
Abstract
Injury is the most common cause of preventable morbidity and death among children under five. This study aimed to describe the epidemiological characteristics of injury-related mortality rates in children under five and to provide evidence for future preventive strategies. Data were obtained from the Under Five Child Mortality Surveillance System in Hunan Province, China, 2015–2020. Injury-related mortality rates with 95% confidence intervals (CI) were calculated by year, residence, gender, age, and major injury subtype (drowning, suffocation, traffic injuries, falls, and poisoning). And crude odds ratios (ORs) were calculated to examine the association of epidemiological characteristics with injury-related deaths. The Under Five Child Mortality Surveillance System registered 4,286,087 live births, and a total of 22,686 under-five deaths occurred, including 7586 (which accounted for 33.44% of all under-five deaths) injury-related deaths. The injury-related under-five mortality rate was 1.77‰ (95% CI 1.73–1.81). Injury-related deaths were mainly attributed to drowning (2962 cases, 39.05%), suffocation (2300 cases, 30.32%), traffic injuries (1200 cases, 15.82%), falls (627 cases, 8.27%), and poisoning (156 cases, 2.06%). The mortality rates due to drowning, suffocation, traffic injuries, falls, and poisoning were 0.69‰ (95% CI 0.67,0.72), 0.54‰ (95% CI 0.51,0.56), 0.28‰ (95% CI 0.26,0.30), 0.15‰ (95% CI 0.13,0.16), and 0.04‰ (95% CI 0.03,0.04), respectively. From 2015 and 2020, the injury-related mortality rates were 1.78‰, 1.77‰, 1.60‰, 1.78‰, 1.80‰, and 1.98‰, respectively, and showed an upward trend (χ2trend = 7.08, P = 0.01). The injury-related mortality rates were lower in children aged 0–11 months than in those aged 12–59 months (0.52‰ vs. 1.25‰, OR = 0.41, 95% CI 0.39–0.44), lower in urban than rural areas (1.57‰ vs. 1.88‰, OR = 0.84, 95% CI 0.80–0.88), and higher in males than females (2.05‰ vs . 1.45‰, OR = 1.42, 95% CI 1.35–1.49). The number of injury-related deaths decreased with children’s age. Injury-related deaths happened more frequently in cold weather (around February). Almost half (49.79%) of injury-related deaths occurred at home. Most (69.01%) children did not receive treatment after suffering an injury until they died, and most (60.98%) injury-related deaths did not receive treatment because it was too late to get to the hospital. The injury-related mortality rate was relatively high, and we have described its epidemiological characteristics. Several mechanisms have been proposed to explain these phenomena. Our study is of great significance for under-five child injury intervention programs to reduce injury-related deaths.
Similar content being viewed by others

Introduction
Injury is a major cause of death of children in China. The overall injury-related under-five mortality rate was 1.6‰ in 2015 in China, and injury is the third leading cause of under-five deaths and the first leading cause of death among children between 1 and 4 years old1. Injury is also a major cause of death of children worldwide2. The injury-related mortality rate in children is much higher in low- and middle-income countries than in high-income countries, and it is estimated that more than 95% of injury-related deaths in children occur in developing countries2,3,4,5. There is still much room for a decline in the injury-related under-five mortality rate in China.
There were some studies focused on the epidemiological characteristics of injury-related under-five deaths. E.g., in Turkey (2014–2017), injury-related under-five deaths were mainly attributed to traffic injuries (36.5%), falls (12.0%), and suffocation (10.2%). Of all injury deaths, 59.9% were males, and 52.7% occurred at home or in its close vicinity6; In Iran (2010–2015), multivariate logistic regression showed that mothers' low education level, age 1–5 years', living in a supportive center, and having financial problems increased the odds of under-5 mortality caused by injury7; In China (2009–2016), injury-related under-five deaths were mainly attributed to suffocation (34.3%), drowning (29.6%), traffic injuries (17.7%), falls (7.2%) or poisoning (4.7%)8; From 2013 to 2019 in Sichuan, China, the top three causes of total under-five deaths were accidental drowning (35.0%), accidental suffocation (32.7%), and traffic accidents (15.5%)9.
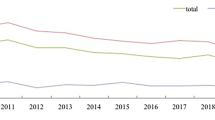
Injury is the most common cause of preventable morbidity and mortality among children10. Therefore, studies on the epidemiological characteristics of injury-related under-five deaths are important for providing evidence for future intervention11. However, the epidemiology of injury-related deaths among children under five has been rarely reported recently, and more studies need to be included in China (Fig. 1).

Time trends in injury-related under-five mortality rate in Hunan Province, China, 2015–2020.
Therefore, we investigated the epidemiology of the injury-related under-five mortality rate in Hunan Province, China, using Under Five Child Mortality Surveillance System data for the period 2015–2020. The aim of this study was to provide some information for under-five child injury intervention programs to reduce injury-related deaths.
Methods
Data sources
This study used data from the Under Five Child Mortality Surveillance System in Hunan Province, China, 2015–2020, which is run by the Hunan Provincial Health Commission and covers all under-five deaths in Hunan Province. Children’s death reports included demographic characteristics such as gender, age, primary cause of death, location of death and other key information. According to the WHO International Classification of Diseases (Tenth Revision, ICD-10), 23 injuries in this study were classified into five types: drowning (W65–W74), traffic injury (V01–V98), suffocation (W75–W84), poisoning (X44–X49), fall (W00–W19), or “other” (W20–W64, W85–W94, X00–X43, X50–X59).
Our data were derived from the Under Five Child Mortality Surveillance System. It is the second use of the data, and no further ethical approval was required for the present study.
Data quality control
To carry out surveillance, the Hunan Provincial Health Commission formulated the "Maternal and Child Health Monitoring Manual in Hunan Province". Data were collected and reported by experienced doctors. To reduce the integrity rate and information error rate, we asked the technical guidance departments to carry out comprehensive quality control each year.
Statistical analysis
The injury-related mortality rate is defined as the number of deaths from injury per 1000 live births (‰). We calculated the injury-related mortality rate and 95% confidence intervals (CI) by Poisson’s regression. Chi-square trend tests (χ2trend) were used to determine trends in mortality rates by year. Crude odds ratios (ORs) were calculated to examine the association of each epidemiological characteristic with injury-related deaths.
All statistical analyses in this study were performed using SPSS 18.0 (International Business Machines Corporation, New York City, United States).
Results
Injury-related under-five mortality rate in Hunan Province, China, 2015–2020
Our study included 4,286,087 live births, and a total of 22,686 under-five deaths occurred, including 7586 (accounted for 33.44% of all under-five deaths) injury-related deaths. The injury-related under-five mortality rate was 1.77‰ (95% CI 1.73–1.81). Table 1 shows the injury-related mortality rates and proportions by year, residence, gender, and age. (Table 1).
Injury-related under-five mortality rate by injury type
Injury-related deaths were mainly attributed to drowning (2962 cases, 39.05%), suffocation (2300 cases, 30.32%), traffic injuries (1200 cases, 15.82%), falls (627 cases, 8.27%), and poisoning (156 cases, 2.06%). The mortality rates due to drowning, suffocation, traffic injuries, falls, and poisoning were 0.69‰ (95% CI 0.67, 0.72), 0.54‰ (95% CI 0.51, 0.56), 0.28‰ (95% CI 0.26, 0.30), 0.15‰ (95% CI 0.13, 0.16), and 0.04‰ (95% CI 0.03, 0.04), respectively. (Table 2).
Injury-related under-five mortality rate by year
From 2015 and 2020, the injury-related mortality rates were 1.78‰, 1.77‰, 1.60‰, 1.78‰, 1.80‰, and 1.98‰, respectively, and showed an upward trend (χ2trend = 7.08, P = 0.01). The mortality rates from suffocation, falls, and poisoning showed increasing trends, too (P < 0.05). (Table 3).
Injury-related under-five mortality rate by age
The injury-related mortality rates were lower in children aged 0–11 months than in those aged 12–59 months (0.52‰ vs. 1.25‰, OR = 0.41, 95% CI 0.39–0.44). Injury-related deaths due to drowning (OR = 0.02, 95% CI 0.02–0.03), traffic injuries (OR = 0.10, 95% CI 0.08–0.12), falls (OR = 0.18, 95% CI 0.14–0.22), and poisoning (OR = 0.27, 95% CI 0.18–0.39) were more common in children aged 12–59 months, while deaths due to suffocation were more common in children aged 0–11 months (OR = 4.03, 95% CI 3.64–4.47). (Table 4).
Injury-related under-five mortality rate by residence
The injury-related mortality rates were lower in urban than rural areas (1.57‰ vs. 1.88‰, OR = 0.84, 95% CI 0.80–0.88). Injury-related deaths due to drowning (OR = 0.89, 95% CI 0.82–0.96), suffocation (OR = 0.79, 95% CI 0.73–0.87), and traffic injuries (OR = 0.81, 95% CI 0.72–0.92) were more common in rural areas. (Table 5).
Injury-related under-five mortality rate by gender
The injury-related mortality rates were higher in males than females (2.05‰ vs. 1.45‰, OR = 1.42, 95% CI 1.35–1.49). Injury-related deaths due to drowning (OR = 1.80, 95% CI 1.66–1.94), suffocation (OR = 1.22, 95% CI 1.12–1.33), traffic injuries (OR = 1.13, 95% CI 1.01–1.27), and falls (OR = 1.35, 95% CI 1.15–1.58) were more common in males. (Table 6).
Proportions of injury-related under-five deaths by injury types and epidemiological characteristics
Table 7 showed the following epidemiological characteristics of injury-related deaths: (1) The number of injury-related deaths decreased with children’s age. (2) Injury-related deaths happened more frequently in cold weather (around February). (3) Almost half (49.79%) of injury-related deaths occurred at home. (4) Most (69.01%) children did not receive treatment after suffering an injury until they died, and most (60.98%) injury-related deaths did not receive treatment because it was too late to get to the hospital.
The epidemiological characteristics of some injury subtypes differed from those described above: (1) Most (71.94%) deaths due to drowning occurred in children aged 12–35 months, and were more common in July. (2) Most (80.13%) deaths due to suffocation occurred in children aged 0–11 months, and were more common in January. (3) Most deaths due to traffic injuries happened on the way to the hospital (41.58%) and in the hospital (34.08%) (Table 7).
Discussion
Overall, we found that drowning and suffocation were the most common injury types for under-five deaths. Injury-related under-five deaths were more common in children aged 12–59 months, those living in rural areas, and males. In addition, we found that injury-related under-five deaths were associated with some epidemiological characteristics.
The overall injury-related under-five mortality rate (1.77‰) in our study is consistent with the reported mortality rate in China (1.6‰ in 2015)1. Several comprehensive studies showed that the injury-related under-five mortality rate in China is higher than in developed countries2,4. The following are injury-related under-five mortality rates reported in some regions: 9.1/100,000 in Turkey in 20176; 39.5/100,000 in Pakistan, 2006–200712; 302/100,000 in India in 200513; 48.96/10,000 in Hunan Province, China, 2009–201414; 1.7–3.8‰ in Sichuan Province, China, 2009–201715. There are major differences between them. It may indicate that there are large geographical differences in injury-related under-five mortality rates, and that injury-related under-five mortality rates are changing over time. In this study, the proportion of injury-related under-five deaths in total under-five deaths increased steadily from 2015 to 2020, and the injury-related under-five mortality rate showed an upward trend, while some previous studies showed downward trends15,16. It suggested that injuries were gradually becoming the leading cause of under-five deaths in Hunan Province, China. Therefore, it deserves our special attention.
Previous studies showed that the leading injury types worldwide for under-five deaths were traffic injuries, drowning, burn, suffocation, and falls4. Chen et al. reported that the leading injury types for under-five deaths were traffic accidents (57.44%) and drowning (35.53%) in China, 2006–201716. It is different from our study. And many other studies also reported different injury types for under-five deaths14,15,17,18,19,20,21,22. It indicated that there are differences in injury types for under-five deaths in different areas, and also that the leading injury types for under-five deaths are changing over time.
In this study, drowning was the leading cause of injury-related under-five deaths, which may be mainly related to open bodies of water, such as rivers and lakes. And it is more common in rural areas. It is consistent with some previous studies9,23,24,25. For most open bodies of water in rural areas, there were no protective measures and little reliable adult supervision for children. And it may increase the risk of drowning. Suffocation was the second-leading cause of injury-related under-five deaths and the leading cause of injury-related deaths for children aged 0–11 months. It is consistent with previous studies9. We have looked at the causes of suffocation and found most deaths due to suffocation occur in bed and through the inhalation of milk. It is consistent with previous studies26,27. It may be mainly related to the negligence and poor first-aid knowledge of caregivers27,28,29. From 2015 to 2020, the injury-related mortality rate due to suffocation increased year over year, while Wang et al. reported a steady suffocation mortality rate among children under five in China, 2006–201628. One possible explanation is China’s two-child policy since 201430, which increases caregivers' burden. It may require further, in-depth research.
Overall, we found injury-related under-five mortality rates were higher in children aged 12–59 months than those aged 0–11 months, higher in rural than urban areas, and higher in males than females. It is consistent with previous studies15,23,24,25,31,32,33,34,35,36. Although the injury-related mortality rate was higher in children aged 12–59 months than those aged 0–11 months, the number of injury-related deaths decreased with age by year. It is consistent with previous studies37. It may be associated with the poor self-protection ability of young children24. Higher injury-related mortality rates in rural areas may be related to the poor living environment, residents' safety literacy, and first-aid ability32,38,39,40. Higher injury-related mortality rates in males may be related to differences in biological temperament, cognitive strategies, exposure opportunity, and gender socialization15.
However, some injury subtypes were inconsistent with the overall injuries in terms of epidemiology. e.g., the mortality rate due to suffocation was higher in children aged 0–11 months than in those aged 12–59 months. Most deaths due to suffocation occurred in bed or through the inhalation of milk, as mentioned in the previous paragraph. It may be mainly related to the negligence and poor first-aid knowledge of caregivers. There were no statistically significant differences in mortality rates from falls and poisoning between urban and rural areas or in the mortality rate due to poisoning between males and females. It has been less well reported. Brito et al. found that use of the high net, the presence of stairs or steps without a handrail, and exits and passages kept with toys, furniture, boxes, or other items that may be obstructive were associated with the risk of falls in children under five years of age41. Children’s falls and poisoning injuries are more often the result of accidents than suicide.
In addition, some other epidemiological characteristics are associated with the injury-related under-five mortality rate. And some of them were rarely covered in previous studies. E.g., total injury deaths happened more often in cold weather (around February), while drowning deaths were more common in July. It is consistent with previous studies9,42,43. It is related to several factors: first, bad weather and poor road conditions in cold weather increase the risks of traffic accidents, and a large number of people travel to celebrate the Chinese Spring Festival (mostly celebrated in February), which also increases the risks of traffic accidents; Second, people take measures to keep warm in cold weather, which increases the risks of suffocation and gas poisoning; Third, higher temperatures in July increase the risks of children's exposure to water and drowning, and summer vacations in July and August also increase the risks of children's exposure to water and drowning. Most deaths due to drowning, suffocation, and poisoning occur at home. It is the result of most injuries occurring suddenly at home, and children receive no treatment until they die because it is too late to go to the hospital44. Instead, most deaths due to traffic injuries and falls occurred in hospitals or on the way to hospitals. It is the result of the fact that most traffic injuries and falls do not cause immediate deaths, leading to a large number of outpatient and hospitalized patients.
Some things could be improved in our study. As such, we did not analyze some epidemiological features due to data limitations, including economic conditions and educational levels of children’s parents.
Conclusion
In summary, our data indicated that the injury-related mortality rate was relatively high, and we have described its epidemiological characteristics. Several mechanisms have been proposed to explain these phenomena. Our study is of great significance for under-five child injury intervention programs to reduce injury-related deaths.
Data availability
All data generated or analysed during this study are included in this published article.
References
He, C. et al. National and subnational all-cause and cause-specific child mortality in China, 1996–2015: A systematic analysis with implications for the Sustainable Development Goals. Lancet Glob. Health. 5(2), e186–e197. https://doi.org/10.1016/s2214-109x(16)30334-5 (2017) (Epub 2016/12/23).
Huang, Y., Wu, Y., Schwebel, D. C., Zhou, L. & Hu, G. Disparities in under-five child injury mortality between developing and developed countries: 1990–2013. Int. J. Environ. Res. Public Health. 13(7), 1. https://doi.org/10.3390/ijerph13070653 (2016) (Epub 2016/07/12).
Li, L. et al. Legislation coverage for child injury prevention in China. Bull. World Health Organ. 93(3), 169–175. https://doi.org/10.2471/blt.14.139998 (2015) (Epub 2015/04/04).
Adeloye, D. et al. Global and regional child deaths due to injuries: an assessment of the evidence. J Glob Health. 8(2), 021104. https://doi.org/10.7189/jogh.08.021104 (2018) (Epub 2019/01/25).
World-Health-Organization. World report on child injury prevention (2008).
Çaylan, N., Yalçın, S.S., Tezel, B., Aydın, Ş., Özen, Ö., & Şengelen, M., et al. Evaluation of injury-related under-five mortality in Turkey between 2014–2017. Turk. J. Pediatr. 63(1), 37–47 (2021). https://doi.org/10.24953/turkjped.2021.01.005(Epub 2021/03/10)
Hooshangi, Z., Salehi, S., & Amini-Rarani, M. Explanatory social variables of under-5 mortality caused by injury in Isfahan Province, Islamic Republic of Iran. East. Medit. Health J. 26(6), 660–667 (2020). https://doi.org/10.26719/emhj.19.086(Epub 2020/07/06)
Xiang, L. et al. Injury-related mortality among children younger than 5 years in China during 2009–2016: An analysis from national surveillance system. Inj. Prev. J. Int. Soc. Child Adolesc. Injury Prev. 25(1), 60–66. https://doi.org/10.1136/injuryprev-2018-042853 (2019) (Epub2018/12/21).
Hu, J., Luo, M., He, L. & Zhao, Z. Analysis of characteristics and forecast of unintentional injury deaths of children under age 5 from 2013 to 2019 in Sichuan, China. BMC Public Health 22(1), 2133. https://doi.org/10.1186/s12889-022-14600-z (2022) (Epub 2022/11/22).
Bonilla-Escobar, F.J., & Gutiérrez, M. I. Injuries are not accidents: towards a culture of prevention. Colombia Med. (Cali, Colombia). 45(3), 132–135 (2014) (Epub 2014/11/12)
Jullien, S. Prevention of unintentional injuries in children under five years. BMC Pediatr. 21(Suppl 1), 311. https://doi.org/10.1186/s12887-021-02517-2 (2021) (Epub2021/09/10).
Razzak, J. A., Khan, U. R., Zia, N. & Azam, I. A child an hour: burden of injury deaths among children under 5 in Pakistan. Arch. Dis. Child. 98(11), 867–871. https://doi.org/10.1136/archdischild-2013-303654 (2013) (Epub 2013/08/21).
Jagnoor, J. et al. Unintentional injury deaths among children younger than 5 years of age in India: A nationally representative study. Inj. Prev. J. Int. Soc. Child Adolesc. Inj. Prev. 17(3), 151–155. https://doi.org/10.1136/ip.2010.029934 (2011) (Epub 2011/04/16).
Lili, X., Jian, H., Liping, L., Zhiyu, L. & Hua, W. Epidemiology of injury-related death in children under 5 years of age in Hunan Province, China, 2009–2014. PLoS ONE 12(1), e0168524. https://doi.org/10.1371/journal.pone.0168524 (2017) (Epub 2017/01/12).
Yao, M., Wu, G., Zhao, Z., Luo, M. & Zhang, J. Unintentional injury mortality among children under age five in urban and rural areas in the Sichuan province of west China, 2009–2017. Sci. Rep. 9(1), 2963. https://doi.org/10.1038/s41598-019-38936-6 (2019) (Epub2019/03/01).
Chen, B., Ye, P., Tang, B., Wang, S., Guo, J., & Wu, J. Unintentional injury mortality among children under five years—China, 2006–2017. China CDC Wkly. 2(10), 156–159 (2020) (Epub 2020/03/06).
Xu, Y. H., Huang, X. W. & Yang, R. L. Under 5 mortality rate and its contributors in Zhejiang Province of China from 2000 to 2009. Transl. Pediatr. 2(1), 34–39. https://doi.org/10.3978/j.issn.2224-4336.2012.04.07 (2013) (Epub2013/01/01).
Yan, S., & Zhu, X. Epidemiological study on the trend of accidental deaths among children under five in Beijing, during 2003–2012. Zhonghua Liu Xing Bing Xue Za Zhi. 35(5), 562–565 2014 (Epub 2014/07/26).
Lin, S. F., Hu, Y., Jiang, L., Xing, Y.F., Xiu, L. J., Liu, H.Y. Epidemiological study on the trend of accidental deaths among children under five in Guangzhou, 2001–2010. Zhonghua Liu Xing Bing Xue Za Zhi. 33(12), 1258–1260 (2012) (Epub 2013/01/23).
Jiang, G. et al. Leading causes of death from injury and poisoning by age, sex and urban/rural areas in Tianjin, China 1999–2006. Injury 42(5), 501–506. https://doi.org/10.1016/j.injury.2009.10.050 (2011) (Epub 2009/11/20).
Wang, S. Y. et al. Injury-related fatalities in China: an under-recognised public-health problem. Lancet (London, England). 372(9651), 1765–1773. https://doi.org/10.1016/s0140-6736(08)61367-7 (2008) (Epub 2008/10/22).
Theurer, W. M. & Bhavsar, A. K. Prevention of unintentional childhood injury. Am. Family Phys. 87(7), 502–509 (2013).
Wang, M. et al. Social and environmental risk factors for the accidental drowning of children under five in China. BMC Public Health 20(1), 1553. https://doi.org/10.1186/s12889-020-09650-0(Epub2020/10/17.) (2020).
Peden, A. E., Franklin, R. C. & Pearn, J. H. The prevention of child drowning: The causal factors and social determinants impacting fatalities in portable pools. Health Promot. J. Austr. 31(2), 184–191. https://doi.org/10.1002/hpja.282 (2020) (Epub 2019/08/02).
Jeong, J. et al. Relationship between drowning location and outcome after drowning-associated out-of-hospital cardiac arrest: Nationwide study. Am. J. Emerg. Med. 34(9), 1799–1803. https://doi.org/10.1016/j.ajem.2016.06.008 (2016) (Epub 2016/06/28).
Kong, F. et al. Healthy China 2030: how to control the rising trend of unintentional suffocation death in children under five years old. BMC Pediatr. 20(1), 376. https://doi.org/10.1186/s12887-020-02281-9 (2020) (Epub 2020/08/15).
Yu, X. et al. Social and environmental risk factors for unintentional suffocation among infants in China: A descriptive analysis. BMC Pediatr. 21(1), 465. https://doi.org/10.1186/s12887-021-02925-4 (2021) (Epub 2021/10/23).
Wang, L. et al. Under-five mortality from unintentional suffocation in China, 2006–2016. J. Glob. Health. 9(1), 010602. https://doi.org/10.7189/jogh.09-010602 (2019) (Epub 2019/02/19).
Gao, Y., Schwebel, D. C. & Hu, G. Infant mortality due to unintentional suffocation among infants younger than 1 year in the United States, 1999–2015. JAMA Pediatr. 172(4), 388–390. https://doi.org/10.1001/jamapediatrics.2017.4887 (2018) (Epub2018/02/21).
Fan, S. L. et al. How does the two-child policy affect the sex ratio at birth in China? A cross-sectional study. BMC Public Health 20(1), 789. https://doi.org/10.1186/s12889-020-08799-y (2020) (Epub 2020/05/29).
Li, Y., Pu, M., Wang, Y., Feng, T. & Jiang, C. Analysis of the reduction in injury mortality disparity between urban and rural areas in developing China from 2010 to 2016. BMC Public Health 20(1), 903. https://doi.org/10.1186/s12889-020-09027-3 (2020) (Epub 2020/06/12).
Mathur, A., Mehra, L., Diwan, V. & Pathak, A. Unintentional childhood injuries in urban and rural Ujjain, India: A community-based survey. Children (Basel). 5(2), 1. https://doi.org/10.3390/children5020023 (2018) (Epub 2018/02/09).
Boland, M., Staines, A., Fitzpatrick, P. & Scallan, E. Urban-rural variation in mortality and hospital admission rates for unintentional injury in Ireland. Inj. Prev. 11(1), 38–42. https://doi.org/10.1136/ip.2004.005371 (2005) (Epub 2005/02/05).
Liu, Q. et al. The gap in injury mortality rates between urban and rural residents of Hubei Province China. BMC Public Health 12, 180. https://doi.org/10.1186/1471-2458-12-180 (2012) (Epub 2012/03/14).
Chen, Y., Mo, F., Yi, Q. L., Jiang, Y., & Mao, Y. Unintentional injury mortality and external causes in Canada from 2001 to 2007. Chronic Dis. Inj. Can. 33(2), 95–102 2013 (Epub 2013/03/09).
Wang, L. et al. Unintentional drowning mortality in China, 2006–2013. Inj. Prev. 25(1), 47–51. https://doi.org/10.1136/injuryprev-2017-042713 (2019) (Epub 2018/04/25).
West, B. A., Rudd, R. A., Sauber-Schatz, E. K. & Ballesteros, M. F. Unintentional injury deaths in children and youth, 2010–2019. J Safety Res. 78, 322–330. https://doi.org/10.1016/j.jsr.2021.07.001 (2021) (Epub 2021/08/18).
Rezapur-Shahkolai, F., Afshari, M., Moghimbeigi, A. & Hazavehei, S. M. M. Home-related injuries among under-five-year children and mothers’ care regarding injury prevention in rural areas. Int. J. Inj. Contr. Saf. Promot. 24(3), 354–362. https://doi.org/10.1080/17457300.2016.1200628 (2017) (Epub 2016/07/09).
Cao, B. L. et al. Effect of a multi-level education intervention model on knowledge and attitudes of accidental injuries in rural children in Zunyi, Southwest China. Int. J. Environ. Res. Public Health. 12(4), 3903–3914. https://doi.org/10.3390/ijerph120403903 (2015) (Epub 2015/04/10).
Forjuoh, S. N. & Li, G. A review of successful transport and home injury interventions to guide developing countries. Soc. Sci. Med. 43(11), 1551–1560. https://doi.org/10.1016/s0277-9536(96)00051-2 (1996) (Epub 1996/12/01).
Brito, M. A. et al. Risk factors in the domestic environment for falls in children under five years of age. Revista gaucha de enfermagem. 38(3), e2017–e2011. https://doi.org/10.1590/1983-1447.2017.03.2017-0001 (2017) (Epub2017/01/01).
Wiratama, B. et al. Evaluating the Effects of Holidays on Road Crash Injuries in the United Kingdom. Int. J. Environ. Res. Publis Health 18(1), 1. https://doi.org/10.3390/ijerph18010280 (2021).
Eyerly-Webb, S. et al. Impact of Holidays on Pediatric Trauma Admissions to a Community Hospital in South Florida. 112(3), 164–169. https://doi.org/10.14423/smj.0000000000000947 (2019).
Kong, F. et al. Trend of unintentional suffocation death for infants under 1 year of age from 2009 to 2018 in Hunan, China: a cross-sectional study. BMJ Open 10(12), e038666. https://doi.org/10.1136/bmjopen-2020-038666 (2020) (Epub 2020/12/10).
Acknowledgements
The authors wish to thank all staff working for the Under Five Child Mortality Surveillance System during 2015–2020.
Author information
Authors and Affiliations
Contributions
Conceptualization: H.W., J.F., X.Z. Data curation: J.H., X.Z., Z.X. Formal analysis: X.Z. Methodology: X.Z. Project administration: H.W., J.F. Supervision: H.W., J.F., Z.X., G.J. Visualization: X.Z. Writing—original draft preparation: X.Z. Writing—review and editing: H.W., H.L., J.X.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhou, X., Xie, Z., He, J. et al. Unintentional injury deaths among children under five in Hunan Province, China, 2015–2020. Sci Rep 13, 5530 (2023). https://doi.org/10.1038/s41598-023-32401-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-32401-1
- Springer Nature Limited