
Abstract
Although national health-related quality of life population norms had been published based on the EuroQol 5-Dimensions 5-levels scale, China is a vast country with diverse cultural and social development in various regions. Therefore, regional population norms may better reflect the health status of residents in a given area. The purpose of the study was to derive the HRQoL population norm for adult general population in southern Jiangsu Province using the EQ-5D-5L scale and explore potential influencing factors. The data were based on a cross-sectional survey conducted in Liyang City from March 2019 to July 2020. EQ-5D-5L utility scores based on Chinese value set and EQ-VAS scores were used to assess HRQoL. The Tobit regression model and generalized linear model were performed to identify the association among potential covariates and HRQoL. The means (95% confidence interval) of the EQ-5D-5L utility scores and EQ-VAS scores were 0.981(0.980–0.983) and 83.6(83.2–83.9), respectively. Younger people (≤ 40 years old) were more likely to experience problems with anxiety or depression. Additionally, women had lower HRQoL scores although multivariate analysis found no statistical difference between the sexes. Lower HRQoL was associated with advanced age, lower socioeconomic status, no spouse, lack of regular physical activities, smoking cessation, and chronic non-communicable diseases. Subjects who declared that they were afflicted by diseases presented significantly lower utility scores, ranging from 0.823 (0.766–0.880) for memory-related diseases to 0.978 (0.967–0.989) for hepatic diseases. Regional population norms of HRQoL are needed in the health economic study owing to the great socioeconomic differences across regions in China. The present study provides HRQoL population norms for adults in southern Jiangsu. These norm values could help policy makers better allocate limited health resources and prioritize service plans.
Similar content being viewed by others


Introduction
In recent years, economic evaluation has been widely adopted to guide clinical practice and public health policy decisions1. One of the most frequently reported benefit measurements in economic evaluations is quality-adjusted life years, which combines the quality of life and length of life into a single health-related quality of life (HRQoL) score2. If a study does not have a control group and wants to evaluate the effect of its intervention, an estimate for HRQoL utility score norms in the general population can serve as a reference group2. Moreover, population norms enable researchers to compare profiles of patients with particular diseases with data on the health status of the general population of similar age and sex and measure health inequalities3. HRQoL population norms can also be treated as the key to determining whether the scores of a specific group or individual are above or below the average level for a similar population4. Therefore, assessing the HRQoL of the general population to construct population norms is helpful for long-term monitoring of health status, determining groups with poor HRQoL, assessing the burden of diseases on HRQoL, and exploring the relationship between different sociodemographic factors and health status5 and ultimately optimizing the efficiency of medical resource allocation. Therefore, it is becoming an inevitable requirement for the development of healthcare in each country.
HRQoL is a self-reported outcome that is increasingly used to monitor the health status of the general population. It is a multidimensional concept that reflects the physical, psychological, social and emotional well-being of the respondents6. To date, there are many different instruments for measuring HRQoL, including the EuroQol five-dimension (EQ-5D), Health Utilities Index (HUI)7, and the Short -form 6-dimension (SF-6D)8. The EQ-5D is one of the major self-reported instruments to evaluate HRQoL due to its simplicity, low respondent burden and high universal acceptance9,10. There are two versions of the EQ-5D, namely, the EQ-5D-3L and the EQ-5D-5L. In recent studies, the EQ-5D-5L has been widely used because it can reduce the ceiling effect (the proportion of respondents reporting “no problems” for all dimensions) detected in the EQ-5D-3L11. This method has higher convergence validity and is more sensitive to slight health changes12,13. Additionally, an existing EQ-5D-5L value set from the Chinese adult general population is now available14. In a given region of China (e.g., southern Jiangsu), the study on the evaluation of HRQoL in the general population by the EQ-5D-5L scale is still quite limited. Therefore, this EQ-5D-5L scale was used to evaluate the quality of life of the respondents in this study.
In the field of public health, the population norm (average population score) of a region is often expressed as the EQ-5Dutility score15, and the population norm is the benchmark for evaluating population health care and health equity. Although the EQ-5D-5L population norm has been reported in China's urban population16, due to its small sample size (1332 people were included in 5 regions), it may not be well representative of the rest of China, let alone southern Jiangsu, which has a relatively developed economic level. The southern region of Jiangsu Province (including Nanjing, Suzhou, Wuxi, Changzhou, Zhenjiang) is located in the centre of the Yangtze River Delta along the southeast coast of China, with over 30 million permanent residents17. All counties (cities) have entered the ranks of the top 100 counties of national comprehensive strength, of which 7 counties (cities) have entered the top 10, which is one of the most developed and modernized regions in China. Therefore, the HRQoL norm in this region can provide a reference for the health level of the population in most developed regions of China. Furthermore, China is a vast country, and the cultural and social development of each province is different18. Thus, regional population norms may better reflect the health status of residents in a given area. The main purpose of this study is to derive the HRQoL population norms in the southern area of Jiangsu Province, China based on a large number of randomly sampled data from the Liyang Chronic Disease Risk Factor Monitoring Cohort Study (The Liyang Study) and the EQ-5D-5L China value set. Second, we examine the association between sociodemographic characteristics, health needs and HRQoL.
Methods
Study design and data collection
The Liyang Study is a face-to-face cross-sectional observational study conducted between March 2019 and June 2020. Liyang is located in the south of Jiangsu Province, with a permanent, year-round population of approximate 0.8 million in 2019. As one of the top 100 counties (top 100 in comprehensive strength of all counties, county-level cities and some municipal districts in China) in China (No. 35), Liyang lies at the crossroads of the Nanjing metropolitan area and Shanghai economic zone. Therefore, the HRQoL status of the general population in Liyang can reflect the basic situation of the population in southern Jiangsu to a certain extent. The method of multi-stage cluster random sampling was adopted to randomly select 17 health centres in 12 towns of Liyang City for investigation (Supplementary Fig. 1). We designed a standardized questionnaire including sociodemographic characteristics, behavioural lifestyle factors, health-related information, and the EQ-5D scale to collect data.
We preliminarily planned to conduct a large-scale survey covering ten thousand people among the general population of Liyang City. First, to ensure a sufficient sample size and facilitate implementation and calculation, a random sample of approximately 600 cases from each of the 17 health centres was planned for the survey. However, the actual final sample size varied from 443 to 633 per site (an average of 600 cases per health centre) for some reason, such as the absence of an address, some residents refusing to be surveyed or being physically unable to be surveyed (Supplementary Table 1). Furthermore, two administrative villages or communities closest to each health centre were selected and approximately 300 cases were randomly selected from each village or community as the investigation objective. Then, under the auspices of the local CDC, randomly selected residents were asked to go to the nearest health centre (or community hospital) for an investigation. Next, trained local health workers were recruited to conduct a questionnaire survey for each selected participant through face-to-face interviews at each health centre, and the interviews were recorded for subsequent quality control. The questionnaires were issued and retrieved on the same day, and missing or incorrect items were supplemented, proofread and logically corrected on time. The inclusion criteria were as follows: local permanent residents (living ≥ 6 months in local before investigation), age ≥ 18 years, complete sociodemographic information, and completion of the EQ-5D-5L scale. Before the study began, participants were informed about the purpose of the study, its health benefits and potential harms. Participants were asked to give written informed consent, and both researchers and respondents agreed to use the data only for scientific research purposes. This study was approved by the Ethics Review Committee of Soochow University and all respondents provided written informed consent. All methods were performed in accordance with the relevant guidelines and regulations.
EQ-5D-5L
The EQ-5D-5L scale for the determination of the population HRQoL consists of a five-dimensional health description system and a self-reported overall health score using the EuroQol Visual Analog Scale (EQ-VAS). The descriptive system comprises the dimensions of mobility (MO), self-care (SC), usual activities (UA), pain/discomfort (PD), and anxiety/depression (AD), and each dimension has five levels of response (from “no problems” to “extreme problems”)19. To better understand the distribution of health problems experienced by respondents, we converted each dimension into the dichotomous variables of "0"(no problems) and "1"(problems, slight/moderate/severe/extreme problems are collectively referred to as “problems”). The utility score is generated by applying the Chinese time trade-off model developed by Liu et al.20. The utility score ranges from − 0.391 for the worst (55,555) to 1 for the best (11,111) EQ-5D-5L health states. The EQ-VAS score is the self-reported overall health perception of the respondents. It records the respondent’s self-rated health on a vertical scale from 0 (the worst health) to 100 (the best health), where the respondents picture their health status on the interview day. Respondents with high utility scores or VAS scores had a better HRQoL than those with low scores.
Ethical approval
This study was approved by the Ethics Review Committee of Soochow University and all respondents provided written informed consent.
Consent to participate
All respondents provided written informed consent prior to the interview.
Covariates
Sociodemographic factors
Sociodemographic factors including sex, age (18–30, 31–40, 41–50, 51–60, 61–70, and 70 + years), residence(urban/rural), education level (primary school and below, junior middle school, high school or similar and junior college and above), marital status(married, unmarried/divorced/widowed), annual household income (< 50,000 yuan, 50,000–99,999 yuan, 10,0000–14,9999, and ≥ 15,0000 yuan, RMB), employment status(employed/full-time/part-time, unemployment/retirement/housework/student), and body mass index(BMI, low BMI, < 18.5 kg/m2; normal BMI, between 18.5 and 24.0 kg/m2; overweight BMI, between 24.0 and 28.0 kg/m2; and obese BMI, ≥ 28.0 kg/m2, following recommendations from the Working Groupon Obesity in China21).
Behavioural lifestyle factors
Behavioural variables included: smoking, defined as at least one cigarette per day for 6 months (never, current, or former); alcohol consumption, defined as at least once a month (never, current); and regular physical activity, defined as moderately intense activity lasting more than 10 min at least once a week (yes, no)22.
Health-related factors
The participants were also asked whether they had a health problem affecting HRQoL (e.g., mental illness, memory-related illness), and their general health needs. Health needs were measured by chronic non-communicable diseases (NCDs), which included hypertension, diabetes, dyslipidemia, stroke, coronary heart disease (CHD), asthma, chronic obstructive pulmonary disease (COPD) and cancer. NCDs were defined as a condition diagnosed by a doctor from a secondary or above medical institution, for which either the symptoms persisted or relevant medical treatment continued over the last 12 months23. Participants were classified as having no NCDs, or one, two or more NCDs.
Statistical analysis
Frequencies and percentages were used for categorical variables, and all covariates including age were entered into the model as categorical variables. Means and 95% confidence intervals [CIs] were calculated for the continuous variables (including the EQ-5D-5L utility score and EQ-VAS score). The differences in utility scores and VAS scores between different subgroups were tested by employing Wilcoxon or Kruskal–Wallis tests. The Wilcoxon test was also used to describe differences in utility scores and EQ-VAS scores between men and women for age categories, education levels, income levels, and BMI categories. To deeply understand the impact of health restrictions in each EQ-5D dimension on HRQoL, we converted each dimension of the EQ-5D scale into binary variables with or without health problems, and then calculated the mean utility scores and VAS scores of respondents with or without health problems in each dimension respectively. Mann–Whitney test was used to examine the difference in the mean utility score and VAS score in different dimensions of the EQ-5D-5L scale. In addition, the chi-square test was used to compare the incidence of problems for each EQ-5D dimension by gender and age.
The relationships between all covariates and EQ-VAS scores were explored using a generalized linear model (GLM) with a Poisson distribution and a log link based on the modified Park test24. Since the distribution of the EQ-5D utility scores was skewed and censored at 1, we used the multivariate Tobit regression model to evaluate the relationship between the EQ-5D utility score and potential influencing factors25. All data analysis was performed in SAS version 9.4(SAS Institute Inc., Cary, NC, USA) and STATA version 15.0. A P value below 0.05 was considered statistically significant.
Results
Sample characteristics
A total of 10,200 individuals aged 18 and above participated in the study, 144 of whom were excluded because they did not meet the inclusion criteria, leaving 10,056(response rate: 98.6%) respondents who enrolled in this study. All respondents completed the five dimension sections of the EQ-5D-5L scale, but only 5080(53.8%) respondents completed the EQ-VAS score section. The sociodemographic characteristics and health needs of the respondents are summarized in Table 1.
EQ-5D-5L utility score and EQ-VAS score according to the baseline characteristics
The respondents possessed a mean EQ-5D-5L utility score of 0.981(0.980–0.983) (95%CI) and a mean EQ-VAS score of 83.6(83.2–83.9). Subjects with lower utility scores were those who were elderly, were women, lived in rural areas, were ex-smokers, were unmarried/divorced/widowed, had no paid employment, had high BMI, had a lower education level or lower annual household income, lacked regular physical activity and suffered from one or more NCDs (All P < 0.05, Table 1). Similar results were observed for EQ-VAS scores except for sex and drinking (Supplementary Table 2).
Distribution of EQ-5D-5L utility score and EQ-VAS score
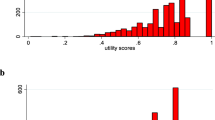
The EQ-5D-5L utility score ranged from − 0.251 to 1, which was left-skewed with the dominant value at 1.00 (i.e., “Full health”). Only 7 subjects had negative utility scores. Of the subjects, 85.6% had the highest utility score (EQ-5D-5L utility score = 1, 11,111 health states). Similarly, the EQ-VAS score ranged from 0 to 100, which was also left-skewed with the major clustering from 80 to 100 (i.e., “the best health you can imagine”). Only 23.6% of subjects had an EQ-VAS score of 90 and above. The other most common health states were 11,121, 11,112, 11,122, and 22,221 in the proportions of 6.4%, 1.3%, 1.2%, and 0.2%, respectively.
EQ-5D-5L utility score and EQ-VAS score according to health conditions by gender
For men, the condition that had the greatest impact on quality of life was memory-related diseases, followed by stroke and mental diseases, while for women, stroke was the most significant, followed by memory-related diseases and asthma (Table 2). In terms of EQ-VAS scores, slightly different from the utility scores, men with COPD had the lowest VAS scores, while women were still most affected by stroke (Supplementary Table 3).
EQ-5D-5L utility scores for age, education, income, and BMI according to gender
The EQ-5D-5L utility score was presented by age, education level, income, and BMI and was divided according to sex. In general, utility scores are higher in men than in women, with especially significant differences in the 41–50 and 61 + age groups, and the scores for both sexes decline with age. Education level, income and BMI also appeared to influence utility scores in which people with low education, low income and a BMI of 24.0 and above generally scored lower. In addition, we found that men and women had different utility scores in household annual income and BMI (All P < 0.05, Table 3).
EQ-5D-5L utility score and EQ-VAS score according to health problems in each dimension
Utility scores and VAS scores varied significantly according to whether the respondents reported any problems in each dimension. Overall, in terms of the EQ-5D-5L utility score, respondents reporting one problem had a utility score of 0.13 points lower than respondents reporting no problems (All P < 0.001, Table 4). Regarding the EQ-VAS, people without problems had 6 scores points higher than people with at least one problem (All P < 0.001, Supplementary Table 4).
Health problems reported by respondents
The highest proportion of all respondents reported problems in PD (11.96%), followed by AD (4.68%), while the lowest percentage reported problems in SC (1.34%). The percentage of reported problems with MO, UA, SC, and PD increased with age in the total, male, and female samples, respectively. In contrast, younger age groups (age 18–30 and age 31–40) reported more health restrictions with AD (All P < 0.001, Table 5).
Potential influencing factors of HRQoL
Advanced age, living in rural regions, no spouse, quitting smoking, lack of regular physical activity, and suffering from NCDs had a statistically negative impact on HRQoL. In contrast, higher education level, higher annual income, and paid employment exerted a positive effect on HRQoL, as measured by the utility score (All P < 0.05, Table 6). The results for the EQ-VAS score were similar, although not statistically significant for physical activity (All P < 0.05, Supplementary Table 5).
Sensitivity analysis for missing data
Sensitivity analyses were conducted to evaluate the impact of missing values on the EQ-VAS score. The results showed that there was basically no statistical difference between respondents with EQ-VAS scores and all the respondents (Supplementary Table 6). Therefore, the remaining VAS scores could be a good representation of all respondents.
Discussion
Our study identified some sociodemographic factors influencing HRQoL: old age, lower education levels, lower income levels, residence in rural areas, no spouse, no paid work, lack of regular physical activities and ex-smokers. In addition, NCDs had a significant impact on HRQoL. To our knowledge, this is the first study to estimate the HRQoL population norms for residents in southern Jiangsu Province of China using the EQ-5D-5L questionnaire based on a randomly selected large sample data. The population norms in the study can be used as reference data to compare profiles for patients with specific conditions with data for the average person in the general population in a similar age and gender group3 and provide evidence for evaluating the effectiveness of future public health interventions. To date, studies have determined the EQ-5D-5L population criteria of other provinces in China, while few studies have included Jiangsu Province, and those that do include Jiangsu adopt very small and unrepresentative sample sizes16,26,27. In addition, previous studies have shown that the EQ-5D-5L scale can effectively reduce the ceiling effect on the 3L scale28,29, so the 5L scale is used in this study.
Generally, the mean EQ-5D-5L utility score is 0.98, which is similar to that of the USA (0.97)30, slightly higher than that of the urban population in China (0.96)16, and significantly higher than those of Poland (0.89)31, and Portugal (0.89)28. The mean VAS score (83.57) is higher than the national average (80.12) of China23. However, a direct comparison of utility scores between different countries or regions is not recommended because regions have different sociodemographic compositions and health policies, which may influence respondents' choice of different dimensions of the EQ-5D scale32. The findings showed that the respondents experienced greater problems with PD and AD and fewer problems with SC and UA, which is consistent with the EQ-5D-5L population studies in other countries5,31,33. Approximately 12% of participants reported PD, similar to the Chinese average23 but well below the averages reported by Poland, the United States, and Greece34,35,36. Interestingly, AD was more common in younger adults (40 years and younger), as has been reported elsewhere16,26. One possible explanation is that the younger generation feels more psychological pressure than the older generation because of the fast pace of life in developed cities16.
Ageing presents a great challenge to the world, in both developed and developing nations37. HRQoL tended to deteriorate with age, as observed in other studies5,23,31,33,38,39. As expected, elderly people were more likely to experience problems in all EQ-5D-5L dimensions. The multivariate models established in our study showed that NCDs were a significant predictor of HRQoL. NCDs have become a major cause of death worldwide40. People with NCDs had lower utility scores and VAS scores resulting in a worse HRQoL. This is consistent with relevant research results27,41.
Previous studies have shown that HRQoL inequality exists in different socioeconomic regions in China, such as Hong Kong (utility score 0.920)26 and the urban population in mainland China (0.957)16,24. Our study also confirmed this phenomenon: people with higher socioeconomic status (higher income, better education, and paid employment) had better HRQoL, which was consistent with previous studies23,42,43. An individual's socioeconomic status is often represented by education, income and employment23,44. Educational attainment is the most important of the three factors that constitute an individual's socioeconomic status because it is fairly stable throughout the life course of a person. Furthermore, it can shape one's career and expected income potential. Through this mechanism, its indirect link to health is stronger than its direct impact45.
In addition, those without a spouse tended to have a lower HRQoL. These people may experience social isolation and financial stress, which could lower their well-being46. People who often engaged in physical activity had relatively better HRQoL. Regularly undertaking both aerobic and muscle-strengthening activities, such as walking and cycling, have significant benefits for health47. Our study also found an interesting phenomenon: ex-smokers had significantly lower utility scores. This is similar to the findings of Choi et al., who suggest that there may be a "healthy smoker" phenomenon, where smokers believe that smoking relieves pain and stress, while ex-smokers are likely forced to quit smoking due to a disease48.
One advantage of our study is that it has a sufficient sample size (10,056) and a high respondent response rate (98.59%) and is generally representative of the general population in the south of Jiangsu Province. In addition, Tobit regression and GLM were used to replace the traditional linear regression model in the multivariate analysis, which was in line with the distribution characteristics of health utility value and EQ-VAS score, making the analysis results more follow the actual situation. Finally, this study provides utility scores and VAS scores for various diseases, which is rare in related studies49 and could be useful for health policymakers when prioritizing resource allocation.
There are some weaknesses worth mentioning in the present study. First, as a cross-sectional design, the correlation between HRQoL and potential variables cannot be interpreted as causal. Moreover, approximately 50% of respondents had missing values for the EQ-VAS. Further analysis indicates that the distribution of all sociodemographic variables for the sample with missing EQ-VAS score values was generally consistent with that for the sample with complete EQ-VAS scores.
Conclusions
This is the first study to provide HRQoL norms using the EQ-5D-5L scale for adults in southern Jiangsu, China and explore its potential influencing factors. These norm values can be used to rationalize the allocation of limited health resources and to evaluate and compare the effects of different medical interventions in health care. In addition, the study found evident socioeconomic inequalities in HRQoL. Therefore, health inequalities deserve the attention of policymakers, and targeted research on each HRQoL domain can promote further understanding of underlying characteristics of inequalities and identify effective strategies to address them to promote greater equity.
References
Ravens-Sieberer, U. Measuring and monitoring quality-of-life in population surveys: Still a challenge for public health research. Soz. Praventivmed. 47, 203–204 (2002).
Poder, T. G., Carrier, N. & Kouakou, C. R. C. Quebec health-related quality-of-life population norms using the EQ-5D-5L: Decomposition by sociodemographic data and health problems. Value Health J. Int. Soc. Pharmacoecon. Outcomes Res. 23, 251–259 (2020).
Hołownia-Voloskova, M., Tarbastaev, A. & Golicki, D. Population norms of health-related quality of life in Moscow, Russia: The EQ-5D-5L-based survey. Qual. Res. Int. J. Qual. Asp. Treat. Care Rehabilit. 30, 831–840 (2021).
Hopman, W. M. et al. Canadian normative data for the SF-36 health survey. Canadian multicentre osteoporosis study research group. CMAJ Can. Med. Assoc. J. 163, 265–271 (2000).
McCaffrey, N. et al. Health-related quality of life measured using the EQ-5D-5L: South Australian population norms. Health Qual. Life Outcomes 14, 133 (2016).
Carr, A. J., Gibson, B. & Robinson, P. G. Measuring quality of life: Is quality of life determined by expectations or experience?. BMJ 322, 1240–1243 (2001).
Feeny, D. et al. Multi-attribute health status classification systems. Health Util.ities Index. Pharmacoeconomics 7, 490–502 (1995).
Brazier, J., Roberts, J. & Deverill, M. The estimation of a preference-based measure of health from the SF-36. J. Health Econ. 21, 271–292 (2002).
Chen, P. C. et al. The relationship between smoking status and health-related quality of life among smokers who participated in a 1-year smoking cessation programme in Taiwan: A cohort study using the EQ-5D. BMJ Open 5, e007249 (2015).
Cunillera, O. et al. Discriminative capacity of the EQ-5D, SF-6D, and SF-12 as measures of health status in population health survey. Qual. Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 19, 853–864 (2010).
Devlin, N. J. & Brooks, R. EQ-5D and the EuroQol Group: Past, present and future. Appl. Health Econ. Health Policy 15, 127–137 (2017).
Feng, Y., Devlin, N. & Herdman, M. Assessing the health of the general population in England: How do the three- and five-level versions of EQ-5D compare?. Health Qual. Life Outcomes 13, 171 (2015).
Nguyen, L. H. et al. Quality of life profile of general Vietnamese population using EQ-5D-5L. Health Qual. Life Outcomes 15, 199 (2017).
Luo, N. et al. Estimating an EQ-5D-5L value set for China. Value Health J. Int. Soc. Pharmacoecon. Outcomes Res. 20, 662–669 (2017).
Norman, R. et al. Australian health-related quality of life population norms derived from the SF-6D. Aust. N. Z. J. Public Health 37, 17–23 (2013).
Yang, Z. et al. EQ-5D-5L norms for the urban Chinese population in China. Health Qual. Life Outcomes 16, 210 (2018).
Yang, J. & Ding, H. A quantitative assessment of sustainable development based on relative resource carrying capacity in Jiangsu Province of China. Int. J. Environ. Res. Public Health 15(12), 2786 (2018).
Sun, S. et al. Regional differences in health status in China: Population health-related quality of life results from the National Health Services Survey 2008. Health Place 17, 671–680 (2011).
Luo, N. et al. Developing the Chinese version of the new 5-level EQ-5D descriptive system: The response scaling approach. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 22, 885–890 (2013).
Liu, G. G. et al. Chinese time trade-off values for EQ-5D health states. Value Health J. Int. Soc. Pharmacoecon. Outcomes Res. 17, 597–604 (2014).
Jia, W. Obesity in China: Its characteristics, diagnostic criteria, and implications. Front Med. 9, 129–133 (2015).
Tierney, M., Fraser, A. & Kennedy, N. Criterion validity of the international physical activity questionnaire short Form (IPAQ-SF) for use in patients with rheumatoid arthritis: Comparison with the SenseWear Armband. Physiotherapy 101, 193–197 (2015).
Sun, S. et al. Population health status in China: EQ-5D results, by age, sex and socio-economic status, from the National Health Services Survey 2008. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 20, 309–320 (2011).
Li, H. et al. Inequalities in health status among rural residents: EQ-5D findings from household survey China. Int. J. Equity Health 13, 41 (2014).
Austin, P. C., Escobar, M. & Kopec, J. A. The use of the Tobit model for analyzing measures of health status. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 9, 901–910 (2000).
Wong, E. L. et al. Normative profile of health-related quality of life for Hong Kong general population using preference-based instrument EQ-5D-5L. Value Health J. Int. Soc. Pharmacoecon. Outcomes Res. 22, 916–924 (2019).
Huang, W. et al. Assessing health-related quality of life of Chinese adults in Heilongjiang using EQ-5D-3L. Int. J. Environ. Res. Public Health 14(3), 224 (2017).
Ferreira, L. N. et al. Comparing the performance of the EQ-5D-3L and the EQ-5D-5L in young Portuguese adults. Health Qual. Life Outcomes 14, 89 (2016).
Shiroiwa, T. et al. Comparison of value set based on DCE and/or TTO Data: Scoring for EQ-5D-5L health states in Japan. Value Health J. Int. Soc. Pharmacoecon. Outcomes Res. 19, 648–654 (2016).
Augustovski, F. et al. An EQ-5D-5L value set based on Uruguayan population preferences. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 25, 323–333 (2016).
Golicki, D. & Niewada, M. EQ-5D-5L Polish population norms. Arch. Med. Sci. 13, 191–200 (2017).
Szende, A. et al. (eds) Self-Reported Population Health: An International Perspective based on EQ-5D (Springer, Dordrecht (NL), 2014).
Hinz, A. et al. The quality of life questionnaire EQ-5D-5L: Psychometric properties and normative values for the general German population. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 23, 443–447 (2014).
Golicki, D. et al. Self-assessed health status in Poland: EQ-5D findings from the Polish valuation study. Pol. Arch. Med. Wewn. 120, 276–281 (2010).
Luo, N. et al. Validity and reliability of the EQ-5D self-report questionnaire in Chinese-speaking patients with rheumatic diseases in Singapore. Ann. Acad. Med. Singap. 32, 685–690 (2003).
Kontodimopoulos, N. et al. Validity of the EuroQoL (EQ-5D) instrument in a Greek general population. Value Health J. Int. Soc. Pharmacoecon. Outcomes Res. 11, 1162–1169 (2008).
Zhang, N. J., Guo, M. & Zheng, X. China: Awakening giant developing solutions to population aging. Gerontologist 52, 589–596 (2012).
Abdin, E. et al. Measuring health-related quality of life among adults in Singapore: Population norms for the EQ-5D. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 22, 2983–2991 (2013).
Shiroiwa, T. et al. Japanese population norms for preference-based measures: EQ-5D-3L, EQ-5D-5L, and SF-6D. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 25, 707–719 (2016).
Mendis, S., Davis, S. & Norrving, B. Organizational update: the world health organization global status report on noncommunicable diseases 2014; one more landmark step in the combat against stroke and vascular disease. Stroke 46, e121–e122 (2015).
Rezaei, S. et al. Determinants of health-related quality of life in Iranian adults: Evidence from a cross-sectional study. Epidemiol. Health 39, e2017038 (2017).
Kularatna, S. et al. EQ-5D-3L derived population norms for health related quality of life in Sri Lanka. PLoS ONE 9, e108434 (2014).
Health-related quality of life and psychological distress among cancer survivors in Southeast Asia: results from a longitudinal study in eight low- and middle-income countries. BMC Med. 2017; 15: 10.
Grundy, E. & Holt, G. The socioeconomic status of older adults: How should we measure it in studies of health inequalities?. J. Epidemiol. Community Health 55, 895–904 (2001).
Singh-Manoux, A., Clarke, P. & Marmot, M. Multiple measures of socio-economic position and psychosocial health: Proximal and distal measures. Int. J. Epidemiol. 31(6), 1192–1199 (2002).
Wickrama, K. A. et al. Changes in family financial circumstances and the physical health of married and recently divorced mothers. Soc. Sci. Med. 63, 123–136 (2006).
Bull, F. C. et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 54, 1451–1462 (2020).
Choi, D., Ota, S. & Watanuki, S. Does cigarette smoking relieve stress? Evidence from the event-related potential (ERP). Int. J. Psychophysiol. 98, 470–476 (2015).
van den Berg, B. Sf-6d population norms. Health Econ. 21, 1508–1512 (2012).
Funding
This work was supported by the National Natural Science Foundation of China (project number 81973143) and the Priority Academic Program Development of Jiangsu Higher Education Institutions (PAPD). All of the authors have participated actively in this study, and agree to the content of the manuscript and their being listed as an author on the paper.
Author information
Authors and Affiliations
Contributions
Study design: W.H., L.Z., J.C., Y.S.. Data collection and management: W.H., N.S., X.C. Data analyses: W.H., S.L. All authors were involved in the manuscript preparation and all authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hu, W., Zhou, L., Chu, J. et al. Estimating population norms for the health-related quality of life of adults in southern Jiangsu Province, China. Sci Rep 12, 9906 (2022). https://doi.org/10.1038/s41598-022-13910-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-13910-x
- Springer Nature Limited
This article is cited by
-
Risk-based lung cancer screening in heavy smokers: a benefit–harm and cost-effectiveness modeling study
BMC Medicine (2024)
-
Cancer population norms using a new value set for the SF-6Dv2 based on the preferences of patients with breast or colorectal cancer in Quebec
Quality of Life Research (2024)
-
Examining the relationship between the Short Warwick-Edinburgh Mental Well-being Scale (SWEMWBS) and EQ-5D-5L and comparing their psychometric properties
Health and Quality of Life Outcomes (2023)
-
Evaluation of health-related quality of life among the older adults with and without hypertension: results of a cross-sectional study
Journal of Public Health (2023)