
Abstract
Background
Primary renal squamous cell carcinoma is a scarce entity, and its presentation as a discharging sinus is still exceptionally rare. We hereby report a case of a renal cell carcinoma in a young gentleman.
Case presentation
We report a case of a 20-year-old gentleman who presented with clinical features suggestive of left side xanthogranulomatous pyelonephritis (XGPN). He had undergone multiple endourological procedures for left side renal calculi in the past. We present the clinical presentation, diagnostic dilemmas and treatment for this patient. We performed an open radical nephrectomy for this patient. Our case report is unique from the point of view of nature of presentation to the final histopathological outcome in terms of age group of the patient.
Here we present the clinical management and dilemmas in the management of this unusual and rare case.
Conclusions
Our case report and presentation has taught us that we as clinicians must have a high index of suspicion for a renal malignancy when treating patients who present with pyonephrosis associated with long-standing calculi diseases, irrespective of the age group of the patient.
Similar content being viewed by others

1 Background
Squamous cell carcinoma (SCC) of the renal parenchyma is an extremely rare disease. It accounts for 0.5–0.8% of all the renal malignancies [1] There is a paucity of the literature regarding this entity and this case is probably the youngest aged patient ever to be reported to the best of our knowledge [2,3,4,5,6]. Etiological factors for renal SCC are large renal calculi, infection, endogenous and exogenous chemicals, hormonal imbalance, and vitamin A deficiency, although it can occur without any etiological factors [7]. Occasionally SCC of the kidney may even masquerade as xanthogranulomatous pyelonephritis (XGPN).
We present a case of primary renal SCC and discuss its diagnostic dilemmas and clinical management.
2 Case presentation
A 20-year-old gentleman presented to us with a left flank discharging sinus and left flank pain (Fig. 1). He had multiple episodes of endourological procedures starting from the age of 2 till the present age. Six months ago, he was diagnosed to have a renal and psoas abscess for which he underwent a left side percutaneous nephrostomy (PCN) placement and he was empirically started on anti- tuberculosis medications.

Demonstrating discharging sinus over the left flank
Subsequently he continued to have low grade fever for which he was managed conservatively. He now presented to us with left flank pain and a discharging sinus.
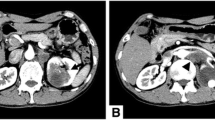
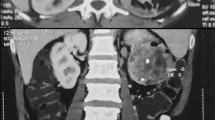
On presentation he was hemodynamically stable with a deranged renal function test with a serum creatinine of 1.86 mg/dl (GFR-50.9 ml/min/1.73m2). A non-contrast computed tomography of the abdomen and pelvis (NCCT) showed a left side grossly enlarged kidney with multiple pockets of pus within it which was suggestive of pyonephrosis. There was also a well-defined loculated collection in the left psoas muscle (Fig. 2). In keeping with his clinical presentation features and imaging findings, a diagnosis of left side XGPN was made and the patient was counselled for the need for left open nephrectomy.

Grossly enlarged left kidney with multiple pockets of collection at the left kidney demonstrating hydronephrosis suggesting pyonephrosis with left ureteral stent noted in situ
Intra-operatively, the peritoneum and left colon were grossly adherent to the left kidney. The kidney along with the mass had grossly eroded the left psoas muscle. A radical nephrectomy was performed and intra-operatively one unit of blood needed to be transfused. The histopathology of the specimen was reported as a well-differentiated squamous cell carcinoma infiltrating the real parenchyma, perinephric and periureteric fat and staged as p T4N0 (Fig. 3).

Histopathological slide: Well-differentiated squamous cell carcinoma. Tumor infiltrates renal parenchyma, perinephric fat and periureteric fat
The patient is afebrile and does not have any local symptoms, now after 4 months of follow-up.
3 Discussion
SCC of the renal pelvis was regarded as urothelial metaplasia [7, 8]; however, the histological origin and mechanism of renal parenchyma SCC remains unknown. It is postulated to originate from convoluted tubules or undifferentiated stem cells of the renal mesenchyme. SCC of the kidney is frequently associated with urolithiasis and hydronephrosis [6,7,8].
To arrive at a diagnosis of SCC renal parenchyma can be quite challenging, as there are no characteristic clinical or radiological features that will help us to clinch a diagnosis [9].
Our case report puts forward a number of interesting points. It is a well-known fact that XGPN acts like a great masquerader mimicking pyonephrosis or even renal cell carcinoma. Histologically XGPN is typically characterized by the presence of lipid laden macrophages, while renal SCC typically demonstrates dysplastic squamous mucosa and presence of keratin pearl formation, XGPN could present as a precursor lesion to SCC [10]. Our case is unusual in the way that our patient presented to us with a discharging sinus in a pyonephrotic kidney. The only possible preoperative factor that could have pointed us in the right direction would have been his past history of being a recurrent stone former.
The uniqueness of our case report lies in the following factors, young age of the patient, a discharging sinus with a left non-functioning kidney, presenting with a left psoas abscess, leading to a diagnostic dilemma of probable tuberculosis in our country. A timely diagnosis is of paramount importance in such a case as renal SCC has an extremely aggressive course an outcome.
The treatment for patients diagnosed with renal SCC continues to be surgery in the form of radical nephrectomy or nephroureterectomy even in the setting of an advanced disease [11].
The 5-year survival rate for advanced renal SCC is less than 10% with the median survival of 5 months [7].
4 Conclusions
Our case report and presentation has taught us that we must have a high index of suspicion when treating patients who present with long-standing calculi diseases with a renal mass, not only in an elderly group of the population but also in a younger group of patients who present with certain atypical presentation patterns, like in the case of our patient.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- XGPN:
-
Xanthogranulomatous pyelonephritis
- SCC:
-
Squamous cell carcinoma
- PCN:
-
Percutaneous nephrostomy
- NCCT:
-
Non-contrast computed tomography of the abdomen and pelvis
References
Li MK, Cheung WL (1987) Squamous cell carcinoma of the renal pelvis. J Urol 138(2):269–271
Terada T (2010) Synchronous squamous cell carcinoma of the kidney, squamous cell carcinoma of the ureter, and sarcomatoid carcinoma of the urinary bladder: a case report. Pathol Res Pract 206(6):379–383
Kulshreshtha P, Kannan N, Bhardwaj R, Batra S (2012) Primary squamous cell carcinoma of the renal parenchyma. Indian J Pathol Microbiol 55(3):370–371
Pusiol T, Zorzi MG, Morini A (2013) Comment on: primary squamous cell carcinoma of the renal parenchyma. Indian J Pathol Microbiol 56(1):70
Ghosh P, Saha K (2014) Primary Intraparenchymal squamous cell carcinoma of the kidney: a rare and unique entity. Case Rep Pathol 2014:1–3
Wang Z, Yan B, Wei YB, Hu NA, Shen Q, Li D, Yang JR, Yang X (2016) Primary kidney parenchyma squamous cell carcinoma mimicking. Oncol Lett 11(3):2179–2181
Palmer CJ, Atty C, Sekosan M, Hollowell CM, Wille MA (2014) Squamous cell carcinoma of the renal pelvis. Urology 84(1):8–11
Jiang P, Wang C, Chen S, Li J, Xiang J, Xie L (2015) Primary renal squamous cell carcinoma mimicking the renal cyst: a case report and review of the recent literature. BMC Urol 15:69
Kalayci OT, Bozdag Z, Sonmezgoz F, Sahin N (2013) Squamous cell carcinoma of the renal pelvis associated with kidney stones: radiologic imaging features with gross and histopathological correlation. J Clin Imaging Sci 29(3):14. https://doi.org/10.4103/2156-7514.109741
Ganpule A, Jagtap J, Ganpule S, Bhattu A, Soni S, Sabnis R, Desai M (2013) Xanthogranulomatous pyelonephritis (XGPN) mimicking a “renal cell carcinoma with renal vein thrombus and paracaval lymphadenopathy.” F1000Res 2:263. https://doi.org/10.12688/f1000research.2-263.v1
Holmäng S, Lele SM, Johansson SL (2007) Squamous cell carcinoma of the renal pelvis and ureter: incidence, symptoms, treatment and outcome. J Urol 178:51–56
Acknowledgements
The authors acknowledge the support received from the staff at the Muljibhai Patel Urological Hospital, Nadiad, India.
Funding
No funding was obtained for this project.
Author information
Authors and Affiliations
Contributions
CV and AP were involved in drafting the manuscript and patient care. AG, SMS, AGS and RBS were involved in supervising and editing the manuscript. MRD was involved in proof reading the manuscript and conceptualization of the idea. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent for participate
The Ethical committee (EC) approval for the project on squamous cell carcinoma of the renal pelvis on January 24, 2022. EC Approval No. EC/796/2022. Updated Ethics committee (MPSRNUEC) approval dated December 13, 2022, with Reference No. EC/907/2022.
Consent for publication
Written informed consent for publication was sought from the patient.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Victor, C., Patil, A., Ganpule, A. et al. A case report: a renal squamous cell carcinoma presenting as a nephrocutaneous fistula. Afr J Urol 29, 2 (2023). https://doi.org/10.1186/s12301-022-00331-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12301-022-00331-5