
Abstract
The aim was to determine the variations in the level of origin of carotid bifurcation and diameters of the common, internal, and external carotid arteries which is clinically important for several interventional procedures. Therefore, 165 human embalmed corpses were dissected. The data collected were analyzed using the Chi square-test and the Pearson correlation test. The results of previous studies have been reviewed. In relation to the level of the carotid bifurcation, taking as a reference point the hyoid bone, the values ranged from 4 cm below the hyoid body to 2.5 cm above the body of the hyoid, being the average height—0.33 cm, with a standard deviation of 1.19 cm. The right carotid bifurcation was established at a higher level (x = − 0.19 cm.) than the left one (x = − 0.48 cm.) (p = 0.046). On the contrary, no significant gender differences could be observed. The arterial calibres of the common and internal carotid arteries were higher in male than female. In the internal carotid artery (X = 0.76 cm.), the left was greater than the right (X = 0.72 cm.) (P = 0.047). However, no differences in the distribution of the calibre of the external carotid artery were found neither by side nor gender. Variations in the level of bifurcation and calibres of carotid arteries are relevant for interventional radiology procedures and head and neck surgeries. Knowledge of these anatomical references might help clinicians in the interpretation of the carotid system.
Similar content being viewed by others


Introduction
The variability of the carotid arteries in relation to their diameters and level of bifurcation varied widely in literature1,2,3,4,5. The importance of the carotid arteries is based on their distribution territories for face, mouth, eye, nose, brain, on associated pathologies as the atheromatosis and on new diagnostic techniques and interventional approaches6,7.
Regarding the descriptions of these arteries, studies were based in different types of sample, founding large samples3,4,5,8,9 or small samples10,11,12,13 studying different characteristics of the carotid system.
About the carotid bifurcation two landmarks have been described: the upper horn of the thyroid cartilage5,9 and the 4th cervical vertebra14,15. However, higher levels have been described, such as the hyoid bone, or lower levels, such as the cricoid cartilage1,5. In relation with the bifurcation the landmarks have been described at the height of the cervical vertebrae, being exceptionally, in levels as low as C7, Th1 and Th216,17.
The asymmetrical level of carotid bifurcation between the left and right side has also been described1,7,9,18,19 even in 48% of the sample size9. Variations depending on ethnicity have also been observed, being of a higher level in African Americans than in Caucasians15, and in Asian population compared with the Caucasian20.
Occasionally, the carotid bifurcation has not been identified in two different situations: one, being associated with an absent common carotid artery, then, the internal and external carotid arteries emerged directly from the brachiocephalic trunk13,21; or, on the contrary, associated with an absent external carotid artery, the remaining common-internal carotid artery branches off the cervical arterial branches on its way up the neck22.
Regarding the calibre of these arteries, the values obtained a great variability. For instance, it can vary between 5.8 mm and 8.6 mm in the case of the common carotid, depending on the technique with which it has been studied (Conventional Angiography, Computerized Digital Angiography, ECO Doppler, ECO Doppler with colour, Angio-CT and Angio-RMN). Most of the bibliography refers to internal diameters since the radiological techniques made measurements from the margins established by the contrasts used.
A few articles referred to the internal arterial calibre measured from a morphometric analysis5,23,24,25.
Nowadays, the variability reported in relation to the level of bifurcation and calibre has been described in independent studies, not showing these details in a unique article. The samples used in these articles were mostly small and not statistical details were specified in terms of these characteristics. In our study we have unified all variables in a reliable sample with the aim of addressing a simple statistical and useful description for interventional radiology procedures and/or surgeries of head, neck, and face.
Material and methods
A total sample of 165 embalmed body donors to science belonged to the Department of Anatomy, University of Cambridge, UK, were dissected. The individuals had given their written informed consent prior to death for their use for scientific and educational purposes and donated their bodies. According to National Law, scientific institutions (in general Institutes, Departments or Divisions of Medical Universities) are entitled to receive the body after death mainly by means of a specific legacy, which is a special form of last will and testament. No bequests were accepted without the donor having registered their legacy and been given appropriate information upon which to make a decision based upon written informed consent (policy of ethics); therefore, an ethics committee approval was waived26.
These body-donors have been previously dissected by preclinical students and completed by the authors. The gender distribution was 74 male and 91 female body-donors, with an age range of 60 to 103 years. Clinical histories were available, in no case containing any reference to vascular surgical interventions.
Based upon the completeness of the neck structures after dissection, 4 different samples of the available body-donors were taken into account in this study following these parameters: (1) the calibre of the common carotid artery 103 cases (47 male and 55 female); (2) the calibre of the internal carotid artery 139 cases (63 male and 77 female); (3) the calibre of the external carotid artery 206 cases (95 male and 111 female) and (4) the height of carotid bifurcation in 141 cases (61 male and 80 female).
Distances and external diameters were measured with callipers. These measurements were verified by a second investigator. Statistical comparisons were made using the chi-square test, with a value of p < 0.05 taken as statistically significant and the Pearson correlation test. Previous published results were carefully reviewed and compared with this sample.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
According to Spanish and Austrian National Law, scientific institutions (in general Institutes, Departments or Divisions of Medical Universities) are entitled to receive the body after death mainly by means of a specific legacy, which is a special form of last will and testament. No bequests are accepted without the donor having registered their legacy and been given appropriate information upon which to make a decision based upon written informed consent (policy of ethics); therefore, an ethics committee approval is not necessary.
Results
In order to improve the clarity, the results obtained have been exposed following the order proposed in the "Material and Methods" section.
-
1)
In relation to the calibre of the common carotid artery, it has been studied in a sample made up of 103 cases (47 in male and 56 in female). The values obtained for the calibre of the common carotid artery ranged from 0.7 to 1.3 cm. The average diameter obtained was 0.97 cm with a standard deviation of 0.14 cm (Fig. 1).
When analyzing the diameter of the common carotid artery depending on the side, no statistically significant differences were observed (p > 0.05). On the contrary, when carrying out the analysis considering the gender variable, these differences have been observed with a significance of p = 0.001. The average arterial calibre of the common carotid artery was higher in male (X = 1.01 cm.) than in female (X = 0.93 cm.).
-
2)
The calibre of the internal carotid artery variable has been studied in a sample made up of 139 cases, 63 in male and 76 in female. The values found for the internal carotid artery ranged from 0.4 cm to 1.8 cm. The average diameter obtained was 0.74 cm. with a standard deviation of 0.16 cm (Fig. 2). When analyzing the diameter of the internal carotid artery according to the side, the diameter of the left internal carotid artery (X = 0.76 cm) was greater than the diameter of the right internal carotid artery (X = 0.72 cm) being statistically significant (p = 0.047). In the case of gender, differences have been observed with a marked tendency towards statistical significance (p = 0.54). The arterial calibre of the internal carotid artery was greater in male (x = 0.77 cm) than in female (x = 0.71 cm).
-
3)
The calibre of the external carotid artery has been studied in a sample consisting of 206 cases, 95 in male and 111 in female. The values found for the external carotid artery ranged from 0.3 to 0.9 cm. The average diameter obtained was 0.49 cm. with a standard deviation of 0.08 cm (Fig. 3.). In the distribution of this arterial calibre by side and gender, statistically significant differences have not been observed (p > 0.05).
Both the internal and external carotid arteries originate from the common carotid artery, specifically from the carotid bifurcation; therefore, a correlation study has been performed between the diameters of the common carotid artery and the internal carotid artery and between the diameters of the common carotid artery and the external carotid artery.
The application of the Pearson correlation test has shown that there was no clear correlation between the diameters of the common and internal carotid artery (Fig. 4), but a tendency towards correlation between the diameters of the common carotid artery and the external carotid artery was verified (p = 0.113) (Fig. 5).
Statistically significant association has been obtained in the correlation between the diameters of the internal and external carotid arteries (p = 0.003) (Fig. 6).
-
4)
In relation to the level of the carotid bifurcation, this variable has been studied in a sample consisting of 141 cases, 61 in male and 80 in female. The level, which has been taken as a reference point, was the body of the hyoid bone. The values obtained for the level of the carotid bifurcation ranged from 4 cm. below the hyoid body and 2.5 cm. above the body of the hyoids. The average height was—0.33 cm., with a standard deviation of 1.19 cm. (Figs. 7, 8A,B). The Klippel-Feil anomaly, typically associated with a low carotid bifurcation, was not found in our sample size.
In the comparative study between sides, a statistical significance of p = 0.046 has been verified, establishing the right carotid bifurcation at a higher point (x = − 0.19 cm.) than the left carotid bifurcation (x = − 0.48 cm.). On the contrary, no significant differences have been observed in relation to the distribution by gender (p > 0.05).

Diameter of the common carotid artery. cm. centimetre, n sample size, X mean, σ standard deviation, min minimum value and max maximum value.

Diameter of the internal carotid artery. cm. centimetre, n sample size, X mean, σ standard deviation, min minimum value and max maximum value.

Diameter of the external carotid artery. cm. centimetre, n sample size, X mean, σ standard deviation, min minimum value and max maximum value.

Correlation between the diameters of the common carotid artery and the internal carotid artery.

Correlation between the diameters of the common carotid artery and the external carotid artery.

Correlation between the diameters of the internal carotid artery and the external carotid artery.

Level of the carotid bifurcation. Negative values are equivalent to heights below the body of the hyoid bone, and positive values are equivalent to heights above the body of the hyoid bone. cm. centimetre, n sample size, X mean, σ standard deviation, min minimum value and max maximum value.

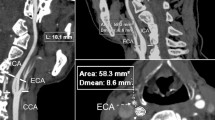
(A) Left lateral view of the division of the CCA lowest to the level of the greater horn of the hyoid bone and just on the level of the higher horn of the thyroid cartilage. (B) Right lateral view of the division of the CCA just at the level of the greater horn of the hyoid bone. CCA common carotid artery, ICA internal carotid artery, ECA external carotid artery, X vagus nerve, LFT linguofacial trunk, st superior thyroid artery, *Greater horn of the hyoid bone, **Higher horn of the thyroid cartilage, Line: level of the carotid bifurcation.
Discussion
Most of the references consulted in this work regarding these arteries refer mainly to anatomical variations in relation to their origin, course, or disposition.
Regarding the calibre of these arteries, the results of the studies, as a whole, presented a great variability since they depended on the technique with which it has been studied (Conventional Angiography, Computerized Digital Angiography, ECO Doppler, ECO Doppler with color, Angio-CT and Angio-RMN)5,23,24,25. Furthermore, the diameter measurements with radiological techniques referred to endoluminal diameters since these were made from the margins established by the contrasts used. Only a few articles have been found that referred to the internal arterial calibre measured from a morphometric analysis5,23,24 (Table 1).
The study by Goubergrits et al.24, was carried out from a morphometric analysis with a digital caliper of the luminal diameter of 86 carotid systems that were corroborated with the results of an ECO Doppler study. In our series, these measurements were performed extraluminally with a caliper in a variable sample depending on the artery studied. Comparing both series, a certain similarity has been observed in the diameters of the internal and external carotid arteries, taking into account that the differences obtained could be in relation to the different measurement performed -digital vs. manual- and with the thickness of the arterial wall. However, regarding the difference observed at the level of the common carotid artery—32 mm—these reasons did not justify this huge difference, nor could any reference in relation to the thickness explain it.
In addition, and although it is another artery, the external carotid, in comparison with a radiological study, such as that of Czerwinski et al.14 did not obtain such irregular results, since the average diameter obtained by this author for this artery was 0.57 cm (n = 240). Delving into our results with regard to the common carotid artery, this study verified that, with a sample of 103 cases, the values obtained ranged from 0.7 cm and 1.3 cm, and the average diameter was 0.97 cm with a standard deviation of 0.14 cm. Therefore, the obtained values were grouped with little dispersion around the mean value in a sample whose size was greater than 100 cases.
Based on the fact that the external and internal carotid arteries originated from the common carotid artery, a correlation study has been performed between these arteries. No statistically significant correlations between the common and internal carotid arteries and the common and external carotid arteries (p > 0.05) have been observed. Curiously, when studying the correlation between the internal and external carotid arteries, this was established in a statistically significant way (p = 0.003), which together with the results of the previous comparison with another author, could lead us to think about the possibility of a measurement error of the common carotid artery that should be confirmed with a larger sample size in future studies.
The diameter of the carotid arteries has been analyzed in relation to the side and gender with the following conclusions:
-
The average diameter of the common carotid artery was higher in male (X = 1.01 cm.) than in female (X = 0.93 cm.) (P = 0.001). We did not observe significant differences regarding the side (p > 0.05).
-
The arterial calibre of the internal carotid artery was greater in male (x = 0.77 cm.) than in female (x = 0.71 cm.) With a p very close to statistical significance (p = 0.05). Also, the diameter of the left internal carotid artery (X = 0.76 cm.) was greater than the diameter of the right internal carotid artery (X = 0.72 cm.) (P = 0.047).
-
On the contrary, in the distribution of the diameter of the external carotid artery by side and gender, no statistically significant differences have been found (p > 0.05).
In relation to the anatomical level at which the carotid bifurcation occurs, two reference points are classically taken. An anterior one that corresponds to the upper edge of the thyroid cartilage1,7,12 and a posterior one, corresponding to the 4th cervical vertebra3,14. The upper edge of the thyroid cartilage would be equivalent to the upper edge of the greater horns of the thyroid cartilage4.
In most cases the choice of one or the other is in relation to the method chosen when making the measurements. Using a surgical approach, the most common option is the anterior anatomical margin given its greater accessibility. However, when measurements are made using radiological techniques, the most feasible option is the anatomical relief of the vertebral column and bone framework, being, on the other hand, more stable regarding the age variable3.
In our case with a study based on body-donor dissection, and an entire sample with an age greater than 65 years, being homogeneous at the age variable, the reference level was the hyoid bone body.
The comparison of our results with those of the consulted bibliography which used a body-donor sample is exposed in Table 2.
In terms of embryogenesis, the first two aortic arches are commonly lost. However, it could happen that the persistent of the dorsal parts of the second arches becomes the root portion of the stapedial artery on each side or the persistent of connection of the dorsal and ventral parts of the aortic arches give rise to the hypoglossal artery27,28. The third and left fourth arches are retained, becoming the root portion of the internal carotid artery and the arcus aortic respectively. On the other hand, both the ventral and dorsal aortae beyond the portion of the third arch are preserved, the former gave rise to the stem of the external carotid directed cranially; some cases of external carotid artery agenesia have been reported29. The latter gave rise to the second part of the internal carotid artery, whereas the ventral aorta between the third and fourth arches becomes the stem of the common carotid artery27. The movement of the heart downward towards the thorax dragging the carotid arteries could be more or less extensive justifying the different level of division30. The asymmetry, right-left, of the blood flow justify differences of caliber observed among the carotid arteries. The collateral and terminal branches of the external carotid artery appear in human embryos of 14 mm to 17 mm by sprouting of the main external carotid trunk27. However, there have been reported cases where the collateral arteries arise from the internal or common carotid arteries10,31,32.
In our study, the percentage of cases in which the carotid bifurcation occurs at a higher level than the reference level taken previously has been clearly higher (20.5% vs. 3.5% for Quain et al.7, 3.3% for Al-Rafiah et al.8, and 0% for Lucev et al.12, Lo et al.9, and Mompeó et al.18). Our results have been more similar to those of McAfee et al.4, who also observed the possibility of high bifurcations more frequently in a series of 140 hemi sides, since in up to 82% of cases the bifurcation was established in a 2.5 cm area inferior to the branch of the jaw.
In the distribution of the height of the carotid bifurcation according to the side and gender, unlike Smith and Larsen et al.19, in our series this height has been established at a higher level on the right side than on the left (p = 0.046) and, unlike Adachi2, no differences regarding gender have been observed (p > 0.05).
Therefore, a precise knowledge of possible variation of the carotid axis morphology could help clinicians planning neck or facial surgery (laryngectomy, thyroidectomy), thrombo-endarterectomy, tumor angiogenesis, severe stenosis, aneurysms etc.33,34,35,36,37,38,39,40. The surgeon should bear in mind, just before starting any process, the normal, variations and possible anomalies of the carotid axis. These variations and anomalies are present in approximately 1.2% of cases. The normal anatomy, variations or anomalies could be detected easily by imaging techniques as preoperative conventional CT angiography, 3D CT angiography magnetic resonance angiography, digital subtraction angiography, doppler ultrasonography, etc.33,34,35,36,37,38,39,40.
The correlation between imaging diagnosis techniques and anatomical studies based on cadaveric samples might be important for accuracy in planning (mini-)invasive carotid techniques. It allows a precise identification of variations or anomalous of the carotid arteries, thereby reducing the possible risk of intraoperative surgery34,35,40.
Conclusions
Variations in the calibres of the carotid arteries (for the common carotid artery 0.97 cm in average, for the internal 0.74 cm in average, and 0.49 cm for the external, respectively) and the carotid bifurcation level (reference point the hyoid bone with an average height of—0.33 cm, right carotid bifurcation at a higher level (x = − 0.19 cm.) than the left one (x = − 0.48 cm.)) are relevant for interventional radiology procedures and head and neck surgeries. A precise knowledge of the anatomical variations could help clinicians in the interpretation of the carotid system allowing them different possibilities in terms of diagnosis and treatment.
Therefore, we should take into account the anatomical variations in the appearance of the carotid system in radio diagnostic images and during surgical approaches, since this variability in the location or size of these structures could have negative consequences for our future patients.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Aaron, C. & Chawaf, A. Variations de la carotide externe et de ses branches. Bull. Assoc. Anat. 13, 125–133 (1967).
Adachi, B. & Kihara, T. Das Arteriensystem der Japaner, Verlag der Kaiserlich-Japanischen Universitat, zu Kyoto. Kommission bei Maruzen Co, 26–46 (1928).
Lippert, H. & Pabst, R. Arterial variations in man: Classification and frequency (Springer, 1985).
McAfee, D. K., Anson, B. J. & McDonald, J. J. Variation in the point of bifurcation of the common carotid artery. Quart. Bull. Northwestern Univ. Med. School 27, 226 (1953).
Ozgur, Z., Govsa, F. & Ozgur, T. Anatomic evaluation of the carotid artery bifurcation in cadavers: Implications for open and endovascular therapy. Surg. Radiol. Anat. 30, 475–480. https://doi.org/10.1007/s00276-008-0351-4 (2008).
Germans, M. R. & Regli, L. Posterior auricular artery as an alternative donor vessel for extracranial-intracranial bypass surgery. Acta Neurochir. 156, 2095–2101. https://doi.org/10.1007/s00701-014-2206-6 (2014).
Quain, R. The Anatomy of the Arteries of the Human Body: And its Applications to Pathology and Operative Surgery with a Series of Lithographic Drawings 55–86 (Taylor and Walton, 1844).
Al-Rafiah, A., El-Haggagy, A., Aal, I. & Zaki, A. Anatomical study of the carotid bifurcation and origin variations of the ascending pharyngeal and superior thyroid arteries. Folia Morphol. 70, 47–55 (2011).
Lo, A. et al. Anatomical variations of the common carotid artery bifurcation. ANZ J. Surg. 76, 970–972. https://doi.org/10.1111/j.1445-2197.2006.03913.x (2006).
Gluncic, V., Petanjek, Z., Marusic, A. & Gluncic, I. High bifurcation of common carotid artery, anomalous origin of ascending pharyngeal artery and anomalous branching pattern of external carotid artery. Surg. Radiol. Anat. 23, 123–125. https://doi.org/10.1007/s00276-001-0123-x (2001).
Gurbuz, J., Cavdar, S. & Ozdogmus, O. Trifurcation of the left common carotid artery: A case report. Clin. Anat. 14, 58–61. https://doi.org/10.1002/1098-2353(200101)14:1%3c58::AID-CA1011%3e3.0.CO;2-M (2001).
Lucev, N., Bobinac, D., Maric, I. & Drescik, I. Variations of the great arteries in the carotid triangle. Otolaryngol. Head Neck Surg. 122, 590–591. https://doi.org/10.1067/mhn.2000.97982 (2000).
Maybody, M., Uszynski, M., Morton, E. & Vitek, J. J. Absence of the common carotid artery: A rare vascular anomaly. AJNR Am. J. Neuroradiol. 24, 711–713 (2003).
Czerwinski, F. Variability of the course of external carotid artery and its rami in man in the light of anatomical and radiological studies. Folia Morphol. (Warsz) 40, 449–453 (1981).
Lemmi, H., Daly, R. F., Kashgarian, M. & Argires, J. A comparison of the level of bifurcation of the common carotid arteries in negroes and whites. Acta Anat. (Basel) 71, 22–27. https://doi.org/10.1159/000143166 (1968).
Charalambous, S., Hatzidakis, A., Peteinarakis, I., Megremis, S. & Karantanas, A. Common left carotid bifurcation at C7–Th1 level: A rare anatomical variant. Surg. Radiol. Anat. 41, 227–229. https://doi.org/10.1007/s00276-018-2140-z (2019).
Krmpotic-Nemanic, J., Draf, W. & Helms, J. Surgical Anatomy of Head and Neck (Springer Science & Business Media, 2012).
Mompeó, B. & Bajo, E. Carotid bifurcation-clinical relevance. Eur. J. Anat. 2, 37–42 (2015).
Smith, D. & Larsen, J. L. On the symmetry and asymmetry of the bifurcation of the common carotid artery: A study of bilateral carotid angiograms in 100 adults. Neuroradiology 17, 245–247. https://doi.org/10.1007/BF00337533 (1979).
Jitpun, E., Wattanasen, Y. & Tirakotai, W. Do asians have higher carotid bifurcation? A computed tomographic angiogram study of the common carotid artery bifurcation and external carotid artery branching patterns. Asian J. Neurosurg. 14, 1082. https://doi.org/10.4103/ajns.AJNS_162_19 (2019).
Hollinshead, W. H. 458–460, 474–480 (Harper and Row, 1968).
Tubbs, R. S., Shoja, M. M. & Loukas, M. Bergman’s Comprehensive Encyclopedia of Human Anatomic Variation 477–486 (John Wiley & Sons, 2016).
de la Arteria, N. B. & Relación, C. C. Common carotid artery bifurcation levels related to clinical relevant anatomical landmarks. Int. J. Morphol. 24, 413–416 (2006).
Goubergrits, L., Affeld, K., Fernandez-Britto, J. & Falcon, L. Geometry of the human common carotid artery. A vessel cast study of 86 specimens. Pathol. Res. Pract. 198, 543–551. https://doi.org/10.1078/0344-0338-00299 (2002).
Sehirli, U. S., Yalin, A., Tulay, C. M., Cakmak, Y. O. & Gurdal, E. The diameters of common carotid artery and its branches in newborns. Surg. Radiol. Anat. 27, 292–296. https://doi.org/10.1007/s00276-005-0322-y (2005).
Konschake, M. & Brenner, E. “Mors auxilium vitae”—Causes of death of body donors in an Austrian anatomical department. Ann. Anat.-Anatomischer Anzeiger 196, 387–393. https://doi.org/10.1016/j.aanat.2014.07.002 (2014).
Evans, H. The development of the vascular system. Manual Hum. Embryol. 2, 570–669 (1912).
Suzuki, T. et al. Anomalous artery directly connecting the external and internal carotid arteries. Ann. Anat.-Anatomischer Anzeiger 182, 59–63 (2000).
Franklin, P., Lee, R., Allard, J., Gibbons, G. & Costello, P. Unilateral absence of the external carotid artery. Can. Assoc. Radiol. J. 39, 293–294 (1988).
Matsumoto, M., Okuda, H., Ishidoh, E. & Mitsui, H. Case report. An anomalous case of the common carotid artery giving off several branches and high division of the internal carotid artery. Okajimas Folia Anat. Jpn. 63, 37–43 (1986).
Kaneko, K., Akita, M., Murata, E., Imai, M. & Sowa, K. Unilateral anomalous left common carotid artery; a case report. Ann. Anat.-Anatomischer Anzeiger 178, 477–480 (1996).
Lemaire, V., Jacquemin, G., Medot, M. & Fissette, J. Thyrolingual trunk arising from the common carotid artery a case report. Surg. Radiol. Anat. 23, 135–137 (2001).
Pia, H. Classification of aneurysms of the internal carotid system. Acta Neurochir. 40, 5–31 (1978).
Anson, J. A., Heiserman, J. E., Drayer, B. P. & Spetzler, R. F. Surgical decisions on the basis of magnetic resonance angiography of the carotid arteries. Neurosurgery 32, 335–343 (1993).
Patel, M. R. et al. Preoperative assessment of the carotid bifurcation: Can magnetic resonance angiography and duplex ultrasonography replace contrast arteriography?. Stroke 26, 1753–1758 (1995).
Netuka, D., Beneš, V., Mandys, V., Hlasenska, J. & Burkert, J. Accuracy of angiography and Doppler ultrasonography in the detection of carotid stenosis: A histopathological study of 123 cases. Acta Neurochir. 148, 511–520 (2006).
Timaran, C. H. et al. Accuracy and utility of three-dimensional contrast-enhanced magnetic resonance angiography in planning carotid stenting. J. Vasc. Surg. 46, 257–264 (2007).
Raghavan, P., Mukherjee, S., Gaughen, J. & Phillips, C. D. Magnetic resonance angiography of the extracranial carotid system. Top. Magn. Reson. Imaging 19, 241–249 (2008).
Yan, D. et al. Significance of the preoperative guidance of dual-source CT in carotid body tumor. Chin. Med. J. 123, 2816–2819 (2010).
Vaiman, M. & Bekerman, I. Preoperative detection of anomalies of carotid arteries in the neck surgery. Eur. Arch. Otorhinolaryngol. 272, 2979–2983 (2015).
Acknowledgements
The authors sincerely thank those who donated their bodies to science so that anatomical research could be performed. Results from such research can potentially increase mankind's overall knowledge that can then improve patient care. Therefore, these donors and their families deserve our highest gratitude.
Author information
Authors and Affiliations
Contributions
Each author has made substantial contributions to the work, approved the submitted version and has agreed both to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature. R.C.: Project development, Data collection, Manuscript writing. S.Q.: Data analysis, Manuscript writing, Manuscript editing. M.K.: Data analysis, Manuscript writing, Manuscript editing, Supervision. P.A.: Manuscript writing, Manuscript editing. X.L.: Data collection, Data analysis. T.V.: Data collection, Data analysis, Manuscript writing, Manuscript editing. J.S.: Data collection, Data analysis, Manuscript writing, Manuscript editing, Supervision. E.M.: Data collection, Data analysis, Manuscript writing, Manuscript editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cobiella, R., Quinones, S., Konschake, M. et al. The carotid axis revisited. Sci Rep 11, 13847 (2021). https://doi.org/10.1038/s41598-021-93397-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-93397-0
- Springer Nature Limited
This article is cited by
-
The vertical topography of the carotid bifurcation – original study and review
Surgical and Radiologic Anatomy (2024)
-
Variations in external carotid artery branches and common carotid bifurcation level: a computed tomography angiography study
Egyptian Journal of Radiology and Nuclear Medicine (2023)