
Abstract
Background
High blood pressure, anxiety, depression and sleep disorder is very common in patients with hypertension. We aimed to perform a meta-analysis to evaluate the effects of adjuvant music therapy for patients with hypertension, to provide insights to the clinical management of hypertension.
Methods
Two authors searched PubMed, Embase, Web of Science, the Cochrane Library, Chinese National Knowledge Infrastructure, China Biomedical Literature Database, Wanfang Databases for randomized controlled trials (RCTs) on the role of music therapy in hypertension up to Oct 15, 2022. RevMan 5.3 software was used for meta-analysis.
Results
A total of 20 RCTs including 2306 patients were finally included. 1154 patients received music therapy. Meta-analysis showed that music therapy can effectively reduce the systolic blood pressure(MD = − 9.00, 95%CI: − 11.99~- 6.00), diastolic blood pressure(MD = -6.53, 95%CI: -9.12~- 3.93), heart rate (MD = -3.76, 95%CI: -7.32~- 0.20), self-rating anxiety scale (SAS) score(MD =-8.55, 95%CI: -12.04~-4.12), self-rating depression scale (SDS) score(MD = -9.17, 95%CI: -13.85~-5.18), Hamilton anxiety scale (HAMA), score(MD = -3.37, 95%CI: − 5.38~- 1.36), PSQI score(MD =-1.61, 95%CI:-2.30~- 0.93) compared with routine therapy in patients with hypertension(all P < 0.05). No publication bias in the synthesized outcomes were found (all P > 0.05).
Conclusion
Music therapy can effectively control blood pressure and heart rate, reduce anxiety and depression levels, and improve sleep quality in hypertensive patients. Limited by the quantity and quality of included studies, the above conclusions need to be verified by more high-quality studies.
Similar content being viewed by others


Background
Hypertension is the first risk factor for cardiovascular associated diseases. With the change of lifestyle and rhythm, the prevalence of hypertension in countries around the world is increasing year by year [1]. Negative emotions such as high-sodium diet, obesity, excessive drinking, and anxiety and depression are all risk factors for hypertension [2, 3]. Negative emotions such as anxiety and depression interact with hypertension. Previous epidemiological studies [4, 5] have found that about 38.5% of Chinese hypertensive patients are associated with anxiety, and 19.8% were associated with depression. Negative emotions such as anxiety and depression can affect the degree of hypertension and reduce the quality of life of patients by affecting the release of vascular endothelial factor, reducing vascular activity, and increasing vascular resistance [6,7,8]. Therefore, it is very important to focus on improving patients’ anxiety and depression while treating hypertension.
At present, there are many drugs for the treatment of hypertension in clinic. Although they can control hypertension to a certain extent, long-term use of drug use is easy to produce drug resistance, and it is easy to relapse after drug withdrawal. Nonpharmacological treatments can be effective in lowering blood pressure without other health risks. As one of the non-drug treatment methods, music therapy has been used as an adjuvant therapy in hypertension treatment. Currently, many scholars [9,10,11] have evaluated the psychological and physiological effects of music therapy on hypertensive patients, but the sample size of each study is small, and the research results remain different. Even though previous meta-analyses [12, 13] have analyzed the of the effect of music therapy on blood pressure in patients with hypertension, with more related studies published, updated meta-analyses on the role of music therapy for hypertention are needed. Therefore, this meta-analysis aimed to use the meta-analysis method to comprehensively evaluate the application effect of music therapy on hypertensive patients, in order to provide evidence-based basis for the treatment and management of hypertension.
Methods
We conducted and reported this meta-analysis according to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement [14].
Document retrieval
Two authors searched PubMed, Embase, Web of Science, the Cochrane Library, Chinese National Knowledge Infrastructure (CNKI), China Biomedical Literature Database, Wanfang Databases for randomized controlled trials (RCTs) on the role of music therapy in hypertension. The retrieval time is from the establishment of the database to Oct 15, 2022. We used a combination of subject headings and free words to search. The language of searched and included publications were limited to English and Chinese. The search terms were as following: (“music” OR “music therapy” OR “sound therapy”) AND (“hypertension” OR “high blood pressure” OR “cardiovascular”)(Supplementary 1). In addition, we conducted a review search of relevant references in the included RCTs and important reviews to broaden the scope of the search.
Inclusion and exclusion criteria
The inclusion criteria for this meta-analysis were: (1) study type: RCT design; (2) study population was the hypertensive patients, who met the diagnostic criteria for hypertension: Systolic blood pressure ≥ 140mmHg and / or diastolic blood pressure ≥ 90mmHg[15, 16]; (3) intervention measures: in addition to receiving routine treatment, patients in the music group accepted the music intervention. The patients in the control group only received the same routine treatment as the music therapy intervention group; (4) The study reported the corresponding outcome indicators, and the data could be extracted.
The exclusion criteria for this meta-analysis were: (1) studies with unclear diagnosis of hypertension or hypertension complicated with risk factors for other diseases; (2) research population were special populations such as pregnant women and military personnel; (3) Low-quality reports(significant data errors, study design problems and incomplete data); (4) reviews, cases and those literature reports with data that could not be extracted for analysis.
Literature screening and data extraction
Literature screening and data extraction were conducted independently by two researchers in a blinded manner, and inconsistent literatures were reviewed and discussed. The following data were extracted according to the designed table: author, publication year, country, sample size, details of intervention measures and reported outcome indicators. The primary outcomes included systolic blood pressure, diastolic blood pressure. The secondary outcomes included heart rate, self-rating anxiety scale (SAS), self-rating depression scale (SDS), Hamilton anxiety scale (HAMA), Pittsburgh sleep quality index (PSQI).
Quality assessment
The quality of the included literature was evaluated according to the risk of bias tool [17] recommended by Cochrane library. The tool includes following items: sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and “other” issues. Every item can be rated as “low risk of bias”, “high risk of bias” or “unclear risk of bias” accordingly.
Statistical analysis
We used Review Manager (RevMan) Version 5.3. software for meta-analysis. Measurement data were expressed as mean difference (MD) and 95% confidence interval (CI). In addition, we performed the heterogeneity test by the Q test, and combined with I2 to quantitatively judge the heterogeneity. If there was homogeneity among studies(I2 < 50%), a fixed-effects model was used to calculate the combined statistics; if there was heterogeneity(I2 ≥ 50%), random-effects model was used. Sensitivity analysis was performed by excluding articles one by one and then recombining the calculation. A funnel plot and Egger’s test were used to assess the publication bias of the pooled results. In this meta-analysis, P < 0.05 was considered to be statistically significant between groups.
Results
Study inclusion
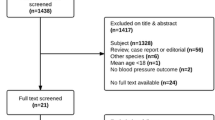
A preliminary search obtained 202 relevant literatures. After screening according to the inclusion and exclusion criteria, a total of 20 RCTs [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37] that met the criteria were finally included in this meta-analysis. The literature screening process is shown in Fig. 1.

PRISMA flow diagram of RCT selection
Characteristics of included studies
Of the included 20 RCTs [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37], a total of 2306 patients with hypertension were included, of whom 1154 patients received music therapy, 1152 received routine anti-hypertension treatment. The characteristics of the included studies are shown in Table 1.
The quality of included studies
The quality of included RCTs is presented in Figs. 2 and 3. The quality of the studies included in the RCTs was generally good taking into account the integrity of research design and data. Most of the RCTs reported the detailed random sequence generation methods, and random assignment concealment and blinding settings were less reported. Given the nature of music interventions, it was difficult to blind researchers. No bias on other items was found.

Risk of bias graph

Risk of bias summary
Meta-analysis
Systolic blood pressure
Seventeen studies [18,19,20, 22,23,24,25,26,27,28, 30,31,32,33,34,35, 37] reported changes in systolic blood pressure in patients before and after the intervention. The pooled results on systolic blood pressure results were heterogeneous (I2 = 91%), so a random-effects model was used to pool the results. The results of meta-analysis showed that the mean systolic blood pressure drop in the music therapy group was greater than that in the control group, and the difference was statistically significant (MD = − 9.00, 95%CI: − 11.99~- 6.00, P<0.001, Fig. 4).

Forest plot for systolic blood pressure change
Diastolic blood pressure
Sixteen studies [19, 20, 22,23,24,25,26,27,28, 30,31,32,33,34,35, 37] reported changes in diastolic blood pressure in patients before and after the intervention. The pooled results on diastolic blood pressure results were heterogeneous (I2 = 94%), so a random-effects model was used to pool the results. The results of meta-analysis showed that the mean diastolic blood pressure drop in the music therapy group was greater than that in the control group, and the difference was statistically significant (MD = -6.53, 95%CI: -9.12~- 3.93, P<0.001, Fig. 5).

Forest plot for diastolic blood pressure change
Heart rate
Five studies [24, 25, 29, 33, 37] reported changes in heart rate in patients before and after the intervention. The pooled results on diastolic blood pressure results were heterogeneous (I2 = 97%), so a random-effects model was used to pool the results. The results of meta-analysis showed that the mean heart rate drop in the music therapy group was greater than that in the control group, and the difference was statistically significant (MD = -3.76, 95%CI: -7.32~- 0.20, P = 0.04, Fig. 6).

Forest plot for heart rate change
Other outcomes
As indicated in Table 2, the results of meta-analysis showed that music therapy reduced the SAS score(MD =-8.55, 95%CI: -12.04~-4.12), SDS score(MD = -9.17, 95%CI: -13.85~-5.18), HAMA score(MD = -3.37, 95%CI: − 5.38~- 1.36), PSQI score(MD =-1.61, 95%CI:-2.30~- 0.93) compared with routine therapy in patients with hypertension(all P < 0.05).
Publication bias
We used funnel plots (Fig. 7) combined with Egger’s test to assess the asymmetry of funnel plots, and the results showed that there was no publication bias in each combined result (all P > 0.05).

Funnel plots for systolic and diastolic blood pressure changes
Sensitivity analysis
After excluding each study in turn, the heterogeneity and results of the remaining included studies did not change significantly after pooling, indicating that the results were robust and reliable.
Discussions
Hypertension is a psychosomatic disease related to psychological and mental factors. Long-term mental stress is one of the risk factors for hypertension [38]. The risk of hypertension in people with long-term anxiety and worry is 1.18 times that of normal people [39]. To a certain extent, it is the physiological response of the patient’s nervous and anxious psychological state. A total of 20 RCTs were included in this meta-analysis study, which preliminarily has evaluated the effect of music therapy on blood pressure in hypertensive patients. The results of this meta-analysis indicate that music therapy is beneficial to reduce the systolic, diastolic blood pressure and heart rate, and it is helpful to reduce the anxiety, depression level and improve the sleep quality of patients with hypertension. Music therapy is safe and effective as an adjuvant therapy for hypertension and is worthy of clinical promotion.
The effects and mechanisms of music therapy in the treatment of hypertension may be explained in following aspects. Firstly, it has been reported that when the sound waves of music act on the brain, it increases the excitability of the nervous system and promotes the secretion of hormones such as acetylcholine, thereby slowing down the heart rate [40,41,42]. Secondly, music diverts the patient’s attention to the disease, reduces sympathetic nerve excitability, produces sedative and antihypertensive effects, and regulates endocrine to reduce renin-angiotensin II secretion to reduce blood pressure [43, 44]. Additionally, the sound wave acts on the brain, adjusts the functional state of the cortex, relieves anxiety and tension, thereby causing changes in physiological and psychological states [45, 46]. In addition, the vitality of the entire nervous system and cell excitability can be enhanced by pleasant music, thereby regulating human physiological activities, eliminating the individual’s tension, reducing their irritable emotions, and ultimately leading to a drop in blood pressure and an improvement in the blood supply function of the heart [47,48,49].
Music therapy is beneficial to reduce the anxiety, depression level of patients with hypertension. Currently, the pathogenesis of anxiety and depression in hypertensive patients has not been fully elucidated, and it is mostly believed that it is caused by the joint action of serum serotonin (5-HT), norepinephrine (NE) and other neurotransmitters, and is related to neurological and endocrine dysfunction [50]. Both 5-HT and NE are important neurotransmitters in the human body, which can participate in the regulation of various physiological and pathological functions such as body temperature, sleep, mental and emotional functions [51,52,53]. Studies [54, 55] have found that 5-HT and NE are in low levels in depressed patients. A study [56] has found that compared with before treatment, the levels of 5-HT and NE in the two groups increased after treatment, and the increase in the music therapy group was better than that in the control group. It has been reported that five-element music can improve the level of central neurotransmitter in patients, improve the anxiety and depression state of patients, and then improve the blood pressure control level of patients [57].
Several previous systematic reviews have evaluated the role of music therapy on the patients with hypertension. Yang et al. [58]. have analyzed a total of 7 reports and have concluded that music therapy can effectively reduce diastolic blood pressure in patients, but it does not have effect on and systolic blood pressure. Systolic blood pressure was highly heterogeneous, and no plausible explanation was given for its heterogeneity. Besides, it has been reported that music therapy is only effective for systolic blood pressure, but not significantly for diastolic blood pressure [10]. However, their research only included two literatures for meta-analysis, and it is difficult to support their views due to the small number of sample size, so the conclusions they draw should be treated with caution. Kühlmann et al. [9] have finally included 10 related studies from PubMed, Medline, Cochrane Central, Web of Science and Google Scholar databases, and analyzed that although both systolic and diastolic blood pressure had a downward trend after music therapy, the decline has not reach statistical significance. It has scientific significance and cannot explain the relationship between hypertension and diastolic blood pressure. Compared with published related studies, this study has certain advantages. more RCTs were included than previous studies. Besides, we have chosen stricter inclusion and exclusion criteria, excluding some studies that might affect the accuracy of the results. Furthermore, the evaluation of SAS score, SDS score, HAMA score, PSQI score, etc. of hypertensive patients have been added in this study, and the current research shows that these may be related to the disease control of hypertensive patients.
There are certain limitations in this study that are worth considering. Firstly, most of the included studies lack allocation concealment and double-blind implementation, and there may be selection bias in the time, and type choice of music, which may affect the results of the study. Secondly, some of the included studies did not provide the mean value of the changes before and after intervention, we calculated the coefficient by reporting the complete study, and the results may have a certain bias. Thirdly, some of the included RCTs did not fully report the characteristics of the study population and music type, and the results of some studies were heterogeneous, but there was insufficient data for subgroup analysis, so the results of this study should be treated with caution.
Conclusions
In conclusion, music therapy can effectively reduce blood pressure and heart rate in patients with hypertension, reduce anxiety and depression levels, and improve sleep quality of patients, thereby improving blood pressure control and prognosis of patients. Compared with drug therapy, music therapy, as a low-cost, easy-to-operate, non-invasive therapy, can reduce medical expenses while achieving therapeutic effects, and it is an adjuvant therapy that clinicians can provide independently. The music therapy is worthy of discussion and application in clinical practice for hypertension management. Still, it is recommended that future studies be designed strictly in accordance with the RCT requirements, and explore the influence of music therapy on more indicators of hypertensive patients, and evaluate the intervention time, music type, playing time, and listening style, so as to provide support for the clinical application of music therapy intervention for hypertensive patients.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- RCTs:
-
Randomized controlled trials
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- CNKI:
-
Chinese National Knowledge Infrastructure
- SAS:
-
Self-rating anxiety scale
- SDS:
-
Self-rating depression scale
- HAMA:
-
Hamilton anxiety scale
- PSQI:
-
Pittsburgh sleep quality index
- MD:
-
Mean difference
- CI:
-
Confidence interval
References
McFadden CB. Update in hypertension. Med Clin North Am. 2022;106(2):259–67.
Boulestreau R, van den Born BH, Lip GYH, Gupta A. Malignant hypertension: current Perspectives and Challenges. J Am Heart Assoc. 2022;11(7):e023397.
Sarathy H, Salman LA, Lee C, Cohen JB. Evaluation and management of secondary hypertension. Med Clin North Am. 2022;106(2):269–83.
Hypertension MCGoHRMi. Multidisciplinary Expert Consensus on Heart Rate Management in Chinese Hypertensive Patients. Chin Gen Med. 2021;24(20):8–15.
Xiaoting YXP, Zhe Q. Trends and influencing factors of hypertension prevalence, awareness rate, treatment rate and control rate in chinese adults from 1991 to 2015. Chin Gen Pract Med. 2022;25(7):12–6.
Manosroi W, Williams GH. Genetics of Human primary hypertension: focus on hormonal mechanisms. Endocr Rev. 2019;40(3):825–56.
Zhang CJ, Shi YN, Liao DF, Du K, Qin L. Molecular mechanism of vascular remodeling in hypertension and chinese medicine intervention. Sheng Li Xue Bao. 2019;71(2):235–47.
Song Y, Jia H, Hua Y, Wu C, Li S, Li K, Liang Z, Wang Y. The molecular mechanism of Aerobic Exercise improving vascular remodeling in hypertension. Front Physiol. 2022;13:792292.
Kuhlmann AY, Etnel JR, Roos-Hesselink JW, Jeekel J, Bogers AJ, Takkenberg JJ. Systematic review and meta-analysis of music interventions in hypertension treatment: a quest for answers. BMC Cardiovasc Disord. 2016;16:69.
do Amaral MA, Neto MG, de Queiroz JG, Martins-Filho PR, Saquetto MB, Oliveira Carvalho V. Effect of music therapy on blood pressure of individuals with hypertension: a systematic review and Meta-analysis. Int J Cardiol. 2016;214:461–4.
Raglio A, De Maria B, Perego F, Galizia G, Gallotta M, Imbriani C, Porta A, Dalla Vecchia LA. Effects of Algorithmic Music on the Cardiovascular Neural Control J Pers Med. 2021;11(11).
Xiao Y, Xiaojuan L, Dianju Q. Meta analysis of the effect of music therapy on blood pressure in patients with hypertension. Contemp Med. 2018;24(10):3–6.
Yaqi D, Daju P, Juan L, Fang C. Meta analysis of the effects of Wuxing music therapy on anxiety, depression and blood pressure after cardiovascular disease. Chin Gen Med. 2020;12(8):1359–62.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700.
Parati G, Lombardi C, Pengo M, Bilo G, Ochoa JE. Current challenges for hypertension management: from better hypertension diagnosis to improved patients’ adherence and blood pressure control. Int J Cardiol. 2021;331:262–9.
Kunshen L, Chao L. Diagnostic criteria and cardiovascular risk stratification of hypertension. Chin J practical Intern Med. 2001;21(8):2–6.
Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA, et al. The Cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
Bekiroglu T, Ovayolu N, Ergun Y, Ekerbicer HC. Effect of turkish classical music on blood pressure: a randomized controlled trial in hypertensive elderly patients. Complement Ther Med. 2013;21(3):147–54.
CR Z, PC J, CM S. Music therapy effects on the quality of life and the blood pressure of hypertensive patients. Arq Bras Cardiol. 2009;93(5):534–40.
Guozhi H, Dahong Z. The effect of music therapy on blood pressure and psychological function in patients with essential hypertension. Chin J Rehabilitation Med. 1995;21(1):28–30.
Hong L, Wuxian C, Zhengli W. The influence of music therapy on the psychological function of hypertensive patients. J Guangxi Med Univ. 2006;18(2):26–7.
Hongmei L, Qing B, Yao W. Analysis of the influence of traditional Chinese medicine five elements music therapy on blood pressure and anxiety in patients with hypertensio. Health Rep. 2018;42(28):198#x2013;9.
Im-Oun S, Kotruchin P, Thinsug P, Mitsungnern T, Techa-Atik P, Pongchaiyakul C. Effect of Thai instrumental folk music on blood pressure: a randomized controlled trial in stage-2 hypertensive patients. Complement Ther Med. 2018;39:43–8.
Jing L. Efficacy observation of amlodipine besylate combined with music therapy in the treatment of primary mild to moderate hypertension. Chin Health Nutr. 2014;24(5):2478–9.
Kunikullaya KU, Goturu J, Muradi V, Hukkeri PA, Kunnavil R, Doreswamy V, Prakash VS, Murthy NS. Music versus lifestyle on the autonomic nervous system of prehypertensives and hypertensives–a randomized control trial. Complement Ther Med. 2015;23(5):733–40.
Lan Y, Qiulu L. Effects of music relaxation adjuvant therapy on the balance of autonomic nervous system in patients with hypertension. China Clin Rehabilitation. 2002;6(15):2247–9.
Min Z, Meijun L. Effects of traditional chinese medicine five elements music therapy on blood pressure and anxiety in hypertensive patients. Med Theory Pract. 2018;31(13):450–2.
Min Z, Wenli S. Effects of five elements music therapy on blood pressure and mood in patients with hypertensive liver-yang hypertensive syndrome. J Xinjiang Med Univ. 2021;44(11):5–9.
VM S, B G. Evaluating the effect of music intervention on hypertension. Curr Sci. 2020;118(4):612–20.
Wenhua L, Xiangang F. The effect of non-drug comprehensive intervention combined with music therapy in the treatment of hypertension. Contemp Nurs. 2018;25(6):27–9.
Teng XF, Wong MY, Zhang YT. The effect of music on hypertensive patients. In: Annual International Confer-ence of the IEEE Engineering in Medicine and Biology Society: 2007; 2007: 4649–4651.
Xiaohong L, Chaxiang L, Li Z. Effects of music therapy on quality of life and blood pressure in hypertensive patients. Shandong Med. 2013;53(20):90–1.
Xuemin T, Yingying J. Effects of bisoprolol combined with music therapy on resting heart rate and sympathetic nerve activity in patients with essential hypertension. China Pharm. 2015;24(12):38–40.
Yingxia C, Zhe Y. The effect of MP3 music therapy on blood pressure in hypertensive patients. Chin Med Innov. 2009;6(22):180–1.
Yongquan S, Kun L. Effects of music therapy on anxiety, blood pressure and sleep status in elderly hypertensive patients. Chin J Gerontol. 2015;35(7):1967–8.
Yu Z, Junhong L, Huiguang T. Effects of music therapy on the health status of patients with essential hypertension. Med Theory Pract. 2015;28(17):2391–4.
Yueping W, Cailing L. The effect of personalized music therapy on the rehabilitation of patients with cardiovascular disease. Int J Nurs. 2009;28(7):884–6.
Ho CY, Wexberg P, Schneider B, Stollberger C. Effect of music on patients with cardiovascular diseases and during cardiovascular interventions: a systematic review. Wien Klin Wochenschr. 2021;133(15–16):790–801.
Shujing M, Liu Y, Min Z. Changes in blood pressure level and hypertension detection rate among chinese children and adolescents from 1991 to 2015. Chin J Epidemiol. 2020;41(2):178–83.
Mir IA, Chowdhury M, Islam RM, Ling GY, Chowdhury A, Hasan ZM, Higashi Y. Relaxing music reduces blood pressure and heart rate among pre-hypertensive young adults: a randomized control trial. J Clin Hypertens (Greenwich). 2021;23(2):317–22.
Yu JY, Huang DF, Li Y, Zhang YT. Implementation of MP3 player for music therapy on hypertension. Annu Int Conf IEEE Eng Med Biol Soc. 2009;2009:6444–7.
Guerrier G, Bernabei F, Lehmann M, Pellegrini M, Giannaccare G, Rothschild PR. Efficacy of preoperative music intervention on Pain and anxiety in patients undergoing cataract surgery. Front Pharmacol. 2021;12:748296.
Vlachopoulos C, Aggelakas A, Ioakeimidis N, Xaplanteris P, Terentes-Printzios D, Abdelrasoul M, Lazaros G, Tousoulis D. Music decreases aortic stiffness and wave reflections. Atherosclerosis. 2015;240(1):184–9.
Watkins GR. Music therapy: proposed physiological mechanisms and clinical implications. Clin Nurse Spec. 1997;11(2):43–50.
Niu JF, Zhao XF, Hu HT, Wang JJ, Liu YL, Lu DH. Should acupuncture, biofeedback, massage, Qi gong, relaxation therapy, device-guided breathing, yoga and tai chi be used to reduce blood pressure?: recommendations based on high-quality systematic reviews. Complement Ther Med. 2019;42:322–31.
Lorber M, Divjak S. Music therapy as an intervention to reduce blood pressure and anxiety levels in older adults with hypertension: a Randomized Controlled Trial. Res Gerontol Nurs. 2022;15(2):85–92.
Teng XF, Wong MY, Zhang YT. The effect of music on hypertensive patients. Annu Int Conf IEEE Eng Med Biol Soc 2007; 2007:4649–4651.
Namdar H, Taban Sadeghi M, Sabourimoghaddam H, Sadeghi B, Ezzati D. Effects of music on cardiovascular responses in men with essential hypertension compared with healthy men based on introversion and extraversion. J Cardiovasc Thorac Res. 2014;6(3):185–9.
Zhan HR, Hong ZS, Chen YS, Hong HY, Weng ZB, Yang ZB, Shi JL, Chen ZB. Non-invasive treatment to grade 1 essential hypertension by percutaneous laser and electric pulse to acupoint with music: a randomized controlled trial. Chin J Integr Med. 2016;22(9):696–703.
Olivieri-Mui BL, Devlin JW, Ochoa A, Schenck D, Briesacher B. Perceptions vs. evidence: therapeutic substitutes for antipsychotics in patients with dementia in long-term care. Aging Ment Health. 2018;22(4):544–9.
DeJesus SA, Diaz VA, Gonsalves WC, Carek PJ. Identification and treatment of depression in minority populations. Int J Psychiatry Med. 2011;42(1):69–83.
Wattanasoei S, Binson B, Kumar R, Somrongthong R, Kanchanakhan N. Quality of life through listening music among Elderly People in Semi-Urban Area, Thailand. J Ayub Med Coll Abbottabad. 2017;29(1):21–5.
Milovanovic B, Trifunovic D, Djuric D. Autonomic nervous system adjustment (ANSA) in patients with hypertension treated with enalapril. Acta Physiol Hung. 2011;98(1):71–84.
Luo C, Fan H, Li S, Zou Y. Therapeutic of Candesartan and Music Therapy in Diabetic Retinopathy with Depression in Rats. Evid Based Complement Alternat Med. 2021;2021:5570356.
Brammer SV. What interventions improve outcomes for the patient who is depressed and in Pain? Pain Manag Nurs. 2018;19(6):580–4.
Kumar AM, Tims F, Cruess DG, Mintzer MJ, Ironson G, Loewenstein D, Cattan R, Fernandez JB, Eisdorfer C, Kumar M. Music therapy increases serum melatonin levels in patients with Alzheimer’s disease. Altern Ther Health Med. 1999;5(6):49–57.
Jinliang L, Hongsheng W, Zhenwei Y. Cognitive therapy combined with five elements music in the treatment of essential hypertension. Chin J Health Psychol. 2010;33(12):2–5.
Xiao Y, Xiaojuan L, Dianju Q. A meta-analysis of the effect of music therapy on blood pressure in patients with hypertension. Contemp Med. 2018;24(10):6–8.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
Cao Min designed research; Cao Min, Zhiyuan Zhang conducted research; Cao Min analyzed data; Cao Min, Zhiyuan Zhang wrote the first draft of manuscript; Cao Min had primary responsibility for final content. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
In this study, all methods were performed in accordance with the relevant guidelines and regulations. Ethics approval and consent to participate is not necessary since our study is a meta-analysis and systematic review.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cao, M., Zhang, Z. Adjuvant music therapy for patients with hypertension: a meta-analysis and systematic review. BMC Complement Med Ther 23, 110 (2023). https://doi.org/10.1186/s12906-023-03929-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12906-023-03929-6