
Abstract
Oncologic patients are subjected to four major treatment types: surgery, radiotherapy, chemotherapy, and immunotherapy. All nonsurgical forms of cancer management are known to potentially violate the structural and functional integrity of the cardiovascular system. The prevalence and severity of cardiotoxicity and vascular abnormalities led to the emergence of a clinical subdiscipline, called cardiooncology. This relatively new, but rapidly expanding area of knowledge, primarily focuses on clinical observations linking the adverse effects of cancer therapy with deteriorated quality of life of cancer survivors and their increased morbidity and mortality. Cellular and molecular determinants of these relations are far less understood, mainly because of several unsolved paths and contradicting findings in the literature. In this article, we provide a comprehensive view of the cellular and molecular etiology of cardiooncology. We pay particular attention to various intracellular processes that arise in cardiomyocytes, vascular endothelial cells, and smooth muscle cells treated in experimentally-controlled conditions in vitro and in vivo with ionizing radiation and drugs representing diverse modes of anti-cancer activity.
Similar content being viewed by others
Introduction, or a few words about cardiooncology
The improved and still expanding diagnostic capabilities translating to earlier detection, along with the steadily increasing effectiveness of therapeutic approaches, luckily contribute to the growing population of people who successfully deal with cancer [1]. The therapy, often very forcible and life-threatening, leaves its imprint in cancer survivors in the form of temporary side-effects and/or long-term sustained abnormalities in many organs and tissues [2, 3]. One of the most affected systems by therapy is the cardiovascular system (CVS) [4]. Adult patients who survived cancer are more prone to develop cardiovascular disease (CVD) than representatives of the general population [5]. Indeed, CVD belongs to the leading causes of morbidity and mortality in cancer survivors [6,7,8]. Cardio- and vasotoxicity in oncology patients is so widespread that a new clinical subdiscipline, cardiooncology, has dynamically emerged [4, 9].
At the moment, cardiooncology is a rapidly developing area of science, but purely clinical observations primarily drive this development. However, the pathological phenomena seen in the CVS in patients with cancer have their basis in pathophysiological processes occurring at the cellular and molecular levels. In our opinion, this aspect of cardiooncology is not sufficiently harmonized on a cause-and-effect basis with clinical observations, resulting in an excessive separation of clinical observations from basic research. Therefore, in this article we confront cardiooncology observed from a patient-oriented perspective, with results of experimental studies that allow gathering the causes and effects of specific dysfunctions into a coherent whole.
Cardiovascular complications in patients with cancer
The CVS disorders that occur in oncology patients undergoing radio- and chemotherapy are driven by a broad range of morphological and functional disturbances within the heart muscle and blood vessels, generally leading to heart failure (HF). Radiation-induced heart disease (RIHD) is the most frequent malfunction that develops in patients experiencing ionizing radiation (IR). The disorder is manifested by a wide range of clinical symptoms, including pericarditis, coronary artery disease, myocardial defects, and inappropriate conduction [10]. Cardiac fibrosis is the most prominent structural defect that is a consequence of both irradiation and chemotherapy, leading to arrhythmia, usually several years after treatment [11]. The functional abnormalities within CVS are far more extensive. They include myocardial dysfunction, myocardial ischemia, valvular heart disease, pericarditis, defective conduction, and arrhythmias. In addition, patients may suffer from some perturbations within systemic and pulmonary blood vessels, including thromboembolic disease, and pulmonary and arterial hypertension. Some of the treatments may also cause more complex perturbations with a strong metabolic component in a long-term perspective, such as: obesity, hyperlipidemia, atherosclerosis, and diabetes [9, 12, 13]. Importantly, therapy-induced cardiotoxicity gives the adverse symptoms that are not limited to resting CVS parameters (e.g., left ventricular ejection fraction). They also engage dynamic cardiac functions, whose deterioration jeopardizes daily quality of cancer survivors’ life, i.a. by interfering with the peak (VO2peak) oxygen consumption and translating to reduced exercise tolerance [14].
The incidence of iatrogenic complications is randomly distributed, depending on the treatment regimen and patient-specific conditions. Their frequency ranges from a few percent to tens of percent of individuals [13]. Cardiologic side-effects of cancer therapy exist in patients with various malignancies, treated with IR and drugs representing multiple groups and modes of action. The most recognized in this area are anthracyclines, platins, taxanes, antimetabolites, proteasome inhibitors, anti-HER2 agents, and immune checkpoint inhibitors [13, 15]. Basic characteristics of radiotherapy and drugs affecting CVS and the most commonly observed therapy-related complications are collected in Table 1.
Mechanistically, the cardiologic disorders that develop in cancer survivors have cellular and molecular determinants. The most important include cellular energetics, electrophysiology, growth and differentiation, proteostasis, senescence, regulation of gene expression (methylation, microRNAs), DNA damage, oxidative stress, inflammation, and cell death (apoptosis, ferroptosis, autophagy, mitophagy). Various mutually interacting signaling pathways control these events at the upstream and downstream levels, and cellular transcriptome and proteome alterations trigger their changes. Because the above-mentioned effectory mechanisms of CVS dysfunction have their specific topography within the heart and blood vessels, their appearance upon radiation and drug exposure will be described and discussed from the perspective of three major cell types forming these multicellular organs and working in concert for the right heart and vessel activity. These will be cardiomyocytes, comprising ~ 80% of the cellular heart volume and responsible for its electro-mechanical activity [16], and endothelial cells and smooth muscle cells that interact, creating heart vascularization and controlling peripheral blood vessel organization and function [17].
Mechanisms of IR-dependent cardiotoxicity and vasotoxicity
Currently, radiotherapy employing gamma and X-rays is applied for about half of all malignancies, and for some, it is the primary treatment modality [18, 19]. At the same time, the molecular background of RIHD that may occur from months to decades following exposure to either oncologically effective doses of IR or low doses of radiation resulting from occupational contacts [20,21,22] is still not sufficiently understood (Fig. 1).

Pathomechanisms of IR-dependent cardio- and vasotoxicity in cardiomyocytes (A), vascular endothelial cells (B), and vascular smooth muscle cells (C). AC acetylation, Me methylation, SM sphingomyelin, OONO− peroxynitrite, aSMase acid sphingomyelinase, PIP3 phosphatidylinositol (3,4,5)-trisphosphate, PLC phospholipase C, DAG diacylglycerol, IP3 inositol 1,4,5-trisphosphate, IP3-R inositol 1,4,5-trisphosphate receptor
Cardiomyocytes
Considering the role of cardiac muscle cells in electrophysiological heart activity, it is more than plausible that IR seriously violates their biology. Experiments on human-induced pluripotent stem cell-derived cardiomyocytes (hiPSC-CMs), a model resembling primary cardiomyocytes [23], allowed for the determination of the radiation doses (5 and 10 Gy) and exposure times [120], reducing cell viability. The cells remained alive when the treatment lasted shorter (e.g., 48 h) or the dose was lower (< 5 Gy). The irradiation performed within dose and time frames, ensuring unaltered viability, revealed that the spontaneous pacemaker activity of the cells was also unaffected. This situation has changed and the beating frequency declined when the hiPSC-CMs were subjected to higher doses of radiation for at least 48 h [24]. Interestingly, cardiomyocyte response to IR was not uniform, because some cells seemed more sensitive to the stressor [24]. This effect was probably associated with the spatial distribution of the cells subjected to IR and their contribution to the formation of the pacemaker center. This random responsiveness of cardiomyocytes to radiation could explain, at least partly, a broad and nonspecific population distribution of arrhythmia [25] and its relatively low frequency (~ 4–5%) among other CVS disorders in IR-treated patients with cancer [26]. Another issue that has to be solved is whether IR doses identified as reducing cardiomyocyte viability translate to in vivo conditions, e.g., in the context of tolerance doses (40 Gy) [27]. However, a trend regarding irradiation doses with potentially cardiotoxic outcomes is recently decreasing and points to the value of 15 Gy as the threshold [28].
The heart muscle loses contractile cells during a lifetime and in response to various challenges. At the same time, the organ has minimal capacity to regenerate because of the postmitotic state of most adult cardiomyocytes [29]. Some hopes regarding improving heart regeneration are associated with the cardiogenic reprogramming of pluripotent stem cells [30]. The radiation issue is thus of particular importance, considering the potential risk of tumorigenesis after stem cell implantation. Unfortunately, the data on the sensitivity of differentiated hiPSC-CMs and their pluripotent precursors are inconclusive. For example, the pluripotent cells giving rise to hiPSC-CMs are more resistant to IR (utilized at cGy doses) than the differentiated cells, as their viability and proliferation were unchanged conversely to the insufficient number of functional, autonomously beating cells [31]. Other authors, also working with irradiated hiPSC-CMs demonstrated that their proliferative capacity does not differ from that characterizing untreated cells, and the same applies to the incidence of apoptosis. At the same time, they postulate that irradiation eliminates highly proliferative pluripotent stem cells that are more sensitive to this stressor. To strengthen this thesis, they employed NOG mice and showed that tumor formation was less frequent in the irradiated than in the unirradiated group, which could be associated with IR-dependent reduction of the number of undifferentiated hiPSC [32], likely due to induction of their apoptotic death [33]. One may not exclude that these discrepancies in IR sensitivity of immature stem cells and differentiated cardiomyocytes may result from experimentally tested doses of radiation. The report showing unaltered proliferation and apoptosis of hiPSC-CMs with a concomitant deterioration of stem cells is based on markedly higher IR dosage (2–8 Gy) than the study demonstrating the opposite findings [31, 32].
Regarding the electrophysiological activity of cardiomyocytes, the irradiated cells display increased predilection to spontaneous release of Ca2+ upon the β-adrenergic stimulation by isoproterenol. This effect may explain, at least to some extent, the proarrhythmic tendency of the heart under adrenergic stress [34]. Further dedicated studies in this respect are, however, needed because the intensity of IR-related Ca2+ waves in cardiomyocytes may depend on the time of exposure. The amplitude of Ca2+ transient increases in the short-term perspective, whereas the prolonged trend (1 week) decreases, corresponding with reduced left ventricular contractility in anesthetized mice. This effect may be probably related to chronically reduced sarcoplasmic reticulum (SR) calcium content [35]. Another issue is that the contractile activity of IR-treated cardiomyocytes is determined not only by Ca2+ level. The cells responded dose-dependently to IR, also by increasing Na+ content, which resulted in Na+-dependent Ca2+ overloading through the Na+/Ca2+ exchanger (NCX) [35].
Adrenergic stimulation of the heart leads to Ca2+ overload and oxidative stress [36]. The role of oxidative stress, understood as the disproportion between the generation and removal of reactive oxygen species (ROS) leading to macromolecular damage [37], in CVS dysfunction is indisputable [38]. Discoveries convincingly connect this phenomenon with cardiovascular challenges seen in oncologic patients undergoing various forms of therapy [39]. Although the list of oxidative stress culprits is long, IR is among the most prominent external causes [40]. A hit of 137Cs γ rays induces the production of ~ 60 ROS/ng of tissue in less than one microsecond [41]. When cardiomyocytes are exposed to even low doses of IR (10 cGy) for 12 days, they exhibit an upregulated expression of transcripts for mitochondrially encoded cytochrome b and 12S ribosomal RNA. Because these transcripts are engaged in electron transport [42] and mitochondrial protein biogenesis [43], the above finding implies that IR intensifies mitochondrial metabolism. These changes may also exemplify a compensatory cell response to restore ATP content that could deteriorate due to IR-related mitochondrial oxidative phosphorylation system failure [31, 44]. The theory of IR-dependent intensification of cellular metabolism followed by ATP depletion was proved by another group of scientists who found an increased expression of some energetic proteins, like fatty acid synthase and solute carrier family 25 member 1 in irradiated mouse hearts. At the same time, the tissues displayed injured mitochondrial inner membranes, decreased ATP content, and accumulated lactic acid [45]. Changes in the cardiomyocyte mitochondrial structure belong, in fact, to the oldest observation of IR-related cellular damage. In 1968, it was described that high doses of radiation (52 Gy) seriously affect the mitochondria architecture, exemplified by their swelling, abnormalities within the cristae, and bonded outer double membranes [46].
Following the trait of increased mitochondrial metabolism, one may anticipate that the production of ROS, treated as by-products of respiratory chain reactions, should also be elevated [47]. This general assumption agrees with experiments using isolated ventricular mouse cardiomyocytes, which overproduced ROS upon irradiation [35]. These elevated ROS could be another factor responsible for altered cardiac Ca2+ handling, particularly its efflux from SR [48]. This statement is based on the observation that electrophysiological effects of IR-dependent oxidative stress (e.g., the diminished systolic Ca2+ transients) were reversible by antioxidants. IR-dependent oxidative stress in cardiomyocytes was mediated by Ca2+/calmodulin-dependent protein kinase II (CaMKII). The activity of this kinase was persistently upregulated after irradiation and correlated with hyperphosphorylation of its targets, RyR2 and PLB [35].
ROS-dependent changes in the mechanical action of the heart are not the only consequences of IR. Decreased viability of irradiated cardiomyocytes may be underlined by excessive DNA injury, leading to apoptosis. Such a sequence of events was observed, e.g., in rat embryonic ventricular H9C2 cardiomyocytes, whose treatment with IR (at 2, 5, 10, and 15 Gy) resulted in a dose-dependent increase in the percentage of apoptotic cells. An upregulated level of proapoptotic protein Bax and a downregulated level of anti-apoptotic protein Bcl-2 accompanied this effect. The augmentation of apoptosis coincided with a dose-dependent induction of ROS and accumulation of DNA damage foci (γ-H2A.X) [49]. The vulnerability of the tested cells to IR may also result from decreased phosphorylation of Akt [49], a multiplayer kinase involved e.g., in the maintenance of the respiratory status of mitochondria, decreasing ROS efflux, and cell self-repair [50]. The activity of PI3K/Akt pathway, cooperating with HER2 signaling, has also been found to be essential for controlling the appropriate functioning of the heart, including the survival of cardiomyocytes [51].
However, IR-dependent apoptosis of cardiomyocytes should be treated with caution because its induction, also reported by other groups [52], seems to not be a universal phenomenon. Moreover, although an increased frequency of apoptosis was found under in vitro cell culture conditions, this outcome was not confirmed by the same group in vivo [49], which may indicate that the cellular model is more sensitive to radiation than tissue structures. Moreover, in the in vivo conditions, the irradiated cardiomyocytes may die due to direct exposure to IR and indirectly due to a reduced vessel density contributing to the formation of ischemic areas [52]. In turn, cardiomyocytes that survived the direct and indirect radiation became hypertrophic to compensate for previous cell loss [52]. Another consequence of this heart remodeling is the accumulation of fibrous tissue, leading to the next and the most critical morphological sign of RIHD, fibrosis [53]. The profibrotic changes observed in the irradiated hearts may be partly associated with the overproduction of transforming growth factor-β1 (TGF-β1) [52, 54], which is one of the key mediators of extracellular matrix (ECM) protein (e.g., collagen) deposition and the loss of tissue elasticity [55].
The phosphorylated variant of histone H2A.X, the γ-H2A.X, is the marker of DNA double-strand breaks involved in the DNA damage response (DDR) reaction. The accumulation of γ-H2A.X foci assembling to injured DNA is a sign of cellular senescence [56]. This phenomenon represents an irreversible cell growth cessation caused by excessive and irreparable DNA damage [57]. Senescent cells accumulate in vivo with age and participate in several pathological processes like chronic inflammation, tissue fibrosis, and cancer [58]. The harmful activity of senescent cells proceeds mainly via their ability to hypersecrete various proinflammatory and ECM remodeling proteins to the environment, known as the senescence-associated secretory phenotype (SASP) [59]. The observation of the γ-H2A.X induction in the irradiated H9C2 cardiomyocytes [49] was positively verified and additionally strengthened by the demonstration of the presence of other senescence indices in these cells. These included an elevated expression of senescence-associated β-galactosidase (SA-β-Gal), upregulated levels of cell cycle inhibitory proteins p16 and p21, and increased expression of transcripts coding for some SASP factors, like IL-6, CCL-2, MMP-2, Col3a1, and CTGF in the irradiated H9C2 cells. Significantly, these cellular changes corresponded to the formation of senescence phenotype in the heart tissue in vivo, in which IR treatment resulted in the telomere shortening and even more excessive SASP formation [60].
IR-induced cardiomyocyte senescence may be associated with lysine acetylation, one of the most critical post-translational protein modifications [61]. Previously, transient lysine acetylation was found to play a regulatory role in cardiological abnormalities like arrhythmia, HF, and hypertension [62]. The hearts of irradiated animals and irradiated cardiomyocytes displayed upregulated lysine residue acetylation level. Nearly half of the hyperacetylated proteins were localized within the mitochondria. Differentially expressed proteins in the acetylation sites were grouped mainly in energy production and conversion, fatty acid and amino acid transport, and utilization phenomena. One of the hyperacetylated targets, Atp5f1c (the lysine 55 site), which is closely related to cell energetics as an element of an ATP synthase complex [63], appeared to be causatively connected with the development of IR-driven senescence phenotype in H9C2 cells. Hypothetically, it could also contribute to fibrotic changes in the heart muscle in vivo [60].
Endothelial cells
Vascular dysfunction is one of the most common complications of radiotherapy [64]. Retrospective, histopathological examination of patients with rectal cancer subjected to preoperative irradiations revealed numerous signs of vasotoxicity, including vascular dystrophy and hypertrophy, vascular and perivascular fibrosis, and intimal hyperplasia connected with luminal narrowing. The vessels were also characterized by increased collagen I and III content [65]. Echocardiographic analysis of irradiated mouse hearts showed a diminished intramyocardial vessel-to-cardiomyocyte ratio in the left ventricle, which is suggestive of retrograde vascular lesions within the cardiac muscle [52]. Irradiated pig coronary arteries revealed, in turn, the presence of perivascular adhesions, vessel enlargement, a thickened adventitia, adventitial neovascularization, and medial necrosis [66]. The damage that develops within the cardiomyocytes in response to IR (discussed in the previous section) is also associated with cell ischemia [67] triggered by injured cardiac nutrient-supplying vessels, i.a. due to apoptosis of endothelial cells [68].
Considering the prominent role of endothelial cells (ECs) in vascular functioning, the above-mentioned morphological disturbances within blood vessels are most likely determined by certain disturbances in EC structure and function. As per the former, scanning electron microscopy revealed that ECs in the irradiated arteries form an intact layer of cells that display a hypertrophic appearance [66]. One of the possible reasons for cellular hypertrophy, usually caused by impaired proteostasis [69], is cellular senescence [70]. Indeed, ECs display several features of senescence phenotype after irradiation with moderate-to-high doses of radiation in vitro [71,72,73]. Irradiated (4 Gy) human umbilical vein endothelial cells (HUVECs) are characterized by a hypertrophic and flattened shape, depressed proliferation, and increased expression of SA-β-Gal, p16, and p21 proteins. Moreover, they display decreased phosphorylation of retinoblastoma protein (pRb) and the activation of DDR, represented by accumulated γ-H2A.X foci and activated protein kinase ataxia telangiectasia mutated (ATM), Chek2, and p53 [72]. A similar EC phenotype was also seen after the in vivo irradiation of experimental animals [74, 75]. A simultaneous upregulation of p16 and p21 in the irradiated, senescent ECs [72, 76] implies that both telomere-dependent [77] and telomere-independent [78] types of senescence machinery are involved. However, the activation of DDR is not required to maintain a senescent state, as rat cerebromicrovascular ECs remained senescent despite near total repair of injured DNA [79]. In turn, the signaling involving activated p53 appeared to be critical for IR-dependent senescence of human lung microvascular ECs (HLMVECs) [76].
The remaining effectory pathways associated with IR-dependent EC senescence are numerous and seem to define the type of investigated cells. Irradiated senescent HUVECs exhibit increased expression of mRNA and production of protein for insulin-like growth factor binding protein 5 (IGFBP5), recognized in the knockdown interventions as the contributing agent in their diminished proliferation, activated SA-β-Gal, and impaired tube formation ability [72]. In pulmonary microvascular endothelium, which displays the morphology as the IR-treated HUVECs, the senescence response that approached after their irradiation was elicited by an X-linked inhibitor of apoptosis-associated factor 1 (XAF1).
The XAF1 is transcriptionally regulated by bromodomain 7 (BRD7), the expression of which increases at both mRNA and protein levels in response to IR, and the downregulation of which leads to a partial reversal of senescence [80]. Studies on human pulmonary artery ECs (HPAEC) showed, in turn, that IR applied at the dose of 10 Gy induced their premature senescence in a mechanism involving a phosphatidylinositol-3-kinase (PI3K) and mammalian target of rapamycin (mTOR) signaling. The involvement of the mTOR pathway was associated with the overproduction of insulin-like growth factor-1 (IGF-1) and hyperphosphorylation of IGF-1 receptor (IGF-1R), the activity of which is upstream of mTOR [73].
Functionally, senescent HUVECs display decreased angiogenic reactions, manifested by deteriorated ability to form capillaries on Matrigel™. This feature was surprising, considering their increased migratory potential, causatively linked with overexpressed matrix metalloproteinase 2 (MMP-2) [72]. The issue of IR-dependent changes in EC motility needs to be further explored, also in the context of findings by other groups who observed that HUVEC irradiation using doses up to 8 Gy led to a depression of their migration, invasion, and the ability to form capillaries [71].
Functional perturbations associated with IR-related toxicity and/or EC senescence are primarily related to the pathogenesis of atherosclerosis. A pathomorphological examination of atherosclerotic arteries indicated the presence of senescent cells in vivo, whereas eliminating these cells decelerated the disease progression [81,82,83]. In this context, the ambiguous role of nitric oxide (NO), the central smooth muscle relaxant [84], is especially intriguing. Classically, senescent ECs are characterized by decreased activity of endothelial nitric oxide synthase (eNOS), leading to NO’s declined generation [85, 86]. Experimental data suggest that NO deficits may causatively participate in EC senescence, as the augmentation of this molecule level appears to inhibit the process. Because this effect coincided with the delayed senescence-associated deterioration of telomerase activity, one may assume that the antisenescence activity of NO was associated with the restoration of telomeric DNA [87]. Analogical findings were derived from the study in which HUVEC transfection with eNOS or their treatment with NO donor reduced the fraction of SA-β-Gal-positive cells. The antisenescence activity of NO was attributed to its antioxidative properties, particularly the ability to neutralize ROS overproduced during EC senescence [81]. The perception of NO function in EC senescence changes radically when IR induces the process. In such conditions, the eNOS-NO axis seems integral to radiation-induced DDR and to the “bad guy” during EC senescence. It has been found that IR induced the eNOS and NO dose-dependently, leading to increased cell migration and sprouting, which corresponded with increased tumor angiogenesis in vivo [88]. IR-treated bovine aortic EC displayed increased eNOS transcription and NO production, and these effects were regulated by upregulated DNA damage-sensing ATM [89]. The same kinase along with heat shock protein 90 (HSP90), also operating within the DDR [90], was also found to be responsible for the phosphorylation of serine 1179 of eNOS, another important step of the enzyme activation [91]. The HUVEC irradiation (< 20 Gy) also led to increased eNOS phosphorylation at Ser-1177 and dephosphorylation at Thr-495, and these events were mediated by increased activity of protein kinase C-βII (PKC-βII) [92]. As a consequence of radiation-induced NO, the cells exhibited decreased cell death incidence and intensified senescence [89]. At the same time, their exposure to N-nitro-l-arginine methyl ester (l-NAME), the NO inhibitor, prevented senescence development after the IR challenge [93]. As per the possible sequence of events staying behind the IR-induced eNOS activity and NO release, activated ATM translocates to the cytosol to stimulate its down-stream effectors, such as NF-κB [94], mTORC1 [95], and p38 MAPK [96]. Therefore, this is the right place to conclude that although NO overproduction, in general, is regarded as a favorable phenomenon from the point of view of CVS function, its excess resulting from cell irradiation should instead be considered as an adverse effect. This prediction was confirmed in several animal models in which uncoupling of NOS and exacerbated mitochondrial ROS generation led to dilatory remodeling and cardiac dysfunction [97]. And conversely, the loss of inducible NOS (iNOS) diminished cardiac remodeling and improved cardiac reserve, postmyocardial infarction [98]. One cannot exclude that these adverse outcomes of NO activity may occur because this molecule may subtly react with mitochondrial superoxides leading to the formation of the highly active and deleterious peroxynitrite [99].
Another aspect of the IR-dependent contribution of senescent EC to atherosclerosis, particularly at its early stage, is monocyte recruitment into the blood vessel wall [100]. The presence of hypertrophic endothelium within atherosclerotic lesions has a long history dating back to when this phenomenon was not linked with senescence phenotype [101, 102]. Human coronary artery ECs irradiated with 10 Gy adopted an enlarged SA-β-Gal-positive appearance and displayed an increased capacity to bind monocytes. The adhesion-promoting activity of senescent ECs was associated with upregulated CD44, allowing them to form monocyte clusters on the surface of senescent cells. This receptor’s role in atherosclerosis pathogenesis was previously established in vivo as the incidence of atherosclerotic lesions in CD44 null animals and was markedly reduced [103]. Increased expression of CD44 in senescent ECs, which another group also reported in irradiated senescent HUVECs [72], was in turn regulated by radiation-dependent demethylation of its promoter CpGs at positions −638 (CpG1), −627 (CpG2), and −607 (CpG3). Of them, the CpG3, whose hypomethylation was the greatest [100], has previously been linked with the activation of the CD44 promoter [104]. It is worth noting that DNA methylation is a potent epigenetic regulator responsible for transcriptional gene silencing. An overall decline in DNA methylation is a well-established feature of senescent cells, contributing to decreased transcription of either immune response genes (CpG sites) or SASP-related genes (non-CpG islands) [105]. The concept of epigenetic regulation of increased monocyte adhesion to senescent ECs is in line with other studies of the same phenomenon, in which the pro-adhesive capacity of cells was linked with an overproduced VCAM-1. Significantly, the VCAM-1 gene promoter was characterized by the open chromatin state due to increased methylation of histone H3 on lysine 4 (H3K4me3), which allowed for its increased accessibility and the transcriptional activity of NF-κB [106].
Another regulatory role regarding gene expression plays short, non-coding RNA molecules (microRNAs/miRNAs) that generally affect this process as its repressors [107]. Experimental overexpression of some miRNAs were found to ameliorate oxidative stress in cardiac cells, serving as potential therapeutic targets in the course of cardiomyopathy [108]. It was demonstrated that IR (2 Gy) modulates miRNA levels in human dermal microvascular endothelial cells (HDMECs). The upregulated targets included let-7 g, miR-16, miR-20a, miR-21, and miR-29c, whereas the expression of miR-18a, miR-125a, miR-127, miR-148b, miR-189, and miR-503 was decreased. The observed changes were biologically valid, as those regarding let-7 g, miR-189, and miR-20a corresponded with cell survival and proliferation, those associated with miR-125a and miR-189 were responsible for radioprotection, whereas those linked with miR-127 and let-7 g contributed to increased radiosensitivity [109].
The pathogenesis of radiation-induced CVS disorders has a strong inflammatory component [110], which is associated to a large extent with cellular senescence potentiating extracellular inflammation due to the development of SASP. For example, microvascular HMVEC-L cells that senesced upon IR exposure displayed increased production of IL-8 [76], whereas HUVECs hyperexpressed mRNA for IL-6 [71]. One of the very first events that underlie inflammation-based cardio- and vasotoxicity is the activation of nuclear factor κB (NF-κB), a molecule prone to be activated in ECs in response to genotoxic action of IR [71, 111] and playing the central role for the SASP development [112]. In vascular endothelium, ROS, DNA injury, and damage-associated molecular patterns (DAMPs) released by injured cells activate NF-κB. Following NF-κB activation and nuclear translocation, the irradiated ECs overproduce and/or hypersecrete an extensive repertoire of proinflammatory agents, including IFNγ, TNFα, TGF-β, IL-1, IL-6, CCL2, CXCL8, ICAM-1, VCAM-1, and E-selectin [113]. Interestingly, the NF-κB-dependent signaling is also crucial for IR-driven EC senescence itself, as the chemical blockade of its essential modulator (NEMO) inhibited the formation of senescence phenotype in the irradiated cells [71].
DAMPs released from breast cancer cells dying after their irradiation (20 Gy) directly promote the recruitment of neutrophils and monocytes in vivo. Significantly, the DAMPs, particularly HSP70, HMGB1, and S100A8/A9, also activate HUVECs through toll-like receptor 4 (TLR4) and/or the TLR2/TLR4 dimer. Upon stimulation, ECs overexpress a variety of surface adhesion molecules (ICAM-1, E-selectin), cytokines, and chemokines (IL-1β, IL-6, CCL2, CXCL1, CXCL8, CXCL2, CCL7) that act as leukocyte chemoattractants [114]. Apart from the activation of NF-κB, DAMPs-related proinflammatory switch also engages other signaling routes, such as mitogen-activated protein kinase (MAPK) and interferon regulatory factor 3 (IRF3) [115, 116]. The irradiation also induces high-mobility group protein-1 (HMGB1) [117], a mediator stimulating human microvascular ECs to produce ICAM-1 and VCAM-1. Moreover, IR-treated ECs display elevated levels of receptors for advanced glycation end products (RAGE), TNFα, PAI-1, and tPA [116].
Another possible cause of a sterile inflammation typical for atherosclerosis is oxidative stress [118], a well-recognized consequence of EC exposure to radiation. Irradiated (15 Gy) microvascular HMVEC-L cells generate increased amounts of mitochondrial ROS, exhibit reduced respiratory complex II activity, and increased superoxide dismutase 2 (SOD2) and glutathione peroxidase 1 (GPX1) expression levels [76]. The causative action of the IR-related oxidative stress confirmed experiments with MnTBAP, the SOD mimetic, the administration of which allowed inhibiting the development of senescence phenotype to a large extent [76]. As per the reasons for mitochondrial dysfunction leading to oxidative stress in irradiated ECs, increased activity of NADPH oxidase plays a role. Brain microvascular ECs subjected to IR undergo oxidative stress accompanied by increased inflammatory indices (NF-κB, ICAM-1), and this phenotype was abolished by pharmacologic and genetic inhibition of the enzyme [119]. NF-κB is, in fact, one of the ROS’s central signaling targets, which exacerbates the inflammation in a self-stimulatory manner [120]. ROS, whose production increased in the irradiated HUVECs, were also engaged in the reported radiation-induced changes in eNOS phosphorylation [92]. It is very plausible that IR-related changes in oxidative EC status largely depend on altered mitochondrial metabolism. Experiments on human telomerase-immortalized coronary artery ECs (TICAE) showed that their irradiation leads to structural disorganization of mitochondria (swelling, cristae disruption), accompanied by lowered basal respiration and ATP synthesis, without changes in mitochondrial oxidative phosphorylation system (OXPHOS) capacity [121]. In contrast to previously cited reports, TICAE irradiation did not result in increased ROS efflux, which may be associated with a relatively low dose of IR (2 Gy) and the fact that telomerase may modulate mitochondria metabolism, counteracting the excessive ROS production [122].
The development of cellular senescence is an alternative cell fate to apoptotic cell death, as the senescent cells are usually resistant to proapoptotic stimuli [123]. As per an interplay between these two processes in irradiated ECs, the final response depends on the strength of the insult. Apoptosis is the primary response to relatively high doses of IR (higher than 10 Gy). It proceeds through the acidic sphingomyelinase-dependent processing of sphingomyelin, leading to the accumulation of ceramide and the upregulation of Bax and Bak proteins [124, 125]. It is hypothesized that the ceramide-dependent mechanism of apoptosis in IR-treated ECs is associated with the exceptionally high activity of this enzyme in comparison with other cell types [126]. At the same time, when irradiation occurs at lower doses, that is between 0.5 and 10 Gy, the development of senescence phenotype is the main reaction [71, 72]. However, this dose-dependency is sometimes obliterated, which may be related to the origin of ECs and the detailed methodological aspects of their experimental irradiation, like culture density and exposure time. Moreover, in some experimental models, like human or bovine pulmonary artery ECs, apoptosis was not detected below a threshold of 30–50 Gy [127]. Above these doses, the apoptosis occurred in a mechanism involving activation of endoplasmic reticulum (ER) stress response and an elevation of the transcription factor X-box binding protein 1 (XBP1) and its downstream target, glucose-regulated protein 78,000 (GRP78), serving as an ER chaperone [127]. Another player in the radiation-dependent apoptosis of ECs is protein kinase C (PKC), which acts as the negative regulator of this process by negating sphingomyelin processing to ceramide [124].
Vascular smooth muscle cells
CVS malfunction triggered by IR exposure largely results from changes in vascular smooth muscle cells (SMCs). Regarding CVS disorders’ etiology, vascular SMCs are of particular importance for the development of atherosclerosis [128]. Atherosclerotic plaque SMCs originate from a fraction of mature medial cells that are clonally replicated to settle the lesion [129, 130]. The activity of SMCs that are localized within the plaque depends on the phenotypic transformations of these cells and may exert both positive and negative outcomes for plaque stability [131, 132]. Research on SMCs lineage tracing (Myh11-ERT2Cre YFP+) mice with experimentally-induced atherosclerosis revealed that IR promotes atherosclerotic plaque destabilization in a mechanism involving SMCs [133]. Animal exposure to high doses of radiation (1200 cGy) results in the loss of SMCs’ tendency to colonize atherosclerotic lesions with a concomitant increase in an intraplaque hemorrhage and necrotic core area and decreased collagen content. Mechanistically this effect was linked with the increased extent of DNA damage within SMCs, pointing at the same time to various susceptibilities of these cells to IR, depending on their primary localization. An extensive DNA injury did not translate to an increased incidence of apoptosis, which is in line with another report based on irradiated (1.25–20 Gy) rat aortic SMC [134]. However, increased apoptotic death was evident in human aortic SMCs subjected to IR (4, 8 Gy). It was causatively connected with the upregulation of NADPH oxidase (NOX), followed by a dose-dependent stimulation of ROS release. Another pathway responsible for cell death induction was the upregulation of C-reactive protein (CRP), leading to an increased ROS and apoptosis in IR-treated SMCs [135]. The CRP level correlates with the magnitude of inflammation, and its production increases after irradiation [136]. At the same time, the CRP may mediate SMCs apoptosis through NOX4-dependent overproduction of ROS [137] and induction of caspases [138]. In the case of irradiated SMCs, CRP assembles with AP-endonuclease/Redox factor-1 (APE/Ref-1), triggering apoptosis based on ROS-dependent disruption of mitochondrial metabolism and activation of p53. Simultaneously, the CRP-Ref1 complex causes transcriptional repression of STAT3, which opposes CRP-induced apoptosis in SMCs [135].
The mitotic activity of SMCs in vivo is small (~ 0.1%) [139], which determines their radioresistance. Another element strengthening the radioresistance is the ability of SMCs to repair DNA damage resulting from the even potentially lethal irradiation doses [140], in which the IR-dependent induction of Ref-1 may play some role [135]. The colonization of some atherosclerotic vessels is associated with the expansion of medial cells making this subset theoretically prone to IR. Such the hypothesis was proved by in vitro studies on cultured SMCs, which exhibited decreased proliferative capacity upon irradiation (1.25–20 Gy) [134, 141, 142] in a mechanism that may involve the induction of cell cycle inhibitors p21 and p53 [143] and the inhibition of growth-promoting STAT3 [135]. These abnormalities may translate to impaired cell reaction to injury, leading to atherosclerotic plaque expansion, restenosis, and vascular hypertrophy [144]. In addition, the irradiated cells displayed reduced contractility [141]. Its weakening was also found in a coculture system when SMCs were grown together with irradiated ECs [65]. In that case, SMCs developed a fibrogenic phenotype manifested by increased mRNA for α-smooth muscle actin (α-SMA), connective tissue growth factor (CTGF), plasminogen activator inhibitor 1 (PAI-1), and collagen III. Notably, developing these traits was not possible in the absence of irradiated ECs. Mechanistically, the formation of the profibrotic phenotype was mediated by the overproduction of TGF-β1 by the irradiated ECs and the subsequent activation of Smad3 signaling in the recipient SMCs [65].
Unfortunately, the literature data regarding radiation’s effects on vascular SMC contractility are conflicting. In contrast to studies showing defective SMCs’ contractility and their profibrotic phenotype, some reports indicate that irradiated animals are characterized by opposite vessel reactions manifested by increased systolic blood pressure [145]. This effect may be related to decreased EC-dependent vessel relaxation (discussed in the previous chapter) and/or increased SMC-dependent vessel contraction. Experiments on animals exposed to whole-body irradiation showed that the vasoconstrictive tendency may be associated with augmented PKC-dependent responsiveness of SMCs’ myofilaments to Ca2+. This effect occurs independently of ECs [146]. The PKC also inhibits large conductance Ca2+-activated K+ channels (BKCa), leading to a depression of an outward K+ current that may also, electrophysiologically, contribute to IR-dependent increase in vascular tone and related arterial hypertension [147]. Another group showed that irradiated (10, 20 Gy) SMCs migrate into 3D collagen matrix gels less efficiently, which was accompanied by a reversal of their secretory to contractile phenotype [148]. In the context of these divergent results, one cannot exclude the scenario that the most reliable results derive from animal models, where the SMC-dependent vascular response is associated with the presence of cells having contractile phenotype. In various artificially-created culture systems, this condition is not fully secured.
Experiments performed under controlled in vitro conditions clearly show that the ultimate response of SMCs to radiation is determined by the paracrine, EC-dependent bystander effect [149]. Apart from the earlier discussed adoption of fibrogenic phenotype, the role of neighboring endothelium also appeared to matter for SMCs motility. More precisely, when the SMCs were irradiated alone, the proliferation, as estimated according to the percentage of cells in the S phase of the cell cycle, clearly declined to confirm previously cited findings. Simultaneously, when the non-irradiated SMCs were cocultured with irradiated ECs, their growth capacity unexpectedly increased. Generally, the same happened in the case of SMC migration [65]. SMCs also proliferate more vigorously upon IR treatment in vitro. This observation agrees with examining tissues from patients with cancer undergoing radiotherapy in which SMCs in hypertrophic vessels displayed a higher PCNA index than those in normal tissues [65]. Although the behavior of SMCs undergoing radiation seems to depend strictly on the presence and irradiation of ECs that coexist in blood vessels in vivo, their ultimate reaction is also associated with the IR dose. Namely, when the ECs were subjected to markedly higher radiation (40 Gy), they failed to promote the proliferation of SMCs [150]. Another issue is that SMCs differ in their responsiveness to IR depending on their origin. It was shown in experiments on human aortic and venous SMCs where the latter were less susceptible to radiation (1–50 Gy). However, in both cases, the proliferation upon IR exposure was decreased [151].
Mechanisms of drug-induced cardiotoxicity and vasotoxicity
Ionizing radiation was the first but not the sole cause of CVS disorders that develop iatrogenically in patients with cancer. Indeed, a much more significant problem and challenge is the cardio- and vasotoxicity induced by the action of various groups of drugs used in oncology, the therapeutic use of which is far broader than irradiation. Cardiac complications in a particular group of high-risk patients are also associated with synergism in the effects of drugs and radiation, as reflected e.g., in the guidelines of the American Society of Clinical Oncology (ASCO) [4].
Anthracyclines
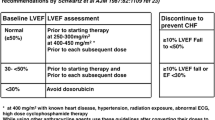
Clinical observations indicate that anthracyclines predispose oncologic patients to the largest extent to the occurrence of cardiotoxicity that affects their life quality and expectancy, irrespective of oncologic prognosis [152]. Predicting the risk of anthracycline-associated disorders is seriously jeopardized by explicit intraindividual variations in the tolerance of high doses of the drugs, which act dose-dependently [153, 154]. In some individuals, cardiologic adverse effects may occur at a cumulative dose of anthracyclines corresponding to 300 mg/m2 or lower. In contrast, other patients have no abnormalities, despite being exposed to doses up to 1000 mg/m2 [155]. Population studies showed that anthracycline‐induced cardiotoxicity (ACT) arising as asymptomatic cardiac dysfunction may affect as much as 57% of patients [156]. Restrictive or dilated cardiomyopathy may occur in up to 16% of cases [157]. Patients who received doxorubicin ≥ 250 mg/m2 or epirubicin ≥ 600 mg/m2, respectively, are defined by the ASCO as those who require intensified cardiomonitoring because of the high risk of developing ACT [4]. Survivors of childhood malignancies subjected to both anthracyclines and radiotherapy are at exceptionally high risk of cardiotoxicity. These patients may experience cardiac events at an early age, and HF may develop in 12.5% of them within 30 years after therapy [158]. In recent years, genetic testing enriching a standard echocardiogram monitoring was proposed to better discriminate between patients with high and low risk of ACT [159]. Proposed cellular pathomechanisms of anthracycline-based cardiotoxicity are depicted in Fig. 2.

Pathomechanisms of anthracycline-dependent cardio- and vasotoxicity in cardiomyocytes (A), vascular endothelial cells (B), and vascular smooth muscle cells (C). ER endoplasmic reticulum, SR sarcoplasmic reticulum, α1AR α1A-adrenoceptor, CLOCK Clock gene
Cardiomyocytes
Cardiomyopathy is a notorious heart abnormality observed in patients treated with anthracyclines [152]. Classically, the pathomechanism of ACT was linked with increased production and deleterious activity of ROS within cardiac myocytes, considered the main targets of anthracycline toxicity [152]. Furthermore, mitochondrial damage and malfunction are pivotal events underlying ACT. Experiments on several human and animal models revealed that doxorubicin (DOX), which is the most widely used anthracycline [160], is a potent generator of ROS [161,162,163]. These highly active molecules derive from mitochondria in which the drug incorporates [163], likely due to its strong affinity to phospholipid cardiolipin [164]. 4′-epidoxorubicin (EPI), a synthetic representative of anthracyclines with less pronounced cardiotoxicity [165], is also known to exert its deleterious activity towards cardiomyocytes via elevated ROS. A comparative analysis of mouse HL-1 cardiomyocytes exposed in vitro to DOX and EPI used at 1 μM showed that both anthracyclines stimulate the production of ROS and the accumulation of DNA damage foci (γ-H2A.X). The effects of both drugs are comparable [166]. As a result of ROS accumulation, DOX induces extensive DNA injury, as exemplified in H9C2 cardiomyocytes that accumulate DNA double-strand breaks [167]. Other studies using the same cell type showed that DOX-related DNA injury, namely oxidized pyrimidines and 8-hydroxyguanosine (8-OH-dG), was largely irreparable. This observation contrasts with cell reaction to hydrogen peroxide, where the stressor withdrawal allowed the repair of DNA damage completely [168]. Hearts of DOX-treated mice also possessed an increased level of 8-OH-dG [169]. The insufficient ability of cardiomyocytes to cope with DNA damage after DOX exposure may be associated with the presence of a missense variant rs2229774 (p.S427L) in the retinoic acid receptor gamma (RARG) gene that was found to predispose the cardiomyocytes to reduced effectiveness of DNA damage repair pathways [170]. A recent study on mice and hiPSC-derived cardiomyocytes markedly improved the understanding of anthracycline-related cardiotoxicity by showing that the pathology requires both DNA damage (double-strand breaks) and chromatin damage underlined by histone eviction at specific sites in the genome. At the same time, when the drug variant exerting only chromatin-damaging activity was applied, DOX-related toxic effects were devoid [171].
Mechanisms of increased ROS release upon DOX exposure are complex and proceed in enzymatic and non-enzymatic fashion. Upon its internalization, the quinone moiety of DOX is subjected to one-electron reduction, leading to the generation of the semiquinone radical. When the molecular oxygen is available, the radical transfers to it its extra electron and undergoes reoxidation yielding superoxide anions (O2–), hydrogen peroxide (H2O2), and the initial quinone entering subsequent redox cycles. In the presence of transition metals, the primary ROS transform to hydroxyl radical (OH·). From the side of mitochondria, NADH dehydrogenase, a component of Complex I of the respiratory chain, was implicated as a final place of DOX reduction and excessive ROS efflux [172, 173]. Another enzymatic factor in DOX-mediated ROS is NADPH oxidase (mitoNOX), which catalyzes one-electron transfer from NADPH to O2 [174]. The inhibition of NOX in DOX-treated HL-1 cells results in decreased ROS production, which implies that the one-electron reduction of the quinone ring to the semiquinones originates from the electron donor NADPH utilizing mitoNOX activity [163]. The role of NOX in DOX-related cardiotoxicity was revealed in experiments on mice, in which animals lacking this enzyme were resistant to the chronic adverse effects of this drug [175]. It has also been shown that DOX-related cardiac dysfunction may be orchestrated by topoisomerase IIB (Top2B). Experimental deletion of Top2b, the gene encoding Top2, was found to protect cardiomyocytes against DNA damage and altered transcriptome caused by DOX, altogether leading to dysfunctional mitochondria synthesis and ROS release. In animals undergoing this manipulation, the development of DOX-induced progressive heart failure was seriously restricted [176].
Regarding non-enzymatic drivers of DOX-related ROS overproduction, the first potentiating event is an interplay between DOX and iron. The formation of DOX-Fe complex allows the bidirectional transition Fe2+-Fe3+ in the presence of reducing agents, participating in additional amounts of O2− [177]. In the absence of reducing equivalents, the anthracycline-Fe2+ complex with H2O2 yields OH· [178]. Upon DOX exposure, the iron accumulates preferentially in the cardiomyocyte mitochondria. When the mitochondrial ABC protein-B8 (ABCB8) engaged in the iron export [179] was overexpressed in culture conditions and in the hearts of mice, the content of mitochondrial iron declined, along with ROS, and the DOX-related cardiomyopathy was alleviated [180]. Interestingly, there is a vicious cycle in which ROS and iron cooperate, potentiating their effects. Experiments on H9c2 rat embryo cardiomyocytes showed that DOX-dependent ROS participate in cardiotoxicity by deactivating iron regulatory proteins (IRPs) that regulate the fate of mRNAs for transferrin receptors and ferritin [181]. The role of the iron–ROS interplay in DOX-induced cardiotoxicity was confirmed in experiments with the iron-chelating derivative of EDTA, dexrazoxane; the administration of which reduced the iron pool in the cardiomyocytes and restricted its complexing with the drug [182]. Animals that received dexrazoxane before DOX exposure did not develop any clinical, macroscopic, histological, or ultrastructural signs of cardiomyopathy. This was accompanied by decreased ROS and DNA damage and improved mtDNA copy number [183]. Recently, dexrazoxane was shown to mitigate DOX-induced cardiac injury in mice in vivo, which was causatively connected with suppressed apoptosis [184]. In another cardiomyocyte model, dexrazoxane inhibited apoptosis caused by daunorubicin [185]. There is also a report that dexrazoxane inhibited apoptosis in the irradiated (20 Gy) rat cardiomyocytes by down-regulating NF-κB p65 subunit, which corresponded with ameliorated myocardial injury [186]. Mechanistically, the compound appeared to exert this effect by upregulating miR-17-5p, a molecule playing a role in inflammatory reactions and apoptotic cell death [187, 188]. Other research revealed that it prevents DOX from binding to the Top2B complex, which translated to decreased accumulation of DNA double-strand breaks [167]. Till now, dexrazoxane (ICRF-187, Zinecard) is the only cardioprotective drug approved by FDA for preventing ACT [189], because similarly beneficial effects were not observed with respect to other iron-chelating agents [190]. This, in turn, questions to some extent the validity of the iron report hypothesis of DOX cardiotoxicity and suggests that the beneficial effects of dexrazoxane may be related to its impact on molecular prosurviving cellular pathways, rather than to regulation of the iron homeostasis.
Another mechanism of DOX-associated ROS excess involves alterations within Ca2+ transporters, including the inhibition of the ions flow via NCX [191], the release of Ca2+ via ryanodine receptor (RyR) [161], the activation of L-type channels [192], and the repression of genes coding for Ca2+ transporters in SR [193].
The causative role of ROS-dependent pathomechanism of cardiotoxicity positively verified experiments with antioxidative vitamin E, the administration of which reduced DOX toxicity [161]. Similarly, a beneficial effect was observed upon cardiomyocyte preincubation with melatonin, but in this case, this outcome was only temporary and weakened over time [163]. Not all experiments using antioxidants resulted in a reduction of DOX-dependent cardiac injury (e.g., a clinical trial using N-acetylcysteine [194]), indicating that the problem is more unspecific and extends beyond the hypothesized role of ROS as the critical pathogenic triggers responsible for the ACT.
As mentioned earlier, the induction of apoptosis constitutes another pathway contributing to anthracycline-related cardiomyocyte failure [195]. Detailed analysis of this phenomenon indicated that its role in acute cardiac events might be dominant and relatively negligible in the case of delayed cardiomyopathy and HF [196]. Increased incidence of apoptosis, marked by annexin V and the activation of caspases-3/7, was found in HL-1 cells exposed to DOX and EPI [166]. A dose-dependent increase in active/cleaved caspase-3 and Bax was also observed in primary mouse cardiomyocytes treated with DOX [184]. Chromatin condensation and DNA fragmentation to low molecular weight fragments (subG1 fraction), typical signs of apoptosis, were also detected in rodent cardiomyocytes exposed to daunorubicin [185]. In rat cardiomyocytes, DOX-induced ROS are in the mutual interplay with Ca2+ liberated from intracellular storages through RyR. When the Ca2+ channels in the sarcoplasmic reticulum were blocked, the ROS overproduction in response to DOX was prevented. The same intervention also reduced the extent of apoptosis, as shown according to caspase-3 activation [161]. In H9c2 cells, DOX elicited apoptosis and reduced mitochondrial inner membrane potential (ΔΨm) values, a common feature of apoptotic cells indicating defective course of oxidative phosphorylation and ATP synthesis [197]. Both these phenomena were associated with the activation of p53 [168]. In some cases, however, DOX-induced apoptosis does not require declined ΔΨm, which is the case e.g., in mouse atrial HL-1 cells [163]. Another plausible mechanism of DOX-induced apoptosis was described in human-induced pluripotent stem cell-derived cardiomyocytes (iPS-CMs), in which the drug, as well as other anthracyclines like EPI, daunorubicin, and idarubicin, were found to upregulate a number of death receptors, including TNFR1, Fas, DR4, and DR5, causing apoptosis through binding TNF-related apoptosis inducing ligand (TRAIL) [198].
Apoptosis is not the only kind of cell death affected by anthracyclines. Research on H9c2 cells showed that the drug inhibits autophagy and increases ferroptosis. Both these effects can be prevented by ectonucleotide pyrophosphatase/phosphodiesterase 2 (ENPP2), regulated at a transcriptional level by FOXO4, the level of which was downregulated by DOX [199]. Molecular determinants of DOX-mediated ferroptosis are of particular importance, taking into account the results of other tests that revealed an engagement of this process in DOX-induced cardiomyopathy and mortality in mice and their reversal by ferroptosis inhibition using ferrostatin-1 and iron chelation [200].
Cardiomyocyte autophagy, the altruistic cell death leading to the recycling of cellular components [201], contributes to cardiomyopathy and clinical signs of HF when it is defective [202]. Animals bearing a cardiomyocyte-specific deletion of autophagy-related 5 (Atg5), a protein engaged in the extension of the phagophore membrane in autophagic vesicles, suffer from dilated cardiomyopathy in adulthood [202]. In H9c2 cardiomyocytes, DOX inhibits autophagy by activating E2F1/mTOR complex 1 (mTORC1) signaling, which is followed by apoptosis triggered by E2F1/AMP-activated protein kinase α2 (AMPKα2) pathway [203]. However, the observations regarding autophagy are ambiguous. For example, DOX stimulated autophagy in neonatal rat ventricular cardiomyocytes and this action was linked with a depletion of GATA4 transcription factor, the positive regulator of autophagy-related genes [204]. One may speculate that the disparities in the perception of DOX impact on autophagy may be interpretive and related to the complexity and multi-stage mechanism of autophagy. Some compromise may come from studies showing that DOX impairs autophagic flux in cultured cardiomyocytes in vitro and mice in vivo, simultaneously promoting the accumulation of noncompetent autolysosomes. The autophagic flux is limited because DOX inhibits lysosome function by alkalization of their pH via suppressing vacuolar H+-ATPase, which eventually prevents autolysosome cargo processing. When the very first events in the autophagic cascade were attenuated, DOX-related cardiotoxicity was diminished. And conversely, when the initiation of autophagy was intensified, cardiotoxic drug effects were exacerbated. As such, the direction of events may indicate that autophagy may protect against DOX-mediated cardiac injury, only when the autophagic flux is efficient. When dysfunctional autolysosomes accumulate and the process cannot proceed further, pathological cardiac remodeling based on ROS activity occurs [205].
Experiments on H9c2 cells followed by studies on primary neonatal cardiomyocytes showed that DOX induces their senescence, marked by the presence of SA-β-Gal, senescence-associated heterochromatin foci (SAHF), and elevated p16 [206]. Neonatal rat cardiomyocytes exposed to DOX displayed increased formation of ROS and SA-β-Gal activity, with no concomitant increase in apoptosis, despite activated p53. The development of the senescence phenotype likely took place instead of entering apoptosis, because the concentration of DOX was relatively low and there was no urgent need to eliminate the affected cells [207]. This assumption agrees with another report in which cardiomyocytes exposed to 0.1 μM of DOX exhibited signs of senescence, whereas their counterparts treated with 1.0 μM of DOX became apoptotic [208]. Similar trends were found in cardiomyocytes exposed to low and high doses of EPI [209]. Intriguingly, cells that approached senescence evolved towards hyperploidy, a downregulation of DNA damage-induced checkpoint kinase Chek2, and chromosomal disturbances, which may indicate the initiation of mitotic catastrophe [210]. Cardiomyocytes subjected to lower and higher doses of DOX displayed diversified changes in telomere binding factors TRF1 and TRF2 at both mRNA and protein levels, and changes in TRF2, regulated by p38 MAPK, were critical for the acquisition of senescence or apoptotic phenotype. The low magnitude of TRF2 downregulation caused senescence in the p53-dependent mechanism and the high magnitude of TRF2 down-regulation caused apoptosis in the p53-independent fashion [208]. DOX-induced senescence of neonatal rat ventricular myocytes and H9c2 is also regulated at the transcriptional level by PPARδ sequestering the transcriptional repressor protein B-cell lymphoma-6 (Bcl6). When PPARδ was experimentally inhibited, the level of Bcl6 increased via p38 MAPK, JNK, and Akt activation, followed by amelioration of the senescence phenotype [211].
One of the elements of DOX-induced cardiomyocyte senescence is an abnormal pattern of troponin phosphorylation that may lead to inefficient cardiac contraction [207]. In fact, another aspect of cardiomyocyte functioning that may be affected by anthracyclines is their contractility [212]. Either DOX or EPI (10 μM/20 min) depress several indices of contractility, including the maximum extent of cell shortening, peak shortening velocity, and peak relaxation velocity of single twitches. The magnitude of effects related to both drugs was comparable. The adverse effects were reversible by cell protection by catalase (CAT), and only partly by superoxide dismutase (SOD), which was suggestive of the role of H2O2 as the central culprit of this abnormality [213]. DOX-related disturbances in cell contractility are strongly connected with the distribution and the transient of Ca2+ using transporters associated with systolic Ca2+ signal. Research on rodent cardiomyocytes showed that RyR, responsible for Ca2+ leak from SR [214], is an early target of DOX and its activation underlies an increase in diastolic Ca2+ and the decrease of caffeine-induced Ca2+ peak amplitude [163]. At the same time, decreased caffeine-induced Ca2+ transient decay rate upon DOX exposure was connected with an inhibition of the NCX activity, which may explain diastolic Ca2+ overload and the successive contractility malfunction [163].
The last, but not the least, element of ACT development is local inflammation [215]. Histopathological examination of hearts isolated from mice treated with DOX showed that a large amount of inflammatory cells were accumulated in the disordered tissue [184]. DOX-treated adult mice also displayed cardiac fibrosis that was accompanied by the accumulation of macrophages M1 and increased levels of NF-κB p65 subunit, with a trend toward increased production of the tumor necrosis factor receptor 2 (TNFR2). At the same time, IL-6 level was decreased, and the levels of tumor necrosis factor (TNF-α) and IL-1β were unchanged [216]. The chemotaxis and the accumulation of the immune cells are mediated by several cytokines overproduced in response to DOX in a mechanism involving activation of p38 MAPK and NF-κB [217, 218]. The role of IL-6, a potent proinflammatory cytokine, in the ACT is elusive. Decreased cardiac production of IL-6 upon DOX exposure [216] may imply that it may exert a cardioprotective function, which is in line with the observation that the knockdown of IL-6 in cultured cardiomyocytes led to the augmentation of DOX-induced apoptosis. This picture is, however, blurred by the observation that plasma levels of IL-6 mRNA positively correlated with the severity of ACT [219]. The unclear and hard-to-interpret direction of changes in DOX-related production of proinflammatory factors may depend partly on the research model used, including in vitro and in vivo tests. This is demonstrated e.g., in the case of H9c2 cardiomyocytes, whose treatment with DOX led to increased production of IL-1, IL-6, and TNFα in NF-κB/p65-dependent manner [220].
Vascular endothelial cells
Endotheliotoxicity of anthracyclines is the next piece of the puzzle constituting ACT and the coronary endothelium, and peripheral blood vessels are the next structures affected by these drugs [221]. Among several traits of vasotoxicity, the DOX-related induction of oxidative stress seems to be the most evident one. Mice subjected to DOX exhibited thoracic aorta damage, as evidenced according to inflammatory infiltration, cell swelling, and interstitial cell hypertrophy. This picture coincided with impaired vascular responsiveness, as shown by quantifying endothelium-dependent dilation [222], decreased density of cardiac capillaries, and increased permeability of cardiac microvessels [223]. At a cellular level, DOX reduced the viability of HUVECs, likely due to the induction of p53-dependent apoptosis (subG1 cells) [224]. Mechanistically, the apoptosis was triggered by activated p53, which propagated the signal to its downstream target CD95 in a transcriptional mechanism.
Moreover, DOX activated executioner caspases, as shown by the proteolytic cleavage of the PARP nuclear substrate and the activation of caspase-3, albeit the caspase activation was disconnected from CD95 signaling. Intriguingly, DOX-related apoptosis was determined by culture density: it was present in low-density cultures and absent in the confluent ones. This observation may explain the antiangiogenic activity of DOX, which appeared to trigger the elimination only of proliferating cells that, in contrast to their resting counterparts, actively contribute to tumor neovascularization [224]. Another group also reported markedly higher sensitivity to DOX of dividing than resting ECs, concerning cell proliferation [225].
Several abnormalities caused by DOX were found within mitochondria, whose function associated with respiration and glycolytic activity was impaired. The production of mitochondrial ROS, along with the cellular species, was intensified, which coincided with reduced ΔΨm values, depressed expression of eNOS, and decreased NO content. Mitochondria in DOX-treated HUVECs play a dual role as the source and the victim of ROS. They are clearly disrupted by ROS, which is manifested by their swelling, opening permeability transition pores (mPTP), and efflux of cytochrome C to the cytosol. At the same time, the released ROS may be absorbed by nearby intact mitochondria, leading to damage propagation in a positive feedback reaction, ultimately initiating an apoptotic cascade. Significantly, negative changes elicited by DOX were reversed by edaravone, a free radical scavenger, supported by an mPTP closing agent. The endothelial function, including cell ability to generate NO was restored, in turn, by edaravone and by the adenovirus pAD/eNOS delivery, clearly reinforcing the causal role of oxidative stress and NO deficit in DOX-related EC dysfunction [222]. Other authors showed that DOX undergoes a reductive activation at the reductase domain of eNOS, generating the semiquinone and O2−, at the expense of reduced production of NO. In this context, the DOX-related cardiotoxicity was attributed to a dynamic dose-dependent switch in the enzymatic activity of eNOS, which may change from a NO-generating enzyme (eNOS activity) to a ROS-generating enzyme (NADPH oxidase activity) [226]. These observations may clarify potentially confusing findings e.g., those derived from experiments on bovine aortic endothelial cells (BAEC). In these cells, DOX increased eNOS transcription and protein activity, and cell preincubation with antisense eNOS mRNA resulted in decreased incidence of DOX-induced apoptosis [227].
The synthesis of NO by ECs is regulated, at least to some extent, by specific miRNA. DOX was found to increase the expression of miR-320a in the hearts of drug-treated mice and in HUVECs in vitro. The attenuation of this molecule translated to improved heart vessel density in vivo, repressed endothelium damage, and inhibited cardiac failure. In culture conditions, miR-320a silencing improved cell proliferative capacity, reduced the frequency of apoptosis, and relieved DOX-induced decline in NO synthesis [189]. Target prediction analysis revealed that vascular endothelial growth factor A (VEGF-A) is one of the theoretical miR-320a targets. Further studies confirmed the negative relationship between these two molecules, which may explain decreased VEGF-A protein levels in hearts after DOX exposure. A reduced level of VEGF-A was also found in vitro in DOX-treated rodent ECs [228]. VEGF-A contributes to DOX-associated deterioration of EC function, as its knockdown resulted in weakened cell proliferation, migration, tube formation, and decreased NO release [189]. The potent role of the second variant of VEGF, that is VEGF-B, in DOX-related cardiotoxicity revealed experiments on mice whose DOX-induced cardiac dysfunction was entirely alleviated by delivery of adeno-associated viral vector expressing VEGF-B. Moreover, in cultured ECs, VEGF-B inhibited DOX-related apoptosis and restored their ability to form capillaries [229].
DOX-related abnormalities in VEGF activity are connected with the development of ACT, and EC senescence seems to play a role in this process. HUVECs exposed to DOX display reduced VEGF receptor type 2 (VEGFR2) production, acting as a tyrosine kinase receptor in ECs, in keeping with observations on DOX-treated rat cardiac microvascular ECs [228]. This alteration was accompanied by the acquisition of senescence phenotype manifested by the activation of SA-β-Gal, p53, and its downstream effector, p21, and deterioration of growth-promoting proteins, cyclin A and lamin B1. At the same time, conversely to the report cited above [189], which was made on the same cell type but using a different dosage regimen (250 nM/24 h vs. 5 μM/12 h), DOX transiently induced VEGF-A at mRNA level. When the cells became senescent, the VEGF-A mRNA expression returned to values typical for untreated cells. The VEGFR2 protein dynamically increased, but did not reach the steady-state values before DOX exposure. The development of senescence phenotype in DOX-treated HUVECs also coincided with increased autophagic flux. Autophagy-related VEGFR2 trafficking and degradation did not turn out to be the reason for the protein decrease upon DOX. The actual cause was the inhibition of the protein synthesis by impinging on the p53-mTOR signaling [230]. At the same time, ECs that senesced upon DOX exposure do not display typical SASP-related overproduction of proinflammatory cytokines, which appeared to be a self-limiting phenomenon in vitro and in vivo. Namely, DOX stimulated transient hypersecretion of IL-6 in a mechanism engaging ROS-dependent activation of p38 MAPK, but it was recognized as an acute secretory profile, distinct from canonical SASP. When the drug induced HUVEC senescence, the SASP could not develop due to the suppression of PI3K/Akt/mTOR axis [231]. Recent studies in which DOX-induced senescence of human aortic ECs was prevented by vitamin D3 administration also pointed to the role of IL-10 being controlled by pAMPKα/SIRT1/FOXO3a signaling complex [232]. Apart from upregulated IL-6, the proinflammatory phenotype of DOX-treated ECs also includes increased expression of VCAM-1 and E-selectin, contributing to increased adhesion of neutrophils to these cells [225].
An integral element of cellular senescence and DOX-related toxicity is DNA damage, the spectrum of which is broad and includes DNA strand breaks, induction of DDR (γ-H2AX), and oxidative modifications [233, 234]. A comparative analysis of DOX and daunorubicin concerning their ability to destroy EC DNA showed that both these analogs are genotoxic, albeit the effects caused by the latter are more pronounced [235]. DOX exerts its deleterious activity also towards cellular lipids, as evidenced according to increased concentration of malondialdehyde (MDA) in treated HUVECs [234].
Vascular smooth muscle cells
SMCs are the second cellular component of blood vessels violated by anthracyclines and thus participating in the ACT. Upon exposure to DOX, they prematurely senesced, displaying hypertrophic appearance, specific markers, and activated DDR [236]. In rat aorta SMCs, the drug deregulates oxidative stress-related parameters [increased ROS production and decreased catalase (CAT)] and intensifies eNOS-NO axis, which coincides with up-regulated PKCα and PKCβ1 [237]. DOX-induced senescence may also involve, apart from exacerbated oxidative stress, increased production of urokinase receptor (uPAR), whose experimental silencing in either in vitro or in vivo conditions abrogated the drug-induced senescence. The prosenescence activity of uPAR was linked with ubiquitination and proteasomal degradation of TRF2 [238].
Research on isolated arteries showed that DOX used at a relatively low dose (0.3 μM) affects SMC functioning by decreasing noradrenaline-induced contractions, which was associated with a depressed induction of α1A-adrenoceptor protein, but not of mRNA. The tissue exposure to SOD partially prevented these abnormalities, suggesting that O2− produced during redox cycling of DOX downregulates the receptor at the protein synthesis level. When the dose of DOX increased to 1 μM, the signs of apoptosis approached, whereas at 10 μM the cultured arteries became necrotic [239]. In addition, experiments on DOX-treated mice or those using mouse aortic segments exposed to this drug (1 μM) ex vivo revealed decreased phenylephrine (PE)-induced SMC contraction, due to a depressed tonic phase of contraction characterized by Ca2+ influx. At the same time, DOX did not change the transient PE contraction related to Ca2+ release from the SR [240]. A systemic administration of DOX into BALB/cJ mice led to detrusor smooth muscle hypertrophy, increased voiding frequency, and a substantial attenuation of the muscle contractility, followed by a slower relaxation. Unlike the cardiovascular effects of DOX, in the case of urinary system dysfunction, the results of the drug were not associated with oxidative stress but with a reduced amount of large-conductance Ca2+-activated K+ channels and suppressed myosin light-chain phosphorylation [241].
DOX also affects lymphatic muscle cells. It leads to a dose-dependent inhibition of rhythmic contractions, remarkably reducing the flow. This effect was paralleled by a tonic rise in cytosolic Ca2+ level, which occurred via the opening of RyR and resulting calcium leak from SR. This discovery reveals that pharmacological blocking of RyR-dependent Ca2+ inflow may be a helpful strategy in reducing DOX-related lymph vessel injury and the development of lymphedema [242].
A substantially different view on contractility and Ca2+ management in SMCs treated with DOX delivered research on cells from C57BL/6 mice, in which the drug intensified both phasic and tonic contractions in denuded vessels and elevated levels of [Ca2+]i in single muscle cells. The study showed, however, how vital the dose of DOX concerning contractile SMC action is. When used at 100 μM, it increased rhythmic contraction amplitude, but when the dose was 1 mM, the amplitude was abolished with an increase in maximal tension [243]. A diminished relaxation of aorta SMCs in response to NO donor, sodium nitrate, was also found in rats treated with DOX. This effect coincided with an induction of cellular senescence, manifested by increased SA-β-Gal, p16, p27, IL-6, and IL-8 [244].
The current view on the proinflammatory phenotype of DOX-treated SMCs attributes this phenomenon to cellular senescence. Primary rat aortic SMCs subjected to DOX become senescent (SA-β-Gal, γ-H2A.X, p21) [245]. This coincided with stimulation of Nlrp3 inflammasome, leading to an upregulated secretion of IL-1β but not, surprisingly, IL-6. The increased IL-1β has been recognized as a mediator of calcification, which appeared to be preventable in vivo in DOX-treated Nlrp3−/− mice. Further research showed a proinflammatory autostimulatory loop in which IL-1β promotes IL-6 mRNA and mRNA for itself, as well as induces the Nlrp3 and the osteogenic marker BMP-2 [245]. Increased mineralization may be another pathogenetic element contributing to increased vessel stiffness and related proatherosclerotic vessel remodeling. The matter of DOX-related vessel stiffening resulting from changes in SMC behavior is, however, still elusive as a recent study showed that it occurs ex vivo translating to decreased cell contractility. In contrast, in vivo this effect was absent [240].
Increased inflammatory response of SMCs e.g., an elevated IL-6 mRNA may also be connected with the activity of brain and muscle Arnt-Like protein-1 (BMAL1), a molecular promotor of SMC proliferation [246], was simultaneously upregulated by DOX. Paradoxically, the overexpressed IL-6 was further raised upon BMAL1 silencing, which also impaired cell viability and increased activity of antiinflammatory nuclear factor erythroid 2-related factor 2 (Nrf2), increased NADPH oxidase 4 mRNA, and increased phosphorylation of p38 MAPK. The causative engagement of activated p38 MAPK in DOX-related inflammation was confirmed by intervention tests in which chemical inhibition of the kinase translated to a deterioration of BMAL1-dependent elevation of IL-6 [247].
Platins
Although the primary adverse events of cancer therapy when using high-dose of platin-based drugs, including cisplatin (CIS) and carboplatin (CPT), include nephrotoxicity, neurotoxicity, ototoxicity, and gastrotoxicity [248, 249], there are also reports pointing to the harmful activity of platins in disturbances encompassing CVS [250, 251]. Much broader evidence concerning potential cardio- and vasotoxicity stem from basic research on cellular models uncoupled from clinical observations.
Cardiomyocytes
Arrhythmias and other CVS disorder manifestations experienced by cancer survivors treated with platins [252,253,254] are causatively connected with the malfunction of cardiac cells. The hearts of animals subjected to CIS are hypertrophic and bear disarrayed cardiac muscle fibers architecture, which corresponds with cardiac dysfunction. The reversal of this trait by exogenous flavonoid kaempferol, known for its antiinflammatory and antioxidative properties [255, 256], suggests the plausible pathomechanism of platin-induced toxicity [257]. Rats exposed to CIS exhibited decreased diastolic blood pressure with unaltered systolic blood pressure and heart rate. At the highest dose of CIS (3 mg/kg), the drug decreased left ventricular developed pressure (LVDP) and increased end-diastolic pressure (EDP) values [258]. An aberrant cardiac histology concomitant with elevated apoptosis is also a consequence of CPT administration [259].
In culture conditions, rat cardiomyocytes exposed to this drug became apoptotic, as shown by increased caspase-3, 9, and cytochrome c, and decreased Bcl-xl. The inhibition of apoptosis incidence in cells pretreated with ROS scavenger, N-acetylcysteine, demonstrated the association between CPT-induced apoptosis and oxidative stress [259]. H9c2 cells exposed to CIS display increased apoptosis, as evidenced according to the increased percentage of TUNEL-positive cells, upregulated expression of Bax, and downregulated expression of Bcl-2. At the stage of apoptosis effectory pathway(s), STING signaling may play a role. CIS enhanced this pathway, and its silencing prevented drug-induced cell death [257]. The translocation of proapoptotic Bax from the cytoplasm to the mitochondria was essential in CIS-induced apoptosis [260]. Other apoptosis indices found in rat ventricular cardiomyocytes subjected to CIS include ΔΨm depolarization and increased leak of cytochrome c from mitochondria to cytosol, confirming the mitochondrial mechanism of apoptosis [261]. An induction of transcription factor Nrf2 and heme oxygenase 1 (HO-1) mitigating CIS-related apoptosis in H9c2 cells delivers other targets involved in the cardiotoxicity of platins and points to the causative role of oxidative stress [262].
Indeed, decreased expression of Nrf2, which protects cells against oxidative stress [263] and reduced activity of HO-1, an enzyme contributing to Nrf2 pathway activation [264], was described in CIS-treated cardiomyocytes. Cardiomyocytes exposed to this drug display signs of oxidative stress, including increased production of ROS, depleted SOD, CAT, and reduced glutathione (GSH), and increased storage of MDA. In addition, CIS upregulates p38 MAPK and ERK1/2 [260, 265]. Experiments with growing doses of CIS showed that the drug stimulates the phosphorylation of ERK1/2 dose-dependently and that the kinase inhibition translates to decreased cell propensity to apoptosis [260]. As per p38 MAPK, the p38α makes cardiomyocytes more vulnerable to apoptosis evoked by various triggers via upregulation of the proapoptotic Bax and Fas and downregulation of ERKs and Akt prosurvival pathways [266, 267].
Immunohistochemical evaluation of myocardial tissues from CIS-treated mice showed the formation of a proinflammatory environment, exemplified by the tissue infiltration with macrophages. This observation was linked with increased mRNA and protein for TNFα and IL-6, and mRNA for MCP-1, likely contributing to monocyte chemotaxis. NF-κB induced transcription of the above genes, and CIS stimulated its activating phosphorylation [257].
Mitochondrial malfunction and cardiomyocyte apoptosis may also underlie disturbances in cardiac muscle contraction. Experiments on C57 mice showed that CIS (10 mg/kg per day) led to the development of myocardial contractile dysfunction, as evidenced by decreased LVDP. This alteration coincided with ultrastructural abnormalities within the mitochondria, the activation of the ER stress response, and apoptosis in CIS-treated cardiomyocytes [268].
Vascular endothelial cells
Platin drug-related damage to ECs predisposes cells to various pathogenetic events, including thrombotic disease, atherosclerosis, and disturbed vascular contractility. In young cancer survivors, delayed complications of CVS may occur 10–20 years from the point at which the therapy was terminated [269]. When it comes to acute cardiotoxicity of platins, it is generally linked with direct damage to ECs, as hypothesized according to the observation of increased release of von Willebrand factor antigen (vWF:AG) [270], the marker of EC injury [271]. Increased incidence of thromboembolic events may also be associated with upregulated production of procoagulant endothelial microparticles (EMPs) by HUVECs and human pulmonary microvascular ECs. The EMPs promoted thrombin generation in a tissue factor-independent mechanism, which coincided with augmented cell death [272]. Direct toxicity of platins may also lead to the deregulation of vascular tone. Experiments focused on the contractile action of thoracic aortic rings obtained from Sprague–Dawley rats revealed that CIS counteracted KCl- and phenylephrine-stimulated contractions in both endothelium-intact aortic rings and endothelium-denuded aortas. Subsequent tests on cultured HUVECs showed that these abnormalities could be associated with CIS-related inhibition of ATP-induced intracellular Ca2+ concentration burst [273].
CIS toxicity also translates to structural abnormalities within the endothelium in vivo, including vacuolation, subendothelial swelling, and internal elastic membrane decomposition. All these negative changes were prevented in animals treated with vitamin E, which implies the contribution of CIS-related oxidative stress [274]. Research on cultured cells (HUVECs) showed that CIS both intensifies the production of ROS and decreases GSH/GSSG ratio compared with untreated cells [275].
Another critical sign of platins’ endotheliotoxicity, likely associated with ROS activity, is DNA damage. When it comes to cancer cells, CIS and CPT bind to the N7 reactive center on purine bases, causing DNA injury that stops replication and turns cancer cells towards apoptosis and/or necrosis [276, 277]. In the context of ECs, CIS inhibited transcription reaching the highest inhibitory effect 24 h after exposure. The products of the drug activity included DNA intrastrand cross-links (i.e., 1,2-GG, 1,3-) and interstrand cross-links, which derive from monoadducts with a slow kinetic, which are the most potent transcription blockers. In addition, CIS caused a massive accumulation of γ-H2AX and 53BP1 foci found in a significant subset of cells 24 h after the exposure, followed by minor phosphorylation of ATM, Chk1, and p53 [278].
Because apoptosis is often a consequence of ROS activity and DNA damage, this aspect of EC biology was tested in cells treated with platins. Experiments on HUVECs showed that CIS induces apoptosis (TUNEL and cleaved caspase-3) dose-dependently, accompanied by decreased Bcl-2 level. Moreover, CIS upregulates hypoxia-inducible factor-1α (HIF-1α), which positively regulates angiogenesis-related genes at the transcriptional level [279], although the production of VEGF remained unchanged. Instead, CIS intensified the interaction of HIF-1α with p53 indicating that this transcription factor may act as a switch directing cells toward p53-dependent apoptosis rather than as a regulator of EC survival and angiogenesis [280]. CIS-treated apoptotic ECs were characterized in vitro by a morphological depopulation, as evidenced according to decreased transendothelial electrical resistance and repressed expression of tight junction proteins, occludin and zonula occludens-2 (ZO-2) [281].
One of the aspects of EC biology most affected by platins is their motility, being a somewhat simplistic measure of angiogenesis [282]. It must be stressed, however, that literature data regarding the modulation of angiogenesis by platins concern tumor vasculature to the most considerable extent; thus, they are basically uncoupled with potential cardio- and vasotoxicity. CIS inhibits dose-dependent proliferation and tube formation in HUVECs in vitro, as well as rabbit corneal neovascularization in vivo [280, 283]. Furthermore, the drug inhibits HUVEC migration and upregulates the activation of p38 MAPK and JNK signaling routes. Intervention tests directed towards the understanding of the mechanism of the attenuated migration showed that it was associated with decreased production of extracellular matrix (ECM) degrading enzyme, matrix metalloproteinase 2 (MMP-2) [284]. Another research project extended these findings by showing that CIS inhibits vascular endothelial growth factor (VEGF)-mediated angiogenesis in Matrigel™ plugs in mice [285]. Interestingly, the inhibitory effects of CIS on HUVEC motility may proceed not only after the direct exposure, but also indirectly in a paracrine manner. This assumption confirms research on HUVECs, whose migration and tube formation capacity was unaltered upon CIS applied at doses between 0.01 and 1 µM. Conversely, when the HUVECs were exposed to a conditioned medium generated by CIS-treated lung cancer cells, the angiogenic behavior of ECs remarkably declined. Mechanistically, this effect was coupled with the activity of cancer cell-derived tissue inhibitor of matrix metalloproteinases-1 (TIMP-1) interacting with p38 MAPK and ERK1/2 signaling pathways [286].
In the case of CPT, its angiogenesis-modulating action seems more complex. Namely, the drug potentiates the production of angiogenesis-promoting VEGF by ECs, and the neutralization of the secreted VEGF led to their sensitization to the drug and massive apoptosis. Interpreting these results, authors of the study postulate that endothelium-derived VEGF is a survival agent that CPT induces to protect tumor vasculature during therapy [287].
Vascular smooth muscle cells
The existing literature provides ambiguous data regarding platin-related changes in blood vessel contractility, which may be associated with different experimental models used (e.g., different species of rats) and different dosage regimens in vivo and in vitro. Experiments on rats showed that their chronic exposure to CIS did not alter the aortic vasoconstrictive reaction to phenylephrine, but suppressed the carbachol-related vasorelaxation [258]. On the other hand, the research cited above was in the context of EC dysfunction and was performed using the same model indicated that CIS inhibits contractions in endothelium-denuded aortas [273], which may suggest the engagement of other cell populations, likely SMCs. However, direct exposure of SMCs to platins has never been tested; thus, their role in vascular reactions still has to be experimentally established. At the same time, there is a risk that functional changes within SMCs may be hard to interpret as they display, as shown using the rat model, high heterogeneity in some biological reactions, specifically proliferation and apoptosis, to external stressors, including CIS [288]. However, some clues regarding plausibly adverse effects of such exposure may be derived from research on rabbits. Intraarterial administration of high-dose of CIS resulted in damage to the tunica media, including vacuolation and disorganization of SMCs, fibrinoid necrosis, and hemorrhage [289].
Taxanes
In cancer therapy, taxanes, especially paclitaxel (PCT) and docetaxel (DCT), hyperstabilize cytoskeletal microtubules that jeopardize various aspects of cancer cell proliferation, particularly chromosome segregation during mitosis [290, 291]. Their effectiveness against several malignancies goes hand in hand with side effects on healthy organs, including the CVS [292]. At the same time, unlike other drug groups with conclusively cardiotoxic activity, the outcomes of taxane administration appear to be more complex and both negative and positive. As per cell types discussed in this article, adverse consequences of taxanes are most noticeable in the case of cardiomyocytes and ECs. Regarding vascular SMCs, PCT activity is used to prevent some CVS disorders e.g., restenosis occurring after percutaneous coronary interventions (PCIs) in patients with coronary heart disease. In addition, cardio- and vasotoxicity of taxanes extended pathophysiologically beyond the cellular context and engaged some indirect effects associated with the excessive histamine release [293, 294]. In response to histamine receptor stimulation, cells, including cardiomyocytes, require more oxygen, which leads to cardiac vessel contraction, contributing to the development of their arrhythmogenic phenotype [295].
Cardiomyocytes
The development of arrhythmias is often associated with taxane therapy, and an abnormal Ca2+ metabolism is the probable cause of this disturbance [292, 296]. Experiments on the guinea pig model revealed that spontaneous Ca2+ oscillations might lead to premature heartbeats, ventricular tachycardia, or ventricular fibrillation [297]. Neonatal rat ventricular cardiomyocytes subjected to PCT (at 800 ng/ml, equivalent to concentrations used in the treatment of patients with cancer) are characterized by an increased frequency of spontaneous Ca2+oscillations [298]. Importantly, this effect was uncoupled from either the primary mode of PCT action affecting microtubules or its secondary result—apoptosis. The prooscillatory impact of PCT was sensitive to prevention by inhibiting the inositol-1,4,5- trisphosphate receptor (InsP3R), which promotes Ca2+ release and interacts with neuronal calcium sensor 1 (NCS-1), and is also upregulated by the drug in vitro and in vivo. At the same time, it was independent of RyR, thus playing an essential role in Ca2+ efflux from SR [299], which shows, in turn, that PCT does not influence SR Ca2+ reservoir [298].
Cardiac ischemic events are the next type of taxane-related CVS disorders [300], and hypoxia plays a vital role in their pathophysiology. Deficits in oxygen delivery cause disturbances in cellular energy metabolism that translate to several structural and functional anomalies [301]. This state rapidly stimulates glycolysis in cardiomyocytes, providing anaerobic ATP and lactate in a process controlled by HIF-1α [302]. In addition, cellular microtubules, playing a pivotal role in the transmission of mechanical forces within the myocardium, are disorganized in hypoxic conditions [303]. Their breakdown level determines cardiomyocyte viability [304]. The outcomes of PCT action on cardiomyocytes under hypoxia depend on its concentration, experimental model, and analyzed cardiac function. High doses of this drug disrupt the microtubular structure, which is accompanied by decreased HIF-1α nuclear content, reduced cell viability (elevated LDH—a measure of a cell injury), downregulated glycolytic enzymes (phosphofructokinase, pyruvate kinase), and depleted ATP. However, when PCT was applied at low doses, the direction of all these effects was the opposite. The drug counteracted hypoxia-related microtubule breakdown and ameliorated energy metabolism and cell viability by increasing HIF-1α content [304]. The above findings suggest that under specific conditions (read: at relatively low doses), PCT may prevent microtubule disruption and, thus, potentially reduce cardiac infarct size. Analogically, DCT decreased LDH release and oxidative stress in confluent cultures of newborn rat cardiomyocytes submitted to cold ischemia–reperfusion [305]. Furthermore, PCT used at doses of 0.3–3 μM enhanced heart rate, LVDP, and work index in isolated rat and rabbit hearts subjected to local ischemia without reperfusion [306]. Experiments on isolated rat hearts showed that PCT used at relatively low doses of 0.1–1.0 μM helped to preserve microtubule structure in ischemic conditions. This effect was coupled with decreased ROS production and increased mitochondrial electron transport chain complexes I and III activities. In addition, PCT increased the phosphorylation of JNK1, which appeared to mediate an elevation in HO-1 expression [307]. Another plausible mechanism of PCT-dependent protection of cardiomyocytes against ischemic ventricular arrhythmias includes restoration of gap junctional protein, connexin 43 (Cx43) [308].
At the same time, other research on guinea pig hearts showed detrimental, arrhythmogenic effects of PCT [309]. In isolated rat hearts maintained under normoxic conditions, PCT exerted a cardiodepressive activity, manifested by decreased dose-dependent heart rate and LVDP, and increased perfusion pressure. At the same time, it failed to reduce infarct size during ischemia, despite its protection against hypercontracture. This lack of protective effect coincided with a higher increase in cytosolic Ca2+ content during ischemia, which may explain the absence of the drug reactivity against infarction observed in isolated hearts. These findings may imply that PCT intensified injury during ischemia, initiating rupture of the sarcolemma in isolated cells, with secondary loss of intracellular cargo, including Ca2+, and the consequent suppression of cell hypercontracture during reperfusion [303]. Last, but not least, the profound increase in perfusion pressure triggered by PCT, along with highly contextual changes remaining, may translate to diversified clinical consequences in oncologic patients. They may be expressed as brady- and tachyarrhythmias, atrioventricular conduction block, or myocardial ischemia and infarction [292, 310].
As shown before, PCT exerts antioxidative activity by modulation of mitochondrial metabolism in rat [307] and rabbit ischemic hearts [311]. The impact of taxanes on oxidative stress-related parameters is more complex and probably associated with an oxygenation tissue status. Under normoxia, PCT induced oxidative stress in adult Wistar rats, as evidenced according to increased concentration of lipid peroxidation product, MDA, and NO. Moreover, cardiac damage was found, including diffused edema, hemorrhage, congestion, hyaline exudates, and necrosis [312]. In H9c2 cells, DCT stimulated ROS production, followed by a compensatory increment of mRNA expression for CAT and GPX, and protein for SOD1. Intensified endoplasmic reticulum stress (increased ATF6 and CHOP) and decreased cell viability, due to increased incidence of apoptosis and necrosis, accompanied this imbalance in redox status [313].
Vascular endothelial cells
Taxanes exert antiangiogenic activity, primarily when used at low concentrations [314]. Experiments on C57BL/6N mice showed that PCT suppresses angiogenic reactions stimulated by cancer-derived conditioned medium inserted in a pellet of Matrigel™ injected subcutaneously (s.c.). Consequently, the drug dose-dependently inhibited various aspects of angiogenesis in vitro, including HUVEC proliferation, migration, invasiveness, and capillary network formation [315, 316]. This antiangiogenic activity of PCT seems to be a universal phenomenon, as it was present in various cellular models, such as HUVECs [315, 316], HDMECs [317], and human microvascular ECs (HMEC-1) [318]. Research conducted on HUVECs and HMEC-1 cells revealed that PCT inhibits angiogenesis by intensifying microtubule dynamicity, manifested by increased growth, shortening rates, and extents. This impact coincided with decreased anaphase/metaphase ratio and was uncoupled from apoptosis [318]. Further research on HUVECs and HMVEC-1 cells showed that PCT inhibits their proliferation in two distinct mechanisms, determined by its dose. Namely, the drug exerts primarily cytostatic activity at low concentrations, whereas at higher doses (> 10 nM), it becomes cytotoxic. The inhibition of EC proliferation occurs exclusively at cytostatic doses, does not involve any structural microtubule modifications, and is based on slowing cell cycle progression instead of any specific cell cycle arrest. In contrast, the cytotoxic effects include G2/M growth arrest, increased Bax/Bcl-2 ratio, mitochondria permeabilization, and apoptosis [314]. In lymphatic ECs (LEC) PCT inhibited their migration, adhesion, and branch point formation by activating autophagy mechanism independent of Akt phosphorylation. In vivo, the permeability of LEC to cancer cells was increased and this effect was ameliorated by the inhibition of autophagic flux. From the clinical point of view these effects of PCT were ambivalent as from one side it effectively reduced tumor size, it also promoted its spread to the sentinel lymph nodes [319]. HDMECs treated with PCT responded, in turn, with decreased proliferation and tube formation, and augmented necrosis [317].
DCT also exerts antiangiogenic effects, but their mechanism is slightly different. The drug inhibited HUVEC migration and tube formation, but not proliferation. It was associated with reducing the reorientation of the cell’s centrosome, acting as the microtubule organizing center [320]. In addition, the antimigratory activity of DCT was linked with ubiquitination and subsequent proteasomal degradation of HSP90, which blocks signals from the focal adhesions causing ECs’ incompetence to interact with VEGF. The drug also attenuated the VEGF-dependent phosphorylation of focal adhesion kinase, Akt, and eNOS, acting as downstream targets for HSP90 [321]. Another research on EA.hy926 hybrid endothelial cells showed that DCT inhibits their proliferation, migration, and invasion and induces apoptosis via the upregulation of p53. Moreover, it inhibited the adhesion of ECs by downregulating adhesion proteins VE-cadherin and PECAM-1. As per effectory signaling, DCT-related inhibition of EC migration and adhesion was controlled by VE-cadherin mediated integrin β1/FAK/ROCK transduction pathway [322].
Because EC senescence is involved in the pathogenesis of CVS disorders, such as atherosclerosis, hypertension, and thrombosis [83, 323, 324], the effect of taxanes on this phenomenon was tested. Research on HUVECs showed that PCT induces SA-β-Gal dose-dependently (2.5–5.0 nM), which coincided with increased prothrombotic PAI-1, one of the endothelial SASP indices [325]. At the same time, the level of eNOS decreased, imposing a vasoconstricting tendency. Although PCT-treated cells also displayed downregulated SIRT1, a mediator of senescence [326], the overexpression of this protein did not translate to ameliorated senescence EC phenotype [327]. The mechanism of PCT-induced HUVEC senescence also probably does not involve oxidative stress, as the MDA and GSH in treated cells remained unchanged [328]. However, this assumption should be clarified, as the experiments in vivo on PCT-treated rats revealed increased ROS release and NADPH oxidase mRNA in arteries and human coronary artery endothelial cells (HCAECs) [329].
As per the secretory prothrombotic profile of ECs, apart from increased PAI-1 [325], PCT potentiated tissue factor (TF) production and reduced expression of thrombomodulin and protein C receptor. Significantly, these effects were achievable only in the presence of a proinflammatory agent, TNFα, acting as the costimulator [330]. This finding does not discount the prothrombotic potential of PCT, as the drug is known to upregulate TNFα production by immune cells [331].
Vascular smooth muscle cells
A body of reports concentrated on PCT usage in drug-eluting stents (DESs) employed during PCIs in patients with coronary artery disease [332]. Because this procedure has some drawbacks, including mechanical damage leading to EC denudation and stimulation of both intravascular thrombosis and smooth muscle proliferation [333,334,335,336], PCT offers clear advantages because it restricts SMC expansion. The experimental background certifying antiproliferative PCT activity towards SMC is quite extensive. Human arterial smooth muscle cells (haSMCs) exposed to PCT displayed inhibited proliferation along with the stabilization of the microtubule network. The in vivo administration of the drug in rabbits led to vessel remodeling, manifested by reduced intima wall area, wall thickness, and magnitude of stenosis [337]. Time- and dose-dependency of SMC response to PCT clarified further experiments on human arterial cells showing that the drug arrests cell growth in the G2/M phase of the cell cycle, which was accompanied by their decreased ability to migrate [338]. A direct comparison of PCT activity against rat thoracic SMC and ECs showed that the antiproliferative reaction of the former was less dynamic, which was associated with a slightly different pattern of cell cycle regulation [339]. A dose-dependent reduction of SMC proliferation was also reported with respect to DCT, which exerted its action via downregulating cyclin-dependent kinase 2 (CDK2), CDK4, cyclin D1, cyclin E, retinoblastoma protein (pRb), and PCNA. The taxane also suppressed the phosphorylation of ERK1/2 and Akt [340]. The effectiveness of PCT delivery in restenosis prevention was demonstrated using various models, including humans, in whom the PCT-eluting stents provided considerable benefits in 6-month angiographic follow-up [341]. The positive outcomes of this drug administration were also found in rats, in which PCT inhibited pulmonary hypertension by modulating vascular remodeling, in particular, reducing the right ventricular hypertrophy index and thickness of the pulmonary arterial tunica media [342].
Antimetabolites
Epidemiologic data indicate that 5-fluorouracil (5-FU) and its prodrug, capecitabine, are the second most common triggers of chemotherapy-related CVS disorders after anthracyclines [343, 344]. Cardiotoxicity was found in up to 35% of patients receiving 5-FU, and its extent differs depending on the dose and dosage algorithm [345]. Because of a relatively short half-life of 5-FU, which approximates 15–20 min [346], the cardiovascular consequences of the bolus drug administration appeared to be lower than those associated with its continuous intravenous delivery [347].
Cardiomyocytes
The mode of cardiotoxic activity of antimetabolites is wide and includes either indirect or direct toxicity. As per the first mechanism, leading to cardiomyopathy, 5-FU drives it through ischemic injury resulting from coronary vasospasm [348, 349]. As per the second mode, cardiomyocytes undergo direct damage via different pathomechanisms. In rats, 5-FU induced structural changes in the myocardium, including cytotoxicity (marked according to increased CK-MB and cTnI), hypertrophy, and dilatation. The damage in aged animals was more significant than in their young counterparts. Echocardiography showed that the drug causes ventricular enlargement and decreases myocardial contractile function. The left ventricular ejection fraction (LVEF) was also reduced, but this feature again only concerned the aged rats [350]. Similar findings derive from experiments on mice, in which left ventricular function indicators, such as ejection fraction, fractional shortening (FS), and cardiac output, were reduced upon treatment with 5-FU, whereas the levels of ventricular end-diastolic anterior wall thickness and LAID were increased [351]. Human cells exposed to 5-FU responded at decreased proliferation rate when the drug dose was 10 μM or higher. The exact concentration also appeared to be a threshold at which the first signs of apoptosis occur [352], staying in line with cardiomyocyte apoptosis in rats exposed to 5-FU in vivo [350]. Importantly, micromolar concentrations that effectively change cardiomyocyte functioning are in the range of therapeutic dosing of 5-FU and its prodrug, capecitabine [353,354,355]. The antiproliferative effects of 5-FU may be directly associated with blunting of CITED4, a key regulator for cardiomyocyte growth [356].
Another phenomenon elicited in cardiomyocytes by 5-FU is autophagy, albeit the concentrations capable of inducing this process are significantly greater (1 mM) than those with cytostatic or apoptotic activities. The extent of autophagy was inhibited by N-acetylcysteine, indicating that oxidative stress exacerbated in these cells leads to this kind of cell remodeling phenomenon [352].
Mechanistically, the toxicity of 5-FU and capecitabine is associated with oxidative stress. Human cardiomyocytes started overproducing ROS at as low concentrations of 5-FU as 0.01 μM [352]. Rat cardiomyocytes exposed to 5-FU and capecitabine displayed increased ROS production combined with depleted GSH and accumulated MDA [351, 355]. Myocardial tissue from guinea pigs exposed to 5-FU showed decreased SOD and GPX activities and increased CAT, which coincided with elevated MDA levels [357]. The intensified oxidative stress originated from mitochondria displaying decreased ΔΨm and transmitted to increased apoptosis and necrosis. A direct comparison of the two drugs showed that 5-FU is more cytotoxic than capecitabine [355]. Mitochondrial origin of 5-FU-induced ROS confirmed experiments on H9c2 rat cardiomyocytes, which when treated with this drug overproduced O −2 [358]. Also, the myocardium of rats treated with 5-FU in vivo experienced severe mitochondrial injury, manifested by reduced ΔΨm value and ATP level. These features were accompanied by morphological deterioration of these organelles in the form of swelling, partial fusion, and ridge breakage. Moreover, an increased number of autophagosomes was found, implying the induction of mitochondrial autophagy (mitophagy) [350].
Changes observed in mitochondria of 5-FU-treated cardiomyocytes included reduced size, crumpled membranes, and small cristae [351], indicating the activation of ferroptosis, the iron-dependent cell death [359]. The level of Fe2+ in the cardiac tissue was increased in response to the drug, and when the ferrostatin-1 (Fer-1), an inhibitor of ferroptosis [360], was used, MDA and GSH contents, initially elevated and decreased upon 5-FU exposure, respectively, changed in the opposite direction indicating the Fe-dependent kind of oxidative stress induction. In addition, Fer-1 relieved the diminished expression of glutathione peroxidase 4 (GPX4), the key inhibitor of ferroptosis [361], which suggests the causative involvement of this type of cell death in 5-FU-mediated cardiotoxicity [351]. The results of in vivo and in vitro studies further strengthened this statement by showing that 5-FU intensifies ferroptosis by reducing the expression of GPX4 and ferritin heavy chain 1 (FTH1) and elevating the expression of transferrin receptor 1 (TfR1) [362].
Energetic deficits in cardiomyocytes treated with 5-FU reported as a result of its direct activity, e.g., in guinea pig myocardium [363], may also proceed indirectly. Fluoroacetate, a catabolite of 5-FU, was found to inhibit aconitase, an enzyme engaged in the tricarboxylic acid cycle (TAC) progression and energy production [364]. Decreased ATP probably activates a vicious cycle in TAC because 5-FU appeared to stimulate α-KGDHC activity [365], the level of which is negatively correlated with ATP content [366]. At the same time, the redox disequilibrium elicited by 5-FU does not include the induction of anaerobic glycolysis, which was showed by experiments on H9c2 cells maintained under hypoxia [367].
An additional mechanism by which 5-FU impairs cardiomyocytes is the induction of cellular senescence, which occurs at concentrations as low as 0.1 μM [352]. Human cardiomyocytes exposed to 5-FU display increased mRNA for p16, a marker of premature cell senescence, and IL-6, exemplifying SASP [368].
Vascular endothelial cells
The development of myocardial ischemia in patients treated with 5-FU and capecitabine is causally linked with alterations within vascular endothelium [345, 369]. Scanning electron microscopy of rabbit vessels showed that the administration of 5-FU leads to severe ECs damage, including intima disruption and denudation of underlying structures, with accompanying platelet accumulation and fibrin deposition [370]. The drug used at 10 μM inhibits HUVEC proliferation and initiates apoptosis. At the same time, conversely to cardiomyocytes, only weak signs of autophagy were found, whereas the induction of senescence was evident between 10 and 1000 μM [352]. Hybrid endothelial cell line, EA.y926, subjected to 5-FU (100 μg/ml), displays reduced proliferation, enlarged and flattened morphology, as well as elevated SA-β-Gal, p16 and VCAM-1 mRNA [371]. Causatively, the induction of senescence was mediated by p38 MAPK and JNK, the inhibition of which prior 5-FU exposure alleviated the senescence phenotype. In addition, the drug decreased eNOS activity and SIRT-1 level in p38 MAPK-dependent mechanism. Interestingly, although 5-FU is known to upregulate ROS release in HUVECs and induce their senescence [352], in the case of EA.hy926 cells, the overproduction of ROS did not approach suggesting that senescence of these cells was uncoupled from oxidative stress [371]. Another exciting finding that had a translational nature was the induction of SA-β-Gal in cultured EA.hy926 cells in response to sera from patients treated with capecitabine. The signaling and secretory profile in these cells changed analogically as in cells exposed to 5-FU [371].
The toxic effect of 5-FU on ECs affecting eNOS-NO may result in coronary spasms and vasoconstriction [371]. Some role in these phenomena may also be played by endothelin-1 (ET-1), the level of which was increased in angina patients receiving 5-FU, likely due to its overproduction by ECs [372]. Increased aortic content of ET-1 was also recorded in Wistar rats treated with 5-FU, and it was accompanied by increased thromboxane A2, (TXA2), another vasoconstrictive agent [373], and reduced phosphorylation of eNOS [374]. In some cellular models, such as bovine ECs, deteriorated proliferation is compensated by a simultaneous elevation of anti-thrombotic factors, like prostacyclin [375].
Vascular smooth muscle cells
Coronary vasospasms resulting from 5-FU exposure are also related to altered functioning of vascular SMCs. Rings of aorta isolated from rabbits that were subjected to 5-FU in vitro displayed vasoconstriction independent from ECs, and this effect was controlled by PKC [376]. Fludarabine, a nucleoside analog, inhibits rat SMC proliferation in vivo and neointima formation after balloon angioplasty in vivo. These activities were regulated via the inhibition of STAT-1. This research, enriched in positive results of fludarabine-eluting stents application, provided evidence that besides causing cardiac ischemia, there are some benefits from antimetabolite usage, e.g., the reduction of in-stent restenosis [377]. Potential prevention of restenosis based on the antiproliferative effect of 5-FU and cytarabine was shown in studies on cultured porcine artery SMCs [378].
Proteasome inhibitors
Proteostasis is one of the essential intracellular processes regulating the biogenesis, folding, trafficking, degradation, and turnover of proteins within a cell [379]. A protein cargo that is unfolded, misfolded, or no longer required to the cell is tagged by ubiquitin to be degraded by an ATP-dependent enzymatic system called a proteasome [380]. Malfunction proteostasis results in various pathological states, including CVS disorders [381]. Among relatively new generations of anticancer drugs are proteasome inhibitors. Some of them, especially carfilzomib (CFZ), exert cardiotoxic activity, including HF and cardiac arrhythmias [382]. The incidence of these adverse cardiovascular events in patients with multiple myeloma, to whom the proteasome inhibitors are clinically designated, reaches 3%–6% [383, 384].
Cardiomyocytes
Because of their minimal proliferative capacity, cardiomyocytes are exceptionally vulnerable to proteasome inhibition. The proteasome activity in cardiomyocytes is also higher compared with other tissues [385]. The suppression of proteasomal protein degradation and turnover leads to proteostasis disequilibrium manifested by an inappropriate accumulation of ubiquitinated proteins that gather, forming large, heterogeneous cytotoxic aggregates [386, 387]. The chymotrypsin-like proteasomal activity of CFZ was revealed in a preclinical pharmacokinetics study and linked with its potentially damaging activity toward mouse hearts at clinically relevant doses [388, 389]. Cardiotoxicity may also result from preventing mature myofibril formation in the cardiomyocytes [390].
Intracellular aggregation of polyubiquitinated proteins in cardiomyocytes triggers autophagy, evidenced in cells undergoing an experimental inhibition of the proteasome. The induction of autophagy is then considered the solution aimed at unloading the aggregate formation within the heart [391]. Molecular analysis performed on mice treated with CFZ (8 mg/kg) revealed that it causes moderate contractile dysfunction and left ventricular dilation, accompanied by the inhibition of AMP-activated protein kinase α (AMPKα) phosphorylation and inactivation of PI3K/Akt/eNOS signaling. Taking into account that AMPKα regulates autophagic degradation via suppression of mTOR complex 1 (mTORC1) [392, 393] and CFZ also downregulates Raptor phosphorylation that translates, in turn, to mTOR signaling inhibition [394], the drug appears to inhibit autophagy, which contradicts findings obtained in culture conditions [391]. At the same time, animals treated with bortezomib (BTZ) did not experience any functional cardiac injury nor altered AMPKα activation [388]. The last finding derived from in vivo experiments agrees with clinical observations pointing to a less cardiotoxic nature of BTZ compared with CFZ [395, 396]. It is also in keeping with the results of comparative analysis of CFZ, BTZ, and ixazomib (IXA), which showed that the most explicit activity on cardiomyocytes of the former is associated with its β5/β2-specific proteasome subunit inhibition pattern [397].
Another fate of cardiomyocytes (primary rat neonatal cells) exposed to CFZ and BTZ is apoptosis that proceeds time-dependently and results from attenuation of proteasomal-dependent constant sarcomeric protein turnover. Notably, when the cells were shortly preexposed to non-toxic doses of both proteosome inhibitors, their sensitivity to the damaging activity of DOX seriously increased, implying the additive mode of these drug cooperations [398].
Besides the direct impact of proteasome inhibitors on protein turnover and the consequences of its malfunction, there are other indirect effects of these drugs associated with alterations in general cellular metabolism and organelles, including mitochondria. These disturbances lead to energy deficits and defective contractility. As shown in hiPSC‐CMs exposed to CFZ (0.01–10 µM), the drug causes a dose- and time-dependent deterioration of cardiomyocyte viability combined with the augmentation of caspase 3/7 activity, suggestive of increased apoptosis. The mitochondrial origin of apoptosis confirmed diminished ΔΨm values, ATP production, mitochondrial oxidative respiration, and increased mitochondrial ROS. Altered mitochondrial metabolism coincided with decreased expression of transcripts engaged in the regulation of mitochondrial function, such as: COQ10A (coenzyme Q10A), MFN1 (mitofusin 1), MFN2 (mitofusin 2), and NDUFB5 (NADH: ubiquinone oxidoreductase subunit B8). The cells displayed impaired contractility in 3D spheroids, which was also associated with compromised Ca2+ transients and decreased integrin‐mediated traction forces. The dysfunctional contractility was possibly caused by reduced expression of genes regulating calcium handling, including SLC8A1 (solute carrier family 8 member A1), RYR2, CASQ2 (calsequestrin 2), and ATP2A2 (ATPase sarcoplasmic/endoplasmic reticulum Ca2+ transporting 2). In addition, CFZ decreased the expression of genes directly associated with cell contractions, that is MYH6 (myosin heavy chain 6) and MYL2 (myosin light chain 2) [399].
Vascular endothelial cells
Endothelial dysfunction participates in adverse cardiotoxic effects of proteasome inhibitors. Brachial artery flow-mediated dilatation allowed the demonstration that CFZ impairs endothelial function in a mechanism involving 26S proteasome activity inhibition [400]. Prothrombotic events fostering myocardial infarction, the significant negative consequence of CFZ activity [401], including thrombotic microangiopathy [402], may be related, in turn, to CFZ-dependent activation of complement, in particular, the deposition of membrane attack complex (C5b-9) on ECs [403]. Proteasome inhibitors may also indirectly exert their effects on ECs e.g., by modulating multiple myeloma cell secretome. BTZ promotes the production of extracellular vesicles (EVs) by the malignant cells, and these particles displayed decreased expression of several angiogenesis mediators, such as vascular endothelial growth factor (VEGF), interleukin 6 (IL-6), and basic fibroblast growth factor (bFGF). Moreover, these EVs suppressed the angiogenic activity of HUVECs, as evaluated using wound healing and tube formation assays. When the HUVECs were subjected to BTZ-generated EVs, they exhibited decreased NF-κB activation and attenuated secretion of autologous angiogenic agents [404]. These findings agree with the observation that BTZ also directly inhibits the proliferation of HUVECs, leading to increased apoptosis. At the level of cell cycle regulation, the drug prevented the G2/M transition and stimulated cyclin B1 and the cdc2/cyclin B complex. The effect of BTZ was likely associated with decreased secretion of proangiogenic VEGF, IL-6, insulin-like growth factor 1 (IGF1), and angiopoietin 1 (ANG1) [405]. Further research showed that the responsiveness of ECs to BTZ depends on their density. Namely, when the cells were confluent, they were resistant to the drug. However, the sub-confluent cultures reacted to BTZ in decreased angiogenic behavior. Intriguingly, the culture density also corresponded to the type of cell death elicited in those cells. In agreement with the previous report [405], sub-confluent cells displayed an increased incidence of apoptosis. In contrast, the confluent BTZ-treated cells initiated autophagy, which was preceded by increased production of ROS [406].
Research on isolated rabbit hearts and aorta also showed that CFZ affects vascular tone and reactivity, which agrees with clinical observations of its spasmogenic activity. CFZ was found to potentiate the vasospastic action elicited by KCl, noradrenaline, and angiotensin II, and impairs the vasodilation following the administration of nitroglycerin and nifedipine. Moreover, aortic strips preincubated with this drug displayed disturbed relaxation after the delivery of acetylcholine, which implies that the vasodilatory effects of CFZ proceed via an EC-dependent mechanism [407].
Vascular smooth muscle cells
Primary murine SMCs and human aortic SMCs treated with CFZ display hypocontraction and increased ROS formation [408]. The altered contractility of vascular SMCs exposed to CFZ may result from disturbed K+ channels altering the amplitude and gating (e.g., efficacy of inactivation) of delayed-rectifier K+ current in response to membrane depolarization [409]. Moreover, primary human pulmonary artery SMCs exposed to BTZ and marizomib (MRZ) displayed inhibited hypoxia-induced proliferation and increased apoptosis marked by cleaved poly (ADP-ribose) polymerase-1 (PARP1), one of the caspase’s substrates [410]. These changes could contribute to BTZ-dependent alleviation of hypoxia-induced pulmonary hypertension. This activity is consistent with the beneficial effect of BTZ on right ventricular hypertrophy and vascular remodeling in hypoxia-exposed and monocrotaline-injected rats, which was linked with inhibited NF-κB and the TGF-β/Smad signaling [411, 412]. Pulmonary artery SMCs exposed to BTZ display attenuated hypoxia-induced elevation of Ca2+ and proliferation, which coincided with the normalization of hypoxia-dependent increase in HIF-1α, bone morphogenetic protein 4 (BMP4), and the hypoxia-driven decline in peroxisome proliferator-activated receptor-γ (PPAR-γ) expression [413].
Anti-HER2 agents
The guidelines of the ASCO (2017) indicate that treatment with trastuzumab (TZM) alone, or its administration following lower doses of anthracyclines (e.g., DOX < 250 mg/m2 or EPI < 600 mg/m2), puts patients with cancer at increased risk of cardiotoxicity [4]; mainly left ventricular systolic dysfunction (LVSD) and HF [414]. These recommendations have been strengthened by later guidelines by the European Society for Medical Oncology (ESMO, 2020) [4]. As per the mechanism of TZM’s anticancer activity, it is a humanized monoclonal antibody directed against human epidermal growth factor receptor 2 (HER2) [415].The incidence of adverse cardiac effects in patients with breast cancer treated with TZM differs among clinical trials and dosage regimens and ranges from 0.7% to 7.25% [416, 417]. Another study showed that the incidence of cardiomyopathy might affect up to 30% of individuals during or following HER2-targeted treatment [418].
Cardiomyocytes
TZM reduces in cardiomyocytes the activity of HER2/neuregulin 1 (NRG1) pathway and its downstream PI3K/Akt and MAPK/Erk1/2 signaling, which are critical for cell survival [419]. Another HER2 downstream molecule that TZM targets is transcription factor E2F-1, playing an essential role in the maintenance of cardiac function [420]. ChIP-sequencing showed that the abrogation of E2F-1 cardiac tissue leads to declined expression of several genes associated with CVS development, cell growth, cardiac hypertrophy, energy metabolism, and stress response [421]. Electron microscopy examination of mice heart cardiomyocytes showed several ultrastructural alterations caused by TZM and impaired left ventricular performance [422]. The morphological disturbances within cardiac myofibers included their disconnection, stretching, and diminished thickness, which could imply inhibition of their contractile activity. This assumption was confirmed in functional observations of TZM-treated animals, which displayed declined LVEF and FS. Transcriptomic analysis revealed that this impaired cardiac function, reflected by morphological and functional indices, has a solid molecular background associated with a downregulated expression of genes regulating contractility, stress response, and adaptation to hemodynamic pressure. These included: My14, My17, Nppa, Ttn, Rxfp, Sln, Fgf12, and Fbx17 [422]. Another transcriptome sequencing report showed the downregulation of genes engaged in small molecule metabolism and cholesterol and sterol processing [423]. Specific changes also occurred within cardiomyocyte mitochondria, in particular, increased intermitochondrial distance and decreased the number of these organelles. The apparent mitochondrial dysfunction was plausibly the cause, and maybe also the secondary consequence, of increased oxidative stress, DNA damage, and apoptosis [422]. Induction of apoptosis, associated with a sharp elevation of proapoptotic Bcl-xS and declined antiapoptotic Bcl-xL, is indeed a fate of cells in which HER2 is inhibited, as shown on neonatal rat cardiomyocytes [424].
Mitochondrial dysfunction and altered cardiac energy metabolism were also recognized as the causes of disturbed contractile (decreased contraction velocity and deformed distance of monolayered cells) and Ca-handling (reduced amplitude and prolonged removal) properties of iPSC-CMs, but in contrast to the above-cited research, these effects occurred without increased ROS, apoptosis, or sarcomere disorganization [425]. A consistent view of cardiomyocyte mechanical properties also provided a study on mouse cardiomyocytes. ROS production and MDA level were increased in this case, accompanied by the loss of mitochondrial cristae, mitochondrial shrinkage, and sarcomere distortion. Mitochondrial damage was associated with decreased activity of peroxisome proliferator-activated receptor-γ coactivator 1-α (PGC1-α), a cofactor of mitochondria biogenesis [426], and mitochondrial uncoupling protein 2 (UCP2), engaged in oxidative phosphorylation management [427]. The ultimate fate of TZM-treated cardiomyocytes was apoptosis, which was also present in vivo in the animals exposed to this drug along with the increased concentration of oxidatively modified DNA and downregulated expression of DNA damage repair enzyme, 8-oxoguanine glycosylase (OGG1). The level of ferroptosis, marked by GPx4 and SLC7A11, decreased in animals exposed to TZM. However, when the ferroptosis was blocked using its specific inhibitor, the intervention alleviated TZM-related changes in cardiomyocyte mechanical and intracellular Ca2+ phenotype. Taking into account that empagliflozin, a sodium-glucose co-transporter 2 (SGLT2) inhibitor [428], efficiently attenuates TZM-induced lipid peroxidation in cardiomyocytes and their contractile defects, and that this activity was nullified by experimental ferroptosis induction, one may assume that this particular kind of cell death exerts rather negative outcomes towards cardiac tissue upon HER2 blockade [429].
As per the causative contribution of oxidative stress in TZM-mediated cardiotoxicity, the negative role of this process was evidenced in research employing curcumin, chrysin and thymoquinone, natural antioxidants, and mitochondria-protective agents [430,431,432]. These compounds were able to alleviate impaired mitochondrial metabolism and oxidative damage and reduce and recover TZM-induced cardiac toxicity in vivo and in vitro [433].
Another consequence of HER2 signaling dysregulation by TZM is the inhibition of autophagy, the process in which the recycling of damaged proteins improves the functioning and survival of cells subjected to certain stressful conditions, e.g., in cardiomyocytes undergoing pressure overload [434]. TZM induces the phosphorylation of HER1-Y845 and HER2-Y1248 and activates ERK1/2. These events lead to the initiation of the mTOR-Ulk1 pathway, which inhibits autophagosome formation, decreasing the levels of effectory proteins Atg 5–12, Atg 7, Atg 14, and Beclin 1. The antiautophagic activity represented by TZM was not shared by another humanized monoclonal antibody, pertuzumab [435], also known to increase the risk of HF in patients with HER2-positive cancer [436]. The issue of TZM-dependent changes in autophagy may be, however, a bit more complex than initially thought. Experiments conducted on iPSC‐CMs showed that the direction of this process might depend on the drug concentration. At a low dose of 1 μM, TZM suppressed the autophagy, whereas at higher doses of 10 μM a significant augmentation of this process was found, which is linked by the authors of this study with higher production of ROS upon 10 μM of TZM [437]. Further transcriptomic analysis of cells exposed to lower doses of TZM showed that it induces an inflammation-like state, as evidenced according to upregulated expression levels of IL1β, TNFRSF8, and PTGS1, oversecreted kallikrein 5 (KLK5) and 8 (KLK8), and increased production of KLK5/KLK8 substrate, PAR2. Moreover, TZM promoted the phosphorylation of ERK1/2 and JNK. Considering the role of these kinases in proinflammatory signals arising in response to PAR2 activation [438, 439], their contribution to the formation of the inflammatory milieu in TZM-treated cardiomyocytes is indisputable [437]. TZM-driven inflammatory conditions confirmed research on rabbits where the drug caused myocardium infiltration with lymphocytes and macrophages [440].
Last, but not least, the synergism between TZM and DOX, yielding cardiotoxicity in patients undergoing combination therapy, is associated with the fact that the HER2 inhibitor is capable of inhibiting, similarly to DOX [176], the activity of Top2B in cardiomyocytes. As a result, DDR is initiated and manifested by the accumulation of DNA double-strand breaks (γ-H2A.X foci) and increased phosphorylation of ataxia telangiectasia and Rad3-related protein (ATR) in cells subjected to TZM. When TZM and DOX were added to cardiomyocytes, the inhibitory effect on Top2B, proliferation, oxidative stress, and apoptosis were remarkably stronger than when the drugs acted separately. Finally, the unique observation was that DOX upregulated the level of HER2 and its downstream signaling in cardiomyocytes, thus sensitizing them to TZM [441]. DOX toxicity was also intensified in hPSC-CMs cardiomyocytes treated with another HER2 inhibitor, lapatinib. The etiology of this synergism was linked with the upregulation of inducible NOS (iNOS) and the overproduction of NO. These findings were confirmed in vivo when the delivery of an iNOS inhibitor in mice subjected to lapatinib and DOX ameliorated myocardial apoptosis and systolic dysfunction [442]. Similarly, as in the case of DOX, TZM was also found to aggravate cardiotoxicity caused by IR, which was evidenced in H9C2 cardiomyocytes. The cells undergoing concurrent TZM and IR displayed increased DNA damage, ROS release, and apoptosis, and this exacerbation of toxicity was associated with inhibited phosphorylation of Akt [49].
Vascular endothelial cells
Overexpression of HER2 in breast cancer cells is strongly associated with increased angiogenesis and VEGF expression. TZM, affecting HER2, was found to inhibit the expression of VEGF, thus limiting the supply of nutrients and oxygen to malignant tissue [443]. Apart from this purely anticancer activity of TZM, its action also deteriorates ECs functioning, which may participate in cardio- and vasotoxicity in cancer survivors. TZM interferes with HER2 dimerization, and EC contribution to this process is associated with the endothelial origin of the natural ligand, which is required for the dimerization, that is, NRG-1 [293]. Direct exposure of ECs to TZM resulted in their increased adhesion to fibronectin, which was accompanied by decreased angiogenic behavior marked by their proliferation and invasion. Moreover, the cells displayed a reduced ability to synthesize heparan sulfate proteoglycans, including perlecan [444]. Since arterial heparan sulfate negatively correlates with tissue cholesterol [445], the above findings may imply that TZM causes proatherosclerotic vascular wall remodeling. As per perlecan, which is a significant heparan sulfate in the basement membrane interacting with ECM proteins and growth factors (e.g., VEGF, FGF, PDGF) [446], its deficiency was found to affect endothelium-dependent relaxation, likely due to decreased eNOS mRNA and protein [447]. These findings may indicate that TZM may also reduce NO production by ECs. The bioavailability of this major vasorelaxant is increased through the activation of protein kinase B (PKB), which participates in HER2 and HER4 receptor dimerization [448]. TZM inhibits this dimerization and restricts the cardioprotective actions of NRG-1 [449], and the suppression of the eNOS-NO axis translates to vasodilator tone deregulation.
Vascular smooth muscle cells
Vascular disorders like atherosclerosis [450] and hypertension [451, 452] are reported CVS complications in patients with breast cancer treated with TZM or TZM combined with anthracyclines. At the same time, the impaired biology of vascular SMCs is undoubtedly a pathophysiological element contributing to the initiation and progression of these pathologies [128, 453]. Despite these indications, the literature lacks experimental data linking SMC exposure to TZM and the development of the above-mentioned abnormalities.
Immune checkpoint inhibitors (ICIs)
Cancer therapy using ICIs represents an antibody-oriented targeted approach primarily focused on restoring the anticancer potency of T cells. ICIs are designed to block molecular targets engaged in T-cell activity suppression and immune tolerance, such as cytotoxic T-lymphocyte antigen 4 (CTLA-4) and programmed cell death 1 (PD-1) ligand 1 (PD-L1) system [454]. Despite enormous success in employing various ICIs in oncology, hyperstimulation of the immune system causes considerable toxicity toward normal cells, including those forming the CVS [455]. Moreover, ICIs are responsible for a wide range of non-inflammatory CVS abnormalities, such as Takotsubo-like syndrome, arrythmias, cardiomyopathy, arterial vascular disease, venous thromboembolism, pulmonary hypertension, myocardial infarction, and pericardial disease [15, 455]. Of the listed ICIs-driven perturbations, myocarditis is the most common [456]. The development of monoclonal antibodies against immune checkpoints was initiated by those counteracting CTLA-4 (Ipilimumab) [457]. Afterward, antibodies blocking PD-1 (e.g., Nivolumab, Pembrolizumab) and PD-L1 (e.g., Atezolizumab) were developed, tested, and approved, which was followed by the development of next generations of ICIs targeting other elements of immune checkpoint system, such as PD-L2, TIM-3, LAG-3, TIGIT, BTLA, and VISTA [458]. Notably, patients with cancer treated with a combination of two ICIs, which strategy is known to potentiate positive clinical outcomes in several kinds of tumors [459], display increased frequency and severity of cardiotoxicity compared with those subjected to a monotherapy [460].
Cardiomyocytes
It cannot be excluded that cardiomyocytes resemble cancer cells in utilizing CTLA-4 and PD-1/PD-L1 mechanisms to restrict T-cell-dependent hyperactivation of the immune reaction. If so, ICIs may relieve T-cell suppression leading to excessive CD8+ T-cell activity within the heart and cardiotoxicity. In fact, PD-1 and PD-L1 are expressed in cardiomyocytes and CTLA-4 and PD-1 deletion in an animal model results in autoimmune myocarditis [461,462,463,464]. Endomyocardial biopsy in patients subjected to ICIs revealed inflammatory infiltration of the heart muscle, mainly by CD8+ T cells, with a smaller admixture of CD68+ or CD163+ macrophages and CD4+ T cells [465,466,467]. This effect was accompanied by cardiomyocyte necrosis, myofibrillar degeneration, and sarcoplasmic tubular dilatation [467]. Necrotic cardiomyocytes are often positive for C4d, indicating the contribution of the activated complement pathway [466]. Cardiomyocytes cocultured with peripheral blood lymphocytes and exposed to ipilimumab or nivolumab confirmed exacerbated inflammatory response, as evidenced according to the stimulation of p65 NF-κB, MyD88, and Nlrp3 inflammasome, as well as increased production of IL-1β, IL-6, IL-8, and TGF-β1. The cell viability was markedly decreased. The effects exerted in response to anti-CTLA-4 antibodies were more pronounced than those associated with PD-1 blockade [468]. Cardiomyocyte apoptosis was seen in C57/BL6J mice treated with a combination of anti-PD-1 and anti-CTLA-4. RNA sequencing showed increased expression of genes coding for oxidative stress and decreased expression of heart-specific transcripts, such as mesencephalic astrocyte-derived neurotrophic factor and heat shock 70-kDa protein 5 [469]. Another study utilizing BALB/c mice revealed that ICIs-related myocarditis proceeds with increased cardiomyocyte autophagy [470].
Vascular endothelial cells
ECs are susceptible to PD-1/PD-L1 axis modulation, and PD-L1 is induced on ECs in response to proinflammatory stimuli [471]. Endothelial expression of PD-L1 within the myocardium in cardiac patients was increased compared with the control group, and this augmentation was more pronounced in those individuals who earlier experienced myocardial infarction. Significantly, the level of PD-L1 appeared to negatively correlate with LVEF and positively correlate with left ventricular end-diastolic volume [472]. Experiments on mice showed that during CD8 + T-cell-induced myocarditis, IFNγ produced by T cells was responsible for the upregulation of PD-L1 on ECs, and the inhibition of this cytokine worsened clinical picture of the disease. An antibody-based inhibition of PD-L1 converted transient myocarditis to lethal disease delivering evidence that endothelial PD-L1 is pivotal for control of immune-mediated cardiotoxicity [462]. Inhibition of CTLA-4 also promotes proinflammatory EC activation, as demonstrated according to increased expression of ICAM-1 in aortic cells. This outcome corresponded to the increased formation of atherosclerotic plaques, especially in the aortic arch of experimental animals [473].
Vascular smooth muscle cells
As mentioned earlier, ICIs may predispose an individual to atherosclerosis development. Preclinical studies on mice revealed that anti-CTLA-4 antibody administration decreases the content of SMCs within atherosclerotic lesions, which is suggestive of a reduced plaque stability [473]. Experiments on animals revealed, in turn, that PD-L1 is expressed in SMCs of the thickened intima in the graft coronary arteries, and the antibodies against PD-L1 promote the progression of graft arterial disease. The administration of anti-PD-L1 antibodies intensified the extent of inflammation, as estimated according to increased IFNγ and TNFα levels in cardiac allografts. Subsequent in vitro tests showed that PD-L1 expression in SMCs increased upon exposure to IFNγ levels, along with their proliferation [474].
An opposite side of cardiooncology, or the effect of cardiologic drugs on cancer cells
Although cardiooncology is classically viewed as a discipline focused on CVS disorders in oncologic patients, it may also describe the effects of cardiologic drugs in patients with cancer and malignant cells. At the same time, this way of thinking about cardiooncology is not yet well-rooted in basic research, and its clinical significance has not yet been sufficiently recognized and appreciated.
Acetylsalicylic acid
Acetylsalicylic acid (AA, Aspirin) is an irreversible inhibitor of two isoforms of cyclooxygenase (COX), COX-1 and COX-2 [475]. COX-1 is an enzyme that produces thromboxane A2 (TXA2) in platelets, promoting their aggregation. COX-2 plays a vital role during inflammation, generating prostaglandin E2 (PGE2). AA is used in secondary prevention of cardiovascular events, e.g., myocardial infarction and ischemic stroke [476], reducing clot risk. There is evidence to suggest an impact of platelets on cancer cells. Namely, they can prevent cancer cells from being recognized by the immune system [477], promoting cell proliferation and facilitating migration [478]. Moreover, AA can induce apoptotic mechanisms by increasing Bax and decreasing Bcl-2 gene expression [479]. Inflammatory processes play an essential role in carcinogenesis [480], and PGE2 intensifies tumor growth and angiogenesis [481]. On the other hand, AA inhibits the overexpression of the COX-2 gene in colon cancer cells, which translates to reduced inflammation [479]. This effect may underlie the decreased risk of colorectal cancer in patients who received AA [482]. Regular use of this drug also reduced the risk of esophageal cancer, gastric cancer, breast cancer, and prostate cancer [483], as well as diminished mortality of patients with colorectal cancer [484].
Cardiac glycosides
Cardiac glycosides are used in the treatment of congestive HF and atrial fibrillation when the ventricular rate increases. The effect of glycosides is to increase cardiac output, reduce the heart rate, and slow the conduction of the atrioventricular node. Cardiac glycosides bind to sodium- and potassium-activated adenosine triphosphatase (Na + K + ATPase) and regulate cell membrane electrical potential. Increasing intracellular Ca2+ and Na+, cardiac glycosides can induce apoptosis in cancer cells [485, 486]. Earlier studies suggested cytotoxic and antiproliferative effects of cardiac glycosides in cells of breast cancer, renal cancer, lung cancer, prostate cancer, melanoma, leukemia, and neuroblastoma [487]. On the other hand, there is also a report demonstrating a higher risk of breast cancer in cardiac glycoside users, which may be associated with the estrogen-like activity of these drugs. In addition, an increase in all-cause mortality in the group that used cardiac glycosides was found. The difference between the results of earlier preclinical studies and clinical trials is possibly due to the use of too high concentrations of cardiac glycosides in experiments in vitro, which are impossible to be reached in the human organism in vivo [488].
Statins
Statins are a group of drugs used to reduce low-density lipoprotein cholesterol (LDL-C) levels in the primary and secondary prevention of atherosclerotic cardiovascular disease (ASCVD) [489]. These drugs are primarily used to treat hypercholesterolemia and hypertriglyceridemia and are one of the cornerstones in the treatment of cardiovascular diseases. The primary mechanism of action of statins is the early suppression of hepatic cholesterol production through competitive and reversible inhibition of 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase. By this mechanism, statins inhibit mevalonate biosynthesis from HMG-CoA. The consequence of this action is inhibiting the production of non-steroidal derivatives of mevalonate, such as farnesyl pyrophosphate and geranyl–geranyl phosphate. These isoprenoid compounds activate signaling proteins, especially G proteins (Rho, Rac, Ras), which allow proteins to attach to the cell membrane and interact with other proteins, causing disturbances in proliferation, migration, cytoskeleton function, and death [490]. Experimental studies have shown that statins inhibit the progression and induce apoptosis in breast cancer cells and esophageal adenocarcinoma cells [491, 492]. Clinical trials confirm the protective effect of statins by showing a reduced risk of gastric and esophageal cancers [493, 494]. They also appeared to reduce colorectal and breast cancer mortality [495, 496].
ACEIs/ARBs
Renin–angiotensin system (RAS) undergoes inhibition by angiotensin-converting enzyme inhibitors (ACE-Is) and angiotensin II receptor blockers (ARBs). ACE converts angiotensin I into angiotensin II, which is a vasoconstrictor. ARBs blocking AT1 receptors inhibit angiotensin II. Both groups of drugs suppress the RAS, regulating vascular function and blood volume, which leads to decreased blood pressure. Experimental data showed local expression components of the RAS in brain, lung, breast, prostate, and pancreatic cancer cells [497]. A metaanalysis of 55 studies showed a significant relationship between RAS inhibition and patients with cancer overall survival, progression-free survival, and disease-free survival [498]. Sub-analysis, according to the RAS inhibitory group, showed that the effects of ARBs are considerably more robust than those of ACEI [498].
Beta blockers
Beta-adrenergic receptor blockers are a heterogeneous group of drugs that inhibit the excessive activity of the sympathetic nervous system, recommended for the treatment of arrhythmias, coronary heart disease, HF, and hypertension. Experimental studies showed that increased sympathetic nervous system activity may promote cancer development [499]. Conversely, metaanalyses of clinical trials showed no conclusive results about using beta-adrenergic receptor blockers in patients with cancer. Overall survival, all-cause mortality, disease-free survival, progression-free survival, and recurrence-free survival did not differ significantly among the beta-adrenergic receptor blockers group [500]. Nonetheless, in some types of cancers, including ovarian cancer, pancreatic cancer, and melanoma, an improvement in overall survival was found in the beta-adrenergic receptor blockers group [500].
Conclusions and future directions
Generally speaking, the roots of cardiooncology come from clinical observations, and the same source determines the decision-making process regarding therapeutic management of oncology patients who developed cardiovascular complications. At the same time, knowledge of the pathomechanisms of these disorders derives from basic research on cellular and animal models. As this paper shows, CVS cellular and molecular mechanisms dysfunctions are well understood and explored down to the level of mediators and signaling pathways. On the other hand, specific issues still need to be clarified, especially where observations of the outcomes of particular drugs have been inconclusive. An excellent way to get meaningful findings will be to optimize research methods. For example, it seems desirable to increase the share of studies using animal organisms, tissue isolates, 3D cultures, and even cocultures, which have a significant advantage over isolated cellular models. The other aspect is the diversity of cell types engaged in therapy-induced cardiotoxicity. In this review, we arbitrarily selected three major types of cells. At the same time, we skipped discussing the role of other types, such as cardiac progenitor cells and fibroblasts, mesenchymal stem cells, and bone marrow cells, whose dysfunction may also be caused by radiation or drugs, and thus may also affect the functioning of the entire CVS. Last, but not least, much more attention must be paid to clinically relevant doses of IR and therapeutics utilized in vitro and in vivo, as the cellular and animal reactions to those stressors discussed in this article undoubtedly depend on their doses and/or times of exposure.
Availability of data and materials
Not applicable.
Abbreviations
- 5-FU:
-
5-Fluorouracil
- AA:
-
Acetylsalicylic acid
- ACT:
-
Anthracycline‐induced cardiotoxicity
- ACE-Is:
-
Angiotensin-converting enzyme inhibitors
- ARBs:
-
Angiotensin II receptor blockers
- BAEC:
-
Bovine aortic endothelial cells
- BTZ:
-
Bortezomib
- CFZ:
-
Carfilzomib
- CIS:
-
Cisplatin
- CPT:
-
Carboplatin
- CTLA-4:
-
Cytotoxic T lymphocyte-associated protein-4
- CVD:
-
Cardiovascular disease
- CVS:
-
Cardiovascular system
- DAMPs:
-
Damage-associated molecular patterns
- DCT:
-
Docetaxel
- DDR:
-
DNA damage response
- DOX:
-
Doxorubicin
- HDMECs:
-
Dermal microvascular endothelial cells
- ECs:
-
Endothelial cells
- eNOS:
-
Endothelial nitric oxide synthase
- EPI:
-
4′-Epidoxorubicin
- hiPSC-CMs:
-
Human induced pluripotent stem cell-derived cardiomyocytes
- HF:
-
Heart failure
- HCAEC:
-
Human coronary artery endothelial cells
- HER2:
-
Human epidermal growth factor receptor 2
- HMEC:
-
Human microvascular endothelial cells
- HUVECs:
-
Human umbilical vein endothelial cells
- ICIs:
-
Immune checkpoint inhibitors
- IR:
-
Ionizing radiation
- LVDP:
-
Left ventricular developed pressure
- LVEF:
-
Left ventricular ejection fraction
- LVSD:
-
Left ventricular systolic dysfunction
- mPTP:
-
Mitochondrial permeability transition pores
- NCX:
-
Na+/Ca2+ exchanger
- NO:
-
Nitic oxide
- NOX:
-
NADPH oxidase
- PCIs:
-
Percutaneous coronary interventions
- PCT:
-
Paclitaxel
- PD-1:
-
Programmed cell death protein-1
- PD-L1:
-
Programmed cell death 1 ligand-1
- RAS:
-
Renin–angiotensin system
- RIHD:
-
Radiation-induced heart disease
- ROS:
-
Reactive oxygen species
- RyR:
-
Ryanodine receptor
- SA-β-Gal:
-
Senescence-associated β-galactosidase
- SASP:
-
Senescence-associated secretory phenotype
- Top2B:
-
Topoisomerase IIB
- TZM:
-
Trastuzumab
- VSMCs:
-
Vascular smooth muscle cells
References
Miller KD, Nogueira L, Mariotto AB, Rowland JH, Yabroff KR, Alfano CM, et al. Cancer treatment and survivorship statistics, 2019. CA Cancer J Clin. 2019;69(5):363–85.
Majeed H, Gupta V. Adverse effects of radiation therapy. StatPearls. Treasure Island (FL)2022.
Albano D, Benenati M, Bruno A, Bruno F, Calandri M, Caruso D, et al. Imaging side effects and complications of chemotherapy and radiation therapy: a pictorial review from head to toe. Insights Imaging. 2021;12(1):76.
Alexandre J, Cautela J, Ederhy S, Damaj GL, Salem JE, Barlesi F, et al. Cardiovascular toxicity related to cancer treatment: a pragmatic approach to the American and European cardio-oncology guidelines. J Am Heart Assoc. 2020;9(18): e018403.
Strongman H, Gadd S, Matthews A, Mansfield KE, Stanway S, Lyon AR, et al. Medium and long-term risks of specific cardiovascular diseases in survivors of 20 adult cancers: a population-based cohort study using multiple linked UK electronic health records databases. Lancet. 2019;394(10203):1041–54.
Dhir AA, Sawant SP. Cardiac morbidity and mortality in patients with breast cancer: a review. Indian J Med Res. 2021;154(2):199–209.
Oeffinger KC, Mertens AC, Sklar CA, Kawashima T, Hudson MM, Meadows AT, et al. Chronic health conditions in adult survivors of childhood cancer. N Engl J Med. 2006;355(15):1572–82.
Moslehi J. The cardiovascular perils of cancer survivorship. N Engl J Med. 2013;368(11):1055–6.
Koutsoukis A, Ntalianis A, Repasos E, Kastritis E, Dimopoulos MA, Paraskevaidis I. Cardio-oncology: a focus on cardiotoxicity. Eur Cardiol. 2018;13(1):64–9.
Adams MJ, Lipshultz SE, Schwartz C, Fajardo LF, Coen V, Constine LS. Radiation-associated cardiovascular disease: manifestations and management. Semin Radiat Oncol. 2003;13(3):346–56.
Senkus-Konefka E, Jassem J. Cardiovascular effects of breast cancer radiotherapy. Cancer Treat Rev. 2007;33(6):578–93.
van den Belt-Dusebout AW, Nuver J, de Wit R, Gietema JA, ten Bokkel Huinink WW, Rodrigus PT, et al. Long-term risk of cardiovascular disease in 5-year survivors of testicular cancer. J Clin Oncol. 2006;24(3):467–75.
Lenneman CG, Sawyer DB. Cardio-oncology: an update on cardiotoxicity of cancer-related treatment. Circ Res. 2016;118(6):1008–20.
Koelwyn GJ, Jones LW, Moslehi J. Unravelling the causes of reduced peak oxygen consumption in patients with cancer: complex, timely, and necessary. J Am Coll Cardiol. 2014;64(13):1320–2.
Herrmann J. Adverse cardiac effects of cancer therapies: cardiotoxicity and arrhythmia. Nat Rev Cardiol. 2020;17(8):474–502.
Trager LE, Lyons M, Kuznetsov A, Sheffield C, Roh K, Freeman R, et al. Beyond cardiomyocytes: cellular diversity in the heart’s response to exercise. J Sport Health Sci. 2022.
Lilly B. We have contact: endothelial cell-smooth muscle cell interactions. Physiology (Bethesda). 2014;29(4):234–41.
Nielsen KM, Offersen BV, Nielsen HM, Vaage-Nilsen M, Yusuf SW. Short and long term radiation induced cardiovascular disease in patients with cancer. Clin Cardiol. 2017;40(4):255–61.
Stewart FA, Seemann I, Hoving S, Russell NS. Understanding radiation-induced cardiovascular damage and strategies for intervention. Clin Oncol (R Coll Radiol). 2013;25(10):617–24.
Baselet B, Rombouts C, Benotmane AM, Baatout S, Aerts A. Cardiovascular diseases related to ionizing radiation: the risk of low-dose exposure (Review). Int J Mol Med. 2016;38(6):1623–41.
Stewart FA. Mechanisms and dose-response relationships for radiation-induced cardiovascular disease. Ann ICRP. 2012;41(3–4):72–9.
Howe GR, Zablotska LB, Fix JJ, Egel J, Buchanan J. Analysis of the mortality experience amongst U.S. nuclear power industry workers after chronic low-dose exposure to ionizing radiation. Radiat Res. 2004;162(5):517–26.
Germanguz I, Sedan O, Zeevi-Levin N, Shtrichman R, Barak E, Ziskind A, et al. Molecular characterization and functional properties of cardiomyocytes derived from human inducible pluripotent stem cells. J Cell Mol Med. 2011;15(1):38–51.
Becker BV, Seeger T, Beiert T, Antwerpen M, Palnek A, Port M, et al. Impact of ionizing radiation on electrophysiological behavior of human-induced ipsc-derived cardiomyocytes on multielectrode arrays. Health Phys. 2018;115(1):21–8.
Errahmani MY, Locquet M, Spoor D, Jimenez G, Camilleri J, Bernier MO, et al. Association between cardiac radiation exposure and the risk of arrhythmia in breast cancer patients treated with radiotherapy: a case-control study. Front Oncol. 2022;12: 892882.
Chang HM, Okwuosa TM, Scarabelli T, Moudgil R, Yeh ETH. Cardiovascular complications of cancer therapy: best practices in diagnosis, prevention, and management: part 2. J Am Coll Cardiol. 2017;70(20):2552–65.
Schultz-Hector S, Trott KR. Radiation-induced cardiovascular diseases: is the epidemiologic evidence compatible with the radiobiologic data? Int J Radiat Oncol Biol Phys. 2007;67(1):10–8.
Mulrooney DA, Yeazel MW, Kawashima T, Mertens AC, Mitby P, Stovall M, et al. Cardiac outcomes in a cohort of adult survivors of childhood and adolescent cancer: retrospective analysis of the Childhood Cancer Survivor Study cohort. BMJ. 2009;339: b4606.
Sdek P, Zhao P, Wang Y, Huang CJ, Ko CY, Butler PC, et al. Rb and p130 control cell cycle gene silencing to maintain the postmitotic phenotype in cardiac myocytes. J Cell Biol. 2011;194(3):407–23.
Pfeiffer MJ, Quaranta R, Piccini I, Fell J, Rao J, Ropke A, et al. Cardiogenic programming of human pluripotent stem cells by dose-controlled activation of EOMES. Nat Commun. 2018;9(1):440.
Baljinnyam E, Venkatesh S, Gordan R, Mareedu S, Zhang J, Xie LH, et al. Effect of densely ionizing radiation on cardiomyocyte differentiation from human-induced pluripotent stem cells. Physiol Rep. 2017;5(15).
Takeda M, Ito E, Minami K, Harada A, Mochizuki-Oda N, Sawa Y, et al. Elimination of residual undifferentiated induced pluripotent stem cells (iPSCs) using irradiation for safe clinical applications of iPSC-derived cardiomyocytes. Biochem Biophys Res Commun. 2021;574:91–6.
Inui S, Minami K, Ito E, Imaizumi H, Mori S, Koizumi M, et al. Irradiation strongly reduces tumorigenesis of human induced pluripotent stem cells. J Radiat Res. 2017;58(4):430–8.
Johnson DM, Antoons G. Arrhythmogenic mechanisms in heart failure: linking beta-adrenergic stimulation, stretch, and calcium. Front Physiol. 2018;9:1453.
Sag CM, Wolff HA, Neumann K, Opiela MK, Zhang J, Steuer F, et al. Ionizing radiation regulates cardiac Ca handling via increased ROS and activated CaMKII. Basic Res Cardiol. 2013;108(6):385.
Shin E, Ko KS, Rhee BD, Han J, Kim N. Different effects of prolonged beta-adrenergic stimulation on heart and cerebral artery. Integr Med Res. 2014;3(4):204–10.
Pizzino G, Irrera N, Cucinotta M, Pallio G, Mannino F, Arcoraci V, et al. Oxidative stress: harms and benefits for human health. Oxid Med Cell Longev. 2017;2017:8416763.
Panda P, Verma HK, Lakkakula S, Merchant N, Kadir F, Rahman S, et al. Biomarkers of oxidative stress tethered to cardiovascular diseases. Oxid Med Cell Longev. 2022;2022:9154295.
Sabbatino F, Conti V, Liguori L, Polcaro G, Corbi G, Manzo V, et al. Molecules and mechanisms to overcome oxidative stress inducing cardiovascular disease in cancer patients. Life (Basel). 2021;11(2):105.
Kim W, Lee S, Seo D, Kim D, Kim K, Kim E, et al. Cellular stress responses in radiotherapy. Cells. 2019;8(9):1105.
Azzam EI, Jay-Gerin JP, Pain D. Ionizing radiation-induced metabolic oxidative stress and prolonged cell injury. Cancer Lett. 2012;327(1–2):48–60.
Blakely EL, Mitchell AL, Fisher N, Meunier B, Nijtmans LG, Schaefer AM, et al. A mitochondrial cytochrome b mutation causing severe respiratory chain enzyme deficiency in humans and yeast. FEBS J. 2005;272(14):3583–92.
Mai N, Chrzanowska-Lightowlers ZM, Lightowlers RN. The process of mammalian mitochondrial protein synthesis. Cell Tissue Res. 2017;367(1):5–20.
Zhang S, Wen G, Huang SX, Wang J, Tong J, Hei TK. Mitochondrial alteration in malignantly transformed human small airway epithelial cells induced by alpha-particles. Int J Cancer. 2013;132(1):19–28.
Xu P, Yi Y, Luo Y, Liu Z, Xu Y, Cai J, et al. Radiation-induced dysfunction of energy metabolism in the heart results in the fibrosis of cardiac tissues. Mol Med Rep. 2021;24(6).
Burch GE, Sohal RS, Sun SC, Miller GC, Colcolough HL. Effects of radiation on the human heart. An electron microscopic study. Arch Intern Med. 1968;121(3):230–4.
Zhao RZ, Jiang S, Zhang L, Yu ZB. Mitochondrial electron transport chain, ROS generation and uncoupling (Review). Int J Mol Med. 2019;44(1):3–15.
Wagner S, Ruff HM, Weber SL, Bellmann S, Sowa T, Schulte T, et al. Reactive oxygen species-activated Ca/calmodulin kinase IIdelta is required for late I(Na) augmentation leading to cellular Na and Ca overload. Circ Res. 2011;108(5):555–65.
Yi P, Li H, Su J, Cai J, Xu C, Chen J, et al. Trastuzumab aggravates radiation induced cardiotoxicity in mice. Am J Cancer Res. 2022;12(1):381–95.
Fan GC, Zhou X, Wang X, Song G, Qian J, Nicolaou P, et al. Heat shock protein 20 interacting with phosphorylated Akt reduces doxorubicin-triggered oxidative stress and cardiotoxicity. Circ Res. 2008;103(11):1270–9.
Rochette L, Guenancia C, Gudjoncik A, Hachet O, Zeller M, Cottin Y, et al. Anthracyclines/trastuzumab: new aspects of cardiotoxicity and molecular mechanisms. Trends Pharmacol Sci. 2015;36(6):326–48.
Salata C, Ferreira-Machado SC, De Andrade CB, Mencalha AL, Mandarim-De-Lacerda CA, de Almeida CE. Apoptosis induction of cardiomyocytes and subsequent fibrosis after irradiation and neoadjuvant chemotherapy. Int J Radiat Biol. 2014;90(4):284–90.
Wang B, Wang H, Zhang M, Ji R, Wei J, Xin Y, et al. Radiation-induced myocardial fibrosis: mechanisms underlying its pathogenesis and therapeutic strategies. J Cell Mol Med. 2020;24(14):7717–29.
Rosenkranz S, Flesch M, Amann K, Haeuseler C, Kilter H, Seeland U, et al. Alterations of beta-adrenergic signaling and cardiac hypertrophy in transgenic mice overexpressing TGF-beta(1). Am J Physiol Heart Circ Physiol. 2002;283(3):H1253–62.
Johnston EF, Gillis TE. Transforming growth factor beta-1 (TGF-beta1) stimulates collagen synthesis in cultured rainbow trout cardiac fibroblasts. J Exp Biol. 2017;220(Pt 14):2645–53.
Siddiqui MS, Francois M, Fenech MF, Leifert WR. Persistent gammaH2AX: a promising molecular marker of DNA damage and aging. Mutat Res Rev Mutat Res. 2015;766:1–19.
Rossiello F, Herbig U, Longhese MP, Fumagalli M, d’Addadi Fagagna F. Irreparable telomeric DNA damage and persistent DDR signalling as a shared causative mechanism of cellular senescence and ageing. Curr Opin Genet Dev. 2014;26:89–95.
Huang W, Hickson LJ, Eirin A, Kirkland JL, Lerman LO. Cellular senescence: the good, the bad and the unknown. Nat Rev Nephrol. 2022;18(10):611–27.
Ohtani N. The roles and mechanisms of senescence-associated secretory phenotype (SASP): can it be controlled by senolysis? Inflamm Regen. 2022;42(1):11.
Zeng Z, Xu P, He Y, Yi Y, Liu Z, Cai J, et al. Acetylation of Atp5f1c mediates cardiomyocyte senescence via metabolic dysfunction in radiation-induced heart damage. Oxid Med Cell Longev. 2022;2022:4155565.
You H, Li Q, Kong D, Liu X, Kong F, Zheng K, et al. The interaction of canonical Wnt/beta-catenin signaling with protein lysine acetylation. Cell Mol Biol Lett. 2022;27(1):7.
Li P, Ge J, Li H. Lysine acetyltransferases and lysine deacetylases as targets for cardiovascular disease. Nat Rev Cardiol. 2020;17(2):96–115.
Srivastava AP, Luo M, Zhou W, Symersky J, Bai D, Chambers MG, et al. High-resolution cryo-EM analysis of the yeast ATP synthase in a lipid membrane. Science. 2018;360(6389):eaas9699.
Venkatesulu BP, Mahadevan LS, Aliru ML, Yang X, Bodd MH, Singh PK, et al. Radiation-induced endothelial vascular injury: a review of possible mechanisms. JACC Basic Transl Sci. 2018;3(4):563–72.
Milliat F, Francois A, Isoir M, Deutsch E, Tamarat R, Tarlet G, et al. Influence of endothelial cells on vascular smooth muscle cells phenotype after irradiation: implication in radiation-induced vascular damages. Am J Pathol. 2006;169(4):1484–95.
Li J, De Leon H, Ebato B, Cui J, Todd J, Chronos NA, et al. Endovascular irradiation impairs vascular functional responses in noninjured pig coronary arteries. Cardiovasc Radiat Med. 2002;3(3–4):152–62.
Taunk NK, Haffty BG, Kostis JB, Goyal S. Radiation-induced heart disease: pathologic abnormalities and putative mechanisms. Front Oncol. 2015;5:39.
Paris F, Fuks Z, Kang A, Capodieci P, Juan G, Ehleiter D, et al. Endothelial apoptosis as the primary lesion initiating intestinal radiation damage in mice. Science. 2001;293(5528):293–7.
Frankowska N, Lisowska K, Witkowski JM. Proteolysis dysfunction in the process of aging and age-related diseases. Front Aging. 2022;3: 927630.
Tang X, Li PH, Chen HZ. Cardiomyocyte senescence and cellular communications within myocardial microenvironments. Front Endocrinol (Lausanne). 2020;11:280.
Dong X, Tong F, Qian C, Zhang R, Dong J, Wu G, et al. NEMO modulates radiation-induced endothelial senescence of human umbilical veins through NF-kappaB signal pathway. Radiat Res. 2015;183(1):82–93.
Kim KS, Kim JE, Choi KJ, Bae S, Kim DH. Characterization of DNA damage-induced cellular senescence by ionizing radiation in endothelial cells. Int J Radiat Biol. 2014;90(1):71–80.
Panganiban RA, Day RM. Inhibition of IGF-1R prevents ionizing radiation-induced primary endothelial cell senescence. PLoS ONE. 2013;8(10): e78589.
Sandor N, Walter FR, Bocsik A, Santha P, Schilling-Toth B, Lener V, et al. Low dose cranial irradiation-induced cerebrovascular damage is reversible in mice. PLoS ONE. 2014;9(11): e112397.
McRobb LS, McKay MJ, Gamble JR, Grace M, Moutrie V, Santos ED, et al. Ionizing radiation reduces ADAM10 expression in brain microvascular endothelial cells undergoing stress-induced senescence. Aging (Albany NY). 2017;9(4):1248–68.
Lafargue A, Degorre C, Corre I, Alves-Guerra MC, Gaugler MH, Vallette F, et al. Ionizing radiation induces long-term senescence in endothelial cells through mitochondrial respiratory complex II dysfunction and superoxide generation. Free Radic Biol Med. 2017;108:750–9.
Herbig U, Jobling WA, Chen BP, Chen DJ, Sedivy JM. Telomere shortening triggers senescence of human cells through a pathway involving ATM, p53, and p21(CIP1), but not p16(INK4a). Mol Cell. 2004;14(4):501–13.
Ramirez RD, Morales CP, Herbert BS, Rohde JM, Passons C, Shay JW, et al. Putative telomere-independent mechanisms of replicative aging reflect inadequate growth conditions. Genes Dev. 2001;15(4):398–403.
Ungvari Z, Podlutsky A, Sosnowska D, Tucsek Z, Toth P, Deak F, et al. Ionizing radiation promotes the acquisition of a senescence-associated secretory phenotype and impairs angiogenic capacity in cerebromicrovascular endothelial cells: role of increased DNA damage and decreased DNA repair capacity in microvascular radiosensitivity. J Gerontol A Biol Sci Med Sci. 2013;68(12):1443–57.
Heo JI, Kim W, Choi KJ, Bae S, Jeong JH, Kim KS. XIAP-associating factor 1, a transcriptional target of BRD7, contributes to endothelial cell senescence. Oncotarget. 2016;7(5):5118–30.
Hayashi T, Matsui-Hirai H, Miyazaki-Akita A, Fukatsu A, Funami J, Ding QF, et al. Endothelial cellular senescence is inhibited by nitric oxide: implications in atherosclerosis associated with menopause and diabetes. Proc Natl Acad Sci U S A. 2006;103(45):17018–23.
Childs BG, Baker DJ, Wijshake T, Conover CA, Campisi J, van Deursen JM. Senescent intimal foam cells are deleterious at all stages of atherosclerosis. Science. 2016;354(6311):472–7.
Minamino T, Miyauchi H, Yoshida T, Ishida Y, Yoshida H, Komuro I. Endothelial cell senescence in human atherosclerosis: role of telomere in endothelial dysfunction. Circulation. 2002;105(13):1541–4.
Tibballs J. The role of nitric oxide (formerly endothelium-derived relaxing factor-EDRF) in vasodilatation and vasodilator therapy. Anaesth Intensive Care. 1993;21(6):759–73.
Hoffmann J, Haendeler J, Aicher A, Rossig L, Vasa M, Zeiher AM, et al. Aging enhances the sensitivity of endothelial cells toward apoptotic stimuli: important role of nitric oxide. Circ Res. 2001;89(8):709–15.
Matsushita H, Chang E, Glassford AJ, Cooke JP, Chiu CP, Tsao PS. eNOS activity is reduced in senescent human endothelial cells: preservation by hTERT immortalization. Circ Res. 2001;89(9):793–8.
Vasa M, Breitschopf K, Zeiher AM, Dimmeler S. Nitric oxide activates telomerase and delays endothelial cell senescence. Circ Res. 2000;87(7):540–2.
Sonveaux P, Brouet A, Havaux X, Gregoire V, Dessy C, Balligand JL, et al. Irradiation-induced angiogenesis through the up-regulation of the nitric oxide pathway: implications for tumor radiotherapy. Cancer Res. 2003;63(5):1012–9.
Nagane M, Kuppusamy ML, An J, Mast JM, Gogna R, Yasui H, et al. Ataxia-telangiectasia mutated (ATM) kinase regulates eNOS expression and modulates radiosensitivity in endothelial cells exposed to ionizing radiation. Radiat Res. 2018;189(5):519–28.
Pennisi R, Ascenzi P, di Masi A. Hsp90: a new player in DNA repair? Biomolecules. 2015;5(4):2589–618.
Nagane M, Yasui H, Sakai Y, Yamamori T, Niwa K, Hattori Y, et al. Activation of eNOS in endothelial cells exposed to ionizing radiation involves components of the DNA damage response pathway. Biochem Biophys Res Commun. 2015;456(1):541–6.
Sakata K, Kondo T, Mizuno N, Shoji M, Yasui H, Yamamori T, et al. Roles of ROS and PKC-betaII in ionizing radiation-induced eNOS activation in human vascular endothelial cells. Vascul Pharmacol. 2015;70:55–65.
Nagane M, Yasui H, Kuppusamy P, Yamashita T, Inanami O. DNA damage response in vascular endothelial senescence: implication for radiation-induced cardiovascular diseases. J Radiat Res. 2021;62(4):564–73.
Hinz M, Stilmann M, Arslan SC, Khanna KK, Dittmar G, Scheidereit C. A cytoplasmic ATM-TRAF6-cIAP1 module links nuclear DNA damage signaling to ubiquitin-mediated NF-kappaB activation. Mol Cell. 2010;40(1):63–74.
Alexander A, Cai SL, Kim J, Nanez A, Sahin M, MacLean KH, et al. ATM signals to TSC2 in the cytoplasm to regulate mTORC1 in response to ROS. Proc Natl Acad Sci U S A. 2010;107(9):4153–8.
Yang Y, Xia F, Hermance N, Mabb A, Simonson S, Morrissey S, et al. A cytosolic ATM/NEMO/RIP1 complex recruits TAK1 to mediate the NF-kappaB and p38 mitogen-activated protein kinase (MAPK)/MAPK-activated protein 2 responses to DNA damage. Mol Cell Biol. 2011;31(14):2774–86.
Takimoto E, Champion HC, Li M, Ren S, Rodriguez ER, Tavazzi B, et al. Oxidant stress from nitric oxide synthase-3 uncoupling stimulates cardiac pathologic remodeling from chronic pressure load. J Clin Invest. 2005;115(5):1221–31.
Liu YH, Carretero OA, Cingolani OH, Liao TD, Sun Y, Xu J, et al. Role of inducible nitric oxide synthase in cardiac function and remodeling in mice with heart failure due to myocardial infarction. Am J Physiol Heart Circ Physiol. 2005;289(6):H2616–23.
Afanas’ev I. ROS and RNS signaling in heart disorders: could antioxidant treatment be successful? Oxid Med Cell Longev. 2011;2011: 293769.
Lowe D, Raj K. Premature aging induced by radiation exhibits pro-atherosclerotic effects mediated by epigenetic activation of CD44 expression. Aging Cell. 2014;13(5):900–10.
Repin VS, Dolgov VV, Zaikina OE, Novikov ID, Antonov AS, Nikolaeva MA, et al. Heterogeneity of endothelium in human aorta. A quantitative analysis by scanning electron microscopy. Atherosclerosis. 1984;50(1):35–52.
Tokunaga O, Fan JL, Watanabe T. Atherosclerosis- and age-related multinucleated variant endothelial cells in primary culture from human aorta. Am J Pathol. 1989;135(6):967–76.
Cuff CA, Kothapalli D, Azonobi I, Chun S, Zhang Y, Belkin R, et al. The adhesion receptor CD44 promotes atherosclerosis by mediating inflammatory cell recruitment and vascular cell activation. J Clin Invest. 2001;108(7):1031–40.
Kagara N, Huynh KT, Kuo C, Okano H, Sim MS, Elashoff D, et al. Epigenetic regulation of cancer stem cell genes in triple-negative breast cancer. Am J Pathol. 2012;181(1):257–67.
Crouch J, Shvedova M, Thanapaul R, Botchkarev V, Roh D. Epigenetic regulation of cellular senescence. Cells. 2022;11(4):672.
Honda S, Ikeda K, Urata R, Yamazaki E, Emoto N, Matoba S. Cellular senescence promotes endothelial activation through epigenetic alteration, and consequently accelerates atherosclerosis. Sci Rep. 2021;11(1):14608.
O’Brien J, Hayder H, Zayed Y, Peng C. Overview of MicroRNA biogenesis, mechanisms of actions, and circulation. Front Endocrinol (Lausanne). 2018;9:402.
Yu M, Sun Y, Shan X, Yang F, Chu G, Chen Q, et al. Therapeutic overexpression of miR-92a-2-5p ameliorated cardiomyocyte oxidative stress injury in the development of diabetic cardiomyopathy. Cell Mol Biol Lett. 2022;27(1):85.
Wagner-Ecker M, Schwager C, Wirkner U, Abdollahi A, Huber PE. MicroRNA expression after ionizing radiation in human endothelial cells. Radiat Oncol. 2010;5:25.
Sylvester CB, Abe JI, Patel ZS, Grande-Allen KJ. Radiation-induced cardiovascular disease: mechanisms and importance of linear energy transfer. Front Cardiovasc Med. 2018;5:5.
Hallahan D, Clark ET, Kuchibhotla J, Gewertz BL, Collins T. E-selectin gene induction by ionizing radiation is independent of cytokine induction. Biochem Biophys Res Commun. 1995;217(3):784–95.
Salminen A, Kauppinen A, Kaarniranta K. Emerging role of NF-kappaB signaling in the induction of senescence-associated secretory phenotype (SASP). Cell Signal. 2012;24(4):835–45.
Baselet B, Sonveaux P, Baatout S, Aerts A. Pathological effects of ionizing radiation: endothelial activation and dysfunction. Cell Mol Life Sci. 2019;76(4):699–728.
Krombach J, Hennel R, Brix N, Orth M, Schoetz U, Ernst A, et al. Priming anti-tumor immunity by radiotherapy: dying tumor cell-derived DAMPs trigger endothelial cell activation and recruitment of myeloid cells. Oncoimmunology. 2019;8(1): e1523097.
Land WG. The role of damage-associated molecular patterns (DAMPs) in human diseases: part II: DAMPs as diagnostics, prognostics and therapeutics in clinical medicine. Sultan Qaboos Univ Med J. 2015;15(2):e157–70.
Fiuza C, Bustin M, Talwar S, Tropea M, Gerstenberger E, Shelhamer JH, et al. Inflammation-promoting activity of HMGB1 on human microvascular endothelial cells. Blood. 2003;101(7):2652–60.
Wang L, He L, Bao G, He X, Fan S, Wang H. Ionizing radiation induces HMGB1 cytoplasmic translocation and extracellular release. Guo Ji Fang She Yi Xue He Yi Xue Za Zhi. 2016;40(2):91–9.
El Hadri K, Smith R, Duplus E, El Amri C. Inflammation, oxidative stress, senescence in atherosclerosis: thioredoxine-1 as an emerging therapeutic target. Int J Mol Sci. 2021;23(1):77.
Collins-Underwood JR, Zhao W, Sharpe JG, Robbins ME. NADPH oxidase mediates radiation-induced oxidative stress in rat brain microvascular endothelial cells. Free Radic Biol Med. 2008;45(6):929–38.
Closa D, Folch-Puy E. Oxygen free radicals and the systemic inflammatory response. IUBMB Life. 2004;56(4):185–91.
Baselet B, Driesen RB, Coninx E, Belmans N, Sieprath T, Lambrichts I, et al. Rosiglitazone protects endothelial cells from irradiation-induced mitochondrial dysfunction. Front Pharmacol. 2020;11:268.
Ahmed S, Passos JF, Birket MJ, Beckmann T, Brings S, Peters H, et al. Telomerase does not counteract telomere shortening but protects mitochondrial function under oxidative stress. J Cell Sci. 2008;121(Pt 7):1046–53.
Hu L, Li H, Zi M, Li W, Liu J, Yang Y, et al. Why senescent cells are resistant to apoptosis: an insight for senolytic development. Front Cell Dev Biol. 2022;10: 822816.
Haimovitz-Friedman A, Kan CC, Ehleiter D, Persaud RS, McLoughlin M, Fuks Z, et al. Ionizing radiation acts on cellular membranes to generate ceramide and initiate apoptosis. J Exp Med. 1994;180(2):525–35.
Wang Y, Boerma M, Zhou D. Ionizing radiation-induced endothelial cell senescence and cardiovascular diseases. Radiat Res. 2016;186(2):153–61.
Marathe S, Schissel SL, Yellin MJ, Beatini N, Mintzer R, Williams KJ, et al. Human vascular endothelial cells are a rich and regulatable source of secretory sphingomyelinase. Implications for early atherogenesis and ceramide-mediated cell signaling. J Biol Chem. 1998;273(7):4081–8.
Panganiban RA, Mungunsukh O, Day RM. X-irradiation induces ER stress, apoptosis, and senescence in pulmonary artery endothelial cells. Int J Radiat Biol. 2013;89(8):656–67.
Basatemur GL, Jorgensen HF, Clarke MCH, Bennett MR, Mallat Z. Vascular smooth muscle cells in atherosclerosis. Nat Rev Cardiol. 2019;16(12):727–44.
Chappell J, Harman JL, Narasimhan VM, Yu H, Foote K, Simons BD, et al. Extensive proliferation of a subset of differentiated, yet plastic, medial vascular smooth muscle cells contributes to neointimal formation in mouse injury and atherosclerosis models. Circ Res. 2016;119(12):1313–23.
Jacobsen K, Lund MB, Shim J, Gunnersen S, Fuchtbauer EM, Kjolby M, et al. Diverse cellular architecture of atherosclerotic plaque derives from clonal expansion of a few medial SMCs. JCI Insight. 2017;2(19).
Shankman LS, Gomez D, Cherepanova OA, Salmon M, Alencar GF, Haskins RM, et al. KLF4-dependent phenotypic modulation of smooth muscle cells has a key role in atherosclerotic plaque pathogenesis. Nat Med. 2015;21(6):628–37.
Cherepanova OA, Gomez D, Shankman LS, Swiatlowska P, Williams J, Sarmento OF, et al. Activation of the pluripotency factor OCT4 in smooth muscle cells is atheroprotective. Nat Med. 2016;22(6):657–65.
Newman AA, Baylis RA, Hess DL, Griffith SD, Shankman LS, Cherepanova OA, et al. Irradiation abolishes smooth muscle investment into vascular lesions in specific vascular beds. JCI Insight. 2018;3(15).
Gajdusek CM, Tian H, London S, Zhou D, Rasey J, Mayberg MR. Gamma radiation effect on vascular smooth muscle cells in culture. Int J Radiat Oncol Biol Phys. 1996;36(4):821–8.
Ryu JW, Jung IH, Park EY, Kim KH, Kim K, Yeom J, et al. Radiation-induced C-reactive protein triggers apoptosis of vascular smooth muscle cells through ROS interfering with the STAT3/Ref-1 complex. J Cell Mol Med. 2022;26(7):2104–18.
Nieder C, Mannsaker B, Dalhaug A, Pawinski A, Haukland E. Palliative radiotherapy in cancer patients with increased serum C-reactive protein level. In Vivo. 2016;30(5):581–6.
Ryu J, Lee CW, Shin JA, Park CS, Kim JJ, Park SJ, et al. FcgammaRIIa mediates C-reactive protein-induced inflammatory responses of human vascular smooth muscle cells by activating NADPH oxidase 4. Cardiovasc Res. 2007;75(3):555–65.
Blaschke F, Bruemmer D, Yin F, Takata Y, Wang W, Fishbein MC, et al. C-reactive protein induces apoptosis in human coronary vascular smooth muscle cells. Circulation. 2004;110(5):579–87.
Reidy MA. Proliferation of smooth muscle cells at sites distant from vascular injury. Arteriosclerosis. 1990;10(2):298–305.
Rosen EM, Goldberg ID, Myrick KV, Halpin PA, Levenson SE. Survival and repair of potentially lethal radiation damage in confluent vascular smooth muscle cell cultures. Radiother Oncol. 1986;5(2):159–63.
Keller PF, Verin V, Ziegler T, Mermillod B, Popowski Y, Delafontaine P. Gamma-irradiation markedly inhibits the hydrated collagen gel contradiction by arterial smooth muscle cells. J Investig Med. 2001;49(3):258–64.
Heckenkamp J, Leszczynski D, Schiereck J, Kung J, LaMuraglia GM. Different effects of photodynamic therapy and gamma-irradiation on vascular smooth muscle cells and matrix : implications for inhibiting restenosis. Arterioscler Thromb Vasc Biol. 1999;19(9):2154–61.
Mayberg MR, London S, Rasey J, Gajdusek C. Inhibition of rat smooth muscle proliferation by radiation after arterial injury: temporal characteristics in vivo and in vitro. Radiat Res. 2000;153(2):153–63.
Dzau VJ, Braun-Dullaeus RC, Sedding DG. Vascular proliferation and atherosclerosis: new perspectives and therapeutic strategies. Nat Med. 2002;8(11):1249–56.
Soloviev AI, Stefanov AV, Tishkin SM, Khromov AS, Parshikov AV, Ivanova IV, et al. Saline containing phosphatidylcholine liposomes possess the ability to restore endothelial function damaged resulting from gamma-irradiation. J Physiol Pharmacol. 2002;53(4 Pt 1):701–12.
Soloviev AI, Tishkin SM, Zelensky SN, Ivanova IV, Kizub IV, Pavlova AA, et al. Ionizing radiation alters myofilament calcium sensitivity in vascular smooth muscle: potential role of protein kinase C. Am J Physiol Regul Integr Comp Physiol. 2005;289(3):R755–62.
Kizub IV, Pavlova OO, Ivanova IV, Soloviev AI. Protein kinase C-dependent inhibition of BK(Ca) current in rat aorta smooth muscle cells following gamma-irradiation. Int J Radiat Biol. 2010;86(4):291–9.
Heckenkamp J, Nigri GR, Waterman PR, Overhaus M, Kossodo SC, Lamuraglia GM. Gamma-irradiation modulates vascular smooth muscle cell and extracellular matrix function: implications for neointimal development. J Vasc Surg. 2004;39(5):1097–103.
Najafi M, Fardid R, Hadadi G, Fardid M. The mechanisms of radiation-induced bystander effect. J Biomed Phys Eng. 2014;4(4):163–72.
de Crom R, Wulf P, van Nimwegen H, Kutryk MJ, Visser P, van der Kamp A, et al. Irradiated versus nonirradiated endothelial cells: effect on proliferation of vascular smooth muscle cells. J Vasc Interv Radiol. 2001;12(7):855–61.
Kim SJ, Masaki T, Rowley R, Leypoldt JK, Mohammad SF, Cheung AK. Different responses by cultured aortic and venous smooth muscle cells to gamma radiation. Kidney Int. 2005;68(1):371–7.
Cardinale D, Iacopo F, Cipolla CM. Cardiotoxicity of anthracyclines. Front Cardiovasc Med. 2020;7:26.
Hershman DL, Shao T. Anthracycline cardiotoxicity after breast cancer treatment. Oncology (Williston Park). 2009;23(3):227–34.
Lipshultz SE, Alvarez JA, Scully RE. Anthracycline associated cardiotoxicity in survivors of childhood cancer. Heart. 2008;94(4):525–33.
Rocca C, Pasqua T, Cerra MC, Angelone T. Cardiac damage in anthracyclines therapy: focus on oxidative stress and inflammation. Antioxid Redox Signal. 2020;32(15):1081–97.
Kremer LC, van der Pal HJ, Offringa M, van Dalen EC, Voute PA. Frequency and risk factors of subclinical cardiotoxicity after anthracycline therapy in children: a systematic review. Ann Oncol. 2002;13(6):819–29.
Kremer LC, van Dalen EC, Offringa M, Voute PA. Frequency and risk factors of anthracycline-induced clinical heart failure in children: a systematic review. Ann Oncol. 2002;13(4):503–12.
van der Pal HJ, van Dalen EC, van Delden E, van Dijk IW, Kok WE, Geskus RB, et al. High risk of symptomatic cardiac events in childhood cancer survivors. J Clin Oncol. 2012;30(13):1429–37.
Aminkeng F, Ross CJ, Rassekh SR, Hwang S, Rieder MJ, Bhavsar AP, et al. Recommendations for genetic testing to reduce the incidence of anthracycline-induced cardiotoxicity. Br J Clin Pharmacol. 2016;82(3):683–95.
Sritharan S, Sivalingam N. A comprehensive review on time-tested anticancer drug doxorubicin. Life Sci. 2021;278: 119527.
Kim SY, Kim SJ, Kim BJ, Rah SY, Chung SM, Im MJ, et al. Doxorubicin-induced reactive oxygen species generation and intracellular Ca2+ increase are reciprocally modulated in rat cardiomyocytes. Exp Mol Med. 2006;38(5):535–45.
Asensio-Lopez MC, Soler F, Pascual-Figal D, Fernandez-Belda F, Lax A. Doxorubicin-induced oxidative stress: the protective effect of nicorandil on HL-1 cardiomyocytes. PLoS ONE. 2017;12(2): e0172803.
Asensio-Lopez MC, Soler F, Sanchez-Mas J, Pascual-Figal D, Fernandez-Belda F, Lax A. Early oxidative damage induced by doxorubicin: source of production, protection by GKT137831 and effect on Ca(2+) transporters in HL-1 cardiomyocytes. Arch Biochem Biophys. 2016;594:26–36.
Goormaghtigh E, Chatelain P, Caspers J, Ruysschaert JM. Evidence of a specific complex between adriamycin and negatively-charged phospholipids. Biochim Biophys Acta. 1980;597(1):1–14.
Smith LA, Cornelius VR, Plummer CJ, Levitt G, Verrill M, Canney P, et al. Cardiotoxicity of anthracycline agents for the treatment of cancer: systematic review and meta-analysis of randomised controlled trials. BMC Cancer. 2010;10:337.
Toldo S, Goehe RW, Lotrionte M, Mezzaroma E, Sumner ET, Biondi-Zoccai GG, et al. Comparative cardiac toxicity of anthracyclines in vitro and in vivo in the mouse. PLoS ONE. 2013;8(3): e58421.
Deng S, Yan T, Jendrny C, Nemecek A, Vincetic M, Godtel-Armbrust U, et al. Dexrazoxane may prevent doxorubicin-induced DNA damage via depleting both topoisomerase II isoforms. BMC Cancer. 2014;14:842.
L’Ecuyer T, Sanjeev S, Thomas R, Novak R, Das L, Campbell W, et al. DNA damage is an early event in doxorubicin-induced cardiac myocyte death. Am J Physiol Heart Circ Physiol. 2006;291(3):H1273–80.
Mizuta Y, Tokuda K, Guo J, Zhang S, Narahara S, Kawano T, et al. Sodium thiosulfate prevents doxorubicin-induced DNA damage and apoptosis in cardiomyocytes in mice. Life Sci. 2020;257: 118074.
Huang H, Christidi E, Shafaattalab S, Davis MK, Tibbits GF, Brunham LR. RARG S427L attenuates the DNA repair response to doxorubicin in induced pluripotent stem cell-derived cardiomyocytes. Stem Cell Reports. 2022;17(4):756–65.
Qiao X, van der Zanden SY, Wander DPA, Borras DM, Song JY, Li X, et al. Uncoupling DNA damage from chromatin damage to detoxify doxorubicin. Proc Natl Acad Sci U S A. 2020;117(26):15182–92.
Doroshow JH, Davies KJ. Redox cycling of anthracyclines by cardiac mitochondria. II. Formation of superoxide anion, hydrogen peroxide, and hydroxyl radical. J Biol Chem. 1986;261(7):3068–74.
Davies KJ, Doroshow JH. Redox cycling of anthracyclines by cardiac mitochondria. I. Anthracycline radical formation by NADH dehydrogenase. J Biol Chem. 1986;261(7):3060–7.
Vermot A, Petit-Hartlein I, Smith SME, Fieschi F. NADPH oxidases (NOX): an overview from discovery, molecular mechanisms to physiology and pathology. Antioxidants (Basel). 2021;10(6):890.
Wojnowski L, Kulle B, Schirmer M, Schluter G, Schmidt A, Rosenberger A, et al. NAD(P)H oxidase and multidrug resistance protein genetic polymorphisms are associated with doxorubicin-induced cardiotoxicity. Circulation. 2005;112(24):3754–62.
Zhang S, Liu X, Bawa-Khalfe T, Lu LS, Lyu YL, Liu LF, et al. Identification of the molecular basis of doxorubicin-induced cardiotoxicity. Nat Med. 2012;18(11):1639–42.
Xu X, Persson HL, Richardson DR. Molecular pharmacology of the interaction of anthracyclines with iron. Mol Pharmacol. 2005;68(2):261–71.
Vejpongsa P, Yeh ET. Topoisomerase 2beta: a promising molecular target for primary prevention of anthracycline-induced cardiotoxicity. Clin Pharmacol Ther. 2014;95(1):45–52.
Ichikawa Y, Bayeva M, Ghanefar M, Potini V, Sun L, Mutharasan RK, et al. Disruption of ATP-binding cassette B8 in mice leads to cardiomyopathy through a decrease in mitochondrial iron export. Proc Natl Acad Sci USA. 2012;109(11):4152–7.
Ichikawa Y, Ghanefar M, Bayeva M, Wu R, Khechaduri A, Naga Prasad SV, et al. Cardiotoxicity of doxorubicin is mediated through mitochondrial iron accumulation. J Clin Invest. 2014;124(2):617–30.
Minotti G, Ronchi R, Salvatorelli E, Menna P, Cairo G. Doxorubicin irreversibly inactivates iron regulatory proteins 1 and 2 in cardiomyocytes: evidence for distinct metabolic pathways and implications for iron-mediated cardiotoxicity of antitumor therapy. Cancer Res. 2001;61(23):8422–8.
Kwok JC, Richardson DR. The cardioprotective effect of the iron chelator dexrazoxane (ICRF-187) on anthracycline-mediated cardiotoxicity. Redox Rep. 2000;5(6):317–24.
Lebrecht D, Geist A, Ketelsen UP, Haberstroh J, Setzer B, Walker UA. Dexrazoxane prevents doxorubicin-induced long-term cardiotoxicity and protects myocardial mitochondria from genetic and functional lesions in rats. Br J Pharmacol. 2007;151(6):771–8.
Yu X, Ruan Y, Shen T, Qiu Q, Yan M, Sun S, et al. Dexrazoxane protects cardiomyocyte from doxorubicin-induced apoptosis by modulating miR-17-5p. Biomed Res Int. 2020;2020:5107193.
Sawyer DB, Fukazawa R, Arstall MA, Kelly RA. Daunorubicin-induced apoptosis in rat cardiac myocytes is inhibited by dexrazoxane. Circ Res. 1999;84(3):257–65.
Li L, Nie X, Zhang P, Huang Y, Ma L, Li F, et al. Dexrazoxane ameliorates radiation-induced heart disease in a rat model. Aging (Albany NY). 2021;13(3):3699–711.
Ji ZR, Xue WL, Zhang L. Schisandrin B attenuates inflammation in LPS-induced sepsis through miR-17-5p downregulating TLR4. Inflammation. 2019;42(2):731–9.
Shen Y, Lu L, Xu J, Meng W, Qing Y, Liu Y, et al. Bortezomib induces apoptosis of endometrial cancer cells through microRNA-17-5p by targeting p21. Cell Biol Int. 2013;37(10):1114–21.
Yin Z, Zhao Y, Li H, Yan M, Zhou L, Chen C, et al. miR-320a mediates doxorubicin-induced cardiotoxicity by targeting VEGF signal pathway. Aging (Albany NY). 2016;8(1):192–207.
Hasinoff BB, Patel D, Wu X. The oral iron chelator ICL670A (deferasirox) does not protect myocytes against doxorubicin. Free Radic Biol Med. 2003;35(11):1469–79.
Caroni P, Villani F, Carafoli E. The cardiotoxic antibiotic doxorubicin inhibits the Na+/Ca2+ exchange of dog heart sarcolemmal vesicles. FEBS Lett. 1981;130(2):184–6.
Keung EC, Toll L, Ellis M, Jensen RA. L-type cardiac calcium channels in doxorubicin cardiomyopathy in rats morphological, biochemical, and functional correlations. J Clin Invest. 1991;87(6):2108–13.
Arai M, Tomaru K, Takizawa T, Sekiguchi K, Yokoyama T, Suzuki T, et al. Sarcoplasmic reticulum genes are selectively down-regulated in cardiomyopathy produced by doxorubicin in rabbits. J Mol Cell Cardiol. 1998;30(2):243–54.
Dresdale AR, Barr LH, Bonow RO, Mathisen DJ, Myers CE, Schwartz DE, et al. Prospective randomized study of the role of N-acetyl cysteine in reversing doxorubicin-induced cardiomyopathy. Am J Clin Oncol. 1982;5(6):657–63.
Narula J, Haider N, Virmani R, DiSalvo TG, Kolodgie FD, Hajjar RJ, et al. Apoptosis in myocytes in end-stage heart failure. N Engl J Med. 1996;335(16):1182–9.
Minotti G, Menna P, Salvatorelli E, Cairo G, Gianni L. Anthracyclines: molecular advances and pharmacologic developments in antitumor activity and cardiotoxicity. Pharmacol Rev. 2004;56(2):185–229.
Zorova LD, Popkov VA, Plotnikov EY, Silachev DN, Pevzner IB, Jankauskas SS, et al. Mitochondrial membrane potential. Anal Biochem. 2018;552:50–9.
Zhao L, Zhang B. Doxorubicin induces cardiotoxicity through upregulation of death receptors mediated apoptosis in cardiomyocytes. Sci Rep. 2017;7:44735.
He L, Yang Y, Chen J, Zou P, Li J. Transcriptional activation of ENPP2 by FoxO4 protects cardiomyocytes from doxorubicin‑induced toxicity. Mol Med Rep. 2021;24(3).
Fang X, Wang H, Han D, Xie E, Yang X, Wei J, et al. Ferroptosis as a target for protection against cardiomyopathy. Proc Natl Acad Sci USA. 2019;116(7):2672–80.
Li DL, Hill JA. Cardiomyocyte autophagy and cancer chemotherapy. J Mol Cell Cardiol. 2014;71:54–61.
Taneike M, Yamaguchi O, Nakai A, Hikoso S, Takeda T, Mizote I, et al. Inhibition of autophagy in the heart induces age-related cardiomyopathy. Autophagy. 2010;6(5):600–6.
Gu J, Fan YQ, Zhang HL, Pan JA, Yu JY, Zhang JF, et al. Resveratrol suppresses doxorubicin-induced cardiotoxicity by disrupting E2F1 mediated autophagy inhibition and apoptosis promotion. Biochem Pharmacol. 2018;150:202–13.
Kobayashi S, Volden P, Timm D, Mao K, Xu X, Liang Q. Transcription factor GATA4 inhibits doxorubicin-induced autophagy and cardiomyocyte death. J Biol Chem. 2010;285(1):793–804.
Li DL, Wang ZV, Ding G, Tan W, Luo X, Criollo A, et al. Doxorubicin blocks cardiomyocyte autophagic flux by inhibiting lysosome acidification. Circulation. 2016;133(17):1668–87.
Altieri P, Barisione C, Lazzarini E, Garuti A, Bezante GP, Canepa M, et al. Testosterone antagonizes doxorubicin-induced senescence of cardiomyocytes. J Am Heart Assoc. 2016;5(1).
Maejima Y, Adachi S, Ito H, Hirao K, Isobe M. Induction of premature senescence in cardiomyocytes by doxorubicin as a novel mechanism of myocardial damage. Aging Cell. 2008;7(2):125–36.
Spallarossa P, Altieri P, Aloi C, Garibaldi S, Barisione C, Ghigliotti G, et al. Doxorubicin induces senescence or apoptosis in rat neonatal cardiomyocytes by regulating the expression levels of the telomere binding factors 1 and 2. Am J Physiol Heart Circ Physiol. 2009;297(6):H2169–81.
Spallarossa P, Altieri P, Pronzato P, Aloi C, Ghigliotti G, Barsotti A, et al. Sublethal doses of an anti-erbB2 antibody leads to death by apoptosis in cardiomyocytes sensitized by low prosenescent doses of epirubicin: the protective role of dexrazoxane. J Pharmacol Exp Ther. 2010;332(1):87–96.
Castedo M, Perfettini JL, Roumier T, Andreau K, Medema R, Kroemer G. Cell death by mitotic catastrophe: a molecular definition. Oncogene. 2004;23(16):2825–37.
Altieri P, Spallarossa P, Barisione C, Garibaldi S, Garuti A, Fabbi P, et al. Inhibition of doxorubicin-induced senescence by PPARdelta activation agonists in cardiac muscle cells: cooperation between PPARdelta and Bcl6. PLoS ONE. 2012;7(9): e46126.
Cai F, Luis MAF, Lin X, Wang M, Cai L, Cen C, et al. Anthracycline-induced cardiotoxicity in the chemotherapy treatment of breast cancer: preventive strategies and treatment. Mol Clin Oncol. 2019;11(1):15–23.
Chan EM, Thomas MJ, Bandy B, Tibbits GF. Effects of doxorubicin, 4’-epirubicin, and antioxidant enzymes on the contractility of isolated cardiomyocytes. Can J Physiol Pharmacol. 1996;74(8):904–10.
Shannon TR, Ginsburg KS, Bers DM. Quantitative assessment of the SR Ca2+ leak-load relationship. Circ Res. 2002;91(7):594–600.
Fabiani I, Aimo A, Grigoratos C, Castiglione V, Gentile F, Saccaro LF, et al. Oxidative stress and inflammation: determinants of anthracycline cardiotoxicity and possible therapeutic targets. Heart Fail Rev. 2021;26(4):881–90.
Reis-Mendes A, Padrao AI, Duarte JA, Goncalves-Monteiro S, Duarte-Araujo M, Remiao F, et al. Role of inflammation and redox status on doxorubicin-induced cardiotoxicity in infant and adult CD-1 male mice. Biomolecules. 2021;11(11):1725.
Sahu R, Dua TK, Das S, De Feo V, Dewanjee S. Wheat phenolics suppress doxorubicin-induced cardiotoxicity via inhibition of oxidative stress, MAP kinase activation, NF-kappaB pathway, PI3K/Akt/mTOR impairment, and cardiac apoptosis. Food Chem Toxicol. 2019;125:503–19.
Zhang Y, Ahmad KA, Khan FU, Yan S, Ihsan AU, Ding Q. Chitosan oligosaccharides prevent doxorubicin-induced oxidative stress and cardiac apoptosis through activating p38 and JNK MAPK mediated Nrf2/ARE pathway. Chem Biol Interact. 2019;305:54–65.
Kanno SI, Hara A. The mRNA expression of Il6 and Pdcd1 are predictive and protective factors for doxorubicin-induced cardiotoxicity. Mol Med Rep. 2021;23(2):1.
Ren D, Li F, Cao Q, Gao A, Ai Y, Zhang J. Yangxin granules alleviate doxorubicin-induced cardiotoxicity by suppressing oxidative stress and apoptosis mediated by AKT/GSK3beta/beta-catenin signaling. J Int Med Res. 2020;48(8):300060520945161.
Cappetta D, Rossi F, Piegari E, Quaini F, Berrino L, Urbanek K, et al. Doxorubicin targets multiple players: a new view of an old problem. Pharmacol Res. 2018;127:4–14.
He H, Wang L, Qiao Y, Zhou Q, Li H, Chen S, et al. Doxorubicin induces endotheliotoxicity and mitochondrial dysfunction via ROS/eNOS/NO pathway. Front Pharmacol. 2019;10:1531.
Wilkinson EL, Sidaway JE, Cross MJ. Cardiotoxic drugs Herceptin and doxorubicin inhibit cardiac microvascular endothelial cell barrier formation resulting in increased drug permeability. Biol Open. 2016;5(10):1362–70.
Lorenzo E, Ruiz-Ruiz C, Quesada AJ, Hernandez G, Rodriguez A, Lopez-Rivas A, et al. Doxorubicin induces apoptosis and CD95 gene expression in human primary endothelial cells through a p53-dependent mechanism. J Biol Chem. 2002;277(13):10883–92.
Abou El Hassan MA, Verheul HM, Jorna AS, Schalkwijk C, van Bezu J, van der Vijgh WJ, et al. The new cardioprotector Monohydroxyethylrutoside protects against doxorubicin-induced inflammatory effects in vitro. Br J Cancer. 2003;89(2):357–62.
Vasquez-Vivar J, Martasek P, Hogg N, Masters BS, Pritchard KA Jr, Kalyanaraman B. Endothelial nitric oxide synthase-dependent superoxide generation from adriamycin. Biochemistry. 1997;36(38):11293–7.
Kalivendi SV, Kotamraju S, Zhao H, Joseph J, Kalyanaraman B. Doxorubicin-induced apoptosis is associated with increased transcription of endothelial nitric-oxide synthase. Effect of antiapoptotic antioxidants and calcium. J Biol Chem. 2001;276(50):47266–76.
Chiusa M, Hool SL, Truetsch P, Djafarzadeh S, Jakob SM, Seifriz F, et al. Cancer therapy modulates VEGF signaling and viability in adult rat cardiac microvascular endothelial cells and cardiomyocytes. J Mol Cell Cardiol. 2012;52(5):1164–75.
Rasanen M, Degerman J, Nissinen TA, Miinalainen I, Kerkela R, Siltanen A, et al. VEGF-B gene therapy inhibits doxorubicin-induced cardiotoxicity by endothelial protection. Proc Natl Acad Sci USA. 2016;113(46):13144–9.
Graziani S, Scorrano L, Pontarin G. Transient exposure of endothelial cells to doxorubicin leads to long-lasting vascular endothelial growth factor receptor 2 downregulation. Cells. 2022;11(2):210.
Bent EH, Gilbert LA, Hemann MT. A senescence secretory switch mediated by PI3K/AKT/mTOR activation controls chemoprotective endothelial secretory responses. Genes Dev. 2016;30(16):1811–21.
Chen L, Holder R, Porter C, Shah Z. Vitamin D3 attenuates doxorubicin-induced senescence of human aortic endothelial cells by upregulation of IL-10 via the pAMPKalpha/Sirt1/Foxo3a signaling pathway. PLoS ONE. 2021;16(6): e0252816.
Damrot J, Nubel T, Epe B, Roos WP, Kaina B, Fritz G. Lovastatin protects human endothelial cells from the genotoxic and cytotoxic effects of the anticancer drugs doxorubicin and etoposide. Br J Pharmacol. 2006;149(8):988–97.
Muresan M, Olteanu D, Filip GA, Clichici S, Baldea I, Jurca T, et al. Comparative study of the pharmacological properties and biological effects of Polygonum aviculare L. herba extract-entrapped liposomes versus quercetin-entrapped liposomes on doxorubicin-induced toxicity on HUVECs. Pharmaceutics. 2021;13(9):1418.
Wojcik T, Buczek E, Majzner K, Kolodziejczyk A, Miszczyk J, Kaczara P, et al. Comparative endothelial profiling of doxorubicin and daunorubicin in cultured endothelial cells. Toxicol In Vitro. 2015;29(3):512–21.
Bielak-Zmijewska A, Wnuk M, Przybylska D, Grabowska W, Lewinska A, Alster O, et al. A comparison of replicative senescence and doxorubicin-induced premature senescence of vascular smooth muscle cells isolated from human aorta. Biogerontology. 2014;15(1):47–64.
Zhang C-R, Tong X, Qiu H-Q, Wang C, Fan Y-Y, Yang C-H. Doxorubicin-induced thoracic aorta smooth muscle cells injury through oxidative stress pathway in rats. Chin J Pharmacol Toxicol. 2022;36(8):578.
Hodjat M, Haller H, Dumler I, Kiyan Y. Urokinase receptor mediates doxorubicin-induced vascular smooth muscle cell senescence via proteasomal degradation of TRF2. J Vasc Res. 2013;50(2):109–23.
Murata T, Yamawaki H, Hori M, Sato K, Ozaki H, Karaki H. Chronic vascular toxicity of doxorubicin in an organ-cultured artery. Br J Pharmacol. 2001;132(7):1365–73.
Bosman M, Kruger DN, Favere K, Wesley CD, Neutel CHG, Van Asbroeck B, et al. Doxorubicin impairs smooth muscle cell contraction: novel insights in vascular toxicity. Int J Mol Sci. 2021;22(23):12812.
Iguchi N, Donmez MI, Carrasco A Jr, Wilcox DT, Pineda RH, Malykhina AP, et al. Doxorubicin induces detrusor smooth muscle impairments through myosin dysregulation, leading to a risk of lower urinary tract dysfunction. Am J Physiol Renal Physiol. 2019;317(1):F197–206.
Stolarz AJ, Sarimollaoglu M, Marecki JC, Fletcher TW, Galanzha EI, Rhee SW, et al. Doxorubicin activates ryanodine receptors in rat lymphatic muscle cells to attenuate rhythmic contractions and lymph flow. J Pharmacol Exp Ther. 2019;371(2):278–89.
Shen B, Ye CL, Ye KH, Zhuang L, Jiang JH. Doxorubicin-induced vasomotion and [Ca(2+)](i) elevation in vascular smooth muscle cells from C57BL/6 mice. Acta Pharmacol Sin. 2009;30(11):1488–95.
Misuth S, Uhrinova M, Klimas J, Vavrincova-Yaghi D, Vavrinec P. Vildagliptin improves vascular smooth muscle relaxation and decreases cellular senescence in the aorta of doxorubicin-treated rats. Vascul Pharmacol. 2021;138: 106855.
Herrmann J, Xia M, Gummi MR, Greco A, Schacke A, van der Giet M, et al. Stressor-induced “inflammaging” of vascular smooth muscle cells via Nlrp3-mediated pro-inflammatory auto-loop. Front Cardiovasc Med. 2021;8: 752305.
Takaguri A, Sasano J, Akihiro O, Satoh K. The role of circadian clock gene BMAL1 in vascular proliferation. Eur J Pharmacol. 2020;872: 172924.
Takaguri AM, M.; Tatsunami, R.; Sato, K.; Satoh, K. Involvement of circadian clock gene BMAL1 in doxorubicin-induced inflammation in vascular smooth muscle cells. Pharmacol Pharm. 2021;12.
Oun R, Moussa YE, Wheate NJ. The side effects of platinum-based chemotherapy drugs: a review for chemists. Dalton Trans. 2018;47(19):6645–53.
Li Z, Li C, Yang D, Song J, Liu T, Zhou Z, et al. Comparing the efficacy and safety of cisplatin and other platinum-based chemotherapies in locally advanced nasopharyngeal carcinoma: a systematic review and meta-analysis. BMC Cancer. 2022;22(1):616.
Hu Y, Sun B, Zhao B, Mei D, Gu Q, Tian Z. Cisplatin-induced cardiotoxicity with midrange ejection fraction: a case report and review of the literature. Medicine (Baltimore). 2018;97(52): e13807.
Pai VB, Nahata MC. Cardiotoxicity of chemotherapeutic agents: incidence, treatment and prevention. Drug Saf. 2000;22(4):263–302.
Schlumbrecht MP, Hehr K. Cisplatin-induced bradycardia and the importance of the QT interval. J Oncol Pharm Pract. 2015;21(2):157–60.
Khan S, Chen CL, Brady MS, Parameswaran R, Moore R, Hassoun H, et al. Unstable angina associated with cisplatin and carboplatin in a patient with advanced melanoma. J Clin Oncol. 2012;30(18):e163–4.
Moore RA, Adel N, Riedel E, Bhutani M, Feldman DR, Tabbara NE, et al. High incidence of thromboembolic events in patients treated with cisplatin-based chemotherapy: a large retrospective analysis. J Clin Oncol. 2011;29(25):3466–73.
Kim HP, Son KH, Chang HW, Kang SS. Anti-inflammatory plant flavonoids and cellular action mechanisms. J Pharmacol Sci. 2004;96(3):229–45.
Dabeek WM, Marra MV. Dietary quercetin and kaempferol: bioavailability and potential cardiovascular-related bioactivity in humans. Nutrients. 2019;11(10):2288.
Qi Y, Ying Y, Zou J, Fang Q, Yuan X, Cao Y, et al. Kaempferol attenuated cisplatin-induced cardiac injury via inhibiting STING/NF-kappaB-mediated inflammation. Am J Transl Res. 2020;12(12):8007–18.
Herradon E, Gonzalez C, Uranga JA, Abalo R, Martin MI, Lopez-Miranda V. Characterization of cardiovascular alterations induced by different chronic cisplatin treatments. Front Pharmacol. 2017;8:196.
Cheng CF, Juan SH, Chen JJ, Chao YC, Chen HH, Lian WS, et al. Pravastatin attenuates carboplatin-induced cardiotoxicity via inhibition of oxidative stress associated apoptosis. Apoptosis. 2008;13(7):883–94.
Qian P, Yan LJ, Li YQ, Yang HT, Duan HY, Wu JT, et al. Cyanidin ameliorates cisplatin-induced cardiotoxicity via inhibition of ROS-mediated apoptosis. Exp Ther Med. 2018;15(2):1959–65.
Zhao L. Protective effects of trimetazidine and coenzyme Q10 on cisplatin-induced cardiotoxicity by alleviating oxidative stress and mitochondrial dysfunction. Anatol J Cardiol. 2019;22(5):232–9.
Wang SH, Tsai KL, Chou WC, Cheng HC, Huang YT, Ou HC, et al. Quercetin mitigates cisplatin-induced oxidative damage and apoptosis in cardiomyocytes through Nrf2/HO-1 signaling pathway. Am J Chin Med. 2022;50(5):1281–98.
Li J, Ichikawa T, Villacorta L, Janicki JS, Brower GL, Yamamoto M, et al. Nrf2 protects against maladaptive cardiac responses to hemodynamic stress. Arterioscler Thromb Vasc Biol. 2009;29(11):1843–50.
Brunt KR, Fenrich KK, Kiani G, Tse MY, Pang SC, Ward CA, et al. Protection of human vascular smooth muscle cells from H2O2-induced apoptosis through functional codependence between HO-1 and AKT. Arterioscler Thromb Vasc Biol. 2006;26(9):2027–34.
Cui Y, Li C, Zeng C, Li J, Zhu Z, Chen W, et al. Tongmai Yangxin pills anti-oxidative stress alleviates cisplatin-induced cardiotoxicity: network pharmacology analysis and experimental evidence. Biomed Pharmacother. 2018;108:1081–9.
Porras A, Zuluaga S, Black E, Valladares A, Alvarez AM, Ambrosino C, et al. P38 alpha mitogen-activated protein kinase sensitizes cells to apoptosis induced by different stimuli. Mol Biol Cell. 2004;15(2):922–33.
Zuluaga S, Alvarez-Barrientos A, Gutierrez-Uzquiza A, Benito M, Nebreda AR, Porras A. Negative regulation of Akt activity by p38alpha MAP kinase in cardiomyocytes involves membrane localization of PP2A through interaction with caveolin-1. Cell Signal. 2007;19(1):62–74.
Ma H, Jones KR, Guo R, Xu P, Shen Y, Ren J. Cisplatin compromises myocardial contractile function and mitochondrial ultrastructure: role of endoplasmic reticulum stress. Clin Exp Pharmacol Physiol. 2010;37(4):460–5.
Meinardi MT, Gietema JA, van der Graaf WT, van Veldhuisen DJ, Runne MA, Sluiter WJ, et al. Cardiovascular morbidity in long-term survivors of metastatic testicular cancer. J Clin Oncol. 2000;18(8):1725–32.
Dieckmann KP, Struss WJ, Budde U. Evidence for acute vascular toxicity of cisplatin-based chemotherapy in patients with germ cell tumour. Anticancer Res. 2011;31(12):4501–5.
Vischer UM. Von Willebrand factor, endothelial dysfunction, and cardiovascular disease. J Thromb Haemost. 2006;4(6):1186–93.
Lechner D, Kollars M, Gleiss A, Kyrle PA, Weltermann A. Chemotherapy-induced thrombin generation via procoagulant endothelial microparticles is independent of tissue factor activity. J Thromb Haemost. 2007;5(12):2445–52.
Jiang Y, Shan S, Gan T, Zhang X, Lu X, Hu H, et al. Effects of cisplatin on the contractile function of thoracic aorta of Sprague-Dawley rats. Biomed Rep. 2014;2(6):893–7.
Ito H, Okafuji T, Suzuki T. Vitamin E prevents endothelial injury associated with cisplatin injection into the superior mesenteric artery of rats. Heart Vessels. 1995;10(4):178–84.
Kobutree P, Tothonglor A, Roumwong A, Jindatip D, Agthong S. Curcumin reduces blood-nerve barrier abnormalities and cytotoxicity to endothelial cells and pericytes induced by cisplatin. Folia Morphol (Warsz). 2022.
Dasari S, Tchounwou PB. Cisplatin in cancer therapy: molecular mechanisms of action. Eur J Pharmacol. 2014;740:364–78.
de Sousa GFRWS, Monteiro G. Carboplatin: molecular mechanisms of action associated with chemoresistance. Braz J Pharm Sci. 2014;50(4):693–701.
Ziegler V, Deussen M, Schumacher L, Roos WP, Fritz G. Anticancer drug and ionizing radiation-induced DNA damage differently influences transcription activity and DDR-related stress responses of an endothelial monolayer. Biochim Biophys Acta Mol Cell Res. 2020;1867(6): 118678.
Zimna A, Kurpisz M. Hypoxia-inducible factor-1 in physiological and pathophysiological angiogenesis: applications and therapies. Biomed Res Int. 2015;2015: 549412.
Chen CH, Chen MC, Hsu YH, Chou TC. Far-infrared radiation alleviates cisplatin-induced vascular damage and impaired circulation via activation of HIF-1alpha. Cancer Sci. 2022;113(6):2194–206.
Tothonglor A, Kobutree P, Roumwong A, Jindatip D, Agthong S. Cisplatin-induced alterations in the blood-nerve barrier: effects of combination of vitamin B1, B6 and B12. Folia Morphol (Warsz). 2022.
Tahergorabi Z, Khazaei M. A review on angiogenesis and its assays. Iran J Basic Med Sci. 2012;15(6):1110–26.
Yoshikawa A, Saura R, Matsubara T, Mizuno K. A mechanism of cisplatin action: antineoplastic effect through inhibition of neovascularization. Kobe J Med Sci. 1997;43(3–4):109–20.
Montiel M, Urso L, de la Blanca EP, Marsigliante S, Jimenez E. Cisplatin reduces endothelial cell migration via regulation of type 2-matrix metalloproteinase activity. Cell Physiol Biochem. 2009;23(4–6):441–8.
Chen CP, Hu CB, Yeh KC, Song JS, Yeh TK, Tung FF, et al. Antiangiogenic activities and cisplatin-combined antitumor activities of BPR0L075. Anticancer Res. 2010;30(7):2813–22.
Ramer R, Schmied T, Wagner C, Haustein M, Hinz B. The antiangiogenic action of cisplatin on endothelial cells is mediated through the release of tissue inhibitor of matrix metalloproteinases-1 from lung cancer cells. Oncotarget. 2018;9(75):34038–55.
Wild R, Dings RP, Subramanian I, Ramakrishnan S. Carboplatin selectively induces the VEGF stress response in endothelial cells: potentiation of antitumor activity by combination treatment with antibody to VEGF. Int J Cancer. 2004;110(3):343–51.
Orlandi A, Francesconi A, Cocchia D, Corsini A, Spagnoli LG. Phenotypic heterogeneity influences apoptotic susceptibility to retinoic acid and cis-platinum of rat arterial smooth muscle cells in vitro: implications for the evolution of experimental intimal thickening. Arterioscler Thromb Vasc Biol. 2001;21(7):1118–23.
Wang ZH, Zhang SZ, Zhang ZY, Zhang CP, Hu HS, Kirwan J, et al. The influence of intraarterial high-dose cisplatin with concomitant irradiation on arterial microanastomosis: an experimental study. Am J Clin Oncol. 2009;32(2):158–62.
Weaver BA. How Taxol/paclitaxel kills cancer cells. Mol Biol Cell. 2014;25(18):2677–81.
Winefield RD, Entwistle RA, Foland TB, Lushington GH, Himes RH. Differences in paclitaxel and docetaxel interactions with tubulin detected by mutagenesis of yeast tubulin. ChemMedChem. 2008;3(12):1844–7.
Rowinsky EK, McGuire WP, Guarnieri T, Fisherman JS, Christian MC, Donehower RC. Cardiac disturbances during the administration of taxol. J Clin Oncol. 1991;9(9):1704–12.
Herrmann J, Yang EH, Iliescu CA, Cilingiroglu M, Charitakis K, Hakeem A, et al. Vascular toxicities of cancer therapies: the old and the new–an evolving avenue. Circulation. 2016;133(13):1272–89.
Schimmel KJ, Richel DJ, van den Brink RB, Guchelaar HJ. Cardiotoxicity of cytotoxic drugs. Cancer Treat Rev. 2004;30(2):181–91.
Zaborowska-Szmit M, Krzakowski M, Kowalski DM, Szmit S. Cardiovascular complications of systemic therapy in non-small-cell lung cancer. J Clin Med. 2020;9(5):1268.
Ter Keurs HE, Boyden PA. Calcium and arrhythmogenesis. Physiol Rev. 2007;87(2):457–506.
Lakireddy V, Bub G, Baweja P, Syed A, Boutjdir M, El-Sherif N. The kinetics of spontaneous calcium oscillations and arrhythmogenesis in the in vivo heart during ischemia/reperfusion. Heart Rhythm. 2006;3(1):58–66.
Zhang K, Heidrich FM, DeGray B, Boehmerle W, Ehrlich BE. Paclitaxel accelerates spontaneous calcium oscillations in cardiomyocytes by interacting with NCS-1 and the InsP3R. J Mol Cell Cardiol. 2010;49(5):829–35.
Ogawa H, Kurebayashi N, Yamazawa T, Murayama T. Regulatory mechanisms of ryanodine receptor/Ca(2+) release channel revealed by recent advancements in structural studies. J Muscle Res Cell Motil. 2021;42(2):291–304.
Schrader C, Keussen C, Bewig B, von Freier A, Lins M. Symptoms and signs of an acute myocardial ischemia caused by chemotherapy with Paclitaxel (Taxol) in a patient with metastatic ovarian carcinoma. Eur J Med Res. 2005;10(11):498–501.
Abe H, Semba H, Takeda N. The roles of hypoxia signaling in the pathogenesis of cardiovascular diseases. J Atheroscler Thromb. 2017;24(9):884–94.
Dang YM, Huang YS, Zhou JL, Zhang JP, Yan H, Zhang M. An experimental study on the influence of hypoxia induction factor-1alpha on the glycolysis of the rat myocardial cell under hypoxic condition. Zhonghua Shao Shang Za Zhi. 2005;21(5):339–42.
Rodriguez-Sinovas A, Abad E, Sanchez JA, Fernandez-Sanz C, Inserte J, Ruiz-Meana M, et al. Microtubule stabilization with paclitaxel does not protect against infarction in isolated rat hearts. Exp Physiol. 2015;100(1):23–34.
Teng M, Dang YM, Zhang JP, Zhang Q, Fang YD, Ren J, et al. Microtubular stability affects cardiomyocyte glycolysis by HIF-1alpha expression and endonuclear aggregation during early stages of hypoxia. Am J Physiol Heart Circ Physiol. 2010;298(6):H1919–31.
Devillard L, Vandroux D, Tissier C, Dumont L, Borgeot J, Rochette L, et al. Involvement of microtubules in the tolerance of cardiomyocytes to cold ischemia-reperfusion. Mol Cell Biochem. 2008;307(1–2):149–57.
Xiao J, Zhao H, Liang D, Liu Y, Zhang H, Liu Y, et al. Taxol, a microtubule stabilizer, improves cardiac contractile function during ischemia in vitro. Pharmacology. 2010;85(5):301–10.
Cao H, Wang Y, Wang Q, Wang R, Guo S, Zhao X, et al. Taxol prevents myocardial ischemia-reperfusion injury by inducing JNK-mediated HO-1 expression. Pharm Biol. 2016;54(3):555–60.
Wang D, Xing W, Wang X, Zhu H. Taxol stabilizes gap junctions and reduces ischemic ventricular arrhythmias in rats in vivo. Mol Med Rep. 2015;11(5):3243–8.
Alloatti G, Penna C, Gallo MP, Levi RC, Bombardelli E, Appendino G. Differential effects of paclitaxel and derivatives on guinea pig isolated heart and papillary muscle. J Pharmacol Exp Ther. 1998;284(2):561–7.
Shah K, Gupta S, Ghosh J, Bajpai J, Maheshwari A. Acute non-ST elevation myocardial infarction following paclitaxel administration for ovarian carcinoma: a case report and review of literature. J Cancer Res Ther. 2012;8(3):442–4.
Xiao J, Zhang H, Liang D, Liu Y, Liu Y, Zhao H, et al. Taxol, a microtubule stabilizer, prevents atrial fibrillation in in vitro atrial fibrillation models using rabbit hearts. Med Sci Monit. 2010;16(11):BR353–60.
Malekinejad H, Ahsan S, Delkhosh-Kasmaie F, Cheraghi H, Rezaei-Golmisheh A, Janbaz-Acyabar H. Cardioprotective effect of royal jelly on paclitaxel-induced cardio-toxicity in rats. Iran J Basic Med Sci. 2016;19(2):221–7.
Lage R, Cebro-Marquez M, Rodriguez-Manero M, Gonzalez-Juanatey JR, Moscoso I. Omentin protects H9c2 cells against docetaxel cardiotoxicity. PLoS ONE. 2019;14(2): e0212782.
Pasquier E, Carre M, Pourroy B, Camoin L, Rebai O, Briand C, et al. Antiangiogenic activity of paclitaxel is associated with its cytostatic effect, mediated by the initiation but not completion of a mitochondrial apoptotic signaling pathway. Mol Cancer Ther. 2004;3(10):1301–10.
Belotti D, Vergani V, Drudis T, Borsotti P, Pitelli MR, Viale G, et al. The microtubule-affecting drug paclitaxel has antiangiogenic activity. Clin Cancer Res. 1996;2(11):1843–9.
Hayot C, Farinelle S, De Decker R, Decaestecker C, Darro F, Kiss R, et al. In vitro pharmacological characterizations of the anti-angiogenic and anti-tumor cell migration properties mediated by microtubule-affecting drugs, with special emphasis on the organization of the actin cytoskeleton. Int J Oncol. 2002;21(2):417–25.
Michailidou M, Brown HK, Lefley DV, Evans A, Cross SS, Coleman RE, et al. Microvascular endothelial cell responses in vitro and in vivo: modulation by zoledronic acid and paclitaxel? J Vasc Res. 2010;47(6):481–93.
Pasquier E, Honore S, Pourroy B, Jordan MA, Lehmann M, Briand C, et al. Antiangiogenic concentrations of paclitaxel induce an increase in microtubule dynamics in endothelial cells but not in cancer cells. Cancer Res. 2005;65(6):2433–40.
Zamora A, Alves M, Chollet C, Therville N, Fougeray T, Tatin F, et al. Paclitaxel induces lymphatic endothelial cells autophagy to promote metastasis. Cell Death Dis. 2019;10(12):956.
Hotchkiss KA, Ashton AW, Mahmood R, Russell RG, Sparano JA, Schwartz EL. Inhibition of endothelial cell function in vitro and angiogenesis in vivo by docetaxel (Taxotere): association with impaired repositioning of the microtubule organizing center. Mol Cancer Ther. 2002;1(13):1191–200.
Murtagh J, Lu H, Schwartz EL. Taxotere-induced inhibition of human endothelial cell migration is a result of heat shock protein 90 degradation. Cancer Res. 2006;66(16):8192–9.
Hu T, Yang C, Fu M, Yang J, Du R, Ran X, et al. Cytotoxic effects of docetaxel as a candidate drug of drug-eluting stent on human umbilical vein endothelial cells and the signaling pathway of cell migration inhibition, adhesion delay and shape change. Regen Biomater. 2017;4(3):167–78.
Lawrie A, Francis SE. Frataxin and endothelial cell senescence in pulmonary hypertension. J Clin Invest. 2021;131(11).
Bochenek ML, Schutz E, Schafer K. Endothelial cell senescence and thrombosis: ageing clots. Thromb Res. 2016;147:36–45.
Comi P, Chiaramonte R, Maier JA. Senescence-dependent regulation of type 1 plasminogen activator inhibitor in human vascular endothelial cells. Exp Cell Res. 1995;219(1):304–8.
Chen C, Zhou M, Ge Y, Wang X. SIRT1 and aging related signaling pathways. Mech Ageing Dev. 2020;187: 111215.
Ota H, Eto M, Ako J, Ogawa S, Iijima K, Akishita M, et al. Sirolimus and everolimus induce endothelial cellular senescence via sirtuin 1 down-regulation: therapeutic implication of cilostazol after drug-eluting stent implantation. J Am Coll Cardiol. 2009;53(24):2298–305.
Mailloux A, Grenet K, Bruneel A, Beneteau-Burnat B, Vaubourdolle M, Baudin B. Anticancer drugs induce necrosis of human endothelial cells involving both oncosis and apoptosis. Eur J Cell Biol. 2001;80(6):442–9.
Serizawa K, Yogo K, Aizawa K, Tashiro Y, Takahari Y, Sekine K, et al. Paclitaxel-induced endothelial dysfunction in living rats is prevented by nicorandil via reduction of oxidative stress. J Pharmacol Sci. 2012;119(4):349–58.
Wood SC, Tang X, Tesfamariam B. Paclitaxel potentiates inflammatory cytokine-induced prothrombotic molecules in endothelial cells. J Cardiovasc Pharmacol. 2010;55(3):276–85.
Sprowl JA, Reed K, Armstrong SR, Lanner C, Guo B, Kalatskaya I, et al. Alterations in tumor necrosis factor signaling pathways are associated with cytotoxicity and resistance to taxanes: a study in isogenic resistant tumor cells. Breast Cancer Res. 2012;14(1):R2.
Chan JM, Rhee JW, Drum CL, Bronson RT, Golomb G, Langer R, et al. In vivo prevention of arterial restenosis with paclitaxel-encapsulated targeted lipid-polymeric nanoparticles. Proc Natl Acad Sci USA. 2011;108(48):19347–52.
Finn AV, Nakazawa G, Joner M, Kolodgie FD, Mont EK, Gold HK, et al. Vascular responses to drug eluting stents: importance of delayed healing. Arterioscler Thromb Vasc Biol. 2007;27(7):1500–10.
Windecker S, Meier B. Late coronary stent thrombosis. Circulation. 2007;116(17):1952–65.
Stone GW, Moses JW, Ellis SG, Schofer J, Dawkins KD, Morice MC, et al. Safety and efficacy of sirolimus- and paclitaxel-eluting coronary stents. N Engl J Med. 2007;356(10):998–1008.
Marx SO, Totary-Jain H, Marks AR. Vascular smooth muscle cell proliferation in restenosis. Circ Cardiovasc Interv. 2011;4(1):104–11.
Axel DI, Kunert W, Goggelmann C, Oberhoff M, Herdeg C, Kuttner A, et al. Paclitaxel inhibits arterial smooth muscle cell proliferation and migration in vitro and in vivo using local drug delivery. Circulation. 1997;96(2):636–45.
Wiskirchen J, Schober W, Schart N, Kehlbach R, Wersebe A, Tepe G, et al. The effects of paclitaxel on the three phases of restenosis: smooth muscle cell proliferation, migration, and matrix formation: an in vitro study. Invest Radiol. 2004;39(9):565–71.
Jing L, Peng X, Xie MJ, Yu ZY, Wang W. Different responses of cell cycle between rat vascular smooth muscle cells and vascular endothelial cells to paclitaxel. J Huazhong Univ Sci Technolog Med Sci. 2014;34(3):370–5.
Park ES, Yoo JM, Lim Y, Tudev M, Yoo HS, Hong JT, et al. Inhibitory effects of docetaxel on platelet-derived growth factor (PDGF)-BB-induced proliferation of vascular smooth muscle cells through blocking PDGF-receptor beta phosphorylation. J Pharmacol Sci. 2011;116(2):204–13.
Gershlick A, De Scheerder I, Chevalier B, Stephens-Lloyd A, Camenzind E, Vrints C, et al. Inhibition of restenosis with a paclitaxel-eluting, polymer-free coronary stent: the European evaLUation of pacliTaxel Eluting Stent (ELUTES) trial. Circulation. 2004;109(4):487–93.
Zhao J, Yang M, Wu X, Yang Z, Jia P, Sun Y, et al. Effects of paclitaxel intervention on pulmonary vascular remodeling in rats with pulmonary hypertension. Exp Ther Med. 2019;17(2):1163–70.
Bonura F, Di Lisi D, Novo S, D’Alessandro N. Timely recognition of cardiovascular toxicity by anticancer agents: a common objective of the pharmacologist, oncologist and cardiologist. Cardiovasc Toxicol. 2012;12(2):93–107.
Zuppinger C, Timolati F, Suter TM. Pathophysiology and diagnosis of cancer drug induced cardiomyopathy. Cardiovasc Toxicol. 2007;7(2):61–6.
Polk A, Vistisen K, Vaage-Nilsen M, Nielsen DL. A systematic review of the pathophysiology of 5-fluorouracil-induced cardiotoxicity. BMC Pharmacol Toxicol. 2014;15:47.
Sara JD, Kaur J, Khodadadi R, Rehman M, Lobo R, Chakrabarti S, et al. 5-fluorouracil and cardiotoxicity: a review. Ther Adv Med Oncol. 2018;10:1758835918780140.
Shiga T, Hiraide M. Cardiotoxicities of 5-fluorouracil and other fluoropyrimidines. Curr Treat Options Oncol. 2020;21(4):27.
Dent RG, McColl I. Letter: 5-fluorouracil and angina. Lancet. 1975;1(7902):347–8.
Keefe DL, Roistacher N, Pierri MK. Clinical cardiotoxicity of 5-fluorouracil. J Clin Pharmacol. 1993;33(11):1060–70.
Li Y, Zhang Y, Zhou X, Lei X, Li X, Wei L. Dynamic observation of 5-fluorouracil-induced myocardial injury and mitochondrial autophagy in aging rats. Exp Ther Med. 2021;22(6):1451.
Li D, Song C, Zhang J, Zhao X. Resveratrol alleviated 5-FU-induced cardiotoxicity by attenuating GPX4 dependent ferroptosis. J Nutr Biochem. 2022:109241.
Focaccetti C, Bruno A, Magnani E, Bartolini D, Principi E, Dallaglio K, et al. Effects of 5-fluorouracil on morphology, cell cycle, proliferation, apoptosis, autophagy and ROS production in endothelial cells and cardiomyocytes. PLoS ONE. 2015;10(2): e0115686.
Becker K, Erckenbrecht JF, Haussinger D, Frieling T. Cardiotoxicity of the antiproliferative compound fluorouracil. Drugs. 1999;57(4):475–84.
Jensen SA, Sorensen JB. Risk factors and prevention of cardiotoxicity induced by 5-fluorouracil or capecitabine. Cancer Chemother Pharmacol. 2006;58(4):487–93.
Eskandari MR, Moghaddam F, Shahraki J, Pourahmad J. A comparison of cardiomyocyte cytotoxic mechanisms for 5-fluorouracil and its pro-drug capecitabine. Xenobiotica. 2015;45(1):79–87.
Bei Y, Fu S, Chen X, Chen M, Zhou Q, Yu P, et al. Cardiac cell proliferation is not necessary for exercise-induced cardiac growth but required for its protection against ischaemia/reperfusion injury. J Cell Mol Med. 2017;21(8):1648–55.
Durak I, Karaayvaz M, Kavutcu M, Cimen MY, Kacmaz M, Buyukkocak S, et al. Reduced antioxidant defense capacity in myocardial tissue from guinea pigs treated with 5-fluorouracil. J Toxicol Environ Health A. 2000;59(7):585–9.
Lamberti M, Porto S, Marra M, Zappavigna S, Grimaldi A, Feola D, et al. 5-Fluorouracil induces apoptosis in rat cardiocytes through intracellular oxidative stress. J Exp Clin Cancer Res. 2012;31(1):60.
Jiang X, Stockwell BR, Conrad M. Ferroptosis: mechanisms, biology and role in disease. Nat Rev Mol Cell Biol. 2021;22(4):266–82.
Miotto G, Rossetto M, Di Paolo ML, Orian L, Venerando R, Roveri A, et al. Insight into the mechanism of ferroptosis inhibition by ferrostatin-1. Redox Biol. 2020;28: 101328.
Song X, Wang X, Liu Z, Yu Z. Role of GPX4-mediated ferroptosis in the sensitivity of triple negative breast cancer cells to gefitinib. Front Oncol. 2020;10: 597434.
Li D, Song C, Zhang J, Zhao X. ROS and iron homeostasis dependent ferroptosis play a vital role in 5-Fluorouracil induced cardiotoxicity in vitro and in vivo. Toxicology. 2022;468: 153113.
Matsubara I, Kamiya J, Imai S. Cardiotoxic effects of 5-fluorouracil in the guinea pig. Jpn J Pharmacol. 1980;30(6):871–9.
Lischke J, Lang C, Sawodny O, Feuer R. Impairment of energy metabolism in cardiomyocytes caused by 5-FU catabolites can be compensated by administration of amino acids. Annu Int Conf IEEE Eng Med Biol Soc. 2015;2015:5363–6.
Knapik-Czajka M, Gawedzka A, Jurczyk M, Drag J, Belczyk M, Aleksandrovych V, et al. The influence of 5-fluorouracil on the α-ketoglutarate dehydrogenase complex in rat’s cardiac muscle—a preliminary study FOLIA MEDICA CRACOVIENSIA.LXII(2).
Strumilo S. Short-term regulation of the alpha-ketoglutarate dehydrogenase complex by energy-linked and some other effectors. Biochemistry (Mosc). 2005;70(7):726–9.
Mandziuk S, Kus P, Dudka J, Madej-Czerwonka B, Cendrowska-Pinkosz M, Iwan M, et al. Effect of hypoxia on toxicity induced by anticancer agents in cardiomyocyte culture. Med Weter. 2014;70(5):287.
Benedetto N, Calabrone L, Gutmanska K, Macri N, Cerrito MG, Ricotta R, et al. An olive oil mill wastewater extract improves chemotherapeutic activity against breast cancer cells while protecting from cardiotoxicity. Front Cardiovasc Med. 2022;9: 867867.
Layoun ME, Wickramasinghe CD, Peralta MV, Yang EH. Fluoropyrimidine-induced cardiotoxicity: manifestations, mechanisms, and management. Curr Oncol Rep. 2016;18(6):35.
Kinhult S, Albertsson M, Eskilsson J, Cwikiel M. Antithrombotic treatment in protection against thrombogenic effects of 5-fluorouracil on vascular endothelium: a scanning microscopy evaluation. Scanning. 2001;23(1):1–8.
Altieri P, Murialdo R, Barisione C, Lazzarini E, Garibaldi S, Fabbi P, et al. 5-fluorouracil causes endothelial cell senescence: potential protective role of glucagon-like peptide 1. Br J Pharmacol. 2017;174(21):3713–26.
Sudhoff T, Enderle MD, Pahlke M, Petz C, Teschendorf C, Graeven U, et al. 5-Fluorouracil induces arterial vasocontractions. Ann Oncol. 2004;15(4):661–4.
Rucker D, Dhamoon AS. Physiology, Thromboxane A2. StatPearls. Treasure Island (FL)2022.
Muhammad RN, Sallam N, El-Abhar HS. Activated ROCK/Akt/eNOS and ET-1/ERK pathways in 5-fluorouracil-induced cardiotoxicity: modulation by simvastatin. Sci Rep. 2020;10(1):14693.
Cwikiel M, Eskilsson J, Albertsson M, Stavenow L. The influence of 5-fluorouracil and methotrexate on vascular endothelium. An experimental study using endothelial cells in the culture. Ann Oncol. 1996;7(7):731–7.
Mosseri M, Fingert HJ, Varticovski L, Chokshi S, Isner JM. In vitro evidence that myocardial ischemia resulting from 5-fluorouracil chemotherapy is due to protein kinase C-mediated vasoconstriction of vascular smooth muscle. Cancer Res. 1993;53(13):3028–33.
Torella D, Curcio A, Gasparri C, Galuppo V, De Serio D, Surace FC, et al. Fludarabine prevents smooth muscle proliferation in vitro and neointimal hyperplasia in vivo through specific inhibition of STAT-1 activation. Am J Physiol Heart Circ Physiol. 2007;292(6):H2935–43.
Cragg AH, Stoll LL, Smith TP, Berbaum K. Effect of antineoplastic agents on smooth muscle cell proliferation in vitro: implications for prevention of restenosis after transluminal angioplasty. J Vasc Interv Radiol. 1992;3(2):273–7.
Labbadia J, Morimoto RI. The biology of proteostasis in aging and disease. Annu Rev Biochem. 2015;84:435–64.
Rousseau A, Bertolotti A. Regulation of proteasome assembly and activity in health and disease. Nat Rev Mol Cell Biol. 2018;19(11):697–712.
Henning RH, Brundel B. Proteostasis in cardiac health and disease. Nat Rev Cardiol. 2017;14(11):637–53.
Zhai Y, Ye X, Hu F, Xu J, Guo X, Cao Y, et al. Cardiovascular toxicity of carfilzomib: the real-world evidence based on the adverse event reporting system database of the FDA, the United States. Front Cardiovasc Med. 2021;8: 735466.
Bringhen S, Milan A, Ferri C, Wasch R, Gay F, Larocca A, et al. Cardiovascular adverse events in modern myeloma therapy—Incidence and risks. A review from the European Myeloma Network (EMN) and Italian Society of Arterial Hypertension (SIIA). Haematologica. 2018;103(9):1422–32.
Waxman AJ, Clasen S, Hwang WT, Garfall A, Vogl DT, Carver J, et al. Carfilzomib-associated cardiovascular adverse events: a systematic review and meta-analysis. JAMA Oncol. 2018;4(3): e174519.
Patel MB, Majetschak M. Distribution and interrelationship of ubiquitin proteasome pathway component activities and ubiquitin pools in various porcine tissues. Physiol Res. 2007;56(3):341–50.
Willis MS, Patterson C. Proteotoxicity and cardiac dysfunction–Alzheimer’s disease of the heart? N Engl J Med. 2013;368(5):455–64.
Willis MS, Patterson C. Proteotoxicity and cardiac dysfunction. N Engl J Med. 2013;368(18):1755.
Efentakis P, Kremastiotis G, Varela A, Nikolaou PE, Papanagnou ED, Davos CH, et al. Molecular mechanisms of carfilzomib-induced cardiotoxicity in mice and the emerging cardioprotective role of metformin. Blood. 2019;133(7):710–23.
Demo SD, Kirk CJ, Aujay MA, Buchholz TJ, Dajee M, Ho MN, et al. Antitumor activity of PR-171, a novel irreversible inhibitor of the proteasome. Cancer Res. 2007;67(13):6383–91.
Wang J, Fan Y, Wang C, Dube S, Poiesz BJ, Dube DK, et al. Inhibitors of the ubiquitin proteasome system block myofibril assembly in cardiomyocytes derived from chick embryos and human pluripotent stem cells. Cytoskeleton (Hoboken). 2021;78(10–12):461–91.
Tannous P, Zhu H, Nemchenko A, Berry JM, Johnstone JL, Shelton JM, et al. Intracellular protein aggregation is a proximal trigger of cardiomyocyte autophagy. Circulation. 2008;117(24):3070–8.
Zaha VG, Young LH. AMP-activated protein kinase regulation and biological actions in the heart. Circ Res. 2012;111(6):800–14.
Horman S, Beauloye C, Vanoverschelde JL, Bertrand L. AMP-activated protein kinase in the control of cardiac metabolism and remodeling. Curr Heart Fail Rep. 2012;9(3):164–73.
Kim DH, Sarbassov DD, Ali SM, King JE, Latek RR, Erdjument-Bromage H, et al. mTOR interacts with raptor to form a nutrient-sensitive complex that signals to the cell growth machinery. Cell. 2002;110(2):163–75.
Cole DC, Frishman WH. Cardiovascular complications of proteasome inhibitors used in multiple myeloma. Cardiol Rev. 2018;26(3):122–9.
Koulaouzidis G, Lyon AR. Proteasome inhibitors as a potential cause of heart failure. Heart Fail Clin. 2017;13(2):289–95.
Mendez-Lopez M, Besse A, Florea B, Zuppinger C, Overkleeft HS, Driessen C, et al. Carfilzomib induces cardiotoxicity via ß5/ß2-specific proteasome subunit inhibition pattern. Blood. 2019;134:3110.
Hasinoff BB, Patel D, Wu X. Molecular mechanisms of the cardiotoxicity of the proteasomal-targeted drugs bortezomib and carfilzomib. Cardiovasc Toxicol. 2017;17(3):237–50.
Forghani P, Rashid A, Sun F, Liu R, Li D, Lee MR, et al. Carfilzomib treatment causes molecular and functional alterations of human induced pluripotent stem cell-derived cardiomyocytes. J Am Heart Assoc. 2021;10(24): e022247.
Kastritis E, Laina A, Georgiopoulos G, Gavriatopoulou M, Papanagnou ED, Eleutherakis-Papaiakovou E, et al. Carfilzomib-induced endothelial dysfunction, recovery of proteasome activity, and prediction of cardiovascular complications: a prospective study. Leukemia. 2021;35(5):1418–27.
Buck B, Kellett E, Addison D, Vallakati A. Carfilzomib-induced cardiotoxicity: an analysis of the FDA adverse event reporting system (FAERS). J Saudi Heart Assoc. 2022;34(3):134–41.
Oshima T, Ikutomi M, Shinohara H, Ishiwata J, Fukino K, Amaki T, et al. Acute myocardial infarction caused by thrombotic microangiopathy complicated with myelodysplastic syndrome. Int Heart J. 2016;57(5):634–6.
Blasco M, Martinez-Roca A, Rodriguez-Lobato LG, Garcia-Herrera A, Rosinol L, Castro P, et al. Complement as the enabler of carfilzomib-induced thrombotic microangiopathy. Br J Haematol. 2021;193(1):181–7.
Guo HM, Sun L, Yang L, Liu XJ, Nie ZY, Luo JM. Microvesicles shed from bortezomib-treated or lenalidomide-treated human myeloma cells inhibit angiogenesis in vitro. Oncol Rep. 2018;39(6):2873–80.
Tamura D, Arao T, Tanaka K, Kaneda H, Matsumoto K, Kudo K, et al. Bortezomib potentially inhibits cellular growth of vascular endothelial cells through suppression of G2/M transition. Cancer Sci. 2010;101(6):1403–8.
Belloni D, Veschini L, Foglieni C, Dell’Antonio G, Caligaris-Cappio F, Ferrarini M, et al. Bortezomib induces autophagic death in proliferating human endothelial cells. Exp Cell Res. 2010;316(6):1010–8.
Chen-Scarabelli C, Corsetti G, Pasini E, Dioguardi FS, Sahni G, Narula J, et al. Spasmogenic effects of the proteasome inhibitor carfilzomib on coronary resistance, vascular tone and reactivity. EBioMedicine. 2017;21:206–12.
Efentakis P, Doerschmann H, Witzler C, Siemer S, Nikolaou PE, Kastritis E, et al. Investigating the vascular toxicity outcomes of the irreversible proteasome inhibitor carfilzomib. Int J Mol Sci. 2020;21(15):5185.
So EC, Liu PY, Lee CC, Wu SN. High effectiveness in actions of carfilzomib on delayed-rectifier K(+) current and on spontaneous action potentials. Front Pharmacol. 2019;10:1163.
Chen IC, Liu YC, Wu YH, Lo SH, Wang SC, Li CY, et al. Proteasome inhibitors decrease the viability of pulmonary arterial smooth muscle cells by restoring mitofusin-2 expression under hypoxic conditions. Biomedicines. 2022;10(4):873.
Wang YY, Luan Y, Zhang X, Lin M, Zhang ZH, Zhu XB, et al. Proteasome inhibitor PS-341 attenuates flow-induced pulmonary arterial hypertension. Clin Exp Med. 2014;14(3):321–9.
Zhang X, Wang ZS, Luan Y, Lin M, Zhu XB, Ma Y, et al. The effect of PS-341 on pulmonary vascular remodeling in high blood flow-induced pulmonary hypertension. Int J Mol Med. 2014;33(1):105–10.
Zhang J, Lu W, Chen Y, Jiang Q, Yang K, Li M, et al. Bortezomib alleviates experimental pulmonary hypertension by regulating intracellular calcium homeostasis in PASMCs. Am J Physiol Cell Physiol. 2016;311(3):C482–97.
Slamon DJ, Leyland-Jones B, Shak S, Fuchs H, Paton V, Bajamonde A, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. 2001;344(11):783–92.
Jerian S, Keegan P. Cardiotoxicity associated with paclitaxel/trastuzumab combination therapy. J Clin Oncol. 1999;17(5):1647–8.
Slamon D, Eiermann W, Robert N, Pienkowski T, Martin M, Press M, et al. Adjuvant trastuzumab in HER2-positive breast cancer. N Engl J Med. 2011;365(14):1273–83.
Cameron D, Piccart-Gebhart MJ, Gelber RD, Procter M, Goldhirsch A, de Azambuja E, et al. 11 years’ follow-up of trastuzumab after adjuvant chemotherapy in HER2-positive early breast cancer: final analysis of the HERceptin Adjuvant (HERA) trial. Lancet. 2017;389(10075):1195–205.
Onitilo AA, Engel JM, Stankowski RV. Cardiovascular toxicity associated with adjuvant trastuzumab therapy: prevalence, patient characteristics, and risk factors. Ther Adv Drug Saf. 2014;5(4):154–66.
Yang Z, Wang W, Wang X, Qin Z. Cardiotoxicity of epidermal growth factor receptor 2-targeted drugs for breast cancer. Front Pharmacol. 2021;12: 741451.
Cloud JE, Rogers C, Reza TL, Ziebold U, Stone JR, Picard MH, et al. Mutant mouse models reveal the relative roles of E2F1 and E2F3 in vivo. Mol Cell Biol. 2002;22(8):2663–72.
Perry MC, Dufour CR, Eichner LJ, Tsang DW, Deblois G, Muller WJ, et al. ERBB2 deficiency alters an E2F-1-dependent adaptive stress response and leads to cardiac dysfunction. Mol Cell Biol. 2014;34(23):4232–43.
ElZarrad MK, Mukhopadhyay P, Mohan N, Hao E, Dokmanovic M, Hirsch DS, et al. Trastuzumab alters the expression of genes essential for cardiac function and induces ultrastructural changes of cardiomyocytes in mice. PLoS ONE. 2013;8(11): e79543.
Necela BM, Axenfeld BC, Serie DJ, Kachergus JM, Perez EA, Thompson EA, et al. The antineoplastic drug, trastuzumab, dysregulates metabolism in iPSC-derived cardiomyocytes. Clin Transl Med. 2017;6(1):5.
Grazette LP, Boecker W, Matsui T, Semigran M, Force TL, Hajjar RJ, et al. Inhibition of ErbB2 causes mitochondrial dysfunction in cardiomyocytes: implications for herceptin-induced cardiomyopathy. J Am Coll Cardiol. 2004;44(11):2231–8.
Kitani T, Ong SG, Lam CK, Rhee JW, Zhang JZ, Oikonomopoulos A, et al. Human-induced pluripotent stem cell model of trastuzumab-induced cardiac dysfunction in patients with breast cancer. Circulation. 2019;139(21):2451–65.
Fernandez-Marcos PJ, Auwerx J. Regulation of PGC-1alpha, a nodal regulator of mitochondrial biogenesis. Am J Clin Nutr. 2011;93(4):884S-S890.
Tian XY, Ma S, Tse G, Wong WT, Huang Y. Uncoupling protein 2 in cardiovascular health and disease. Front Physiol. 2018;9:1060.
Neumiller JJ. Empagliflozin: a new sodium-glucose co-transporter 2 (SGLT2) inhibitor for the treatment of type 2 diabetes. Drugs Context. 2014;3: 212262.
Min J, Wu L, Liu Y, Song G, Deng Q, Jin W, et al. Empagliflozin attenuates trastuzumab-induced cardiotoxicity through suppression of DNA damage and ferroptosis. Life Sci. 2023;312: 121207.
Jakubczyk K, Druzga A, Katarzyna J, Skonieczna-Zydecka K. Antioxidant potential of curcumin-a meta-analysis of randomized clinical trials. Antioxidants (Basel). 2020;9(11):1092.
Kohandel Z, Farkhondeh T, Aschner M, Samarghandian S. Anti-inflammatory effects of thymoquinone and its protective effects against several diseases. Biomed Pharmacother. 2021;138: 111492.
Khezri S, Sabzalipour T, Jahedsani A, Azizian S, Atashbar S, Salimi A. Chrysin ameliorates aluminum phosphide-induced oxidative stress and mitochondrial damages in rat cardiomyocytes and isolated mitochondria. Environ Toxicol. 2020;35(10):1114–24.
Shirmard LR, Shabani M, Moghadam AA, Zamani N, Ghanbari H, Salimi A. Protective effect of curcumin, chrysin and thymoquinone injection on trastuzumab-induced cardiotoxicity via mitochondrial protection. Cardiovasc Toxicol. 2022;22(7):663–75.
Nakai A, Yamaguchi O, Takeda T, Higuchi Y, Hikoso S, Taniike M, et al. The role of autophagy in cardiomyocytes in the basal state and in response to hemodynamic stress. Nat Med. 2007;13(5):619–24.
Mohan N, Shen Y, Endo Y, ElZarrad MK, Wu WJ. Trastuzumab, but not pertuzumab, dysregulates HER2 signaling to mediate inhibition of autophagy and increase in reactive oxygen species production in human cardiomyocytes. Mol Cancer Ther. 2016;15(6):1321–31.
Alhussein MM, Mokbel A, Cosman T, Aghel N, Yang EH, Mukherjee SD, et al. Pertuzumab cardiotoxicity in patients with HER2-positive cancer: a systematic review and meta-analysis. CJC Open. 2021;3(11):1372–82.
Sasaki R, Kurebayashi N, Eguchi H, Horimoto Y, Shiga T, Miyazaki S, et al. Involvement of kallikrein-PAR2-proinflammatory pathway in severe trastuzumab-induced cardiotoxicity. Cancer Sci. 2022;113(10):3449–62.
Moriyuki K, Sekiguchi F, Matsubara K, Nishikawa H, Kawabata A. Proteinase-activated receptor-2-triggered prostaglandin E(2) release, but not cyclooxygenase-2 upregulation, requires activation of the phosphatidylinositol 3-kinase/Akt / nuclear factor-kappaB pathway in human alveolar epithelial cells. J Pharmacol Sci. 2009;111(3):269–75.
Ghorpade DS, Ozcan L, Zheng Z, Nicoloro SM, Shen Y, Chen E, et al. Hepatocyte-secreted DPP4 in obesity promotes adipose inflammation and insulin resistance. Nature. 2018;555(7698):673–7.
Laird-Fick HS, Tokala H, Kandola S, Kehdi M, Pelosi A, Wang L, et al. Early morphological changes in cardiac mitochondria after subcutaneous administration of trastuzumab in rabbits: possible prevention with oral selenium supplementation. Cardiovasc Pathol. 2020;44: 107159.
Jiang J, Mohan N, Endo Y, Shen Y, Wu WJ. Type IIB DNA topoisomerase is downregulated by trastuzumab and doxorubicin to synergize cardiotoxicity. Oncotarget. 2018;9(5):6095–108.
Hsu WT, Huang CY, Yen CYT, Cheng AL, Hsieh PCH. The HER2 inhibitor lapatinib potentiates doxorubicin-induced cardiotoxicity through iNOS signaling. Theranostics. 2018;8(12):3176–88.
Kumar R, Yarmand-Bagheri R. The role of HER2 in angiogenesis. Semin Oncol. 2001;28(5 Suppl 16):27–32.
Onyeisi JOS, Castanho de Almeida Pernambuco Filho P, de Araujo Lopes S, Nader HB, Lopes CC. Heparan sulfate proteoglycans as trastuzumab targets in anoikis-resistant endothelial cells. J Cell Biochem. 2019;120(8):13826–40.
Edwards IJ, Wagner JD, Vogl-Willis CA, Litwak KN, Cefalu WT. Arterial heparan sulfate is negatively associated with hyperglycemia and atherosclerosis in diabetic monkeys. Cardiovasc Diabetol. 2004;3:6.
Iozzo RV. Basement membrane proteoglycans: from cellar to ceiling. Nat Rev Mol Cell Biol. 2005;6(8):646–56.
Nonaka R, Iesaki T, de Vega S, Daida H, Okada T, Sasaki T, et al. Perlecan deficiency causes endothelial dysfunction by reducing the expression of endothelial nitric oxide synthase. Physiol Rep. 2015;3(1):e12272.
Lemmens K, Doggen K, De Keulenaer GW. Role of neuregulin-1/ErbB signaling in cardiovascular physiology and disease: implications for therapy of heart failure. Circulation. 2007;116(8):954–60.
Pentassuglia L, Sawyer DB. The role of Neuregulin-1beta/ErbB signaling in the heart. Exp Cell Res. 2009;315(4):627–37.
Yersal O, Eryilmaz U, Akdam H, Meydan N, Barutca S. Arterial stiffness in breast cancer patients treated with anthracycline and trastuzumab-based regimens. Cardiol Res Pract. 2018;2018:5352914.
Pacheco Mendes A, Nogueira J, Mendes A, Cochicho J, Lavadinho I. A case report of an emergency hypertensive episode during trastuzumab therapy. Cureus. 2021;13(8): e17015.
Herrmann J, Herrmann SM, Haddad TC. New-onset heart failure in association with severe hypertension during trastuzumab therapy. Mayo Clin Proc. 2014;89(12):1734–9.
Touyz RM, Alves-Lopes R, Rios FJ, Camargo LL, Anagnostopoulou A, Arner A, et al. Vascular smooth muscle contraction in hypertension. Cardiovasc Res. 2018;114(4):529–39.
Tan S, Day D, Nicholls SJ, Segelov E. Immune checkpoint inhibitor therapy in oncology: current uses and future directions: JACC: cardiooncology state-of-the-art review. JACC CardioOncol. 2022;4(5):579–97.
Hu JR, Florido R, Lipson EJ, Naidoo J, Ardehali R, Tocchetti CG, et al. Cardiovascular toxicities associated with immune checkpoint inhibitors. Cardiovasc Res. 2019;115(5):854–68.
Zhou YW, Zhu YJ, Wang MN, Xie Y, Chen CY, Zhang T, et al. Immune checkpoint inhibitor-associated cardiotoxicity: current understanding on its mechanism, diagnosis and management. Front Pharmacol. 2019;10:1350.
Hodi FS, O’Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363(8):711–23.
Varricchi G, Galdiero MR, Marone G, Criscuolo G, Triassi M, Bonaduce D, et al. Cardiotoxicity of immune checkpoint inhibitors. ESMO Open. 2017;2(4): e000247.
Liang L, Ge K, Zhang F, Ge Y. The suppressive effect of co-inhibiting PD-1 and CTLA-4 expression on H22 hepatomas in mice. Cell Mol Biol Lett. 2018;23:58.
Larkin J, Hodi FS, Wolchok JD. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N Engl J Med. 2015;373(13):1270–1.
Okazaki T, Tanaka Y, Nishio R, Mitsuiye T, Mizoguchi A, Wang J, et al. Autoantibodies against cardiac troponin I are responsible for dilated cardiomyopathy in PD-1-deficient mice. Nat Med. 2003;9(12):1477–83.
Grabie N, Gotsman I, DaCosta R, Pang H, Stavrakis G, Butte MJ, et al. Endothelial programmed death-1 ligand 1 (PD-L1) regulates CD8+ T-cell mediated injury in the heart. Circulation. 2007;116(18):2062–71.
Lucas JA, Menke J, Rabacal WA, Schoen FJ, Sharpe AH, Kelley VR. Programmed death ligand 1 regulates a critical checkpoint for autoimmune myocarditis and pneumonitis in MRL mice. J Immunol. 2008;181(4):2513–21.
Wei SC, Meijers WC, Axelrod ML, Anang NAS, Screever EM, Wescott EC, et al. A genetic mouse model recapitulates immune checkpoint inhibitor-associated myocarditis and supports a mechanism-based therapeutic intervention. Cancer Discov. 2021;11(3):614–25.
Sobol I, Chen CL, Mahmood SS, Borczuk AC. Histopathologic characterization of myocarditis associated with immune checkpoint inhibitor therapy. Arch Pathol Lab Med. 2020;144(11):1392–6.
Champion SN, Stone JR. Immune checkpoint inhibitor associated myocarditis occurs in both high-grade and low-grade forms. Mod Pathol. 2020;33(1):99–108.
Palaskas NL, Segura A, Lelenwa L, Siddiqui BA, Subudhi SK, Lopez-Mattei J, et al. Immune checkpoint inhibitor myocarditis: elucidating the spectrum of disease through endomyocardial biopsy. Eur J Heart Fail. 2021;23(10):1725–35.
Quagliariello V, Passariello M, Rea D, Barbieri A, Iovine M, Bonelli A, et al. Evidences of CTLA-4 and PD-1 blocking agents-induced cardiotoxicity in cellular and preclinical models. J Pers Med. 2020;10(4):179.
Zhang Y, Sun C, Li Y, Qin J, Amancherla K, Jing Y, et al. Hormonal therapies up-regulate MANF and overcome female susceptibility to immune checkpoint inhibitor myocarditis. Sci Transl Med. 2022;14(669):eabo1981.
Liu YX, Song YJ, Liu XH, Xu SC, Kong C, Chen LF, et al. PD-1 inhibitor induces myocarditis by reducing regulatory T cells, activating inflammatory responses, promoting myocardial apoptosis and autophagy. Cytokine. 2022;157: 155932.
Veluswamy P, Wacker M, Scherner M, Wippermann J. Delicate role of PD-L1/PD-1 axis in blood vessel inflammatory diseases: current insight and future significance. Int J Mol Sci. 2020;21(21):8159.
Kushnareva E, Kushnarev V, Artemyeva A, Mitrofanova L, Moiseeva O. Myocardial PD-L1 expression in patients with ischemic and non-ischemic heart failure. Front Cardiovasc Med. 2021;8: 759972.
Poels K, van Leent MMT, Reiche ME, Kusters PJH, Huveneers S, de Winther MPJ, et al. Antibody-mediated inhibition of CTLA4 aggravates atherosclerotic plaque inflammation and progression in hyperlipidemic mice. Cells. 2020;9(9):1987.
Koga N, Suzuki J, Kosuge H, Haraguchi G, Onai Y, Futamatsu H, et al. Blockade of the interaction between PD-1 and PD-L1 accelerates graft arterial disease in cardiac allografts. Arterioscler Thromb Vasc Biol. 2004;24(11):2057–62.
Smith WL, Garavito RM, DeWitt DL. Prostaglandin endoperoxide H synthases (cyclooxygenases)-1 and -2. J Biol Chem. 1996;271(52):33157–60.
Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Back M, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021;42(34):3227–337.
Rachidi S, Metelli A, Riesenberg B, Wu BX, Nelson MH, Wallace C, et al. Platelets subvert T cell immunity against cancer via GARP-TGFbeta axis. Sci Immunol. 2017;2(11):eaai7911.
Lichtenberger LM, Fang D, Bick RJ, Poindexter BJ, Phan T, Bergeron AL, et al. Unlocking Aspirin’s chemopreventive activity: role of irreversibly inhibiting platelet cyclooxygenase-1. Cancer Prev Res (Phila). 2017;10(2):142–52.
Bagheri M, Tabatabae Far MA, Mirzaei H, Ghasemi F. Evaluation of antitumor effects of aspirin and LGK974 drugs on cellular signaling pathways, cell cycle and apoptosis in colorectal cancer cell lines compared to oxaliplatin drug. Fundam Clin Pharmacol. 2020;34(1):51–64.
Janakiram NB, Rao CV. The role of inflammation in colon cancer. Adv Exp Med Biol. 2014;816:25–52.
Shao J, Jung C, Liu C, Sheng H. Prostaglandin E2 Stimulates the beta-catenin/T cell factor-dependent transcription in colon cancer. J Biol Chem. 2005;280(28):26565–72.
Kune GA, Kune S, Watson LF. Colorectal cancer risk, chronic illnesses, operations, and medications: case control results from the Melbourne Colorectal Cancer Study. Cancer Res. 1988;48(15):4399–404.
Ishida J, Konishi M, Ebner N, Springer J. Repurposing of approved cardiovascular drugs. J Transl Med. 2016;14:269.
Rothwell PM, Wilson M, Elwin CE, Norrving B, Algra A, Warlow CP, et al. Long-term effect of aspirin on colorectal cancer incidence and mortality: 20-year follow-up of five randomised trials. Lancet. 2010;376(9754):1741–50.
Kawazoe N, Aiuchi T, Masuda Y, Nakajo S, Nakaya K. Induction of apoptosis by bufalin in human tumor cells is associated with a change of intracellular concentration of Na+ ions. J Biochem. 1999;126(2):278–86.
Raghavendra PB, Sreenivasan Y, Ramesh GT, Manna SK. Cardiac glycoside induces cell death via FasL by activating calcineurin and NF-AT, but apoptosis initially proceeds through activation of caspases. Apoptosis. 2007;12(2):307–18.
Prassas I, Diamandis EP. Novel therapeutic applications of cardiac glycosides. Nat Rev Drug Discov. 2008;7(11):926–35.
Osman MH, Farrag E, Selim M, Osman MS, Hasanine A, Selim A. Cardiac glycosides use and the risk and mortality of cancer; systematic review and meta-analysis of observational studies. PLoS ONE. 2017;12(6): e0178611.
Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111–88.
Gelosa P, Castiglioni L, Camera M, Sironi L. Repurposing of drugs approved for cardiovascular diseases: opportunity or mirage? Biochem Pharmacol. 2020;177: 113895.
Ogunwobi OO, Beales IL. Statins inhibit proliferation and induce apoptosis in Barrett’s esophageal adenocarcinoma cells. Am J Gastroenterol. 2008;103(4):825–37.
Kang S, Kim ES, Moon A. Simvastatin and lovastatin inhibit breast cell invasion induced by H-Ras. Oncol Rep. 2009;21(5):1317–22.
Wu XD, Zeng K, Xue FQ, Chen JH, Chen YQ. Statins are associated with reduced risk of gastric cancer: a meta-analysis. Eur J Clin Pharmacol. 2013;69(10):1855–60.
Singh S, Singh AG, Singh PP, Murad MH, Iyer PG. Statins are associated with reduced risk of esophageal cancer, particularly in patients with Barrett’s esophagus: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2013;11(6):620–9.
Li L, Cui N, Hao T, Zou J, Jiao W, Yi K, et al. Statins use and the prognosis of colorectal cancer: a meta-analysis. Clin Res Hepatol Gastroenterol. 2021;45(5): 101588.
Beckwitt CH, Brufsky A, Oltvai ZN, Wells A. Statin drugs to reduce breast cancer recurrence and mortality. Breast Cancer Res. 2018;20(1):144.
Deshayes F, Nahmias C. Angiotensin receptors: a new role in cancer? Trends Endocrinol Metab. 2005;16(7):293–9.
Sun H, Li T, Zhuang R, Cai W, Zheng Y. Do renin-angiotensin system inhibitors influence the recurrence, metastasis, and survival in cancer patients? Evidence from a meta-analysis including 55 studies. Medicine (Baltimore). 2017;96(13): e6394.
Thaker PH, Han LY, Kamat AA, Arevalo JM, Takahashi R, Lu C, et al. Chronic stress promotes tumor growth and angiogenesis in a mouse model of ovarian carcinoma. Nat Med. 2006;12(8):939–44.
Na Z, Qiao X, Hao X, Fan L, Xiao Y, Shao Y, et al. The effects of beta-blocker use on cancer prognosis: a meta-analysis based on 319,006 patients. Onco Targets Ther. 2018;11:4913–44.
Jain D, Russell RR, Schwartz RG, Panjrath GS, Aronow W. Cardiac complications of cancer therapy: pathophysiology, identification, prevention, treatment, and future directions. Curr Cardiol Rep. 2017;19(5):36.
Alves AC, Ribeiro D, Horta M, Lima J, Nunes C, Reis S. A biophysical approach to daunorubicin interaction with model membranes: relevance for the drug’s biological activity. J R Soc Interface. 2017;14(133):20170408.
Jain D, Aronow W. Cardiotoxicity of cancer chemotherapy in clinical practice. Hosp Pract (1995). 2019;47(1):6–15.
Meinardi MT, Van Der Graaf WT, Gietema JA, Van Den Berg MP, Sleijfer DT, De Vries EG, et al. Evaluation of long term cardiotoxicity after epirubicin containing adjuvant chemotherapy and locoregional radiotherapy for breast cancer using various detection techniques. Heart. 2002;88(1):81–2.
Chiorcea-Paquim AM, Oliveira-Brett AM. Electrochemistry of chemotherapeutic alkylating agents and their interaction with DNA. J Pharm Biomed Anal. 2023;222: 115036.
Morandi P, Ruffini PA, Benvenuto GM, Raimondi R, Fosser V. Cardiac toxicity of high-dose chemotherapy. Bone Marrow Transplant. 2005;35(4):323–34.
Polk A, Vaage-Nilsen M, Vistisen K, Nielsen DL. Cardiotoxicity in cancer patients treated with 5-fluorouracil or capecitabine: a systematic review of incidence, manifestations and predisposing factors. Cancer Treat Rev. 2013;39(8):974–84.
Depetris I, Marino D, Bonzano A, Cagnazzo C, Filippi R, Aglietta M, et al. Fluoropyrimidine-induced cardiotoxicity. Crit Rev Oncol Hematol. 2018;124:1–10.
Siddall E, Khatri M, Radhakrishnan J. Capillary leak syndrome: etiologies, pathophysiology, and management. Kidney Int. 2017;92(1):37–46.
Khan MF, Gottesman S, Boyella R, Juneman E. Gemcitabine-induced cardiomyopathy: a case report and review of the literature. J Med Case Rep. 2014;8:220.
Abu Samaan TM, Samec M, Liskova A, Kubatka P, Busselberg D. Paclitaxel’s mechanistic and clinical effects on breast cancer. Biomolecules. 2019;9(12):789.
Wordeman L, Vicente JJ. Microtubule targeting agents in disease: classic drugs, novel roles. Cancers (Basel). 2021;13(22):5650.
Skubnik J, Pavlickova VS, Ruml T, Rimpelova S. Vincristine in combination therapy of cancer: emerging trends in clinics. Biology (Basel). 2021;10(9):849.
Adao R, de Keulenaer G, Leite-Moreira A, Bras-Silva C. Cardiotoxicity associated with cancer therapy: pathophysiology and prevention strategies. Rev Port Cardiol. 2013;32(5):395–409.
Johnstone TC, Park GY, Lippard SJ. Understanding and improving platinum anticancer drugs–phenanthriplatin. Anticancer Res. 2014;34(1):471–6.
Gao Y, Shang Q, Li W, Guo W, Stojadinovic A, Mannion C, et al. Antibiotics for cancer treatment: a double-edged sword. J Cancer. 2020;11(17):5135–49.
Murray V, Chen JK, Chung LH. The Interaction of the metallo-glycopeptide anti-tumour drug bleomycin with DNA. Int J Mol Sci. 2018;19(5):1372.
Madeddu C, Deidda M, Piras A, Cadeddu C, Demurtas L, Puzzoni M, et al. Pathophysiology of cardiotoxicity induced by nonanthracycline chemotherapy. J Cardiovasc Med (Hagerstown). 2016;17(Suppl 1):S12–8.
Fink EC, Ebert BL. The novel mechanism of lenalidomide activity. Blood. 2015;126(21):2366–9.
Lee DH, Fradley MG. Cardiovascular complications of multiple myeloma treatment: evaluation, management, and prevention. Curr Treat Options Cardiovasc Med. 2018;20(3):19.
Copeland-Halperin RS, Liu JE, Yu AF. Cardiotoxicity of HER2-targeted therapies. Curr Opin Cardiol. 2019;34(4):451–8.
Zhou C. Multi-targeted tyrosine kinase inhibitors for the treatment of non-small cell lung cancer: an era of individualized therapy. Transl Lung Cancer Res. 2012;1(1):72–7.
Chung R, Tyebally S, Chen D, Kapil V, Walker JM, Addison D, et al. Hypertensive cardiotoxicity in cancer treatment-systematic analysis of adjunct, conventional chemotherapy, and novel therapies-epidemiology, incidence, and pathophysiology. J Clin Med. 2020;9(10):3346.
Jin Y, Xu Z, Yan H, He Q, Yang X, Luo P. A comprehensive review of clinical cardiotoxicity incidence of FDA-approved small-molecule kinase inhibitors. Front Pharmacol. 2020;11:891.
Karaagac M, Eryilmaz MK. Pazopanib-induced fatal heart failure in a patient with unresectable soft tissue sarcoma and review of literature. J Oncol Pharm Pract. 2020;26(3):768–74.
Nunes AT, Annunziata CM. Proteasome inhibitors: structure and function. Semin Oncol. 2017;44(6):377–80.
Wu P, Oren O, Gertz MA, Yang EH. Proteasome inhibitor-related cardiotoxicity: mechanisms, diagnosis, and management. Curr Oncol Rep. 2020;22(7):66.
Lyon AR, Yousaf N, Battisti NML, Moslehi J, Larkin J. Immune checkpoint inhibitors and cardiovascular toxicity. Lancet Oncol. 2018;19(9):e447–58.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Conceptualization: PU and KK, formal analysis: AT and KK, Writing—original draft: PU, JM, AL, DR, AN, JMP, and KK, Writing—final version of the manuscript: PU, JMP, AT, and KK. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Uruski, P., Matuszewska, J., Leśniewska, A. et al. An integrative review of nonobvious puzzles of cellular and molecular cardiooncology. Cell Mol Biol Lett 28, 44 (2023). https://doi.org/10.1186/s11658-023-00451-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s11658-023-00451-y