
Abstract
Background
Intrauterine copper devices are a popular type of contraceptives, being in use for a long time. Migration of IUCD into the bladder is one of the many side effects of this contraceptive measure. Though a rare phenomenon, IUCD acting as a foreign body can cause stone formation in the bladder.
Case presentation
We present a 42-year-old female patient who presented with increased urinary frequency, dysuria, and suprapubic pain. Examination showed mild tenderness in the suprapubic region. On X-ray pelvis, she was found to have a giant stone covering IUCD in the bladder. She ultimately underwent cystolithotomy, and her IUCD with stone was removed. Consequently, she was discharged on the 4th postoperative day with a satisfactory condition.
Conclusion
Vesical calculus can form following migration of IUCD in the bladder. This article highlights the importance of careful insertion and follow-up investigation of IUCD. Radiological modalities like X-rays pelvis provide excellent visualization of the IUCD and can be used to confirm the accurate location of the contraceptive device.
Similar content being viewed by others


1 Background
Intrauterine copper devices IUCD are widely used contraceptive measures in the last few decades. Their safety and longer duration of action make them an excellent choice for contraceptives. Out of many side effects, movement of IUCD out of the bladder causing uterine perforation is the most severe but least common one. The migration of IUCD is a rare phenomenon, and only a few cases have been reported. The incidence is estimated to be around 0 to 1.6 in 1000 insertions [1]. Once the IUCD transmigrates into the bladder, it acts as a nidus for calculus formation [2, 3]. The typical presentation is quite similar to the vesical calculus. Common symptoms include haematuria, dysuria, increased urinary frequency, and suprapubic pain [3]. This article sheds light on the importance of expertise for IUCD insertion. It also provides details on the usual presentation of IUCD migration and its treatment modalities.
2 Case presentation
A 42-year-old female patient presented with complaints of lower urinary tract symptoms associated with suprapubic pain for the last two years. Past history revealed that she underwent IUCD insertion around 18 years ago. However, after four years, following an episode of hematuria and suprapubic pain, her IUCD threads were removed and her symptoms settled after few weeks. She delivered a boy a year later.
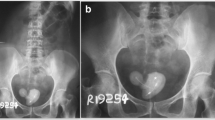
On her abdominal examination, suprapubic tenderness was noted. Baseline laboratory studies were within normal parameters. However, urinalysis showed pyuria and haematuria. Her urinary culture grew Escherichia coli, for which injection ceftriaxone one gram twice a day was started. Ultrasound KUB showed a large vesical calculus. Further evaluation with X-ray KUB revealed a large bladder stone associated with what appeared to be an IUCD (Fig. 1). For detailed investigations and management planning, a cystoscopy was scheduled which confirmed the presence of a giant calculus covering a part of the intrauterine copper device.

X-rays pelvis showing a large vesical calculus associated with IUCD
Due to the larger size of the bladder stone and the presence of a foreign body, open cystolithotomy was planned. The patient underwent surgery in spinal anesthesia, and a floating IUCD without the threads covered with a large bladder stone was removed from her bladder (Fig. 2). Neither the IUCD nor the stone was adherent to the bladder wall. On chemical analysis, the stone was found to be composed of calcium oxalate. The patient was discharged on the 4th postoperative day with a satisfactory condition. On her follow-up visit in 2nd week, her urinary catheter was removed. She remained stable and symptoms-free on follow-up visits at the 4th and 8th weeks. An X-ray pelvis was done at 8th week and was unremarkable.

Image showing a giant vesical calculus along with IUCD removed through open cystolithotomy
3 Discussion
Intrauterine copper devices have been in use for around five decades now. Their relative safety and longevity are the most important factors for their preference over other contraceptive measures. As with any other treatment or intervention, IUCD also brings various unfavorable side effects. A few of the potential serious side effects of IUCD include dysmenorrhoea, ectopic pregnancy, pelvic infection, abscess, and septic abortion [3,4,5]. Transmigration of IUCD into adjacent structures is another side effect that is extremely rare. Typically, migration occurs into the surrounding organs, most commonly into the bladder, but few cases of IUCD migrating into the peritoneum, omentum, and colon are also reported in the literature [4, 6, 7]. In our case, IUCD migrated into the urinary bladder.
Expertise and skills play a significant role in the development of uterine perforation by an IUCD migration. Most of the migrations (86%) result during the procedure of insertion of the intrauterine copper device. A study emphasized the importance of skills by determining the chances of perforation. It showed that doctors with experience of fewer than ten device insertions were more likely to report uterine perforation than those with more experience [8].
Foreign bodies in the bladder can cause vesical calculus formation. Though rare, intrauterine copper devices can act as a nidus to form bladder stones. Calcium accumulation on the intrauterine copper device is also believed to play a role in the development of stones [9, 10]. Vesical calculi are relatively rare in women, as typically they are associated with obstructive urinary symptoms in men. The presence of bladder stones in females should bring suspicion of a foreign body such as IUCD in our patient [4].
Classically, patients present with symptoms like hematuria, irritative voiding symptoms (increased urinary frequency), suprapubic pain, and urinary incontinence [3]. Similarly, our patient had suprapubic pain, hematuria, and increased urinary frequency. Due to the overlapping of symptoms with those of cystitis, these patients should be managed with extreme care. Investigations like USG and X-rays can be beneficial in confirming the suspected diagnosis of migrated IUCD. Timely diagnosis can avoid unnecessary use of antibiotics as many of such patients get multiple antibiotic courses before the actual diagnosis is reached [11]. This is true in our case, as the patient took various antibiotics before she presented to us.
According to the International Planned Parenthood Federation, any perforated IUCD should be immediately removed [12]. It is even more critical if migration occurs into the urinary bladder with the potential of stone formation. Various methods like vaginal or suprapubic cystotomy can be used to remove IUCD alongside the adherent stone [1]. Literature review shows methods like cytoscopic removal, laser lithotripsy and even laparotomy have been used to remove migrant IUCD. However, open cystolithotomy is the most commonly used procedure [13]. Similarly, open cystolithotomy through a suprapubic approach was preferred in our case due to the significantly larger stone.
4 Conclusions
-
X-ray pelvis can provide excellent visualization of IUCD along with the stone.The size and position of IUCD and bladder stone on X-ray can help the surgeons decide the type of surgery.
-
Pelvic USG or X-ray should be done after insertion of the IUCD to confirm its position within the bladder.
-
Female patients presenting with symptoms related to cystitis, like urinary frequency and suprapubic pain should be investigated for potential migration of IUCD.
4.1 Patient Perspective
I was very frustrated as I remained undiagnosed for many years. Getting various treatments for different possibilities overwhelmed the situation. Once I was admitted here, I was properly guided through all of my workup and management. The surgery relieved my complaints that were present for years and I am very satisfied with the treatment and the overall outcome.
Availability of data and materials
Not Applicable.
Abbreviations
- IUCD:
-
Intrauterine contraceptive device
- USG:
-
Ultrasonography
- KUB:
-
Kidneys, ureters, bladder
References
Gillis E, Chhiv N, Kang S, Sayegh R, Lotfipour S (2006) Case of Urethral Foreign Body: IUD perforation of the bladder with calculus formation. California J Emerg Med 7(3):47–53
Atakan RH, Kaplan M, Ertrk E (2002) Intravesical migration of intrauterine device resulting in stone formation. Urology 60(5):911
Dietrick DD, Issa MM, Kabalin JN, Bassett JB (1992) Intravesical migration of intrauterine device. J Urol 147(1):132–134
Schoenfeld A, Pardo J, Engelstein D, Ovadia J, Servadio C (1991) Bladder perforation by an intrauterine device. J Clin Ultrasound JCU 19(3):175–177
El-Diasty TA, Shokeir AA, El-Gharib MS, Sherif LS, Shamaa MA (1993) Bladder stone: a complication of intravesical migration of Lippes loop. Scand J Urol Nephrol 27(2):279–80
McNamara M, Kennan N, Buckley AR (1985) Copper-7 perforation of the uterus and urinary bladder with calculus formation–sonographic demonstration. Br J Radiol 58(690):558–559
Güvel S, Tekin MI, Kilinç F, Peskircioglu L, Ozkardeş H (2001) Bladder stones around a migrated and missed intrauterine contraceptive device. Int J Urol Off J Japanese Urol Assoc 8(2):78–79
Harrison-Woolrych M, Ashton J, Coulter DJC (2003) Uterine perforation on intrauterine device insertion: is the incidence higher than previously reported? Science 67(1):53–6
Chamary VJB (1995) An unusual cause of iatrogenic bladder stone. Science 76(1):116
Eckford S, Persad R, Brewster S, Gingell JJB (1992) Intravesical foreign bodies: five-year review. Science 69(1):41–5
Ozgür A, Sişmanoğlu A, Yazici C, Coşar E, Tezen D, Ilker Y (2004) Intravesical stone formation on intrauterine contraceptive device. Int Urol Nephrol 36(3):345–348
Singh MM (1995) IUDs and transmigration–putting an old concern to rest. IPPF Med Bull 29(1):2–3
Akhtar OS, Rasool S, Nazir SSJC (2021) Migrated intravesical intrauterine contraceptive devices: a case series and a suggested algorithm for management. Science 13(1):689
Acknowledgements
Not applicable
Funding
The authors didn't receive any kind of funding.
Author information
Authors and Affiliations
Contributions
SM, RN and AQ contributed to the data collection and manuscript writing, and literature review. AY and MS did the literature review. All authors revised and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The patient's data was used anonymously, so approval from ethics committee was waived.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Competing interests
We obtained written informed consent from the patient to use clinical images and data anonymously for publication.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Muhammad, S., Yousaf, A., Shah, M.T. et al. Giant vesical calculus associated with migrant IUCD: a case report. Afr J Urol 27, 142 (2021). https://doi.org/10.1186/s12301-021-00245-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12301-021-00245-8