
Abstract
Background
Prostate cancer (PC) is a significant public health problem affecting men worldwide and ranks third in incidence and mortality in East Africa. Cost of prostate cancer management is high in low-income countries because majority of patients presents with advanced (metastatic) PC. The cost related to management of PC including castrate resistant cancer in Tanzania has remained unknown; hence, policy makers do not have enough information for planning and resource allocation. This study therefore aimed to document costs related to the management of patients with prostate cancer including castrate resistant prostate cancer (CRPC) at Muhimbili National Hospital in Tanzania.
Methods
This was a retrospective descriptive hospital-based study which was conducted at Muhimbili National Hospital (MNH). Case notes of patients who were treated for prostate cancer were retrieved from medical records for review. A structured checklist was used to extract information regarding age, clinical presentation, investigations, stage of disease, type of treatment, payment modality and reimbursement. We considered data on the direct costs of prostate cancer management (diagnosis, treatment and follow-up) based on hospital price list of different categories. Costs reported were based on payment category in total and unit cost but also source of funding. Descriptive statistics were prepared and summarized as tables and figures.
Results
A total of 292 case notes of patients with prostate cancer were reviewed of which 189 patients received androgen deprivation therapy. Ninety-six (50.8%) met the criteria for the diagnoses of CRPC, and their mean age was 71.23 ± 4.2. Most of the patients had a poorly differentiated histology with prostate-specific antigen (PSA) over 100 ng/l. Bilateral orchiectomy was the most common treatment modality offered for advanced prostate cancer. Total cost for all PC patients was $148,136.4, equivalent to a unit cost per patient of $507.3. However, patients were in different categories of payment, 53% were public patients with an average cost of $471.3 per patient; 36.6% were cost sharing patients with an average cost of $441.8 per patient; 8.2% were National Health Insurance (NHIF) patients with an average cost of $893.8 per patient; and only 2.2% were private patients with an average cost of $1060.9 per patient.
Conclusion
Costs related to prostate cancer management need harmonization to accommodate different categories of patients in need.
Similar content being viewed by others


1 Background
Prostate cancer (PC) is now the second most frequent cancer in men and fifth cause of cancer-related mortality globally by contributing to 1.3 million cases and 359,000 deaths [1, 2]. In East Africa and sub-Saharan Africa, patients with cancer including prostate cancer do present with advanced stages of cancer warranting them to be treated for palliative intention through androgen deprivation therapy (ADT) which is the standard treatment for advanced prostate cancer androgen deprivation by surgical or medical castration [3,4,5].
In Tanzania, like many low-income countries (LICs), cancer rates are on the rising horizon, and the extreme poverty of its population presents many obstacles to cancer care [5,6,7]. Some patients live far from healthcare facilities and are often unable to pay for transportation and accommodation during treatment, a reality that further limits access to care [5]. It is further documented that the average amount of money patients’ need to buy anticancer medicines is TZS 151,100 (equivalent to $66) for one course of treatment which is too costly due to the fact that few patients are covered by health insurance [4, 8]. In Tanzania, the cost related to management of PC including has remained unknown; hence, policy makers do not have enough information for planning and resource allocation. This study therefore aimed to document costs related to the management of patients with prostate cancer at Muhimbili National Hospital in Tanzania.
2 Methods
A retrospective hospital-based descriptive study, involving patient records review, was carried out at Muhimbili National Hospital (MNH). Perspectives used for costing were health provider perspective. The reviewed records were for patients that were treated at the hospital between 2018 and 2019. Muhimbili National Hospital receives patients with prostate cancer at various stages from the whole country. The hospital has capacity to diagnose and treat prostate cancer, in collaboration with a sister institution, the Ocean Road Cancer Institute—ORCI, that specializes in cancer care (12). PC in our context is diagnosed by digital rectal examination, prostate-specific antigen and finger-guided tru-cut biopsy followed by histological evaluation [7, 9].
We included patients who had a diagnosis of PC and treated by androgen deprivation therapy (medical or surgical). Surgical androgen deprivation therapy was by bilateral orchiectomy while medical androgen deprivation was by goserelin 3.6 mg SubQ Q28d and bicalutamide 50 mg OD for 2 weeks: Patient then continues with goserelin monotherapy. Testosterone levels were checked at three months to establish attainment of castrate levels, ≥ 0.7 nmol/L. Patients with castrate resistance were considered at three months if: PSA levels remained high or continued to rise; clinical or radiological features of disease show progression or onset of new symptoms related to PC.
We identified medical registration numbers of patients with histological diagnosis of PC from the hospital central pathology laboratory registry. Then traced their case notes from the hospital’s records department. A data collection form was used to extract information form the patient records. This was done by a trained research assistant.
The following variables were extracted: patients’ age, clinical presentation at follow-up, Gleason score, investigations done, PSA level (at baseline and at three months), any comorbidities, clinical presentation and price per category related to investigations and treatment, as well as the mode of payment. We considered the existing modes of health financing categories: 1. Insured patients are those who are insured either through NHIF or other private insurance companies where their costs are covered by the insurance companies. 2. Private (IPPM) patients are those self-referral or referrals from private hospitals will pay out of pocket for their medical services. Public and cost sharing patients are those referred from regional hospitals whose costs are usually subsidized.
We considered data on the direct costs of prostate cancer (e.g., diagnosis, treatment and follow-up) based on hospital price list of different categories. Diagnosis included the following categories—cost of full blood picture, PSA level, abd–pelvic USS, CXR, electrolytes (sodium), electrolytes (potassium), creatinine, BUN, tissue biopsy, lumbo-sacral X-ray and spine MRI. Treatment and follow-up included the following categories—hospitalization, BSO, consumables, consultation and radical prostatectomy.
The collected data were checked for completeness and entered in Statistical Package for Social Scientists (SPSS) version 23 and Microsoft Excel for analysis. For demographic characteristics of study population, continuous variables were summarized as means with standard deviations while categorical variables were summarized as frequency with percentages. For cost analysis, total costs were calculated by summing the cost of all resources used in the management of PC. Unit costs were calculated by dividing total cost of PC management by the number of patients in the study. Costs were analyzed considering all patient categories, by source of financing and by type of service. Deterministic sensitivity analysis is conducted to check how changes in variable assumptions will affect final results. Costs are reported in 2018 US$. Tables and charts are used to summarize results as presented in the subsequent section.
3 Results
A total of 292 patients were treated for PC by androgen deprivation therapy (surgical and/or medical) at MNH in 2018/2019. Majority 189 (64.5%) had reached castrate levels of which 96 (50.8%) met the criteria for the diagnoses of CRPC. The mean age of CRPC patients was 71.23 ± 4.2 (63–94) years. Out of the 292 clients, 128 (43.6%) were unemployed. Employment status was not documented in 38 cases (13.1%).
Figure 1 presents clinical presentation among patients, PC with CRPC inclusive of which lower urinary tract symptoms was the most frequent symptom reported by 256 (87.5%) of the patients, followed by urinary bladder obstruction and back pain in 168 (57.3%) and 165 (56.3%), respectively. Some patients—126(43.8%)—presented with paraplegia. Majority of patients with PC and CRPC had clinical progression or development of new prostate cancer-related symptoms.

Bar chart showing clinical presentation among patients with PC and CRPC at MNH. LUTS, Lower Urinary Tract Symptoms; HMT, Hematuria; BOO, Urinary Bladder Outlet Obstruction; BP, Back Pain; LLS, Lower Limb Swelling; PP, Paraplegia
All patients had histology results of prostate adenocarcinoma. The most common reported Gleason score was 9 at 122(41%) which signifies poorly differentiated prostate cancer. All patients had a baseline PSA of more than 50 ng/mL and majority of which had a baseline PSA of more than 100 ng/mL. The most common imaging done in these patients was abdominal–pelvic ultrasound with only 13.5% having a spine MRI. Most patients were primarily treated by bilateral subcapsular orchiectomy (Table 1).
Figure 2 shows proportion of patients in the different payment categories, of which 155 (53%) were public patients, 107(36.6%) were cost sharing patients, 24(8.2%) were National Health Insurance (NHIF) patients and only 6(2.2%) were private patients.

Distribution of payment categories
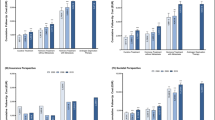
Table 2 shows the number of services utilized by patients by payment mechanism, and Table 3 shows the price per procedure according to the payment category.
Most patients 181 (61.8%) had been admitted at least once due prostate cancer, and all of them had attended outpatient clinic at least once. During admission and clinics, investigations and treatments were offered. Taking into account the investigations done, consultations during clinic visits, accommodation during admissions and the treatment given, the total and average cost for each category are shown on Table 4.
4 Discussion
We conducted this descriptive study to estimate costs related to the management of patients presenting with PC at Muhimbili National Hospital. This study aimed to document and give an overview of costs related to the management of patients with PC. This is a first costing study done among patients with PC in Tanzania, and the findings are representative of the general scope of PC management including CRPC and related costs. We therefore discuss with a view of how much cost is relatively likely to be spent in the management of patients with PC and CRPC in the Tanzanian setting.
Most of patients with prostate cancer in low-income countries Tanzania included present with advanced disease and CRPC which both bring a dilemma given the morbidity and the cost needed to manage such patients [10]. Patients in sub-Saharan Africa have been shown to have poor access to active treatment of PC and CRPC [4, 11]; it is expected that Tanzanian men will present with advanced stages and incurable forms of PC [5, 12]. This late stage at presentation is probably due to a weak health system in the country with scarcity of skilled human resources for health [4].
Androgen deprivation by bilateral orchiectomy is commonly practiced in our setting; this would mean that it is acceptable though we lack such evidence on its acceptability by patients [13]. This has proved to be a very effective androgen deprivation strategy in settings with scarce resources. It can be advocated for widespread use in our settings along with early diagnosis strategies. We did not study influence of the type of androgen deprivation therapy (ADT) medical versus surgical on the development of CRPC but it could be important to study in our setting [14, 15]. Being in a public healthcare setting, few patients in our study were capable to choose and pay for medical androgen deprivation. It is our feeling that it is good to ensure that castrate levels have been achieved by any of the strategies by checking for testosterone levels, typically at or less than 0.7 nmol/L. This should be done for all patients who demonstrate disease progression (new symptoms or progression of preexisting symptoms or rising PSA levels) before declaring CRPC. Our findings are in line to the definition of the diagnosis of CRPC of it cannot be reliably made before realization of attainment of castrate levels of testosterone: It should therefore be a practice to have all patients check testosterone levels during routine follow-up visits in urology clinics [16, 17].
Even though our study did not assess the treatment strategies offered, it should be noted that algorithms for such patients have been developed and used extensively in other settings. But as cancer services are covered by government, it is important to do cost-benefit analysis of what it would take to aggressively treat CRPC in such a fragile healthcare system with rampant out of pocket payment. Radiotherapy and chemotherapeutics are largely “free” of payment by patients but only when available [15, 18]. Additionally, the use of chemotherapy in Africa is often limited by cost and non-availability of the drugs [4, 18, 19]. Cost related to management strategies for patients with PC and CRPC differs according to the type of presentation: biochemical without evidence of disease versus metastatic presentation in which most of our patients had progression with evidence of disease hence [20] fall in the mCRPC which requires additional management strategies including: secondary hormonal manipulation, chemotherapy, radiotherapy and immunotherapy that has cost implications as docetaxel price is about 160,000 TZS (equivalent to $70) while abiraterone price was 20,000TZS (equivalent to $9) per tablet of 250 mg. Patients need to be assigned one of the six classes for better treatment outcomes as outlined by America Urology Association [4, 8, 18].
Patients diagnosed at earlier stages with low-grade cancer may receive watchful waiting which has the effect of lowering costs relative to patients diagnosed at higher stages [18, 20]; the findings from this study are impressive by exposing that the cost related to the management of PC/CRPC is likely to be influenced by advanced stage to disease leading CRPC which is costly regardless of the mode of payment with big variation from those who pays in the category of public patient to those who pays as private patients.
5 Conclusion
Our study findings offer an insight into the magnitude of total and unit cost of patients with PC diagnosis in an era of improved awareness, screening and treatment. The reported variation in costs across different categories is due to differing payments options and not due to differences in detection and management practices as would be expected. Long-term estimates are useful for understanding the upper limit of treatment costs that could be avoided should prevention strategies prove effective in reducing incident PC cases. Costs related to prostate cancer management need harmonization to accommodate different categories of patients in need. More studies are encouraged to assess cost effectives of different treatment options for prostate cancer.
Availability of data and materials
It is declared that data and materials are available. They can be sought from the corresponding author (first author).
Abbreviations
- PC:
-
Prostate cancer
- DR:
-
Document review
- SSA:
-
Sub-Saharan Africa
- LMICs:
-
Low- and middle-income countries
- MNH:
-
Muhimbili National Hospital
- MUHAS:
-
Muhimbili University of Health and Allied Sciences
- CRPC:
-
Castrate resistant prostate cancer
- ADT:
-
Androgen deprivation therapy
- BSO:
-
Bilateral subcapsular orchiectomy
- NHIF:
-
National insurance fund
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A et al (2021) Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71:209–249
Wang L, Lu B, He M, Wang Y, Wang Z, Du L (2022) Prostate cancer incidence and mortality: global status and temporal trends in 89 countries from 2000 to 2019. Front Public Heal. https://doi.org/10.3389/fpubh.2022.811044
Adeloye D, David RA, Aderemi AV, Iseolorunkanmi A, Oyedokun A, Iweala EEJ et al (2016) An estimate of the incidence of prostate cancer in Africa: a systematic review and meta-analysis. PLoS ONE 11:1–18
Ngwa W, Addai BW, Adewole I, Ainsworth V, Alaro J, Alatise OI et al (2022) Cancer in sub-Saharan Africa: a lancet oncology commission. Lancet Oncol 23:e251-312
Makene FS, Ngilangwa R, Santos C, Cross C, Ngoma T, Mujinja PGM et al (2022) Patients’ pathways to cancer care in Tanzania: documenting and addressing social inequalities in reaching a cancer diagnosis. BMC Health Serv Res 22:1–14
Lyimo EP, Rumisha SF, Mremi IR, Mangu CD, Kishamawe C, Chiduo MG et al (2020) Cancer mortality patterns in Tanzania: a retrospective hospital-based study, 2006–2015. J Glob Oncol 6:224–232
Mmbaga EJ. Clinical characteristics, survival rate and patients’ perceptions among patients diagnosed with prostate cancer receiving treatment at Ocean Road Cancer Institute in Dar Es Salaam, Tanzania: A mixed-method study. 2022.
Mattila PO, Ahmad R, Hasan SS, Babar ZUD (2021) Availability, affordability, access, and pricing of anti-cancer medicines in low- and middle-income countries: a systematic review of literature. Front Public Health. https://doi.org/10.3389/fpubh.2021.628744
Nyagabona SK, Luhar R, Ndumbalo J, Mvungi N, Ngoma M, Meena S, Siu S, Said M, Mwaiselage J, Tarimo E, Buckle G (2021) Views from multidisciplinary oncology clinicians on strengthening cancer care delivery systems in Tanzania. Oncol 26(7):e1197–e1204
Mbugua RG, Oluchina S, Karanja S (2021) Prostate cancer awareness and screening among men in a rural community in Kenya : a cross - sectional study. African J Urol. https://doi.org/10.1186/s12301-020-00108-8
Freddie B, Ariana Z, Cueva P, Korir A, Swaminathan R, Ullrich A, et al. (2021) Planning and Developing Population-Based Cancer Registration in Low- or Middle-Income Settings
Nyongole OV, Kivuyo NE, Mushi FA, Akoko LO, Mizinduko M, Mtaturu GF, Aboud M, Mkony CA (2020) A retrospective study of patients with castrate resistant prostate cancer at Muhimbili national hospital Tanzania. Tanzan Med J 31(2):1
Stokes ME, Ishak J, Proskorovsky I, Black LK, Huang Y (2011) Lifetime economic burden of prostate cancer. BMC Health Serv Res 11:349
Godfrey N, Obadia N, Jasper M (2014) Metabolic syndrome in patients on androgen deprivation therapy for prostate cancer as seen at Kilimanjaro Christian medical center, moshi Tanzania. East Cent Afr J Surg 19:102–108
Nguyen C, Du XL, Lairson DR, Swartz MD (2019) Cost-effectiveness of adding androgen deprivation therapy to radiation therapy for men with advanced prostate cancer from a U.S. payer’s perspective. J Manag Care Spec Pharm. 25:225–234
Modi PK, Yan P, Hollenbeck BK, Kaufman SR, Borza T, Skolarus TA et al (2021) Urologist practice structure and quality of prostate cancer care. Urology practice 7:419–424
Sanghera S, Mohiuddin S, Coast J, Garfield K, Noble S, Metcalfe C et al (2020) Modelling the lifetime cost-effectiveness of radical prostatectomy, radiotherapy and active monitoring for men with clinically localised prostate cancer from median 10-year outcomes in the ProtecT randomised trial. BMC Cancer 20:1–10
Kowalchuk RO, Kim H, Harmsen WS, Jeans EB, Morris LK, Mullikin TC et al (2022) Cost effectiveness of treatment strategies for high risk prostate cancer. Cancer 128:3815–3823
Parmar A, Timilshina N, Emmenegger U, Smoragiewicz M, Sander B, Alibhai S et al (2022) A cost-utility analysis of apalutamide for metastatic castrationsensitive prostate cancer. Can Urol Assoc J. https://doi.org/10.5489/cuaj.7495
Bayoumi AM, Brown AD, Garber AM (2000) Cost-effectiveness of androgen suppression therapies in advanced prostate cancer. J Natl Cancer Inst 92:1731–1739
Acknowledgements
We acknowledge the support MUHAS and Hospital authorities, research assistants, healthcare providers (HCP) and patients with prostate cancer for their participation.
Funding
This was partially funded by MUHAS through SIDA project small grant for capacity building.
Author information
Authors and Affiliations
Contributions
OVN and NEK developed research proposal, collected and analyzed data and developed manuscript. LOA, HS and NK reviewed the proposal and manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We obtained ethical clearance from the Research and Ethics Committee of the Muhimbili University of Health and Allied Sciences. Permission to collect data was sought from Muhimbili National Hospital.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Nyongole, O.V., Kivuyo, N.E., Akoko, L.O. et al. Estimating cost of prostate cancer management: an experience from Tanzania. Afr J Urol 30, 17 (2024). https://doi.org/10.1186/s12301-024-00422-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12301-024-00422-5