcastle–Ottawa Quality Assessment Scale [16, 19, 23]; two SRs used the Cochrane Risk of Bias Tool [22, 25]; one SR used a modified version of the Newcastle–Ottawa Quality Assessment scale and Consensus-based Standards for the selection of health Measurement Instruments (COSMIN) criteria [21]; one SR used Grading of Recommendations, Assessment, Development and Evaluations (GRADE) [27]; one SR used the Oxford levels of evidence [17]; one SR used the Scottish Intercollegiate Guidelines Network (SIGN) checklists for cohort studies and RCTs [18]; one SR used the Quality in Prognostic Studies tool [26]; one SR used the Quality Assessment Tool for Quantitative Studies [20]; and, finally, one SR did not use a quality evaluation method to assess the quality of its included studies [24].
Quality of the evidence
The quality of the included SRs was assessed using AMSTAR 2 checklist, which is presented in Table 4. The supplementary of three papers could not be accessed [18, 20, 25]. The authors of these SRs were contacted to request access to their supplementary material; however, we did not receive a response. The SRs by Lamplot et al. and Martinez et al. could, therefore, not be fully assessed using the AMSTAR 2 checklist [18, 25]. The SR by Wetzel et al. had enough information in its full text and therefore was fully assessed; however, we cannot say if their supplementary material contains information that may alter their AMSTAR 2 tool results [20].
According to the criteria of AMSTAR 2, seven of the ten SRs that could be fully assessed were of critically low quality, two were of low quality and one was of high quality. Items 2, 7 10, 11, 12 and 15 were rated particularly low amongst the included SRs. Only one SR that was able to be fully assessed reported the funding sources of the included SRs [16]. A summary of the 20 recommendations domains, and the presence or not of SRs and their respective degree of certainty is presented in Table 5.
Discussion
Main findings
The aim of this overview was to summarise the evidence and critically assess the quality of SRs that are relevant to the ten priorities of the Levy consensus and the ten priorities of the Forget consensus [2, 8]. This overview has identified a total of 12 SRs, which related to only six out of the ten priorities of the Levy consensus and two of the ten priorities of the Forget consensus. This means that a total of 12 priorities from both consensuses do not have evidence that could be identified through the methods of this overview that either supports or opposes them. Thus, we have identified a gap in research that requires further attention and efforts to fill to enhance stewardship of opioid prescribing for acute postoperative pain.
The SRs that were identified were generally of low quality according to the AMSTAR 2 checklist (seven were critically low, two were low, one was high and two could not be fully appraised). Hence, further research is required to produce evidence of a higher quality to support the consensuses and pave the way for future safer opioid prescribing. The AMSTAR 2 tool was developed in 2017 as an upgraded version of the original AMSTAR tool. It is a well-used valid and reliable appraisal tool [28].
Implications of findings within current literature
The prescribing of opioids for acute postoperative pain remains a highly controversial topic. The two consensus statements provide very promising progress for the development of national protocols for the safe prescribing and stewardship of postoperative opioids. With regards to these two consensus statements, both at patient/prescriber and system/Public Health levels, they are based on variable levels of certainty and on analyses of variable quality. This has implications when integrating these aspects into clinical practice. Indeed, levels of certainty can impact both guidelines and guidance, even if both can be based on other sources, at the condition that generalisable, high quality, evidence, is identifiable. Expert opinion can then be considered when evidence is lacking or impossible to generate. Differentiating these levels of evidence is essential to robustly secure high quality local guidance and educational programmes, which have been described as essential to implement recommendations and to confirm their local validity [7]. Sng et al. graded education as the highest priority that determines the use of opioid-sparing analgesia. Their recommendation is that more leadership and specific guidelines for multimodal analgesia could increase the adoption of these techniques. Our work could inform that kind of efforts and, here, follow specific suggestions that could be considered for implementation, in regard to the level of certainty and quality.
Specific suggestions for improvement
With regards to priority 1 of the Levy consensus (“all patients undergoing surgery should be assumed to be at risk of developing persistent postoperative opioid use and opioid-induced ventilatory impairment and may need interventions to mitigate those risks”) [8], the SR by Lawal et al. provided evidence to support this statement. They concluded that strategies, such as proactively screening for at-risk individuals, should be priorities to reduce the substantial burden that persistent opioid use after surgery elicits on public health. Lawal et al. reported that preoperative use of opioids and cocaine and the presence of comorbid pain conditions before surgery were found to have the strongest associations with persistent opioid use after surgery [19]. These modifiable risk factors could be included in a comprehensive approach to identify patients at higher risk of persistent opioid use and opioid-induced ventilatory impairment. However, it should be noted that this evidence was of critically low quality according to the AMSTAR 2 checklist.
Priority 2 of the Levy consensus (“Consider optimising management of pre-operative pain and psychological risk-factors before surgery, including weaning of opioids where possible. Ensure realistic expectations of postoperative pain control, both in hospital and after discharge”) [8] has three included SRs that provide evidence to support it. First of all, the SR by Horn et al. concluded that addressing the psychological needs of patients through preoperative education can decrease acute postoperative pain, and therefore decrease the need for opioid consumption [17]. Additionally, the SR by Powell et al. found evidence that suggested preoperative psychological preparation may be beneficial for various outcomes, such as postoperative pain, behavioural recovery, negative affect and length of stay in hospital [22]. However, the strength of evidence they found was insufficient, thus they recommended that further research is required to support this. Finally, the SR by Sobol-Kwapinska et al. analysed the relations between presurgical psychological factors and acute postoperative pain. They identified numerous psychological variables that could be considered for optimising preoperative psychological risk factors before surgery, as recommended by Levy et al. [8, 26]. The quality of evidence according to the AMSTAR 2 checklist was noted to be critically low for the SRs by Horn et al. and Sobol-Kwapinska et al., but was high for the Powell et al. SR [17, 22, 26].
Baamer et al. provided evidence for priority 3 of the Levy consensus (“provision of opioid analgesia should be guided by functional outcomes, rather than unidimensional pain scores alone”) [8] by challenging the validity and reliability of unidimensional tools to quantify acute postoperative pain. They also discovered that studies on functional outcomes assessment tools were scarce, and therefore proposed more research is necessary to assess the validity and reliability of such tools [21]. The quality of this SR was low, according to the AMSTAR 2 tool. Thus, future research of a higher quality could be beneficial to further support priority 3 of the Levy consensus.
Priority 4 of the Levy consensus (“multimodal analgesia should be optimised and patients educated about the use of non-pharmacological and non-opioid analgesia to reduce the amount and duration of opioids required to restore function”) [8] was supported through evidence from the SR by Martinez et al. This paper concluded that a multimodal regimen of non-opioid analgesics was superior to solitary use of a single non-opioid analgesia in reducing acute postoperative pain and morphine consumption [25]. The supplementary material of this SR was unavailable, resulting in full quality appraisal being unachievable. More research could be done to further assess multimodal analgesic regimens to increase the validity of this recommendation from Levy et al.
There are two SRs found through the methodology of this overview that provide evidence for the 6th priority of the Levy consensus (“a patient-centred approach should be used to limit the number of tablets and the duration of usual discharge opioid prescriptions, typically to less than a week”) [8]. Arwi and Schug suggest that the current opioid prescribing practices could be improved. The studies they analysed showed that discharge opioids contribute to prolonged opioid use [23]. However, more high-quality research with comparable outcomes is needed. Additionally, the SR by Feinberg et al. reported that surgical patients are using substantially less opioid than prescribed, leading to excess opioids that may be used inappropriately by patients or others. The authors agreed that strategies and clinical practice guidelines are needed to better educate prescribers and help standardise postoperative opioid prescriptions [24]. It should be noted that both these SRs were of critically low quality according to the AMSTAR 2 tool. It would be beneficial for research of a higher quality be carried out to further support the Levy consensus.
The 10th priority of the Levy consensus (“patients should be advised on safe storage and disposal of unused opioids and directed to avoid opioid diversion to other individuals (e.g. sharing with friends and family)”) [8] was also supported by the Arwi and Schug SR. This paper reported that a lack of patient education regarding safe storage and disposal of opioids contributes to the increasing rate of opioid misuse, diversion and unintended persistent opioid use. However, the authors recommend that more high-quality research is needed on this topic [23]. The SR by Bicket et al. provides further evidence for the 10th priority. This paper concluded that postoperative opioid prescriptions often go unused, unlocked and undisposed, leading to a reservoir of opioids that contribute to the non-medical use of these products [16]. Although both these SRs are of critically low quality according to the AMSTAR 2 checklist, they still provide important evidence that supports the 10th priority of the Levy consensus.
The SR by Lamplot et al. provides further evidence for priority 10 of the Levy consensus. They found that opioids are overprescribed for acute postoperative pain, and baseline rates of surplus opioid disposal are low. Furthermore, their results showed that drug disposal kits or bags help to significantly increase these rates [18]. Due to the supplementary material being unavailable, we could not fully assess the quality of this SR. However, it provides valuable evidence for future strategies to increase the safe disposal of unused opioids.
With regards to the Forget consensus, the 1st priority (“the presence of a Pain Management, Analgesia or Opioid Stewardship Steering Committee, with multidisciplinary representation from Key Stakeholders is a priority in the context of acute pain, especially in the hospital”) [2] has one included SR that provides supporting evidence. Their results showed evidence that clinician-mediated and organisation-level interventions are effective at reducing postoperative opioid prescribing [20]. The quality of this SR was critically low. However, it provides useful evidence to aid the development of an evidence-based clinical practice guidelines.
Finally, Albrecht et al. found that there is overall low certainty of evidence that high-dose intraoperative opioids in patients under general anaesthesia increases pain scores and contributes to hyperalgesia in the postoperative period when compared to low-dose regimen. However, they proposed that additional robust methodology trials could better define the impact of each opioid regime on hospital and health-system recourses [27]. This agrees with priority 4 of the Forget consensus (“policies should be developed providing guidelines on maximum doses and duration of treatment for high-risk medications such as opioids and high-risk combinations”) [2] by suggesting more trials should be undertaken in order to help develop such policies. The quality of the Albrecht et al. SR was low according to the AMSTAR 2 checklist.
Implications of findings for future research
The number of drug-related deaths has vastly risen over the past few decades in the UK. According to the National Drug-Related Deaths Database (NDRDD) for Scotland, there were 1,209 deaths in 2018 that were drug related in Scotland. Opioids were implicated in 77% of these deaths. This is a significant increase from 2017, when there were 867 drug-related deaths in Scotland [29]. In England and Wales, there were 3,756 drug-related deaths in 2018, a 16% increase from 2017 [30]. The rise in drug-related deaths is thought to be due to the increased availability and misuse of prescription and illicit opioids due to irrational prescribing, amongst other factors. There are concerns that the UK is closely following the trends of the devastating opioid epidemic seen in the USA. A solution to the contributing factor of liberal opioid prescribing for acute postoperative pain could be the implementation of national guidance and protocols.
The Levy and Forget consensuses provide a strong framework for such protocols. They are predominantly expert opinion based [2, 8]. Historically, medicine was based on the consensus of experts and their opinions on best practices. Though expert opinion is a highly regarded and useful method of gathering information, it is more valid when used concomitant with evidence-based literature for the creation of healthcare policies and protocols [9]. Further research is required to provide evidence of a higher quality to support these consensus statements.
Strengths & limitations
This overview included SRs of varying settings that covered a range of topics regarding rational opioid prescribing, enabling the concise evaluation and summarisation of literature related to the ten priorities of the Levy consensus and the ten priorities of the Forget consensus [2, 8]. It therefore offers valuable insight into the evidence behind the two consensuses that are predominantly based on expert opinion. Furthermore, this overview was conducted in accordance with the Cochrane Handbook for the Systematic Review of Interventions, which is well-known and well-used guidance, thus increasing reliability [11].
There are several limitations of this overview. Firstly, there was one SR that could not be accessed for full-text analysis which may have offered valuable evidence [31]. Additionally, the supplementary material of three included SRs was not available, despite requesting access from the authors, resulting in full quality appraisals being incomplete [18, 20, 25].
There was significant heterogeneity amongst the SRs regarding interventions, outcome measures, and quality evaluation method, with only four out of the 12 included SRs including meta-analysis. This meant that the SRs were not comparable. However, they provided valuable evidence for the aim of this overview.
The search strategy aimed to identify SRs for evidence for the ten priorities of the Levy consensus and the ten priorities of the Forget consensus through various database searches [2, 8]. However, predefined search strategies cannot be solely relied upon as it is probable that these various searches may have failed to identify all available relevant SRs. Backward snowballing was used to identify potential missed SRs. Finally, another limitation of this overview is that the included papers were from a wide range of countries. Though this may provide useful information that could shape future rational opioid prescribing protocols, it may not be applicable to UK guidance.
Conclusion
In conclusion, this overview of SRs provides valuable insight into the evidence behind the Levy et al. and Forget et al. consensus statements on rational opioid prescribing. However, there is a dearth of research that is required to implement valid and reliable nation opioid prescribing protocols. This overview found that there are not enough papers with high quality evidence to support the Levy et al. and Forget et al. consensus statements. The papers that were identified were mainly of low quality. Therefore, more research of a higher quality is required. The liberal prescribing of opioids for acute postoperative pain requires urgent attention. For now, it could be greatly beneficial to implement the recommendations given in the Levy et al. and Forget et al. consensus statements. The consensus papers provide guidance based on the consensus of expert opinion that is based on the best available evidence. However, efforts to further analyse interventions that aim to promote safter opioid prescribing and reduce their adverse effects should continue.
Search terms for database search
-
1.
((wean opioids) OR (taper opioids)) AND (acute pain) AND ((postsurg*) OR (postop*)).
Results = 24
-
2.
((preoperative education) OR (opioid education)) AND (acute pain) AND ((postsurg*) OR postop*)).
Results = 20
-
3.
(unidimensional pain score) AND ((postsurg*) OR (postop*)).
Results = 2
-
4.
(abnormal pain trajectory) AND (acute pain) AND ((postsurg*) OR (postop*)).
Results = 0
-
5.
((non-opioid) OR (opioid-free) AND (acute pain) AND ((postsurg*) OR (postop*)).
Results = 12
-
6.
(long-acting opioids) AND (acute pain) AND ((postsurg*) OR (postop*)).
Results = 2
-
7.
(compound opioids) AND (acute pain) AND ((postsurg*) OR (postop*)).
Results = 1
-
8.
(multimodal analgesia) AND (acute pain) AND ((postsurg*) OR (postop*)).
Results = 30
-
9.
((weaning opioids) OR (tapering opioids)) AND (acute pain) AND ((postsurg*) OR (postop*)).
Results = 1
-
10.
(repeat prescription) AND (acute pain) AND ((postsurg*) OR (postop*)).
Results = 0
-
11.
((persistent pain) OR (chronic pain) AND (acute pain) AND ((postsurg*) OR (postop*)).
Results = 190
Availability of data and materials
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Curtis HJ, Croker R, Walker AJ, Richards GC, Quinlan J, Goldacre B. Opioid prescribing trends and geographical variation in England, 1998–2018: a retrospective database study. Lancet Psychiatry. 2019;6(2):140–50. https://doi.org/10.1016/S2215-0366(18)30471-1.
Forget P, Patullo C, Hill D, Ambekar A, Baldacchino A, Cata J, Chetty S, Cox FJ, de Boer HD, Dinwoodie K, Dom G, Eccleston C, Fullen B, Jutila L, Knaggs RD, Lavand’homme P, Levy N, Lobo DN, Pogatzki-Zahn E, Scherbaum N, Smith BH, van Griensven J, Gilbert S. System-level policies on appropriate opioid use, a multi-stakeholder consensus. BMC Health Serv Res. 2022;22:329. https://doi.org/10.1186/s12913-022-07696-x.
Gomes T, Tadrous M, Mamdani MM, Paterson JM, Juurlink DN. The burden of opioid-related mortality in the United States. JAMA Netw Open. 2018;1(2):e180217. https://doi.org/10.1001/jamanetworkopen.2018.0217.
Ladha KS, Neuman MD, Broms G, Bethell J, Bateman BT, Wijeysundera DN, Bell M, Hallqvist L, Svensson T, Newcomb CW, Brensinger CM, Gaskins LJ, Wunsch H. Opioid prescribing after surgery in the United States, Canada, and Sweden. JAMA Netw Open. 2019;2(9):e1910734. https://doi.org/10.1001/jamanetworkopen.2019.10734.
Levy N, Sturgess J, Mills. “Pain as the fifth vital sign” and dependence on the “numerical pain scale” is being abandoned in the US: why? Br J Anaesth. 2018;120(3):435–8. https://doi.org/10.1016/j.bja.2017.11.098.
Faculty of Pain Medicine (FPM). Surgery and opioids: best practice guidelines 2021. Royal College of Anaesthetists. 2021. Available at: https://fpm.ac.uk/sites/fpm/files/documents/2021-03/surgery-and-opioids-2021_4.pdf. Accessed 16 Nov 2022.
Sng DD, Uitenbosch G, de Boer HD, Carvalho HN, Cata JP, Erdoes G, Heytens L, Lois FJ, Pelosi P, Rousseau AF, Forget P, Nesvadba D, Pain AND Opioids after Surgery (PANDOS) European Society of Anaesthesiology, Intensive Care (ESAIC) Research Group. Developing expert international consensus statements for opioid-sparing analgesia using the Delphi method. BMC Anesthesiol. BMC Anesthesiol. 2023;23(1):62. https://doi.org/10.1186/s12871-023-01995-4.
Levy N, Quinlan J, El-Boghdadly K, Fawcett WJ, Agarwal V, Bastable RB, Cox FJ, de Boer HD, Dowdy SC, Hattingh K, Knaggs RD, Mariano ER, Pelosi P, Scott MJ, Lobo DN, Macintyre PE. An international multidisciplinary consensus statement on the prevention of opioid-related harm in adult surgical patients. Anaesthesia. 2020;76:520–36. https://doi.org/10.1111/anae.15262.
Tonelli MR. In defense of expert opinion. Acad Med. 1999;74(11):1187–92. https://doi.org/10.1097/00001888-199911000-00010.
Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ. 1996;312(7023):71–2. https://doi.org/10.1136/bmj.312.7023.71.
Pollock M, Fernandes RM, Becker LA, Pieper D, Hartling L. Chapter V: Overviews of Reviews. In: Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane. 2022. Available from www.training.cochrane.org/handbook. Accessed 14 Nov 2022.
Gates M, Gates A, Pieper D, Fernandes RM, Tricco AC, Moher D, Brennan SE, Li T, Pollock M, Lunny C, Sepúlveda D, McKenzie JE, Scott SD, Robinson KA, Matthias K, Bougiouskas KI, Fusar-Poli P, Whiting P, Moss SJ, Hartling L. Reporting guideline for overviews of reviews of healthcare interventions: development of the PRIOR statement. BMJ. 2022;378:e070849. https://doi.org/10.1136/bmj-2022-070849.
Schug SA, Palmer GM, Scott DA, Alcock M, Halliwell R, Mott FD. Acute pain management: scientific evidence (fifth edition). Australian and New Zealand College of Anaesthetists and Faculty of Pain Medicine. 2020. Available at: https://www.anzca.edu.au/resources/college-publications/acute-pain-management/apmse5.pdf. Accessed 9 Nov 2022.
Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, Moher D, Tugwell P, Welch V, Kristjansson E, Henry DA. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. https://doi.org/10.1136/bmj.j4008.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whitling P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:71. https://doi.org/10.1136/bmj.n71.
Bicket MC, Long JJ, Pronovost PJ, Alexander GC, Wu CL. Prescription opioid analgesics commonly unused after surgery: a systematic review. JAMA Surg. 2017;152(11):1066–71. https://doi.org/10.1001/jamasurg.2017.0831.
Horn A, Kaneshiro K, Tsui B. Preemptive and preventive pain psychoeducation and its potential application as a multimodal perioperative pain control option: a systematic review. Anesth Analg. 2020;130(3):559–73. https://doi.org/10.1213/ANE.0000000000004319.
Lamplot JD, Premkumar A, James EW, Lawton CD, Pearle AD. Postoperative disposal of unused opioids: a systematic review. HSS J. 2021;17(2):235–43. https://doi.org/10.1177/15563316211001366.
Lawal OD, Gold J, Murthy A, Ruchi R, Bavry E, Hume AL, Lewkowitz AK, Brothers T, Wen X. Rate and risk factors associated with prolonged opioid use after surgery: a systematic review and meta-analysis. JAMA Network Open. 2020;3(6):e207367. https://doi.org/10.1001/jamanetworkopen.2020.7367.
Wetzel M, Hockenberry J, Raval MV. Interventions for postsurgical opioid prescribing: a systematic review. JAMA Surg. 2018;53(10):948–54. https://doi.org/10.1001/jamasurg.2018.2731.
Baamer RM, Iqbal A, Lobo DN, Knaggs RD, Levy NA, Toh LS. Utility of unidimensional and functional pain assessment tools in adult postoperative patients: a systematic review. Br J Anaesth. 2022;128(5):874–88. https://doi.org/10.1016/j.bja.2021.11.032.
Powell R, Scott NW, Manyande A, Bruce J, Vogele C, Byrne-Davis LMT, Unsworth M, Osmer C, Johnston M. Psychological preparation and postoperative outcomes for adults undergoing surgery under general anaesthesia. Cochrane Database Syst Rev. 2016;(5). https://doi.org/10.1002/14651858.CD008646.pub2
Arwi GA, Schug SA. Potential for harm associated with discharge opioids after hospital stay: a systematic review. Drugs. 2020;80:573–85. https://doi.org/10.1007/s40265-020-01294-z.
Feinberg AE, Chesney TR, Srikandarajah S, Acuna SA, Mcleod RS. Best practice in surgery group Opioid use after discharge in postoperative patients: a systematic review. Ann Surg. 2018;267(6):1056–62. https://doi.org/10.1097/SLA.0000000000002591.
Martinez V, Beloeil H, Marret E, Fletcher D, Ravaud P, Trinquart L. Non-opioid analgesics in adults after major surgery: systematic review with network meta-analysis of randomized trials. Br J Anaesth. 2017;118(1):22–31. https://doi.org/10.1093/bja/aew391.
Sobol-Kwapinska M, Babel P, Plotek W, Stelcer B. Psychological correlates of acute postsurgical pain: a systematic review and meta-analysis. Eur J Pain. 2016;20:1573–86. https://doi.org/10.1002/ejp.886.
Albrecht E, Grape S, Frauenknecht J, Kilchoer L, Kirkham K. Low- versus highdose intraoperative opioids: a systematic review with meta-analyses and trial sequential analyses. Acta Anaesthesiol Scand. 2019;64(1):6–22. https://doi.org/10.1111/aas.13470.
Lorenz RC, Matthias K, Pieper D, Wegewitz U, Morche J, Nocon M, Rissling O, Schirm J, Jacobs A. A psychometric study found AMSTAR 2 to be a valid and moderately reliable appraisal tool. J Clin Epidemiol. 2019;114:133–40. https://doi.org/10.1016/j.jclinepi.2019.05.028.
Public Health Scotland. National drug related death database (Scotland): analysis of deaths occurring in 2017 and 2018. Public Health Scotland. 2022. Available at: https://publichealthscotland.scot/publications/national-drug-related-death-database-scotland/the-national-drug-related-deaths-database-scotland-report-analysis-of-deaths-occurring-in-2017-and-2018/. Accessed 9 Dec 2022.
John E, Butt A, McQuade G. Deaths related to drug poisoning in England and Wales: 2018 registrations. Office for National Statistics. 2019. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsrelatedtodrugpoisoninginenglandandwales/2018registrations#drug-poisoning-deaths-registered-in-2018-increased-significantly. Accessed 9 Dec 2022.
Zorrilla-Vaca A, Mena GE, Ramirez PT, Lee BH, Sideris A, Wu CL. Effectiveness of postoperative opioid educational initiatives: a systematic review and meta-analysis. Anesth Analg. 2022;134(5):940–51. https://doi.org/10.1213/ANE.0000000000005634.
Acknowledgements
Not applicable.
Funding
The authors received no specific funding for this work.
Author information
Authors and Affiliations
Contributions
CM wrote the main manuscript text. CM and RT screened the identified articles. CM and RG appraised the included articles. CM and PF reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Due to the nature of this literature-based project, no ethics approval was required. However, each of the systematic reviews included state the ethics considerations and approval that they required.
Consent for publication
Not applicable.
Competing interests
Forget P received speaker/advisory board fees from Grunethal and Oncomfort.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
McCorquodale, C.L., Greening, R., Tulloch, R. et al. Opioid prescribing for acute postoperative pain: an overview of systematic reviews related to two consensus statements relevant at patient, prescriber, system and public health levels. BMC Anesthesiol 23, 294 (2023). https://doi.org/10.1186/s12871-023-02243-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-023-02243-5