
Abstract
Lymph nodes (LNs) are important hubs for metastatic cell arrest and growth, immune modulation, and secondary dissemination to distant sites through a series of mechanisms, and it has been proved that lymph node metastasis (LNM) is an essential prognostic indicator in many different types of cancer. Therefore, it is important for oncologists to understand the mechanisms of tumor cells to metastasize to LNs, as well as how LNM affects the prognosis and therapy of patients with cancer in order to provide patients with accurate disease assessment and effective treatment strategies. In recent years, with the updates in both basic and clinical studies on LNM and the application of advanced medical technologies, much progress has been made in the understanding of the mechanisms of LNM and the strategies for diagnosis and treatment of LNM. In this review, current knowledge of the anatomical and physiological characteristics of LNs, as well as the molecular mechanisms of LNM, are described. The clinical significance of LNM in different anatomical sites is summarized, including the roles of LNM playing in staging, prognostic prediction, and treatment selection for patients with various types of cancers. And the novel exploration and academic disputes of strategies for recognition, diagnosis, and therapeutic interventions of metastatic LNs are also discussed.
Similar content being viewed by others


Introduction
Lymph nodes (LNs) serve as essential components of the mammalian immune system, functioning as a barrier against systemic pathogen dissemination while facilitating the induction and maturation of specific immune responses and serving as central hubs that orchestrate interactions among immune cell populations.1 Malignant tumor cells, however, can hijack the lymphatic system to facilitate their metastatic dissemination throughout the body, just like thieves using the ventilation ducts to move to various rooms in a building, and LNs serve as major hubs for metastatic cell growth, secondary dissemination to other tissue compartments, and the modulation of antitumor immune responses.2 Lymph node metastasis (LNM) is thus a key consideration when evaluating cancer patients, as it has major implications for disease staging, clinical management, and prognostic outcomes. Recent advances in medical technologies and LNM-focused research have enabled the more effective detection and treatment of LNM. As such, this review was developed with the goal of providing a systematic overview of the physiological and anatomical characteristics of LNs, as well as the mechanistic basis for LNM and its clinical significance. These discussions are further supported by a survey of approaches to the detection, diagnosis, and therapeutic management of metastatic LNs, thereby providing a comprehensive foundation for researchers and clinicians focused on the role of the lymphatic system in cancer.
Anatomy and physiology of lymph nodes
As central hubs for the induction of adaptive immunity, individual LNs process lymph containing local information from the tissues that drains via collecting lymphatic vessels from proximal tissues and organs.3 The human body contains an estimated 500 to 600 LNs that are surrounded by dense connective tissue and associated with particular nerves, lymphatic vessels, and blood vessels, with many of these LNs presenting in concentrated clusters found in specific anatomical locations.4,5
Afferent lymphatic vessels deliver lymph to the LNs. Each LN is comprised of a complex series of lymphatic sinuses associated with organized parenchyma consisting of reticular fibers, fibroblastic reticular cells (FRCs), specialized vasculature, and a range of immune cell populations. A fibrous capsule surrounds the outer layer of each LN (Fig. 1), and connective tissue projections radiating from this capsule, known as trabeculae, extend into the node. The trabecular sinuses separate human LNs into multiple compartments, which are associated with the opening of each afferent lymphatic vessel, or each of its terminal branches, into the subcapsular sinus, though these same trabecular compartments are not evident in murine LNs.6 The entirety of the LN cortex and paracortex is overlaid by the subcapsular sinus, and lymphatic endothelial cells (LECs) line each sinus, forming a barrier between the lymph and the parenchymal compartment. The trabecular sinuses connect the medullary and subcapsular sinuses, with direct connections between the latter two sinuses also forming at the margins of each LN.7 After flowing through the medullary sinuses, lymph passes into efferent lymphatic vessels.8 The macrophage, B cell-, and antibody-producing plasma-cell-rich medullary cords, together with the medullary sinuses, comprise the medulla layer within LNs.9 In the cortex, germinal follicle-associated antigen-presenting follicular dendritic cells (DCs) can activate naïve B cells, while in the paracortical T cell zone, antigen-presenting DCs promote naïve T cell activation.6

An anatomical overview of the structural characteristics of lymph nodes. LEC lymphatic endothelial cell, FRC fibroblastic reticular cell
Lymphocytes circulating in the blood enter LNs through specialized cuboid blood vessels known as high endothelial venules (HEVs), which exhibit a large surface area and consist of specialized blood endothelial cells (BECs).10 These HEVs are found in the extrafollicular cortical zone and extend into the peripheral paracortex before transitioning into standard venules upon entry into the medullary cords.6 HEV endothelial cells express a range of adhesion molecules that improve the rates of lymphocyte capture and entry into the associated LN, including CD34, glycosylation-dependent cell adhesion molecule 1 (GLYCAM1; only in mice), podocalyxin, endomucin, nepmucin, and 6-sulpho sialyl Lewis X.11
FRCs are lymphoid-specialized fibroblasts that form the structural framework for scaffolding that defines specific microenvironmental immune cell niches within LNs.10 These FRCs can secrete a range of extracellular matrix (ECM) proteins and form a three-dimensional conduit network system,12 which acts as a pipeline to monitor the status of fluid-draining peripheral tissues while exporting antibodies and other molecules produced within the local lymphoid compartment.13 FRCs can be further classified into functionally distinct subtypes localized to specific sites within LNs, including T cell zone FRCs (TRCs), follicular DCs (fDCs), marginal reticular cells (MRCs), and medullary FRCs (medRCs), all of which express a range of ligands, chemokines, and other cytokines important for the maintenance of LN homeostasis.14
Molecular mechanisms of lymph node metastasis
Lymphatic dissemination has been documented for myriad cancer types, underscoring the need for research focused on clarifying how tumor cells migrate to and survive within LNs.8 Several mechanistic studies have provided detailed insight into the mechanistic basis for LNM.15 The ability of tumor cells to migrate to and invade LNs is often associated with the expression of particular receptor proteins and cytokines, eventually culminating in the evasion and/or suppression of normal immune function such that these malignant cells can thrive within the LN microenvironment.3 In this section, we provide a summary of the current understanding of the molecular basis for LNM with a particular focus on recent research progress (Fig. 2).

Molecular mechanisms of lymph node metastasis.15 LN lymph node, LEC lymphatic endothelial cell, ECM extracellular matrix, FRC fibroblastic reticular cell
Tumor cell migration toward lymph nodes
Fluid dynamics play an important role in the initiation of LNM. The blood vessels present are generally abnormally permeable and exhibit aberrant blood flow such that plasma persistently accumulates in extracellular sites and is not effectively drained owing to the compression of local lymphatic vessels by the growing tumor. This results in a pronounced increase in the intratumoral interstitial fluid pressure (IFP),16 forming an IFP gradient that favors the flow of interstitial fluid from tumors through the surrounding stroma and into areas of lower IFP, thereby enabling tumor cells and tumor-derived compounds to more readily access LNs.17 Through the establishment of a corresponding mathematical model, Jain et al.18 posited that this IFP gradient in the tumor margin, rather than high intratumoral IFP alone, is responsible for determining the rate of tumor cell entry into the surrounding lymphatic system and the associated induction of angiogenic activity. In further support of such a model, dynamic contrast-enhanced magnetic resonance imaging (MRI) studies have reaffirmed that higher IFP levels are detectable in the primary tumors of mice positive for metastatic progression as compared to mice without such metastases, as has further been confirmed in patients with cervical cancer positive for pelvic LNM.19 However, direct experimental data conclusively demonstrating the role of this IFP gradient as a driver of LNM incidence is lacking at present. In addition, as flow velocity and associated shear stress increase, cells may be more prone to growth arrest, fragmentation, and death. Even so, the lower levels of shear stress to which tumor cells are exposed in the lymphatic system, as compared to the higher flow velocities evident in blood vessels, are conducive to the survival of these malignant cells and their subsequent invasion of LNs.16
LNM can also be induced and regulated by the responses of tumor cells and other cells in the local microenvironment to interstitial fluid flow-related mechanical signals. Indeed, there is strong evidence for the ability of interstitial fluid flow to enhance the glioma cell invasion via the CXCR4/CXCL12 signaling axis.20 Interstitial fluid flow can also control breast cancer cell ameboid migration,21 and transcellular CCR7 ligand gradients can reportedly be shaped by this interstitial flow, thereby promoting the migratory activity of tumor cells and associated LNM.22 Interstitial flow can also promote macrophage M2 polarization and enable these cells to travel against this flow to access tumors, thus contributing to metastatic progression.23
Chemokines are also essential mediators of the ability of tumor cells to migrate toward LNs. The upregulation of CCL21 in LECs can, for example, enable tumor cells expressing CCR7 to more readily migrate toward the lymphatic vessels.24 Similarly, TNF, IL-1β, and LPS can induce the upregulation of CCL1, which is present in the lymphatic sinuses of LNs but absent in the peripheral lymphatic system, providing a gradient that allows tumor cells to migrate to LECs.25 LECs also express a variety of other chemokine ligands, including CXCL10, CXCL12, CXCL1, and CCL5, that respectively bind to CXCR3, CXCR4, CXCR2, and CCR5, thereby shaping tumor cell migration through lymphatic vessels and to LNs.26
Tumor cells can additionally adopt more aggressive phenotypic characteristics conducive to LN migration. The epithelial-mesenchymal transition (EMT) process entails the loss of epithelial-like characteristics such as polarization and a high degree of differentiation by tumor cells, which instead adapt invasive and migratory mesenchymal-like phenotypes, allowing these cells to more readily migrate and disseminate away from the primary tumor site.27 In hepatocellular carcinoma (HCC), for example, significantly elevated rates of EMT-associated features are evident in tumor samples from cases exhibiting LNM.28 Many different factors that can induce this EMT process have been identified and shown to be closely related to LNM. Heat shock factor 1 (HSF1), for instance, promotes the upregulation of lymphoid enhancer‐binding factor 1 (LEF1) to drive EMT induction and LNM.29 PRMT5 can similarly induce EMT and LNM via the modulation of Wnt4/β-catenin pathway signaling.30 NQO1/PKLR alters glycolytic reprogramming in tumor cells to favor EMT onset and migratory activity.31 Moreover, Zhao et al.32 have further demonstrated the upregulation of dynamin-related protein 1 (Drp1), which is associated with mitochondrial fission, in invasive breast carcinoma patients exhibiting LNM, revealing that this protein promotes the redistribution of mitochondrial to lamellipodial regions at the leading edge of cancer cells in a manner that supports migration.
Regulation of lymphangiogenesis
More dense lymphatic vessels have been reported in peritumoral regions as compared to healthy tissues, and intratumoral lymphatic vessel growth has also been documented.33 The process of lymphangiogenesis is closely associated with the formation of new lymphatic vessels within sentinel lymph nodes (SLN), ultimately supporting metastatic tumor spread. The enhancement of lymphangiogenic activity is thus crucial to the effective dissemination of tumor cells into LNs, and many different lymphangiogenesis-related factors have been demonstrated to be important in the context of LNM.
Vascular endothelial growth factor (VEGF)-C and VEGF-D play key roles in the regulation of lymphangiogenesis. Cancer cell-derived VEGF-C/D activates its receptor, vascular endothelial growth factor receptor (VEGFR)-3 found on LECs to activate a protein kinase C/ERK signaling cascade which ultimately triggers the phosphorylation of AKT and the proliferation and migration of these LECs, thus promoting lymphangiogenesis.34 VEGFR-3 activation can also drive the activation of HOXD10, which is a homeobox family transcription factor that regulates cord-like structure formation and the migration of LECs via the control of VE-cadherin, claudin-5, and nicotinamide adenine dinucleotide phosphate oxidase 3 (NOS3) expression.35 The promotional effect of VEGF-C/D and VEGFR-3 on lymphangiogenesis and LNM has been documented in a range of cancer types.36,37,38,39,40,41
Additionally, there are many cytokines, enzymes, bioactive lipids, chemokines, adhesion molecules, and noncoding RNAs that participate in lymphangiogenesis by functioning in either a VEGF-C/D-dependent or -independent manner.
Several lymphangiogenesis- and LNM-related growth factors have been characterized to date, including fibroblast growth factor (FGF)-2, which can bind FGFR3 on the surface of LECs to promote the development of lymphatic vessels.42 Platelet-derived growth factor (PDGF)-BB can similarly promote vessel growth by binding to PDGF receptor α (PDGFRα) and PDGFRβ of LEC.43 In cholangiocarcinoma, fibroblasts have been shown to produce elevated VEGF-C levels and to promote lymphatic vessel expansion following PDGF-D stimulation.44 Signaling via the angiopoietin 2 (Ang2)/Tie/PI3K axis is essential for the expression of VEGFR-3 on the surface of cells, making this pathway critical in the context of lymphangiogenesis.45 Interactions between FGF-2 and VEGF-C are also capable of driving intratumoral lymphangiogenesis.46 In a model of colorectal cancer (CRC), lymphangiogenesis and metastatic growth were shown to be induced by insulin-like growth factor (IGF)-1.47 Epidermal growth factor (EGF) is associated with the induction of melanoma primary tumor lymphangiogenesis.48 There is also evidence for the ability of hepatocyte growth factor (HGF) to promote the proliferation of LECs and the development of lymphatic vessels via a VEGFR-3-independent pathway.49 TGF-β/Smad signaling is also central to the regulation of lymphangiogenesis, as TGF-β can promote VEGF-C upregulation via the Smad and Smad-independent AKT pathways, which has been documented in gastric cancer cells.50 However, TGF-β also downregulates the lymphangiogenic function of collagen and calcium-binding EGF domain-1 (CCBE1) in cancer‐associated fibroblasts (CAFs) and colorectal cancer cells by directly binding Smads to the CCBE1 gene locus.51 Furthermore, VEGF-D promoter activity and protein level expression can also be induced by TNF-α through ERK1/2/AP-1 pathway signaling, ultimately eliciting tube-forming activity in LECs.52
The interaction between interleukin (IL) and lymphangiogenesis reflects the influence of immune cells on lymphangiogenesis in LNM. For instance, IL-6 has been demonstrated to promote lymphangiogenesis in gastric cancer via the signal pathway of JAK-STAT3-VEGF-C.53 Similarly, IL-7 can promote the development of lymphatic vessels in lung and breast cancers by inducing VEGF-D upregulation.54,55 In non-small cell lung cancer (NSCLC), IL-17 has also been linked to poorer patient survival outcomes owing to its ability to drive VEGF-C secretion and lymphangiogenesis.56
Fatty acid synthase (FASN) is a central coordinator of lipid metabolism that is upregulated in many cancers.57 In melanoma cells, a link between FASN and VEGF-C/D expression has been noted, likely influencing lymphatic vessel permeability.58 FASN can also reportedly promote PDGF-AA and IGFBP3 secretion in cervical cancer, thus promoting lymphangiogenesis.59 The cyclooxygenase-2 (COX-2)/prostaglandin E2 (PGE2)/EP signaling axis is also important in this regulatory context, promoting tumor-associated lymphangiogenesis via inducing VEGF-C and VEGFR-3 upregulation in the tumor stroma in a manner that can be suppressed by COX-2 inhibitor celecoxib.60
Sphingosine 1-phosphate (S1P), which is generated by sphingosine kinase 1 (SphK1), has further been established as a mediator of lymphangiogenic activity in murine breast cancer metastasis model systems.61 By binding to S1PR1 expressed on the surface of tumor-associated macrophages (TAMs), S1P can induce lymphatic vessel development in a macrophage-dependent manner.62 Lysophosphatidic acid (LPA) is another lymphangiogenesis-related lipid, with both LPA1 and LPA3 reportedly inducing the upregulation of VEGF-C in prostate cancer through a calreticulin-dependent mechanism that induces lymphangiogenesis.63
Both chemokines and adhesion molecules are key mediators of lymphangiogenic activity. For example, integrin α4β1, which is expressed by proliferating LECs, is essential for lymphangiogenesis in the context of LNM.64 CCL21/CCR7 signaling can also promote enhanced VEGF-C secretion and consequent lymphatic vessel growth.65 Bieniasz-Krzywiec et al.66 determined that binding interactions between podoplanin on the surface of TAMs and galectin 8 (GAL8) expressed by LECs can promote pro-migratory integrin β1 activation, thereby enabling TAMS to migrate toward and adhere to LECs, facilitating TAM‐mediated lymphangiogenesis. The adhesion molecule CD146 is expressed by endothelial cells and many different tumor types, and functions as a receptor for VEGF-C that can regulate lymphangiogenesis.67
A growing body of research has also documented the importance of ncRNAs as regulators of lymphangiogenic and metastatic activity. For example, He et al.68 revealed a role for the long noncoding RNA (lncRNA) bladder cancer-associated transcript 2 (BLACAT2) as a regulator of VEGF-C expression through its ability to associate with the core H3K4 methyltransferase complex subunit WDR5, ultimately inducing bladder cancer-related lymphangiogenesis. Chen et al.69 further identified LNM-associated transcript 2 (LNMAT2) as a lncRNA packaged in exosomes that can stimulate LEC migration, tube formation, and bladder cancer-associated lymphangiogenesis and LNM. Zheng et al.70 investigated the biological effects of novel triple-negative breast cancer (TNBC) lymph node-associated lncRNA LINC00857, also known as lncRNA highly upregulated in metastatic TNBC (HUMT). They found that HUMT could recruit Y-box binding protein 1 (YBX1) to form a novel transcriptional complex capable of activating forkhead box k1 (FOXK1) to promote VEGF-C upregulation. Circular RNAs (circRNAs) can exert similar regulatory roles in this context, as in the case of circEHBP1, which reportedly favors bladder cancer-associated lymphangiogenesis through the miR-130a-3p/TGFβR1/VEGF-D signaling axis.71 Meanwhile, circNFIB1 (hsa_circ_0086375) can inhibit lymphangiogenesis and LNM via the miR-486-5p/PIK3R1/VEGF-C axis in pancreatic cancer.72
Formation of premetastatic niche in lymph nodes
Secondary metastatic tumor development is thought to be enabled by the establishment of a premetastatic niche, which consists of a microenvironment shaped and seeded by a range of tumor-derived factors such that it is better suited to supporting the proliferation and survival of disseminated malignant cells.8 Premetastatic niche formation is controlled by the coordinated effects of cytokines, chemokines, and extracellular vesicles (EVs).
Changes in the LN vasculature are central to the process of premetastatic niche establishment within these LNs. Exosomes produced by melanoma cells can be home to SLNs, wherein they induce the production of VEGF-B, HIF-1α, and other angiogenic growth factors that induce local vascular proliferation.73 Particularly, HEV remodeling is a characteristic process in the formation of premetastatic niches in LNs, with SLNs reportedly exhibiting increased HEV density prior to tumor cell arrival.74 The tall endothelial cells within HEVs undergo morphological changes such that they exhibit flat endothelial cell phenotypes. These changes coincide with the remodeling of HEVs from thick-walled endothelial vessels with a small lumen to thin-walled vessels with a larger lumen, causing a functional shift away from lymphocyte recruitment in favor of greater blood flow that is conducive to metastatic tumor cell arrival.75 Bone morphogenetic protein-4 (BMP-4) loss has also been linked to this thin-walled HEV remodeling,76 as has CCL21 dysregulation in perivascular FRCs and associated CCL21-saturated lymphocyte accumulation.77
Premetastatic niche formation is also associated with changes in LEC characteristics. For example, The activation of integrin α4β1 on LECs through a VEGF-C/PI3Kα-associated pathway can promote LN remodeling via the expansion of the local lymphatic endothelium and the enhanced capture of metastatic cells expressing vascular cell adhesion molecule 1 (VCAM-1).78 CAFs expressing high periostin levels that are present within the metastatic LN-associated stroma can interfere with the integrity of the lymphatic endothelial barrier as a consequence of LEC-specific integrin‐FAK/Src‐VE‐cadherin pathway activation, thus promoting LNM.79 Integrin αIIb is also upregulated in LECs present within tumor-draining LNs (TDLNs), enabling these LECs to adhere to fibrinogen in a manner that may improve metastatic tumor cell adherence and survival.80
The remodeling of the ECM is also integral to the process of premetastatic niche formation in various organs.81 Exosomes produced by tumor cells can promote the upregulation of a range of ECM-associated factors that can ultimately better entrap migratory tumor cells within SLNs.73 FRCs are the primary cell type responsible for ECM production within LNs, and they may thus serve as particularly important mediators of ECM remodeling within LNs in the context of LNM.82 The production of laminin α4 by FRCs, for example, can enhance T cell migration while promoting the differentiation of Tregs and interfering with the development and activation of other T cell subsets, contributing to the formation of a tolerogenic LN niche.83 Evidence regarding the ability of FRCs to directly regulate the ECM in premetastatic LNs, however, is currently lacking, underscoring a need for further research.
FRCs can also shape the premetastatic niche through various other mechanisms. Riedel et al.84 showed that before metastatic colonization, tumor-derived lactic acid could drain to LNs, contributing to IL-7 downregulation and altered FRC mitochondrial function. IL-1 production by melanoma cells can suppress FRC contractility through JAK1/STAT3 pathway inhibition, with the consequent relaxation of the 3D FRC network, better-enabling melanoma cells to invade this niche.85 Transcriptional analyses of FRCs in TDLNs have provided evidence of microenvironmental reprogramming, including the expansion and structural reorganization of stromal compartments and the suppression of CCL21 and IL-7 production by FRCs, enabling greater tumor cell immune evasion and impaired immune cell homing.86
The ability of tumor cells to seed LNs is strongly dependent on the establishment of an immunosuppressive microenvironment. Strikingly, single-cell studies focused on human prostate cancer progression have revealed that immunological changes precede metastatic progression.87 Otto et al.88 collected tumor regional and distant lymph nodes from patients with esophageal cancer and found that premetastatic LNs associated with more advanced tumors exhibited characteristics consistent with a greater degree of immunosuppression. In patients with breast carcinoma, lower levels of Th1 response induction and DC maturation have also been reported in SLNs before LNM.89 Comparative analyses of breast cancer patient SLNs have further revealed that increased Treg and myeloid-derived suppressor cell (MDSC) activity occurs before nodal involvement, together with the general anergy of T cells within these LNs as a consequence of impaired LN-resident DC activation.90 TAM accumulation in gastric cancer-associated premetastatic LNs can also reportedly facilitate tumor progression by promoting the production of VEGF and MMP while also suppressing antitumor immune responses by releasing cytokines, including IL-10.91 In a Lewis lung carcinoma (LLC) metastasis model system, DCs present in LN subcapsular regions were found to induce the recruitment of Tregs during LNM through the COX-2/EP3-dependent production of stromal cell-derived factor 1 (SDF-1).92 In a mouse mammary tumor model system, high levels of immunosuppressive Treg accumulation were also noted during primary tumor growth in compartments, including TDLNs, wherein these cells were able to suppress NK cell activation and support more robust LNM.93 In the context of gastric cancer LNM, IL-8 production by CAFs can induce CD8 + T cells to upregulate PD-1 within the premetastatic niche, thereby hamstringing the induction of antitumor immunity. The intratumoral upregulation of S1PR1/STAT3 can also spur the production of S1PR1/STAT3-activating factors by various cells within LNs and other premetastatic sites, thereby better enabling myeloid cell colonization and consequent metastasis.94 B cells can also reportedly shape the process of premetastatic niche development. Substantial B cell recruitment and proliferation in TDLNs can be induced by primary tumor cells, potentially resulting in the production of pathogenic antibodies targeting HSPA4/ITGB5 that can activate Src/NF-κB signaling within tumor cells, ultimately supporting metastasis via the CXCR4/SDF-1α axis.95 Neutrophils similarly serve as regulators of premetastatic niche formation, with IL-17 produced by γδ T cells serving to promote the systemic expansion and polarization of neutrophils in a granulocyte colony-stimulating factor (G-CSF)-dependent manner, ultimately suppressing CD8 + T cells activity and promoting LNM.96
Metabolic adaptation of tumor cells in lymph nodes
After reaching the LNs, tumor cells undergo a series of metabolic changes to adapt to the microenvironment. LNs are rich in lipids, and it has been confirmed that tumor cells present in metastatic LNs reportedly exhibit increased reliance on lipid metabolism, stimulating signaling via the fatty acid oxidation (FAO) and peroxisome proliferator–activated receptor (PPAR)-αpathways, allowing these cells to accumulate larger volumes of FAs as compared to the primary tumor cells.97 Fatty acid-binding protein 5 (FABP5) can reportedly reprogram FA metabolism in cervical cancer in a manner that favors FA synthesis and lipolysis, thus supporting LNM.98 Shang et al.99 confirmed that the lncRNA LNMICC is capable of recruiting the nuclear factor NPM1 to FABP5, which could be directly targeted and suppressed by miR-190, thus promoting LNM. The overexpression of CD36, a receptor at the top of the signaling cascade that takes up lipids from the extracellular environment, greatly promotes LNM in cell lines or patient-derived cells with low metastatic potential oral carcinomas, with penetrance increasing from less than 20% to 75–80%.100 Furthermore, bile acids can additionally trigger yes-associated protein (YAP)-dependent metabolic changes in tumor cells that ultimately favor their metabolic shift towards increased FAO activity.97 Jia et al.101 found that RPRD1B, a transcriptional coactivator, facilitates FA metabolism and promotes LNM via the c-Jun/c-Fos sterol regulatory element-binding protein 1 (SREBP1) axis, which is enhanced by lncRNA nuclear enriched abundant transcript 1 (NEAT1).
Immune evasion in metastatic lymph nodes
Tumor cells that successfully colonize LNs generally exhibit phenotypes conducive to the evasion of immune-mediated detection. Major histocompatibility complex (MHC) expression is crucial for the presentation of tumor cell-derived antigens to local immune cells, and many tumor cells exhibit decreased MHC expression such that they can avoid T cell-mediated elimination.102,103 Yoshii et al. observed MHC downregulation in metastatic LNs compared with its expression in primary lesions in clinical samples of gastric carcinoma.104 The loss of MHC-I expression has also been documented in the TDLNs of many breast cancer patients.105 Consistently, the expression of higher MHC-II levels in breast cancer has been linked to a lower risk of lymphovascular invasion and better prognostic outcomes in patients with LNM.106 In a murine melanoma LNM model system, however, strong upregulation of MHC-I-encoding genes was observed, thereby enabling tumor cells to evade NK cell-mediated cytotoxicity normally induced by the loss of MHC-I.107 Therefore, the precise role that MHC proteins play in shaping the process of LNM thus warrants further research. Moreover, PD-L1 upregulation has been noted in the TDLNs for various tumor types, contributing to the suppression of T-cell responses and enhanced LNM.107,108
The ability of tumor cells within LNs to interact with immune cells shapes the consequent induction of immune tolerance, thereby enabling tumor cells to evade immune-mediated killing such that distant metastases can continue developing. LN metastases have been demonstrated to suppress NK cell-mediated cytotoxicity in cases of early-stage head and neck cancer.109 These metastatic cells in LNs can resist the cytotoxic effects of CD8+ T cells while promoting the differentiation of antigen-specific naïve CD4+ T cells into Tregss.107 In breast cancer TDLNs, higher frequencies of Tregs have been noted in the context of nodal invasion. These Tregs also express elevated co-inhibitory/stimulatory receptor protein levels relative to effector cells and function as mediators of immunosuppressive activity within the LNs.110 Tregs also secrete TGF-β1, which promotes the Smad2/3/4-mediated upregulation of the oncogenic receptor protein IL-17rb on cancer cells within the TDLNs, facilitating sustained oncogenic progression.111
Clinical significance of lymph node metastasis
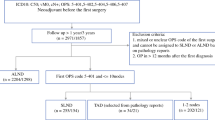
LNM is a key parameter that is taken into consideration when evaluating cancer patients, with the ability of LNM to strongly predict cancer patient survival being a subject of intensive scrutiny and debate.112 The presence of cancer cells in LNs could not only reflects the metastatic ability of the primary tumor, but also leave and colonize in distant organs.113 Multiple pre-clinical reports have highlighted the ability of metastatic cells from LNs to migrate to distant sites.114,115,116 Naxerova et al.,117 for example, conducted an analysis of 213 archived biopsy samples from 17 CRC patients, and ultimately found that the lymphatic and distant metastases developed from separate primary tumor subclones in 65% of cases, while they exhibited a shared subclonal origin in the remaining 35% of cases. This suggests that, at least in certain cancer types, metastatic tumor cells within LNs may subsequently disseminate to other organs.3 Lymphatic staging thus plays a key role in the evaluation of cancer patients, as when it is accurately performed, this can ensure that patients receive the most appropriate therapies in order to maximize their odds of positive clinical outcomes.118 If understaging occurs, patients may be subjected to unnecessary local surgery/radiotherapy or the omission of appropriate systemic therapy, whereas the opposite may occur in cases of overstaging as a result of inadequate LN staging.119 The most widely used cancer staging system in the world at present is the 8th edition of the tumor-node-metastasis (TNM) system established by the American Joint Committee on Cancer (AJCC), which serves as a benchmark for tumor patient classification, treatment selection, and prognostic evaluation.120,121,122 The TNM system takes several factors into consideration, including the morphology and location of the primary tumor, the number and location of involved regional LNs, and the absence or presence of distant metastases. In the following section, we provide a detailed overview of the clinical significance of LNM in different anatomical sites (Fig. 3).

Representative tumors types involving lymph node metastasis in different anatomical regions
Lymph nodes of the head and neck
The cervical region of the head and neck harbors an estimated 150–300 LNs, the majority of which are located at the border between the head and neck. As such, LNM evaluation is particularly important in cases of thyroid or head and neck cancer.123 The AJCC classification system separates the cervical LNs into seven levels, with levels I, II, III, IV, V, VI, and VII, respectively, including the submental and submandibular LNs, upper internal jugular chain LNs, middle internal jugular chain LNs, lower internal jugular chain LNs, spinal accessory and transverse cervical chain LNs, anterior cervical nodes, and upper mediastinal LNs (Fig. 4).124 Nodes not included in these levels are instead referred to by their nodal groups, and include the periparotid, postauricular, suboccipital, retropharyngeal, and buccinator LNs.125

Schematic diagram of the neck showing the AJCC classification of the cervical nodes124
In thyroid carcinoma patients, patient nodal status is assessed based on the regions of metastatic LNs and whether they exhibit ipsilateral, bilateral, or contralateral locations.126 In head and neck cancer, however, factors including LN size, LN staging, location (bilateral/contralateral/ipsilateral), and extranodal extension (ENE) are taken into consideration, with ENE being characteristic of aggressive tumors such as cancer of the oral cavity.127 ENE status is associated with marked differences in head and neck cancer patient survival, and it has been best studied in this cancer type as a result.128 The left supraclavicular node, also known as Virchow’s node, is a terminal thoracic duct LN and a common site of distal metastasis in patients with abdominal and pelvic cancers that can influence treatment planning. Supraclavicular nodes are also relevant when diagnosing metastatic thoracic malignancies, although thoracic tumors do not exhibit any specific preference for the left or right supraclavicular nodes.129
When treating head and neck cancer patients, multidisciplinary assessment is vital, given that the most appropriate treatment options vary as a function of disease stage, anatomical region, and accessibility for surgical treatment.130 Cervical LN management comprises an important aspect of the surgical treatment of affected patients, with the choice of selective or comprehensive neck dissection being performed in accordance with preoperative clinical staging results.131 When selective neck dissection is performed, the target region is chosen based on the primary tumor location and the risk of occult metastasis within the corresponding nodal basin. The ipsilateral side of the neck generally exhibits the greatest risk of LNM. Bilateral neck dissection is generally necessary for tumors situated in areas that are often subject to bilateral lymphatic drainage, such as the base of the tongue, palate, supraglottic larynx, hypopharynx, nasopharynx, and deep pre-epiglottic space. In patients exhibiting advanced lesions involving the floor of the anterior tongue, the floor of the mouth, or alveolus that approximate or cross the midline, contralateral selective/modified neck dissection is required.127 In patients with advanced disease and regional LNM, chemoradiotherapy or radiotherapy can offer benefits both in the form of adjuvant treatment after surgical resection and neck dissection, or as the primary treatment in cases of unresectable disease.130
Lymph nodes of the upper extremity
The axillary LNs are closely associated with breast cancer, and include the apical axillary (infraclavicular), interpectoral (Rotter’s), central axillary, lateral axillary (humeral), posterior axillary (subscapular), and anterior axillary (pectoral) nodes. The ipsilateral axilla is the predominant site of mammary lymphatic drainage, while ~3% of the mammary lymph drains to the internal mammary chain LNs, and even less drains to other LNs that can include the intercostal, interpectoral, periclavicular, paramammary, contralateral breast, or abdominal nodes.132 LN status is among the most important prognostic factors in breast cancer patients, with LNM being evident in approximately one in three patients and associated with a worse prognosis as compared to node-negative status.133 The LN staging for breast cancer in the AJCC 8th edition is determined by the status of axillary, internal mammary, and supraclavicular LNs.134 The axillary LNs are separated into levels I, II, and III. Level I LNs are located lateral to the lateral border of the pectoralis minor muscle, while level II LNs, which include the Rotter nodes, are positioned beneath the pectoralis minor muscle between its lateral and medial borders, and level III LNs, which are associated with a poorer prognosis, are infraclavicular LNs positioned medial to the medial margin of the pectoral minor muscle and beneath the clavicle.135
SLN biopsy (SLNB) is routined performed when staging breast cancer patients and selecting appropriate treatments.136 In two different randomized clinical trials (American College of Surgeons Oncology Group-Z0011 and International Breast Cancer Study Group 23-01),137,138 no clinical improvements were noted for breast cancer patients that underwent additional axillary surgery beyond the sentinel TDLN, with axillary LN dissection (LND) instead often resulting in severe complications such as shoulder dysfunction, dysaesthesia, and lymphoedema.139,140 The predictive utility and accuracy of SLNB have since been demonstrated in multiple reports such that SLNB has replaced LND as the standard approach to evaluating the axillary LN status of clinical LN-negative breast cancer patients.139,141
In the randomized “After Mapping of the Axilla: Radiotherapy or Surgery” clinical trial, excellent axillary control was successfully achieved through both axillary LND and axillary radiotherapy,142 with comparable overall and disease-free survival rates in these two treatment groups.143 This suggests that axillary radiotherapy in primary breast cancer patients with positive anterior LN biopsy results is as efficacious as axillary LND. Prospective randomized trials conducted in Denmark and Canada have further demonstrated that post-mastectomy adjuvant chemotherapy treatment can improve patient survival while reducing the risk of local recurrence, reflecting the value of adjuvant chemotherapy and radiotherapy as a means of preventing tumor recurrence and fatal metastasis.144,145 Neoadjuvant chemotherapy is also increasingly being employed as a treatment option in breast cancer patients,146,147,148,149 and it has been shown to reduce the likelihood of axillary LND in both patients undergoing mastectomy and patients with biopsy-confirmed LNM.150
The epitrochlear LNs positioned in the subcutaneous connective tissue on the medial elbow 4–5 cm above the humeral epitrochlea are also superficial nodes present in the upper extremities.151 The epitrochlear and axillary LNs are often regarded as “in transit” targets for tumor cells derived from primary tumors situated on the hand, wrist, or forearm in cases of rhabdomyosarcoma or melanoma, and the association between epitrochlear LN status and prognostic outcomes should be taken into consideration.152,153
Lymph nodes of the chest
LNs situated on the chest wall can serve as sites for metastatic tumor progression. Much like axillary LNs, the internal mammary nodes, also referred to as the parasternal nodes, are regarded as first-tier sites for breast cancer drainage. The chain of internal mammary LNs spans the first to the sixth intercostal spaces.135 An estimated 4–9% and 16–65% of axillary node-negative and axillary node-positive patients, respectively, exhibit internal mammary LN metastasis. As a result, the treatment of breast cancer often entails both surgical axillary clearance and the elective irradiation of non-dissected internal mammary and medial supraclavicular LNs in patients exhibiting axillary node positivity or tumors that are medially or centrally located.151 These intercostal nodes can also rarely serve as sites of extra-axillary breast tumor metastasis, although they rarely have any impact on treatment selection or patient prognosis.154 These intercostal nodes can also be sites of metastatic involvement in patients diagnosed with malignant pleural mesothelioma, which is among the deadliest forms of cancer.155,156
A growing number of studies have explored the associations between thoracic visceral tumors, such as esophageal and lung cancers, and thoracic LNs. The pulmonary lymph drains from the lungs to the LNs proximal to the lobar bronchi, with subsequent drainage to extrapulmonary tracheobronchial LNs. The efferent lymphatics of these nodes, in turn, extend to the left and right mediastinal lymph trunks, potentially draining into the thoracic duct or directly into the ipsilateral brachiocephalic vein.157 Nodal status is among the most reliable prognostic indicators in lung cancer patients, making it vital to the selection of optimal therapeutic approaches.158,159 The International Association for the Study of Lung Cancer (IASLC) established an LN map in 2009 that provides detailed anatomic definitions for all LN stations (numbered 1–14), which are grouped into the supraclavicular, upper, aortopulmonary (AP), subcarinal, lower, hilar/interlobar, and peripheral zones, enabling more reliable analyses of the association between these nodes and survival outcomes (Fig. 5).160 According to the TNM staging system, lung cancer nodal status of lung cancer is based upon the anatomical locations of metastatic nodes rather than on the number thereof, in which N1 refers to metastasis in ipsilateral peribronchial and/or ipsilateral hilar LNs and intrapulmonary nodes (including involvement by direct extension), N2 refers to metastasis in ipsilateral mediastinal and/or subcarinal LN(s), and N3 refers to metastasis in contralateral mediastinal, contralateral hilar, ipsilateral or contralateral scalene, or supraclavicular LN(s); whereas in esophageal cancer, which shares many of the same lymphatic pathways within the thoracic cavity, nodal status is only based on the number of metastatic nodes.158 In a multivariate analysis of 3,971 patients with NSCLC who underwent complete resection and systematic LND, the nodal status of different LN zones and stations were identified as independent predictors of recurrence and overall survival.161 Both the number and locations of metastatic nodes offer prognostic significance in patients with NSCLC, with more proximal N1 station involvement correlating with a worse prognosis.162 N1 and N2 staging based on the involvement of nodes from one or more stations has yet to be adopted, as results derived from pathologically staged tumors could not be validated at clinical staging, and the degree of examination thoroughness can readily impact the results of staging performed according to the number of involved stations.163

The IASLC LN map for lung cancer160
In stage I or II NSCLC patients, surgery offers the greatest chance of curative outcomes.164 The current NCCN guidelines for NSCLC patients indicate that N1 and N2 node resection and mapping should be standard in patients undergoing lung tumor resection, with a minimum of three N2 stations undergoing sampling or complete LND being performed. For patients undergoing respective treatment of stage IIIA (N2) NSCLC, formal ipsilateral mediastinal LND is recommended.165 In cases of pathologic N1 disease, current recommendations suggest the administration of a platinum-based dual adjuvant chemotherapy regimen after surgery.166 Neoadjuvant chemotherapy and resection can provide benefits to stage IIIA (N2) patients exhibiting preoperative mediastinal LN negativity and one positive node <3 cm in size, with definitive chemoradiotherapy otherwise being recommended.167 Surgery is not recommended for individuals diagnosed with N3 disease, who should instead be administered systematic regimens consisting of some combination of radiotherapy, chemotherapy, immunotherapy, and targeted therapy.168
Lymph nodes of the abdomen
Abdominal lymphatic drainage pathways parallel the vessels that supply blood to or drain blood from organs. Many abdominal LNs are located in the mesentery, mesocolon, and peritoneal ligaments, providing sites for the potential metastasis of gastric, hepatic, renal, pancreatic, intestinal, or gallbladder tumors. Here, gastric cancer was selected as a representative tumor type. There are four primary zones of gastric lymph drainage. The superior gastric nodes that surround the left gastric artery are responsible for the lymphatic drainage of the proximal portion of the stomach, whereas the suprapyloric nodes drain the lesser curvature, the subpyloric nodes drain the right gastroepiploic vessels, and the pancreaticosplenic nodes drain the stomach body and fundus along a course that parallels the left gastroepiploic and short gastric arteries. All lymph draining from the stomach ultimately flows to the celiac nodes situated at the base of the celiac artery.169 As the stomach has an extensive lymphatic network,170,171 LNM is a common finding in gastric cancer patients.172 Even in patients with early gastric cancer, the incidence of LNM is approximately 10%,173 while the incidence of bloodstream metastases is just 0.2% of these same patients.174 Per the Japanese Gastric Cancer Association (JGCA) anatomical definitions of LN stations (Table 1 and Fig. 6), LN stations 1–12 and 14 v are defined as regional gastric LNs, with metastases to any other nodes resulting in M1 classification.175 In the AJCC 8th edition TNM staging of gastric cancer, the number of metastatic nodes is used to determine nodal status, including N1 (1–2 regional metastatic LNs), N2 (3–6 regional metastatic LNs), and N3 (7+ regional metastatic LNs). N3 cases can also be subdivided into N3a (7–15 metastatic regional LNs) and N3b (16+ metastatic regional LNs).176

Location of LN stations for nodal status evaluation of gastric cancer175
When the LNM of gastric cancer is limited to the perigastric LNs, it can generally be cured by lymph node dissection (LND).177 However, the more appropriate extent of LND in gastric cancer patients remains somewhat controversial. While incomplete LND has the potential to contribute to tumor recurrence as a result of inadequate tumor clearance, broader LND procedures are associated with a greater risk of postoperative complications.178 At present, the “D” numbering system is used when discussing the extent of LND in gastric cancer patients, which is classified as D1, D1+, D2, or D3. Under this system, D1 and D2 respectively correspond to the complete dissection of group 1 and 2 LNs. The locations of these nodes, however, are defined by the surgery type (distal or total gastrectomy), rather than by the location of the primary tumor (Fig. 7). D3 entails the resection of all D2 LNs, together with the removal of well-defined abdominal paraaortic and hepatoduodenal nodes. In patients with T1N0 disease, D1 or D1+ are recommended, whereas D2 is the approach of choice for individuals with T2 to T4 disease, and D3 LNM is not a recommended approach.179 Prophylactic LND has been validated as a treatment option in gastric cancer patients, and those early gastric cancer patients that undergo gastrectomy and prophylactic LND can exhibit 5-year survival rates upwards of 98%.172 D2 LND is a standard surgical approach in individuals diagnosed with resectable advanced gastric cancer.177

A schematic overview of lymphadenectomy for standard gastric cancer surgery.425 a The extent of lymphadenectomy after total gastrectomy. b The extent of lymphadenectomy after distal gastrectomy. c The extent of lymphadenectomy after pylorus-preserving gastrectomy. d The extent of lymphadenectomy after proximal gastrectomy
Patients with extensive lymph node metastases (ELM) from gastric cancer generally have a poor prognosis; however, preoperative neoadjuvant chemotherapy may improve surgical outcomes. The phase II JCOG 0001 study focused on gastric cancer patients with ELM employed a neoadjuvant chemotherapy regimen composed of irinotecan and cisplatin followed by gastrectomy and expanded LND (including PAND).180 The study was terminated because three treatment-related deaths were reported. Subsequent analyses of the trial data revealed a median survival time of 14.6 months and a 27% 3-year survival rate, which was higher than expected, although the 15% pathological remission rate fell below expectations. In the phase II JCOG 0405 study of surgery following neoadjuvant chemotherapy,181 following a neoadjuvant S-1 + cisplatin regimen and laparoscopy to exclude peritoneal metastases, gastrectomy with expanded LND was associated with respective 3- and 5-year survival rates of 59 and 53%, well above expected levels. Based on JCOG 0405, the JCOG1002 trial added docetaxel to the S-1 plus cisplatin with the goal of attaining better response and survival rates,182 although this regimen was ultimately associated with a response rate below that from the JCOG 0405 study, albeit with a 62% 3-year survival rate. In light of these results, D2-plus PAN dissection following treatment with a regimen consisting of S-1 plus cisplatin offers promise as a tentative treatment standard for individuals diagnosed with potentially curable gastric cancer with ELM. Future research efforts focused on exploring less toxic and more efficacious treatment regimens are warranted, as is an examination of whether these patients need to undergo expanded LND, particularly after exhibiting favorable clinical responses to neoadjuvant chemotherapy.
Lymph nodes of the pelvis
The pelvic LNs primarily include the obturator, sacral, common iliac, external iliac, and internal iliac nodes, all of which have the potential for involvement in patients with pelvic urogenital or gastrointestinal tumors. In rectal cancer patients, for example, LN staging is important in the context of disease evaluation and treatment selection, given that a high LN ratio (PNR) is associated with worse disease-free and overall survival outcomes.183 Rectal lymphatic drainage follows the rectal vasculature and is separated to include the superior, lateral, and inferior drainage tracts. Of these, the superior pathway is responsible for the drainage of the upper and middle rectum into the inferior mesenteric LNs, while the lateral pathway terminates at the subaortic LNs, and the inferior pathway drains the anal canal into the superficial inguinal LNs, in addition to draining the lower rectum in some cases.184 Proper staging generally requires the evaluation of at least 12 nodes.185 In the AJCC 8th edition TNM staging for LNM in rectal cancer, N1 indicates 1–3 positive regional LNs with intranodal tumors ≥0.2 mm in size or the presence of any number of tumor deposits with all identifiable LNs being negative, whereas N2 indicates the presence of 4+ positive regional LNs.186 Total rectal mesenteric excision (TME) or tumor-specific rectal mesenteric resection with lateral pelvic LND are the standard surgical approaches to treating advanced low-grade rectal cancer. While preoperative radiotherapy can reduce the local recurrence risk for these patients, it is not associated with any significant survival benefit.187,188 Retrospective analyses have suggested that for low-grade rectal cancer patients, preoperative radiotherapy can achieve efficacy comparable to that of lateral LND.189 In line with the above, a Swedish trial performed in the 1980s found that local recurrence rates were lower for patients that underwent preoperative radiotherapy before surgery as compared to patients that underwent surgery alone.190 Similarly, a Dutch trial noted significant reductions in local recurrence in response to preoperative radiotherapy, and found that the combination of this approach with TME yielded even better outcomes.187 At present, long-term irradiation is a commonly employed therapeutic strategy that can reduce tumor burden more readily than short-term irradiation, and the combination of this approach and fluorouracil-based chemotherapy is expected to emerge as a new standard of care that can improve anal preservation rates in the near future.
In addition to TNM staging, a specific staging system for gynecologic malignancies has been established by the Federation of International of Gynecologists and Obstetricians (FIGO). This FIGO staging system strongly emphasizes the significance of LN evaluation. In cervical cancer patients, for example, the prior FIGO staging systems failed to assess LNM, resulting in the understaging of 20–40% of patients with stage IB-IIB diseases and the overstaging of 64% of stage IIIB cancers.191 Adequately evaluation of the abdominopelvic retroperitoneal LNs was incorporated into the 2018 revision of these FIGO staging criteria (Table 2), underscoring the importance of pretreatment CT, MRI, and PET-CT imaging evaluations, together with the pathological assessment of LNs.192
Lymph nodes of the lower extremity
Lower limb LNs are primarily distributed in the popliteal area and inguinal canal. The superficial inguinal LNs are classified into a central group and four quadrants separated by the great saphenous vein and a horizontal line at the saphenofemoral junction. Deep inguinal nodes are situated proximal to the femoral artery and vein. These inguinal LNs are a common site of metastatic progression for tumors of the external genitalia, including vulvar and penile cancers. The superior medial LNs are the most common site of lymphatic drainage for the genital area, with the superior lateral, central, and inferior medial LNs also frequently draining this area, although the same is rarely true for the inferior lateral LNs.193 Penile and vulvar cancer patients exhibiting inguinal LNM are diagnosed with stage III or higher disease. In penile cancer, specifically, the 5-year survival of patients with inguinal LNM but no pelvic LNM can be as high as 80%, whereas, for patients with both pelvic LNM and distant metastases, this rate falls to 0–33%. The early surgical management of non-bulky (<4 cm) LNM has been linked to significant improvements in patient survival.194 In penile cancer patients with high-risk disease (≥pT1G2) and clinically negative inguinal LNs, modified inguinal LND and dynamic SLNB are recommended.195 The comprehensive evaluation of patients with palpable inguinal LNs at diagnosis via MRI, PET-CT, and fine-needle aspiration is also warranted, given that metastatic disease will not arise in upwards of 70% of these patients.196 In patients exhibiting bulky or fixed inguinal LNs, it is recommended that neoadjuvant chemotherapy and subsequent consolidative surgery be provided, given that primary surgery is unlikely to be curative.194 Moreover, inguinal LN involvement can also occur in anal canal carcinoma and lower rectal carcinoma patients, with LNM affecting 5.9–15.1% and 2.0–4.5% of patients, respectively.197
The popliteal LNs are divided into superficial and deep popliteal LNs by the deep fascia.193 While these popliteal LNs are generally regarded as minor players in the context of lower limb LNM, they should be taken into consideration during tumor staging. Popliteal LN involvement can be observed for lower limb tumors of the distal extremities. In some patients with primary melanoma tumors situated below the knee, popliteal LN drainage may occur such that assessing the popliteal nodes can predict recurrence and overall survival, although popliteal LND does not confer any survival benefits to these patients.152,198 An estimated 67% of N1 patients diagnosed with rhabdomyosarcoma of lower extremities exhibit popliteal LN positivity, underscoring the importance of performing popliteal LN biopsy procedures for tumors of the lower extremities, particularly for tumors of the distal extremities.153
Summary
Tumor LNM is a highly clinically significant event with direct implications for tumor staging, treatment selection, and patient prognosis. Ongoing research efforts with contribute to the more accurate and consistent classification of LNM, helping to clarify the most appropriate interventions and their associated patient outcomes. In general, patients affected by LNM tend to exhibit worse outcomes than node-negative patients. Surgery is generally used to remove local nodes harboring metastatic lesions, but the precise association between the extent of LN clearance and patient therapeutic responses warrants further evaluation. When the extent of LND is overly extensive, this may contribute to harmful complications and a reduction in overall survival. Conversely, if LND is incomplete, local recurrence may result from the remaining tumor cells, potentially contributing to even higher rates of mortality than those associated with excessive dissection. Integrated approaches that employ combinations of chemotherapy, radiotherapy, and immunotherapy are increasingly emerging as strategies for the management of primary tumor-derived LNM. Pre- or post-surgical chemotherapeutic, radiotherapeutic, and immunotherapeutic inventions can lower the risk of local LN recurrence, thereby prolonging patient survival and improving associated prognostic outcomes. Rapid biomedical advances are expected to provide an increasingly detailed understanding of the most appropriate LNM treatment strategies in the coming years.
Diagnosis and therapeutic interventions of metastatic lymph nodes
Methods of recognition and diagnosis
Preoperatively detecting metastases is a persistent challenge, with a wide array of imaging modalities having been tested for their utility in the context of LNM tracing, including magnetic resonance imaging (MRI), ultrasonography, computed tomography (CT), single photon emission computed tomography (SPECT)-CT, and positron emission tomography (PET)-CT.199,200,201,202,203,204,205,206 While PET-CT remains the gold standard imaging approach for most tumor types, all of these modalities exhibit unsatisfactory sensitivity and specificity, with CT and other traditional approaches primarily relying on metastatic LN detection based on the identification of specific morphological characteristics.207,208,209 At present, preoperative approaches that can reliably assess the extent of LND remain lacking.
A wide array of targeted antibody-, peptide-, nanoparticle-, and small molecule-based imaging probes have been employed in the context of LNM evaluation (Table 3). Nanoparticles, in particular, have been the focus of marked research progress in recent years.210,211 Nanoparticles could be promising agents for the detection of metastatic LNs as they can be readily modified and offer unique properties conducive to tumor-specific targeting and imaging enhancement.212 For instance, ultrasmall superparamagnetic iron oxide (USPIO) nanoparticles have commonly been tested in MRI-based studies of LNM detection213,214,215 (Fig. 8a). Metastatic LNs tend to exhibit fewer macrophages, and those macrophages that are present generally exhibit impaired phagocytic activity such that USPIO nanoparticles uptake is impaired and metastatic nodes appear brighter on T2-weighted images.216 Nanoparticles can also facilitate imaging using more recently developed imaging techniques, including near-infrared (NIR) fluorescence imaging (Fig. 8b), Raman mapping, photoacoustic (PA) imaging, and multimodal imaging.217,218,219,220,221,222

a Application of USPIO nanoparticles in the detection of metastases in normal-sized pelvic LNs of patients with bladder and prostate cancer. USPIO nanoparticles taken up by macrophages lead to a signal decrease on T2- or T2*- weighted MRI, which is lacking in the malignant LN (arrow) due to few macrophages and little USPIO nanoparticle uptake compared to the benign LN (arrowhead).213 Copyright 2013, European Association of Urology. b Application of a NIR probe in the detection of LNM in mice. The pictures present NIR imaging-guided SLN surgery in an orthotopic 4T1 breast cancer model.217 Copyright 2020, Wiley-VCH. USPIO, ultrasmall superparamagnetic iron oxide; LN lymph node, MRI magnetic resonance imaging, NIR near-infrared, LNM lymph node metastasis, SLN sentinel lymph node
Several tumor-specific antigen-based targeting strategies have been developed for LNM detection to date. For example, the surface modification of certain probes with HER2-specific antibodies can endow them with a high degree of tumor-binding specificity.223,224 Prostate-specific membrane antigen (PSMA)-based PET-CT has been shown to offer the greatest degree of diagnostic utility for LNM imaging in patients with prostate cancer, given the expression of markedly high PSMA levels by a majority of prostate cancer cells.225 The RGD (Arg-Gly-Asp) peptide, which specifically engages in high-affinity interactions with the αvβ3 integrin receptor commonly overexpressed by cancer cells, can also enable efficient tumor cell targeting.226 RGD-decorated NPs have shown promise as tools for LNM detection.220,227,228,229 Folate receptor (FR)-α, which is heavily upregulated in many cancers derived from epithelial cells, has also been advanced as an attractive target for cancer-specific targeting that has been applied to the modification of NPs in tumor and LNM detection-focused research efforts.218,230,231,232 The efficacy of folic acid (FA)-modified nanomedicines, however, appears to be limited by FA-associated increases in IgM absorption to the surface of the prepared liposomes such that they are rapidly removed from systemic circulation and internalized by macrophages within the liver, spleen, and tumor.233 Macrophage-containing LNs also exhibit detectable FR-β expression, potentially resulting in a false-positive nodal signal when utilizing FR-targeting NPs in a clinical setting.230,234 Other targets with less cross-reactivity or the combination of multiple imaging agents and targets of interest may thus represent promising approaches to enabling more reliable imaging-based evaluation of LNM in the future.232
Metastatic LNs also harbor a unique tumor-associated microenvironment with changes in pH levels, proteinase activity, redox potential, and reactive nitrogen and oxygen species production that can be leveraged for tumor-targeted delivery efforts.235 Bennet et al.,236 for example, generated indocyanine green-conjugated ultra-pH sensitive (UPS) NPs capable of amplifying NIR signals in response to pH changes within the local tumor microenvironment (TME). These UPS NPs can successfully discriminate between metastatic and benign LNs. Liu et al.222 successfully achieved the specific delivery of drugs to metastatic LNs via the targeting of the hypoxic TME. Matrix metalloproteinases 2/9 (MMP-2/9) are proteases that are commonly active within the TME, wherein they facilitate angiogenesis and metastatic progression.237 MMP-2/9-responsive nanoprobes have similarly shown great promise when employed in studies of LNM.229,238
Surgical treatment: balance of the extent of lymph node dissection
LND has been firmly established as a core component of the surgical treatment of many cancer types.239 LND can not only eliminate tumor lesions in TDLNs to prevent recurrence, but also provide accurate tumor staging information for further treatments.240,241,242,243 For these reasons, LND is generally believed to improve prognostic outcomes and patient survival.244 Nevertheless, with research development and technical advancement in diagnosis and surgery, the guidelines for LN management have been constantly discussed and modified. Researchers have claimed to restrict the extent of LND and prevent unnecessary LND because removal of unnecessary LNs did not refine the prognosis; instead, it increased the incidence of complications that are detrimental to patients’ quality of life.245 In particular, the impact of micrometastasis in LNs on survival and the benefits of LND for prognosis improvement when micrometastasis is found by biopsy remain controversial.246,247 In addition, LND may cause damage to regional immune function, leading to impaired antitumor immune responses and reduced efficacy of immunotherapy.239,248 These LND-related advantages and disadvantages are presented in Fig. 9. In this section, we discuss arguments regarding LND strategies in various tumors and the role of LNs in antitumor immunity.

Overview diagram of the advantages and disadvantages of LND. LND lymph node dissection
Antitumor immunity and LND
Given that LNs serve as secondary lymphoid organs important for the coordination of immune responses, many experts are concerned that surgical overdissection of LNs may have negative effects on antitumor immune responses. Many researchers have proposed that SLN or TDLNs are immune-suppressed and the immunosuppressive state may be present even without tumor cells, which could be enhanced by tumor invasion; further, a growing number of studies have proved their potential in antitumor immunity in support of the view that LNs must be treated cautiously.110,249,250 Tumor-free SLNs reportedly exhibit higher DC and T cell concentrations than tumor-bearing SLNs, suggesting that these nodes can serve as hubs for the induction of tumor-specific immune responses in the absence of direct tumor invasion.251,252 In a mouse model designed to simulate LND, surgical damage to the lymphatic system resulted in the progression of the established tumor as a consequence of impaired adaptive immunity.248 Molodtsov et al.253 found that tumor-specific resident memory T (Trm) cells that persist in regional LNs are key players in the prevention of metastatic disease progression. Moreover, Inamori et al.254 detected significant T cell repertoire overlap and no improvement in long-term prognostic outcomes following excessive LND. These results support the important role that regional LNs play in the induction of antitumor immune responses. Conventional type 1 DCs (cDC1s) can also migrate to TDLNs and prime the activation of antitumor lymphocytes present therein255 (Fig. 10a). Given the ability of these cDC1s to support the maintenance of a reservoir of TCF-1+ CD8+ T cells with antitumor activity, complete TDLN removal has the potential to interfere with CD8 + T cell priming and subsequent effort responses.107,256

a cDC1s take up and transport tumor antigens to TDLNs for presentation to naïve CD8+ T cells, priming cytotoxic effector CD8+ T cells.255 Copyright 2018, Francis Crick Institute. b TDLNs are enriched for tumor-specific PD-1+ T cells and blocking PD-L1 in TDLNs generates progenitor-exhausted T cells that seed the tumor, which enhances antitumor immunity.257 Copyright 2020, Elsevier Inc. cDC1 conventional type 1 dendritic cells, TDLN tumor-draining lymph node
Rapid advances in immunotherapeutic techniques in recent years have led to the reconsideration of the importance of regional LNs. Immune checkpoint blockade (ICB) treatment can provide benefits both locally within the tumor microenvironment as well as systemically, indicating that peripheral T cell activation and expansion may be critical for robust ICB responses. This further highlights the potential importance of TDLNs as a site where antitumor immune responses may arise in the context of ICB treatment.239 Indeed, in mice, LNs have been shown to be enriched for PD-1+ tumor-specific progenitor T cells that can play a central role in antitumor immune responses following PD-1 blockade257 (Fig. 10b). Fransen et al.258 additionally observed higher levels of PD-1 blockade-induced immune activity in the TDLNs as compared to non-TDLNs, with TDLN resection eliminating treatment-related tumor regression as a consequence of impaired immune cell infiltration of the tumor microenvironment. Recently, Rahim et al.259 confirmed the central role that LNs play in shaping cancer patient response to immunotherapeutic treatment by studying CD8+ T cells from the primary tumors, blood, and regional LNs of head and neck squamous cell carcinoma patients. These analyses revealed that uninvolved LNs contained abundant levels of progenitor-exhausted CD8+ T cells (Tpex), which are vital for endogenous and ICB-mediated CD8+ T cell responses, and these cells were clonally related to terminally exhausted cells identified within tumors. Following PD-L1 blockade treatment, Tpex and intermediate-exhausted CD8+ T cells (Tex-int), both of which are relevant ICB targets, were found to be localized proximal to DCs in uiLNs, with responses coinciding with an increase in circulating Tex-int. While anti-PD-L1 therapy-associated Tpex and Tex-int responses in metastatic LNs were abnormal, even metastatic LN patients exhibited limited increases in circulating post-treatment CD8+ T cell responses. While these above studies suggest the importance of limiting the extent of LND, additional clinical trial-derived evidence will be essential to support the evidence-based revision of guidelines for LN management.
Controversy regarding LND in various tumors
As a crucial part of surgery in oncology, the strategies of LND have been developing with the improvement of tumor evaluation and the progression of surgical techniques during the past few decades.260,261 However, the guidelines for LND are still controversial and need further refinement. Although LND plays an important role in lesion elimination and recurrence control, improper LND can do harm to the survival of patients due to impaired antitumor immunity, which has been discussed above, as well as postoperative complications caused by excessive surgical procedures.262,263 In clinical practice, many factors may have an influence on decisions of LND, including preoperative tumor staging and the ability of patients to tolerate the operation.240,264,265 Disagreements also exist among regions regarding optimal LN management owing to differences in tumor incidence, medical conditions, routine medical approaches, and histories of oncology-related surgical practices.266,267,268 In this part, we illustrate the advantages and disadvantages of LND with examples of arguments in various types of tumors.
Thyroid cancer: is LND necessary for prophylactic central compartment LN dissection (pCND)?
Thyroid cancer rates have steadily risen over the past 30 years,269 with papillary thyroid carcinoma (PTC) accounting for approximately 90% of new thyroid cancer diagnoses.270,271 As this tumor type is prone to lymphotropic metastasis, PTC patients commonly present with LNM.272 An estimated 35% of PTC patients present with cN1 disease, and of those with cN0 disease, microscopically positive nodes are estimated to be present in as many as 80% of cases.273 The central compartment is the most common site of PTC-associated LNM, and central compartment LND is thus recommended in cN1 PTC patients.246 Nevertheless, the benefit of pCND for patients with cN0 disease remains controversial.
Researchers that support pCND for cN0 patients assert that it can lower rates of locoregional recurrence as it offers accurate staging-related information, in addition to guiding radioactive 131I ablation therapy.274,275 It can also reduce the odds of reoperation-related morbidity, which can entail damage to the parathyroid glands, recurrent laryngeal nerves (RLNs), parathyroid glands, and major great vessels.276
Despite these assertions, data from several clinical trials have also provided support for researchers that oppose the pCND treatment of cN0 patients. Relative to patients that undergo total thyroidectomy alone, those that undergo pCND face higher rates of complications.277 Of these complications, the most common and relevant in patients undergoing central neck dissection procedures is hypocalcemia arising as a consequence of parathyroid gland dysfunction,273,278 which can occur following mechanical or thermal injury, parathyroid blood supply disruption, or the unintended or intended removal of this gland.279 As they are small and exhibit coloration similar to that of LNs, fat, and thyroid tissue, surgeons can also face difficulty accurately identifying the parathyroid glands.280 The risk of RLN or superior laryngeal nerve injury should also be taken into account, particularly for surgeons that do not routinely perform these procedures.281
Some clinical trials have found that there is no clear evidence in support of pCND-associated reductions in recurrence or improvements in survival.277,282,283,284,285 In a retrospective trial focused on 695 PTC patients, Dismukes et al.282 observed no differences in recurrence, distant metastasis, or persistent disease outcomes over a 38-month follow-up period when comparing cN0 patients that underwent thyroidectomy and pCND to those who underwent thyroidectomy alone.
Subclinical central LNM is also of relatively minor prognostic significance. While pCND in cN0 patients can enable more accurate TNM staging, such staging does not take differences between micro- and macrometastases in LNs into consideration.277 Ahn et al.286 conducted a prospective randomized controlled trial in which they found that LNM was confirmed to be evident in 27.5% of patients that underwent pCND, with this rate being significantly higher than that for patients in the non-pCND group. Despite this difference, no structural recurrence occurred over a 46.6 ± 9.1 month follow-up period among those 14 patients with LNMs in the pCND group, 8 of whom exhibited micro-LNMs (0.02–0.2 cm) and 6 of whom exhibited small LNMs (0.2–1.0 cm). These metastatic nodes are thus regarded as low-risk (<5% risk of recurrence) in pN1 patients, suggesting that pCND is not clinically important with respect to its value as a tool for LN risk stratification. The AJCC TNM staging system has been updated accordingly, including N0 classifications for cytologically or histologically confirmed (N0a) disease or disease without supporting radiologic or clinical evidence (N0b).287
Lung cancer: the debate regarding lobe-specific systematic lymph node dissection (L-SLND)
Lung cancer is the leading cause of cancer-related mortality, with approximately 1.8 million deaths globally each year. Of these lung cancer cases, 85% are of the NSCLC subtype.288,289 In early-stage NSCLC patients, surgery is the standard of care approach for staging, and the NCCN guidelines recommend systematic LND (SLND), which includes the complete dissection of the hilar and mediastinal LNs, as a routine component of lung resection procedures. The most appropriate extent of mediastinal LND (MLND), however, remains a topic of controversy. L-SLND has recently emerged as an alternative to SLND, allowing clinicians to use information on the location of the primary tumor to tailor the extent of MLND based on the corresponding lymphatic pathway.290
Several clinical trials have affirmed the benefits of L-SLND to the perioperative recovery, recurrence risk, and survival outcomes of patients, particularly among individuals with early-stage NSCLC.264,291,292,293,294 Deng et al.264 explored lobe-specific LNM patterns in clinical stage IA peripheral NSCLC (cT1N0M0) patients with tumors ≤3 cm and presented their recommendations for L-SLND. In this study, rates of upper lobe tumor metastasis to the subcarinal (0.3%) and lower LN zones (0.3%) were very low, and no such lower mediastinal LN metastases were evident for right middle lobe tumors. No lower lobe tumors ≤2 cm metastasized to the upper LN zone. Based on these results, the authors recommended L-SLND for upper lobe tumors only in cases where upper LN zone dissection is required, while for right middle lobe tumors, upper and subcarinal LN zone dissection is necessary for L-SLND. In patients with lower lobe tumors ≤2 cm, L-SLND was only recommended in cases where subcarinal and lower LN zone dissection was required. In other cases, systematic LN sampling or SLND should be performed instead of L-SLND.
Moreover, Chen et al.295 developed six preoperative imaging- and intraoperative frozen pathology-based criteria for the prediction of negative nodal station status for use when planning selective LND for peripheral clinical T1N0 invasive NSCLC patients. First, MLND was deemed unwarranted in cases with a tumor consolidation ratio ≤0.5. Second, MLND was also considered unnecessary for patients an intraoperative diagnosis of lepidic-predominant adenocarcinoma. Third, inferior MLND was not considered necessary for patients with apical segment tumors. Fourth, inferior MLND was not indicated for patients with negative hilar nodes and an absence of visceral pleural invasion. Fifth, left superior segment tumor patients did not require 4 L LND if their hilar nodes were negative. Lastly, superior MLND was not required for any patients with left basal segment tumors exhibiting hilar node negativity. The authors tested these criteria in a prospective multicenter trial enrolling 720 patients, with systematic MLND being conducted in all cases to confirm the accuracy of this approach to predicting LN involvement. Strikingly, negative node status in particular mediastinal zones was accurately predicted using this approach in all cases, providing strong support for the clinical implementation of selective LND for early-stage NSCLC patients.
Despite the above evidence, some researchers posit that following metastasis, all LN zones are at risk and should be dissected irrespective of the fact that the odds of mediastinal LNM differ as a function of primary tumor location.290 Handa et al.240 reviewed 375 patients that had undergone lobectomy with lymphadenectomy for clinical T2–3 N0–1 M0 hypermetabolic NSCLC, and determined that SLND procedures harvested more metastatic nodes than L-SLND, potentially contributing to better oncological outcomes. Notably, an estimated 6% of patients in the L-SLND group may have harbored metastatic LNs not present in lobe-specific stations that would have been missed by this procedure, potentially denying ~6% of patients in clinical practice from accessing adjuvant systemic treatment. The number of examined LNs may also be related to improved survival rates as a result of a reduction in the risk of misstaging, supporting the need for SLND.296,297 In a clinical trial focused on early-stage NSCLC, SLND was found to be associated with better disease-free survival than L-SLND.298 Further large-scale systematic clinical trials are thus warranted to clarify the advantages and limitations associated with SLND and L-SLND. The ongoing large-scale prospective randomized controlled trials currently underway in China (ChiCTR2100048415) and Japan (JCOG 1413) have the potential to further guide such LND-related decision-making for NSCLC patients.299,300
Melanoma and breast cancer: decision making after positive sentinel lymph node biopsy (SLNB)
The consensus criteria for LN management have undergone many changes in recent decades owing to the advent of SLNB procedures that use dyes or radiotracers to facilitate the identification, excision, and evaluation of SLN metastases.301 SLNB can enable clinicians to accurately stage metastatic spread with minimal risk of complications.302,303,304 Owing to the superficial nature of these tumors, melanoma, and breast cancer patients are particularly likely to benefit from SLNB given the great amenability of these neoplasms to preoperative tracer injection.301
It remains a matter of controversy as to whether complete LND (CLND) should be performed in melanoma patients with positive SLNB results. This is in part because melanoma is an extremely aggressive subtype of skin cancer with a high propensity for LNM.305,306 Most centers routinely perform CLND in melanoma patients with at least one positive LN, despite the fact that ~80% of patients that undergo CLND do not exhibit any additional non-sentinel node (NSN) metastases.307 The landmark DeCOG-SLT and MSLT-II trials provided particularly important evidence for this clinical context. The DeCOG-SLT trial247 screened 5547 patients, of whom 1269 (23%) were included based on the identification of a positive SLN. Of these patients, 483 were randomly assigned to undergo CND or nodal observation with nodal basin ultrasonography every 3 months. No differences in recurrence rates or 3-year overall, relapse-free, or disease-free survival were observed between these groups. Given that 66% of the included patients exhibited a low SLN tumor burden (diameter ≤1 mm), the trial researchers concluded that CLND is not appropriate for melanoma patients with SLN metastases ≤1 mm. Researchers of the MSLT-II trial308 evaluated 1934 and 1755 patients in intention-to-treat and per-protocol analyses, respectively, and further concluded that immediate CLND did not improve melanoma-specific survival. While CLND can contribute to greater regional nodal control and provide additional prognostic insight, it does so at the cost of potential lymphedema and other forms of morbidity.
The purported actual benefits of CLND after positive SLNB vary among studies. In an analysis of 471 SLNB-positive patients, 5-year microsatellite stability (MSS) and nodal recurrence rates were improved by CLND.309 Another study was conducted in the Bay of Plenty District Health Board (BOPDHB) of New Zealand.267 A larger mean SLN metastatic deposit size was observed in 157 SLNBs as compared to the MSLT-II trial (3.53 vs 1.07/1.11 mm), highlighting a pronounced difference between these two studies. Metastatic deposits >1 mm were also more common in the BOPDHB study (54.8 vs. 33.2/34.5%), and the rate of NSN involvement on CLND was higher (23.8% vs. 11.5%). This suggests that failing to complete CLND may expose patients to a higher degree of risk.
The above results suggest that positive SLN tumor burden in melanoma patients may have an important bearing on decision-making pertaining to CLND. A few trials to date have sought to evaluate the utility of CLND for melanoma patients in whom micrometastases were detected on SLNB.310,311 Susok et al.311 studied 258 patients with micrometastases in SLNB and performed a 20-year survival analysis, and observed no significant increase in the risk of relapse or impaired MSS when comparing patients that did undergo CLND (HR: 1.3, 95% CI: 0.8–2.3) and did not undergo CLND (HR: 1.2, 95% CI: 0.8–1.9).
CLND offers independent prognostic insights not available from other sources.312 In the MSLT-2 and De-COG trials, serial ultrasonographic nodal exams were performed for participating patients, yet such scans remain far from routine in many areas.267,313 As such, practical limitations pertaining to medical resource availability confer continued prognostic and therapeutic value to CLND in many cases. Overall, additional research is warranted to more fully explore the necessity of CLND in SLNB-positive melanoma patients and the relationship between positive SLN tumor burden and CLND-related approaches and outcomes.
Regarding breast cancer, strong evidence has been provided for forgoing axillary lymph node dissection (ALND) when SLNB is positive with micrometastases.314,315 The DFS rates of breast cancer patients with 1 or more micrometastatic SLNs ≤2 mm in the IBCSG 23-01 trial on 10-year follow-up were 74.9% (95% CI: 70.5–79.3) and 76.8% (95% CI: 72.5–81.0) for patients that did and did not undergo ALND, respectively (HR: 0.85, 95% CI: 0.65–1.11; log-rank p = 0.24 and p = 0.0024, respectively, for non-inferiority).315 These results indicated that the omission of ALND was not inferior to ALND. As a result, ALND is not currently recommended by the NCCN in patients with micrometastasis-positive SLNs.
Gastric cancer and bladder cancer: the extent of LND for advanced cancer
In 2020 alone, approximately 1,000,000 patients were diagnosed with gastric cancer, while 769,000 succumbed to this disease, ranking it as the fourth deadliest cancer type globally in large part owing to the fact that the disease is often relatively advanced when first diagnosed.288 In patients with advanced gastric cancer, gastrectomy remains the primary treatment approach, and the optimal extent of LND in these patients is a topic of ongoing debate.177 Divergent opinions on this topic have emerged in Eastern and Western nations, with D1 and D2 LND procedures being the two strategies most commonly discussed in this context. D1 LND entails the dissection of all perigastric and left gastric artery LNs, as they exhibit the highest degree of metastatic risk. In contrast, D2 dissection entails the removal of all D1 LNs, nodes along the celiac axis, and nodes along the common hepatic, proper hepatic, and splenic artery other than the splenic hilar nodes.316
In Eastern nations, D2 LND has been the standard approach for patients undergoing gastrectomy for several decades, reportedly offering significant advantages over D1 LND with respect to long-term survival benefits.317 Under the established Japanese guidelines for the treatment of gastric cancer, D2 LND is indicated, whereas potential nodal involvement cannot be excluded.316 In contrast, guidelines in Western nations recommend D2 LND but do not mandate this procedure.176 This is partially attributable to the results of the phase III Medical Research Council randomized surgical trial and the Dutch Gastric Cancer Trial. In both of these trials, D2 LND was not associated with any initial survival benefits, potentially owing to very high postoperative mortality rates following D2 dissection.318,319 The differences in the conclusions of clinical trials conducted in Eastern and Western nations may be attributable to the greater proportion of younger patients with less abdominal fat and fewer comorbidities in the East, as these factors may simplify the D2 procedure.320 Additional analyses of subgroups and long-term follow-up data revealed that pancreatectomy and splenectomy were major risk factors associated with elevated D2-related morbidity rates. Among non-pancreatectomy/splenectomy patients, the OS of individuals that underwent D2 LND was significantly longer than that of those that underwent D1 LND.319 The 15-year follow-up results from the Italian Gastric Cancer Study Group randomized controlled trial observed no differences in procedural outcomes between D1 and D2 dissection in the overall population, yet D2 LND was associated with significant improvements in gastric cancer-related and disease-specific survival when focusing specifically on individuals with advanced resectable disease (pT >1 N+) and LNMs.321 These results suggested that pancreatectomy and splenectomy had adverse effects on D2 patient outcomes. Long-term clinical trial follow-up led to the suggestion by surgeons in Japan that spleen- and pancreas-preserving modified D2 LND approaches be implemented, leading to the rapid global adoption of this approach throughout the Western world.266 Meta-analyses have demonstrated that pancreas- and spleen-preserving therapies can contribute to improved survival outcomes and lower rates of gastric cancer-associated death among patients that had undergone D2 LND.322,323 Given that specialized centers are equipped to perform pancreas- and spleen-preserving D2 resection procedures, there is international consensus regarding the inclusion of D2 LND in gastrectomy procedures for medically fit advanced gastric cancer patients, with all such procedures being conducted in specialized, high-volume centers.177
Ongoing clinical efforts have sought to refine D1 and D2 LND protocols for patients undergoing gastrectomy. Kang et al.,324 for example, observed comparable long-term survival outcomes when comparing patients with ≥ pT2 or pN + gastric cancer that underwent D2 LND or D1 + LND, the latter of which omits the resection of LNs at the proximal splenic (No. 11p) and proper hepatic artery (No. 12a), highlighting the potential adequacy of D1 + LND as a treatment for advanced gastric cancer. Besides, Yu et al.325 also confirmed that D2 + LND was safe and effective in patients with advanced distal gastric cancer through the additional dissection of the hepatoduodenal ligament LNs along the common bile duct (No. 12b), posterior LNs along the common hepatic artery (No. 8p), LNs behind the head of the pancreas (No. 13), and LNs along the superior mesenteric vein (No. 14 v). When focusing on patients exhibiting duodenal involvement, significant improvements in 3-year DFS were observed for patients that underwent D2 + LND as compared to D2 LND. Further large-scale clinical trials are thus warranted to provide surgeons with sufficient evidence to select the most appropriate LND extent when addressing gastric cases affecting different sites or exhibiting differing degrees of invasion.
The optimal extent of LND for advanced bladder cancer patients also remains an area of active controversy. In patients with muscle-invasive bladder cancer, radical cystectomy with pelvic lymph node dissection (PLND) is the standard-of-care treatment. In these cases, LND procedures fall into three major categories: (i) standard PLND, which entails the removal of the internal iliac, presacral, obturator fossa, and external iliac LNs up to the bifurcation of the common iliac arteries; (ii) extended PLND, which entails to the removal of LNs between the aortic bifurcation and common iliac vessels proximally, the genitofemoral nerve laterally, the circumflex iliac vein distally, and the internal iliac vessels posteriorly; and (iii) super-extended PLND, which includes continued proximal dissection to the root of the inferior mesenteric artery.326 A meta-analysis of six comparative studies that incorporated 2824 bladder cancer patients undergoing radical cystectomy found extended PLND to improve the recurrence-free survival of patients relative to standard PLND, although no additional survival benefits were conferred by super-extended PLND. In contrast, a recently conducted randomized multicenter phase III trial found that extended LND did not offer significant advantages over standard LND with respect to patient overall, cancer-specific, or recurrence-free survival.245 The negative result may be related to the fact that 14% of the cohort was comprised of T1G3 patients, given that they tend to exhibit low rates of nodal positivity. However, the mean LN yield for extended LND was almost 30% higher, increasing the odds of positive LN detection. One retrospective study focused on bladder cancer patients undergoing radical cystectomy and lymphadenectomy found super-extended PLND to be associated with elevated LN yields and increased N2/N3 rates relative to standard PLND and extended PLND, but without any corresponding increases in complication rates.327 The identification of additional positive LNs was conducive to more precise nodal staging such that more patients could be appropriately evaluated for adjuvant systemic treatment, translating the diagnostic benefits of extended or super-extended PLND into improved therapeutic options that support the application of this approach.328,329
Prevention and treatment of complications in LND
As noted above, LND procedures can result in complications that adversely impact patient quality of life, including lymphedema (interstitial edema caused by lymphatic insufficiency), lymphocele (lymphatic-filled cystic lesion), lymphatic or chylous fistula, hematoma, and neuroparalysis. The management of the complications is also an important part of surgical therapy for patients undergoing LND.
To prevent complications after LND, the operator should be familiar with the local anatomy of regions of dissection, and avoid damage to blood vessels, lymphatics, and nerves. Also, surgeons have made great efforts to improve the surgical procedures. For example, novel LND techniques have been proposed to avoid postoperative RLN paralysis, which is the most worrying complication for thoracic surgeons when performing LND. Chen et al.330 presented an advanced lymphadenectomy approach in which the two-dimensional pedicled nerve flap, which includes the left RLN, LNs along the left RLN, and tracheoesophageal vessels, was exfoliated on both sides via the dorsal suspension of the esophagus and the pushing of the trachea to the ventral side, after which isolating forceps were used to separate LNs from the left RLN. This strategy enabled surgeons to reliably identify the local anatomical structures such that they were able to avoid any RLN injury. Saeki et al.331 reported an alternative means of preventing RLN paralysis that consisted of using scissors to cut the vessels surrounding the RLN, rather than ultrasonic coagulating devices or similar equipment, followed by the hemostatic application of mini-clips before the vessels were cut. Otsuka et al.332 similarly developed what they termed a “native tissue preservation” technique aimed at lowering the odds of RLN paralysis by preserving the native tissue layer surrounding this nerve during LND and thereby avoiding the traction and bending of the left RLN.
Accurately visualizing regional lymphatic structures can also lower the risk of LND-related complications. In breast cancer, axillary reverse mapping (ARM) can benefit patients undergoing SLNB or ALND by injecting a blue dye, radioisotope, or fluorescent agent that allows for differentiation between the lymphatic channels of the breast and those of the upper arm. By allowing for the preservation of upper extremity lymphatic drainage, ARM can lower the incidence of arm lymphedema.333 ARM has also been confirmed to be safe in cN0 patients with positive SLNs.334,335
Many different medical materials have been explored as tools to help mitigate the procedural complications of LND. Fibrin glues are commonly used in surgical settings to promote tissue adherence and hemostasis, allowing for reductions in seroma magnitude, duration, and necessary evacuative punctures following SLNB or ALND.336,337 Applying fibrin glue in this setting, however, remains a matter of some controversy. Conversano et al.338 noted no reduction in postoperative seroma formation in breast cancer patients undergoing ALND following the application of a low-thrombin fibrin sealant glue. Even so, this glue was able to support ALND without wound drainage and to reduce the duration of postoperative hospitalization. Researchers have also tested the use of a gelatin-thrombin matrix in gynecologic cancer patients, revealing its ability to decrease pelvic lymphocele incidence.339
When they do arise, the complications resulting from LND must be treated in a timely fashion. For patients suffering from lymphedema, combined decongestive therapy (CDT) is the accepted standard of care supportive therapy, consisting of manual lymphatic drainage, gradient compression bandaging, therapeutic exercises, and skin care that allows for the conservative and surgical management of this condition as appropriate.340 Microsurgical lymphatic-venous anastomoses (LVA) also provide an opportunity to treat lymphedema cases that respond poorly to CDT via the reconstruction of the lymphatic vasculature.341 Lymphocele and lymphatic or chylous fistulae are primarily treated through percutaneous drainage and the injection of povidone-iodine, alcohol, or bleomycin as sclerosing agents.342 Surgical approaches for affected patients include marsupialization, which can be conducted in instances of clinically symptomatic lymphocele or cases that fail to respond to percutaneous drainage and sclerosis.343 Conservative means are usually sufficient to manage lymphatic or chylous fistulae, but surgery is required if leakage persists.344,345 Nonresolving neuroparalysis can benefit from surgical interventions aimed at promoting functional recovery, including arytenoid adduction with Type I thyroplasty in individuals suffering from RLN paralysis.346
Future perspectives of LND
In summary, even if LND has been established as a standard surgical treatment that can improve prognostic outcomes for patients, a range of issues related to this procedure warrant further research and discussion. These include:
-
1.
The need for further discussion regarding the indications for and extent of LND. Besides, as the resection extent of primary tumor has become more and more diverse in different tumor conditions for all types of tumors, the guidelines for the extent of LND seem to be not specific enough to adapt to these different conditions.
-
2.
The requirement for additional evidence regarding the relationship between excessive LND and immune function, with a further focus on the associated impact on immunotherapeutic efficacy.
-
3.
The need for improved surgical techniques. While there have been marked improvements in surgical approaches in recent years, LND remains a highly precise procedure that requires the excision of LNs located in close proximity to particular nerves, blood vessels, and lymphatic structures, often requiring a prolonged operative duration and causing substantial surgical trauma.
-
4.
The suboptimal sensitivity of current preoperative LNM detection techniques and the lack of a reliable approach to determining the extent of LND.
Researchers can seek to address the abovementioned issues through several approaches, including the following:
-
1.
Conducting additional systematic large-scale clinical trials focused on the extent of LND, which have the potential to improve guidelines pertaining to LND and to ensure that they are better tailored to the degree of tumor invasion.
-
2.
Performing further basic research and clinical trials exploring the impact of LND on antitumor immunity and immunotherapy efficacy, highlighting trade-offs between LN preservation and resection while guiding the design of combined surgical and immunotherapeutic interventional strategies.
-
3.
Developing more efficient and less traumatic LND surgical procedures. For particularly difficult procedures, the extent of LND can be tailored to minimize procedure-related damage to the health of the patient, particularly for low-volume centers.
-
4.
Further studying approaches to LNM diagnosis, as through the design of specific PET-CT probes and the clinical application of nanoparticles that can provide superior preoperative staging information such that an optimal LND strategy can be selected.
Medical treatment: exploration of therapeutic targets
While a combination of radiotherapy and chemotherapy has traditionally been employed to treat lymphatic metastases, recent advances in immunotherapies, targeted treatment regimens, and nanodelivery systems have increasingly provided patients with the opportunity for precision medicine-based treatment (Fig. 11). New antitumor drugs can suppress both tumor growth and metastatic progression in many cases.27,347

Exploration of medical treatment strategies for lymph node metastasis. Created with BioRender.com
Targeted therapy
As lymphangiogenesis and LNM are orchestrated by many molecules and pathways, there are many hypothetical targets for clinical efforts to prevent or abrogate LNM. These include the VEGF-C/D-VEGFR-3, CCL21-CCR7, CXCL12-CXCR4, and COX-2-PGE2 signaling pathways, as well as the lipid metabolism pathway.
VEGF-C/D-VEGFR-3
The lymphatic vessels form a channel through which tumor cells can spread, while also enabling the active recruitment of malignant cells to LNs and regulating immune activity. Growth factors released from tumors, including VEGF-C, can promote lymphangiogenesis and anterior LN drainage in the primary tumor, thus inducing LNM.348 Many different VEGF-C and VEGF-D/VEGFR-3 pathway-targeting drugs have been developed and demonstrated to offer efficacy as inhibitors of solid tumor LNM.37 Multikinase inhibitors such as Sunitinib, Sorafenib, and Pazopanib, have received approval for the treatment of various cancers including HCC, renal cell carcinoma, and gastrointestinal mesenchymal tumors.348,349
CCL21-CCR7 and CXCL12-CXCR4
The chemokine CCL21 is primarily secreted by LECs. The resultant protein includes a long C-terminal domain that can combine with glycosaminoglycans (GAGs) to affix to the cell surface or ECM,350 providing a signal that can be leveraged by lymphocytes for homing to secondary lymphoid organs and the subsequent regulation of metastatic tumor development.351 The G protein-coupled receptor CCR7 is the only receptor for CCL21, and it is expressed on the surface of immune cells, including B cells, T cells, and DCs. CCL21-induced CCD7 signaling regulates the lymphoid migration and LN homing of T cells, DCs, and other immune cell types.352
Efforts to target this CCL21-CCD7 signaling axis have included CCR7-neutralizing antibodies, CCR7 agonists, specific siRNA constructs, CCR7 traps, and CCL21 mutations aimed at suppressing the lymphatic migration and invasion of tumor cells. Using a retroviral vector to overexpress CCR7 in B16 cells that were subsequently injected into murine footpads, Wiley et al.353 observed enhanced CCR7-B16 cell migration to regional LNs at early and late time points (1 and 3 weeks) relative to vector control, while the use of a CCL21-neutralizing antibody was sufficient to interfere with CCR7-mediated metastatic progression. This suggests that the expression of CCD7 alone can enhance B16 cell metastasis to TDLNs such that tumor cells are capable of coopting standard LN homing strategies to facilitate lymphatic metastasis, with the upregulation of a specific chemokine receptor being sufficient to enable metastatic progression. One phase IIa study found that combining intravenous pembrolizumab with the CXCR4 antagonist motixafortide was associated with improved chemotherapeutic outcomes in metastatic pancreatic ductal adenocarcinoma patients.37,354
COX-2-PGE2
DCs form an integral part of the tumor microenvironment owing to their ability to prime and regulate T cells.355 DC-regulating compounds such as PGE2, which strongly influences DC maturation and function, can have a pronounced impact on the local niche.3,356 Using a lung parenchymal tumor model generated through the direct injection of GFPV-transfected LLC cells in the soft tissue of the left lung, Ogawa et al.92 determined that at 1 to 3 days post-tumor implantation, regional LNs harbored COX-2-positive cells in the subcapsular region. Moreover, they found that COX-2 inhibitor therapy was sufficient to disrupt regional LNM in these animals. COX-2 may thus be expressed at early time points in premetastatic LNs, with the COX-2-mediated PGE2-EP3 signaling pathway ultimately contributing to a more robust LNM.
Lipid metabolism
Tumors are characterized by pronounced metabolic changes conducive to enhanced proliferation, survival, and immune evasion.357 Most notably, the oncogenic shift toward aerobic glycolysis, known as the Warburg effect, is a canonical hallmark of cancer.121 Through a comparative analysis of primary and LN metastatic tumors in mice, Lee et al.97 found that LNM is associated with a shift in tumor metabolic activity in favor of FAO. They subsequently found that the selective stimulation of FAO highlighted a potential role for accumulated bile acid-drive YAP activation, thereby driving the development of LNM. YAP or FAO inhibition thus provides a means of depriving tumor cells of access to bile acids and FAs within LNs as a source of energy, highlighting the promise of these approaches as a means of preventing or treating LNM.
Immunotherapy
Rather than targeting tumors directly, immunotherapeutic regimens rely on targeting the immune system in order to activate or restore appropriate antitumor defense mechanisms as a means of indirectly killing malignant cells.358 The development of increasingly robust immunotherapies has spurred growing interest in TDLNs as the key secondary lymphoid organs to which immune cells are recruited for the induction of antitumor immunty.359 Extant immunotherapy strategies include cell-based therapies, immune checkpoint inhibitors (ICIs), cancer vaccines, and oncolytic viruses. The first three of these modalities are discussed in greater length below.360
Immune cell therapy
Immune cell therapy relies on leveraging the properties of particular cells of interest through in vitro expansion under defined culture conditions and/or bioengineering. The resultant cells can directly kill target tumor cells or pathogens, enhance immune function, and promote tissue regeneration as a means of treating disease.361 Chimeric antigen receptor (CAR)-T cells are currently the most common form of cell-based antitumor immunotherapy. The FDA and other regulatory bodies have approved multiple CAR-T regimens for specific indications in light of the results of appropriate clinical trials. These engineered cells can engage a range of target proteins, including CD19, CD20, CD22, GPC3, and B-cell maturation antigen (BCMA).362 Trials using CAR-T cells targeting the B cell antigen CD19 have exhibited a high degree of efficacy against acute lymphocytic leukemia,363,364,365,366,367 chronic lymphocytic leukemia,347,368,369 and non-Hodgkin lymphoma.370,371,372,373,374,375 Meanwhile, CAR-T cells targeting BCMA have demonstrated activity in multiple myeloma.376,377,378,379
Immune detection blocker
ICIs such as those targeting the CTLA-4 and PD-1 pathways provide a means of overcoming the ability of tumor cells to suppress T cell activity, thereby restoring effective T cell-mediated tumor recognition and killing.358 The binding of PD-L1 to PD-1 triggers co-inhibitor signaling that inhibits the activation and function of effector T cells, instead favoring regulatory T cell differentiation and activity in a manner that suppresses adaptive immunity. Elevated cell surface PD-L1 and PD-L2 expression by tumor cells is a common strategy conducive to immune escape.380,381 A growing number of antibodies targeting PD-1 and PD-L1 have been developed and approved for clinical use to date. The US FDA has improved anti-PD-1 monoclonal antibodies, including Nivolumab, Pembrolizumab, Cemiplimab, Toripalimab, Cindilimab, and Camrelizumab, as well as anti-PD-L1 monoclonal antibodies including Atezolizumab, Avelumab, and Durvalumab.382
Cancer vaccine
Cancer vaccines are a form of active immunotherapy that rely on the use of tumor-specific antigens to induce a directed and robust antitumor immune response in immunized patients. These vaccines seek to engage both T and B cells to produce humoral and cellular immunity directed against target tumors, preventing oncogenic progression and tumor clearance. Despite intensive research in both academic and pharmaceutical settings, however, efforts to design cancer vaccines have been largely unsuccessful. Efforts to optimize therapeutic cancer vaccines center around both structural design and the selection of appropriate antigens.383 Ideal antigens are those that can direct immune cells to generate a robust adaptive response sufficient to target cancer stem cells and prevent recurrence while avoiding any off-target damage to healthy cells.384 Tailored vaccine design efforts seek to optimize professional antigen-presenting cell-mediated T cell activation and to engage a range of complementary mechanisms to overcome tumor-associated immunosuppression.384,385,386
Nanodelivery system
As drug uptake by the lymphatic system is relatively limited, drug delivery to this compartment tends to be suboptimal.387 Indeed, most small molecules drain primarily from interstitial spaces through blood capillaries, given that blood flow rates are 100 to 500 times faster than lymphatic flow rates, constraining drug delivery. Macromolecular constructs, however, can facilitate more targeted lymphatic drug delivery owing to the exclusion of these constructs from the blood due to their larger size, which is not a barrier to lymphatic entry.15 In light of this, researchers have employed a range of approaches to chemically modify drugs with nanocarrier materials aimed at enhancing drug enrichment within the lymphatic system, through strategies such as the covalent coupling of drugs with lipids, including FAs, diglycerides, or phosphoglycerides.3,388 Various delivery methods have also been employed for this purpose as well, such as the mucosal administration of particulate materials, parenteral or interstitial delivery of macromolecular materials, and intestinal or oral delivery of lipophilic drugs.15 Below, we provide a brief overview of nanomaterial-based approaches that seek to enhance drug delivery and retention in the LNs. These strategies include insoluble drug encapsulation,389,390 the protection of therapeutic molecules,391 and the modulation of nanomaterial biodistribution and circulation dynamics.392,393 Broadly speaking, these targeting strategies can be classified as being active or passive.394
Passive targeting strategy
Passive targeting approaches rely on the manipulation of nanomaterial properties such as size, shape, surface charge, and chemical composition in a manner aimed at ensuring the lymphatic enrichment of these modified nanostructures.395
Size
Unlike the endothelial layer that encloses blood vessels, the lymphatic endothelium consists of loosely connected LECs with an incomplete basement membrane layer. As a result, certain drugs can pass freely into the lymphatic system such that they can be captured by macrophages within LNs, providing an avenue for the targeted delivery of therapeutic agents to this compartment.112 Relative to larger NPs 100–200 nm in diameter, lipid diameters closer to 30 nm in size are better optimized for uptake by DCs, suggesting that they may be better able to target LNs.396
Shape
Efforts to adjust the shape of NPs have the potential to address certain limitations associated with the extent of therapeutic strategies, as the geometry of these particles can heavily impact their organ/tumor-targeting, cellular uptake, pharmacokinetic properties, and biodistribution.397 Flexible or non-spherical parties tend to exhibit a longer half-life in the systemic circulation. However, the optimal geometric properties necessary to engineer tumor-targeted NPs remain to be established, highlighting key avenues for future research.398
Surface charge
The interstitium has a net negative charge due to the glycosaminoglycans present therein.399 Small particles and neutral or negatively charged particles can be absorbed into the lymphatic vessels whereupon they can accumulate within LNs, while NPs with a positive charge are primarily restricted to uptake by DCs at the site of injection and direct transport through the lymphatic vessels.396
Chemical composition
Modifying the functional groups of drug molecules can enable them to more readily aggregate at lytic sites.400 PEGylation, for example, can decrease the immunogenicity and toxicity of certain drugs while enhancing their bioavailability, thus improving lymphatic exposure. When evaluating a subcutaneously administered dendrimer, Ryan et al.401 observed an increase in systemic bioavailability from 26% to nearly 100% following complete PEGylation. Hanson et al.398 employed PEG lipid NPs to encapsulate cyclic dinucleotides, enabling the redirection of the adjuvant to appropriate draining LNs and thus enhancing adjuvant efficacy, resulting in stronger polypeptide vaccine-induced CD8+ T cell responses and more robust antitumor immunotherapy. Cabral et al.402 recently demonstrated that polyethylene glycol (PEG)-based micelles containing platinum anticancer agents (DACHPt/m) can accumulate and inhibit melanoma LN metastases following intravenous delivery.
Active targeting strategy
Active targeting approaches rely on approaches that factor nanoparticle transport and internalization through the modification of nanoparticle surfaces using ligands capable of binding receptor proteins overexpressed by tumor cells. The primary ligands that have been employed in this context to date include LyP-1, TMTP1, and RGD.403
LyP-1
The nine amino acid cyclic LyP-1 homing peptide can bind specifically to the P32 cell surface receptor, which is overexpressed by tumor cells and tumor-associated LECs, whereas LyP-1 cannot bind normal LECs.404 Song et al.405 produced LyP-1 peptide-modified 131I-labeled dendrimers that exhibited good cytocompatibility. Stable 131I labeling was effectively achieved at a high degree of radiochemical purity in their study, allowing for the use of these dendrimers as a diagnostic tool in the context of SPECT imaging and as a radionuclide therapy agent capable of counteracting metastatic tumor progression in vitro and in vivo in a subcutaneous tumor model system.
TMTP1
The tumor-targeting peptide TMTP1 (NVVRQ) enables the specific targeting of metastatic tumors, even when they are early-stage occult metastatic foci. Through the fusion of TMPT1 with proteins or peptides with therapeutic efficacy, it can exert robust in vitro and in vivo antitumor activity.406 Wei et al.407 successfully combined this TMTP1 peptide with ICG-loaded PEG-PLGA micelles. They then established a model of SLN metastasis by BALB/c nude mice injected in the right hock using HeLa cells expressing firefly luciferase. These analyses revealed that the ICG-loaded TMTP1-PEG-PLGA micelles were able to rapidly diffuse from the injection site along lymphatic capillaries, reaching SLNs and then remaining present therein for 12 h.
RGD
Tumor cells primarily overexpress isoforms of αvβ3 integrin capable of interacting with the RGD motif with a cryptic CendR CendR motif, and this interaction is central to LNM progression. Researchers have taken advantage of this process to produce RGD-modified complexes that can facilitate targeted anticancer drug delivery following receptor-mediated internalization. Murphy et al.408 generated RGD-modified nanoparticles containing Dox (1 mg/kg) that were able to suppress pancreatic carcinoma growth and hilar LNM more readily than control preparations not conjugated to RGD.
Theranostics: novel direction of development
Theranostic applications, which integrate both diagnostic and therapeutic tools, have emerged as a focus of growing research interest in cancer and other diseases in recent years. Theranostic advances have the potential to aid precision oncology efforts by facilitating patient selection, treatment planning, and subsequent monitoring. Progress in the theranostic spaces has been driven by the combined interdisciplinary research contributions from fields including chemistry, pharmacology, biomedicine, tissue engineering, nanotechnology, and material sciences.409,410
Some studies have sought to apply theranostic approaches to target LNM. Oh et al.411 employed a combination of docetaxel-loaded Pluronic nanoparticles and the molecular imaging dye FPR-675 such that the delivery of both metastatic LNs and primary tumors would enable effective imaging and treatment. Cai et al.412 also prepared hybrid nanocomposite materials that were used for the multimodal imaging-guided photothermal treatment of LNM. Specifically, they utilized Fe3O4 to enable MRI imaging, 99mTc as a radiotracer for SPECT imaging, and IR-1061 to facilitate photoacoustic imaging, NIR fluorescent imaging, and photothermal treatment. Moreover, Liu et al.222 additionally utilized carbon nanoparticles, which exhibit excellent NIR absorption and utility in the context of photoacoustic imaging-guided photothermal therapy. By loading these particles with perfluorohexane and docetaxel and mixing them with PLGA nanoparticles modified with anti-HIF-1α, they were able to achieve the US/PA dual imaging-guided and laser-triggered release of docetaxel in situ through a passive intracellular LNM targeting approach (Fig. 12).

A visualized precision medicine nanoplatform of metastatic LNs for US/PA dual-modal imaging-guided in situ targeted hyperthermia-combined chemotherapy.222 Copyright 2021, Springer Nature. NP nanoparticle, PFH perfluorohexane, PLGA poly (lactatco-glycolic acid), LN lymph node, US ultrasonic, PA photoacoustic
Conclusion
Over the last several decades, hundreds of systematic studies have explored the mechanisms that underlie the metastasis of primary tumor cells to lymph nodes, highlighting a complex array of regulatory interactions between primary tumors, disseminated tumor cells, the immune system, and the TDLN microenvironment in this context. Clinical trials focused on patients with metastatic LNs have emphasized the relevance of LNM to tumor staging, treatment planning, and prognostic outcomes. As metastatic LNs are far harder to detect than primary tumors, reliably identifying and diagnosing these metastatic nodes remains a persistent clinical problem. However, the advent of nanoparticles and other novel techniques has the potential to improve the reliability of LNM diagnosis. The number of available therapeutic targets and associated treatments undergoing testing in clinical trials also continued to expand, providing new opportunities for clinical advancement. In conclusion, the ongoing exploration of the mechanisms that govern LNM is likely to enable the identification of novel diagnostic and therapeutic strategies, ultimately contributing to the establishment of more effective LN management strategies that will improve lives and prolong the survival of countless cancer patients.
References
Gasteiger, G., Ataide, M. & Kastenmüller, W. Lymph node - an organ for T-cell activation and pathogen defense. Immunol. Rev. 271, 200–220 (2016).
Rezzola, S., Sigmund, E. C., Halin, C. & Ronca, R. The lymphatic vasculature: an active and dynamic player in cancer progression. Med. Res. Rev. 42, 576–614 (2022).
Zhou, H., Lei, P. J. & Padera, T. P. Progression of metastasis through lymphatic system. Cells 10, 627 (2021).
Obinu, A. et al. Lymph node metastases: importance of detection and treatment strategies. Expert Opin. Drug Deliv. 15, 459–467 (2018).
Takeda, A., Salmi, M. & Jalkanen, S. Lymph node lymphatic endothelial cells as multifaceted gatekeepers in the immune system. Trends Immunol. 44, 72–86 (2023).
Sainte-Marie, G. The lymph node revisited: development, morphology, functioning, and role in triggering primary immune responses. Anat. Rec. 293, 320–337 (2010).
Jalkanen, S. & Salmi, M. Lymphatic endothelial cells of the lymph node. Nat. Rev. Immunol. 20, 566–578 (2020).
Gillot, L., Baudin, L., Rouaud, L., Kridelka, F. & Noel, A. The pre-metastatic niche in lymph nodes: formation and characteristics. Cell Mol. Life Sci. 78, 5987–6002 (2021).
Li, Y. L. & Hung, W. C. Reprogramming of sentinel lymph node microenvironment during tumor metastasis. J. Biomed. Sci. 29, 84 (2022).
Krishnamurty, A. T. & Turley, S. J. Lymph node stromal cells: cartographers of the immune system. Nat. Immunol. 21, 369–380 (2020).
Girard, J. P., Moussion, C. & Förster, R. HEVs, lymphatics and homeostatic immune cell trafficking in lymph nodes. Nat. Rev. Immunol. 12, 762–773 (2012).
Novkovic, M., Onder, L., Bocharov, G. & Ludewig, B. Topological structure and robustness of the lymph node conduit system. Cell Rep. 30, 893–904.e896 (2020).
Acton, S. E., Onder, L., Novkovic, M., Martinez, V. G. & Ludewig, B. Communication, construction, and fluid control: lymphoid organ fibroblastic reticular cell and conduit networks. Trends Immunol. 42, 782–794 (2021).
Li, L., Wu, J., Abdi, R., Jewell, C. M. & Bromberg, J. S. Lymph node fibroblastic reticular cells steer immune responses. Trends Immunol. 42, 723–734 (2021).
Trevaskis, N. L., Kaminskas, L. M. & Porter, C. J. From sewer to saviour - targeting the lymphatic system to promote drug exposure and activity. Nat. Rev. Drug Discov. 14, 781–803 (2015).
Follain, G. et al. Fluids and their mechanics in tumour transit: shaping metastasis. Nat. Rev. Cancer 20, 107–124 (2020).
Swartz, M. A. & Lund, A. W. Lymphatic and interstitial flow in the tumour microenvironment: linking mechanobiology with immunity. Nat. Rev. Cancer 12, 210–219 (2012).
Jain, R. K., Tong, R. T. & Munn, L. L. Effect of vascular normalization by antiangiogenic therapy on interstitial hypertension, peritumor edema, and lymphatic metastasis: insights from a mathematical model. Cancer Res. 67, 2729–2735 (2007).
Hompland, T., Ellingsen, C., Øvrebø, K. M. & Rofstad, E. K. Interstitial fluid pressure and associated lymph node metastasis revealed in tumors by dynamic contrast-enhanced MRI. Cancer Res. 72, 4899–4908 (2012).
Cornelison, R. C., Brennan, C. E., Kingsmore, K. M. & Munson, J. M. Convective forces increase CXCR4-dependent glioblastoma cell invasion in GL261 murine model. Sci. Rep. 8, 17057 (2018).
Huang, Y. L., Tung, C. K., Zheng, A., Kim, B. J. & Wu, M. Interstitial flows promote amoeboid over mesenchymal motility of breast cancer cells revealed by a three dimensional microfluidic model. Integr. Biol. 7, 1402–1411 (2015).
Shields, J. D. et al. Autologous chemotaxis as a mechanism of tumor cell homing to lymphatics via interstitial flow and autocrine CCR7 signaling. Cancer Cell 11, 526–538 (2007).
Li, R. et al. Interstitial flow promotes macrophage polarization toward an M2 phenotype. Mol. Biol. Cell 29, 1927–1940 (2018).
Issa, A., Le, T. X., Shoushtari, A. N., Shields, J. D. & Swartz, M. A. Vascular endothelial growth factor-C and C-C chemokine receptor 7 in tumor cell-lymphatic cross-talk promote invasive phenotype. Cancer Res. 69, 349–357 (2009).
Das, S. et al. Tumor cell entry into the lymph node is controlled by CCL1 chemokine expressed by lymph node lymphatic sinuses. J. Exp. Med. 210, 1509–1528 (2013).
Farnsworth, R. H., Karnezis, T., Maciburko, S. J., Mueller, S. N. & Stacker, S. A. The interplay between lymphatic vessels and chemokines. Front. Immunol. 10, 518 (2019).
Guan, X. Cancer metastases: challenges and opportunities. Acta Pharm. Sin. B 5, 402–418 (2015).
Woo, H. Y. et al. Lung and lymph node metastases from hepatocellular carcinoma: comparison of pathological aspects. Liver Int. 42, 199–209 (2022).
Huang, M. et al. HSF1 facilitates the multistep process of lymphatic metastasis in bladder cancer via a novel PRMT5-WDR5-dependent transcriptional program. Cancer Commun. 42, 447–470 (2022).
Wang, N. et al. PRMT5/Wnt4 axis promotes lymph-node metastasis and proliferation of laryngeal carcinoma. Cell Death Dis. 11, 864 (2020).
Yang, Y. et al. The NQO1/PKLR axis promotes lymph node metastasis and breast cancer progression by modulating glycolytic reprogramming. Cancer Lett. 453, 170–183 (2019).
Zhao, J. et al. Mitochondrial dynamics regulates migration and invasion of breast cancer cells. Oncogene 32, 4814–4824 (2013).
Abe, N. et al. Clinicopathological significance of lymphangiogenesis detected by immunohistochemistry using D2-40 monoclonal antibody in breast cancer. Fukushima J. Med. Sci. 62, 57–63 (2016).
Mäkinen, T. et al. Isolated lymphatic endothelial cells transduce growth, survival and migratory signals via the VEGF-C/D receptor VEGFR-3. EMBO J. 20, 4762–4773 (2001).
Klein, S. et al. DeepCAGE transcriptomics identify HOXD10 as a transcription factor regulating lymphatic endothelial responses to VEGF-C. J. Cell Sci. 129, 2573–2585 (2016).
Sammarco, G. et al. Mast cells, angiogenesis and lymphangiogenesis in human gastric cancer. Int. J. Mol. Sci. 20, 2106 (2019).
Liu, S., Chen, X. & Lin, T. Lymphatic metastasis of bladder cancer: molecular mechanisms, diagnosis and targeted therapy. Cancer Lett. 505, 13–23 (2021).
Zhang, Y. Q. et al. Over-expression of both VEGF-C and Twist predicts poor prognosis in human breast cancer. Clin. Transl. Oncol. 21, 1250–1259 (2019).
Qin, T. et al. Clinical importance of VEGFC and PD-L1 co-expression in lung adenocarcinoma patients. Thorac. Cancer 11, 1139–1148 (2020).
Lala, P. K., Nandi, P. & Majumder, M. Roles of prostaglandins in tumor-associated lymphangiogenesis with special reference to breast cancer. Cancer Metastasis Rev. 37, 369–384 (2018).
Sha, M. et al. Expression of VEGFR-3 in intrahepatic cholangiocarcinoma correlates with unfavorable prognosis through lymphangiogenesis. Int. J. Biol. Sci. 14, 1333–1342 (2018).
Shin, J. W. et al. Prox1 promotes lineage-specific expression of fibroblast growth factor (FGF) receptor-3 in lymphatic endothelium: a role for FGF signaling in lymphangiogenesis. Mol. Biol. cell 17, 576–584 (2006).
Cao, R. et al. PDGF-BB induces intratumoral lymphangiogenesis and promotes lymphatic metastasis. Cancer Cell 6, 333–345 (2004).
Cadamuro, M. et al. Platelet-derived growth factor-D enables liver myofibroblasts to promote tumor lymphangiogenesis in cholangiocarcinoma. J. Hepatol. 70, 700–709 (2019).
Korhonen, E. A. et al. Lymphangiogenesis requires Ang2/Tie/PI3K signaling for VEGFR3 cell-surface expression. J. Clin. Invest. 132, e155478 (2022).
Cao, R. et al. Collaborative interplay between FGF-2 and VEGF-C promotes lymphangiogenesis and metastasis. Proc. Natl Acad. Sci. USA 109, 15894–15899 (2012).
Li, Z. J. et al. Insulin-like growth factor-1 induces lymphangiogenesis and facilitates lymphatic metastasis in colorectal cancer. World J. Gastroenterol. 19, 7788–7794 (2013).
Bracher, A. et al. Epidermal growth factor facilitates melanoma lymph node metastasis by influencing tumor lymphangiogenesis. J. Invest Dermatol. 133, 230–238 (2013).
Kajiya, K., Hirakawa, S., Ma, B., Drinnenberg, I. & Detmar, M. Hepatocyte growth factor promotes lymphatic vessel formation and function. EMBO J. 24, 2885–2895 (2005).
Pak, K. H., Park, K. C. & Cheong, J. H. VEGF-C induced by TGF- beta1 signaling in gastric cancer enhances tumor-induced lymphangiogenesis. BMC Cancer 19, 799 (2019).
Song, J. et al. CCBE1 promotes tumor lymphangiogenesis and is negatively regulated by TGFbeta signaling in colorectal cancer. Theranostics 10, 2327–2341 (2020).
Hong, H. et al. TNF-alpha promotes lymphangiogenesis and lymphatic metastasis of gallbladder cancer through the ERK1/2/AP-1/VEGF-D pathway. BMC Cancer 16, 240 (2016).
Zhao, G. et al. IL-6 mediates the signal pathway of JAK-STAT3-VEGF-C promoting growth, invasion and lymphangiogenesis in gastric cancer. Oncol. Rep. 35, 1787–1795 (2016).
Al-Rawi, M. A., Watkins, G., Mansel, R. E. & Jiang, W. G. Interleukin 7 upregulates vascular endothelial growth factor D in breast cancer cells and induces lymphangiogenesis in vivo. Br. J. Surg. 92, 305–310 (2005).
Ming, J., Zhang, Q., Qiu, X. & Wang, E. Interleukin 7/interleukin 7 receptor induce c-Fos/c-Jun-dependent vascular endothelial growth factor-D up-regulation: a mechanism of lymphangiogenesis in lung cancer. Eur. J. Cancer 45, 866–873 (2009).
Chen, X. et al. Role of interleukin-17 in lymphangiogenesis in non-small-cell lung cancer: Enhanced production of vascular endothelial growth factor C in non-small-cell lung carcinoma cells. Cancer Sci. 101, 2384–2390 (2010).
Flavin, R., Peluso, S., Nguyen, P. L. & Loda, M. Fatty acid synthase as a potential therapeutic target in cancer. Future Oncol. 6, 551–562 (2010).
Bastos, D. C. et al. Effects of fatty acid synthase inhibitors on lymphatic vessels: an in vitro and in vivo study in a melanoma model. Lab. Invest. 97, 194–206 (2017).
Du, Q. et al. FASN promotes lymph node metastasis in cervical cancer via cholesterol reprogramming and lymphangiogenesis. Cell Death Dis. 13, 488 (2022).
Kubo, H. et al. Host prostaglandin EP3 receptor signaling relevant to tumor-associated lymphangiogenesis. Biomed. Pharmacother. 64, 101–106 (2010).
Nagahashi, M. et al. Sphingosine-1-phosphate produced by sphingosine kinase 1 promotes breast cancer progression by stimulating angiogenesis and lymphangiogenesis. Cancer Res. 72, 726–735 (2012).
Weichand, B. et al. S1PR1 on tumor-associated macrophages promotes lymphangiogenesis and metastasis via NLRP3/IL-1β. J. Exp. Med. 214, 2695–2713 (2017).
Lin, Y. C. et al. LPA(1/3) signaling mediates tumor lymphangiogenesis through promoting CRT expression in prostate cancer. Biochim. Biophys. Acta Mol. Cell Biol. Lipids 1863, 1305–1315 (2018).
Garmy-Susini, B. et al. Integrin alpha4beta1 signaling is required for lymphangiogenesis and tumor metastasis. Cancer Res. 70, 3042–3051 (2010).
Tutunea-Fatan, E., Majumder, M., Xin, X. & Lala, P. K. The role of CCL21/CCR7 chemokine axis in breast cancer-induced lymphangiogenesis. Mol. Cancer 14, 35 (2015).
Bieniasz-Krzywiec, P. et al. Podoplanin-expressing macrophages promote lymphangiogenesis and lymphoinvasion in breast cancer. Cell Metab. 30, 917–936.e910 (2019).
Yan, H. et al. CD146 is required for VEGF-C-induced lymphatic sprouting during lymphangiogenesis. Sci. Rep. 7, 7442 (2017).
He, W. et al. Long noncoding RNA BLACAT2 promotes bladder cancer-associated lymphangiogenesis and lymphatic metastasis. J. Clin. Invest. 128, 861–875 (2018).
Chen, C. et al. Exosomal long noncoding RNA LNMAT2 promotes lymphatic metastasis in bladder cancer. J. Clin. Invest. 130, 404–421 (2020).
Zheng, S. et al. Long non-coding RNA HUMT hypomethylation promotes lymphangiogenesis and metastasis via activating FOXK1 transcription in triple-negative breast cancer. J. Hematol. Oncol. 13, 17 (2020).
Zhu, J. et al. circEHBP1 promotes lymphangiogenesis and lymphatic metastasis of bladder cancer via miR-130a-3p/TGFbetaR1/VEGF-D signaling. Mol. Ther. 29, 1838–1852 (2021).
Kong, Y. et al. circNFIB1 inhibits lymphangiogenesis and lymphatic metastasis via the miR-486-5p/PIK3R1/VEGF-C axis in pancreatic cancer. Mol. Cancer 19, 82 (2020).
Hood, J. L., San, R. S. & Wickline, S. A. Exosomes released by melanoma cells prepare sentinel lymph nodes for tumor metastasis. Cancer Res. 71, 3792–3801 (2011).
Chung, M. K. et al. Lymphatic vessels and high endothelial venules are increased in the sentinel lymph nodes of patients with oral squamous cell carcinoma before the arrival of tumor cells. Ann. Surg. Oncol. 19, 1595–1601 (2012).
Qian, C. N. et al. Preparing the "soil": the primary tumor induces vasculature reorganization in the sentinel lymph node before the arrival of metastatic cancer cells. Cancer Res. 66, 10365–10376 (2006).
Farnsworth, R. H. et al. A role for bone morphogenetic protein-4 in lymph node vascular remodeling and primary tumor growth. Cancer Res. 71, 6547–6557 (2011).
Bekkhus, T. et al. Remodeling of the lymph node high endothelial venules reflects tumor invasiveness in breast cancer and is associated with dysregulation of perivascular stromal cells. Cancers 13, 211 (2021).
Garmy-Susini, B. et al. PI3Kα activates integrin α4β1 to establish a metastatic niche in lymph nodes. Proc. Natl Acad. Sci. USA 110, 9042–9047 (2013).
Wei, W. F. et al. Periostin(+) cancer-associated fibroblasts promote lymph node metastasis by impairing the lymphatic endothelial barriers in cervical squamous cell carcinoma. Mol. Oncol. 15, 210–227 (2021).
Commerford, C. D. et al. Mechanisms of tumor-induced lymphovascular niche formation in draining lymph nodes. Cell Rep. 25, 3554–3563.e3554 (2018).
Paolillo, M. & Schinelli, S. Extracellular matrix alterations in metastatic processes. Int. J. Mol. Sci. 20, 4947 (2019).
Martinez, V. G. et al. Fibroblastic reticular cells control conduit matrix deposition during lymph node expansion. Cell Rep. 29, 2810–2822.e2815 (2019).
Li, L. et al. Lymph node fibroblastic reticular cells preserve a tolerogenic niche in allograft transplantation through laminin α4. J. Clin. Invest. 132, e156994 (2022).
Riedel, A. et al. Tumor-derived lactic acid modulates activation and metabolic status of draining lymph node stroma. Cancer Immunol. Res. 10, 482–497 (2022).
Rovera, C. et al. Secretion of IL1 by dedifferentiated melanoma cells inhibits JAK1-STAT3-driven actomyosin contractility of lymph node fibroblastic reticular cells. Cancer Res. 82, 1774–1788 (2022).
Riedel, A., Shorthouse, D., Haas, L., Hall, B. A. & Shields, J. Tumor-induced stromal reprogramming drives lymph node transformation. Nat. Immunol. 17, 1118–1127 (2016).
Chen, S. et al. Single-cell analysis reveals transcriptomic remodellings in distinct cell types that contribute to human prostate cancer progression. Nat. Cell Biol. 23, 87–98 (2021).
Otto, B. et al. Molecular changes in pre-metastatic lymph nodes of esophageal cancer patients. PLoS ONE 9, e102552 (2014).
Matsuura, K. et al. Maturation of dendritic cells and T-cell responses in sentinel lymph nodes from patients with breast carcinoma. Cancer 106, 1227–1236 (2006).
van Pul, K. M. et al. Selectively hampered activation of lymph node-resident dendritic cells precedes profound T cell suppression and metastatic spread in the breast cancer sentinel lymph node. J. Immunother. Cancer 7, 133 (2019).
Go, Y. et al. Tumor-associated macrophages extend along lymphatic flow in the pre-metastatic lymph nodes of human gastric cancer. Ann. Surg. Oncol. 23, S230–S235 (2016).
Ogawa, F. et al. Prostanoid induces premetastatic niche in regional lymph nodes. J. Clin. Invest. 124, 4882–4894 (2014).
Kos, K. et al. Tumor-educated T(regs) drive organ-specific metastasis in breast cancer by impairing NK cells in the lymph node niche. Cell Rep. 38, 110447 (2022).
Deng, J. et al. S1PR1-STAT3 signaling is crucial for myeloid cell colonization at future metastatic sites. Cancer Cell 21, 642–654 (2012).
Gu, Y. et al. Tumor-educated B cells selectively promote breast cancer lymph node metastasis by HSPA4-targeting IgG. Nat. Med. 25, 312–322 (2019).
Coffelt, S. B. et al. IL-17-producing γδ T cells and neutrophils conspire to promote breast cancer metastasis. Nature 522, 345–348 (2015).
Lee, C. K. et al. Tumor metastasis to lymph nodes requires YAP-dependent metabolic adaptation. Science 363, 644–649 (2019).
Zhang, C. et al. FABP5 promotes lymph node metastasis in cervical cancer by reprogramming fatty acid metabolism. Theranostics 10, 6561–6580 (2020).
Shang, C. et al. LNMICC promotes nodal metastasis of cervical cancer by reprogramming fatty acid metabolism. Cancer Res. 78, 877–890 (2018).
Pascual, G. et al. Targeting metastasis-initiating cells through the fatty acid receptor CD36. Nature 541, 41–45 (2017).
Jia, Y. et al. Long non-coding RNA NEAT1 mediated RPRD1B stability facilitates fatty acid metabolism and lymph node metastasis via c-Jun/c-Fos/SREBP1 axis in gastric cancer. J. Exp. Clin. Cancer Res. 41, 287 (2022).
Dhatchinamoorthy, K., Colbert, J. D. & Rock, K. L. Cancer immune evasion through loss of MHC class I antigen presentation. Front. Immunol. 12, 636568 (2021).
Axelrod, M. L., Cook, R. S., Johnson, D. B. & Balko, J. M. Biological consequences of MHC-II expression by tumor cells in cancer. Clin. Cancer Res. 25, 2392–2402 (2019).
Yoshii, M. et al. Association of MHC class I expression and lymph node metastasis of gastric carcinoma. Hepatogastroenterology 60, 611–615 (2013).
Messaoudene, M. et al. T-cell bispecific antibodies in node-positive breast cancer: novel therapeutic avenue for MHC class I loss variants. Ann. Oncol. 30, 934–944 (2019).
Park, I. A. et al. Expression of the MHC class II in triple-negative breast cancer is associated with tumor-infiltrating lymphocytes and interferon signaling. PLoS ONE 12, e0182786 (2017).
Reticker-Flynn, N. E. et al. Lymph node colonization induces tumor-immune tolerance to promote distant metastasis. Cell 185, 1924–1942.e1923 (2022).
Erdogdu, I. H. MHC class 1 and PDL-1 status of primary tumor and lymph node metastatic tumor tissue in gastric cancers. Gastroenterol. Res. Pract. 2019, 4785098 (2019).
Kessler, D. J., Mickel, R. A. & Lichtenstein, A. Depressed natural killer cell activity in cervical lymph nodes containing focal metastatic squamous cell carcinoma. Arch. Otolaryngol. Head Neck Surg. 114, 313–318 (1988).
Nunez, N. G. et al. Tumor invasion in draining lymph nodes is associated with Treg accumulation in breast cancer patients. Nat. Commun. 11, 3272 (2020).
Huang, S. C. et al. TGF-β1 secreted by Tregs in lymph nodes promotes breast cancer malignancy via up-regulation of IL-17RB. EMBO Mol. Med. 9, 1660–1680 (2017).
Padera, T. P., Meijer, E. F. & Munn, L. L. The lymphatic system in disease processes and cancer progression. Annu. Rev. Biomed. Eng. 18, 125–158 (2016).
Nathanson, S. D., Kwon, D., Kapke, A., Alford, S. H. & Chitale, D. The role of lymph node metastasis in the systemic dissemination of breast cancer. Ann. Surg. Oncol. 16, 3396–3405 (2009).
Quinn, J. J. et al. Single-cell lineages reveal the rates, routes, and drivers of metastasis in cancer xenografts. Science 371, eabc1944 (2021).
Brown, M. et al. Lymph node blood vessels provide exit routes for metastatic tumor cell dissemination in mice. Science 359, 1408–1411 (2018).
Pereira, E. R. et al. Lymph node metastases can invade local blood vessels, exit the node, and colonize distant organs in mice. Science 359, 1403–1407 (2018).
Naxerova, K. et al. Origins of lymphatic and distant metastases in human colorectal cancer. Science 357, 55–60 (2017).
Leong, S. P. et al. The lymphatic system and sentinel lymph nodes: conduit for cancer metastasis. Clin. Exp. Metastasis 39, 139–157 (2022).
Farjah, F. & Tanner, N. T. Mediastinal staging for lung cancer. Chest 160, 1552–1559 (2021).
De Marco, C., Biondi, A. & Ricci, R. N staging: the role of the pathologist. Transl. Gastroenterol. Hepatol. 2, 10 (2017).
Hanahan, D. & Weinberg, R. A. Hallmarks of cancer: the next generation. Cell 144, 646–674 (2011).
Amin, M. B. et al. The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more "personalized" approach to cancer staging. CA Cancer J. Clin. 67, 93–99 (2017).
Iwanaga, J., Lofton, C., He, P., Dumont, A. S. & Tubbs, R. S. Lymphatic system of the head and neck. J. Craniofac. Surg. 32, 1901–1905 (2021).
Ying, M. & Ahuja, A. Sonography of neck lymph nodes. Part I: normal lymph nodes. Clin. Radiol. 58, 351–358 (2003).
Robbins, K. T. et al. Neck dissection classification update: revisions proposed by the American Head and Neck Society and the American Academy of Otolaryngology–Head and Neck Surgery. Arch. Otolaryngol. Head Neck Surg. 128, 751–758 (2002).
Zanoni, D. K., Patel, S. G. & Shah, J. P. Changes in the 8th edition of the American Joint Committee on Cancer (AJCC) Staging of Head and Neck Cancer: rationale and implications. Curr. Oncol. Rep. 21, 52 (2019).
Caudell, J. J. et al. NCCN Guidelines® Insights: head and neck cancers, version 1.2022. J. Natl Compr. Cancer Netw. 20, 224–234 (2022).
Bhattacharya, P. & Mukherjee, R. Lymph node extracapsular extension as a marker of aggressive phenotype: classification, prognosis and associated molecular biomarkers. Eur. J. Surg. Oncol. 47, 721–731 (2021).
Adler, C., Lubner, M. G., Menias, C. O., Lubner, S. J. & Dahiya, N. What’s in a node? The clinical and radiologic significance of Virchow’s node. Abdom. Radiol. 47, 2244–2253 (2022).
Chow, L. Q. M. Head and neck cancer. N. Engl. J. Med. 382, 60–72 (2020).
Robbins, K. T. et al. Consensus statement on the classification and terminology of neck dissection. Arch. Otolaryngol. Head. Neck Surg. 134, 536–538 (2008).
Giammarile, F. et al. Sentinel lymph node methods in breast cancer. Semin. Nucl. Med. 52, 551–560 (2022).
Jana, S., Muscarella, R. A. Jr. & Jones, D. The multifaceted effects of breast cancer on tumor-draining lymph nodes. Am. J. Pathol. 191, 1353–1363 (2021).
Teichgraeber, D. C., Guirguis, M. S. & Whitman, G. J. Breast cancer staging: updates in the AJCC Cancer Staging Manual, 8th Edition, and current challenges for radiologists, from the AJR special series on cancer staging. Am. J. Roentgenol. 217, 278–290 (2021).
Sun, S. X., Moseley, T. W., Kuerer, H. M. & Yang, W. T. Imaging-based approach to axillary lymph node staging and sentinel lymph node biopsy in patients with breast cancer. Am. J. Roentgenol. 214, 249–258 (2020).
Qiu, S. Q. et al. Evolution in sentinel lymph node biopsy in breast cancer. Crit. Rev. Oncol. Hematol. 123, 83–94 (2018).
Olson, J. A. Jr. et al. Impact of immediate versus delayed axillary node dissection on surgical outcomes in breast cancer patients with positive sentinel nodes: results from American College of Surgeons Oncology Group Trials Z0010 and Z0011. J. Clin. Oncol. 26, 3530–3535 (2008).
Galimberti, V. et al. Axillary dissection versus no axillary dissection in patients with sentinel-node micrometastases (IBCSG 23-01): a phase 3 randomised controlled trial. Lancet Oncol. 14, 297–305 (2013).
Krag, D. N. et al. Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial. Lancet Oncol. 11, 927–933 (2010).
Dominick, S. A., Natarajan, L., Pierce, J. P., Madanat, H. & Madlensky, L. The psychosocial impact of lymphedema-related distress among breast cancer survivors in the WHEL Study. Psychooncology 23, 1049–1056 (2014).
Gentilini, O. & Veronesi, U. Abandoning sentinel lymph node biopsy in early breast cancer? A new trial in progress at the European Institute of Oncology of Milan (SOUND: Sentinel node vs Observation after axillary UltraSouND). Breast 21, 678–681 (2012).
Donker, M. et al. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer (EORTC 10981-22023 AMAROS): a randomised, multicentre, open-label, phase 3 non-inferiority trial. Lancet Oncol. 15, 1303–1310 (2014).
Donker, M. et al. Comparison of the sentinel node procedure between patients with multifocal and unifocal breast cancer in the EORTC 10981-22023 AMAROS Trial: identification rate and nodal outcome. Eur. J. Cancer 49, 2093–2100 (2013).
Overgaard, M. et al. Postoperative radiotherapy in high-risk premenopausal women with breast cancer who receive adjuvant chemotherapy. Danish Breast Cancer Cooperative Group 82b Trial. N. Engl. J. Med. 337, 949–955 (1997).
Ragaz, J. et al. Adjuvant radiotherapy and chemotherapy in node-positive premenopausal women with breast cancer. N. Engl. J. Med. 337, 956–962 (1997).
Fisher, B. et al. Effect of preoperative chemotherapy on local-regional disease in women with operable breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-18. J. Clin. Oncol. 15, 2483–2493 (1997).
van der Hage, J. A. et al. Preoperative chemotherapy in primary operable breast cancer: results from the European Organization for Research and Treatment of Cancer trial 10902. J. Clin. Oncol. 19, 4224–4237 (2001).
Bear, H. D. et al. The effect on tumor response of adding sequential preoperative docetaxel to preoperative doxorubicin and cyclophosphamide: preliminary results from National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J. Clin. Oncol. 21, 4165–4174 (2003).
Golshan, M. et al. Impact of neoadjuvant chemotherapy in stage II-III triple negative breast cancer on eligibility for breast-conserving surgery and breast conservation rates: surgical results from CALGB 40603 (Alliance). Ann. Surg. 262, 434–439 (2015).
Hunt, K. K. et al. Sentinel lymph node surgery after neoadjuvant chemotherapy is accurate and reduces the need for axillary dissection in breast cancer patients. Ann. Surg. 250, 558–566 (2009).
Poortmans, P. M. et al. Internal mammary and medial supraclavicular lymph node chain irradiation in stage I-III breast cancer (EORTC 22922/10925): 15-year results of a randomised, phase 3 trial. Lancet Oncol. 21, 1602–1610 (2020).
Jinnai, S., Namikawa, K., Takahashi, A., Ogata, D. & Yamazaki, N. Incidence and patterns of lymphatic drainage to the epitrochlear and popliteal sentinel lymph nodes in malignant melanoma of the distal extremities: a single-institution retrospective study. Int. J. Dermatol. 61, 855–860 (2022).
Terwisscha van Scheltinga, C. E. J. et al. In transit metastases in children, adolescents and young adults with localized rhabdomyosarcoma of the distal extremities: analysis of the EpSSG RMS 2005 study. Eur. J. Surg. Oncol. 48, 1536–1542 (2022).
Zhou, Y. et al. Case report: intercostal lymph node metastasis: a case report and review of the literature. Front. Oncol. 11, 638948 (2021).
Friedberg, J. S. et al. Posterior intercostal lymph nodes double recurrence and death risk in malignant pleural mesothelioma. Ann. Thorac. Surg. 110, 241–250 (2020).
Berger, I. et al. CT for detection of malignant posterior intercostal lymph nodes in patients undergoing pre-operative staging for malignant pleural mesothelioma. Lung Cancer 152, 34–38 (2021).
Shamji, F. M., Beauchamp, G. & Sekhon, H. J. S. The lymphatic spread of lung cancer: an investigation of the anatomy of the lymphatic drainage of the lungs and preoperative mediastinal staging. Thorac. Surg. Clin. 31, 429–440 (2021).
Asamura, H. et al. The International Association for the Study of Lung Cancer Lung Cancer Staging Project: proposals for the revision of the N descriptors in the forthcoming 8th edition of the TNM classification for lung cancer. J. Thorac. Oncol. 10, 1675–1684 (2015).
Fu, Z. et al. Excellent survival of pathological N0 small cell lung cancer patients following surgery. Eur. J. Med. Res. 28, 91 (2023).
Rusch, V. W. et al. The IASLC lung cancer staging project: a proposal for a new international lymph node map in the forthcoming seventh edition of the TNM classification for lung cancer. J. Thorac. Oncol. 4, 568–577 (2009).
Yun, J. K. et al. Comparison between lymph node station- and zone-based classification for the future revision of node descriptors proposed by the International Association for the Study of Lung Cancer in surgically resected patients with non-small-cell lung cancer. Eur. J. Cardiothorac. Surg. 56, 849–857 (2019).
Rena, O. et al. Metastasis to subsegmental and segmental lymph nodes in patients resected for non-small cell lung cancer: prognostic impact. Ann. Thorac. Surg. 97, 987–992 (2014).
Osarogiagbon, R. U. et al. The International Association for the Study of Lung Cancer Lung Cancer Staging Project: overview of challenges and opportunities in revising the nodal classification of lung cancer. J. Thorac. Oncol. 18, 410–418 (2022).
Howington, J. A., Blum, M. G., Chang, A. C., Balekian, A. A. & Murthy, S. C. Treatment of stage I and II non-small cell lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 143, e278S–e313S (2013).
Ettinger, D. S. et al. NCCN guidelines insights: non-small cell lung cancer, version 2.2021. J. Natl Compr. Cancer Netw. 19, 254–266 (2021).
Toubat, O. et al. Disparities in guideline-concordant treatment for pathologic N1 non-small cell lung cancer. Ann. Thorac. Surg. 109, 1512–1520 (2020).
Cerfolio, R. J. & Bryant, A. S. Survival of patients with unsuspected N2 (stage IIIA) nonsmall-cell lung cancer. Ann. Thorac. Surg. 86, 362–366 (2008).
Miller, M. & Hanna, N. Advances in systemic therapy for non-small cell lung cancer. BMJ 375, n2363 (2021).
Cho, H. S. & Ahn, J. H. Nomenclature and lymphatic drainage patterns of abdominal lymph nodes. J. Korean Soc. Radiol. 83, 1240–1258 (2022).
Lehnert, T., Erlandson, R. A. & Decosse, J. J. Lymph and blood capillaries of the human gastric mucosa. A morphologic basis for metastasis in early gastric carcinoma. Gastroenterology 89, 939–950 (1985).
Alexander, J. S., Ganta, V. C., Jordan, P. A. & Witte, M. H. Gastrointestinal lymphatics in health and disease. Pathophysiology 17, 315–335 (2010).
Katai, H. et al. Five-year survival analysis of surgically resected gastric cancer cases in Japan: a retrospective analysis of more than 100,000 patients from the nationwide registry of the Japanese Gastric Cancer Association (2001–2007). Gastric Cancer 21, 144–154 (2018).
Kinami, S. et al. Precision surgical approach with lymph-node dissection in early gastric cancer. World J. Gastroenterol. 25, 1640–1652 (2019).
Koufuji, K., Takeda, J., Hashimoto, K., Tanaka, T. & Kakegawa, T. Early gastric cancer associated with synchronous liver metastasis. Kurum. Med. J. 38, 271–274 (1991).
Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer 14, 101–112 (2011).
Ajani, J. A. et al. Gastric cancer, version 2.2022, NCCN clinical practice guidelines in oncology. J. Natl Compr. Cancer Netw. 20, 167–192 (2022).
Smyth, E. C., Nilsson, M., Grabsch, H. I., van Grieken, N. C. & Lordick, F. Gastric cancer. Lancet 396, 635–648 (2020).
Li, G. Z., Doherty, G. M. & Wang, J. Surgical management of gastric cancer: a review. JAMA Surg. 157, 446–454 (2022).
Sasako, M. et al. D2 lymphadenectomy alone or with para-aortic nodal dissection for gastric cancer. N. Engl. J. Med. 359, 453–462 (2008).
Yoshikawa, T. et al. Phase II study of neoadjuvant chemotherapy and extended surgery for locally advanced gastric cancer. Br. J. Surg. 96, 1015–1022 (2009).
Tsuburaya, A. et al. Neoadjuvant chemotherapy with S-1 and cisplatin followed by D2 gastrectomy with para-aortic lymph node dissection for gastric cancer with extensive lymph node metastasis. Br. J. Surg. 101, 653–660 (2014).
Takahari, D. et al. Long-term outcomes of preoperative docetaxel with cisplatin plus S-1 therapy for gastric cancer with extensive nodal metastasis (JCOG1002). Gastric Cancer 23, 293–299 (2020).
Jin, C. et al. Lymph node ratio is an independent prognostic factor for rectal cancer after neoadjuvant therapy: a meta-analysis. J. Evid. Based Med. 11, 169–175 (2018).
Bates, D. D. B. et al. MRI for rectal cancer: staging, mrCRM, EMVI, lymph node staging and post-treatment response. Clin. Colorectal Cancer 21, 10–18 (2022).
Kim, H. J. & Choi, G. S. Clinical implications of lymph node metastasis in colorectal cancer: current status and future perspectives. Ann. Coloproctol. 35, 109–117 (2019).
Benson, A. B. et al. Rectal cancer, version 2.2022, NCCN clinical practice guidelines in oncology. J. Natl Compr. Cancer Netw. 20, 1139–1167 (2022).
Kapiteijn, E. et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N. Engl. J. Med. 345, 638–646 (2001).
Sebag-Montefiore, D. et al. Preoperative radiotherapy versus selective postoperative chemoradiotherapy in patients with rectal cancer (MRC CR07 and NCIC-CTG C016): a multicentre, randomised trial. Lancet 373, 811–820 (2009).
Watanabe, T. et al. Extended lymphadenectomy and preoperative radiotherapy for lower rectal cancers. Surgery 132, 27–33 (2002).
Swedish Rectal Cancer, T. et al. Improved survival with preoperative radiotherapy in resectable rectal cancer. N. Engl. J. Med. 336, 980–987 (1997).
Lee, S. I. & Atri, M. 2018 FIGO staging system for uterine cervical cancer: enter cross-sectional imaging. Radiology 292, 15–24 (2019).
Bhatla, N. et al. Revised FIGO staging for carcinoma of the cervix uteri. Int. J. Gynaecol. Obstet. 145, 129–135 (2019).
Shinaoka, A. et al. Lower-limb lymphatic drainage pathways and lymph nodes: a CT lymphangiography cadaver study. Radiology 294, 223–229 (2020).
Leone, A., Diorio, G. J., Pettaway, C., Master, V. & Spiess, P. E. Contemporary management of patients with penile cancer and lymph node metastasis. Nat. Rev. Urol. 14, 335–347 (2017).
Clark, P. E. et al. Penile cancer: clinical practice guidelines in oncology. J. Natl Compr. Cancer Netw. 11, 594–615 (2013).
Spiess, P. E. et al. Current concepts in penile cancer. J. Natl Compr. Cancer Netw. 11, 617–624 (2013).
Sato, H. et al. Management of inguinal lymph node metastases from rectal and anal canal adenocarcinoma. Colorectal Dis. 24, 1150–1163 (2022).
Nijhuis, A. A. G., de, A. O. S. F. I. D., Uren, R. F., Thompson, J. F. & Nieweg, O. E. Clinical importance and surgical management of sentinel lymph nodes in the popliteal fossa of melanoma patients. Eur. J. Surg. Oncol. 45, 1706–1711 (2019).
Schmid-Bindert, G. et al. Predicting malignancy in mediastinal lymph nodes by endobronchial ultrasound: a new ultrasound scoring system. Respirology 17, 1190–1198 (2012).
Li, F. et al. Using ultrasound features and radiomics analysis to predict lymph node metastasis in patients with thyroid cancer. BMC Surg. 20, 315 (2020).
Shin, S. Y., Hong, I. K. & Jo, Y. S. Quantitative computed tomography texture analysis: can it improve diagnostic accuracy to differentiate malignant lymph nodes? Cancer Imaging 19, 25 (2019).
Ohno, Y. et al. Metastases in mediastinal and hilar lymph nodes in patients with non-small cell lung cancer: quantitative and qualitative assessment with STIR turbo spin-echo MR imaging. Radiology 231, 872–879 (2004).
Usuda, K. et al. Advantages of diffusion-weighted imaging over positron emission tomography-computed tomography in assessment of hilar and mediastinal lymph node in lung cancer. Ann. Surg. Oncol. 20, 1676–1683 (2013).
Apostolova, I., Wedel, F. & Brenner, W. Imaging of tumor metabolism using positron emission tomography (PET). Recent Results Cancer Res. 207, 177–205 (2016).
Hofman, M. S. et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): a prospective, randomised, multicentre study. Lancet 395, 1208–1216 (2020).
Paydary, K. et al. The evolving role of FDG-PET/CT in the diagnosis, staging, and treatment of breast cancer. Mol. Imaging Biol. 21, 1–10 (2019).
Marino, M. A., Avendano, D., Zapata, P., Riedl, C. C. & Pinker, K. Lymph node imaging in patients with primary breast cancer: concurrent diagnostic tools. Oncologist 25, e231–e242 (2020).
Kikano, E. G. et al. PET/CT variants and pitfalls in breast cancers. Semin. Nucl. Med. 51, 474–484 (2021).
Wilkinson, M. J. et al. CT diagnosis of ilioinguinal lymph node metastases in melanoma using radiological characteristics beyond size and asymmetry. BJS Open 5, zraa005 (2021).
Hsu, J. C. et al. Nanoparticle contrast agents for X-ray imaging applications. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 12, e1642 (2020).
Ji, H. et al. Lanthanide-based metal-organic frameworks solidified by gelatin-methacryloyl hydrogels for improving the accuracy of localization and excision of small pulmonary nodules. J. Nanobiotechnol. 20, 60 (2022).
Han, X., Xu, K., Taratula, O. & Farsad, K. Applications of nanoparticles in biomedical imaging. Nanoscale 11, 799–819 (2019).
Birkhauser, F. D. et al. Combined ultrasmall superparamagnetic particles of iron oxide-enhanced and diffusion-weighted magnetic resonance imaging facilitates detection of metastases in normal-sized pelvic lymph nodes of patients with bladder and prostate cancer. Eur. Urol. 64, 953–960 (2013).
Vallabani, N. V. S., Singh, S. & Karakoti, A. S. Magnetic nanoparticles: current trends and future aspects in diagnostics and nanomedicine. Curr. Drug Metab. 20, 457–472 (2019).
Nie, Y. et al. A stable USPIO capable for MR lymphography with ultra-low effective dosage. Nanomedicine 29, 102233 (2020).
Dadfar, S. M. et al. Iron oxide nanoparticles: diagnostic, therapeutic and theranostic applications. Adv. Drug Deliv. Rev. 138, 302–325 (2019).
Tian, R. et al. Multiplexed NIR-II probes for lymph node-invaded cancer detection and imaging-guided surgery. Adv. Mater. 32, e1907365 (2020).
Bao, Z. et al. Ratiometric Raman nanotags enable intraoperative detection of metastatic sentinel lymph node. Biomaterials 276, 121070 (2021).
Dong, J. et al. A natural cuttlefish melanin nanoprobe for preoperative and intraoperative mapping of lymph nodes. Nanomedicine 41, 102510 (2022).
Atallah, I. et al. Role of near-infrared fluorescence imaging in the resection of metastatic lymph nodes in an optimized orthotopic animal model of HNSCC. Eur. Ann. Otorhinolaryngol. Head. Neck Dis. 132, 337–342 (2015).
Hall, M. A. et al. Imaging prostate cancer lymph node metastases with a multimodality contrast agent. Prostate 72, 129–146 (2012).
Liu, W. et al. A novel targeted multifunctional nanoplatform for visual chemo-hyperthermia synergy therapy on metastatic lymph nodes via lymphatic delivery. J. Nanobiotechnol. 19, 432 (2021).
Sampath, L., Kwon, S., Hall, M. A., Price, R. E. & Sevick-Muraca, E. M. Detection of cancer metastases with a dual-labeled near-infrared/positron emission tomography imaging agent. Transl. Oncol. 3, 307–217 (2010).
Qiu, S. et al. Detection of lymph node metastasis with near-infrared upconversion luminescent nanoprobes. Nanoscale 10, 21772–21781 (2018).
Farolfi, A. et al. Current and emerging clinical applications of PSMA PET diagnostic imaging for prostate cancer. J. Nucl. Med. 62, 596–604 (2021).
Sheikh, A., Md, S. & Kesharwani, P. RGD engineered dendrimer nanotherapeutic as an emerging targeted approach in cancer therapy. J. Control Release 340, 221–242 (2021).
Shi, H. et al. Tumor-targeting CuS nanoparticles for multimodal imaging and guided photothermal therapy of lymph node metastasis. Acta Biomater. 72, 256–265 (2018).
Chen, F. et al. Molecular phenotyping and image-guided surgical treatment of melanoma using spectrally distinct ultrasmall core-shell silica nanoparticles. Sci. Adv. 5, eaax5208 (2019).
Yin, L. et al. Rational design and synthesis of a metalloproteinase-activatable probe for dual-modality imaging of metastatic lymph nodes in vivo. J. Org. Chem. 84, 6126–6133 (2019).
Hoogstins, C. E. et al. A novel tumor-specific agent for intraoperative near-infrared fluorescence imaging: a translational study in healthy volunteers and patients with ovarian cancer. Clin. Cancer Res. 22, 2929–2938 (2016).
Bonvin, D., Bastiaansen, J. A. M., Stuber, M., Hofmann, H. & Mionic Ebersold, M. Folic acid on iron oxide nanoparticles: platform with high potential for simultaneous targeting, MRI detection and hyperthermia treatment of lymph node metastases of prostate cancer. Dalton Trans. 46, 12692–12704 (2017).
de Jong, J. M., Hoogendam, J. P., Braat, A., Zweemer, R. P. & Gerestein, C. G. The feasibility of folate receptor alpha- and HER2-targeted intraoperative fluorescence-guided cytoreductive surgery in women with epithelial ovarian cancer: a systematic review. Gynecol. Oncol. 162, 517–525 (2021).
Wang, H. et al. Interrogation of folic acid-functionalized nanomedicines: the regulatory roles of plasma proteins reexamined. ACS Nano 14, 14779–14789 (2020).
Randall, L. M., Wenham, R. M., Low, P. S., Dowdy, S. C. & Tanyi, J. L. A phase II, multicenter, open-label trial of OTL38 injection for the intra-operative imaging of folate receptor-alpha positive ovarian cancer. Gynecol. Oncol. 155, 63–68 (2019).
Kim, J., Archer, P. A. & Thomas, S. N. Innovations in lymph node targeting nanocarriers. Semin. Immunol. 56, 101534 (2021).
Bennett, Z. T. et al. Detection of lymph node metastases by ultra-pH-sensitive polymeric nanoparticles. Theranostics 10, 3340–3350 (2020).
Gialeli, C., Theocharis, A. D. & Karamanos, N. K. Roles of matrix metalloproteinases in cancer progression and their pharmacological targeting. FEBS J. 278, 16–27 (2011).
Cho, H. J. et al. Tumor microenvironment-responsive fluorogenic nanoprobe for ratiometric dual-channel imaging of lymph node metastasis. Colloids Surf. B Biointerfaces 179, 9–16 (2019).
du Bois, H., Heim, T. A. & Lund, A. W. Tumor-draining lymph nodes: at the crossroads of metastasis and immunity. Sci. Immunol. 6, eabg3551 (2021).
Handa, Y. et al. Systematic versus lobe-specific mediastinal lymphadenectomy for hypermetabolic lung cancer. Ann. Surg. Oncol. 28, 7162–7171 (2021).
Perera, M. et al. Pelvic lymph node dissection during radical cystectomy for muscle-invasive bladder cancer. Nat. Rev. Urol. 15, 686–692 (2018).
John, N. T., Blum, K. A. & Hakimi, A. A. Role of lymph node dissection in renal cell cancer. Urol. Oncol. 37, 187–192 (2019).
Karachun, A. et al. Short-term outcomes of a multicentre randomized clinical trial comparing D2 versus D3 lymph node dissection for colonic cancer (COLD trial). Br. J. Surg. 107, 499–508 (2020).
Brenkman, H. J. F. et al. A high lymph node yield is associated with prolonged survival in elderly patients undergoing curative gastrectomy for cancer: a Dutch population-based cohort study. Ann. Surg. Oncol. 24, 2213–2223 (2017).
Gschwend, J. E. et al. Extended versus limited lymph node dissection in bladder cancer patients undergoing radical cystectomy: survival results from a prospective, randomized trial. Eur. Urol. 75, 604–611 (2019).
Patel, K. N. et al. The American Association of Endocrine Surgeons Guidelines for the definitive surgical management of thyroid disease in adults. Ann. Surg. 271, e21–e93 (2020).
Leiter, U. et al. Complete lymph node dissection versus no dissection in patients with sentinel lymph node biopsy positive melanoma (DeCOG-SLT): a multicentre, randomised, phase 3 trial. Lancet Oncol. 17, 757–767 (2016).
Nakamura, Y. et al. Surgical damage to the lymphatic system promotes tumor growth via impaired adaptive immune response. J. Dermatol. Sci. 90, 46–51 (2018).
Grotz, T. E., Mansfield, A. S., Jakub, J. W. & Markovic, S. N. Regional lymphatic immunity in melanoma. Melanoma Res. 22, 9–18 (2012).
Li, X. et al. Immune characters and plasticity of the sentinel lymph node in colorectal cancer patients. J. Immunol. Res. 2021, 5516399 (2021).
Poindexter, N. J., Sahin, A., Hunt, K. K. & Grimm, E. A. Analysis of dendritic cells in tumor-free and tumor-containing sentinel lymph nodes from patients with breast cancer. Breast Cancer Res. 6, R408–R415 (2004).
Kohrt, H. E. et al. Profile of immune cells in axillary lymph nodes predicts disease-free survival in breast cancer. PLoS Med. 2, e284 (2005).
Molodtsov, A. K. et al. Resident memory CD8(+) T cells in regional lymph nodes mediate immunity to metastatic melanoma. Immunity 54, 2117–2132.e2117 (2021).
Inamori, K. et al. Importance of lymph node immune responses in MSI-H/dMMR colorectal cancer. JCI Insight 6, e137365 (2021).
Bottcher, J. P. & Reis e Sousa, C. The role of type 1 conventional dendritic cells in cancer immunity. Trends Cancer 4, 784–792 (2018).
Schenkel, J. M. et al. Conventional type I dendritic cells maintain a reservoir of proliferative tumor-antigen specific TCF-1(+) CD8(+) T cells in tumor-draining lymph nodes. Immunity 54, 2338–2353.e2336 (2021).
Dammeijer, F. et al. The PD-1/PD-L1-checkpoint restrains T cell immunity in tumor-draining lymph nodes. Cancer Cell 38, 685–700.e688 (2020).
Fransen, M. F. et al. Tumor-draining lymph nodes are pivotal in PD-1/PD-L1 checkpoint therapy. JCI Insight 3, e124507 (2018).
Rahim, M. K. et al. Dynamic CD8(+) T cell responses to cancer immunotherapy in human regional lymph nodes are disrupted in metastatic lymph nodes. Cell 186, 1127–1143.e1118 (2023).
Fisher, C. S., Margenthaler, J. A., Hunt, K. K. & Schwartz, T. The landmark series: axillary management in breast cancer. Ann. Surg. Oncol. 27, 724–729 (2020).
Qiu, M. L. et al. Current state of esophageal cancer surgery in China: a national database analysis. BMC Cancer 19, 1064 (2019).
Asai, S. et al. The impact of cervical lymph node dissection on acid and duodenogastroesophageal reflux after intrathoracic esophagogastrostomy following transthoracic esophagectomy. Surg. Today 49, 1029–1034 (2019).
Mano, R., Di Natale, R. & Sheinfeld, J. Current controversies on the role of retroperitoneal lymphadenectomy for testicular cancer. Urol. Oncol. 37, 209–218 (2019).
Deng, H. Y. et al. Lobe-specific lymph node dissection for clinical early-stage (cIA) peripheral non-small cell lung cancer patients: what and how? Ann. Surg. Oncol. 27, 472–480 (2020).
Harter, P. et al. A randomized trial of lymphadenectomy in patients with advanced ovarian neoplasms. N. Engl. J. Med. 380, 822–832 (2019).
Faiz, Z., Hayashi, T. & Yoshikawa, T. Lymph node dissection for gastric cancer: establishment of D2 and the current position of splenectomy in Europe and Japan. Eur. J. Surg. Oncol. 47, 2233–2236 (2021).
Williams, T. S., Tallon, B. & Adams, B. M. Melanoma sentinel lymph node biopsy and completion lymph node dissection: a regional hospital experience. J. Plast. Reconstr. Aesthet. Surg. 75, 730–736 (2022).
Elhusseini, M. & Aly, E. H. Lateral pelvic lymph node dissection in the management of locally advanced low rectal cancer: Summary of the current evidence. Surg. Oncol. 35, 418–425 (2020).
Filetti, S. et al. Thyroid cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-updagger. Ann. Oncol. 30, 1856–1883 (2019).
McLeod, D. S. A., Sawka, A. M. & Cooper, D. S. Controversies in primary treatment of low-risk papillary thyroid cancer. Lancet 381, 1046–1057 (2013).
Chen, L. et al. Prophylactic central neck dissection for papillary thyroid carcinoma with clinically uninvolved central neck lymph nodes: a systematic review and meta-analysis. World J. Surg. 42, 2846–2857 (2018).
Randolph, G. W. et al. The prognostic significance of nodal metastases from papillary thyroid carcinoma can be stratified based on the size and number of metastatic lymph nodes, as well as the presence of extranodal extension. Thyroid 22, 1144–1152 (2012).
Agrawal, N. et al. Indications and extent of central neck dissection for papillary thyroid cancer: an American Head and Neck Society Consensus Statement. Head. Neck 39, 1269–1279 (2017).
Hughes, D. T. et al. Prophylactic central compartment neck dissection in papillary thyroid cancer and effect on locoregional recurrence. Ann. Surg. Oncol. 25, 2526–2534 (2018).
Sieda, B., Tawfik, M. M. & Khatur, H. Is routine dissection of central lymph node and radio-active iodine therapy, necessary for papillary thyroid carcinoma, T1-2 N0? A randomized controlled trial. Int. J. Surg. Open 24, 117–124 (2020).
Mazzaferri, E. L., Doherty, G. M. & Steward, D. L. The pros and cons of prophylactic central compartment lymph node dissection for papillary thyroid carcinoma. Thyroid 19, 683–689 (2009).
Dobrinja, C. et al. Rationality in prophylactic central neck dissection in clinically node-negative (cN0) papillary thyroid carcinoma: is there anything more to say? A decade experience in a single-center. Int. J. Surg. 41, S40–S47 (2017).
Salem, F. A., Bergenfelz, A., Nordenström, E. & Almquist, M. Central lymph node dissection and permanent hypoparathyroidism after total thyroidectomy for papillary thyroid cancer: population-based study. Br. J. Surg. 108, 684–690 (2021).
Anastasiou, O. E. et al. Secretory capacity of the parathyroid glands after total thyroidectomy in normocalcemic subjects. J. Clin. Endocrinol. Metab. 97, 2341–2346 (2012).
Orloff, L. A. et al. American thyroid association statement on postoperative hypoparathyroidism: diagnosis, prevention, and management in adults. Thyroid 28, 830–841 (2018).
Kandil, E., Noureldine, S. I., Abbas, A. & Tufano, R. P. The impact of surgical volume on patient outcomes following thyroid surgery. Surgery 154, 1346–1352 (2013). discussion 1352-1343.
Dismukes, J. et al. Prophylactic central neck dissection in papillary thyroid carcinoma: all risks, no reward. J. Surg. Res. 264, 230–235 (2021).
Lee, D. Y. et al. The benefits and risks of prophylactic central neck dissection for papillary thyroid carcinoma: prospective cohort study. Int. J. Endocrinol. 2015, 571480 (2015).
Sippel, R. S. et al. A randomized controlled clinical trial: no clear benefit to prophylactic central neck dissection in patients with clinically node negative papillary thyroid cancer. Ann. Surg. 272, 496–503 (2020).
Sanabria, A., Betancourt, C., Sanchez, J. G. & Garcia, C. Prophylactic central neck lymph node dissection in low-risk thyroid carcinoma patients does not decrease the incidence of locoregional recurrence: a meta-analysis of randomized trials. Ann. Surg. 276, 66–73 (2022).
Ahn, J. H. et al. A prospective randomized controlled trial to assess the efficacy and safety of prophylactic central compartment lymph node dissection in papillary thyroid carcinoma. Surgery 171, 182–189 (2022).
Tuttle, R. M., Haugen, B. & Perrier, N. D. Updated American Joint Committee on cancer/tumor-node-metastasis staging system for differentiated and anaplastic thyroid cancer (Eighth Edition): what changed and why? Thyroid 27, 751–756 (2017).
Sung, H. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71, 209–249 (2021).
Herbst, R. S., Morgensztern, D. & Boshoff, C. The biology and management of non-small cell lung cancer. Nature 553, 446–454 (2018).
Liang, R. B. et al. Incidence and distribution of lobe-specific mediastinal lymph node metastasis in non-small cell lung cancer: data from 4511 resected cases. Ann. Surg. Oncol. 25, 3300–3307 (2018).
Adachi, H. et al. Lobe-specific lymph node dissection as a standard procedure in surgery for non-small cell lung cancer: a propensity score matching study. J. Thorac. Oncol. 12, 85–93 (2017).
Abughararah, T. Z. et al. Lobe-specific lymph node dissection in stage IA non-small-cell lung cancer: a retrospective cohort study. Eur. J. Cardiothorac. Surg. 59, 783–790 (2021).
Wang, Z. et al. Lobe-specific node dissection can be a suitable alternative to systematic lymph node dissection in highly selective early-stage non-small-cell lung cancer patients: a meta-analysis. Ann. Thorac. Cardiovasc. Surg. 27, 143–150 (2021).
Zhao, Y. et al. Lobe-specific lymph node dissection in clinical stage IA solid-dominant non-small-cell lung cancer: a propensity score matching study. Clin. Lung Cancer 22, e201–e210 (2021).
Zhang, Y. et al. Selective mediastinal lymph node dissection strategy for clinical T1N0 invasive lung cancer: a prospective, multicenter, clinical trial. J. Thorac. Oncol. 18, 931–939 (2023).
Ray, M. A., Smeltzer, M. P., Faris, N. R. & Osarogiagbon, R. U. Survival after mediastinal node dissection, systematic sampling, or neither for early stage NSCLC. J. Thorac. Oncol. 15, 1670–1681 (2020).
Yendamuri, S. et al. Effect of the number of lymph nodes examined on the survival of patients with stage I non-small cell lung cancer who undergo sublobar resection. J. Thorac. Cardiovasc. Surg. 156, 394–402 (2018).
Wang, W. et al. Impact of different types of lymphadenectomy combined with different extents of tumor resection on survival outcomes of stage I non-small-cell lung cancer: a large-cohort real-world study. Front. Oncol. 9, 642 (2019).
Huang, W. et al. LobE-Specific lymph node diSsectiON for clinical early-stage non-small cell lung cancer: protocol for a randomised controlled trial (the LESSON trial). BMJ Open 12, e056043 (2022).
Hishida, T. et al. A randomized phase III trial of lobe-specific vs. systematic nodal dissection for clinical stage I-II non-small cell lung cancer (JCOG1413). Jpn. J. Clin. Oncol. 48, 190–194 (2018).
Moncayo, V. M., Alazraki, A. L., Alazraki, N. P. & Aarsvold, J. N. Sentinel lymph node biopsy procedures. Semin. Nucl. Med. 47, 595–617 (2017).
Magnoni, F. et al. Axillary surgery in breast cancer: an updated historical perspective. Semin. Oncol. 47, 341–352 (2020).
Noguchi, M. et al. Axillary surgery for breast cancer: past, present, and future. Breast Cancer 28, 9–15 (2020).
Poulsen, L. et al. Comparison of upper extremity lymphedema after sentinel lymph node biopsy and axillary lymph node dissection: patient-reported outcomes in 3044 patients. Breast Cancer Res. Treat. 191, 87–96 (2021).
Schadendorf, D. et al. Melanoma. Lancet 392, 971–984 (2018).
Banting, S. et al. Negative sentinel lymph node biopsy in patients with melanoma: the patient’s perspective. Ann. Surg. Oncol. 26, 2263–2267 (2019).
van der Ploeg, A. P. et al. Prognosis in patients with sentinel node-positive melanoma without immediate completion lymph node dissection. Br. J. Surg. 99, 1396–1405 (2012).
Faries, M. B. et al. Completion dissection or observation for sentinel-node metastasis in melanoma. N. Engl. J. Med. 376, 2211–2222 (2017).
Lee, D. Y. et al. Impact of completion lymph node dissection on patients with positive sentinel lymph node biopsy in melanoma. J. Am. Coll. Surg. 223, 9–18 (2016).
Satzger, I. et al. Is there a therapeutic benefit of complete lymph node dissection in melanoma patients with low tumor burden in the sentinel node? Melanoma Res. 24, 454–461 (2014).
Susok, L. et al. Waiving subsequent complete lymph node dissection in melanoma patients with positive sentinel lymph node does not result in worse outcome on 20-year analysis. Cancers 13, 5425 (2021).
Bello, D. M. & Faries, M. B. The landmark series: MSLT-1, MSLT-2 and DeCOG (management of lymph nodes). Ann. Surg. Oncol. 27, 15–21 (2020).
Falk Delgado, A., Zommorodi, S. & Falk Delgado, A. Sentinel lymph node biopsy and complete lymph node dissection for melanoma. Curr. Oncol. Rep. 21, 54 (2019).
Garcia-Etienne, C. A. et al. Management of the axilla in patients with breast cancer and positive sentinel lymph node biopsy: An evidence-based update in a European breast center. Eur. J. Surg. Oncol. 46, 15–23 (2020).
Galimberti, V. et al. Axillary dissection versus no axillary dissection in patients with breast cancer and sentinel-node micrometastases (IBCSG 23-01): 10-year follow-up of a randomised, controlled phase 3 trial. Lancet Oncol. 19, 1385–1393 (2018).
Japanese Gastric Cancer, A. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer 24, 1–21 (2021).
Wu, C.-W. et al. Nodal dissection for patients with gastric cancer: a randomised controlled trial. Lancet Oncol. 7, 309–315 (2006).
Cuschieri, A. et al. Patient survival after D1 and D2 resections for gastric cancer: long-term results of the MRC randomized surgical trial. Surgical Co-operative Group. Br. J. Cancer 79, 1522–1530 (1999).
Songun, I., Putter, H., Kranenbarg, E. M.-K., Sasako, M. & van de Velde, C. J. H. Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol. 11, 439–449 (2010).
Symeonidis, D., Diamantis, A., Bompou, E. & Tepetes, K. Current role of lymphadenectomy in gastric cancer surgery. J. BUON 24, 1761–1767 (2019).
Degiuli, M. et al. D2 dissection improves disease-specific survival in advanced gastric cancer patients: 15-year follow-up results of the Italian Gastric Cancer Study Group D1 versus D2 randomised controlled trial. Eur. J. Cancer 150, 10–22 (2021).
Jiang, L. et al. Systematic review and meta-analysis of the effectiveness and safety of extended lymphadenectomy in patients with resectable gastric cancer. Br. J. Surg. 101, 595–604 (2014).
El-Sedfy, A. et al. Personalized surgery for gastric adenocarcinoma: a meta-analysis of D1 versus D2 lymphadenectomy. Ann. Surg. Oncol. 22, 1820–1827 (2015).
Kang, J. H., Ryu, S. Y., Jung, M. R. & Jeong, O. Comparison of long term survival outcomes between D1+ and D2 lymph node dissection for >/= pT2 or pN+ gastric carcinoma: a large scale case-control study using propensity score matching. Eur. J. Surg. Oncol. 46, 1239–1246 (2020).
Yu, P., Du, Y., Xu, Z., Huang, L. & Cheng, X. Comparison of D2 and D2 plus radical surgery for advanced distal gastric cancer: a randomized controlled study. World J. Surg. Oncol. 17, 28 (2019).
Lobo, N. et al. Landmarks in the treatment of muscle-invasive bladder cancer. Nat. Rev. Urol. 14, 565–574 (2017).
D’Andrea, D. et al. Association of super-extended lymphadenectomy at radical cystectomy with perioperative complications and re-hospitalization. World J. Urol. 38, 121–128 (2020).
Gakis, G. Re: extended versus limited lymph node dissection in bladder cancer patients undergoing radical cystectomy: survival results from a prospective, randomized trial. Eur. Urol. 76, 126 (2019).
May, M. et al. Association between the number of dissected lymph nodes during pelvic lymphadenectomy and cancer-specific survival in patients with lymph node-negative urothelial carcinoma of the bladder undergoing radical cystectomy. Ann. Surg. Oncol. 18, 2018–2025 (2011).
Chen, W. S. et al. Novel technique for lymphadenectomy along left recurrent laryngeal nerve during thoracoscopic esophagectomy. World J. Gastroenterol. 26, 1340–1351 (2020).
Saeki, H. et al. "Energy-less technique" with mini-clips for recurrent laryngeal nerve lymph node dissection in prone thoracoscopic esophagectomy for esophageal cancer. Am. J. Surg. 216, 1212–1214 (2018).
Otsuka, K. et al. Minimally invasive esophagectomy and radical lymph node dissection without recurrent laryngeal nerve paralysis. Surg. Endosc. 34, 2749–2757 (2020).
Wijaya, W. A., Peng, J., He, Y., Chen, J. & Cen, Y. Clinical application of axillary reverse mapping in patients with breast cancer: a systematic review and meta-analysis. Breast 53, 189–200 (2020).
Noguchi, M., Inokuchi, M., Yokoi-Noguchi, M. & Morioka, E. The involvement of axillary reverse mapping nodes in patients with clinically node-negative breast cancer. Breast Cancer 29, 209–215 (2022).
Abdelhamid, M. I., Bari, A. A., Farid, M. I. & Nour, H. Evaluation of axillary reverse mapping (ARM) in clinically axillary node negative breast cancer patients - Randomised controlled trial. Int. J. Surg. 75, 174–178 (2020).
Jain, R. & Wairkar, S. Recent developments and clinical applications of surgical glues: an overview. Int. J. Biol. Macromol. 137, 95–106 (2019).
Ruggiero, R. et al. Axillary lymphadenectomy for breast cancer and fibrin glue. Ann. Ital. Chir. 85, 88–92 (2014).
Conversano, A. et al. Use of low-thrombin fibrin sealant glue after axillary lymphadenectomy for breast cancer to reduce hospital length and seroma. Clin. Breast Cancer 17, 293–297 (2017).
Kim, Y. H., Shin, H. J., Ju, W. & Kim, S. C. Prevention of lymphocele by using gelatin-thrombin matrix as a tissue sealant after pelvic lymphadenectomy in patients with gynecologic cancers: a prospective randomized controlled study. J. Gynecol. Oncol. 28, e37 (2017).
McLaughlin, S. A. et al. Considerations for clinicians in the diagnosis, prevention, and treatment of breast cancer-related lymphedema, recommendations from an expert panel: part 2: preventive and therapeutic options. Ann. Surg. Oncol. 24, 2827–2835 (2017).
Lawenda, B. D., Mondry, T. E. & Johnstone, P. A. Lymphedema: a primer on the identification and management of a chronic condition in oncologic treatment. CA Cancer J. Clin. 59, 8–24 (2009).
Lee, H. J. & Kane, C. J. How to minimize lymphoceles and treat clinically symptomatic lymphoceles after radical prostatectomy. Curr. Urol. Rep. 15, 445 (2014).
Liss, M. A. et al. Outcomes and complications of pelvic lymph node dissection during robotic-assisted radical prostatectomy. World J. Urol. 31, 481–488 (2013).
Singh, M., Deo, S. V., Shukla, N. K. & Pandit, A. Chylous fistula after axillary lymph node dissection: incidence, management, and possible cause. Clin. Breast Cancer 11, 320–324 (2011).
Gerken, A. L. H. et al. Definition and severity grading of postoperative lymphatic leakage following inguinal lymph node dissection. Langenbeck’s Arch. Surg. 405, 697–704 (2020).
Sano, Y. et al. Hoarseness after radical surgery with systematic lymph node dissection for primary lung cancer. Eur. J. Cardiothorac. Surg. 55, 280–285 (2019).
Porter, D. L. et al. Chimeric antigen receptor T cells persist and induce sustained remissions in relapsed refractory chronic lymphocytic leukemia. Sci. Transl. Med. 7, 303ra139 (2015).
Leong, S. P., Naxerova, K., Keller, L., Pantel, K. & Witte, M. Molecular mechanisms of cancer metastasis via the lymphatic versus the blood vessels. Clin. Exp. Metastasis 39, 159–179 (2022).
Meadows, K. L. & Hurwitz, H. I. Anti-VEGF therapies in the clinic. Cold Spring Harb. Perspect. Med. 2, a006577 (2012).
Morla, S. Glycosaminoglycans and glycosaminoglycan mimetics in cancer and inflammation. Int. J. Mol. Sci. 20, 1963 (2019).
Van Raemdonck, K., Umar, S. & Shahrara, S. The pathogenic importance of CCL21 and CCR7 in rheumatoid arthritis. Cytokine Growth Factor Rev. 55, 86–93 (2020).
Zhang, L. et al. [Progress in targeting therapy of cancer metastasis by CCL21/CCR7 axis]. Sheng Wu Gong. Cheng Xue Bao 36, 2741–2754 (2020).
Wiley, H. E., Gonzalez, E. B., Maki, W., Wu, M. T. & Hwang, S. T. Expression of CC chemokine receptor-7 and regional lymph node metastasis of B16 murine melanoma. J. Natl Cancer Inst. 93, 1638–1643 (2001).
Bockorny, B. et al. BL-8040, a CXCR4 antagonist, in combination with pembrolizumab and chemotherapy for pancreatic cancer: the COMBAT trial. Nat. Med. 26, 878–885 (2020).
Jones, D., Pereira, E. R. & Padera, T. P. Growth and immune evasion of lymph node metastasis. Front. Oncol. 8, 36 (2018).
Baluk, P. et al. Functionally specialized junctions between endothelial cells of lymphatic vessels. J. Exp. Med. 204, 2349–2362 (2007).
Sun, L., Zhang, H. & Gao, P. Metabolic reprogramming and epigenetic modifications on the path to cancer. Protein Cell 13, 877–919 (2022).
Yang, Y. Cancer immunotherapy: harnessing the immune system to battle cancer. J. Clin. Invest. 125, 3335–3337 (2015).
Goode, E. F., Roussos Torres, E. T. & Irshad, S. Lymph node immune profiles as predictive biomarkers for immune checkpoint inhibitor response. Front. Mol. Biosci. 8, 674558 (2021).
Zhang, Y. & Zhang, Z. The history and advances in cancer immunotherapy: understanding the characteristics of tumor-infiltrating immune cells and their therapeutic implications. Cell Mol. Immunol. 17, 807–821 (2020).
Kennedy, L. B. & Salama, A. K. S. A review of cancer immunotherapy toxicity. CA Cancer J. Clin. 70, 86–104 (2020).
Boyiadzis, M. M. et al. Chimeric antigen receptor (CAR) T therapies for the treatment of hematologic malignancies: clinical perspective and significance. J. Immunother. Cancer 6, 137 (2018).
Maude, S. L. et al. Chimeric antigen receptor T cells for sustained remissions in leukemia. N. Engl. J. Med. 371, 1507–1517 (2014).
Lee, D. W. et al. T cells expressing CD19 chimeric antigen receptors for acute lymphoblastic leukaemia in children and young adults: a phase 1 dose-escalation trial. Lancet 385, 517–528 (2015).
Turtle, C. J. et al. CD19 CAR-T cells of defined CD4+:CD8+ composition in adult B cell ALL patients. J. Clin. Invest. 126, 2123–2138 (2016).
Brentjens, R. J. et al. CD19-targeted T cells rapidly induce molecular remissions in adults with chemotherapy-refractory acute lymphoblastic leukemia. Sci. Transl. Med. 5, 177ra138 (2013).
Davila, M. L. et al. Efficacy and toxicity management of 19-28z CAR T cell therapy in B cell acute lymphoblastic leukemia. Sci. Transl. Med. 6, 224ra225 (2014).
Turtle, C. J. et al. Durable molecular remissions in chronic lymphocytic leukemia treated with CD19-specific chimeric antigen receptor-modified T cells after failure of ibrutinib. J. Clin. Oncol. 35, 3010–3020 (2017).
Porter, D. L., Levine, B. L., Kalos, M., Bagg, A. & June, C. H. Chimeric antigen receptor-modified T cells in chronic lymphoid leukemia. N. Engl. J. Med. 365, 725–733 (2011).
Kochenderfer, J. N. et al. B-cell depletion and remissions of malignancy along with cytokine-associated toxicity in a clinical trial of anti-CD19 chimeric-antigen-receptor-transduced T cells. Blood 119, 2709–2720 (2012).
Kochenderfer, J. N. et al. Chemotherapy-refractory diffuse large B-cell lymphoma and indolent B-cell malignancies can be effectively treated with autologous T cells expressing an anti-CD19 chimeric antigen receptor. J. Clin. Oncol. 33, 540–549 (2015).
Turtle, C. J. et al. Immunotherapy of non-Hodgkin’s lymphoma with a defined ratio of CD8+ and CD4+ CD19-specific chimeric antigen receptor-modified T cells. Sci. Transl. Med. 8, 355ra116 (2016).
Kochenderfer, J. N. et al. Lymphoma remissions caused by anti-CD19 chimeric antigen receptor T cells are associated with high serum interleukin-15 levels. J. Clin. Oncol. 35, 1803–1813 (2017).
Locke, F. L. et al. Phase 1 results of ZUMA-1: a multicenter study of KTE-C19 anti-CD19 CAR T cell therapy in refractory aggressive lymphoma. Mol. Ther. 25, 285–295 (2017).
Kochenderfer, J. N. et al. Long-duration complete remissions of diffuse large B cell lymphoma after anti-CD19 chimeric antigen receptor T cell therapy. Mol. Ther. 25, 2245–2253 (2017).
Ali, S. A. et al. T cells expressing an anti-B-cell maturation antigen chimeric antigen receptor cause remissions of multiple myeloma. Blood 128, 1688–1700 (2016).
Brudno, J. N. et al. T cells genetically modified to express an anti-B-cell maturation antigen chimeric antigen receptor cause remissions of poor-prognosis relapsed multiple myeloma. J. Clin. Oncol. 36, 2267–2280 (2018).
Mikkilineni, L. & Kochenderfer, J. N. Chimeric antigen receptor T-cell therapies for multiple myeloma. Blood 130, 2594–2602 (2017).
Brudno, J. N. & Kochenderfer, J. N. Recent advances in CAR T-cell toxicity: mechanisms, manifestations and management. Blood Rev. 34, 45–55 (2019).
Zou, W. & Chen, L. Inhibitory B7-family molecules in the tumour microenvironment. Nat. Rev. Immunol. 8, 467–477 (2008).
Li, Y. et al. A mini-review for cancer immunotherapy: molecular understanding of PD-1/PD-L1 pathway & translational blockade of immune checkpoints. Int. J. Mol. Sci. 17, 1151 (2016).
Yi, M. et al. Combination strategies with PD-1/PD-L1 blockade: current advances and future directions. Mol. Cancer 21, 28 (2022).
Morse, M. A., Gwin, W. R. 3rd & Mitchell, D. A. Vaccine therapies for cancer: then and now. Target Oncol. 16, 121–152 (2021).
Hollingsworth, R. E. & Jansen, K. Turning the corner on therapeutic cancer vaccines. NPJ Vaccines 4, 7 (2019).
Saxena, M., van der Burg, S. H., Melief, C. J. M. & Bhardwaj, N. Therapeutic cancer vaccines. Nat. Rev. Cancer 21, 360–378 (2021).
Ma, M., Liu, J., Jin, S. & Wang, L. Development of tumour peptide vaccines: from universalization to personalization. Scand. J. Immunol. 91, e12875 (2020).
Obinu, A. et al. Nanoparticles in detection and treatment of lymph node metastases: an update from the point of view of administration routes. Expert Opin. Drug Deliv. 15, 1117–1126 (2018).
Morisaki, T. et al. Lymph nodes as anti-tumor immunotherapeutic tools: intranodal-tumor-specific antigen-pulsed dendritic cell vaccine immunotherapy. Cancers 14, 2438 (2022).
Kipp, J. E. The role of solid nanoparticle technology in the parenteral delivery of poorly water-soluble drugs. Int. J. Pharm. 284, 109–122 (2004).
Zhang, L. et al. Self-assembled lipid-polymer hybrid nanoparticles: a robust drug delivery platform. ACS Nano 2, 1696–1702 (2008).
Whitehead, K. A., Langer, R. & Anderson, D. G. Knocking down barriers: advances in siRNA delivery. Nat. Rev. Drug Discov. 8, 129–138 (2009).
Alexis, F., Pridgen, E., Molnar, L. K. & Farokhzad, O. C. Factors affecting the clearance and biodistribution of polymeric nanoparticles. Mol. Pharm. 5, 505–515 (2008).
Bertrand, N. & Leroux, J. C. The journey of a drug-carrier in the body: an anatomo-physiological perspective. J. Control Release 161, 152–163 (2012).
Bertrand, N., Wu, J., Xu, X., Kamaly, N. & Farokhzad, O. C. Cancer nanotechnology: the impact of passive and active targeting in the era of modern cancer biology. Adv. Drug Deliv. Rev. 66, 2–25 (2014).
Cote, B., Rao, D., Alany, R. G., Kwon, G. S. & Alani, A. W. G. Lymphatic changes in cancer and drug delivery to the lymphatics in solid tumors. Adv. Drug Deliv. Rev. 144, 16–34 (2019).
Nakamura, T. et al. The effect of size and charge of lipid nanoparticles prepared by microfluidic mixing on their lymph node transitivity and distribution. Mol. Pharm. 17, 944–953 (2020).
Shah, S. et al. Nanotechnology based drug delivery systems: Does shape really matter? Int. J. Pharm. 625, 122101 (2022).
Cheng, Z., Que, H., Chen, L., Sun, Q. & Wei, X. Nanomaterial-based drug delivery system targeting lymph nodes. Pharmaceutics 14, 1372 (2022).
McLennan, D. N., Porter, C. J. & Charman, S. A. Subcutaneous drug delivery and the role of the lymphatics. Drug Discov. Today Technol. 2, 89–96 (2005).
Cho, K. J., Cho, Y. E. & Kim, J. Locoregional lymphatic delivery systems using nanoparticles and hydrogels for anticancer immunotherapy. Pharmaceutics 14, 2752 (2022).
Ryan, G. M., Kaminskas, L. M. & Porter, C. J. Nano-chemotherapeutics: maximising lymphatic drug exposure to improve the treatment of lymph-metastatic cancers. J. Control Release 193, 241–256 (2014).
Makino, J. et al. cRGD-installed polymeric micelles loading platinum anticancer drugs enable cooperative treatment against lymph node metastasis. J. Control Release 220, 783–791 (2015).
Singh, N., Handa, M., Singh, V., Kesharwani, P. & Shukla, R. Lymphatic targeting for therapeutic application using nanoparticulate systems. J. Drug Target. 30, 1017–1033 (2022).
Laakkonen, P., Porkka, K., Hoffman, J. A. & Ruoslahti, E. A tumor-homing peptide with a targeting specificity related to lymphatic vessels. Nat. Med. 8, 751–755 (2002).
Song, N. et al. LyP-1-modified multifunctional dendrimers for targeted antitumor and antimetastasis therapy. ACS Appl. Mater. Interfaces 12, 12395–12406 (2020).
Li, F. et al. Evaluation of (99m)Tc-HYNIC-TMTP1 as a tumor-homing imaging agent targeting metastasis with SPECT. Nucl. Med. Biol. 42, 256–262 (2015).
Wei, R. et al. TMTP1-modified indocyanine green-loaded polymeric micelles for targeted imaging of cervical cancer and metastasis sentinel lymph node in vivo. Theranostics 9, 7325–7344 (2019).
Murphy, E. A. et al. Nanoparticle-mediated drug delivery to tumor vasculature suppresses metastasis. Proc. Natl Acad. Sci. USA 105, 9343–9348 (2008).
Lecocq, Q. et al. Theranostics in immuno-oncology using nanobody derivatives. Theranostics 9, 7772–7791 (2019).
Caballero, D. et al. Precision biomaterials in cancer theranostics and modelling. Biomaterials 280, 121299 (2022).
Oh, K. S. et al. Accurate sequential detection of primary tumor and metastatic lymphatics using a temperature-induced phase transition nanoparticulate system. Int. J. Nanomed. 9, 2955–2965 (2014).
Cai, W. et al. Self-assembled hybrid nanocomposites for multimodal imaging-guided photothermal therapy of lymph node metastasis. ACS Appl Mater. Interfaces 12, 49407–49415 (2020).
Huang, X. et al. Long-term multimodal imaging of tumor draining sentinel lymph nodes using mesoporous silica-based nanoprobes. Biomaterials 33, 4370–4378 (2012).
Tseng, Y. C., Xu, Z., Guley, K., Yuan, H. & Huang, L. Lipid-calcium phosphate nanoparticles for delivery to the lymphatic system and SPECT/CT imaging of lymph node metastases. Biomaterials 35, 4688–4698 (2014).
Partridge, S. C., Kurland, B. F., Liu, C. L., Ho, R. J. & Ruddell, A. Tumor-induced lymph node alterations detected by MRI lymphography using gadolinium nanoparticles. Sci. Rep. 5, 15641 (2015).
Spaliviero, M. et al. Detection of lymph node metastases with SERRS nanoparticles. Mol. Imaging Biol. 18, 677–685 (2016).
Tang, L. et al. Aptamer-functionalized, ultra-small, monodisperse silica nanoconjugates for targeted dual-modal imaging of lymph nodes with metastatic tumors. Angew. Chem. 51, 12721–12726 (2012).
Qiao, R. et al. Ultrasensitive in vivo detection of primary gastric tumor and lymphatic metastasis using upconversion nanoparticles. ACS Nano 9, 2120–2129 (2015).
Yang, X. et al. Mapping sentinel lymph node metastasis by dual-probe optical imaging. Theranostics 7, 153–163 (2017).
Xu, G. et al. Long-distance tracing of the lymphatic system with a computed tomography/fluorescence dual-modality nanoprobe for surveying tumor lymphatic metastasis. Bioconjug. Chem. 30, 1199–1209 (2019).
Liu, L. et al. Ultrasmall superparamagnetic nanoparticles targeting E-selectin: synthesis and effects in mice in vitro and in vivo. Int. J. Nanomed. 14, 4517–4528 (2019).
Dai, Y. et al. Metastatic status of sentinel lymph nodes in breast cancer determined with photoacoustic microscopy via dual-targeting nanoparticles. Light Sci. Appl. 9, 164 (2020).
Feng, X., Li, Y., Zhang, S., Li, C. & Tian, J. Quantitative hypoxia mapping using a self-calibrated activatable nanoprobe. J. Nanobiotechnol. 20, 142 (2022).
Han, J., Zhang, L., Cui, M., Su, Y. & He, Y. Rapid and accurate detection of lymph node metastases enabled through fluorescent silicon nanoparticles-based exosome probes. Anal. Chem. 93, 10122–10131 (2021).
Japanese Gastric Cancer, A. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer 20, 1–19 (2017).
Acknowledgements
This work was jointly supported by the National Natural Science Foundation of China (Nos. 82072567) and the Foundation of Shanghai Ninth People’s Hospital (Nos. YBKB202112).
Author information
Authors and Affiliations
Contributions
H.J.: Conceptualization and writing—original draft. C.H.: Conceptualization and writing—reviewing & editing. X.Y.: Writing—reviewing & editing. Y.L.: Visualization. G.J.: Writing—direction. S.G.: Writing—reviewing & direction. X.W.: Supervision, writing—reviewing & direction. M.W.: Supervision, project administration, and funding acquisition. H.J. and C.H. contributed equally to this work.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ji, H., Hu, C., Yang, X. et al. Lymph node metastasis in cancer progression: molecular mechanisms, clinical significance and therapeutic interventions. Sig Transduct Target Ther 8, 367 (2023). https://doi.org/10.1038/s41392-023-01576-4
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41392-023-01576-4
- Springer Nature Limited
This article is cited by
-
Combination of tumor antigen drainage and immune activation to promote a cancer-immunity cycle against glioblastoma
Cellular and Molecular Life Sciences (2024)
-
SPDYC serves as a prognostic biomarker related to lipid metabolism and the immune microenvironment in breast cancer
Immunologic Research (2024)
-
Setting-up a training programme for intraoperative molecular imaging and sentinel node mapping: how to teach? How to learn?
European Journal of Nuclear Medicine and Molecular Imaging (2023)