
Abstract
To systematically evaluate the intervention effect of music therapy on anxiety and depression in breast cancer patients. Randomised controlled trial (RCT) on music therapy for anxiety and depression in breast cancer patients was searched from 7 major databases, PubMed, Embase, the Cochrane Library, WOS, CNIC, Wanfang, and Wipro, spanning the period of library construction to 23 October 2023, and the literature screening of music therapy for anxiety or depression in breast cancer patients was carried out by 2 experimentalists, each of whom conducted a literature screening RCT independently of the other anxiety or depression in a RCT. Methodological quality was evaluated using the PEDro scale; GRADE profiler software for quality of evidence; and RevMan 5.4 was used for effect size merging and forest plots; publication bias tests and sensitivity analyses were performed using Stata 17.0; and standardized mean difference (SMD) and 95% CI were used as the effect statistics. A total of 13 RCTs with 1326 subjects (aged 18–70 years) were included in the literature, with a mean PEDro score of 6.8, and the literature was overall of good methodological quality. Meta-analysis showed that music therapy improved anxiety in breast cancer patients (841 cases), with a combined effect size (SMD = − 0.82, 95% CI [− 1.03, − 0.61] and P < 0.001); and improved depression in breast cancer patients (387 cases) with a combined effect size (SMD = − 0.76, 95% CI [− 1.15, − 0.38], P < 0.001). Subgroup analyses showed that music intervention with off-site music (757 cases) and music choice of non-self-selected music (537 cases) had the best effect on anxiety improvement, with corresponding combined effect sizes (SMD = − 0.88, P < 0.001; SMD = − 0.83, P < 0.001), respectively; followed by an intervention length of < 30 min (589 cases), a frequency of 2 times/day (382 cases), and intervention period of 2–3 weeks (101 cases) had the best effect on anxiety improvement, and the corresponding combined effect sizes were (SMD = − 0.80, P < 0.001; SMD = − 0.91, P < 0.001; SMD = − 1.02, P < 0.001), respectively; and the music selection was the choice of one's own favourite music among the expert recommendations (219 cases) (270 cases) had the best effect on the improvement of depressed mood, with combined effect sizes of (SMD = − 1.15, P < 0.001; SMD = − 0.71, P < 0.001) and music with an intervention duration of 30 min (287 cases), an intervention frequency of 1 time/day (348 cases), and an intervention period of 2–4 weeks (120 cases), respectively, with corresponding combined effect sizes of (SMD = − 0.75, P < 0.001; SMD = − 0.86, P < 0.001; SMD = − 1.06, P < 0.001), respectively. Music therapy can improve anxiety and depression in breast cancer patients, and the level of evidence is moderate. Although the heterogeneity between studies is high, which may lead to bias in the results, we explored the source of heterogeneity through subgroup and sensitivity analyses, providing a good evidence-based basis for clinical practice. The heterogeneity of anxiety and depression was explored by subgroup analysis, with anxiety due to music duration and music cycle; and depression due to intervention cycles and music duration. Sensitivity analyses also identified music duration and music cycle as contributing to the heterogeneity. Also, this study has some limitations since the included literature did not take into account the duration of the disease, education, and family economic status and did not categorize the age stages. This study found that music therapy improves anxiety and depression in breast cancer patients and the results can be used as a basis for clinical practice and researcher enquiry. This research has been registered on the INPLASY platform (https://inplasy.com/contact/) under the number: INPLASY2023100057.
Similar content being viewed by others


Introduction
The incidence of female breast cancer often ranks first among female malignant tumours1, accounting for 7–10% of all malignant tumors in the body. In the past 20 years, the incidence of breast cancer in China has increased by 37.6%, with an average annual growth rate of 2.3%2. Breast cancer patients are the phenomenon of uncontrolled proliferation of breast epithelial cells under the action of multiple carcinogenic factors; physiologically, the early stage often manifests symptoms such as breast lumps and enlarged axillary lymph nodes, and in the late stage, due to distant metastasis of the cancer cells, multi-organ lesions may occur, and even threaten the patients' lives3. Patients need to endure the pain and side effects of chemotherapy during treatment, and psychologically they often show emotional instability, anxiety depression, etc., and most of them have psychological problems such as moderate and severe anxiety levels.
Music therapy is an emerging psychotherapeutic modality in which the unique physiological and psychological effects of music enable patients to regulate their psychological disorders through musical experience and distraction. Music therapy is considered to be one of the most effective psychotherapeutic methods for clinical non-pharmacological treatment to eliminate psychosomatic disorders4. Music can affect patients' heart rate, blood pressure, respiratory rate, and blood cortisol levels through rhythm and tone5, thus relieving emotions such as anxiety or depression6. A study by Zhi Yanhong et al. found that patients use the sonic vibrations of music to produce beneficial resonance with certain physiological structures of the human body and achieve the elimination of psychological barriers7; a study by LAGATTOLLA F et al. 8 showed that music can promote relaxation in patients with breast cancer, lower anger, heart rate, respiratory rate, reduce pain, reduce the need for anesthesia, analgesia9 and other recourse, and shorten the recovery time, thus reducing anxiety and depression10.
Previous research has shown that music therapy can effectively improve anxiety and depression symptoms in breast cancer patients11,12, but the specific intervention protocol is unclear, especially the choice of music, intervention duration, intervention period, and intervention frequency need to be further clarified. The results of some of the previous research are controversial, such as studies found that the duration of music intervention is most effective when it is less than 30 min, and some research has also shown that the longer the duration, the better the effect. Based on this, this research intends to further explore the effects of music selection, intervention mode, intervention duration, intervention period, and intervention frequency on anxiety and depression in breast cancer patients based on previous studies, to provide precise music intervention programs for clinics and references for researchers.
Methods
Literature search strategy
This study was reported in accordance with PRISMA (Preferred Reporting Items for Systematic Evaluation and Meta-Analysis) guidelines to ensure transparency of the research13. The research protocol was registered on INPLASY No.INPLASY2023100057.
Data sorting and statistical analysis were conducted for the included literature in accordance with the requirements of the International Guidelines for Writing Systematic Reviews14. The two researchers independently computer-searched six databases from China Knowledge, Wanfang, PubMed, Embase, the Cochrane Library, and Web of Science for RCTs of music therapy for breast cancer patients. The search date of each database was 23 October 2023. The search was conducted by combining subject terms with free words, using the Boolean symbols "AND" and "OR" for combinatorial concatenation, and was determined after repeated pre-testing. In case of disagreement between two researchers, the decision was discussed with the third researcher. This was supplemented by tracking down the relevant systematic reviews and references of the included literature. Table 1.
Inclusion criteria
This research is based on the ICD and ACJJ classification system to construct a PICO framework for systematically evaluating and analysing the intervention effect of music therapy on anxiety and depression in breast cancer patients, and the research shows that the intervention effect of music therapy on anxiety and depression in breast cancer patients is significant. Table 2.
Exclusion Criteria
(1) Literature with repeated publications or PEDro score < 4. (2) No detailed data is provided, and specific data cannot be obtained. (3) The experimental group received a combination intervention, such as music therapy combined with aerobic exercise.
Data extraction
After retrieving the relevant literature, the literature was imported into Endnote for weight removal. Literature screening and data extraction were performed by 2 researchers using an independent double-blind approach respectively. The extracted data from eligible studies were entered into RevMan 5.4 and double-checked for accuracy, and in case of disagreement, the 3rd researcher joined the discussion to decide whether to include them or not. The extraction included basic information about the literature (first author, year of publication), basic information about the experimental subjects (sample size, age, gender), music therapy (classical Chinese folk music, world-famous music, soft, beautiful tracks, etc.), testing methods, specific outcome indicators: anxiety and depression, and extraction of baseline and posttest data.
Quality evaluation
The quality of the literature was evaluated using a modified version of the PEDro scale15 to assess the methodological quality of the included literature. The scale included 10 criteria: ITT intention-to-treat analysis, random allocation, allocation concealment, baseline similarity, blinding of the research subjects, blinding of the outcome assessment, dropout rate ≤ 15%, intention-to-treat analysis, blinding of the therapists, as well as the point measure and the discrepancy measure. A total of 10 points was assigned to the scale, with a score of less than 4 considered poor quality, 4 to 5 considered moderate quality, 6 to 8 considered good quality, and 9 to 10 considered high quality, and only literature with a score of 5 or higher was included.
Quality of evidence evaluation16 was done through GRADE profiler software, and the quality of evidence for outcome indicators was evaluated on five downgraded factors including publication bias, inconsistency, imprecision, indirectness, and limitations of the research. Among them, a downgrade of 3 was considered as very low-level evidence, a downgrade of 2 was considered as low-level evidence, a downgrade of 1 was considered intermediate-level evidence, and no downgrade was considered as high-level evidence, and the final grade of evidence was categorized into 4 grades: high level, intermediate level, low level, and very low level. Quality ratings were conducted independently by two researchers, with a third researcher contributing to the discussion if there was disagreement.
Statistical methods
Review Manager 5.4 was used to statistically analyze the data. The outcome indicators of the literature included in this paper are all continuous variables, and the measurement tools are inconsistent across research, so the effect indicators were calculated using the effect size (Standard Mean Difference (SMD)); when the effect size is < 0.2, it is a small effect, 0.20–0.49 is a medium-small effect, 0.50–0.79 is a medium effect, and ≥ 0.8 is a large effect17. Heterogeneity was quantified objectively by I2, and heterogeneity was quantified by the I2 statistic. 75%, 50%, and 25% were the boundary values of high, medium, and low heterogeneity, respectively18.If there was no statistical heterogeneity among the results, the fixed effect model was used. If heterogeneity exists, the random effects model is used to combine the effect sizes. And the Stata 17.0 Egger test is used to publication bias. If there is publication bias, the scission-supplement method is used to correct it.
Results
Literature search results
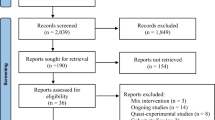
As shown in Fig. 1, a total of 1738 pieces of literature were retrieved through PubMed, Embase, Web of Science, Cochrane, CNKI, Wanfang, and VIP databases, and 48 pieces of literature were selected after preliminary screening by eliminating duplicates, reading titles, and abstracting. According to the inclusion and exclusion criteria, the full text was re-screened, and finally 13 articles were included in the meta-analysis.

Document retrieval flow chart.
Basic features of the included literature
The 13 articles19,20,21,22,23,24,25,26,27,28,29,30,31 included were published between 2006 and 2022, with a total of 1326 cancer patients. The intervention content of the experimental group was music therapy combined with conventional intervention, and the control group was conventional chemotherapy intervention (Table 3).
Article quality evaluation
All studies described ITT intention-to-treat analyses, statistical analyses were performed between groups, point measures and difference-in-difference scales, random allocation with similar baselines, dropout rates ≤ 15%, five studies described allocation concealment, three studies blinded study participants, three studies blinded outcome assessments, and no studies blinded therapists. Of the 13 studies included, the PEDro scale scores ranged from 6 to 8, with a mean of 6.8, giving good overall research quality (Table 4) (Fig. 2).

Forest map of anxiety in breast cancer patients with music therapy.
Results of meta-analysis
Meta-analysis of music therapy on anxiety in breast cancer patients
As shown in Fig. 2, among the included literature, 12 studies (1278 patients) evaluated the effect of music therapy on anxiety in breast cancer patients. Heterogeneity test I2 = 75%, P < 0.01. There was a high degree of statistical heterogeneity among the studies, so the random effects model was used to combine the effect sizes. The results of the meta-analysis showed that the effect size was -0.82, 95%CI[-1.03,-0.61], and the difference between the experimental group and the control group was statistically significant. 0.001, indicating that music therapy was effective in reducing anxiety in breast cancer patients compared to the control group.
As shown in Figs. 3, 4, 5, 6, 7, 8 and 9.In order to explore the source of heterogeneity, subgroup analysis was performed for the main outcome indicator, anxiety.The effect of music therapy on the anxiety of breast cancer patients may be influenced by factors such as average age, intervention duration, intervention cycle, intervention frequency, music selection, professional degree, and music style. The results of subgroup analysis showed that intervention cycle, intervention duration, intervention frequency, music selection, professionalism, period, average age and subgroup analysis of music style were statistically significant (P < 0.001). From the perspective of heterogeneity sources, intervention duration, average age, intervention period and intervention cycle may be the sources of heterogeneity (Table 5).

Subgroup analysis of the influence of different music duration on anxiety of breast cancer patients.

Subgroup analysis of influence of average age of patients on anxiety of breast cancer patients.

Subgroup analysis of the influence of different music intervention cycles on anxiety of breast cancer patients.

Subgroup analysis of the influence of music intervention frequency on anxiety of breast cancer patients.

Subgroup analysis of the influence of different music choices on anxiety of breast cancer patients.

Is it a subgroup analysis of the influence of music recommended by experts on anxiety of breast cancer patients.

Subgroup analysis of the influence of different music intervention methods on anxiety of breast cancer patients.
Meta-analysis of depression in breast cancer patients with music therapy
As shown in Fig. 10, six studies in the included literature evaluated the effect of music therapy on depression in breast cancer patients, including 411 patients. Heterogeneity test I2 = 84%, P < 0.01. There was a high degree of statistical heterogeneity among the studies, so the random effects model was used to combine the effect sizes. The results of meta-analysis showed that the effect size was -0.76, 95%CI[-1.15,-0.38], and the difference was statistically significant. 0.00001, indicating that music therapy was effective in alleviating depression in breast cancer patients compared to controls.

Music therapy for overall depression in breast cancer patients.
As shown in Figs. 11, 12, 13, 14 and 15.To explore the source of heterogeneity, subgroup analysis was performed for depression, the main outcome indicator. The effect of music therapy on anxiety and depression in breast cancer patients may be limited by the intervention cycle, music duration, professional degree, music choice and frequency. The results of subgroup analysis in the table showed that intervention cycle, intervention duration, age specialization, music selection and subgroup analysis of group music style were statistically significant. From the source of heterogeneity, intervention cycle and duration may be the main source of heterogeneity(Table 6).

Subgroup analysis of the impact of different music intervention cycles on depression in breast cancer patients.

Subgroup analysis of the influence of different music intervention duration on depression in breast cancer patients.

Subgroup analysis of whether experts recommend music for depression in breast cancer patients.

Subgroup analysis of the influence of music selection on depression in breast cancer patients.

Subgroup analysis of the influence of music intervention frequency on depression in breast cancer patients.
Risk bias analysis
As shown in Fig. 16, it can be found that the funnel diagram of music therapy on the anxiety of breast cancer patients is basically symmetric. The Egger test result shows that Z = − 0.22, P >|z|= 0.8224, indicating that there is no publication bias in the study.

Music therapy for breast cancer patients funnel diagram.
Sensitivity analyses
As shown in Fig. 17, to investigate whether the heterogeneity between studies was caused by individual studies, the overall effects were analyzed by screening individual studies one by one. The normal value of the amplitude of the effect of music therapy on anxiety in breast cancer patients included in all studies was in the range (-0.91 to -0.71). The analysis results showed that the data sensitivity of this study was relatively low and did not fundamentally change the results of the meta-analysis, indicating that the research results have a certain stability and reliability.

Sensitivity analysis of music therapy on anxiety in breast cancer patients.
Evaluation of evidence quality level
As shown in Fig. 18, the GRADEpro evidence rating system was used to assess the quality of evidence for the outcome indicators. It was found that the quality of evidence for music therapy for improving anxiety and depression in breast cancer patients was high, and the actual effect was close to the research findings. However, the heterogeneity of the articles is high, so we downgraded the quality of evidence to moderate.

Quality of evidence for the effect of music therapy on improving anxiety and depression in breast cancer patients.
Adverse events
No adverse events resulting from music therapy were reported in any of the 13 included papers.
Discussion
Influence of music therapy on the anxiety of breast cancer patients
The results of this study show that music therapy can significantly improve anxiety in breast cancer patients, and the results are consistent with previous studies. Previous meta-analyses found that music therapy eliminated psychological barriers through unique effects. Longitudinal studies21,32 have found that music can reduce pain33and shift attention away from negative stimuli to things that are familiar, soothing, and pleasant10,11. It has also been confirmed that music therapy can reduce the anxiety and depression of patients with other diseases34,35,36,37,38,39.
A Total of 13 papers were included in this study to systematically evaluate the intervention effect of music therapy on anxiety and depression in breast cancer patients using the PEDro scale to evaluate the risk of bias of the included papers in 9 aspects, with a mean score of 6.8, which was found to be of good quality, but this study did not carefully classify the condition and type of the breast cancer patients in the included papers, and with an I2 > 50%, there was a high degree of heterogeneity among the studies and the existence of a considered some inconsistency. In the research, a dose–effect relationship was found for the effects of music therapy on anxiety and depression in breast cancer patients, which raised the level of evidence to one. Limitations of the research:1) The types of music selected for the interventions included in the literature were different, with no fixed criteria, whether it was recommended by the experts in English or selected by their favorite music, and the repertoire selected was more often than not classified specifically, which inspired the expectation of more high-quality RCT articles to be further developed. The study was conducted to identify the effects of music therapy on anxiety and depression in patients with breast cancer. RCT articles on music categorization to further complement and demonstrate. In conclusion, music therapy is given high-level quality of evidence for both anxiety and depression intervention effects in breast cancer patients.
This study found that breast cancer patients had the best improvement effect on anxiety when the music was their favorite music recommended by experts, the intervention method was non-live music, the intervention duration was less than or equal to 30 min, the intervention frequency was 2 times per day, and the intervention cycle was 2–3 weeks. Anxiety in breast cancer patients is mostly induced by low estrogen levels, and the decrease in estrogen levels is accompanied by a decline in serotonin transmitters. The possible mechanism by which music can improve anxiety in patients may be as follows: Music can increase the levels of estrogen40 and oxytocin41, and also reduce the concentration of serum cortisol in women, so that the value of serum cortisol in breast cancer patients can return to normal42. In terms of the nervous system, music can increase the dopamine activity of nucleus accumbens (NAc) and ventral tegmental cortex (VTA), alter the structural changes of the mesolimbic brain (e.g., nucleus accumbens [NAc], ventral tegmental area [VTA]), and effectively control the influence of emotional stimuli on the autonomic and physiological responses of the hypothalamus and insula43. Inhibition of sympathetic nervous system reactivity reduces negative emotional experiences42, thereby reducing anxiety. Choosing their favorite music has a better effect on breast cancer patients44 to perform non-live music, which may be because patients can get into the state more quickly when choosing their favorite music and local music45, so that patients can resonate the cranial cavity, chest cavity, or a certain tissue cavity through rhythm, frequency, and regular sound wave vibration46. It directly affects people's brain waves, heart rate, and breathing rhythm, thereby reducing anxiety. It may also be because, when listening to recorded music, patients can enter the music environment faster by restricting light, sound, visitors, and phone calls, thus regulating their emotional state47. A music intervention with a duration of no more than 30 min, a frequency of 2 times per day, and a cycle of 2–3 weeks is more effective for breast cancer patients. PALMER23also found that music therapy can reduce anxiety within only 5 min and can significantly reduce anxiety during 15–30 min of hypnotic intervention. Regarding the frequency of intervention, 2/day are statistically significant, and the reason remains unclearly, more high-quality RCTs need to complement and prove this in the future. The effect of music intervention on patients' anxiety may present an inverted "U" curve, and the intervention effect is the best at the hour, followed by more than 3 weeks, and the effect is not good within 2 weeks6.
This study also found that the duration of the intervention was inconsistent with that of Fu Yanzhi et al.23,24,27. The duration of music intervention did not become more effective over time, and the range of change from pre-treatment to post-treatment did not decrease over time. The reason might be that the patients studied by Fu Yanzhi and others were patients with advanced breast cancer, and this might also be related to the timeliness of behavioral habits. At the same time, it also brings inspiration to future generations to further explore the impact of music duration on anxiety in breast cancer patients and look forward to more high-quality RCT articles to further supplement and prove. We also found that different types of music (such as classical music, soothing music, and cheerful music) have different effects on anxiety in breast cancer patients, but the number of previous literature is too small to classify, which also needs more high-quality RCTs to verify.
Influence of music therapy on depression in breast cancer patients
This study found that music selected as expertly recommended music, an intervention duration of 30 min, an intervention frequency of 1 time per day, and an intervention cycle of 2–4 weeks had the best effect on improving depression in breast cancer patients. This is consistent with previous results11,12. Longitudinal studies48 have found that music can stimulate the cerebral cortex in many ways, evoking pleasant thought associations and emotions in patients.
Patients with breast cancer are more prone to depression symptoms, subsyndromic depression due to circadian rhythm disturbance and fatigue, and higher intrinsic melatonin secretion than normal people. Musical stimulation can activate or increase specific pathways in several brain regions related to emotional behaviour, such as the insular and cingulate cortex49,50, hypothalamus, hippocampus, amygdala and prefrontal cortex51. Thus, some biochemical mediators, such as increased endorphins52,53, endocannabinoids54 and dopamine55,56,57 and decreased nitric oxide58 regulate positive emotional states58. In this study, it was found that, in terms of music selection, the effect of music suggested by experts is better. It may be that experts choose according to the current physiological and psychological state of each patient and the different personality of the patient so as to solve the emotional problems of the patient in a targeted way59,60. In terms of intervention cycle, 2–4 weeks is the best effect size for the music intervention cycle61, The effect size is moderate when the intervention cycle is less than or equal to 2 weeks, and the effect size is second when the intervention cycle is more than 4 weeks. Qishou Tang also said in the study62 that the effect of short-term and medium-term interventions is higher than that of long-term interventions20,24,30. However, the reason remains uncleraly, and more high quality RCT to further complement and prove this. The intervention duration ≤ 30 min has a better effect on alleviating depression in breast cancer patients, because with the extension of listening time, the response to two types of auditory stimuli in the human body is different63, and the effect of music intervention may be weakened by the timeliness of behavioural habits or distraction of human attention after the intervention duration is higher than 30 min.Intervention duration of 30 min and frequency of 1 time per day had a better effect on depression relief in breast cancer patients60,61, which may be related to the timeliness of behavioural habits. It may also be that the frequency of intervention once a day can regulate the stress response of the hypothalamic–pituitary–adrenal axis64, which has the effect of regulating the spirit, pleasing the heart, and relieving depression in patients. Similarly, we have observed through research that the course of the disease, family economic conditions and educational background of breast cancer patients may affect their depression, and the type, tone and rhythm of music may also have different effects on the improvement of depression in breast cancer patients. This will inspire some researchers today who can further explore the effects of demographic characteristics and musical elements on depression in breast cancer patients, and look forward to more high-quality RCT articles to further complement and prove.
In summary, based on the literature of high quality controlled trials, each intervention element has different effects on anxiety and depression in breast cancer patients, providing clinical practice and researchers with more precise music intervention programmes. Meanwhile an increasing number of healthcare organisations and government departments are incorporating music therapy into guidelines and policies for breast cancer treatment, and music therapy professionals are being trained and accredited to provide appropriate music interventions for patients. These policy measures help to increase the recognition and acceptance of music therapy interventions by patients and promote the psychological recovery of breast cancer patients. As scientific research continues, we can further understand the specific mechanisms of action and effects of music therapy on patients, and how to better apply music therapy for personalised interventions.
This research has been registered on the INPLASY platform (https://inplasy.com/contact/) under the number INPLASY2023100057.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
He, L. et al. Status quo of self advocacy ability of chemotherapy patients with breast cancer and analysis of influencing factors. Chin. J. Nurs. 58(07), 788–793 (2023).
Our editorial department The 5th National breast cancer Young and Middle aged Expert Forum and the 3rd Tianjin breast cancer Multidisciplinary Comprehensive Diagnosis and Treatment International Forum were successfully held Clinical oncology in China, 2017, 44(21): 1107.
Yu, L. et al. Decision aids for breast cancer screening in women approximately 50 years of age: A systematic review and meta-analysis of randomised controlled trials. J. Clin. Nurs. https://doi.org/10.1111/jocn.16112 (2021).
[Expert consensus on the diagnosis and treatment of young breast cancer in China (2022 Edition)] . Zhonghua Yi Xue Za Zhi, 2023, 103(6): 387–403.
Meerwijk, E. L. Psychological pain in depressive disorder: A concept analysis. J. Clin. Nurs. 32(23–24), 8154 (2023).
Na, L. et al. Research progress on the application of music therapy in the quality of life of breast cancer patients. Gener. Nurs. 19(24), 3371–3374 (2021).
Nilsson, U. The anxiety- and pain-reducing effects of music interventions: A systematic review. Aorn J. 87(4), 780–807 (2008).
Guétin, S. et al. Effect of music therapy on anxiety and depression in patients with Alzheimer’s type dementia: randomised, controlled study. Dement Geriatr. Cogn. Disord. 28(1), 36–46 (2009).
Yanhong, Z. et al. Exploring the impact of music therapy on the quality of life of advanced cancer patients in community hospice wards. Mod. Diagn. Treat. 33(01), 124–126 (2022).
Lagattolla, F. et al. Receptive music therapy versus group music therapy with breast cancer patients hospitalized for surgery. Support Care Cancer 31(3), 162 (2023).
Sánchez-Jáuregui, T. et al. Clinical hypnosis and music in breast biopsy: A randomized clinical trial. Am. J. Clin. Hypn. 61(3), 244–257 (2019).
Lanfear, C. & Harding, S. The effectiveness of nurse-led care in supporting self-management in patients with cancer: A systematic review. J. Clin. Nurs. 32(23–24), 7996–8006 (2023).
Page, M. J. et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Bmj 372, n71 (2021).
Liberati, A. et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med 6(7), e1000100 (2009).
Ludyga, S. et al. Systematic review and meta-analysis investigating moderators of long-term effects of exercise on cognition in healthy individuals. Nat. Hum. Behav. 4(6), 603–612 (2020).
Howick, G. G. J. Understanding GRADE: An introduction. J. Evid. Based Med. 2013.
Cohen, J. A power primer. Psychol. Bull. https://doi.org/10.1037/0033-2909.112.1.155 (1992).
Higgins, J. P. et al. Measuring inconsistency in meta-analyses. Bmj 327(7414), 557–560 (2003).
Li, X. M. et al. Effects of music therapy on anxiety of patients with breast cancer after radical mastectomy: A randomized clinical trial. J. Adv. Nurs. 68(5), 1145–1155. https://doi.org/10.1111/j.1365-2648.2011.05824.x (2012).
Chirico, A. et al. Virtual reality and music therapy as distraction interventions to alleviate anxiety and improve mood states in breast cancer patients during chemotherapy. J. Cell Physiol. 235(6), 5353–5362 (2020).
Lima, T. U. et al. Impact of a music intervention on quality of life in breast cancer patients undergoing chemotherapy: A randomized clinical trial. Integr. Cancer Ther. 19, 1534735420938430 (2020).
Hanser, S. B. et al. Effects of a music therapy intervention on quality of life and distress in women with metastatic breast cancer. J. Soc. Integr. Oncol. 4(3), 116–124 (2006).
Palmer, J. B. et al. Effects of music therapy on anesthesia requirements and anxiety in women undergoing ambulatory breast surgery for cancer diagnosis and treatment: A randomized controlled trial. J. Clin. Oncol. 33(28), 3162–3168 (2015).
Zhou, K. N. et al. Effects of music therapy on depression and duration of hospital stay of breast cancer patients after radical mastectomy. Chin. Med. J. 124(15), 2321–2327 (2011).
Shu-Xian, H. U. & Bo, S. Effect of different types of music to alleviate the chemotherapy anxiety and depression of the patients with breast cancer. Matern. Child Health Care China 28(02), 359–361 (2013).
Zhen-Qi, L. U. The effect of music relaxation therapy on the adverse reactions induced by chemotherapy in patients with breast cancer. Chin. J. Nurs. 45(05), 405–408 (2010).
Yanzhi, F. et al. Investigation on the application of music therapy to improve anxiety and depression in FEC chemotherapy for advanced breast cancer. Chin. J. Misdiagn. 9(33), 8312–8313 (2009).
Chang, Y. The influence of music therapy on the postoperative mood of patients with breast cancer. Mod. Pract. Med. 34(02), 249–250 (2022).
Yuting, L. et al. The effect of music therapy on perioperative breast cancer patients. Chin. Commun. Phys. 12(02), 46–47 (2010).
Lin, M. F. et al. A randomised controlled trial of the effect of music therapy and verbal relaxation on chemotherapy-induced anxiety. J. Clin. Nurs. 20(7–8), 988–999 (2011).
Hongmei, L. V. et al. Effect of personalized music intervention on the preoperative anxiety in patients undergoing breast cancer surgery. J. Nurs. Sci. 10, 4–6 (2008).
Xiao, Y. et al. Effects of aroma therapy and music intervention on pain and anxious for breast cancer patients in the perioperative period. Zhong Nan Da Xue Xue Bao Yi Xue Ban 43(6), 656–661 (2018).
Aalbers, S. et al. Music therapy for depression. Cochr. Database Syst. Rev. 11(11), cd004517 (2017).
Sun, C. et al. Effects of music therapy on anxiety in patients with cancer: Study protocol of a randomised controlled trial. BMJ Open 13(5), e067360 (2023).
Mazet-Carpentier, A. et al. Chronic obstructive pulmonary disease and music therapy. Rev. Infirm. 72(290), 43–45 (2023).
Cao, M. & Zhang, Z. Adjuvant music therapy for patients with hypertension: A meta-analysis and systematic review. BMC Complem. Med. Ther. 23(1), 110 (2023).
Yuxing, P. et al. Clinical efficacy analysis of receptive music therapy for anxiety disorder. Pract. Med. China 17(12), 64–67 (2022).
Xiaoli, Z. et al. Study on the effect of psychological nursing combined with music therapy on anxiety and depression in elderly female stroke patients Chinese. Med. Sci. 12(06), 85–88 (2022).
Yanhong, Z. et al. Meta analysis of the physiological and psychological effects of music therapy on patients with chronic obstructive pulmonary disease. General Nursing 20(26), 3620–3624 (2022).
Fukui, H. & Toyoshima, K. Music facilitate the neurogenesis, regeneration and repair of neurons. Med. Hypotheses 71(5), 765–769 (2008).
Grape, C. et al. Does singing promote well-being? An empirical study of professional and amateur singers during a singing lesson. Integr. Physiol. Behav. Sci. 38(1), 65–74 (2003).
Yongpeng, H. et al. Detection of 20 amino acids in serum of breast cancer patients and its significance in screening breast cancer. J. Second Mil. Med. Univ. 42(11), 1238–1245 (2021).
Gorresen, P. M. et al. Multi-state occupancy models of foraging habitat use by the Hawaiian hoary bat (Lasiurus cinereus semotus). PLoS One 13(10), e0205150 (2018).
Tavakoli, F. et al. Role of music in morphine rewarding effects in mice using conditioned place preference method. Neuro Endocrinol. Lett. 33(7), 709–712 (2012).
Hao, P. et al. Systematic evaluation of the necessity of interpleural lymph node management during axillary lymph node dissection in breast cancer patients. J. Second Mil. Med. Univ. 42(04), 439–444 (2021).
Peng, S. & Jie, J. Persistent pain after breast cancer surgery and rehabilitation(review). Chin. J. Rehabil. Theory Pract. 24(2), 128–133 (2018).
Jingyue, P. et al. Research progress of music therapy in breast cancer rehabilitation. Massage Rehabil. Med. 12(21), 78–82 (2021).
Hong, G. Effects of yoga music on anxiety and pain of PICC catheterization in patients after breast cancer surgery. Contemp. Nurses 02, 71–72 (2015).
Kai-Na, Z. & Xiao-Mei, L. I. Effect of music therapy on pain of breast cancer patients after radical mastectomy. Chin. J. Nurs. 26(28), 55–57 (2010).
Liu, C. H. et al. Enhanced functional connectivity between insular subregions correlates with the efficacy of music and instruction-guided relaxation in depression. Neuroreport 31(17), 1215–1224 (2020).
Usui, C. et al. Music intervention reduces persistent fibromyalgia pain and alters functional connectivity between the insula and default mode network. Pain Med. 21(8), 1546–1552 (2020).
Kesler, S. R., Kent, J. S. & O’Hara, R. Prefrontal cortex and executive function impairments in primary breast cancer. Arch. Neurol. 68(11), 1447–1453 (2011).
Boso, M. et al. Neurophysiology and neurobiology of the musical experience. Funct. Neurol. 21(4), 187–191 (2006).
Kang, J., Scholp, A. & Jiang, J. J. A review of the physiological effects and mechanisms of singing. J. Voice. 32(4), 390–395 (2018).
Bonassi, G. et al. How music moves us: Music-induced emotion influences motor learning. Neuroscience 526, 246–255 (2023).
Ferreri, L. et al. Dopamine modulates the reward experiences elicited by music. Proc. Natl. Acad. Sci. USA 116(9), 3793–3798 (2019).
Vik, B. M. D., Skeie, G. O. & Specht, K. Neuroplastic effects in patients with traumatic brain injury after music-supported therapy. Front. Hum. Neurosci. https://doi.org/10.3389/fnhum.2019.00177 (2019).
Orak, Y. et al. Effects of music therapy on pain and oxidative stress in oocyte pick-up: A randomized clinical trial. Braz. J. Anesthesiol. 70(5), 491–499 (2020).
Weiwei, S. et al. Observation on the effect of personalized music therapy on alleviating the adverse psychological reaction of chemotherapy in breast cancer patients. Anhui Pharmac. 17(08), 1441–1443 (2013).
Li, Y. et al. Clinicopathological and prognostic role of STAT3/p-STAT3 in breast cancer patients in China: A meta-analysis. Sci. Rep. 9(1), 11243 (2019).
Turner, M. C. et al. Sleep and breast and prostate cancer risk in the MCC-Spain study. Sci. Rep. 12(1), 21807 (2022).
van Assche, E., de Backer, J. & Vermote, R. Music therapy and depression. Tijdschr. Psychiatr. 57(11), 823–829 (2015).
Tang, Q. et al. Effects of music therapy on depression: A meta-analysis of randomized controlled trials. PLoS One 15(11), e0240862 (2020).
Zhao, K. et al. A systematic review and meta-analysis of music therapy for the older adults with depression. Int. J. Geriatr. Psychiatry 31(11), 1188–1198 (2016).
Acknowledgements
We thank all of the staf who contributed their time to our research.
Author information
Authors and Affiliations
Contributions
X.Z.H. designed the study and search strategy. X.Z.H. and L.C. performed abstract and full-text screening, methodological quality, and GRADE assessment, and contributed to the completion of screening and data extraction for all data within this manuscript. X.Z.H. and L.S.F. designed and calculated meta-analyses, subgroup analyses, sensitivity analyses, and publication bias, and created images and tables. X.Z.H. wrote the original draft preparation, performed review and editing, and prepared the final draft. F.W.J. contributed to the critical evaluation of the findings and the drafting of the manuscript. X.Z.H., L.C., L.Y.Z., and L.Y.Z. contributed to editing and revising the manuscript in its final version. All authors read and approved the final version of the manuscript and agree with the order of presentation of the authors. All authors agreed the possible publication of our article on journal of clinical nursing. The participant has consented to the submission of the article to the journal.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix A
Appendix A


Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Xu, Z., Liu, C., Fan, W. et al. Effect of music therapy on anxiety and depression in breast cancer patients: systematic review and meta-analysis. Sci Rep 14, 16532 (2024). https://doi.org/10.1038/s41598-024-66836-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-66836-x
- Springer Nature Limited