
Abstract
The COVID-19 pandemic forced governments globally to impose lockdown measures and mobility restrictions to curb the transmission of the virus. As economies slowly reopen, governments face a trade-off between implementing economic recovery and health policy measures to control the spread of the virus and to ensure it will not overwhelm the health system. We developed a mathematical model that measures the economic losses due to the spread of the disease and due to different lockdown policies. This is done by extending the subnational SEIR model to include two differential equations that capture economic losses due to COVID-19 infection and due to the lockdown measures imposed by the Philippine government. We then proceed to assess the trade-off policy space between health and economic measures faced by the Philippine government. The study simulates the cumulative economic losses for 3 months in 8 scenarios across 5 regions in the country, including the National Capital Region (NCR), to capture the trade-off mechanism. These scenarios present the various combinations of either retaining or easing lockdown policies in these regions. Per region, the trade-off policy space was assessed through minimising the 3-month cumulative economic losses subject to the constraint that the average health-care utilisation rate (HCUR) consistently falls below 70%, which is the threshold set by the government before declaring that the health system capacity is at high risk. The study finds that in NCR, a policy trade-off exists where the minimum cumulative economic losses comprise 10.66% of its Gross Regional Domestic Product. Meanwhile, for regions that are non-adjacent to NCR, a policy that hinges on trade-off analysis does not apply. Nevertheless, for all simulated regions, it is recommended to improve and expand the capacity of the health system to broaden the policy space for the government in easing lockdown measures.
Similar content being viewed by others


Introduction
The Philippine population of 110 million comprises a relatively young population. On May 22, 2021, the number of confirmed COVID-19 cases reported in the country is 1,171,403 with 55,531 active cases, 1,096,109 who recovered, and 19,763 who died. As a consequence of the pandemic, the real gross domestic product (GDP) contracted by 9.6% year-on-year in 2020—the sharpest decline since the Philippine Statistical Agency (PSA) started collecting data on annual growth rates in 1946 (Bangko Sentral ng Pilipinas, 2021). The strictest lockdown imposed from March to April 2020 had the most severe repercussions to the economy, but restrictions soon after have generally eased on economic activities all over the country. However, schools at all levels remain closed and minimum restrictions are still imposed in business operations particularly in customer accommodation capacity in service establishments.
The government is poised for a calibrated reopening of business, mass transportation, and the relaxation of age group restrictions. The government expects a strong recovery before the end of 2021, when enough vaccines have been rolled out against COVID-19. However, the economic recovery plan and growth targets at the end of the year are put in doubt with the first quarter of 2021 growth rate of GDP at -4.2%. This is exacerbated by the surge of cases in March 2021 that took the National Capital Region (NCR) and contiguous provinces by surprise, straining the hospital bed capacity of the region beyond its limits. The government had to reinforce stricter lockdown measures and curfew hours to stem the rapid spread of the virus. The country’s economic development authority proposes to ensure hospitals have enough capacity to allow the resumption of social and economic activities (National Economic and Development Authority, 2020). This is justified by pointing out that the majority of COVID-19 cases are mild and asymptomatic.
Efforts in monitoring and mitigating the spread of COVID-19 requires understanding the behaviour of the disease through the development of localised disease models operationalized as an ICT tool accessible to policymakers. FASSSTER is a scenario-based disease surveillance and modelling platform designed to accommodate multiple sources of data as input allowing for a variety of disease models and analytics to generate meaningful information to its stakeholders (FASSSTER, 2020). FASSSTER’s module on COVID-19 currently provides information and forecasts from national down to city/municipality level that are used for decision-making by individual local government units (LGUs) and also by key government agencies in charge of the pandemic response.
In this paper, we develop a mathematical model that measures the economic losses due to the spread of the disease and due to different lockdown policies to contain the disease. This is done by extending the FASSSTER subnational Susceptible-Exposed-Infectious-Recovered (SEIR) model to include two differential equations that capture economic losses due to COVID-19 infection and due to the lockdown measures imposed by the Philippine government. We then proceed to assess the trade-off policy space faced by the Philippine government given the policy that health-care utilisation rate must not be more than 70%, which is the threshold set by the government before declaring that the health system capacity is at high risk.
We simulate the cumulative economic losses for 3 months in 8 scenarios across 5 regions in the country, including the National Capital Region (NCR) to capture the trade-off mechanism. These 8 scenarios present the various combinations of either retaining or easing lockdown policies in these regions. Per region, the trade-off policy space was assessed through minimising the 3-month cumulative economic losses subject to the constraint that the average health-care utilisation rate (HCUR) consistently falls below 70%. The study finds that in NCR, a policy trade-off exists where the minimum economic losses below the 70% average HCUR comprise 10.66% of its Gross Regional Domestic Product. Meanwhile, for regions that are non-adjacent to NCR, a policy that hinges on trade-off analysis does not apply. Nevertheless, for all simulated regions, it is recommended to improve and expand the capacity of the health system to broaden the policy space for the government in easing lockdown measures.
The sections of the paper proceed as follows: the first section reviews the literature, the second section explains the FASSSTER SEIR model, the third section discusses the economic dynamic model, the fourth section specifically explains the parameters used in the economic model, the fifth section briefly lays out the policy trade-off model, the sixth discusses the methods used in implementing the model, the seventh section presents the results of the simulations, the eighth section discusses and interprets the results, and the final section presents the conclusion.
Review of related literature
Overview of the economic shocks of pandemics
The onslaught of the Coronavirus Disease 2019 (COVID-19) pandemic since 2020 has disrupted lifestyles and livelihoods as governments restrict mobility and economic activity in their respective countries. Unfortunately, this caused a –3.36% decline in the 2020 global economy (World Bank, 2022), which will have pushed 71 million people into extreme poverty (World Bank, 2020; 2021).
As an economic phenomenon, pandemics may be classified under the typologies of disaster economics. Particularly, a pandemic’s impacts may be classified according to the following (Benson and Clay, 2004; Noy et al., 2020; Keogh-Brown et al., 2010; 2020; McKibbin and Fernando, 2020; Verikios et al., 2012): (a) direct impacts, where pandemics cause direct labour supply shocks due to mortality and infection; (b) indirect impacts on productivity, firm revenue, household income, and other welfare effects, and; (c) macroeconomic impacts of a pandemic.
For most pandemic scenarios, social distancing and various forms of lockdowns imposed by countries around the world had led to substantial disruptions in the supply-side of the economy with mandatory business closures (Maital and Barzani, 2020; Keogh-Brown et al., 2010). Social distancing will have contracted labour supply as well, thus contributing to contractions in the macroeconomy (Geard et al., 2020; Keogh-Brown et al., 2010). Thus, in general, the literature points to a pandemic’s impacts on the supply- and demand-side, as well as the displacement of labour supply; thus, resulting in lower incomes (Genoni et al., 2020; Hupkau et al., 2020; United Nations Development Programme, 2021). Often, these shocks result from the lockdown measures; thus, a case of a trade-off condition between economic losses and the number of COVID-19 casualties.
Static simulations for the economic impacts of a pandemic
The typologies above are evident in the analyses and simulations on welfare and macroeconomic losses related to a pandemic. For instance, computable general equilibrium (CGE) and microsimulation analyses for the 2009 H1N1 pandemic and the COVID-19 pandemic showed increases in inequities, welfare losses, and macroeconomic losses due to lockdown and public prevention strategies (Cereda et al., 2020; Keogh-Brown et al., 2020; Keogh-Brown et al., 2010). Public prevention-related labour losses also comprised at most 25% of the losses in GDP in contrast with health-related losses, which comprised only at most 17% of the losses in GDP.
Amidst the COVID-19 pandemic in Ghana, Amewu et al. (2020) find in a social accounting matrix-based analysis that the industry and services sectors will have declined by 26.8% and 33.1%, respectively. Other studies investigate the effects of the pandemic on other severely hit sectors such as the tourism sector. Pham et al. (2021) note that a reduction in tourism demand in Australia will have caused a reduction in income of tourism labourers. Meanwhile, in a static CGE-microsimulation model by Laborde, Martin, and Vos (2021), they show that as the global GDP will have contracted by 5% following the reduction in labour supply, this will have increased global poverty by 20%, global rural poverty by 15%, poverty in sub-Saharan Africa by 23%, and in South Asia by 15%.
However, due to the static nature of these analyses, the clear trade-off between economic and health costs under various lockdown scenarios is a policy message that remains unexplored, as the simulations above only explicitly tackle a pandemic’s macroeconomic effects. This gap is mostly due to these studies’ usage of static SAM- and CGE-based analyses.
Dynamic simulations for the economic impacts of a pandemic
An obvious advantage of dynamic models over static approaches in estimating the economic losses from the pandemic is the capacity to provide forward-looking insights that have practical use in policymaking. Epidemiological models based on systems of differential equations explicitly model disease spread and recovery as movements of population across different compartments. These compartmental models are useful in forecasting the number of infected individuals, critically ill patients, death toll, among others, and thus are valuable in determining the appropriate intervention to control epidemics.
To date, the Susceptible-Infectious-Recovered (SIR) and SEIR models are among the most popular compartmental models used to study the spread of diseases. In recent years, COVID-19 has become an important subject of more recent mathematical modelling studies. Many of these studies deal with both application and refinement of both SIR and SEIR to allow scenario-building, conduct evaluation of containment measures, and improve forecasts. These include the integration of geographical heterogeneities, the differentiation between isolated and non-isolated cases, and the integration of interventions such as reducing contact rate and isolation of active cases (Anand et al., 2020; Chen et al., 2020; Hou et al., 2020; Peng et al., 2020; Reno et al., 2020).
Typical epidemiological models may provide insight on the optimal lockdown measure to reduce the transmissibility of a virus. However, there is a need to derive calculations on economic impacts from the COVID-19 case projections to arrive at a conclusion on the optimal frontier from the trade-off between health and economic losses. In Goldsztejn, Schwartzman and Nehorai (2020), an economic model that measures lost economic productivity due to the pandemic, disease containment measures and economic policies is integrated into an SEIR model. The hybrid model generates important insight on the trade-offs between short-term economic gains in terms of productivity, and the continuous spread of the disease, which in turn informs policymakers on the appropriate containment policies to be implemented.
This approach was further improved by solving an optimal control of multiple group SIR model to find the best way to implement a lockdown (Acemoglu et al., 2020). Noting the trade-offs between economic outcomes and spread of disease implied in lockdown policies, Acemoglu et al. (2020) find that targeted lockdown yields the best result in terms of economic losses and saving lives. However, Acemoglu et al. (2020) only determine the optimal lockdown policy and their trade-off analysis through COVID-associated fatalities. Kashyap et al. (2020) note that hospitalisations may be better indicators for lockdown and, as a corollary, reopening policies.
Gaps in the literature
With the recency of the pandemic, there is an increasing but limited scholarship in terms of jointly analysing the losses brought about by the pandemic on health and the economy. On top of this, the literature clearly has gaps in terms of having a trade-off model that captures the context of low- and middle-income countries. Devising a trade-off model for said countries is an imperative given the structural and capability differences of these countries from developed ones in terms of responding to the pandemic. Furthermore, the literature has not explicitly looked into the trade-off between economic losses and health-care system capacities, both at a national and a subnational level.
With this, the paper aims to fill these gaps with the following. Firstly, we extend FASSSTER’s subnational SEIR model to capture the associated economic losses given various lockdown scenarios at a regional level. Then, we construct an optimal policy decision trade-off between the health system and the economy in the Philippines’ case at a regional level. From there, we analyse the policy implications across the different regions given the results of the simulations.
The FASSSTER SEIR model
The FASSSTER model for COVID-19 uses a compartmental model to describe the dynamics of disease transmission in a community, and it is expressed as a system of ordinary differential equations (Estadilla et al., 2021):
where β = β0(1–λ), \(\alpha _a = \frac{c}{\tau }\), \(\alpha _s = \frac{{1 - c}}{\tau }\), and N(t) = S(t) = E(t) + Ia(t) + Is(t) + C(t) + R(t).
The six compartments used to divide the entire population, namely, susceptible (S), exposed (E), infectious but asymptomatic (Ia), infectious and symptomatic (Is), confirmed (C), and recovered (R), indicate the status of the individuals in relation to the disease. Compartment S consists of individuals who have not been infected with COVID-19 but may acquire the disease once exposed to infectious individuals. Compartment E consists of individuals who have been infected, but not yet capable of transmitting the disease to others. The infectious members of the population are split into two compartments, Ia and Is, based on the presence of disease symptoms. These individuals may eventually transition to compartment C once they have been detected, in which case they will be quarantined and receive treatment. The individuals in the C compartment are commonly referred to as active cases. Finally, recovered individuals who have tested negative or have undergone the required number of days in isolation will move out to the R compartment. Given that there had only been rare instances of reinfection (Gousseff et al., 2020), the FASSSTER model assumes that recovered individuals have developed immunity from the disease. A description of the model parameters can be found in Supplementary Table S1.
The model has several nonnegative parameters that govern the movement of individuals along the different compartments. The parameter β represents the effective transmission rate, and it is expressed as a product of the disease transmission rate β0 and reduction factor 1 − λ. The rate β0 is derived from an assumed reproduction number R0, which varies depending on the region. The parameter λ reflects the effect of mobility restrictions such as lockdowns and compliance of the members of the population to minimum health standards (such as social distancing, wearing of face masks etc.). In addition, the parameter ψ captures the relative infectiousness of asymptomatic individuals in relation to those who exhibit symptoms.
The incubation period τ and fraction of asymptomatic cases c are used to derive the transfer rates αα and αs from the exposed compartment to Ia and Is compartments, respectively. Among those who are infectious and asymptomatic, a portion of them is considered pre-symptomatic, and hence will eventually develop symptoms of the disease; this is reflected in the parameter ω. The respective detection rates δa and δs of asymptomatic and symptomatic infectious individuals indicate the movement from the undetected infectious compartment to the confirmed compartment. These parameters capture the entire health system capacity to prevent-detect-isolate-treat-reintegrate (PDITR) COVID-19 cases; hence, they will henceforth be referred to as HSC parameters. The recoveries of infectious asymptomatic individuals and among the active cases occur at the corresponding rates θ and r. Death rates due to the disease, on the other hand, are given by ∈I and ∈T for the infectious symptomatic and confirmed cases, respectively.
Aside from the aforementioned parameters, the model also utilises parameters not associated with the COVID-19 disease, such as the recruitment rate A into the susceptible population. This parameter represents the birth rate of the population and is assumed to be constant. In addition, a natural death rate per unit of time is applied to all compartments in the model, incorporating the effect of non-COVID-19 related deaths in the entire population.
Economic dynamic model
The trade-off model aims to account for the incurred economic losses following the rise and fall of the number of COVID-19 cases in the country and the implementation of various lockdown measures. The model variables are estimated per day based on the SEIR model estimate of daily cases and are defined as follows. Let YE(t) be the economic loss due to COVID-19 infections (hospitalisation, isolation, and death of infected individuals) and YE(t) be the economic loss due to the implemented lockdown at time t. The dynamics of each economic variable through time is described by an ordinary differential equation. Since each equation depends only on the values of the state variables of the epidemiological model, then it is possible to obtain a closed form solution.
Economic loss due to COVID-19 infections (hospitalisation, isolation, and health)
The economic loss due to hospitalisation, isolation, and death YE is described by the following differential equation:
where z = annual gross value added of each worker (assumed constant for all future years and for all ages), w = daily gross value added, ιi = % population with ages 0–14 (i = 1), and labour force with ages 15–34 (i = 2), 35–49 (i = 3) and 50–64 (i = 4), sr = social discount rate, κ = employed to population ratio, Ti = average remaining productive years for people in age bracket i, i = 1, 2, 3, 4, and T5 = average age of deaths from 0–14 years old age group. Note that the above formulation assumes that the young population 0–14 years old will start working at age 15, and that they will work for T1−15 years.
Solving Eq. (7), we obtain for t ≥ 0,
In this equation, the terms on the right-hand side are labelled as (A), (B), and (C). Term (A) is the present value of all future gross value added of 0–14 years old who died due to COVID-19 at time t. Similarly, term (B) is the present value of all future gross value added of people in the labour force who died due to COVID-19 at time t. Term (C) represents the total gross value added lost at time t due to sickness and isolation.
The discounting factors and the population age group shares in (A) and (B) can be simplified further into K1 and K2, where \(K_1 = \iota _1\left( {\frac{{\left( {s_r + 1} \right)^{T_1 + T_5 - 13} - \left( {s_r + 1} \right)}}{{s_r\left( {s_r + 1} \right)^{T_1 + 1}}}} \right)\) and \(K_2 = \mathop {\sum}\nolimits_{i = 2}^4 {\iota _i\left( {\frac{{\left( {s_r + 1} \right)^{T_i + 2} - \left( {s_r + 1} \right)}}{{s_r\left( {s_r + 1} \right)^{T_i + 1}}}} \right)}\). By letting L1 = z(K1 + K2)∈I + κw(1 – ∈I) and L2 = z(K1 + K2)∈T + κw(1 – ∈T), we have:
Economic losses due to lockdown policies
Equation (7) measures the losses due mainly to sickness and death from COVID-19. The values depend on the number of detected and undetected infected individuals, C and Is. The other losses sustained by the other part of the population are due to their inability to earn because of lockdown policies. This is what the next variable YL represents, whose dynamics is given by the differential equation
where φ = the displacement rate, and κ and w are as defined previously.
Solving the differential equation, then
Note that [S(t) + E(t) + Ia(t) + R(t)] is the rest of the population at time t, i.e., other than the active and infectious symptomatic cases. Multiplying this by κ and the displacement rate φ yields the number of employed people in this population who are displaced due to the lockdown policy. Thus, κwφ[S(t) + E(t) + Ia(t) + R(t)] is the total foregone income due to the lockdown policy.
Economic model parameters
The values of the parameters were derived from a variety of sources. The parameters for employment and gross value added were computed based on the data from the Philippine Statistics Authority (2021, 2020, 2019a, 2019b), the Department of Health’s Epidemiology Bureau (DOH-EB) (2020), the Department of Trade and Industry (DTI) (2020a, 2020b) and the National Economic Development Authority (NEDA) (2016) (See Supplementary Tables S2 and S3 for the summary of economic parameters).
Parameters determined from related literature
We used the number of deaths from the data of the DOH-EB (2020) to disaggregate the long-term economic costs of the COVID-related deaths into age groups. Specifically, the COVID-related deaths were divided according to the following age groups: (a) below 15 years old, (b) 15 to 34 years old, (c) 35 to 49 years old, and (d) 50 to 64 years old. The average remaining years for these groups were computed directly from the average age of death of the respective cluster. Finally, we used the social discount rate as determined by NEDA (2016) to get the present value of the stream of foregone incomes of those who died from the disease.
Parameters estimated from local data
The foregone value added due to labour displacement was estimated as the amount due to workers in a geographic area who were unable to work as a result of strict lockdown measures. It was expected to contribute to the total value added in a given year if the area they reside or work in has not been locked down.
The employed to population ratio κi for each region i was computed as
where ei was total employment in region i, and Pi was the total population in the region. Both ei and Pi were obtained from the quarterly labour force survey and the census, respectively (Philippine Statistics Authority, 2020, 2019a, 2019b).
The annual gross value added per worker zi for region i was computed as
where gji was the share of sector j in total gross value added of region i, GVAji was the gross value added of sector j in region i (Philippine Statistics Authority, 2021), and eji was the number of employed persons in sector j of region i. If individuals worked for an average of 22.5 days for each month for 12 months in a year, then the daily gross value added per worker in region i was given by
Apart from this, labour displacement rates were calculated at regional level. The rates are differentiated by economic reopening scenarios from March 2020 to September 2020, from October 2020 to February 2021, and from March 2021 onwards (Department of Trade and Industry, 2020a, 2020b, 2021). These were used to simulate the graduate reopening of the economy. From the country’s labour force survey, each representative observation j in a region i is designated with a numerical value in accordance with the percentage operating capacity of the sector where j works in. Given the probability weights pji, the displacement rate φi for region i was calculated by
where xji served as the variable representing the maximum operating capacity designated for j’s sector of work.
Policy trade-off model
The trade-off between economic losses and health measures gives the optimal policy subject to a socially determined constraint. From the literature, it was pointed out that the optimal policy option would be what minimises total economic losses subject to the number of deaths at a given time (Acemoglu et al., 2020). However, for the Philippines’ case, lockdown restrictions are decided based on the intensive care unit and health-care utilisation rate (HCUR). The health system is said to reach its critical levels if the HCUR breaches 70% of the total available bed capacity in intensive care units. Once breached, policymakers would opt to implement stricter quarantine measures.
Given these, a policy mix of various quarantine restrictions may be chosen for as long as it provides the lowest amount of economic losses subject to the constraint that the HCUR threshold is not breached. Since economic losses are adequately captured by the sum of infection-related and lockdown-related losses, YE(t) + YL(t), then policy option must satisfy the constrained minimisation below:
where the objective function is evaluated from the initial time value t0 to T.
Methods
The COVID-19 case information data including the date, location transformed into the Philippine Standard Geographic Code (PSGC), case count, and date reported were used as input to the model. Imputation using predictive mean matching uses the mice package in the R programming language. It was performed to address data gaps including the date of onset, date of specimen collection, date of admission, date of result, and date of recovery. Population data was obtained from the country’s Census of Population and Housing of 2015. The scripts to implement the FASSSTER SEIR model were developed using core packages in R including optimParallel for parameter estimation and deSolve for solving the ordinary differential equations. The output of the model is fitted to historical data by finding the best value of the parameter lambda using the L-BFGS-B method under the optim function and the MSE as measure of fitness (Byrd et al., 1995). The best value of lambda is obtained by performing parameter fitting with several bootstraps for each region, having at least 50 iterations until a correlation threshold of at least 90% is achieved. The output generated from the code execution contains values of the different compartments at each point in time. From these, the economic variables YE(t) and YL(t) were evaluated using the formulas in Eq. (7) and (8) in their simplified forms, and the parameter and displacement rate values corresponding to the implemented lockdown scenario (Fig. 1).

The different population states are represented by the compartments labelled as susceptible (S), exposed (E), infectious but asymptomatic (Ia), infectious and symptomatic (Is), confirmed (C), and recovered (R).
Results
We simulate the economic losses and health-care utilisation capacity (HCUR) for the National Capital Region (NCR), Ilocos Region, Western Visayas, Soccsksargen, and for the Davao Region by implementing various combinations of lockdown restrictions for three months to capture one quarter of economic losses for these regions. The National Capital Region accounts for about half of the Philippines’ gross domestic product, while the inclusion of other regions aim to represent the various areas of the country. The policy easing simulations use the four lockdown policies that the Philippines uses, as seen in Table 1.
Simulations for the National Capital Region
Table 2 shows the sequence of lockdown measures implemented for the NCR. Each lockdown measure is assumed to be implemented for one month. Two sets of simulations are implemented for the region. The first set assumes a health systems capacity (HSC) for the region at 17.99% (A), while the second is at 21.93% (B). A higher HSC means an improvement in testing and isolation strategies for the regions of concern.
From the sequence of lockdown measures in Table 2, Fig. 2 shows the plot of the average HCUR as well as the corresponding total economic losses for the two sets of simulations for one quarter. For the scenario at 17.99% HSC (A), the highest loss is recorded at 16.58% of the annual gross regional domestic product (GRDP) while the lowest loss is at 12.19% of its GRDP. Lower average HCUR corresponds to more stringent scenarios starting with Scenario 1. Furthermore, under the scenarios with 21.93% HSC (B), losses and average HCUR are generally lower. Scenarios 1 to 4 from this set lie below the 70% threshold of the HCUR, with the lowest economic loss simulated to be at 9.11% of the GRDP.

These include the set of trade-off decisions under a health system capacity equal to 17.99%, and another set equal to 21.93% (Source of basic data: Authors’ calculations).
Overall, the trend below shows a parabolic shape. The trend begins with an initial decrease in economic losses as restrictions loosen, but this comes at the expense of increasing HCUR. This is then followed by an increasing trend in losses as restrictions are further loosened. Notably, the subsequent marginal increases in losses in the simulation with 21.93% HSC are smaller relative to the marginal increases under the 17.99% HSC.
Simulations for the Regions Outside of NCR
Table 2 also shows the lockdown sequence for the Ilocos, Western Visayas, Soccsksargen, and Davao regions. The sequence begins with Level III only. Meanwhile, the lowest lockdown measure simulated for the regions is Level I. Two sets of simulations with differing health system capacities for each scenario are done as well.
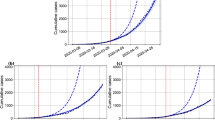
With this lockdown sequence, Fig. 3 shows the panel of scatter plot between the average HCUR and total economic losses as percentage of the respective GRDP, with both parameters covering one quarter. Similar to the case of the NCR, the average HCUR for the simulations with higher health system capacity (B) is lower than the simulations with lower health system capacity (A). However, unlike in NCR, the regions’ simulations do not exhibit a parabolic shape.

These include trade-offs for a Ilocos Region, b Western Visayas Region, c Soccsksargen Region, and d Davao Region (Source of basic data: Authors’ calculations).
Discussion and interpretation
The hypothetical simulations above clearly capture the losses associated with the pandemic and the corresponding lockdown interventions by the Philippine government. The trend of the simulations clearly shows the differences in the policy considerations for the National Capital Region (NCR) and the four other regions outside of NCR. Specifically, the parabolic trend of the former suggests an optimal strategy that can be attained through a trade-off policy even with the absence of any constraint in finding the said optimal strategy. This trend is borne from the countervailing effects between the economic losses due to COVID-19 infection (YE) and the losses from the lockdown measures (YL) implemented for the region. Specifically, Fig. 4(a), (b) show the composition of economic losses across all scenarios for the NCR simulation under a lower and higher health system capacity (HSC), respectively.

These include losses under a HSC = 17.99% and b HSC = 21.93% in the National Capital Region (Source of basic data: Authors’ calculations).
In both panels of Fig. 4, as quarantine measures loosen, economic losses from infections (YE) tend to increase while the converse holds for economic losses due to quarantine restrictions (YL). The results are intuitive as loosening restrictions may lead to increased mobility, and therefore increased exposure and infections from the virus. In fact, economic losses from infections (YE) take up about half of the economic losses for the region in Scenario 7A, Fig. 4(a).
While the same trends can be observed for the scenarios with higher HSC at 21.93%, the economic losses from infections (YE) do not overtake the losses simulated from lockdown restrictions (YL) as seen in Fig. 4(b). This may explain the slower upward trend of economic losses in Fig. 2 at HSC = 21.93%.
The output of the simulation for the Davao region shows that the economic losses from COVID-19 infections (YE) remain low even as the lockdown restrictions ease down. At the same time, economic losses from lockdown restrictions (YL) show a steady decline with less stringent lockdown measures. Overall, the region experiences a decreasing trend in total economic losses even as the least stringent lockdown measure is implemented for a longer period. This pattern is similar with the regions of Ilocos, Western Visayas, and Soccsksarkgen.
The results of the simulations from Figs. 2 and 3 also demonstrate differing levels of economic losses and health-care utilisation between the two sets of scenarios for NCR and the four other regions. Clearly, lower economic losses and health-care utilisation rates were recorded for the scenarios with higher HSC. Specifically, lower total economic losses can be attributed to a slower marginal increase in losses from infections (YE) as seen in Fig. 4(b). Thus, even while easing restrictions, economic losses may be tempered with an improvement in the health system.
With the above analysis, the policy trade-off as a constrained minimisation problem of economic losses subject to HCUR above appears to apply in NCR but not in regions outside of NCR. The latter is better off in enhancing prevention, detection, isolation, treatment, and reintegration (PDITR) strategy combined with targeted small area lockdowns, if necessary, without risking any increases in economic losses. But, in all scenarios and anywhere, the enhancement of the HSC through improved PDITR strategies remains vital to avoid having to deal with local infection surges and outbreaks. This also avoids forcing local authorities in a policy bind between health and economic measures to implement. Enhancing PDITR in congested urban centres (i.e., NCR) is difficult especially with the surge in new daily cases. People are forced to defy social distance rules and other minimum health standards in public transportation and in their workplaces that help spread the virus.
Conclusion
We extended the FASSSTER subnational SEIR model to include two differential equations that capture economic losses due to COVID-19 infection and due to the lockdown measures, respectively. The extended model aims to account for the incurred economic losses following the rise and fall of the number of active COVID-19 cases in the country and the implementation of various lockdown measures. In simulating eight different scenarios in each of the five selected regions in the country, we found a tight policy choice in the case of the National Capital Region (NCR) but not in the cases of four other regions far from NCR. This clearly demonstrates the difficult policy decision in the case of NCR in minimising economic losses given the constraint of its intensive care unit (ICU) bed capacity.
On the other hand, the regions far from the NCR have wider policy space towards economic reopening and recovery. However, in all scenarios, the primary significance of improving the health system capacity (HSC) to detect and control the spread of the disease remains in order to widen the trade-off policy space between public health and economic measures.
The policy trade-off simulation results imply different policy approaches in each region. This is also to consider the archipelagic nature of the country and the simultaneous concentration of economic output and COVID-19 cases in NCR and contiguous provinces compared to the rest of the country. Each local region in the country merits exploration of different policy combinations in economic and health measures depending on the number of active COVID-19 cases, strategic importance of economic activities and output specific in the area, the geographic spread of the local population and their places of work, and considering local health system capacities. However, we would like to caution that the actual number of cases could diverge from the results of our simulations. This is because the parameters of the model must be updated regularly driven generally by the behaviour of the population and the likely presence of variants of COVID-19. Given the constant variability of COVID-19 data, we recommend a shorter period of model projections from one to two months at the most.
In summary, this paper showed how mathematical modelling can be used to inform policymakers on the economic impact of lockdown policies and make decisions among the available policy options, taking into consideration the economic and health trade-offs of these policies. The proposed methodology provides a tool for enhanced policy decisions in other countries during the COVID-19 pandemic or similar circumstances in the future.
Data availability
The raw datasets used in this study are publicly available at the Department of Health COVID-19 Tracker Website: https://doh.gov.ph/covid19tracker. Datasets will be made available upon request after completing request form and signing non-disclosure agreement. Code and scripts will be made available upon request after completing request form and signing non-disclosure agreement.
References
Acemoglu D, Chernozhukov V, Werning I, Whinston M (2020) Optimal targeted lockdowns of a multi-group SIR model. In: National Bureau of Economic Research Working Papers. National Bureau of Economic Research (NBER). https://www.nber.org/system/files/working_papers/w27102/w27102.pdf. Accessed 16 Jun 2021
Amewu S, Asante S, Pauw K, Thurlow J (2020) The economic costs of COVID-19 in Sub-Saharan Africa: insights from a simulation exercise for Ghana. Eur J Dev Res 32(5):1353–1378. https://doi.org/10.1057/s41287-020-00332-6
Anand N, Sabarinath A, Geetha S, Somanath S (2020) Predicting the spread of COVID-19 using SIR model augmented to incorporate quarantine and testing. Trans Indian Natl Acad Eng 5:141–148. https://doi.org/10.1007/s41403-020-00151-5
Bangko Sentral ng Pilipinas (2021) 2021 Inflation Report First Quarter. https://www.bsp.gov.ph/Lists/Inflation%20Report/Attachments/22/IR1qtr_2021.pdf. Accessed 16 Jun 2021
Benson C, Clay E (2004) Understanding the economic and financial impacts of natural disasters. In: World Bank Disaster Risk Management Paper. World Bank. https://elibrary.worldbank.org/doi/abs/10.1596/0-8213-5685-2. Accessed Jan 2022
Byrd R, Lu P, Nocedal J, Zhu C (1995) A limited memory algorithm for bound constrained optimization. SIAM J Sci Comput 16:1190–1208. https://doi.org/10.1137/0916069
Cereda F, Rubião R, Sousa L (2020) COVID-19, Labor market shocks, and poverty in brazil: a microsimulation analysis. In: poverty and equity global practice. World Bank. https://openknowledge.worldbank.org/bitstream/handle/10986/34372/COVID-19-Labor-Market-Shocks-and-Poverty-in-Brazil-A-Microsimulation-Analysis.pdf?sequence=1&isAllowed=y. Accessed 21 Feb 2021
Chen D, Lee S, Sang J (2020) The role of state-wide stay-at-home policies on confirmed COVID-19 cases in the United States: a deterministic SIR model. Health Informatics Int J 9(2/3):1–20. https://doi.org/10.5121/hiij.2020.9301
Department of Health-Epidemiology Bureau (2020) COVID-19 tracker Philippines. https://doh.gov.ph/covid19tracker. Accessed 12 Feb 2021
Department of Trade and Industry (2020a) Revised category I-IV business establishments or activities pursuant to the revised omnibus guidelines on community quarantine dated 22 May 2020 Amending for the purpose of memorandum circular 20-22s. https://dtiwebfiles.s3-ap-southeast-1.amazonaws.com/COVID19Resources/COVID-19+Advisories/090620_MC2033.pdf. Accessed 09 Feb 2021
Department of Trade and Industry (2020b) Increasing the allowable operational capacity of certain business establishments of activities under categories II and III under general community quarantine. https://dtiwebfiles.s3-ap-southeast-1.amazonaws.com/COVID19Resources/COVID-19+Advisories/031020_MC2052.pdf. Accessed 09 Feb 2021
Department of Trade and Industry (2021) Prescribing the recategorization of certain business activities from category IV to category III. https://www.dti.gov.ph/sdm_downloads/memorandum-circular-no-21-08-s-2021/. Accessed 15 Mar 2021
Estadilla C, Uyheng J, de Lara-Tuprio E, Teng T, Macalalag J, Estuar M (2021) Impact of vaccine supplies and delays on optimal control of the COVID-19 pandemic: mapping interventions for the Philippines. Infect Dis Poverty 10(107). https://doi.org/10.1186/s40249-021-00886-5
FASSSTER (2020) COVID-19 Philippines LGU Monitoring Platform. https://fassster.ehealth.ph/covid19/. Accessed Dec 2020
Geard N, Giesecke J, Madden J, McBryde E, Moss R, Tran N (2020) Modelling the economic impacts of epidemics in developing countries under alternative intervention strategies. In: Madden J, Shibusawa H, Higano Y (eds) Environmental economics and computable general equilibrium analysis. Springer Nature Singapore Pte Ltd., Singapore, pp. 193–214
Genoni M, Khan A, Krishnan N, Palaniswamy N, Raza W (2020) Losing livelihoods: the labor market impacts of COVID-19 in Bangladesh. In: Poverty and equity global practice. World Bank. https://openknowledge.worldbank.org/bitstream/handle/10986/34449/Losing-Livelihoods-The-Labor-Market-Impacts-of-COVID-19-in-Bangladesh.pdf?sequence=1&isAllowed=y. Accessed 21 Feb 2021
Goldsztejn U, Schwartzman D, Nehorai A (2020) Public policy and economic dynamics of COVID-19 spread: a mathematical modeling study. PLoS ONE 15(12):e0244174. https://doi.org/10.1371/journal.pone.0244174
Gousseff M, Penot P, Gallay L, Batisse D, Benech N, Bouiller K, Collarino R, Conrad A, Slama D, Joseph C, Lemaignen A, Lescure F, Levy B, Mahevas M, Pozzetto B, Vignier N, Wyplosz B, Salmon D, Goehringer F, Botelho-Nevers E (2020) Clinical recurrences of COVID-19 symptoms after recovery: viral relapse, reinfection or inflammatory rebound? J Infect 81(5):816–846. https://doi.org/10.1016/j.jinf.2020.06.073
Hou C, Chen J, Zhou Y, Hua L, Yuan J, He S, Guo Y, Zhang S, Jia Q, Zhang J, Xu G, Jia E (2020) The effectiveness of quarantine in Wuhan city against the Corona Virus Disease 2019 (COVID-19): A well-mixed SEIR model analysis. J Med Virol 92(7):841–848. https://doi.org/10.1002/jmv.25827
Hupkau C, Isphording I, Machin S, Ruiz-Valenzuela J (2020) Labour market shocks during the Covid-19 pandemic: inequalities and child outcomes. In: Covid-19 analysis series. Center for Economic Performance. https://cep.lse.ac.uk/pubs/download/cepcovid-19-015.pdf. Accessed 21 Feb 2021
Inter-Agency Task Force for the Management of Emerging Infectious Diseases (2020) Omnibus Guidelines on the Implementation of Community Quarantine in the Philippines with Amendments as of June 3, 2020. https://www.officialgazette.gov.ph/downloads/2020/06jun/20200603-omnibus-guidelines-on-the-implementation-of-community-quarantine-in-the-philippines.pdf. Accessed 09 Feb 2021
Kashyap S, Gombar S, Yadlowsky S, Callahan A, Fries J, Pinsky B, Shah N (2020) Measure what matters: counts of hospitalized patients are a better metric for health system capacity planning for a reopening. J Am Med Inform Assoc 27(7):1026–1131. https://doi.org/10.1093/jamia/ocaa076
Keogh-Brown M, Jensen H, Edmunds J, Smith R (2020) The impact of Covid-19, associated behaviours and policies on the UK economy: a computable general equilibrium model. SSM Popul Health 12:100651. https://doi.org/10.1016/j.ssmph.2020.100651
Keogh-Brown M, Smith R, Edmunds J, Beutels P (2010) The macroeconomic impact of pandemic influenza: estimates from models of the United Kingdom, France, Belgium and The Netherlands. Eur J Health Econ 11:543–554. https://doi.org/10.1007/S10198-009-0210-1
Laborde D, Martin W, Vos R (2021) Impacts of COVID-19 on global poverty, food security, and diets: insights from global model scenario analysis. Agri Econ (United Kingdom) 52(3):375–390. https://doi.org/10.1111/agec.12624
Maital S, Barzani E (2020) The global economic impact of COVID-19: a summary of research. https://www.neaman.org.il/en/Files/Global%20Economic%20Impact%20of%20COVID19.pdf. Accessed Jan 2022
McKibbin W, Fernando R (2020) The global macroeconomic impacts of COVID-19: seven scenarios. https://www.brookings.edu/research/the-global-macroeconomic-impacts-of-covid-19-seven-scenarios/. Accessed Jan 2022
National Economic and Development Authority (2020) Impact of COVID-19 on the economy and the people, and the need to manage risk. https://www.sec.gov.ph/wp-content/uploads/2020/12/2020CG-Forum_Keynote_NEDA-Sec.-Chua_Impact-of-COVID19-on-the-Economy.pdf. Accessed Feb 2021
National Economic Development Authority-Investment Coordination Committee (2016) Revisions on ICC Guidelines and Procedures (Updated Social Discount Rate for the Philippines). http://www.neda.gov.ph/wp-content/uploads/2017/01/Revisions-on-ICC-Guidelines-and-Procedures-Updated-Social-Discount-Rate-for-the-Philippines.pdf. Accessed 12 Feb 2021
Noy I, Doan N, Ferrarini B, Park D (2020) The economic risk of COVID-19 in developing countries: where is it highest? In: Djankov S, Panizza U (eds) COVID-19 in developing economies. Center for Economic Policy Research Press, London, pp. 38–52
Peng T, Liu X, Ni H, Cui Z, Du L (2020) City lockdown and nationwide intensive community screening are effective in controlling the COVID-19 epidemic: analysis based on a modified SIR model. PLoS ONE 15(8):e0238411. https://doi.org/10.1371/journal.pone.0238411
Pham T, Dwyer L, Su J, Ngo T (2021) COVID-19 impacts of inbound tourism on australian economy. Ann. Tourism Res. 88:103179. https://doi.org/10.1016/j.annals.2021.103179
Philippine Statistics Authority (2019a) 2018 Labor Force Survey (Microdata). https://psa.gov.ph/content/2018-annual-estimates-tables. Accessed 12 Feb 2021
Philippine Statistics Authority (2019b) Updated population projections based on the results of 2015 POPCEN. https://psa.gov.ph/content/updated-population-projections-based-results-2015-popcen. Accessed 12 Feb 2021
Philippine Statistics Authority (2020) Census of population and housing. https://psa.gov.ph/population-and-housing. Accessed May 2020
Philippine Statistics Authority (2021) National Accounts Data Series. https://psa.gov.ph/national-accounts/base-2018/data-series. Accessed 05 Apr 2021
Reno C, Lenzi J, Navarra A, Barelli E, Gori D, Lanza A, Valentini R, Tang B, Fantini MP (2020) Forecasting COVID-19-associated hospitalizations under different levels of social distancing in Lombardy and Emilia-Romagna, Northern Italy: results from an extended SEIR compartmental model. J Clin Med 9(5):1492. https://doi.org/10.3390/jcm9051492
United Nations Development Programme (2021) The Socioeconomic Impact Assessment of COVID-19 in the Bangsamoro Autonomous Region in Muslim Mindanao. UNDP in the Philippines. https://www.ph.undp.org/content/philippines/en/home/library/the-socioeconomic-impact-assessment-of-covid-19-on-the-bangsamor.html. Accessed Nov 2021.
Verikios G, McCaw J, McVernon J, Harris A (2012) H1N1 influenza and the Australian macroeconomy. J Asia Pac Econ 17(1):22–51. https://doi.org/10.1080/13547860.2012.639999
World Bank (2020) Projected Poverty Impacts of COVID-19 (Coronavirus). https://www.worldbank.org/en/topic/poverty/brief/projected-poverty-impacts-of-COVID-19. Accessed Jan 2022
World Bank (2021) Global economic perspectives. World Bank, Washington DC
World Bank (2022) GDP growth (annual %). https://data.worldbank.org/indicator/NY.GDP.MKTP.KD.ZG. Accessed Jan 2022
Acknowledgements
We thank Dr. Geoffrey M. Ducanes, Associate Professor, Ateneo de Manila University Department of Economics, for giving us valuable comments in the course of developing the economic model, and Mr. Jerome Patrick D. Cruz, current Ph.D. student, Massachusetts Institute of Technology, for initiating and leading the economic team in FASSSTER in the beginning of the project for their pitches in improving the model. We also thank Mr. John Carlo Pangyarihan for typesetting the manuscript. The project is supported by the Philippine Council for Health Research and Development, United Nations Development Programme and the Epidemiology Bureau of the Department of Health.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Model conceptualization, data collection and analysis were performed by EPdL-T, MRJEE, JTS, CKL, CJTC, TRYT, LPT, JMRM, and GMV. All authors commented on previous versions of the manuscript, and read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
Proponents of the project are corresponding authors in the study. Research and corresponding publications are integral to the development of the models and systems. The authors declare no conflict nor competing interest.
Ethical approval
Not applicable
Informed consent
Not applicable
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
de Lara-Tuprio, E.P., Estuar, M.R.J.E., Sescon, J.T. et al. Economic losses from COVID-19 cases in the Philippines: a dynamic model of health and economic policy trade-offs. Humanit Soc Sci Commun 9, 111 (2022). https://doi.org/10.1057/s41599-022-01125-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1057/s41599-022-01125-4
- Springer Nature Limited