
Abstract
The focus of this study was to explore the association between the non-HDL-cholesterol to HDL-cholesterol (non-HDLc/HDLc) ratio and mortality in septic patients. This was a retrospective cohort study of patients with sepsis in the eICU Collaborative Research Database (eICU-CRD) from 208 distinct ICUs across the United States between 2014 and 2015 that explored. All-cause mortality within 28 days after ICU admission. A multivariable logistic regression model was used to estimate the risk of death. Of the 724 patients with a median age of 68 years, 43 (5.94%) died within 28 days after ICU admission. When the non-HDLc/HDLc ratio was < 3.3, the mortality rate decreased with an adjusted odds ratio (OR) of 0.60 (95% CI 0.37–0.99, P = 0.043) for every 1 increment in the non-HDLc/HDLc ratio. When the non-HDLc/HDLc ratio was ≥ 3.3, the mortality rate increased with an adjusted OR of 1.28 (95% CI 1.01–1.62, P = 0.039) for every one increment in the non-HDLc/HDLc ratio. For patients with sepsis, the association between the non-HDLc/HDLc ratio and the 28-day mortality risk was a U-shaped curve. A higher or lower non-HDLc/HDLc ratio was associated with an increased risk of 28-day mortality.
Similar content being viewed by others


Introduction
Sepsis is a common and lethal syndrome. The systemic inflammatory response is biologically complex, redundant, and activated by infectious and noninfectious triggers. Its manipulation can bring benefits and harm1. Therefore, a closer examination of the phenotypes and subphenotypes of patients who exhibit strong survival signals in sepsis may enable us to understand novel mechanisms for improving treatment.
High-density lipoprotein-cholesterol (HDLc) or low-density lipoprotein-cholesterol (LDLc) cholesterol is inversely associated with coronary heart disease (CHD)2,3 and can respond differently to changes in diet and treatment. A pool of 458 population-based studies involving 82.1 million participants in 23 countries in Asia and in western Korea found that HDL cholesterol increased in many Western countries, Japan and South Korea4. The non-HDLc to high-HDLc (non-HDLc/HDLc) ratio can be obtained from the standard lipid profile without additional cost and is highly correlated with levels of LDL particle number4, which has been confirmed as a strong cardiovascular risk marker by multiple studies5,6. We previously showed that non-HDLc/HDLc ratio is an independent risk factor for the development of chronic kidney disease (CKD)7.
A recent clinical study showed that during a median follow-up of 1.72 years, the mortality rate associated with the range of LDLc/HDLc ratios was U-shaped in hypertensive patients8. A retrospective cohort study conducted at a tertiary-care academic medical centre found an association of presepsis baseline LDLc and triglyceride levels with hospital mortality in sepsis. This showed that high (≥ 200 mg/dL) or low levels (≤ 75 mg/dL) of both led to increased mortality. However, there is a lack of evidence to guide the emergency management of patients with sepsis.
We hypothesised that in patients with sepsis, even high and low non-HDLc/HDLc ratios are associated with a higher risk of all-cause mortality within 28-days after admission to the intensive care unit (ICU). In this retrospective multicentre cohort study, we used the eICU Collaborative Research Database (eICU-CRD) from the Philips Healthcare eICU program from 208 distinct ICUs in the United States between 2014 and 2015. We aimed to explore the threshold of the non-HDLc/HDLc ratio where the risk of death significantly increases, which is a high priority in patients with sepsis.
Methods
Data source
This was a retrospective observational study in which data were extracted from an online international database, the eICU Collaborative Research Database (eICU-CRD)9. The eICU-CRD is a multicentre ICU database with high granularity data for over 200,000 admissions to ICUs monitored by eICU programme across the United States. From 2014 to 2015, all data were automatically stored through the Philips Healthcare eICU program and retrieved electronically9. The eICU-CRD has been used for observational research10,11,12. It is possible to access this database by passing an examination and obtaining a certification in accordance with the data usage agreement of the PhysioNet Review Board. The utilized database is released under the Health Insurance Portability and Accountability Act (HIPAA) Safe Harbor provision. Access to the data was approved after completing the Collaborative Institutional Training Initiative (CITI) program “Data or Specimens Only Research”. The study was exempt from approval from the institutional review board of the Massachusetts Institute of Technology (our record ID: 40859994) due to the retrospective design, lack of direct patient intervention, and the security schema for which the reidentification risk was certified as meeting safe harbor standards by Privacert (Cambridge, MA). Informed consent was waived for the same reason. The study was performed in accordance with the Declaration of Helsinki. All methods were performed in accordance with the relevant guidelines and regulations.
Study population
All patients diagnosed with sepsis on admission to the ICU were included. Sepsis was defined as suspected or documented infection plus an acute increase in Sequential Organ Failure Assessment (SOFA) score greater than 2 points13 recorded in the Acute Physiology and Chronic Health Evaluation (APACHE) IV dataset14. Infection was identified from the ICD-9 code in the eICU Collaborative Research Database. The following exclusion criteria were used: (1) not first ICU admission, (2) ICU stay < 48 h, (3) < 18 years old, (4) missing ICU outcome, and (5) missing total cholesterol after ICU admission or system error. The study flowchart was presented in Fig. 1.

Flow chart of study population. ICU intensive care unit.
Variables
The eICU database includes demographic records, physiological indicators of bedside monitors, diagnosis via the International Classification of Diseases, 9th Edition, Clinical Modification (ICD-9-CM) codes, and other laboratory data obtained during routine medical care.
All participant data within the first 24 h after hospital admission were collected from the eICU-CRD. The physiological variables, including temperature (°C), respiratory rate, heart rate (HR) and mean arterial pressure (MAP), were obtained from the apacheApsVar table. Baseline characteristics such as age, gender, ethnicity, and weight were collected from the tables of patient and apachePatientResult tables. The laboratory indices of lactate level, total cholesterol, triglycerides, HDLc, and LDLc were collected from the laboratory tables. Non-HDLc refers to total cholesterol (TC), including cholesterol in atherogenic lipoproteins, minus HDLc. Comorbidities including acute immunodeficiency syndrome (AIDS), hepatic failure, metastatic cancer, leukaemia, immunosuppression, and cirrhosis were extracted from the APACHE IV score. Septic shock was defined as sepsis with a septic shock diagnosis code and was extracted from the table diagnosis table. Severity at admission was measured by the SOFA score, Apache IV score, Glasgow Coma Scale (GCS) score, and Acute Physiology Score III.
Outcomes
The outcome of the study was all-cause ICU mortality within 28 days after admission to the ICU. In the supplemental analysis, we also analysed the 14-day mortality rate after admission to the ICU.
Statistical analysis
Continuous variables are described as the means ± SD or median and interquartile ranges (IQR). Categorical data are presented as numbers and percentages. The difference according to the tertiles of the non-HDLc/HDLc ratio was compared using one-way analysis of variance (ANOVA) for continuous data and chi-squared tests for categorical variables.
We used a generalized additive model (GAM) to investigate the dose–response relationship between the non-HDLc/HDLc ratio and mortality (Fig. 1). We used a logistic regression model to estimate the association between the non-HDLc/HDLc ratio and 28-day mortality. The results are presented as odds ratios (ORs) with its 95% confidence intervals (95% CIs). Crude regression estimates are presented and estimates adjusted for covariates are presented. We selected these confounders on the basis of their association with the outcomes of interest or changes in effect estimates of more than 10%15. After considering the clinical significance, we adjusted for the following covariates: age (years), sex, weight, heart rate, lactate level, Apache IV score, SOFA score, septic shock, and site of infection.
We then used a two-piece-wise linear regression model to examine the threshold effect of the non-HDLc/HDLc ratio on mortality (Table 3). The turning point for the non-HDLc/HDLc ratio was determined using “exploratory” analyses, which is to move the trial turning point along the pre-defined interval and pick up the one which gave maximum model likelihood. We also performed a log-likelihood ratio test and compared the one-line linear regression model with the two-piece-wise linear model. We used the bootstrap resampling method to calculate the 95% CI for the turning point16, as described in the previous analysis17,18.
To examine the robustness of the results, we conducted sensitivity analyses. Dummy variables were used to indicate missing covariate values, which was performed when continuous variables were missing more than 1% of value. We explored the potential for unmeasured confounding between the non-HDLc/HDLc ratio and 28-day mortality by calculating E-values19. The E-value quantifies the required magnitude of an unmeasured confounder that could negate the observed association between the non-HDLc/HDLc ratio and 28-day mortality. The two-sided alpha level was set at 0.05. All the statistical analyses were performed using the EmpowerStats (www.empowerstats.com, X&Y solutions, Inc. Boston MA) and R software version 3.6.1 (http://www.r-project.org).
Ethics approval and consent to participate
Data was extracted from the eICU Collaborative Research Database (eICU-CRD)9 in accordance with the data usage agreement (our record ID: 40859994) by the PhysioNet review committee. The utilized database is released under the Health Insurance Portability and Accountability Act (HIPAA) safe harbor provision. This was a retrospective analysis based on an anonymous database for researchers and did not require ethical approval from the local ethics committee.
Results
Baseline characteristics
Data from 724 patients were analysed. The median age was 68 years (IQR 58–78 years). 334 patients (46.1%) were women. Table 1 compares the patient's demographics, vital signs, laboratory results, site of infection, and severity of illness through the tertiles of the non-HDLc/HDLc ratio. Compared with subjects in the lowest tertile of the non-HDLc/HDLc ratio, subjects in the highest tertile were younger and had higher weight at admission.
28-day mortality
The 28-day ICU mortality rate was 43/724 = 5.94% (95% CI 4.22–7.66) in our cohort. The 28-day mortality rate from the lowest tertile (0.28–2.24) to the highest (3.84–10) non-HDLc/HDLc ratio was 17 (7.1%), 8 (3.3%), and 18 (7.4%) (Table 1).
Unadjusted association between baseline variables and 28-day mortality
Table 2 shows the univariate logistic models. The analysis showed that compared with the low temperature group (30–36.38 °C), the high temperature group (36.4–36.72 °C) had a lower risk of mortality (OR = 0.28, 95% CI 0.11–0.72, P = 0.0082). Compared with the low SOFA score group (all = 0), the middle and high groups (range 1–3 and 4–15) had a higher risk of mortality (OR = 9.28, 95% CI 1.21–70.97, P = 0.0318; OR = 14.61, 95% CI 1.97–108.56, P = 0.0088).
Identification of nonlinear relationship
We observed a nonlinear dose–response relationship between the non-HDLc/HDLc ratio and mortality (Fig. 2 and Table 3). When the non-HDLc/HDLc ratio was < 3.3, the mortality rate decreased with an adjusted OR of 0.60 (95% CI 0.37–0.99, P = 0.043) for every 1 increment in the non-HDLc/HDLc ratio. When the non-HDLc/HDLc ratio was ≥ 3.3, the mortality rate increased with an adjusted OR of 1.28 (95% CI 1.01–1.62, P = 0.039) for every 1 increment in the non-HDLc/HDLc ratio. As the non-HDLc/HDLc ratio increased per SD, when the non-HDLc/HDLc ratio was ≥ 3.3, the OR for mortality was 1.64 (95% CI 1.02–2.63, P = 0.039). When the non-HDLc/HDLc ratio was < 3.3, the OR for mortality was 0.36 (95% CI 0.13–0.97, P = 0.043) (Table 3).

Associations between the non-HDLc/HDLc ratio and 28-day mortality in all patients with sepsis. A threshold, nonlinear association between the non-HDLc/HDLc ratio and 28-day mortality was found in a generalized additive model (GAM). Solid rad line represents the smooth curve fit between variables. Blue bands represent the 95% of confidence interval from the fit. Adjusted for age (years), sex, weight, heart rate, lactate level, Apache IV score, SOFA score, septic shock and site of infection.
Using the generalized additive model, a U-shaped association between the non-HDLc/HDLc ratio and 28-day mortality was detected (Table 3). The linear regression model and a two-piece-wise linear regression model were compared, and the P value of the log-likelihood ratio test was 0.023. The 95% CI for turning point of the non-HDLc/HDLc ratio was 2.9–3.9 (Table 3). This result indicates that the two-piece-wise linear regression model should be used to fit the model.
The trend of the sensitivity analysis was consistent with that of the main analysis. In the supplementary analysis, we also analysed the 14-day mortality rate, and the results were generally similar to our main results (Fig. S1 and Table S1). Dummy variables were used to indicate missing covariate values. Similar results were obtained after considering the impact of missing data (Table S2). We generated an E-value to assess the sensitivity to unmeasured confounding. The primary findings were robust, unless there was an unmeasured confounder with an OR greater than 1.88.
Discussion
This retrospective cohort study found a higher or lower non-HDLc/HDLc ratio was associated with a higher risk of 28-day mortality in patients with sepsis in the eICU-CRD database from 208 distinct ICUs across the United States between 2014 and 2015. The major finding was that the association between the non-HDLc/HDLc ratio and the risk of all-cause mortality was U-shaped, and the risk was highest in those with very low or very high non-HDLc/HDLc ratios. To our knowledge, this is the first study to report the association between the non-HDLc/HDLc ratio and 28-day mortality in septic patients.
Most studies investigating the relationship between levels of LDLc and the risk of death found no association20,21,22 or an inverse association23,24,25. A prospective population-based cohort study with 5 years of follow-up and a validation cohort of African American participants with a 4.25-year follow-up showed that neither HDLc nor LDLc was associated with mortality20. Data from 1948 to 1980 on 5209 men and women enrolled in the Framingham Heart Study found that the negative results for all-cause morality in the oldest age group appeared to be due to a negative relationship with LDLc levels rather than the protective effect of high HDLc levels21. You et al.26 included 356 patients with intracranial haemorrhage (mean follow-up = 0.22 years) and found that the LDLc/HDLc ratio was negatively correlated with all-cause mortality. Liu et al.27 recruited 3250 stroke patients and found a negative relationship between the LDLc/HDLc ratio and all-cause mortality.
Observational studies have established that HDLc is inversely associated with both cardiovascular disease and mortality across a wide range of concentrations3. A study by Bowe et al.28 included 1,764,986 men who were US veterans (mean follow-up = 9.1 years) and found a U-shaped relationship between HDL cholesterol and the risk of all-cause mortality. A study by Madsen et al.29 included 116,508 individuals from the general population. The association between HDL cholesterol and all-cause mortality was U-shaped, with both extremely high and low HDL cholesterol levels associated with high mortality. No previous study has examined HDLc or LDLc levels associated with the lowest risk of mortality in patients with sepsis. To our knowledge, although the relationship between blood lipid levels and mortality has been a concern, the association between the non-HDLc/HDLc ratio and 28-day mortality is still unclear, which prompted us to conduct the current study.
The 28-day mortality was 5.94% (43/724) in our cohort. Sepsis-related mortality was lower than that in other studies30, which may be related to severity of illness. A retrospective cohort study involving sepsis patients was conducted using the same database (eICU Collaborative Research Database)31. The in-hospital mortality was 16.7% (3828/22,868) in the total study cohort. The purpose of this research was to define persistent critical illness based on growth trajectories in patients with sepsis. Five latent classes were identified. Class 3 (51.7%), which had an in-hospital mortality rate of 6.7%, was characterized by moderate initial SOFA scores followed by decreasing severity of illness during the course of ICU stay. We have collected severity of illness indicators, including SOFA score, GCS score, Apache IV score and Acute Physiology Score III. Some important confounding factors can affect mortality in septic patients, including septic shock, lactate level, and comorbidities. In our study, those who lacked data on total cholesterol after ICU admission were excluded, so a large number of patients with sepsis were excluded.
We used non-HDL cholesterol rather than LDL cholesterol because our database measures TC and HDL cholesterol, which can be calculated by subtracting non-HDL cholesterol from it. Of the 724 patients included, 178 did not have LDL measurements. In addition, the most commonly used estimation method, the Friedewald equation, can be inaccurate32. Non-HDL and LDL cholesterol were correlated in studies with data on both variables (r = 0.93)4. In our study, the correlation coefficient between non-HDL and LDL cholesterol was 0.92 (95% CI 0.91–0.94), showing a high correlation. Non-HDL cholesterol predicts CHD risk at least as well as LDL cholesterol33 because it includes cholesterol in LDL, lipoprotein(a), intermediate-density lipoprotein, very-low-density lipoprotein and lipoprotein remnants and is thus a simple measure of cholesterol content within all atherogenic lipoproteins.
In addition, a recent study of 6941 hypertensive patients aged 65 years or older from a Chinese hypertension registry study who were not treated with lipid-lowering drugs showed that during a median follow-up of 1.72 years, 157 all-cause deaths occurred, and a U-shaped relationship between the LDLc/HDLc ratio and all-cause mortality was found8. This is similar to our result showing that the mortality rate associated with non-HDLc/HDLc ratios is not linear.
The association between low levels of non-HDLc and an increased risk of all-cause mortality could not be explained by causal effects. A possible explanation for our findings was that debilitation and illness caused a decrease in the levels of cholesterol34,35. Nonetheless, cholesterol-related risks are more complex and involve the interplay of several factors, such as cholesterol particle concentration, reverse cholesterol transport, and triglyceride-rich lipoproteins, to mention a few36. The observation that the association between non-HDLc/HDLc ratio and risk of death follows a U-shaped curve was not expected, and the mechanism underpinning the association of high HDLc and mortality is not clear. Our study did not examine the cause of death; however, we noted that the prevalence of comorbid diseases was not higher among those with a low non-HDLc/HDLc ratio, suggesting that comorbid disease events are unlikely to explain the increased risk of death in these subjects. We also noted a slightly higher percentage of patients with pulmonary infection and a higher average age among those with a low non-HDLc/HDLc ratio. Whether pulmonary infection or conditions associated with increased ageing (infections and chronic inflammation) explain the increased risk of death among patients with a low non-HDLc/HDLc ratio merits additional investigation.
The current retrospective cohort study is based on the eICU-CRD database and may be important for understanding non-HDLc/HDLc ratios in septic patients (i.e., when the focus is not limited to myocardial infarction or atherosclerotic cardiovascular disease).
Study limitations
A common problem in observational studies is unmeasured confounders. As seen in Table 1, compared with subjects in the lowest tertile of the non-HDLc/HDLc ratio, subjects in the highest tertile were younger and had a higher admission weight and a higher rate of septic shock. These differences may be indicative of unmeasured confounders, such as income and medical insurance, which may affect the risk of 28-day mortality. Although ethnicity, in-hospital period, and age were included in the datasets, it is not possible to estimate the effect of unmeasured confounders on the ORs. We adjusted for possible confounding factors, including age (years), sex, weight, heart rate, lactate level, Apache IV score, SOFA score, septic shock and site of infection. We used E-value sensitivity analysis to quantify the potential implications of unmeasured confounders and found that an unmeasured confounder was unlikely to explain the entirety of the association. Additional limitations of our study include missing data for some variables. Nevertheless, we used contemporary methods to deal with missing data to minimize bias.
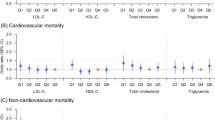
Another limitation is related to the fact that the diagnosis was based on the ICD-9 coding, which the responsible physician found relevant, and we did not have information concerning causes of death. Since we are examining mortality over a short period after the date of visit to the ICU, we did not find it beneficial to distinguish between cardiovascular and non-cardiovascular death.
Furthermore, lack of information on interventions during initial stabilization may have influenced non-HDLc/HDLc ratio levels and survival. It is noteworthy that the potential resulting from interventions would bias towards to the null and thus result in an underestimation of the association between non-HDLc/HDLc ratio level and mortality.
Finally, the 28-day mortality was 5.94% (43/724) in our cohort. The mortality of sepsis is lower than that in other studies. The possible reason is that the subjects included in this study excluded those who lacked total cholesterol after ICU admission, so that a large number of patients with sepsis were excluded. We acknowledge that the participants were patients referred to the emergency department for some reason, limiting the generalization of the findings to other populations.
Conclusions
Data from the eICU-CRD database were used to identify 724 patients with sepsis. This study identified a nonlinear dose–response relationship between non-HDLc/HDLc ratios and 28-day mortality. The association between the non-HDLc/HDLc ratio and the 28-day mortality risk was a U-shaped curve. A higher or lower non-HDLc/HDLc ratio was associated with an increased risk of 28-day mortality.
Data availability
Data were fully available at https://eicu-crd.mit.edu/.
References
Marshall, J. C. Why have clinical trials in sepsis failed?. Trends Mol. Med. 20, 195–203 (2014).
Lewington, S. et al. Blood cholesterol and vascular mortality by age, sex, and blood pressure: A meta-analysis of individual data from 61 prospective studies with 55,000 vascular deaths. Lancet. 370, 1829–1839 (2007).
Di Angelantonio, E. et al. Major lipids, apolipoproteins, and risk of vascular disease. JAMA. 302, 1993–2000 (2009).
National trends in total cholesterol obscure heterogeneous changes in HDL and non-HDL cholesterol and total-to-HDL cholesterol ratio: A pooled analysis of 458 population-based studies in Asian and Western countries. Int. J. Epidemiol. 49, 173–192 (2020).
Eliasson, B., Gudbjörnsdottir, S., Zethelius, B., Eeg-Olofsson, K. & Cederholm, J. LDL-cholesterol versus non-HDL-to-HDL-cholesterol ratio and risk for coronary heart disease in type 2 diabetes. Eur. J. Prev. Cardiol. 21, 1420–1428 (2014).
Wang, D. et al. Higher non-HDL-cholesterol to HDL-cholesterol ratio linked with increased nonalcoholic steatohepatitis. Lipids Health Dis. 17, 67 (2018).
Zuo, P. Y. et al. Non-HDL-cholesterol to HDL-cholesterol ratio as an independent risk factor for the development of chronic kidney disease. Nutr. Metab. Cardiovasc. Dis. 25, 582–587 (2015).
Yu, Y. et al. A U-shaped association between the LDL-cholesterol to HDL-cholesterol ratio and all-cause mortality in elderly hypertensive patients: A prospective cohort study. Lipids Health Dis. 19, 238 (2020).
Pollard, T. J. et al. The eICU collaborative research database, a freely available multi-center database for critical care research. Sci Data. 5, 180178 (2018).
Serpa, N. A. et al. Mechanical power of ventilation is associated with mortality in critically ill patients: An analysis of patients in two observational cohorts. Intensive Care Med. 44, 1914–1922 (2018).
van den Boom, W. et al. The search for optimal oxygen saturation targets in critically ill patients: Observational data from large ICU databases. Chest. 157, 566–573 (2020).
Davidson, S. et al. Vital-sign circadian rhythms in patients prior to discharge from an ICU: A retrospective observational analysis of routinely recorded physiological data. Crit Care. 24, 181 (2020).
Singer, M. et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 315, 801–810 (2016).
Zimmerman, J. E., Kramer, A. A., McNair, D. S. & Malila, F. M. Acute Physiology and Chronic Health Evaluation (APACHE) IV: Hospital mortality assessment for today’s critically ill patients. Crit. Care Med. 34, 1297–1310 (2006).
Jaddoe, V. W. et al. First trimester fetal growth restriction and cardiovascular risk factors in school age children: Population based cohort study. BMJ 348, g14 (2014).
Lin, L. et al. The analysis of threshold effect using empower stats software. Chin. J. Epidemiol. 34, 1139–1141 (2013).
Yu, X., Cao, L. & Yu, X. Elevated cord serum manganese level is associated with a neonatal high ponderal index. Environ. Res. 121, 79–83 (2013).
Yu, X. et al. Threshold effects of moderately excessive fluoride exposure on children’s health: A potential association between dental fluorosis and loss of excellent intelligence. Environ. Int. 118, 116–124 (2018).
Haneuse, S., VanderWeele, T. J. & Arterburn, D. Using the E-value to assess the potential effect of unmeasured confounding in observational studies. JAMA 321, 602–603 (2019).
Fried, L. P. et al. Risk factors for 5-year mortality in older adults: The cardiovascular health study. JAMA 279, 585–592 (1998).
Kronmal, R. A., Cain, K. C., Ye, Z. & Omenn, G. S. Total serum cholesterol levels and mortality risk as a function of age. A report based on the Framingham data. Arch. Intern. Med. 153, 1065–1073 (1993).
Psaty, B. M. et al. The association between lipid levels and the risks of incident myocardial infarction, stroke, and total mortality: The cardiovascular health study. J. Am. Geriatr. Soc. 52, 1639–1647 (2004).
Akerblom, J. L. et al. Relation of plasma lipids to all-cause mortality in Caucasian, African–American and Hispanic Elders. Age Ageing. 37, 207–213 (2008).
Schupf, N. et al. Relationship between plasma lipids and all-cause mortality in nondemented elderly. J. Am. Geriatr. Soc. 53, 219–226 (2005).
Bathum, L. et al. Association of lipoprotein levels with mortality in subjects aged 50+ without previous diabetes or cardiovascular disease: A population-based register study. Scand. J. Prim. Health Care. 31, 172–180 (2013).
You, S. et al. LDL-C/HDL-C ratio and risk of all-cause mortality in patients with intracerebral hemorrhage. Neurol. Res. 38, 903–908 (2016).
Liu, L. et al. Association of LDL-C/HDL-C ratio with stroke outcomes within 1 year after onset: A hospital-based follow-up study. Front. Neurol. 11, 408 (2020).
Bowe, B. et al. High density lipoprotein cholesterol and the risk of all-cause mortality among US veterans. Clin. J. Am. Soc. Nephrol. 11, 1784–1793 (2016).
Madsen, C. M., Varbo, A. & Nordestgaard, B. G. Extreme high high-density lipoprotein cholesterol is paradoxically associated with high mortality in men and women: Two prospective cohort studies. Eur. Heart J. 38, 2478–2486 (2017).
Chen, H., Zhao, C., Wei, Y. & Jin, J. Early lactate measurement is associated with better outcomes in septic patients with an elevated serum lactate level. Crit. Care. 23, 351 (2019).
Zhang, Z., Ho, K. M., Gu, H., Hong, Y. & Yu, Y. Defining persistent critical illness based on growth trajectories in patients with sepsis. Crit. Care. 24, 57 (2020).
Martin, S. S. et al. Friedewald-estimated versus directly measured low-density lipoprotein cholesterol and treatment implications. J. Am. Coll. Cardiol. 62, 732–739 (2013).
Arsenault, B. J. et al. Beyond low-density lipoprotein cholesterol: Respective contributions of non-high-density lipoprotein cholesterol levels, triglycerides, and the total cholesterol/high-density lipoprotein cholesterol ratio to coronary heart disease risk in apparently healthy men and women. J. Am. Coll. Cardiol. 55, 35–41 (2009).
Jacobs, D. et al. Report of the conference on low blood cholesterol: Mortality associations. Circulation 86, 1046–1060 (1992).
Ranieri, P., Rozzini, R., Franzoni, S., Barbisoni, P. & Trabucchi, M. Serum cholesterol levels as a measure of frailty in elderly patients. Exp. Aging Res. 24, 169–179 (1998).
Sanin, V., Pfetsch, V. & Koenig, W. Dyslipidemias and cardiovascular prevention: Tailoring treatment according to lipid phenotype. Curr. Cardiol. Rep. 19, 61 (2017).
Acknowledgements
The author is very grateful to the data providers of the study.
Funding
Z.X.Y. received funding from the Key Technologies Research and Development of China (Grant no. 2017YFB1104104).
Author information
Authors and Affiliations
Contributions
X.L.C. performed statistical analysis. L.C. cleaned the data. C.L. conceived and designed the research. X.L.C. and L.C. drafted the manuscript. C.L. made critical revision of the manuscript for key intellectual content.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chang, L., Chen, X. & Lian, C. The association between the non-HDL-cholesterol to HDL-cholesterol ratio and 28-day mortality in sepsis patients: a cohort study. Sci Rep 12, 3476 (2022). https://doi.org/10.1038/s41598-022-07459-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-07459-y
- Springer Nature Limited