
Abstract
Although people all know that nicotine in tobacco smoke is the key to cause health damage, they ignore the synergistic effect of a large number of Volatile Organic Compounds (VOCs) produced by incomplete tobacco combustion on nicotine or cotinine metabolism. Our aim is to investigate the association between serum VOCs and cotinine in smokers infected with HIV, HBV or HCV. National Health and Nutrition Examination Survey (NHANES 2005–2018) database, including 13,652 nationally representative subjects’ sociodemographic characteristics and serological indicators, was used in this study. Smokers living with human immunodeficiency virus (HIV), hepatitis B virus (HBV) or hepatitis C virus (HCV) were compared to non-infected population. The correlation between VOCs and cotinine as well as the effects of VOCs on cotinine metabolism were analyzed by Spearman correlation analysis and multivariable logistic regression analysis, respectively. Among HIV, HBV, or HCV infected smokers with the largest exposure dose to tobacco, the intensity of the association between VOCs and cotinine was the strongest. The results of multivariable binary logistic regression showed that high concentrations of 1,2-Dichlorobenzene (OR:1.036, CI:1.009–1.124), Benzene (OR:1.478, CI:1.036–2.292), Carbon Tetrachloride (OR:1.576, CI:1.275–2.085) and 2,5-Dimethylfuran (OR:1.091, CI:1.030–1.157) in blood might be independent risk factors leading to the increase of serum metabolite cotinine in smokers.
Similar content being viewed by others


Introduction
Cotinine has been proved to be an exposure biomarker for monitoring tobacco use, which is most often determined in urine, serum and saliva, has longer half-life (16-h) than its precursor nicotine (2-h), and reflects the amount of smoking and metabolic status of the body1,2. The serum cotinine level increased in a dose-dependent manner with the increase of tobacco use or exposure3. A study showed that smokers exposed to the same amount of tobacco were more likely to become addicted if the body absorbed more nicotine, resulting in the decline of smokers' ability to quit smoking4. Exposure to nicotine, a precursor of cotinine in tobacco, could lead to green tobacco sickness and DNA damage5. Cotinine could also affect the reproductive function of men and women and increase the risk of cancer in offspring6.
Tobacco could produce a large number of toxic substances under incomplete combustion, and the most typical was VOCs7,8. Studies have shown that benzene was one of the carcinogenic and popular toxins in cigarette smoke, which belonged to VOCs and was related to smokers' leukemia9,10. One study measured the individual cotinine exposure of 72 smokers, and then calculated the benzene exposure. Compared with non-smokers, smokers have higher benzene exposure11. In addition, researchers also found other VOCs types in tobacco smoke, such as monoaromatic hydrocarbons (including ethylbenzene, toluene, styrene and xylene), and these might pose a certain risk to health12,13. Smoking, a social behavior, would lead to the absorption of nicotine and VOCs. At the same time, VOCs absorbed into the blood could inhibit the metabolism of cotinine by cytochrome P45014,15,16,17. It showed that when the body absorbed the above two at the same time, there could be a synergistic effect. Therefore, The quantitative measurement and joint analysis of VOCs and cotinine or nicotine are essential, because all of these toxins can circulate to important organs and tissues with the blood18.
Obviously, different VOCs have the same status of harm to human health, but the relationship between VOCs and cotinine is also indivisible, because their joint harm to health may be greater than that caused by them alone. For example, one study found that 2,5-dimethylfuran in VOCs could be used as a smoking monitoring biomarker comparable to cotinine19. In addition, Pauwels C's study pointed out the correlation between VOCs and cotinine, but did not show the one-way effect of VOCs on the metabolic level of cotinine20. Therefore, now it is urgent to use more representative samples to identify the synergistic effect of VOCs content in bleeding fluid on cotinine absorption and metabolism levels, because a few small sample studies only confirmed the correlation between them, rather than the causal relationship18,21. The key subjects we selected were smokers living with human immunodeficiency virus (HIV), hepatitis B virus (HBV) or hepatitis C virus (HCV), whose tobacco exposure was much higher than that of ordinary smokers, which was an effective and special place for us to solve this research question.
Generally speaking, the smoking rate of some patients with blood infectious diseases was often higher than that of the general population. According to a study report based on the United States integrated health system, people living with HIV were more likely to smoke and more vulnerable to the harmful effects of smoking than people without HIV22. Another study showed that hepatitis patients in the United States were mainly drug users, non-Hispanic blacks, the poor, people with low education and people with mental health disorders23. The typical feature of these groups was the high smoking rate24. Therefore, in this study, smokers living with HIV, HBV and HCV were studied as a group of high tobacco exposure people, in order to find out the more real association between serum VOCs and cotinine metabolism than the general smokers, compared with non-infected smokers.
Methods
Study sample selection
The materials used in this study were 14-year long-term follow-up survey data from Centers for Disease Control and Prevention (CDC) in the United States, which were a biennial survey conducted by the National Center for Health Statistics (NCHS). The 2005–2018 National Health and Nutrition Examination Survey (NHANES) data sets required for the analysis were downloaded from the NHANES website and combined using SAS software version 9.4. A total of 13,652 eligible subjects aged 21–59 was included in this study (Fig. 1). They had complete general sociodemographic information, as well as serological measurements that mainly included cotinine and VOCs.

Flow chart of research subjects selection.
HIV, HBV, and HCV diagnosis
The HIV-1 antibody status was determined by the blood test results of NHANES. According to the test results, the subjects were divided into two categories: HIV positive or HIV negative. The VITROS Hepatitis B surface antigen (HBsAg) test using by NHANES was used to determine the infection status of HBV, which was divided into HBV positive and HBV negative according to the test results. In addition, in vitro nucleic acid amplification test (COBAS AMPLICOR HCV MONITOR Test, version 2.0) was used to quantitatively determine HCV RNA in human serum or plasma to determine HCV infection status (HCV positive and HCV negative).
Measurement of exposure and outcome
Participants' blood VOCs concentrations were automatically analyzed by capillary gas chromatography (GC) and mass spectrometry (MS) combined with selective ion monitoring (SIM) detection and isotope dilution. Serum cotinine was determined by isotope dilution high performance liquid chromatography / atmospheric pressure chemical ionization tandem mass spectrometry (ID HPLC-APCI-MS / MS). Smoking status was assessed from one self-reported item in the questionnaire: “Have you ever smoked cigarettes?”25 Thus, it might be described as “Smoker: yes/no” (as indicated in Supplementary Table S1), including smokers who reported they smoked at least 100 cigarettes in their lifetime and non-smokers who reported they had not smoked 100 cigarettes in their lifetime26. It was worth emphasizing that cotinine was defined as an effective biomarker of smoking in this study, while VOCs blood indicators were exposure biomarkers of cigarettes. We used the median (0.14 ng/mL) of serum cotinine in 3114 smokers as the boundary to divide it into a binary dependent variable (‘ ≥ 0.14 ng/mL’ was defined as high cotinine group of smokers; ‘ < 0.03 ng/mL’ was defined as low cotinine group of smokers), and the measured values of VOCs were included in the follow-up analysis as continuous independent variables. Similarly, the median (0.02 ng/mL) of serum cotinine in 10,538 non-smokers was defined as the boundary between high cotinine group (≥ 0.02 ng/mL) and low cotinine group (< 0.02 ng/mL) of non-smokers.
Classification of confounders
Potential confounders in the relationship between VOCs and cotinine were selected for inclusion into multivariable logistic regression model. This study identified age, gender, race/ethnicity, education, family poverty index ratio (PIR), depression status, and substance use behavior. The sociodemographic variables included in this study were described in Supplementary Table S1. Only age (in years) was continuous variable, and the rest were classified variables.
Statistical analysis
Independent Samples t-test was used for continuous variables that obeyed normal distribution, while Nonparametric test (Mann–Whitney U test) was used for continuous variables that did not obey normal distribution. All categorical variables were tested by Chi-square test. The single factor correlation analysis results were presented through the heat map based on Spearman algorithm. Correlation coefficient greater than 0.6 was defined as a strong correlation. Multivariable logistic regression analysis, adjusted for all potential confounders, was performed to determine the final relationship between VOCs and cotinine and to identify the independent risk factors leading to the increase of cotinine among smokers living with HIV, HBV, or HCV (HIV|HBV|HCV). The variance inflation factor was used to diagnose the multicollinearity between independent variables in the regression model (the multivariable regression model established in this study did not have multicollinearity, and all VIF values were less than 10). Cohen’s criteria for gauging small, medium and large effect sizes of R2 were 0.2, 0.5 and 0.8, which were calculated from Cohen’s d values27. A two-tailed P value less than 0.05 was considered statistically significant.
Data processing, statistical analysis, and graphic drawing were carried out with SAS version 9.4 (SAS Institute Inc., Cary, NC), IBM SPSS version 22.0, and R version 4.0.2 (http://www.R-project.org, The R Foundation).
Institutional review board statement
Ethical review and approval were waived for this study, since all the data from NHANES is publicly accessible.
Informed consent
Informed consent from all subjects was obtained by NHANES.
Results
This study preliminarily compared the differences of sociodemographic variables, blood VOCs and cotinine between people living with HIV|HBV|HCV and those without HIV, HBV, and HCV (HIV&HBV&HCV). The sociological characteristics of the subjects and the test results of the differences of these blood indexes were shown in Supplementary Table S1. Compared with the HIV&HBV&HCV non-infected group, people living with HIV|HBV|HCV were more likely to be older (44.6 years vs 40.2 years, P < 0.001), males (67.4% vs 45.5%, P < 0.001), non-Hispanic Black (36.0% vs 19.3%, P < 0.001), lower educational level (45.0% vs 37.2%, P = 0.013), lower economic level (21.9% vs 15.7%, P = 0.010), depression (42.9% vs 32.9%, P = 0.009), drug users (60.3% vs 44.4%, P < 0.001), current smokers (44.6% vs 22.4%, P < 0.001). In addition, we also conducted a statistical test on the blood indexes between above two groups, and the results showed that the serum Cotinine (ng/mL), 1,2-Dichlorobenzene (ng/mL), Tetrachloroethene (ng/mL), Carbon Tetrachloride (ng/mL), Methylene Chloride (ng/mL), 1,1,1-Trichloroethane (ng/mL), and Nitrobenzene (ng/mL) were significantly (P < 0.05) higher in current smokers than in non-smokers.
In order to further find possible differential serum VOCs, which might be associated with cotinine, we subdivided HIV|HBV|HCV infected group and HIV&HBV&HCV non-infected group into the following four subgroups (Supplementary Table S2): (1) Smokers living with HBV| HCV|HIV; (2) Non-smokers living with HIV|HBV|HCV; (3) Smokers living without HIV&HBV&HCV; (4) Non-smokers living without HIV&HBV&HCV. The results showed that the content of cotinine in the blood of the four groups was significantly different, that is, there was a statistical difference between each two groups (“Smokers living with HIV| HBV|HCV” vs. “Non-smokers living with HIV|HBV|HCV”, P < 0.01; “Smokers living with HIV| HBV|HCV” vs. “Smokers living without HIV&HBV&HCV”, P < 0.01; “Smokers living with HIV| HBV|HCV” vs. “Non-smokers living without HIV&HBV&HCV”, P < 0.001; “Non-smokers living with HIV|HBV|HCV” vs. “Smokers living without HIV&HBV&HCV”, P < 0.05; “Non-smokers living with HIV|HBV|HCV” vs. “Non-smokers living without HIV&HBV&HCV”, P < 0.05; “Smokers living without HIV&HBV&HCV” vs. “Non-smokers living without HIV&HBV&HCV”, P < 0.001). Figure 2 visualized above differences of serum cotinine content between each two groups. The results demonstrated that smokers living with HIV|HBV|HCV had significantly higher serum cotinine level than non-smokers living with HIV|HBV|HCV, and that smokers living without HIV&HBV&HCV had also significantly higher serum cotinine level than non-smokers living without HIV&HBV&HCV. Most obviously, smokers living with HIV|HBV|HCV had the highest serum cotinine level among the four groups. In addition, Supplementary Table S2 showed that four differential blood VOCs indicators, including 1,2-Dichlorobenzene (ng/mL), Tetrachloroethene (ng/mL), Benzene (ng/mL), and 2,5-Dimethylfuran (ng/mL), had positive dose effects on serum cotinine level.

The distribution of serum cotinine levels in the different infection groups (***P < 0.001; **P < 0.01; *P < 0.05).
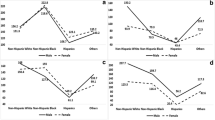
Subsequently, this study conducted Spearman correlation analysis on exploring the correlation between serum cotinine and VOCs among the above four groups. The results showed that the correlation heatmap between them was significantly different between different groups. From a macro perspective, the intensity and density of the correlation between blood indexes in the HIV|HBV|HCV infected group were higher than those in the HIV&HBV&HCV noninfected group. Compared to non-smokers living with HIV|HBV|HCV, the correlation between different blood indexes was more and stronger in smokers living with HIV|HBV|HCV. Compared to non-smokers living without HIV&HBV&HCV, the correlation between different blood indexes was more and stronger in smokers living without HIV&HBV&HCV. Specifically, there were 12 pairs of exclusively strong interaction items in smokers living with HBV|HCV|HIV (correlation coefficient greater than 0.6), including 1 pair of negative correlation indicators (correlation coefficient r = −0.83) and 12 pairs of positive correlation indicators (correlation coefficient fluctuation range is 0.81–0.92). All the above correlation coefficients mentioned were lower than the level of statistical significance (all P < 0.05), please see Fig. 3 for the details.

Spearman correlation analysis between serum VOCs and cotinine in different groups (a. Smokers living with HIV, HBV, or HCV; b. Non-smokers living with HIV, HBV, or HCV; c. Smokers living without HIV, HBV, and HCV; d. Non-smokers living without HIV, HBV, and HCV).
As for the association between serum VOCs and cotinine levels in 3114 smokers, multivariable binary logistic regression model, adjusting for age, gender, race/ethnicity, education, PIR, depression status, and drug use history, was conducted to identify potential associated VOCs of cotinine (Table 1). The results showed that 1,2-Dichlorobenzene, Benzene, Carbon Tetrachloride, 2,5-Dimethylfuran are all independent associated factors of cotinine. That was to say, high concentrations of 1,2-Dichlorobenzene (OR:1.036, CI:1.009–1.124), Benzene (OR:1.478, CI:1.036–2.292), Carbon Tetrachloride (OR:1.576, CI:1.275–2.085) and 2,5-Dimethylfuran (OR:1.091, CI:1.030–1.157) in blood might be independent risk factors leading to the increase of serum metabolite cotinine in smokers. Similarly, in 10,538 non-smokers, the results of the multivariable binary logistic regression model in Table 2 showed that high cotinine (≥ 0.02 ng/mL) group had higher levels of 1,2-Dichlorobenzene (OR:1.135, CI:1.079–1.193) and Carbon Tetrachloride (OR:1.493, CI:1.209–1.846), which might also be independent risk factors leading to the increase of serum metabolite cotinine in non-smokers.
Discussion
The harm of smoking to human health was well known, but few studies had mentioned the harmful effects of the synergistic factors (specifically VOCs in this study). Even though the studies of Pauwels C and others only studied the association between VOCs and smoking, they did not emphasize interactions or causal relationship between them20,28,29. Cotinine might be used as a biomarker of tobacco exposure for smokers because it was a main metabolite of nicotine (a compound whose concentration in the human body was produced in a high percentage by exposure to tobacco) and could be quantified in the body up to 72 h after the last cigarette30. However, Castellanos M believed that VOCs often accompanied by smoking were also the focus of studies, and could even be used as a biomarker of tobacco exposure19. It might be the reason that a large number of VOCs were produced in the process of smoking and competing with nicotine for cytochrome P450, which affected the metabolic efficiency of nicotine in the body, leading to smokers' addiction to tobacco and difficulty in quitting smoking31,32.
In this study, all subjects were divided into different groups (“People living with HBV, HCV, or HIV” and “People living without HBV, HCV, and HIV”), and the results showed that serum cotinine of smokers living with HBV, HCV, or HIV was the highest (Supplementary Table S1 and Fig. 2). In addition, we also found that all infected people had more and more dangerous sociological characteristics than non-infected people, which could explain that the distribution level of cotinine was actually affected by different socio-demographic characteristics. For example, compared with the HIV&HBV&HCV non-infected group, people living with HIV|HBV|HCV were more likely to be older, males, non-Hispanic Black, lower educational level, lower economic level, depression, drug users, current smokers. Consistently, one study also suggested that age, gender and race might affect the metabolism of nicotine and cotinine33. Therefore, this study adjusted above potential confounding factors, so as to obtain more accurate and reliable analysis results.
We also found a strong correlation between serum cotinine and eight VOCs (1,2-Dichlorobenzene, 1,2-Dichloroethane, Chlorobenzene, Carbon Tetrachloride, Methylene Chloride, Trichloroethene, 1,1,1-Trichloroethane, Nitrobenzene) in smokers infected with HIV|HBV|HCV. Studies showed that the smoking rate and tobacco exposure dose of this population were much higher than that of the general population22,23,34,35, so there were higher concentrations of cotinine and VOCs in the serum. Since the tobacco exposure of smokers infected with HIV|HBV|HCV was much higher than that of the general population, it could be inferred that the harm of serum cotinine and VOCs in the population would increase with the increase of tobacco exposure level. Our study also indicated a more obvious relationship between serum cotinine and VOCs in the population exposed to higher exposure of tobacco than lower the figure for tobacco. Therefore, we speculated that there might be a similar regularity in the non-infected population with the same unhealthy behavior (especially smoking in this study). In addition, there could be a possibility that the smoking cessation measures applied to the smokers of infected persons might also be extended to the non-infected smokers, which might indirectly provide new ideas for solving the public health problem of smoking. However, it requires more prospective multicenter cohort studies to prove whether this is possible in the future.
Our research also had some limitations. First of all, although the smokers among HIV|HBV|HCV infected people whose smoking rate was higher than that of the general population were integrated into the analysis, the sample size was still small. However, our study was consistent with other research results. For example, there was a significant positive correlation between serum cotinine and VOCs among smokers18. Secondly, the clear causal relationship between serum VOCs and cotinine needs to be further explored, because our study only found that the association between them in the body, and the relevant mechanism of serum cotinine level co-affecting by the external environment or other biochemical factors in the body might be more complicated than we expected. Finally, although NHANES had accurately measured the internal exposure dose of smoking, that exposure dose was far lower than the external exposure dose of subjects, so the existing data results might be underestimated.
Conclusions
Among smokers living with HIV|HBV|HCV, the serum cotinine was the highest, and the association between serum VOCs and cotinine was also very significant. Therefore, there might be a dose–response relationship between the impact intensity of four VOCs (such as 1,2-Dichlorobenzene, Benzene, Carbon Tetrachloride, 2,5-Dimethylfuran) on serum cotinine metabolism, that is, the higher the tobacco exposure, the stronger the impact intensity. In addition, this study used molecular epidemiology to indirectly provide new ideas and perspectives on smoking hazards for smokers.
Data availability
Data described in the manuscript, codebook, and analytic code will not be made available because the data used in this study were from the NHANES database, which is a free and open database for all researchers around the world. The link to the database is https://wwwn.cdc.gov/nchs/nhanes/Default.aspx.
References
Benowitz, N. L., Bernert, J. T., Caraballo, R. S., Holiday, D. B. & Wang, J. Optimal serum cotinine levels for distinguishing cigarette smokers and nonsmokers within different racial/ethnic groups in the United States between 1999 and 2004. Am. J. Epidemiol. 169, 236–248. https://doi.org/10.1093/aje/kwn301 (2009).
Benowitz, N. L. et al. Urine nicotine metabolite concentrations in relation to plasma cotinine during low-level nicotine exposure. Nicotine Tob. Res. 11, 954–960. https://doi.org/10.1093/ntr/ntp092 (2009).
Lawson, G. M. et al. Application of serum nicotine and plasma cotinine concentrations to assessment of nicotine replacement in light, moderate, and heavy smokers undergoing transdermal therapy. J. Clin. Pharmacol. 38, 502–509. https://doi.org/10.1002/j.1552-4604.1998.tb05787.x (1998).
Jain, R. B. Trends in serum cotinine concentrations among daily cigarette smokers: data from NHANES 1999–2010. Sci. Total Environ. 472, 72–77. https://doi.org/10.1016/j.scitotenv.2013.11.002 (2014).
Alves, J. et al. Impact of nicotine-induced green tobacco sickness on DNA damage and the relation with symptoms and alterations of redox status in tobacco farmers. Ecotoxicol. Environ. Saf. 206, 111397. https://doi.org/10.1016/j.ecoenv.2020.111397 (2020).
Zenzes, M. T. Smoking and reproduction: gene damage to human gametes and embryos. Hum. Reprod. Update 6, 122–131. https://doi.org/10.1093/humupd/6.2.122 (2000).
Bi, X., Sheng, G., Feng, Y., Fu, J. & Xie, J. Gas- and particulate-phase specific tracer and toxic organic compounds in environmental tobacco smoke. Chemosphere 61, 1512–1522. https://doi.org/10.1016/j.chemosphere.2005.04.057 (2005).
Pandey, S. K. & Kim, K. H. Determination of hazardous VOCs and nicotine released from mainstream smoke by the combination of the SPME and GC-MS methods. ScientificWorldJournal 10, 1318–1329. https://doi.org/10.1100/tsw.2010.127 (2010).
Mitacek, E. J. et al. Rising leukemia rates in Thailand: The possible role of benzene and related compounds in cigarette smoke. Oncol. Rep. 9, 1399–1403 (2002).
Korte, J. E., Hertz-Picciotto, I., Schulz, M. R., Ball, L. M. & Duell, E. J. The contribution of benzene to smoking-induced leukemia. Environ. Health Perspect. 108, 333–339. https://doi.org/10.1289/ehp.00108333 (2000).
Schettgen, T., Ochsmann, E., Alt, A. & Kraus, T. A biomarker approach to estimate the daily intake of benzene in non-smoking and smoking individuals in Germany. J. Expo Sci. Environ. Epidemiol. 20, 427–433. https://doi.org/10.1038/jes.2009.32 (2010).
Maltoni, C., Conti, B., Cotti, G. & Belpoggi, F. Experimental studies on benzene carcinogenicity at the Bologna Institute of Oncology: Current results and ongoing research. Am. J. Ind. Med. 7, 415–446. https://doi.org/10.1002/ajim.4700070508 (1985).
Xu, X. et al. Association between exposure to alkylbenzenes and cardiovascular disease among National Health and Nutrition Examination Survey (NHANES) participants. Int. J. Occup. Environ. Health 15, 385–391. https://doi.org/10.1179/oeh.2009.15.4.385 (2009).
Kondrová, E., Stopka, P. & Soucek, P. Cytochrome P450 destruction by benzene metabolites 1,4-benzoquinone and 1,4-hydroquinone and the formation of hydroxyl radicals in minipig liver microsomes. Toxicol. In Vitro 21, 566–575. https://doi.org/10.1016/j.tiv.2006.11.002 (2007).
Soucek, P., Filipcova, B. & Gut, I. Cytochrome P450 destruction and radical scavenging by benzene and its metabolites. Evidence for the key role of quinones. Biochem. Pharmacol. 47, 2233–2242. https://doi.org/10.1016/0006-2952(94)90261-5 (1994).
James, C. A., Xin, G., Doty, S. L. & Strand, S. E. Degradation of low molecular weight volatile organic compounds by plants genetically modified with mammalian cytochrome P450 2E1. Environ. Sci. Technol. 42, 289–293. https://doi.org/10.1021/es071197z (2008).
Zhang, L., Routsong, R. & Strand, S. E. Greatly enhanced removal of volatile organic carcinogens by a genetically modified houseplant, Pothos Ivy (Epipremnum aureum) expressing the mammalian cytochrome P450 2e1 gene. Environ. Sci. Technol. 53, 325–331. https://doi.org/10.1021/acs.est.8b04811 (2019).
Chambers, D. M., Ocariz, J. M., McGuirk, M. F. & Blount, B. C. Impact of cigarette smoking on volatile organic compound (VOC) blood levels in the U.S. population: NHANES 2003–2004. Environ. Int. 37, 1321–1328. https://doi.org/10.1016/j.envint.2011.05.016 (2011).
Castellanos, M., Suñer, R., Fernández-Real, J. M. & Sanchez, J. M. 2,5-Dimethylfuran as a validated biomarker of smoking status. Nicotine Tob. Res. 21, 828–834. https://doi.org/10.1093/ntr/nty078 (2019).
Pauwels, C. et al. Smoking regular and low-nicotine cigarettes results in comparable levels of volatile organic compounds in blood and exhaled breath. J. Breath Res. 15, 016010. https://doi.org/10.1088/1752-7163/abbf38 (2020).
Keith, R. J. et al. Characterization of volatile organic compound metabolites in cigarette smokers, electronic nicotine device users, dual users, and nonusers of tobacco. Nicotine Tob. Res. 22, 264–272. https://doi.org/10.1093/ntr/ntz021 (2020).
Lam, J. O. et al. Smoking and cessation treatment among persons with and without HIV in a U.S. integrated health system. Drug Alcohol Depend. 213, 108128. https://doi.org/10.1016/j.drugalcdep.2020.108128 (2020).
Kim, R. S. et al. Cigarette smoking in persons living with Hepatitis C: The National Health and Nutrition Examination Survey (NHANES), 1999–2014. Am. J. Med. 131, 669–675. https://doi.org/10.1016/j.amjmed.2018.01.011 (2018).
Greene, S. K., Levin-Rector, A., Hadler, J. L. & Fine, A. D. Disparities in reportable communicable disease incidence by census tract-level poverty, New York City, 2006–2013. Am. J. Public Health 105, e27-34. https://doi.org/10.2105/ajph.2015.302741 (2015).
Asfar, T. et al. National estimates of prevalence, time-trend, and correlates of smoking in US people living with HIV (NHANES 1999–2016). Nicotine Tob. Res. 23, 1308–1317. https://doi.org/10.1093/ntr/ntaa277 (2021).
Kravietz, A., Angara, P., Le, M. & Sargi, Z. Disparities in screening for head and neck cancer: Evidence from the NHANES, 2011–2014. Otolaryngol. Head Neck Surg. 159, 683–691. https://doi.org/10.1177/0194599818773074 (2018).
Gülkesen, K. H., Bora, F., Ilhanli, N., Avsar, E. & Zayim, N. Cohen’s d and physicians’ opinion on effect size: A questionnaire on anemia treatment. J. Investig. Med. 70, 814–819. https://doi.org/10.1136/jim-2021-002031 (2022).
St Helen, G. et al. Nicotine and carcinogen exposure after water pipe smoking in hookah bars. Cancer Epidemiol. Biomark. Prev. 23, 1055–1066. https://doi.org/10.1158/1055-9965.Epi-13-0939 (2014).
Vardoulakis, S. et al. Indoor exposure to selected air pollutants in the home environment: A systematic review. Int. J. Environ. Res. Public Health 17, 8972. https://doi.org/10.3390/ijerph17238972 (2020).
Ahijevych, K. L., Tyndale, R. F., Dhatt, R. K., Weed, H. G. & Browning, K. K. Factors influencing cotinine half-life during smoking abstinence in African American and Caucasian women. Nicotine Tob. Res. 4, 423–431. https://doi.org/10.1080/1462220021000018452 (2002).
Pohl, H. R. & Scinicariello, F. The impact of CYP2E1 genetic variability on risk assessment of VOC mixtures. Regul. Toxicol. Pharmacol. 59, 364–374. https://doi.org/10.1016/j.yrtph.2011.01.013 (2011).
Waller, C. L., Evans, M. V. & McKinney, J. D. Modeling the cytochrome P450-mediated metabolism of chlorinated volatile organic compounds. Drug Metab. Dispos. 24, 203–210 (1996).
Ware, L. J. et al. Assessing tobacco use in an African population: Serum and urine cotinine cut-offs from South Africa. Drug Alcohol Depend. 195, 82–89. https://doi.org/10.1016/j.drugalcdep.2018.11.022 (2019).
Giles, M. L., Gartner, C. & Boyd, M. A. Smoking and HIV: what are the risks and what harm reduction strategies do we have at our disposal?. AIDS Res. Ther. 15, 26. https://doi.org/10.1186/s12981-018-0213-z (2018).
Vaughan Watson, C., Naik, S., Lewin, M., Ragin-Wilson, A. & Irvin-Barnwell, E. Associations between select blood VOCs and hematological measures in NHANES 2005–2010. J. Expo Sci. Environ. Epidemiol. 31, 366–376. https://doi.org/10.1038/s41370-019-0192-8 (2021).
Acknowledgements
We thank the director of Major Infectious Diseases Management Department and the leaders of the Public Health Clinical Center of Chengdu for their full support during the implementation of the project.
Funding
The research received the support of public health clinical center of chengdu. The findings and conclusions expressed in this article were the authors’ and do not necessarily represent the official position of the CDC or the U.S. Department of Health and Human Services. There was no private sponsor who played any role in the decision to design the study, collect data, analyze or interpret data, write reports, or submit manuscripts.
Author information
Authors and Affiliations
Contributions
The authors’ responsibilities were as follows—Jie Yang, Lei Peng, Hao Zhang, Jin-Long Lin: contributed to data collection, analysis, and manuscript writing; Lei Peng, Xiao-Wen Jiang, Jing Liu: devoted to research design and implementation. All authors declare that they have read and approved the manuscript and final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yang, J., Zhang, H., Lin, JL. et al. Association between serum cotinine and volatile organic compounds (VOCs) in adults living with HIV, HBV, or HCV (NHANES 2005–2018). Sci Rep 12, 21769 (2022). https://doi.org/10.1038/s41598-022-26420-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-26420-7
- Springer Nature Limited