
Abstract
Musculoskeletal disorders (MSDs) are highly prevalent, burdensome, and putatively associated with an altered human resting muscle tone (HRMT). Osteopathic manipulative treatment (OMT) is commonly and effectively applied to treat MSDs and reputedly influences the HRMT. Arguably, OMT may modulate alterations in HRMT underlying MSDs. However, there is sparse evidence even for the effect of OMT on HRMT in healthy subjects. A 3 × 3 factorial randomised trial was performed to investigate the effect of myofascial release (MRT), muscle energy (MET), and soft tissue techniques (STT) on the HRMT of the corrugator supercilii (CS), superficial masseter (SM), and upper trapezius muscles (UT) in healthy subjects in Hamburg, Germany. Participants were randomised into three groups (1:1:1 allocation ratio) receiving treatment, according to different muscle-technique pairings, over the course of three sessions with one-week washout periods. We assessed the effect of osteopathic techniques on muscle tone (F), biomechanical (S, D), and viscoelastic properties (R, C) from baseline to follow-up (primary objective) and tested if specific muscle-technique pairs modulate the effect pre- to post-intervention (secondary objective) using the MyotonPRO (at rest). Ancillary, we investigate if these putative effects may differ between the sexes. Data were analysed using descriptive (mean, standard deviation, and quantiles) and inductive statistics (Bayesian ANOVA). 59 healthy participants were randomised into three groups and two subjects dropped out from one group (n = 20; n = 20; n = 19–2). The CS produced frequent measurement errors and was excluded from analysis. OMT significantly changed F (−0.163 [0.060]; p = 0.008), S (−3.060 [1.563]; p = 0.048), R (0.594 [0.141]; p < 0.001), and C (0.038 [0.017]; p = 0.028) but not D (0.011 [0.017]; p = 0.527). The effect was not significantly modulated by muscle-technique pairings (p > 0.05). Subgroup analysis revealed a significant sex-specific difference for F from baseline to follow-up. No adverse events were reported. OMT modified the HRMT in healthy subjects which may inform future research on MSDs. In detail, MRT, MET, and STT reduced the muscle tone (F), decreased biomechanical (S not D), and increased viscoelastic properties (R and C) of the SM and UT (CS was not measurable). However, the effect on HRMT was not modulated by muscle–technique interaction and showed sex-specific differences only for F.
Trial registration German Clinical Trial Register (DRKS00020393).
Similar content being viewed by others

Introduction
Globally, musculoskeletal disorders (MSDs) accounted for ~ 1.3 billion prevalent and ~ 334.7 million incident cases in 20171. Notably, most of the prevalence and incidence are attributable to gout, rheumatoid arthritis, osteoarthritis, neck pain (NP), and low back pain (LBP)2,3. In 2017, MSDs were the main contributor to global disability and LBP was the leading cause of disability since 19904. Similarly, the global costs of MSDs due to health expenditure and production loss are reported to be immense5. However, these high health costs mismatch with low research investments6, and policy responses are thus required to close the gap7. Hence, MSDs are highly prevalent, burdensome, and costly.
Manual therapy seems to benefit patients with MSDs but is merely endorsed as an adjuvant treatment8 due to limited high-quality evidence9. Still, among the non-surgical and non-pharmacological interventions preferred by patients with LBP10,11, manual therapy provides the best evidence for an immediate-term reduction of pain and disability12. Thus, patients with MSDs may consult an osteopath in primary care (depending on varying country regulations and professional recognitions across the world)9,13.
Osteopathy is a person-centered approach to healthcare13 deploying both manual and patient management approaches (ranging from touch and manipulation to psychological support and lifestyle advice)14. Manual findings are treated using osteopathic manipulative treatment (OMT)15, which is primarily, but not exclusively, applied to treat MSDs like back pain conditions16,17. To date, there is promising evidence that OMT could be an effective and safe treatment for patients with MSDs18, particularly for improving pain and function in patients with spinal complaints19 like NP20 and LBP21,22,23,24. Hence, OMT was recommended for patients with LBP15,25 and was even reported to be dominant and cost-effective compared to usual care in the management of LBP and NP, respectively26. Still, the current body of evidence lacks robustness due to methodological shortfalls and counterevidence is available as well27,28,29.
MSDs and OMT are complex health conditions and interventions, respectively. Both are underpinned by poorly understood mechanisms30,31 and are associated with various biological, psychological, and social factors32,33. Another commonality is that MSDs34,35 and OMT36,37,38,39 are reputed to be associated with changes in muscle tone. On the one hand, alterations in lumbar myofascial tone and stiffness seem to contribute to the development and symptoms of LBP34,35,40. On the other hand, OMT may alter muscle tone and stiffness in patients with MSDs36,37,38,39. Hence, we hypothesise that a putative mechanism of action underpinning the treatment of MSDs with OMT might be the modulation of muscle tone.
However, not every technique and muscle may be relevant in the context of MSDs. On the one hand, manual techniques should be assessed that were shown to improve pain and function in patients with MSDs (e.g., LBP), which includes myofascial release techniques (MRT), muscle energy techniques (MET), and soft tissue techniques (STT)41,42,43,44,45,46,47,48,49. On the other hand, muscles should be tested that have demonstrated elevated muscle stiffness (or hyperactivity) in patients with MSDs (e.g., NP, temporomandibular disorder, and tension-type headache, but also migraine headaches), which includes the corrugator supercilii muscles (CS), superficial masseter muscles (SM), and upper trapezius muscles (UT)50,51.
Muscle tone is defined as the resting tension of the tissue in response to stretch, which comprises active (i.e., electrical activity within muscle cells) and passive muscle tone (intrinsic biomechanical and viscoelastic properties of the muscle)35,52. Moreover, the human resting muscle tone (HRMT) describes the resting tension of the whole myofascial continuum (a biotensegrity system that includes muscle and connective tissues)53. Although not conclusively determined54, the HRMT may arise due to slowly cycling cross-bridges between myosin heads and actin filaments40,53,55.
Previous work suggested that palpable muscle tension in patients with MSDs may reflect alterations of the HRMT53. Nonetheless, earlier studies on the effect of osteopathic interventions on muscle tone relied on palpation and electromyography (EMG) as measures56,57,58. However, manual palpation is reported to be unreliable59,60,61,62,63,64,65,66 and EMG is not informative of the HRMT53. Instead, an objective and reliable myotonometer should be used to assess the HRMT34,54. This includes the MyotonPRO, which induces oscillations in the muscle fibres as a means of quantifying biomechanical and viscoelastic muscle properties34,35,67. More precisely, it measures muscle tone (F [oscillation frequency]), stiffness (S [dynamic stiffness]), decrement (D [logarithmic decrement]), relaxation (R [mechanical stress relaxation time]), and creep (C [ratio of deformation and relaxation time])68.
Manual therapists commonly argue that treatment reduces tension and increases elasticity in muscles at rest. We hypothesize that these palpable changes may reflect a decrease in muscle tone, stiffness, and decrement as well as an increase in muscle relaxation and creep as measured with the MyotonPRO. Notably, the myometric parameter decrement (D) is inversely proportional to the muscle’s elasticity (if decrement decreases, elasticity increases)69. Further, we speculated that the putative effects may differ depending on which type of manual technique (e.g., MRT, MET, STT) is applied to which kind of muscle (e.g., CS, SM, UT). For example, practical experience suggests that low-pressure techniques might be preferred for smaller and thinner muscles, whereas high-pressure techniques may be favoured for larger and thicker muscles. Another factor to consider is that changes in muscle properties probably differ between sexes (although the effect seems to vary depending on the treated muscles and measured parameters)70,71,72,73,74,75.
Hence, in this study, we aimed to assess the effect of (OMT-related) manual techniques with different characteristics (MRT, MET, and STT) on (HRMT-related) muscle tone and biomechanical and viscoelastic muscle properties (F, S, D, R, and C) of (MSD-related) muscles with different sizes and thicknesses (CS, SM, and UT) in healthy subjects.
Objectives
The primary objective was to evaluate the effect of MRT, MET, and STT on the HRMT (expressed by myometric parameters: F, S, D, R, and C) of the CS, SM, and UT. The effect was measured for all groups from baseline to follow-up using the MyotonPRO. We hypothesized that MRT, MET, and STT decrease F, S, and D (inverse of elasticity), and increase R and C.
The secondary objective was to evaluate if specific techniques (MRT, MET, and STT) are more effective for modulating the HRMT (expressed by myometric parameters: F, S, D, R, and C) of specific muscles (CS, SM, and UT). The effect was measured for each group from pre- to post-intervention using the MyotonPRO. We hypothesized that the predicted changes in muscle properties are preferentially achieved through MRT for the CS, MET for the SM, and STT for the UT.
The ancillary objective was to analyse if the putative effects assessed in the primary and secondary objectives differ between the sexes.
Methods
Trial design
This single-blinded 3 × 3 factorial randomised trial was conducted in Hamburg, Germany. No changes to the methods were made after trial commencement. The study is largely reported according to the Consolidated Standards of Reporting Trials (CONSORT) statement76,77 since there are currently no specific guidelines available for randomised trials using a factorial design78.
Trial procedure
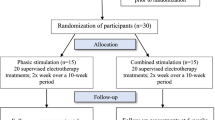
Demographic data was collected one month prior to the trial (t0). Participants were randomly allocated into three groups (G1, G2, and G3) undergoing three treatment sessions (t1-t3). The trial comprised one-week washout periods between each of the sessions. A session consisted of one intervention day (lasting from approximately 9 am to 4 pm), which encompassed 5 min of measurement, followed by 5 min of treatment, and renewed 5 min of measurement per subject. Baseline and follow-up refer to the first (pre-intervention) measurement at t1 and the last (post-intervention) measurement at t3, respectively.
Data were collected before and after treatment (pre- and post-intervention) in each of the three sessions. Overall, each group was measured six times. Participants started with 5 min delay to one another to allow measurement by one assessor who was not involved with the interventions. All interventions and measurements were applied (1) to the right side of the participant’s body to ensure comparability, and (2) in relaxed supine position to maintain resting muscle state. In this trial, all groups were intervention groups that were treated at one muscle per session, while all three muscles were measured. Thus, measures from untreated muscles were used as control values (Table 1). For example, in session 1, G1 was treated (and measured) at the UT, whereas the UT was not treated (but measured) in G2 or G3. Thus, G2 and G3 provided the UT control values for G1. In other words, the control values for the treated muscle in each group were generated by the untreated muscles in the other two groups.
During each session, each group received treatment with the same osteopathic technique but applied by another practitioner to another muscle. Over the course of the trial, all three groups were treated (1) with all three osteopathic techniques (MRT, MET, and SST); (2) at all three muscles (CS, SM, and UT); and (3) by all three practitioners (P1, P2, P3). However, the muscle-technique-practitioner combination was distinct for each group during each session (Table 1).
Participants
Undergraduate osteopathy students were recruited from the Osteopathie Schule Deutschland in Hamburg, Germany. The sample was limited to healthy subjects from this specific setting. The eligibility criteria were specified to include participants between 18 and 50 years old and exclude participants with health complaints (particularly muscle disorders) to minimise the risk of age-71,79 and disease-related80 changes of the musculature.
Interventions
Three manual techniques from the osteopathic field (MRT, MET, and STT)81 were selected and administered for ~ 5 min. These osteopathic techniques were adjusted to fit the structure and function of each muscle and were applied with the aim of modifying the HRMT in healthy participants. However, it is notable that the mechanisms of action underpinning these manual techniques are not fully understood but may involve diverse (neuro-)biological processes46,49,82,84,85,86,87,88,89,90,90. The interventions were performed by three osteopaths (1:2 female to male ratio), who showed similar characteristics in terms of age (24.28 [0.20] years) and practice experience (4.83 [0.29] years). A consensus training comprising three sessions of one hour (sixty minutes per technique) was implemented prior to the trial to ensure that all therapists applied the interventions coherently. During the first session, MRT was applied to the right CS (G3), SM (G2), and UT (G1). During the second session, MET was applied to the right CS (G2), SM (G1), and UT (G3). During the third session, STT was applied to the right CS (G1), SM (G3), and UT (G2) (Table 1). Overall, the interventions were chosen to represent the broad range of osteopathic techniques and their diverse characteristics (Box 1), whereas the muscles were chosen due to their apparent differences in size and thickness (Box 2).
Myofascial Release Technique (MRT)
MRT is an indirect (or direct) and passive technique where pressure and stretch with low load and long duration (which are adjusted based on palpatory feedback) is applied to release myofascial tissues41,42. The muscle is palpated (covering origin and insertion) and guided alongside the path of least resistance into a position of ease98, thereby following the tissues’ micro–movements away from the restricted barrier until a release occurs (Fig. 1).
Muscle Energy Technique (MET)
MET is a direct and active technique where the patient is instructed to voluntarily contract muscles into a controlled direction against the therapist counter-pressure99. In detail, the therapist brings the muscle into a position of stretch and holds it at the restriction barrier. The participant then performs an isometric contraction of the muscle (with 25% of maximum effort/force) away from this restricted barrier and against the therapist’s counterforce100. After approximately 3–6 s of contraction, the participant relaxes, and the therapist adjusts the tissue towards its renewed movement/restriction barrier. This post–isometric relaxation approach is repeated 3–6 times (Fig. 1).
Soft Tissue Technique (STT)
STT is a direct and passive technique where stretch, traction and/or deep pressure is applied to soft tissues81. Herein, the therapist uses repeated, slow, high and deep pressure gliding strokes applied with the thumb alongside the muscle fibres (which is similar to muscle stripping massage101,96,103) of the CS (from origin towards insertion), SM (from origin towards insertion), and UT (from insertion towards origin). This approach is similar to the treatment of a trigger band according to the fascial distortion model104 but is applied to palpably firm muscle fibres and their fascial surroundings (Fig. 1).

Osteopathic techniques; Legend: red arrows = therapists’ motion; black arrows = participants’ motion; four-headed arrows = motion applied in all directions; Abbreviations: MRT = myofascial release technique; MET = muscle energy technique; STT = soft tissue technique; UT = upper trapezius muscle; SM = superficial masseter muscle; CS = corrugator supercilii muscle.
Outcomes
We used the handheld digital palpation device MyotonPRO [Version 5.0.0] as the outcome measure (Fig. 2). This myotonometer assesses the muscle’s tone, biomechanical and viscoelastic properties using five parameters by means of dynamic oscillation mechanosignals54,68 (Table 2). The MyotonPRO is a valid and reliable measurement tool for healthy and diseased participants105,106 (Box 3) that has been applied to evaluate muscle tone, muscle stiffness, and HRMT in multiple studies investigating various structures and conditions34,54,67,107,109,109. The myotonometer measurements were carried out at all three sessions (t1-t3) before and after the treatment intervention. Measurement points (MPs) were predefined for the myotonometer measurements of each muscle prior to the trial (Box 4). MPs were identified by manual palpation following anatomical landmarks and marked before each session using a dermatological skin marker pen.

MyotonPRO; Legend: MyotonPRO and application for the CS, SM, and UT (from left to right).
Sample size
The sample size was calculated prospectively using G*Power, which is a power analysis for ANOVA with repeated measures (within-between interaction)118,119. We assumed a type I error level of 0.05 and statistical power of 95%. Based on an estimated partial η2 of 0.1 (unpublished data), an effect size of 0.33, and three measurements and four groups, a total sample size of 52 participants was calculated. Using an estimated drop-out rate of 15%, the sample size was planned with 60 participants.
Randomisation
The sample was randomly allocated into three groups (G1, G2, G3) by block randomization (1:1:1 allocation ratio) using computer-generated allocation schedule (http://www.randomization.com). Furthermore, we randomly assigned which technique would be applied in which session by throwing the dice. Afterwards, we randomly assigned the muscles and therapists to the groups and session in the same manner. The principal investigator generated the random allocation sequence, enrolled participants, and assigned them to sequences of intervention while having no clinical involvement in the trial. Treatments were scheduled according to allocation sequence and therapists and participants were first introduced to each other during the respective sessions.
Blinding
Participants and statisticians, but not therapists and assessors, were blinded to the conditions. However, we assume that blinding was compromised because the participants were osteopathy students that were likely able to distinguish between the interventions.
Statistical methods
The outcomes from myotonometer measurements were assessed by calculating the within-participant difference of each parameter for all groups between t1 and t3 (primary objective) and the between-participant difference of each parameter for each group between pre- and post-treatment of each session (secondary objective). Statistical analysis was conducted by employing the software R Studio. Myotonometer properties (F, S, D, R, and C) were used as parameters and converted into factors. To control for intergroup comparability, myotonometer properties were tested between groups before the interventions using a one-way ANOVA. There were no outliers in the data. The variables were normally distributed as determined by the Shapiro–Wilk test (p > 0.05). Homogeneity of error variances between groups was met for all these variables according to Levene’s test (p > 0.05). The descriptive statistic for the primary objective was presented by mean, standard deviation, and quantiles, whereas the secondary objective was presented by standard deviation and quantiles. Due to the limitations of standard repeated measures ANOVA for categorical variables and unbalanced data, the inductive statistics for the primary and secondary objectives as well as subgroup analysis were calculated using the Bayesian version of the repeated-measures analysis of variance (BANOVA)120. Post hoc analysis was interpreted using simple effects. Heidelberger & Welch’s diagnostic was used to run length diagnostic and convergence diagnostic. The p-values of the multiple comparisons were adjusted using the Bayesian model121. The significance level was set to 5% (p ≤ 0.05). Missing completely at random values were included for further analysis. Missing at random and missing not at random values were excluded as they are dependent on one factor and bias the results122.
Ethics approval and consent to participate
This study has obtained informed consent from participants, was carried out in accordance with the Declaration of Helsinki123 and was approved by the ethics committee of the Osteopathic Research Institute (Nr. 020–01). Written informed consent for publication of the images was obtained from the subjects.
Results
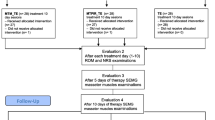
Overall, 82 participants were screened and 23 declined to participate or had scheduling issues. The remaining 59 participants were randomly allocated into groups, leading to a sample of 20 participants for groups G1 and G2, and 19 participants for the G3 group. Two participants from group G3 cancelled their participation in the study due to personal reasons and were excluded from interventions and analysis prior to the first session. Therefore, the first trial session started with the final sample size (n = 57) distributed across groups as follows: G1 (n = 20), G2 (n = 20), and G3 (n = 17). Unfortunately, some participants missed scheduled appointments and thereby allocated interventions and measurements. These participants were not excluded from study participation and data was included for analysis unless all three sessions were missed, which did not occur. In detail, appointments were missed during the: (1) first session by two participants from group G1 and one participant from group G2; (2) second session by three participants from group G3; and (3) third session by five participants from group G1, two participants from group G2, and two participants from group G3 (Fig. 3).

Participant flow chart; Legend: Not applicable.
Recruitment
Participants were recruited, provided written informed consent, and reported demographic data in December 2019 (t0). The trial was implemented over the course of one month between January and February 2020 (t1−3).
Demographic data
Demographics were recorded and included sex, handedness, age, and body mass index (BMI). The sample was predominantly female (68%), right-handed (91%), young (22.7 ± 4.5 years), and of normal weight (22.0 ± 2.5 BMI) (Table 3).
Numbers analysed
The data were examined for availability and normality to rule out statistical errors during analysis. Overall, 8.9% of the collected data did not correspond to the confidence interval of the MyotonPRO (set to 90%) and was thus not available for analysis. All missing values arose from measurements of the CS, demonstrating that the data was not missing at random. The CS was consequently excluded from analysis because correct coefficient estimation was not guaranteed. After exclusion, data from 104 treatments (54 for SM and 50 for UT) were included for analysis (104 of 156 measures).
Outcomes
Here, full outcome data are reported (Table 4). Subsequently, results will be presented (excluding the CS) according to the primary and secondary objectives.
Effect of osteopathic techniques on muscle tone and biomechanical and viscoelastic properties
No significant group differences were determined by the one-way ANOVA before treatment in F (F[2,308] = 0.61; p = 0.545), S (F[2,308] = 0.94; p = 0.390), D (F[2,308] = 0.79; p = 0.454), R (F[2,308] = 1.15; p = 0.319), and C (F[2,308] = 1.63; p = 0.198). The outcomes for the primary objective were assessed by means of the standardized mean difference. The data passed all of Heidelberger's and Welch's convergence diagnoses and showed that: F (−0.163 [0.060]; p = 0.008), S (−3.060 [1.563]; p = 0.048), R (0.594 [0.141]; p < 0.001), and C (0.038 [0.017]; p = 0.028) changed significantly, while D (0.011 [0.017]; p = 0.527) did not change significantly (Table 5). In other words, muscle tone (F [p = 0.008]) and biomechanical properties (S [p = 0.048] not D [p = 0.527]) decreased, while the viscoelastic properties (R [p < 0.001] and C [p = 0.028]) increased. Subgroup analysis for sex-specific changes revealed a significant interaction for F (−0.192 [0.089]; p = 0.030), but not for S (0.008 [0.0125]; p = 0.510), D (0.008 [0.013]; p = 0.555), R (−0.423 [0.218]; p = 0.057), and C (−0.019 [0.015]; p = 0.237). Due to the significant interaction, simple effects were interpreted for sex-specific differences in muscle property changes from baseline to follow-up (Table 5).
Modulation of the effect of osteopathic techniques on muscle properties through muscle-technique pairing
Since there was a significant interaction between treatment and muscle (0.037 [0.014]; p = 0.009), the simple effects were interpreted for the secondary objective. There was a tendency for a difference in comparison between MRI, MET and STT, but all multiple comparisons between treatment and muscle were not significant (p > 0.05) (Table 6). There was no sex-specific simple effect for the significant interaction but some tendency (p > 0.05). For example, in males compared to females, F of the UT showed a higher increase and decrease following MET and MRT, respectively (Table 7 and Figs. 4, 5).

Mean differences in frequency of UT for MET; Legend: Not applicable.

Mean differences in frequency of UT for MRT; Legend: Not applicable.
Harms
Participants were instructed to report harms to their physical or mental health to the principal investigator by phone or e–mail, pending their severity. No harms were reported.
Discussion
To the best of our knowledge, this study is the first to investigate the effect of OMT on the HRMT of healthy subjects. In detail, we used biomechanical and viscoelastic measures to assess the effect of manual techniques with different modalities on muscles with different characteristics. The sample comprised 57 participants (computed: 60; screened: 82; randomised 59) and showed acceptable recruitment and retention rates (72% and 96%, respectively). First, we report significant results for the primary objective. In detail, MET, MRT, and STT applied to the SM and UT (CS was excluded) resulted in significantly decreased muscle tone (F [p = 0.008]), decreased biomechanical (S [p = 0.048] not D [p = 0.527]), and increased viscoelastic properties (R [p < 0.001] and C [p = 0.028]) from baseline to follow-up (Table 5). Notably, decrement (D [p = 0.527]) did not change significantly, but this muscle parameter was previously proposed to be a constant124. In contrast, others have reported significant changes of decrement (D) in paraspinal muscles following the application of spinal mobilization in patients with LBP125. However, the control group (where participants lay relaxed) showed similar results, and it was hypothesised that the effect may arise due to the relaxed body state125. The data suggest that the primary hypothesis can be confirmed, showing that osteopathic techniques modulated the HRMT of treated muscles in healthy subjects by decreasing muscle tone and stiffness while increasing relaxation and creep (decrement did not change significantly). Future studies might assess the effect of OMT on the HRMT of people with MSDs because conditions like LBP and NP are associated with altered muscle properties109,126,127. For example, in patients with LBP compared to healthy controls, the lumbar extensor myofascia generally shows increased muscle tone (F), stiffness (S), and decrement (D)73,126,128,129 as well as decreased relaxation (R) and creep (C)69,127,130. Hence, we propose to examine the effect of OMT on the muscle properties of, for example, the lumbar extensor myofascia or the upper trapezius muscles in patients with LBP or NP, respectively. Based on the present findings, we hypothesise that osteopathic interventions will decrease muscle tone, stiffness, and possibly decrement, and increase relaxation and creep in this population. However, future studies are needed to validate or falsify this hypothesis. Second, we demonstrate no significant results for the secondary objective (using simple effects). However, we detected a non-significant trend (p > 0.05) suggesting that the decrease in muscle tone (F), decrease in biomechanical (D not S), and increase in viscoelastic properties (R and C) were achieved through MET and MRT (not STT) when applied to the SM, and through STT (not MET and MRT) when applied to the UT (Table 6). Notably, this tendency was consistent for all muscle properties except for muscle stiffness (S). In other words, the smaller and thinner muscle (SM) responded (as expected) to the active (MET) and low-pressure technique (MRT), whereas the larger and thicker muscle (UT) responded (as expected) to the high-pressure technique (STT). The reported trend is fairly consistent with the secondary hypothesis (considering that the CS was excluded) but requires further scrutiny for verification or falsification. Lastly, subgroup analysis for the primary objective revealed a significant sex-specific difference for muscle tone (p = 0.030) but no other muscle properties (p > 0.05). Overall, female subjects showed greater descriptive changes (mean values for primary objective) in all muscle properties than male subjects (Table 5). For the secondary objective, no significant sex-specific difference was found but an interesting tendency showed that the muscle tone of the UT increased after MET and decreased after MRT in males, whereas the opposite was reported for females (Table 7 and Figs. 4, 5). The reason for this trend is unclear but we hypothesise, based on clinical experience, that males tend to exaggerate the counterpressure during MET techniques (presumably to demonstrate strength) which may have increased muscle tone.
To date, the mechanisms underlying these reported changes in HRMT following OMT are unclear and require further investigation. There might be biological, psychological, and social factors involved. However, based on the context of this study (comprising a short treatment time, strong manual focus, and unsound therapeutic alliance), we speculate that a biological mechanism of action is most probable. Though it might be the case that the three techniques have the same, different, overlapping, or multiple mechanisms of action, we suggest that mechanotransduction may underlie these changes. In detail, mechanotransduction suggests that extracellular mechanical signals are converted into intracellular chemical signals (and changes in gene expression) via integrins, which physically couple the extracellular matrix (including collagen fibres) with the intracellular cytoskeleton (including actomyosin filaments)131. As the HRMT depends on the interaction of cellular actomyosin filaments53, we hypothesise that mechanical stimuli provided during osteopathic treatment may change the tensional forces within the (collagen fibres of the) extracellular matrix and, through integrins, within the (actomyosin filaments of the) intracellular cytoskeleton, thereby modifying the HRMT.
Overall, there is a scarcity of studies assessing the effect of manual treatment on muscle properties. Moreover, the available literature is focused on muscle stiffness and tone, whereas decrement, relaxation, and creep are mostly not considered. Therefore, our findings complement the existing body of evidence. Taking these factors into account, our results are largely consistent with the current literature. For example, in healthy participants, it was shown that manual therapy can reduce muscle stiffness132; this was demonstrated for MET133, MRT (or self-MRT, respectively, which mimics manual MRT with a foam roller)134, and STT (or massage, respectively, which resembles STT using deep pressure gliding strokes)135. Similarly, it was revealed that trigger points have an increased muscle tone and stiffness106, which can be decreased through manual myofascial release136. Notably, manual techniques might also reduce muscle tone and stiffness in participants with MSDs137. Particularly in patients with LBP, increased paravertebral muscle tone and stiffness were demonstrated127, which could be reduced through manual techniques like spinal mobilisation125. However, further research is required to substantiate these findings. Also, it is important to note that muscle properties like stiffness do not seem to correlate with pain (in patients with chronic NP and LBP), because muscle stiffness typically returns to baseline one day after treatment (using cupping massage) even if the pain improves138. Moreover, we need to consider other factors that could have swayed the results, such as sex, age, and handedness. The sample in this study was relatively homogenous comprising predominantly female (68%), young (22.7 ± 4.5 years), and right-handed (91%) subjects. In general, muscle tone and stiffness are reported to be greater in males than females72,73,74, however, there are also (partially) conflicting findings70,71,75. Nonetheless, higher muscle tone and stiffness in males may arise due to differences in muscle size, mass, conditioning, and fiber composition between the sexes124,139, which possibly relate to differences in sex hormones70 and skinfold thickness75. Beyond sex, significant differences in muscle stiffness have also been reported between age groups (higher in elderly and middle-aged than young individuals)74 and handedness (higher on the side of the dominant hand)73. Although subgroup analysis was performed for sex, we did not consider the impact of age (because only two subjects were over thirty years old) and handedness (because all measures were taken on the right side and only five subjects were left-handed).
There are limitations to consider when interpreting the results of this study. First and foremost, one of the three conditions was dropped because of frequent measurement errors. In detail, all missing values (8.9% of all numbers analysed) originated from myotonometer measurements of the CS (not SM or UT), which was consequently excluded from the analysis. These dependent missing values limited the number of observations available to analysis and therefore reduced the statistical power140. Further, dropping one condition increases the likelihood of reporting false-positive results141. Presumably, these missing values arose because the feasibility of the MyotonPRO is limited to measurements of muscles that are thicker than 3 mm68 and not located near the bone142,143 (Box 5).
Another shortfall is that the results are informative of an immediate-term effect (approximately five minutes after treatment). Thus, the measured tissue response may be reflective of the thixotropy effect144; albeit the size of this effect remains unclear145. Future research may assess if these changes are enduring in the short, medium, and long term. Further, it is noteworthy that participants were assessed in supine position although the HRMT relates to the biotensegrity system and posture53. Similarly, it would have been reasonable to measure active muscle tone using EMG. Without it, we cannot verify that participants were fully relaxed. This may have biased the results because active muscle contractions increase muscle tone, stiffness, and elasticity146. In the future, myotonometer and EMG measurements may be applied simultaneously (where possible) to ensure that HRMT is measured (i.e., ensuring that active muscle tone is avoided, and passive muscle tone is maintained). Furthermore, a disadvantage of the study procedure was that participants were measured and treated at different times of the day (between 9 a.m. and 4 p.m.). Therefore, time-dependent physiological variations in muscle tone were not considered. This might have affected the results because the resting muscle tone was shown to fluctuate across the day147. Other barriers to interpreting the results relate to the interventions. For one, manual techniques are often loosely defined, and it was particularly difficult to find literature describing the same manual procedure as the STT used in this study. In the end, we settled to include research on massage techniques, which employ similar parameters than the STT. Future research might consider not examining manual techniques (e.g., MET, MRT, and STT) but rather their biophysical parameters (e.g., stretch, compression, shear, and torque forces) to ensure optimal comparability148,149. Furthermore, the manual techniques were applied for five minutes, which appears brief but seems to be sufficient for one muscle to be treated with one technique (because the therapists perceived palpatory signs of release/relaxation). Also, we cannot rule out that differences between therapists might have influenced the results (e.g., due to sex differences). However, consensus training was implemented before the trial and the therapists exhibited similar characteristics in terms of age and experience. Moreover, the interventions encompassed common manual techniques with different characteristics, however, single manual techniques are not representative of person-centered osteopathic care. Further, subgroup analysis revealed a significant sex-specific difference in F (but no other muscle properties) from baseline to follow-up for the primary objective (but not secondary objective). Thus, the generalisability of this result may be limited to females. However, male subjects were underrepresented in our sample (n = 18; 32%) and future research should recruit sex-balanced samples to substantiate these findings. Lastly, it is unclear if OMT could also have the opposite effect. In detail, it has previously been assumed that OMT restores normal muscle tone where it is altered36,37,38,39, meaning that high muscle tone decreases, and low muscle tone increases, when OMT is applied57. Therefore, future studies might assess the effect of OMT on conditions associated with both hypertonia and hypotonia.
In this study, we demonstrate that OMT modifies the HRMT in healthy participants without significant interaction of muscle-technique pairs. The mechanisms underlying these changes are unclear and the results are limited by the exclusion of one condition. Our findings are largely consistent with previous research but limited by the immediate term measurement. Future studies should modify the protocol and assess if these effects are reproducible (and beneficial) in patients with MSDs. In the end, although speculative, we hypothesise that modifying the HRMT may be a mechanism of action underlying manual techniques.
Conclusion
Taken together, MRT, MET, and STT significantly decreased F and S (not D) and increased R and C of the SM and UT (CS was not measurable) in healthy subjects. Hence, OMT effectively modified the HRMT, and the primary objective can be confirmed. In contrast, the effect of MRT, MET, and STT on the HRMT was not significantly modulated by muscle–technique pairs in healthy subjects. Hence, it is uncertain if some techniques change the HRMT of some muscles more effectively, and the secondary objective must be rejected. Subgroup analysis revealed a significantly greater reduction of F (but no other muscle properties) in female subjects for the primary, but not the secondary, objective. These findings may inform future research investigating the effect of OMT on the HRMT in patients with MSDs.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article.
Abbreviations
- MRT:
-
Myofascial release technique
- MET:
-
Muscle energy technique
- STT:
-
Soft tissue technique
- CS:
-
Corrugator supercilii muscle
- SM:
-
Superficial masseter muscle
- UT:
-
Upper trapezius muscle
- F:
-
Oscillation frequency
- S:
-
Dynamic stiffness
- D:
-
Logarithmic decrement
- R:
-
Mechanical stress relaxation time
- C:
-
Ratio of deformation and relaxation time
- MSDs:
-
Musculoskeletal disorders
- HRMT:
-
Human resting muscle tone
- OMT:
-
Osteopathic manipulative treatment
- EMG:
-
Electromyography
- MPs:
-
Measurement points
- NP:
-
Neck pain
- LBP:
-
Low back pain
References
Safiri, S. et al. Prevalence, deaths, and disability-adjusted life years due to musculoskeletal disorders for 195 countries and territories 1990–2017. Arthritis Rheumatol. 73, 702–714. https://doi.org/10.1002/art.41571 (2021).
Safiri, S. et al. Global, regional, and national burden of other musculoskeletal disorders 1990–2017: Results from the Global Burden of Disease Study 2017. Rheumatology 60, 855–865. https://doi.org/10.1093/rheumatology/keaa315 (2021).
Jin, Z. et al. Incidence trend of five common musculoskeletal disorders from 1990 to 2017 at the global, regional and national level: Results from the global burden of disease study 2017. Ann. Rheum. Dis. 79, 1014–1022. https://doi.org/10.1136/annrheumdis-2020-217050 (2020).
GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 Diseases and Injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–858. https://doi.org/10.1016/S0140-6736(18)32279-7.
Bornhöft, L. et al. More cost-effective management of patients with musculoskeletal disorders in primary care after direct triaging to physiotherapists for initial assessment compared to initial general practitioner assessment. BMC Musculoskelet. Disord. 20, 1–9. https://doi.org/10.1186/s12891-019-2553-9 (2019).
GBD 2019 Viewpoint Collaborators. Five insights from the Global Burden of Disease Study 2019. Lancet. 2020;396:1135–59. https://doi.org/10.1016/S0140-6736(20)31404-5.
Blyth, F. M., Briggs, A. M., Huckel Schneider, C., Hoy, D. G. & March, L. M. The global burden of musculoskeletal pain - where to from here?. Am. J. Public Health 109, 35–40. https://doi.org/10.2105/AJPH.2018.304747 (2019).
Lin, I. et al. What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines: Systematic review. Br. J. Sports Med. 54, 79–86. https://doi.org/10.1136/bjsports-2018-099878 (2020).
Babatunde, O. O. et al. Effective treatment options for musculoskeletal pain in primary care: A systematic overview of current evidence. PLoS ONE 12, e0178621. https://doi.org/10.1371/journal.pone.0178621 (2017).
Kløjgaard, M. E., Manniche, C., Pedersen, L. B., Bech, M. & Søgaard, R. Patient preferences for treatment of low back pain—A discrete choice experiment. Value Heal. 17, 390–396. https://doi.org/10.1016/j.jval.2014.01.005 (2014).
Goertz, C. M. & George, S. Z. Insurer coverage of nonpharmacological treatments for low back pain—Time for a change. JAMA Netw. Open. 1, e183037 (2018).
Gianola, S. et al. Effectiveness of treatments for acute and subacute mechanical non-specific low back pain: a systematic review with network meta-analysis. Br. J. Sports Med. 56, 41–50. https://doi.org/10.1136/bjsports-2020-103596 (2022).
Vaucher, P., Macdonald, R. J. D. & Carnes, D. The role of osteopathy in the Swiss primary health care system: A practice review. BMJ Open 8, e023770. https://doi.org/10.1136/bmjopen-2018-023770 (2018).
Bohlen, L., Shaw, R., Cerritelli, F. & Esteves, J. E. Osteopathy and mental health: An embodied, predictive, and interoceptive framework. Front Psychol. 12, 1–22. https://doi.org/10.3389/fpsyg.2021.767005 (2021).
Task Force on the Low Back Pain Clinical Practice Guidelines. American Osteopathic Association guidelines for osteopathic manipulative treatment (OMT) for patients with low back pain. J Am Osteopath Assoc. 2016;116:536–49. https://doi.org/10.7556/jaoa.2016.107.
Johnson, J. C. & Degenhardt, B. F. Who uses osteopathic manipulative treatment? A prospective, observational study conducted by DO-Touch.NET. J. Am. Osteopath. Assoc. 119, 802–812. https://doi.org/10.7556/jaoa.2019.133 (2019).
Sciomachen, P. et al. Core competencies in osteopathy: Italian register of osteopaths proposal. Int. J. Osteopath. Med. 27, 1–5. https://doi.org/10.1016/j.ijosm.2018.02.001 (2018).
Bagagiolo, D., Rosa, D. & Borrelli, F. Efficacy and safety of osteopathic manipulative treatment: an overview of systematic reviews. BMJ Open 12, e053468 (2022).
Verhaeghe, N., Schepers, J., van Dun, P. & Annemans, L. Osteopathic care for spinal complaints: A systematic literature review. PLoS ONE 13, e0206284. https://doi.org/10.1371/journal.pone.0206284 (2018).
Franke, H. Osteopathic manipulative treatment for chronic nonspecific neck pain: A systematic review and meta-analysis. Int. J. Osteopath. Med. 18, 255–267. https://doi.org/10.1016/j.ijosm.2015.05.003 (2015).
Dal Farra, F., Risio, R. G., Vismara, L. & Bergna, A. Effectiveness of osteopathic interventions in chronic non-specific low back pain: A systematic review and meta-analysis. Complement. Ther. Med. 56, 102616. https://doi.org/10.1016/j.ctim.2020.102616 (2021).
Franke, H., Franke, J. D. & Fryer, G. Osteopathic manipulative treatment for nonspecific low back pain: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 15, 1–18. https://doi.org/10.1186/1471-2474-15-286 (2014).
Licciardone, J. C., Brimhall, A. K. & King, L. N. Osteopathic manipulative treatment for low back pain: A systematic review and meta-analysis of randomized controlled trials. BMC Musculoskelet. Disord. 6, 1–12. https://doi.org/10.1186/1471-2474-6-43 (2005).
Franke, H., Franke, J.-D., Belz, S. & Fryer, G. Osteopathic manipulative treatment for low back and pelvic girdle pain during and after pregnancy: A systematic review and meta-analysis. J. Bodyw. Mov. Ther. 21, 752–762. https://doi.org/10.1016/j.jbmt.2017.05.014 (2017).
Licciardone, J. C. & Gatchel, R. J. Osteopathic medical care with and without osteopathic manipulative treatment in patients with chronic low back pain: A pain registry–based study. J. Am. Osteopath. Assoc. 120, 64–73. https://doi.org/10.7556/jaoa.2020.016 (2020).
Verhaeghe, N., Schepers, J., van Dun, P. & Annemans, L. Osteopathic care for low back pain and neck pain: A cost-utility analysis. Complement. Ther. Med. 40, 207–213. https://doi.org/10.1016/j.ctim.2018.06.001 (2018).
Nguyen, C. et al. Effect of osteopathic manipulative treatment vs sham treatment on activity limitations in patients with nonspecific subacute and chronic low back pain a randomized clinical trial. JAMA Intern. Med. 181, 620–630. https://doi.org/10.1001/jamainternmed.2021.0005 (2021).
Orrock, P. J. & Myers, S. P. Osteopathic intervention in chronic non-specific low back pain: A systematic review. BMC Musculoskelet. Disord. 14, 1–7. https://doi.org/10.1186/1471-2474-14-129 (2013).
Posadzki, P. & Ernst, E. Osteopathy for musculoskeletal pain patients: A systematic review of randomized controlled trials. Clin. Rheumatol. 30, 285–291. https://doi.org/10.1007/s10067-010-1600-6 (2011).
Lewis, R. et al. Strategies for optimising musculoskeletal health in the 21st century. BMC Musculoskelet. Disord. 20, 1–15. https://doi.org/10.1186/s12891-019-2510-7 (2019).
Tamburella, F. et al. Cerebral perfusion changes after osteopathic manipulative treatment: A randomized manual placebo-controlled trial. Front. Physiol. 10, 1–10. https://doi.org/10.3389/fphys.2019.00403 (2019).
Dunn, M., Rushton, A. B., Mistry, J., Soundy, A. & Heneghan, N. R. Which biopsychosocial factors are associated with the development of chronic musculoskeletal pain? Protocol for an umbrella review of systematic reviews. BMJ Open 11, e053941. https://doi.org/10.1136/bmjopen-2021-053941 (2021).
Sampath, K. K. et al. Barriers and facilitators experienced by osteopaths in implementing a biopsychosocial (BPS) framework of care when managing people with musculoskeletal pain—A mixed methods systematic review. BMC Health Serv Res. 21, 1–15. https://doi.org/10.1186/s12913-021-06720-w (2021).
Hu, X. et al. Quantifying paraspinal muscle tone and stiffness in young adults with chronic low back pain: A reliability study. Sci. Rep. 8, 1–10. https://doi.org/10.1038/s41598-018-32418-x (2018).
Lo, W. L. A. et al. Lumbar muscles biomechanical characteristics in young people with chronic spinal pain. BMC Musculoskelet. Disord. 20, 1–9. https://doi.org/10.1186/s12891-019-2935-z (2019).
Chin, J., Qiu, W., Lomiguen, C. M. & Volokitin, M. Osteopathic manipulative treatment in tension headaches. Cureus. 12, e12040. https://doi.org/10.7759/cureus.12040 (2020).
Tramontano, M. et al. Brain connectivity changes after osteopathic manipulative treatment: A randomized manual placebo-controlled trial. Brain Sci. 10, 1–15. https://doi.org/10.3390/brainsci10120969 (2020).
Goldfinger, M. S. et al. An osteopathic, non pharmacologic approach to parkinson’s disease, restless leg syndrome & essential tremor. Osteopath. Fam. Physician 9, 30–38. https://doi.org/10.1016/ofp.v9i6.525 (2017).
Collebrusco, L. et al. Osteopathy and emergency: A model of osteopathic treatment aimed at managing the post-traumatic stress—brief and useful guide—part 2. Health (Irvine Calif). 10, 1597–1608. https://doi.org/10.4236/health.2018.1011120 (2018).
Nair, K. et al. Stiffness of resting lumbar myofascia in healthy young subjects quantified using a handheld myotonometer and concurrently with surface electromyography monitoring. J. Bodyw. Mov. Ther. 20, 388–396. https://doi.org/10.1016/j.jbmt.2015.12.005 (2016).
Ajimsha, M. S., Al-Mudahka, N. R. & Al-Madzhar, J. A. Effectiveness of myofascial release: Systematic review of randomized controlled trials. J. Bodyw. Mov. Ther. 19, 102–112. https://doi.org/10.1016/j.jbmt.2014.06.001 (2015).
McKenney, K., Elder, A. S., Elder, C. & Hutchins, A. Myofascial release as a treatment for orthopaedic conditions: A systematic review. J. Athl. Train. 48, 522–527. https://doi.org/10.4085/1062-6050-48.3.17 (2013).
Laimi, K. et al. Effectiveness of myofascial release in treatment of chronic musculoskeletal pain: a systematic review. Clin. Rehabil. 32, 440–450. https://doi.org/10.1177/0269215517732820 (2018).
Chen, Z., Wu, J., Wang, X., Wu, J. & Ren, Z. The effects of myofascial release technique for patients with low back pain: A systematic review and meta-analysis. Complement. Ther. Med. 59, 102737. https://doi.org/10.1016/j.ctim.2021.102737 (2021).
Wu, Z. et al. Myofascial release for chronic low back pain: A systematic review and meta-analysis. Front. Med. 8, 1–14. https://doi.org/10.3389/fmed.2021.697986 (2021).
Thomas, E., Cavallaro, A. R., Mani, D., Bianco, A. & Palma, A. The efficacy of muscle energy techniques in symptomatic and asymptomatic subjects: A systematic review. Chiropr. Man Ther. 27, 1–18. https://doi.org/10.1186/s12998-019-0258-7 (2019).
Furlan, A. D., Brosseau, L., Imamura, M. & Irvin, E. Massage for low-back pain: A systematic review within the framework of the Cochrane Collaboration Back Review Group. Spine (Phila Pa 1976) 27, 1896–1910. https://doi.org/10.1097/00007632-200209010-00017 (2002).
Furlan, A. D., Imamura, M., Dryden, T. & Irvin, E. Massage for low-back pain: An updated systematic review within the framework of the Cochrane Back Review Group. Spine (Phila Pa 1976) 34, 1669–1684. https://doi.org/10.1097/BRS.0b013e3181ad7bd6 (2009).
Furlan, A. D., Giraldo, M., Baskwill, A., Irvin, E. & Imamura, M. Massage for low-back pain. Cochrane Database Syst Rev. 2015, CD001929. https://doi.org/10.1002/14651858.CD001929.pub3 (2015).
Kolding, L. T., Do, T. P., Ewertsen, C. & Schytz, H. W. Muscle stiffness in tension-type headache patients with pericranial tenderness. Cephalalgia Rep. 1, 1–6 (2018).
Gualdi, A. et al. Selective denervation of the corrugator supercilii muscle for the treatment of idiopatic trigeminal neuralgia purely paroxysmal distributed in the supraorbital and suprathrochlear dermatomes. J. Headache Pain 22, 1–7 (2021).
Knutson, G. A. & Owens, E. F. Active and passive characteristics of muscle tone and their relationship to models of subluxation/joint dysfunction: Part I. J. Can. Chiropr. Assoc. 47, 168–179 (2003).
Masi, A. T. & Hannon, J. C. Human resting muscle tone (HRMT): Narrative introduction and modern concepts. J. Bodyw. Mov. Ther. 12, 320–332. https://doi.org/10.1016/j.jbmt.2008.05.007 (2008).
Schoenrock, B. et al. Bed rest, exercise countermeasure and reconditioning effects on the human resting muscle tone system. Front. Physiol. 9, 1–20. https://doi.org/10.3389/fphys.2018.00810 (2018).
Mense S, Masi AT. Increased Muscle Tone as a Cause of Muscle Pain. In: Muscle Pain: Understanding the Mechanisms. 2010. p. 207–49. doi:https://doi.org/10.1007/978-3-540-85021-2.
Boesler, D., Warner, M., Alpers, A., Finnerty, E. P. & Kilmore, M. A. Efficacy of high-velocity low-amplitude manipulative technique in subjects with low-back pain during menstrual cramping. J. Am. Osteopath. Assoc. 93, 203–214. https://doi.org/10.7556/jaoa.1993.93.2.203 (1993).
Korotkov, K. et al. Stress reduction with osteopathy assessed with GDV electrophotonic imaging: Effects of osteopathy treatment. J. Altern. Complement. Med. 18, 251–257. https://doi.org/10.1089/acm.2010.0853 (2012).
Rajaii, R. M., Cox, G. J. & Schneider, R. P. Role of osteopathic manipulative treatment in the management of stiff person syndrome. J. Am. Osteopath. Assoc. 115, 394–398. https://doi.org/10.7556/jaoa.2015.081 (2015).
Alexander, N., Rastelli, A., Webb, T. & Rajendran, D. The validity of lumbo-pelvic landmark palpation by manual practitioners: a systematic review. Int. J. Osteopath. Med. 39, 10–20. https://doi.org/10.1016/j.ijosm.2020.10.008 (2021).
Basile, F., Petracca, M. & Scionti, R. Diagnostic reliability of osteopathic tests: A systematic review. Int. J. Osteopath. Med. 25, 21–29. https://doi.org/10.1016/j.ijosm.2017.03.004 (2017).
May, S., Littlewood, C. & Bishop, A. Reliability of procedures used in the physical examination of non-specific low back pain: A systematic review. Aust. J. Physiother. 52, 91–102. https://doi.org/10.1016/S0004-9514(06)70044-7 (2006).
Najm, W. I. et al. Content validity of manual spinal palpatory exams - A systematic review. BMC Complement Altern Med. 3, 1–14 (2003).
Póvoa, L. C., Ferreira, A. P. A. & Silva, J. G. Validation of palpatory methods for evaluating anatomical bone landmarks of the cervical spine: A systematic review. J. Manipulative Physiol. Ther. 38, 302–310. https://doi.org/10.1016/j.jmpt.2015.04.002 (2015).
Cooperstein, R. & Hickey, M. The reliability of palpating the posterior superior iliac spine: A systematic review. J. Can. Chiropr. Assoc. 60, 36–46 (2016).
Stochkendahl, M. J. et al. Manual examination of the spine: a systematic critical literature review of reproducibility. J. Manipulative Physiol. Ther. 29, 475–485. https://doi.org/10.1016/j.jmpt.2006.06.011 (2006).
Nolet, P. S. et al. Reliability and validity of manual palpation for the assessment of patients with low back pain: a systematic and critical review. Chiropr. Man Ther. 29, 1–20 (2021).
Chen, G. et al. Reliability of a portable device for quantifying tone and stiffness of quadriceps femoris and patellar tendon at different knee flexion angles. PLoS ONE 14, e0220521. https://doi.org/10.1371/journal.pone.0220521 (2019).
Myoton. MyotonPRO User Manual. 2013. https://www.myoton.com/UserFiles/Updates/MyotonPRO_User_Manual.pdf.
White, A., Abbott, H., Masi, A. T., Henderson, J. & Nair, K. Biomechanical properties of low back myofascial tissue in younger adult ankylosing spondylitis patients and matched healthy control subjects. Clin. Biomech. 57, 67–73. https://doi.org/10.1016/j.clinbiomech.2018.06.006 (2018).
Ramazanoglu, E., Turhan, B. & Usgu, S. Evaluation of the tone and viscoelastic properties of the masseter muscle in the supine position, and its relation to age and gender. Dent. Med. Probl. 58, 155–161 (2021).
Agyapong-Badu, S., Warner, M., Samuel, D. & Stokes, M. Measurement of ageing effects on muscle tone and mechanical properties of rectus femoris and biceps brachii in healthy males and females using a novel hand-held myometric device. Arch. Gerontol. Geriatr. 62, 59–67. https://doi.org/10.1016/j.archger.2015.09.011 (2016).
Taş, S. & Salkın, Y. An investigation of the sex-related differences in the stiffness of the Achilles tendon and gastrocnemius muscle: Inter-observer reliability and inter-day repeatability and the effect of ankle joint motion. Foot 41, 44–50. https://doi.org/10.1016/j.foot.2019.09.003 (2019).
Ilahi, S. et al. Quantified biomechanical properties of lower lumbar myofascia in younger adults with chronic idiopathic low back pain and matched healthy controls. Clin. Biomech. 73, 78–85. https://doi.org/10.1016/j.clinbiomech.2019.12.026 (2020).
Wu, Z. et al. Effects of age and sex on properties of lumbar erector spinae in healthy people: Preliminary results from a pilot study. Front. Physiol. 12, 1–10. https://doi.org/10.3389/fphys.2021.718068 (2021).
Mencel, J. et al. Effect of gender, muscle type and skinfold thickness on myometric parameters in young people. PeerJ 9, e12367. https://doi.org/10.7717/peerj.12367 (2021).
Schulz, K. F., Altman, D. G., Moher, D., CONSORT Group. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. BMJ 340, 698–702. https://doi.org/10.1136/bmj.c332 (2010).
Moher, D. et al. CONSORT 2010 Explanation and Elaboration: updated guidelines for reporting parallel group randomised trials. BMJ 340, 1–28. https://doi.org/10.1136/bmj.c869 (2010).
McAlister, F. A., Straus, S. E., Sackett, D. L. & Altman, D. G. Analysis and reporting of factorial trials: A systematic review. JAMA 289, 2545–2553. https://doi.org/10.1001/jama.289.19.2545 (2003).
Létocart, A. J. et al. Muscles adaptation to aging and training: Architectural changes—A randomised trial. BMC Geriatr. 21, 1–18. https://doi.org/10.1186/s12877-020-02000-0 (2021).
Ghaoui, R., Clarke, N., Hollingworth, P. & Needham, M. Muscle disorders: The latest investigations. Intern. Med. J. 43, 970–978. https://doi.org/10.1111/imj.12234 (2013).
Giusti R. Glossary of Osteopathic Terminology. 3rd edition. American Association of Colleges of Osteopathic Medicine; 2017. https://www.aacom.org/docs/default-source/insideome/got2011ed.pdf.
D’Alessandro, G., Cerritelli, F. & Cortelli, P. Sensitization and interoception as key neurological concepts in osteopathy and other manual medicines. Front. Neurosci. https://doi.org/10.3389/fnins.2016.00100 (2016).
Weerapong, P., Hume, P. A. & Kolt, G. S. The mechanisms of massage and effects on performance, muscle recovery and injury prevention. Sport Med. 35, 235–256. https://doi.org/10.2165/00007256-200535030-00004 (2005).
Loghmani, M. T. & Whitted, M. Soft tissue manipulation: A powerful form of mechanotherapy. J. Physiother. Phys. Rehabil. 1, 1–6. https://doi.org/10.4172/2573-0312.1000122 (2016).
Waters-Banker, C., Dupont-Versteegden, E. E., Kitzman, P. H. & Butterfield, T. A. Investigating the mechanisms of massage efficacy: The role of mechanical immunomodulation. J. Athl Train. 49, 266–273. https://doi.org/10.4085/1062-6050-49.2.25 (2014).
Fryer, G. Muscle energy technique: An evidence-informed approach. Int. J. Osteopath. Med. 14, 3–9. https://doi.org/10.1016/j.ijosm.2010.04.004 (2011).
Beardsley, C. & Škarabot, J. Effects of self-myofascial release: A systematic review. J. Bodyw. Mov. Ther. 19, 747–758. https://doi.org/10.1016/j.jbmt.2015.08.007 (2015).
Krause, F., Wilke, J., Niederer, D., Vogt, L. & Banzer, W. Acute effects of foam rolling on passive tissue stiffness and fascial sliding: Study protocol for a randomized controlled trial. Trials 18, 1–6 (2017).
Zein-Hammoud, M. & Standley, P. R. Modeled osteopathic manipulative treatments: A review of their in vitro effects on fibroblast tissue preparations. J. Am. Osteopath. Assoc. 115, 490–502. https://doi.org/10.7556/jaoa.2015.103 (2015).
Parravicini, G. & Bergna, A. Biological effects of direct and indirect manipulation of the fascial system. Narrative review. J. Bodyw. Mov. Ther. 21, 435–445. https://doi.org/10.1016/j.jbmt.2017.01.005 (2017).
Tozzi, P. A unifying neuro-fasciagenic model of somatic dysfunction - Underlying mechanisms and treatment—Part II. J. Bodyw. Mov. Ther. 19, 526–543. https://doi.org/10.1016/j.jbmt.2015.03.002 (2015).
Hsu, J. J. et al. Morphometric evaluation of the frontal migraine trigger site. Plast. Reconstr. Surg. 141, 726–732. https://doi.org/10.1097/PRS.0000000000004296 (2018).
Duráo, A. P. R., Morosolli, A., Brown, J. & Jacobs, R. Masseter muscle measurement performed by ultrasound: A systematic review. Dentomaxillofac. Radiol. 46, 20170052. https://doi.org/10.1259/dmfr.20170052 (2017).
Salavati, M., Akhbari, B., Ebrahimi Takamjani, I., Ezzati, K. & Haghighatkhah, H. Reliability of the upper trapezius muscle and fascia thickness and strain ratio measures by ultrasonography and sonoelastography in participants with myofascial pain syndrome. J. Chiropr. Med. 16, 316–323. https://doi.org/10.1016/j.jcm.2017.06.003 (2017).
Pinar, Y., Govsa, F., Ozer, M. A. & Ertam, I. Anatomocosmetic implication rules of the corrugator supercilii muscle for youthful eye appearance. Surg. Radiol. Anat. 38, 1045–1051. https://doi.org/10.1007/s00276-016-1666-1 (2016).
Azaroual, M. F., Fikri, M., Abouqal, R., Benyahya, H. & Zaoui, F. Relationship between dimensions of muscles of mastication (masseter and lateral pterygoid) and skeletal dimensions: Study of 40 cases. Int. Orthod. 12, 111–124. https://doi.org/10.1016/j.ortho.2013.09.001 (2014).
Tiwari, R. & Snow, G. B. Role of myocutaneous flaps in reconstruction of the head and neck. J. Laryngol. Otol. 97, 441–458. https://doi.org/10.1017/s0022215100094378 (1983).
Minasny, B. Understanding the process of fascial unwinding. Int. J. Ther. Massage Bodyw. 2, 10–17. https://doi.org/10.3822/ijtmb.v2i3.43 (2009).
Franke, H., Fryer, G., Ostelo, R. W. J. G. & Kamper, S. J. Muscle energy technique for non-specific low-back pain. A Cochrane systematic review. Int. J. Osteopath. Med. 20, 41–52. https://doi.org/10.1016/j.ijosm.2016.01.002 (2016).
Moore, S. D., Laudner, K. G., McLoda, T. A. & Shaffer, M. A. The immediate effects of muscle energy technique on posterior shoulder tightness: A randomized controlled trial. J. Orthop. Sports Phys. Ther. 41, 400–407. https://doi.org/10.2519/jospt.2011.3292 (2011).
Koren, Y. & Kalichman, L. Deep tissue massage: What are we talking about?. J. Bodyw. Mov. Ther. 22, 247–251. https://doi.org/10.1016/j.jbmt.2017.05.006 (2018).
El-Hafez, H. M. et al. Instrument-assisted soft tissue mobilisation versus stripping massage for upper trapezius myofascial trigger points. J. Taibah Univ. Med. Sci. 15, 87–93. https://doi.org/10.1016/j.jtumed.2020.01.006 (2020).
Bell, J. Massage therapy helps to increase range of motion, decrease pain and assist in healing a client with low back pain and sciatica symptoms. J. Bodyw. Mov. Ther. 12, 281–289. https://doi.org/10.1016/j.jbmt.2008.01.006 (2008).
Harrer, G. The Fascial Distortion Model originated by Stephen P. Typaldos. In Fascia in the Osteopathic Field (eds Liem, T. et al.) 359–368 (Handspring Publishing, 2017).
Garcia-Bernal, M. I., Heredia-Rizo, A. M., Gonzalez-Garcia, P., Cortés-Vega, M. D. & Casuso-Holgado, M. J. Validity and reliability of myotonometry for assessing muscle viscoelastic properties in patients with stroke: A systematic review and meta-analysis. Sci. Rep. 11, 1–12. https://doi.org/10.1038/s41598-021-84656-1 (2021).
Roch, M., Morin, M. & Gaudreault, N. The MyotonPRO: A reliable tool for quantifying the viscoelastic properties of a trigger point on the infraspinatus in non-traumatic chronic shoulder pain. J. Bodyw. Mov. Ther. 24, 379–385. https://doi.org/10.1016/j.jbmt.2020.05.002 (2020).
Kim, K. R., Shin, H. S., Lee, S. B., Hwang, H. S. & Shin, H. J. Effects of negative pressure soft tissue therapy to ankle plantar flexor on muscle tone, muscle stiffness, and balance ability in patients with stroke. J. Int. Acad. Phys. Ther. Res. 9, 1468–1474. https://doi.org/10.20540/JIAPTR.2018.9.2.1468 (2018).
Wang, J. S. Therapeutic effects of massage and electrotherapy on muscle tone, stiffness and muscle contraction following gastrocnemius muscle fatigue. J. Phys. Ther. Sci. 29, 144–147. https://doi.org/10.1589/jpts.29.144 (2017).
Kocur, P., Wilski, M., Lewandowski, J. & Łochyński, D. Female office workers with moderate neck pain have increased anterior positioning of the cervical spine and stiffness of upper trapezius myofascial tissue in sitting posture. PM&R 11, 476–482. https://doi.org/10.1016/j.pmrj.2018.07.002 (2019).
Kisilewicz, A. et al. Eccentric exercise reduces upper trapezius muscle stiffness assessed by shear wave elastography and myotonometry. Front. Bioeng. Biotechnol. 8, 1–9. https://doi.org/10.3389/fbioe.2020.00928 (2020).
Taş, S., Yaşar, Ü. & Kaynak, B. A. Interrater and intrarater reliability of a handheld myotonometer in measuring mechanical properties of the neck and orofacial muscles. J. Manipulative Physiol. Ther. 44, 42–48. https://doi.org/10.1016/j.jmpt.2020.08.002 (2021).
Kisilewicz, A. et al. Changes in muscle stiffness of the trapezius muscle after application of ischemic compression into myofascial trigger points in professional basketball players. J. Hum. Kinet. 64, 35–45. https://doi.org/10.2478/hukin-2018-0043 (2018).
Janis, J. E., Ghavami, A., Lemmon, J. A., Leedy, J. E. & Guyuron, B. Anatomy of the corrugator supercilii muscle: Part I. Corrugator topography. Plast. Reconstr. Surg. 120, 1647–1653. https://doi.org/10.1097/01.prs.0000282725.61640.e1 (2007).
Janis, J. E., Ghavami, A., Lemmon, J. A., Leedy, J. E. & Guyuron, B. The anatomy of the corrugator supercilii muscle: Part II. Supraorbital nerve branching patterns. Plast. Reconstr. Surg. 121, 233–240. https://doi.org/10.1097/01.prs.0000299260.04932.38 (2008).
Lee, J. Y. et al. Topographic anatomy of the masseter muscle focusing on the tendinous digitation. Clin. Anat. 25, 889–892. https://doi.org/10.1002/ca.22024 (2012).
Kitai, N. et al. Human masticatory muscle volume and zygomatico-mandibular form in adults with mandibular prognathism. J. Dent. Res. 81, 752–756. https://doi.org/10.1177/154405910208101106 (2002).
Kawczyńskia, A. et al. Trapezius viscoelastic properties are heterogeneously affected by ecceentric exercise. J. Sci. Med Sport. 21, 864–869. https://doi.org/10.1016/j.jsams.2018.01.005 (2018).
Faul, F., Erdfelder, E., Lang, A.-G. & Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 39, 175–191. https://doi.org/10.3758/bf03193146 (2007).
Heinrich-Heine-Universität. G*Power: Statistical Power Analyses for Windows and Mac. 2015. http://www.gpower.hhu.de/.
Dong, C. & Wedel, M. BANOVA: An R Package for Hierarchical Bayesian ANOVA. J. Stat. Softw. 10, 10. https://doi.org/10.18637/jss.v081.i09 (2017).
Westfall, P. H., Johnson, W. O. & Utts, J. M. A Bayesian perspective on the Bonferroni adjustment. Biometrika 84, 419–427. https://doi.org/10.1093/biomet/84.2.419 (1997).
Kang, H. The prevention and handling of the missing data. Korean J. Anesthesiol. 64, 402–406 (2013).
World Medical Association. World medical association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 310, 2191–2194. https://doi.org/10.1001/jama.2013.281053 (2013).
Coates, B., Barry, A., Dougherty, J., Schaefer, E., Kelly, J., Aldag, J., et al. Quantifying intrinsic properties of resting lumbar muscle in healthy subjects using a handheld myometer. In: Proceedings of the 40th Annual Northeast Bioengineering Conference by IEEE Xplore. Boston; 2014.
Hamilton, R. I., Garden, C. L. P. & Brown, S. J. Immediate effect of a spinal mobilisation intervention on muscle stiffness, tone and elasticity in subjects with lower back pain—A randomized cross-over trial. J. Bodyw. Mov. Ther. 29, 60–67. https://doi.org/10.1016/j.jbmt.2021.09.032 (2022).
Alcaraz-Clariana, S. et al. Paravertebral muscle mechanical properties and spinal range of motion in patients with acute neck or low back pain: A case-control study. Diagnostics 11, 1–21. https://doi.org/10.3390/diagnostics11020352 (2021).
Alcaraz-Clariana, S. et al. Influence of spinal movements associated with physical evaluation on muscle mechanical properties of the lumbar paraspinal in subjects with acute low back pain. Diagnostics 12, 1–10 (2022).
Wu, Z. et al. Analysis of biomechanical properties of the lumbar extensor myofascia in elderly patients with chronic low back pain and that in healthy people. Biomed. Res. Int. 2020, 7649157. https://doi.org/10.1155/2020/7649157 (2020).
Andonian, B. J. et al. Greater resting lumbar extensor myofascial stiffness in younger ankylosing spondylitis patients than age-comparable healthy volunteers quantified by myotonometry. Arch. Phys. Med. Rehabil. 96, 2041–2047. https://doi.org/10.1016/j.apmr.2015.07.014 (2015).
Garrido-Castro, J. L. et al. Mechanical properties of lumbar and cervical paravertebral muscles in patients with axial spondyloarthritis: A case-control study. Diagnostics 11, 1–12. https://doi.org/10.3390/diagnostics11091662 (2021).
Ingber, D. E. Tensegrity and mechanotransduction. J. Bodyw. Mov. Ther. 12, 198–200. https://doi.org/10.1016/j.jbmt.2008.04.038 (2008).
Albin, S. R. et al. The effect of manual therapy on gastrocnemius muscle stiffness in healthy individuals. Foot 38, 70–75. https://doi.org/10.1016/j.foot.2019.01.006 (2019).
Kisilewicz, A., Urbaniak, M. & Kawczyński, A. Effect of muscle energy technique on calf muscle stiffness increased after eccentric exercise in athletes. J. Kinesiol. Exerc. Sci. 28, 21–29. https://doi.org/10.5604/01.3001.0012.7985 (2018).
Chang, T. T., Li, Z., Zhu, Y. C., Wang, X. Q. & Zhang, Z. J. Effects of self-myofascial release using a foam roller on the stiffness of the gastrocnemius-achilles tendon complex and ankle dorsiflexion range of motion. Front. Physiol. 12, 1–9. https://doi.org/10.3389/fphys.2021.718827 (2021).
Pérez-Bellmunt, A. et al. Effects of a massage protocol in tensiomyographic and myotonometric proprieties. Int. J. Environ. Res. Public Health. 18, 1–9. https://doi.org/10.3390/ijerph18083891 (2021).
Gordon, C. M., Andrasik, F., Schleip, R., Birbaumer, N. & Rea, M. Myofascial triggerpoint release (MTR) for treating chronic shoulder pain: A novel approach. J. Bodyw. Mov. Ther. 20, 614–622. https://doi.org/10.1016/j.jbmt.2016.01.009 (2016).
Park, S. J., Kim, S. H. & Kim, S. H. Effects of thoracic mobilization and extension exercise on thoracic alignment and shoulder function in patients with subacromial impingement syndrome: A randomized controlled pilot study. Healthcare 8, 1–11. https://doi.org/10.3390/healthcare8030316 (2020).
Lederer, A. K., Maly, C., Weinert, T. & Huber, R. Tissue stiffness is not related to pain experience: an individually controlled study in patients with chronic neck and back pain. Evidence-Based Complement Altern. Med. 2019, 1907168. https://doi.org/10.1155/2019/1907168 (2019).
Ng, J. K. F., Richardson, C. A., Kippers, V. & Parnianpour, M. Relationship between muscle fiber composition and functional capacity of back muscles in healthy subjects and patients with back pain. J. Orthop. Sports Phys. Ther. 27, 389–402. https://doi.org/10.2519/jospt.1998.27.6.389 (1998).
Couper, D. J., Hosking, J. D., Cisler, R. A., Gastfriend, D. R. & Kivlahan, D. R. Factorial designs in clinical trials: Options for combination treatment studies. J. Stud. Alcohol. Drugs. 15, 24–32. https://doi.org/10.15288/jsas.2005.s15.24 (2005).
Simmons, J. P., Nelson, L. D. & Simonsohn, U. False-positive psychology: Undisclosed flexibility in data collection and analysis allows presenting anything as significant. Psychol. Sci. 22, 1359–1366. https://doi.org/10.1177/0956797611417632 (2011).
Bizzini, M. & Mannion, A. F. Reliability of a new, hand-held device for assessing skeletal muscle stiffness. Clin. Biomech. 18, 459–461. https://doi.org/10.1016/S0268-0033(03)00042-1 (2003).
Kerins, C. M., Moore, S. D., Butterfield, T. A., McKeon, P. O. & Uhl, T. L. Reliability of the myotonometer for assessment of posterior shoulder tightness. Int. J. Sports Phys. Ther. 8, 248–255 (2013).
Weir, A. et al. A manual therapy technique for chronic adductor-related groin pain in athletes: A case series. Scand. J. Med. Sci. Sports 19, 616–620. https://doi.org/10.1111/j.1600-0838.2008.00841.x (2009).
Simons, D. G. & Mense, S. Understanding and measurement of muscle tone as related to clinical muscle pain. Pain 75, 1–17 (1998).
Agyapong-Badu, S., Warner, M., Samuel, D. & Stokes, M. Practical considerations for standardized recording of muscle mechanical properties using a myometric device: Recording site, muscle length, state of contraction and prior activity. J. Musculoskelet. Res. 21, 1–13 (2018).
Basti, A. et al. Diurnal variations in the expression of core-clock genes correlate with resting muscle properties and predict fluctuations in exercise performance across the day. BMJ Open Sport Exerc. Med. 7, 1–16. https://doi.org/10.1136/bmjsem-2020-000876 (2021).
Standley, P. R. My personal journey that led to the crossroads of interdisciplinary manual medicine research: Serendipitous opportunities afforded a basic scientist. J. Am. Osteopath. Assoc. 113, 179–183. https://doi.org/10.7556/jaoa.2013.113.2.179 (2013).
Standley, P. R. Towards a Rosetta Stone of manual therapeutic methodology. J. Bodyw. Mov. Ther. 18, 586–587. https://doi.org/10.1016/j.jbmt.2014.06.004 (2014).
Lorenc, Z. P., Smith, S., Nestor, M., Nelson, D. & Moradi, A. Understanding the functional anatomy of the frontalis and glabellar complex for optimal aesthetic botulinum toxin type A therapy. Aesthetic Plast. Surg. 37, 975–983. https://doi.org/10.1007/s00266-013-0178-1 (2013).
Macdonald, M. R., Spiegel, J. H., Raven, R. B., Kabaker, S. S. & Maas, C. S. An anatomical approach to glabellar rhytids. JAMA Otolaryngol. Head Neck Surg. 124, 1315–1320. https://doi.org/10.1001/archotol.124.12.1315 (1998).
Acknowledgements
We like to express our gratitude to (i) the students and staff of the Osteopathie Schule Deutschland for their participation and assistance during the trial; (ii) Alexander Karner, MSc, Christian Selzle, MSc, Stephan Rohde, MSc, and Charline Krohn for providing intellectual, organizational, and spatial support; (iii) Ass. Prof. Jan Porthun, MMMSc for helpful discussions about the study design and statistics; and (iv) Dr. Christine Lohr, MSc, and Marius Dickmann, MSc for proofreading the manuscript and providing thoughtful comments.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
L.B.: Conceptualization, Methodology, Writing—Original Draft, Writing—Review & Editing, Visualization, Supervision, Project administration; J.S.: Formal analysis, Investigation, Writing—Review & Editing, Visualization; J.R.: Investigation, Writing—Review & Editing; B.G.: Investigation, Writing—Review & Editing, Project administration; C.L.: Investigation, Writing—Review & Editing; A.K.: Formal analysis, Writing—Review & Editing; A.B.: Formal analysis, Writing—Review & Editing; T.S.: Writing—Review & Editing, Supervision.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bohlen, L., Schwarze, J., Richter, J. et al. Effect of osteopathic techniques on human resting muscle tone in healthy subjects using myotonometry: a factorial randomized trial. Sci Rep 12, 16953 (2022). https://doi.org/10.1038/s41598-022-20452-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-20452-9
- Springer Nature Limited