
Abstract
Indoor air pollution is an environmental health challenge in Kenya, particularly in rural households, and low-income urban areas. This review aims to provide an overview of the sources, health effects and mitigation strategies for indoor air pollutants in Kenya. The main goal of our study was to review existing literature on indoor air pollution in Kenya with the aim of identifying research gaps for future research. Our methodology involved a critical examination of the existing literature review. This is because traditional fuel burning for cooking and heating, and kerosene lamps are major sources of indoor air pollution. Exposure to air pollutants can lead to respiratory and cardiovascular disease among women and children who are more vulnerable. Despite efforts to improve indoor air quality, significant challenges remain including access to clean fuels and technologies, inadequate infrastructure, and low awareness of health impact of indoor air pollution. Mitigation strategies include the transition to cleaner cooking sources, solar lamps for lighting and education campaigns on health impacts. The review concludes that a multifaceted approach involving various stakeholders is necessary to effectively address indoor air pollution in Kenya and improve public health.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
1 Introduction
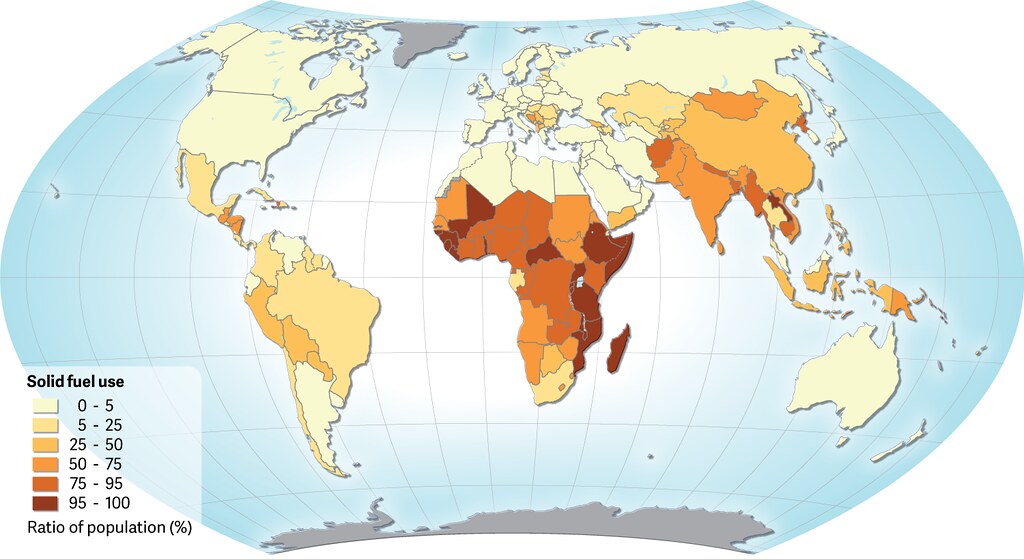
Clean air is essential for good health, globally. It is estimated that over 99% of the global population breathes air that exceeds the World Health Organization (WHO) limits, but worse in low-income countries (Shaddick et al. 2020; WHO 2022a) (Fig. 1a). The United Nations’ Sustainable Development Goals (SDGs) have sought to reduce environmental pollution. SDG 3.9 specifically seeks to ‘reduce the number of deaths and illnesses from hazardous chemicals and air, water and soil pollution and contamination’ by 2030 (UN 2015). In 2020, over 3.2 million people on estimation died from household air pollution (WHO 2022c). In 2012 it was estimated that 4.3 million deaths were associated with indoor air pollution representing a 7.7% mortality rate (Landrigan et al. 2015; Matus et al. 2012; Roser 2021; Samet et al. 2016). Indoor air pollution is caused by a variety of factors including the burning of fuels for cooking and heating (Jung and Huxham 2018; Rafiq et al. 2022) as well as clearing land for farming. These fuels release harmful pollutants such as carbon monoxide, particulate matter (PM) (combination of tiny particles of dust, solids and soot present in the atmosphere), and volatile organic compounds (VOCs) (Fig. 1b, c) into the air which can cause respiratory and other health problems such as cancer, negative pregnancies outcomes, infertility, cardiovascular diseases, stroke, and cognitive decline (Checa Vizcaíno et al. 2016; Jacobs et al. 2017; Khreis et al. 2017; Liu et al. 2018; Mokoena et al. 2019; Power et al. 2016).

Source: https://farm1.staticflickr.com/491/31513651944_6acb986a41_b.jpg. Source: https://airqualitynews.com/wp-content/uploads/2019/03/Mukuru-street-scene-Photo-credit-Dennis-Waweru-1024x683.jpg. Source: https://energypedia.info/images/thumb/6/6f/GIZ-Feldmann-Malawi-3-stone-fire.jpg/1280px-GIZ-Feldmann-Malawi-3-stone-fire.jpg
a Global solid fuel use, b indoor air pollution from a food vendor in Nairobi, c three-stone fireplace.
Particulate matter is a major source of air pollution in Kenya which is generated from the traffic, burning fossil fuels for lighting and transportation, chemicals in mines, burning garbage in open areas, burning forests and fields, and using indoor stoves (Kinney et al. 2011; Mbandi et al. 2019; van Vliet and Kinney 2007). A study done by deSouza (2020a) indicates that the entire Kenyan population lives in areas with greater particulate matter (PM2.5) which exceeds the recommended WHO air guidelines of 10 µm/m3. In developing countries, 2.5 billion people cook using biomass which has been hastened further by rapid urbanization (Gouda et al. 2019; Hanna et al. 2016; IEA 2006; Kirago et al. 2022; Lelieveld et al. 2001; Philibert 2022; Pratiti 2021; Vichit-Vadakan et al. 2008). Biomass from wood is the most significant energy from primary source consumption contributing to 74% of the country’s entire primary energy supply (Kiplagat et al. 2011; KNBS 2023; Okoko et al. 2017; Welfle et al. 2020). The rural areas use biomass approximately 86 and 21% of the urban population use wood stoves as the primary source of fuels (Ministry of Energy 2019) (Fig. 2). The emissions produced from the burning of solid fuels lead to indoor pollution, with the urban dwellers experiencing Indoor Air Pollution (IAP) being those in the slums or low-cost housing. According to the State of the Global Air Report, IAP led to approximately 23,000 deaths in 2020 ranking it the eighth cause of premature deaths in Kenya (Ministry of Energy 2019).

Cooking and heating source in rural and urban areas in Kenya. Source: (Ministry of Energy 2019)
Approximately, 90% of the global population spend most of their time indoors exposing themselves to IAP and HAP (LEECH et al. 2002; Nardocci et al. 2023; Nazaroff and Goldstein 2015) with characteristics such as building type and ventilation playing a greater role (Ferguson et al. 2020). Despite various initiatives put in place by both governments and NGOs, uptake is still low and still calls for efforts ranging from awareness and socio-economic empowerment to promote the use of clean energy. Kenya, like many other developing countries, has limited air quality monitoring programs and related studies are scanty. This review examines indoor pollution in Kenya including its causes, effects on human health, and potential solutions. By understanding the impact of indoor air pollution in Kenya, we can work towards finding effective ways to reduce exposure and improve the health and well-being of the Kenyan population as well as developing nations. The criticality of this paper is to provide relevant literature on the forms of indoor air pollution which builds up knowledge for future research by providing a basis buildup for a detailed quality experimental study on the field. This literature identifies the existing gaps to fill in actual studies in the discipline of indoor air pollution.
2 Methodology
2.1 Methods Used in Collecting Indoor Air Pollution Literature
This review paper aimed to assess the current state of knowledge on indoor air pollution and its morbidity. To achieve this, a systematic review of relevant literature was conducted which was in line with the defined question “What is the current state of indoor air pollution and its impact on human health in Kenya?”. The inclusion and exclusion criteria while choosing the articles from the previous journals, government reports and policy papers as well as data from external bodies such as WHO related to indoor air pollution, refined further to studies published between 2010 and 2023. Based on our review of the mentioned databases, we ran such queries related to our study with keywords such as “indoor air pollution”, and “health impact on indoor air pollution”. These enabled us to find the available research articles which had undergone peer reviews from Google Scholar, Web of Science, Science Direct, and PubMed. The total number of journal articles was 177, government policy papers and government reports were 19 (Fig. 3).

Source: Web of Science
Distribution of published articles within the scope of our study as per the various scientific disciplines.
The identified papers were further screened to those relevant to the study area from the full texts’ journals and web search with 28 being relevant to the study (Fig. 4). The data of interest extracted in the refined study included the methodology (Fig. 5) used in getting the data, study population, exposure assessment, indoor air quality monitoring and evaluation, health outcomes, and findings from the studies discussed in the results section.

Source: Web of Science
Distribution of published articles within the selected years of our study.

Source: Authors design, 2023
Diagrammatic flow of the methods used in assessing air pollution.
The details obtained from the study were classified into tables and how the data was collected was added which would help in identifying the challenges and the roles in which the data on indoor air pollution can be collected using. The use of household surveys appeared to be the most common with the use of remote sensing least used in the study for studying indoor air pollution.
3 Results and Discussion
3.1 Air Quality and Monitoring (Comparison Between WHO and Kenyan Standards)
Air quality is an important aspect of building design and maintenance. Indoor air quality can be affected by factors ranging from inadequate ventilation, the use of certain chemicals and products, and outdoor air pollution. Evaluating indoor air pollution is essential to identify and control common pollutants that can lead to indoor health concerns. Indoor air quality evaluations can help determine the presence and concentration of indoor pollutants such as particulate matter (PM), volatile organic compounds (VOCs) and mold which can help in the informed decisions about building designs, ventilation, and maintenance practice. Evaluating indoor air quality helps identify potential health risks and take appropriate steps to mitigate them which can help improve the occupant’s perception of the indoor environment which can have a significant impact on their comfort and well-being. As for now, the Kenya has not developed the guidelines on the IAP but relies on the World Health Organization guidelines.
3.2 Indoor Air Pollution Studies and Performance Comparison
Smoke stratification is one of the major contributors to indoor air pollution since the small particulate matter rise (less dense) from the region with high temperature (fire) until they reach a level where there is no longer a temperature difference with surrounding. Temperature plays a critical role in the formation and severity of smoke stratification a study done by Zeng et al. (2018) for longitudinal fires concluded that the temperature ratio proposed by Newman on “stratification velocity” was feasible. It hypothesized that temperature has an impact on smoke stratification contributing to indoor air pollution in poorly ventilated houses. According to a study done by Haggerty et al. (2020) on ventilation in rural homes using thermocouples and 80-Watt heat sources in open and closed wind scenarios. The results showed an average of 4.8 °C temperature differentials being observed in open scenarios than closed concluding that natural ventilation does not necessarily improve air quality.
The demand for solid fuels in Kenya surpasses the supply resulting in forest cover changes (Mutuku 2022; Oduor et al. 2020). Traditional fuels are still common in rural and urban households in Kenya with incomplete combustion generating polycyclic aromatic hydrocarbons (PAHs) (Gachanja and Maritim 2018). Adeola et al. (2022) did a study in Bomet and Narok counties on the PAHs contribution from the fuels type, combustion device, climate, and nature of households with results showing the having concentration of 0.82–173.69 µg/m3) with three-stone and burning of wood having higher PAH emissions, while charcoal burning jiko (meaning a traditional ceramic cooking stove) had higher toxic equivalence quotient, which is dangerous and need of having safe stoves. Johnson et al. (2021) used single-zone modeling, indirect exposure models, and area-level measurements in estimating exposure to cooking fuel combustion and its contribution to household air pollution. The study measured emissions and personal exposure to PM2.5 and black Carbon from cooking stoves, behavioral, socio-economic, and household characteristics i.e., kitchen size and ventilation. Using the single model with kitchen concentration lacked precision by showing a correlation of R2 = 0.45 for PM2.5 and CO, regression model had R2 = 0.76 and RMSE of 85 µg/m3 while the survey-only regression model predicted an R2 = 0.51 on PM2.5 exposure.
The efficiency of Traditional Cookstoves (TCS) was estimated to be between 5 and 15% while the ICS has increased efficiency such as Kenya Ceramic jiko is 30–40%. The studies done on the reduction of emission from the ICS shows a potential of up to 80% (Yip et al. 2017). Lung and Espira (2019) compared the effectiveness of modified traditional kitchens for 7 years in Western Kenya. The mean household wood consumption was 0.70 kg/day using a three-stone fire, but with the introduction of ICS the daily household consumption dropped to 0.47 kg/day relating to about 37.7% exposure reduction and mean savings. Pilishvili et al. (2016) found that using the ICS compared to TSF reduced the PM2.5 by about 11.9–42.3%, which ranged between 319 to 518 µg/m3, the CO reduced from − 5.8 to 34.5%. Munyao et al. (2022) did a comparative study with population size 383 on the TCS and ICS in estimating the emissions with findings having 1.5 and 1.3 kg/day for ICS i.e., Cheprocket and mud-rocket stoves, respectively, compared to traditional three-stone stoves. Pyrolytic stoves help in carbon sequestration and are efficient to use. According to a study by Mahmoud et al. (2021) who used 150 households between 2013 and 2019 on smoke exposure from biochar production found that the technology is feasible in reducing the IAP and had high efficiency. The use of solar lamps in replacing kerosene lamps reduces exposure to indoor pollutants. Lam et al. (2018) evaluated 20 households in Busia County where they used the kerosene lamps and the exposure in which the pupils were exposed before and after the provision of 3 solar lamps. Averagely, the 48-h exposure dropped from 210 to 104 µg/m3 representing about 50% decline among adults and 132 to 35 µg/m3 among the pupils.
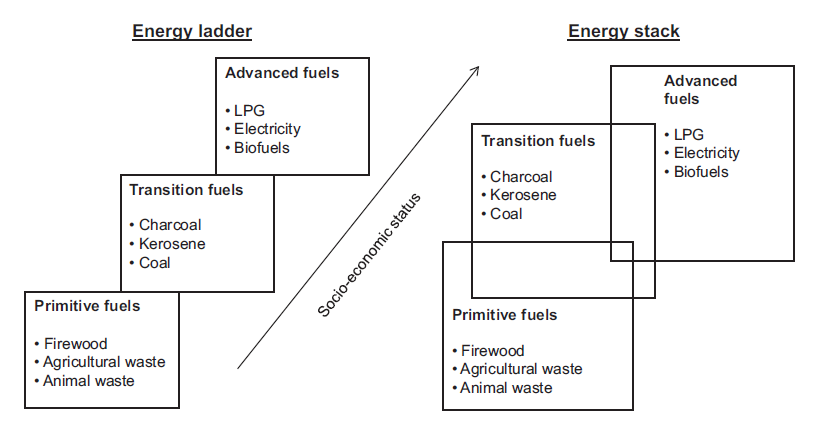
The reliability of fuel in most parts of the country still lack in Kenya which is mostly contributed during the seasons and perception of food tastes leading to fuel stacking, a phenomenon in which multiple fuels sources are utilized for cooking (Ochieng et al. 2020). Most households use different fuel combinations like firewood for cooking and charcoal used for both cooking and heating. Fuel stacking is driven by various factors such as income, access to energy infrastructure, cooking practices, and cultural preferences (Clemens et al. 2018; Yonemitsu et al. 2015) as seen in Fig. 5. Even though stacking helps in meeting households’ energy needs, it leads to emissions of toxic ultra-fine particles from woodsmoke (Wagner et al. 2022). Musyoka and Muindi (2022) studied 42 households stacking future and exposure of the gases produced with results showing that daily averaged concentrations in using wood using households having PM2.5 and PM10 had 268.80 and 623 µg/m3, while the Liquefied Petroleum Gas (LPG) had PM2.5 and PM10 53.6 and 168 µg/m3. Ang’u et al. (2022) quantified the emission produced from biomass stoves, kerosene stoves, ceramic, and saw dust jiko. The average PM2.5 concentrations were: three stone—481.2 µg/m3, chepkube—304.3 µg/m3, ceramic jiko—162.4 µg/m3, sawdust jiko—273.1 µg/m3, and kerosene stove—80.2 µg/m3 (Fig. 6).

Energy ladder. Source: https://energypedia.info/images/5/5a/The_Energy_Ladder_%28Paunio%2C_2018%29_03.PNG
Global cities are greatly affected by IAP due to emissions from vehicles and cooking fuels in low-income households (slums) majority with poor ventilation. A study done in 12 cities by Kumar et al. (2022) factored in fuel type used, kitchen volume, ventilation, and cooking time. From the findings, Nairobi residents spend more than 40% of cooking time with charcoal being the main fuel type. The study recommended increasing awareness to improve cooking practices and minimize occupancy in the kitchen to reduce emissions. Combining the effects of outdoor and indoor air pollution makes city dwellers more prone to health-related issues due to exhaust from motor vehicles. Singh et al. (2021) aimed at creating awareness through repeated static and dynamic monitoring in a range of urban locations in cities in Kenya, Uganda, and Tanzania. From the findings, Nairobi and Kampala had higher concentrations but did not fully explore the link between the emissions impact to the houses located nearby the roads. Mutahi et al. (2021) did a study on indoor and outdoor air quality in informal urban and rural settlements in Ng'ando and Leshau. The sampling was done using gravimetrical, elemental composition, and black carbon analysis of PM2.5 with findings having up to 1000 µg/m3. The results exceeded the recommended WHO limits with children and women who are exposed to more than 12 h/day affected.
3.3 Health Statistics
Indoor air pollution is a significant health concern that contributes majorly to premature deaths due to emissions of particulate matter. It is reported that the mortality rate from indoor air pollution has greatly risen from 60/100,000 persons in 2012 to 78/100,000 persons in 2016.
3.4 Eye Infections and Headaches
Biomass and solid fuels lead to rise of IAP causing headaches and eye problems. Dida et al. (2022) established from sampled population that over 92.8% had eyesight related problems related to IAP. 87% reported to have watery eyes, 72.1% with eye irritation, and 43.3% with red eyes while 11% reported other eye problems. 98% recorded to have experienced headaches in the year, with 34.6% having persistent headaches. 28% had it weekly while 2% had it daily. studies also show that cooking using stoves and lighting caused some eye problems with some reporting that tears coming out from eyes and itching of eyes, sleeping problems, partial blindness from cataracts, trachoma and conjunctivitis caused by IAP (Ezzati et al. 2000; Rana et al. 2019).
3.5 ALRI
Dida et al. (2022) on the coughing on vulnerable population established that 92% had coughs varying for 12-month period, 45.9% had persistent cough, 30.3% persistently coughed for 1–2 months, 33.2% reported coughing persistently in for a period of 2 years. Most of the children had coughing associated with kitchen condition (Exact chi = 7.11, p = 0.02). About 95.4% had cough in the previous week with 51.2% of coughs associated with increased rate of breathing. The other related challenges experienced include burns (42%), drowsiness (8%) and asthma related problems 2%. 31.5% had wheezing, 79.8% wheezed during the cold seasons, 35% had chest congestion in the past 2 years, 24.4% during the previous year, 21.2% in five years. 62.5% produced sputum. Sputum production was significantly associated with house type (exact chi = 7.29, p = 0.03). Ezzati and Kammen (2001) study in Laikipia showed the relationship and how it is associated with lower respiratory tract. The relationship between higher particulate levels had higher rates of respiratory illness. Ng’ang’a Gicheru (2021) studied IAPs exposure on children found that 2–59 months at Kenyatta National Hospital (KNH) on the Pneumonia prevalence from 127 respondents. He established that the relationship between the high levels of IAP were greatly significant with poor response to Pneumonia treatment with an odds ratio of 1.49, 95% confidence interval of 1.02 to 2.21 and p value of 0.0406. Raufman et al. (2020) did a study on environmental health literacy (EHL) from household air pollution (HAP) aimed at reducing health risks from residents of Kasarani. Baseline characteristics compared included the cough, shortness of breathing and phlegm production. 28% reported one or more symptoms at least 5 times a month, including 31.2% of solid fuel users. Majdan et al. (2015) assessed respiratory illness caused by IAP in 125 rural homes using questionnaires and spirometers in Kwale district. The findings showed that the WHO levels had been exceeded and there was relatively high respiratory illness with spirometers showing 80% of the inhabitants had lung issues.
3.6 COPD and IHD
The relationship between the exposure of IAP with LRI, COPD and lung cancer; studies show some correlation (Kurmi et al. 2012). Agarwal et al. (2018) found a high possibility of cardiac dysfunction from increased exposure to household air pollution. Further, Ang’u et al. (2022) modeled Acute Lower Respiratory Infections (ALRI), COPD, IHD, and lung cancer using AirQ + and found that there were approximately 484 mortality cases in Vihiga from IAP. Ortega et al. (2021) research on the impact of the replacement of kerosene lighting to renewables estimated that the transition could reduce the deaths and disability-adjusted life years (DALYs) (Fig. 7). It was estimated that carbon emissions would reduce by 4.4 Gg/year of 3957 CO2 in East Africa if the full transition of kerosene-based lamps to electricity is successful.

Indoor air pollution attributed to disease disability-adjusted life years (DALYs).
Comparing the deaths caused by IAP in Kenya, it is evident that nearly equal ratios which goes against the hypothetical gender influence on exposure. Women are mostly exposed but considering that most deaths recorded due to lower respiratory illness occur in children below 5 years old, the population is approximately equal. Calculating the burden of diseases, most of the “adult” disease conditions such as IHD and COPD are more common in men than in women and thus net results nearly become equal, notwithstanding the IAP exposure in women (Ministry of Health 2021).
3.7 Groups with Higher Exposure
The exposure to IAP concentrations varies with cooking stoves having over 20,000 µg/m3 (Saksena et al. 1992) predisposing more women and children to these levels. Juntarawijit and Juntarawijit (2019) did a study and found that cooking frequency which predisposed more women to IAP with 10 weekly exposures could increase the risk of coughing, wheezing, sore throats, and breath shortness. The socio-economic exposure is a challenge in Kenya with a study done by Dida et al. (2022) showing that over 66% of the households studied, children slept in the kitchen. Poor people from lower socio-economic status and refuges lack access to clean energy and are more likely to use the traditional fuels exposing them greatly (Elbayoumi and Albelbeisi 2023; Masekela and Vanker 2020). Elderly individuals may be more vulnerable to the negative effects of indoor air pollution due to their weakened immune systems and pre-existing health conditions, while children are more susceptible due to their still-developing lungs and breathing rates (Bentayeb et al. 2013; Simoni et al. 2003). Women, kitchen helpers in institutions (hospitals, schools, etc.), and children may spend more time indoors and thus have higher exposure to indoor air pollution (Rylance et al. 2019). Pregnant women are also at greater risk which can lead to pre-term birth, low birth weight, stillbirth, or congenital abnormalities (Pope et al. 2010; Stankovic et al. 2011). People with weakened immunities from diseases such as chronic illness and HIV are more susceptible to illness caused by IAP since their bodies cannot fight off germs and sickness as effectively (Kim et al. 2018; Suter et al. 2018). The WHO Air Quality Guidelines values such as the annual guideline for PM2.5 of 10 µg/m3 and the 24-h guideline for CO of 7 mg/ml, consider scientific evidence on health risks among susceptible populations.
3.8 Plans and Interventions in Combating Indoor Air Pollution
Indoor pollution is still a challenging problem in rural areas where dependence on traditional solid fuels is still sought for. However, plans have been set to try to regulate the spread of use. The promotion of the use of clean fuels through shifting to cleaner fuels such as LPG, biogas, or electricity is projected to reduce IAP. To achieve this program, the government and other stakeholders have tried to offer subsidies, education campaigns, and partnerships with companies (van den Berg 2018; KNA 2022; Pilishvili et al. 2016; Shilenje et al. 2022; SNV 2023). The Indoor Air Quality Roadmap 2022–2030 plan which is being supported by WHO serves as a reference for planning, implementing, monitoring, and evaluating policies, and strategies for indoor air quality (WHO 2022b). The rural community is mostly affected health-wise greatly which prompted the Ministry of Health to develop a document dubbed “Lets Act Together to Save Lives” outlining procedures that would guide the communities and health workers on the prevention control of indoor air pollutants responsible for cardiovascular, cancer and respiratory diseases (Ministry of Health 2021). In addressing the issues on IAP, the researchers interested in improving monitoring and research will help in identifying sources and extent of pollution and help in informing policy decisions and interventions to address the problem which led to the formation of Kenya Air Quality Network (deSouza 2020b; NEMA 2020). According to the National Roadmap on Indoor Air Quality 2022–2023, the plan simulates a well-detailed plan on how to handle the challenge on IAP, but the implementation has not been fully initiated.
3.9 Challenges Experienced in Curbing Indoor Air Pollution
Despite the huge potential of reducing the IAP, Kenya still faces an impact in the transition due to over-dependence on traditional fuel. The need to have a consistent and reliable source of fuel has been marred by the entrance of invasive weeds. A study by Rotich et al. (2021) shows the biomethane potential of invasive weeds which can help in reducing the dependence on traditional fuel. There have always been plans and measures of shifting to clean energy sources such as solar and wind to reduce emissions, but socio-economic and cultural differences have hindered the move. The cultural differences have led to more fuel stacking in some potential families because they believe that there are foods that cannot be prepared over LPG such as githeri (cooked mixture of maize/corn and beans). Other challenges influencing the spread of clean cooking technologies are economic status (most people live in a hand-to-mouth situation), fuel accessibility, affordability, and lack of knowledge on how to handle it. The perception among some demographic ages with the old wish to use traditional fuels since it is easy to use compared to the LPGs. In some places where the guidelines and standards have been set such as Net Zero Energy Buildings and ventilation being incorporated in the building code, the implementation becomes a challenge in enforcing since most houses are not properly planned to leave out the IAP, and a significant percentage of the population are unaware of IAP. To achieve a safe transition, the government needs to prioritize increasing finances to help in the affordability of clean cooking technologies, create mass awareness on the proper ventilation and increase educational levels on research and development in aiming at reducing IAP and achieving SDGs.
4 Conclusion
In conclusion, we found that indoor air pollution is still a significant health concern in Kenya with 99% of total population affected. In the energy matrix, woody biomass constitutes 68%, with 80% of the population relying on charcoal and firewood for cooking and heating. Nationally, 65% of the total Kenyan population use wood stove, with 86 and 21% being in rural and urban areas, respectively. The combustion of these fuels releases harmful pollutants such as carbon monoxide, particulate matter, and nitrogen oxides, which can lead to a range of health problems, including respiratory infections, cardiovascular disease, and cancer. Based on the Ministry of Health, it is recorded that over 23,000 Kenyans die annually due to indoor air pollution. Studies in Kenya have shown that indoor air pollution disproportionately affects women and children, who spend more time in the home and are, therefore, exposed to higher levels of pollutants. In addition, poor ventilation exacerbates the problem by trapping pollutants indoors. To address indoor air pollution in Kenya, a multifaceted approach is necessary, including promoting the use of cleaner cooking fuels and stoves, improving ventilation in homes, and raising public awareness about the health risks associated with indoor air pollution. With concerted efforts from policymakers, health professionals, and the public, it is possible to reduce the impact of indoor air pollution on the health and well-being of Kenyan communities. Our future research will embark on creating awareness in the population who have little or minimal knowledge of the effects of indoor air pollution on their health and help reformulate existing policies for better health of the Kenyan population.
References
Adeola AO, Nsibande SA, Osano AM, Maghanga JK, Naudé Y, Forbes PBC (2022) Analysis of gaseous polycyclic aromatic hydrocarbon emissions from cooking devices in selected rural and urban kitchens in Bomet and Narok counties of Kenya. Environ Monit Assess 194(6):435. https://doi.org/10.1007/s10661-022-10062-3
Agarwal A, Kirwa K, Eliot MN, Alenezi F, Menya D, Mitter SS, Velazquez EJ, Vedanthan R, Wellenius GA, Bloomfield GS (2018) Household air pollution is associated with altered cardiac function among women in Kenya. Am J Respir Crit Care Med 197(7):958–961. https://doi.org/10.1164/rccm.201704-0832LE
Ang’u C, Muthama NJ, Mutuku MA, M’IKiugu MH (2022) Household air pollution and its impact on human health: the case of Vihiga County, Kenya. Air Qual Atmos Health 15(12):2255–2268. https://doi.org/10.1007/s11869-022-01249-1
Bentayeb M, Simoni M, Norback D, Baldacci S, Maio S, Viegi G, Annesi-Maesano I (2013) Indoor air pollution and respiratory health in the elderly. J Environ Sci Health Part A 48(14):1783–1789. https://doi.org/10.1080/10934529.2013.826052
Checa Vizcaíno MA, González-Comadran M, Jacquemin B (2016) Outdoor air pollution and human infertility: a systematic review. Fertil Steril 106(4):897-904.e1. https://doi.org/10.1016/j.fertnstert.2016.07.1110
Clemens H, Bailis R, Nyambane A, Ndung’u V (2018) Africa Biogas Partnership Program: a review of clean cooking implementation through market development in East Africa. Energy Sustain Dev 46:23–31. https://doi.org/10.1016/j.esd.2018.05.012
deSouza P (2020a) Air pollution in Kenya: a review. Air Qual Atmos Health 13(12):1487–1495. https://doi.org/10.1007/s11869-020-00902-x
deSouza P (2020b) Nairobi’s air has been polluted for decades: new review suggests a path forward. The Conversation
Dida GO, Lutta PO, Abuom PO, Mestrovic T, Anyona DN (2022) Factors predisposing women and children to indoor air pollution in rural villages, Western Kenya. Arch Public Health 80(1):46. https://doi.org/10.1186/s13690-022-00791-9
Elbayoumi M, Albelbeisi AH (2023) Biomass use and its health effects among the vulnerable and marginalized refugee families in the Gaza Strip. Front Public Health. https://doi.org/10.3389/fpubh.2023.1129985
Ezzati M, Kammen DM (2001) Indoor air pollution from biomass combustion and acute respiratory infections in Kenya: an exposure-response study. Lancet 358(9282):619–624. https://doi.org/10.1016/S0140-6736(01)05777-4
Ezzati M, Saleh H, Kammen DM (2000) The contributions of emissions and spatial microenvironments to exposure to indoor air pollution from biomass combustion in Kenya. Environ Health Perspect 108(9):833–839. https://doi.org/10.1289/ehp.00108833
Ferguson L, Taylor J, Davies M, Shrubsole C, Symonds P, Dimitroulopoulou S (2020) Exposure to indoor air pollution across socio-economic groups in high-income countries: a scoping review of the literature and a modelling methodology. Environ Int 143:105748. https://doi.org/10.1016/j.envint.2020.105748
Gachanja AN, Maritim PK (2018) Polycyclic aromatic hydrocarbons-determination. Reference module in chemistry, molecular sciences and chemical engineering. Elsevier, Amsterdam. https://doi.org/10.1016/B978-0-12-409547-2.14107-1
Gouda HN, Charlson F, Sorsdahl K, Ahmadzada S, Ferrari AJ, Erskine H, Leung J, Santamauro D, Lund C, Aminde LN, Mayosi BM, Kengne AP, Harris M, Achoki T, Wiysonge CS, Stein DJ, Whiteford H (2019) Burden of non-communicable diseases in sub-Saharan Africa, 1990–2017: results from the Global Burden of Disease Study 2017. Lancet Glob Health 7(10):e1375–e1387. https://doi.org/10.1016/S2214-109X(19)30374-2
Haggerty L, Reischl U, Handy RG, Sleeth DK, Adams K, Schaefer C (2020) The thermodynamics of indoor air pollution: a pilot study emulating traditional Kenyan homesteads. Sustain Cities Soc 53:101926. https://doi.org/10.1016/j.scs.2019.101926
Hanna R, Duflo E, Greenstone M (2016) Up in smoke: the influence of household behavior on the long-run impact of improved cooking stoves. Am Econ J Econ Pol 8(1):80–114. https://doi.org/10.1257/pol.20140008
IEA (2006) Energy for cooking in developing countries. OECD, pp 419–445. https://doi.org/10.1787/weo-2006-16-en
Jacobs M, Zhang G, Chen S, Mullins B, Bell M, Jin L, Guo Y, Huxley R, Pereira G (2017) The association between ambient air pollution and selected adverse pregnancy outcomes in China: a systematic review. Sci Total Environ 579:1179–1192. https://doi.org/10.1016/j.scitotenv.2016.11.100
Johnson M, Piedrahita R, Pillarisetti A, Shupler M, Menya D, Rossanese M, Delapeña S, Penumetcha N, Chartier R, Puzzolo E, Pope D (2021) Modeling approaches and performance for estimating personal exposure to household air pollution: a case study in Kenya. Indoor Air 31(5):1441–1457. https://doi.org/10.1111/ina.12790
Jung J, Huxham M (2018) Firewood usage and indoor air pollution from traditional cooking fires in Gazi Bay, Kenya. Biosci Horiz Int J Stud Res. https://doi.org/10.1093/biohorizons/hzy014
Juntarawijit Y, Juntarawijit C (2019) Cooking smoke exposure and respiratory symptoms among those responsible for household cooking: a study in Phitsanulok, Thailand. Heliyon 5(5):e01706. https://doi.org/10.1016/j.heliyon.2019.e01706
Khreis H, Kelly C, Tate J, Parslow R, Lucas K, Nieuwenhuijsen M (2017) Exposure to traffic-related air pollution and risk of development of childhood asthma: a systematic review and meta-analysis. Environ Int 100:1–31. https://doi.org/10.1016/j.envint.2016.11.012
Kim C, Jary H, Mortimer K, Schweitzer KS, Curran-Everett D, Gordon S, Petrache I (2018) Effects of household air pollution in malawi and human immunodeficiency virus status on respiratory symptoms and inflammation, injury, and repair markers. Ann Am Thorac Soc 15(Supplement_2):S132–S133. https://doi.org/10.1513/AnnalsATS.201707-614MG
Kinney PL, Gichuru MG, Volavka-Close N, Ngo N, Ndiba PK, Law A, Gachanja A, Gaita SM, Chillrud SN, Sclar E (2011) Traffic impacts on PM2.5 air quality in Nairobi, Kenya. Environ Sci Policy 14(4):369–378. https://doi.org/10.1016/j.envsci.2011.02.005
Kiplagat JK, Wang RZ, Li TX (2011) Renewable energy in Kenya: resource potential and status of exploitation. Renew Sustain Energy Rev 15(6):2960–2973. https://doi.org/10.1016/j.rser.2011.03.023
Kirago L, Gatari MJ, Gustafsson Ö, Andersson A (2022) Black carbon emissions from traffic contribute substantially to air pollution in Nairobi, Kenya. Commun Earth Environ 3(1):74. https://doi.org/10.1038/s43247-022-00400-1
KNA (2022) 60,000 gas cylinders to benefit low-income households. Kenya News Agency. https://www.kenyanews.go.ke/60000-cylinders-to-benefit-low-income-households/
KNBS (2023) Demographic and health survey 2022 key indicators Report. http://www.DHSprogram.com
Kumar P, Hama S, Abbass RA, Nogueira T, Brand VS, Wu H-W, Abulude FO, Adelodun AA, Anand P, Andrade MDF, Apondo W, Asfaw A, Aziz KH, Cao S-J, El-Gendy A, Indu G, Kehbila AG, Ketzel M, Khare M et al (2022) In-kitchen aerosol exposure in twelve cities across the globe. Environ Int 162:107155. https://doi.org/10.1016/j.envint.2022.107155
Kurmi OP, Lam KBH, Ayres JG (2012) Indoor air pollution and the lung in low- and medium-income countries. Eur Respir J 40(1):239–254. https://doi.org/10.1183/09031936.00190211
Lam NL, Muhwezi G, Isabirye F, Harrison K, Ruiz-Mercado I, Amukoye E, Mokaya T, Wambua M, Bates MN (2018) Exposure reductions associated with introduction of solar lamps to kerosene lamp-using households in Busia County, Kenya. Indoor Air 28(2):218–227. https://doi.org/10.1111/ina.12433
Landrigan PJ, Fuller R, Horton R (2015) Environmental pollution, health, and development: a Lancet-Global Alliance on Health and Pollution-Icahn School of Medicine at Mount Sinai Commission. Lancet 386(10002):1429–1431. https://doi.org/10.1016/S0140-6736(15)00426-2
Leech JA, Nelson WC, Burnett RT, Aaron S, Raizenne ME (2002) It’s about time: a comparison of Canadian and American time–activity patterns. J Eposure Sci Environ Epidemiol 12(6):427–432. https://doi.org/10.1038/sj.jea.7500244
Lelieveld J, Crutzen PJ, Ramanathan V, Andreae MO, Brenninkmeijer CAM, Campos T, Cass GR, Dickerson RR, Fischer H, de Gouw JA, Hansel A, Jefferson A, Kley D, de Laat ATJ, Lal S, Lawrence MG, Lobert JM, Mayol-Bracero OL, Mitra AP et al (2001) The Indian Ocean experiment: widespread air pollution from South and Southeast Asia. Science 291(5506):1031–1036. https://doi.org/10.1126/science.1057103
Liu W, Xu Z, Yang T (2018) Health effects of air pollution in china. Int J Environ Res Public Health. https://doi.org/10.3390/ijerph15071471
Lung MA, Espira A (2019) A large-scale, village-level test of wood consumption patterns in a modified traditional cook stove in Kenya. Energy Sustain Dev 49:11–20. https://doi.org/10.1016/j.esd.2018.12.004
Mahmoud Y, Njenga M, Sundberg C, Roing de Nowina K (2021) Soils, sinks, and smallholder farmers: examining the benefits of biochar energy transitions in Kenya. Energy Res Soc Sci 75:102033. https://doi.org/10.1016/j.erss.2021.102033
Majdan M, Svaro M, Bodo J, Taylor M, Muendo R (2015) Assessment of the biomass related indoor air pollution in Kwale district in Kenya using short term monitoring. Afr Health Sci 15(3):972. https://doi.org/10.4314/ahs.v15i3.35
Masekela R, Vanker A (2020) Lung health in children in Sub-Saharan Africa: addressing the need for cleaner air. Int J Environ Res Public Health 17(17):6178. https://doi.org/10.3390/ijerph17176178
Matus K, Nam K-M, Selin NE, Lamsal LN, Reilly JM, Paltsev S (2012) Health damages from air pollution in China. Glob Environ Change 22(1):55–66. https://doi.org/10.1016/j.gloenvcha.2011.08.006
Mbandi AM, Böhnke JR, Schwela D, Vallack H, Ashmore MR, Emberson L (2019) Estimating on-road vehicle fuel economy in Africa: a case study based on an urban transport survey in Nairobi, Kenya. Energies 12(6):1177. https://doi.org/10.3390/en12061177
Ministry of Energy (2019) Assessment of the supply and demand of cooking solutions at the household level. https://eedadvisory.com/wp-content/uploads/2020/09/MoE-2019-KenyaCooking-Sector-Study-compressed.pdf
Ministry of Health (2021) Household air pollution module 14. http://www.health.go.ke
Mokoena KK, Ethan CJ, Yu Y, Shale K, Liu F (2019) Ambient air pollution and respiratory mortality in Xi’an, China: a time-series analysis. Respir Res 20(1):139. https://doi.org/10.1186/s12931-019-1117-8
Munyao CM, Kiptoo GKK, Odinga C, Simiyu GM (2022) Assessment of improved biomass Cookstove Technologies and kitchen characteristics on indoor air quality and fuel consumption in rural settings of Western, Kenya. Eur J Health Sci 7(5):58–83. http://www.ajpojournals.org
Musyoka D, Muindi K (2022) A descriptive assessment of household air pollution in rural kitchens in Kenya. Atmosphere 13(12):2115. https://doi.org/10.3390/atmos13122115
Mutahi AW, Borgese L, Marchesi C, Gatari MJ, Depero LE (2021) Indoor and outdoor air quality for sustainable life: a case study of rural and urban settlements in poor neighbourhoods in Kenya. Sustainability 13(4):2417. https://doi.org/10.3390/su13042417
Mutuku KB (2022) Potential of agroforestry in sustainable fuelwood supply in Kenya. J Energy Nat Resour 11(1):1. https://doi.org/10.11648/j.jenr.20221101.11
Nardocci AC, Nogueira T, de Almeida Piai K, Cavendish TA, Kumar P (2023) Indoor environment exposure and children’s health. Curr Opin Environ Sci Health 32:100449. https://doi.org/10.1016/j.coesh.2023.100449
Nazaroff WW, Goldstein AH (2015) Indoor chemistry: research opportunities and challenges. Indoor Air 25(4):357–361. https://doi.org/10.1111/ina.12219
NEMA (2020) Kenya air quality and emission reduction strategy (developed for upstream petroleum sector)
Ng’ang’a Gicheru F (2021) Exposure to indoor air pollution from household fuels and effect on treatment response amongst children aged between 2 and 59 months admitted with pneumonia at the Kenyatta national hospital, Nairobi, Kenya
Ochieng CA, Zhang Y, Nyabwa JK, Otieno DI, Spillane C (2020) Household perspectives on cookstove and fuel stacking: a qualitative study in urban and rural Kenya. Energy Sustain Dev 59:151–159. https://doi.org/10.1016/j.esd.2020.10.002
Oduor N, Kitheka E, Ogutu C (2020) Energy in woody biomass 2020. In: Forest and energy, Issue 47. https://www.kefri.org/assets/publications/articles/ENERGY%20IN%20WOODY%20BIOMASS%202020.pdf
Okoko A, Reinhard J, von Dach SW, Zah R, Kiteme B, Owuor S, Ehrensperger A (2017) The carbon footprints of alternative value chains for biomass energy for cooking in Kenya and Tanzania. Sustain Energy Technol Assess 22:124–133. https://doi.org/10.1016/j.seta.2017.02.017
Ortega N, Curto A, Dimitrova A, Nunes J, Rasella D, Sacoor C, Tonne C (2021) Health and environmental impacts of replacing kerosene-based lighting with renewable electricity in East Africa. Energy Sustain Dev 63:16–23. https://doi.org/10.1016/j.esd.2021.05.004
Philibert C (2022) Power to the Cooks! New clean cooking opportunities for sustainable development in Sub-Saharan Africa. Briefings de l’Ifri, Ifri. ISBN: 979-10-373-0472-8
Pilishvili T, Loo JD, Schrag S, Stanistreet D, Christensen B, Yip F, Nyagol R, Quick R, Sage M, Bruce N (2016) Effectiveness of six improved cookstoves in reducing household air pollution and their acceptability in rural Western Kenya. PLoS ONE 11(11):e0165529. https://doi.org/10.1371/journal.pone.0165529
Pope DP, Mishra V, Thompson L, Siddiqui AR, Rehfuess EA, Weber M, Bruce NG (2010) Risk of low birth weight and stillbirth associated with indoor air pollution from solid fuel use in developing countries. Epidemiol Rev 32(1):70–81. https://doi.org/10.1093/epirev/mxq005
Power MC, Adar SD, Yanosky JD, Weuve J (2016) Exposure to air pollution as a potential contributor to cognitive function, cognitive decline, brain imaging, and dementia: a systematic review of epidemiologic research. Neurotoxicology 56:235–253. https://doi.org/10.1016/j.neuro.2016.06.004
Pratiti R (2021) Household air pollution related to biomass cook stove emissions and its interaction with improved cookstoves. AIMS Public Health 8(2):309–321. https://doi.org/10.3934/publichealth.2021024
Rafiq L, Zahra Naqvi SH, Shahzad L, Ali SM (2022) Exploring the links between indoor air pollutants and health outcomes in South Asian countries: a systematic review. Rev Environ Health. https://doi.org/10.1515/reveh-2022-0154
Rana J, Uddin J, Peltier R, Oulhote Y (2019) Associations between indoor air pollution and acute respiratory infections among under-five children in Afghanistan: do SES and sex matter? Int J Environ Res Public Health 16(16):2910. https://doi.org/10.3390/ijerph16162910
Raufman J, Blansky D, Lounsbury DW, Mwangi EW, Lan Q, Olloquequi J, Hosgood HD (2020) Environmental health literacy and household air pollution-associated symptoms in Kenya: a cross-sectional study. Environ Health 19(1):89. https://doi.org/10.1186/s12940-020-00643-5
Roser M (2021) Data review: how many people die from air pollution? https://ourworldindata.org/data-review-air-pollution-deaths#:~:text=4.5%20million%20people%20died%20prematurely,from%20indoor%20and%20outdoor%20pollution
Rotich I, Marialigeti K, Kalapos T, Masenge E, Mbithi V (2021) Evaluation of optimal bio-methane potential of Cuscuta japonica. J Eng Agric Environ. https://doi.org/10.37017/jeae-volume7-no2.2021-2
Rylance S, Nightingale R, Naunje A, Mbalume F, Jewell C, Balmes JR, Grigg J, Mortimer K (2019) Lung health and exposure to air pollution in Malawian children (CAPS): a cross-sectional study. Thorax 74(11):1070–1077. https://doi.org/10.1136/thoraxjnl-2018-212945
Saksena S, Prasad R, Pal RC, Joshi V (1992) Patterns of daily exposure to TSP and CO in the Garhwal Himalaya. Atmos Environ A Gen Top 26(11):2125–2134. https://doi.org/10.1016/0960-1686(92)90096-4
Samet JM, Bahrami H, Berhane K (2016) Indoor air pollution and cardiovascular disease. Circulation 133(24):2342–2344. https://doi.org/10.1161/CIRCULATIONAHA.116.023477
Shaddick G, Thomas ML, Mudu P, Ruggeri G, Gumy S (2020) Half the world’s population are exposed to increasing air pollution. Npj Clim Atmos Sci 3(1):23. https://doi.org/10.1038/s41612-020-0124-2
Shilenje ZW, Maloba S, Ongoma V (2022) A review on household air pollution and biomass use over Kenya. Front Environ Sci. https://doi.org/10.3389/fenvs.2022.996038
Simoni M, Jaakkola MS, Carrozzi L, Baldacci S, Di Pede F, Viegi G (2003) Indoor air pollution and respiratory health in the elderly. Eur Respir J 21(Supplement 40):15S-20S. https://doi.org/10.1183/09031936.03.00403603
Singh A, Ng’ang’a D, Gatari MJ, Kidane AW, Alemu ZA, Derrick N, Webster MJ, Bartington SE, Thomas GN, Avis W, Pope FD (2021) Air quality assessment in three East African cities using calibrated low-cost sensors with a focus on road-based hotspots. Environ Res Commun 3(7):075007. https://doi.org/10.1088/2515-7620/ac0e0a
SNV (2023) Home our projects Improved Cookstoves (ICS)—Kenya. Improved Cookstoves (ICS), Kenya
Stankovic A, Mitrovic V, Zivadinovic R (2011) Influence of air pollution on pregnant women’s health and pregnancy outcomes. Med Pregl 64(5–6):279–284. https://doi.org/10.2298/MPNS1106279S
Suter M, Karr C, John-Stewart G, Gómez L, Moraa H, Nyatika D, Wamalwa D, Paulsen M, Simpson C, Ghodsian N, Boivin M, Bangirana P, Benki-Nugent S (2018) Implications of combined exposure to household air pollution and HIV on neurocognition in children. Int J Environ Res Public Health 15(1):163. https://doi.org/10.3390/ijerph15010163
van den Berg IC (2018) Kenya’s strategy to make liquefied petroleum gas the nation’s primary cooking fuel. Live Wire; 2018/89. © World Bank, Washington, DC. http://hdl.handle.net/10986/30391
van Vliet EDS, Kinney PL (2007) Impacts of roadway emissions on urban particulate matter concentrations in sub-Saharan Africa: new evidence from Nairobi, Kenya. Environ Res Lett 2(4):045028. https://doi.org/10.1088/1748-9326/2/4/045028
Vichit-Vadakan N, Vajanapoom N, Ostro B (2008) The Public Health and Air Pollution in Asia (PAPA) Project: estimating the mortality effects of particulate matter in Bangkok, Thailand. Environ Health Perspect 116(9):1179–1182. https://doi.org/10.1289/ehp.10849
Wagner DN, Odhiambo SR, Ayikukwei RM, Boor BE (2022) High time-resolution measurements of ultrafine and fine woodsmoke aerosol number and surface area concentrations in biomass burning kitchens: a case study in Western Kenya. Indoor Air. https://doi.org/10.1111/ina.13132
Welfle DA, Chingaira S, Kassenov A (2020) Decarbonising Kenya’s domestic & industry Sectors through bioenergy: an assessment of biomass resource potential & GHG performances. Biomass Bioenergy 142:105757. https://doi.org/10.1016/j.biombioe.2020.105757
WHO (2022a) Billions of people still breathe unhealthy air: new WHO data. https://www.who.int/news/item/04-04-2022-billions-of-people-still-breathe-unhealthy-air-new-who-data
WHO (2022b) Indoor air pollution control: determining milestones of the national strategy to improve indoor air quality. https://www.who.int/indonesia/news/detail/21-02-2022-indoor-air-pollution-control-determining-milestones-of-the-national-strategy-to-improve-indoor-air-quality
WHO (2022c) Household air pollution. WHO. https://www.who.int/news-room/fact-sheets/detail/household-air-pollution-and-health
Yip F, Christensen B, Sircar K, Naeher L, Bruce N, Pennise D, Lozier M, Pilishvili T, Loo Farrar J, Stanistreet D, Nyagol R, Muoki J, de Beer L, Sage M, Kapil V (2017) Assessment of traditional and improved stove use on household air pollution and personal exposures in rural western Kenya. Environ Int 99:185–191. https://doi.org/10.1016/j.envint.2016.11.015
Yonemitsu A, Njenga M, Iiyama M, Matsushita S (2015) A choice experiment study on fuel preference of Kibera slum households in Kenya. Int J Environ Sci Dev 6(3):196–200. https://doi.org/10.7763/IJESD.2015.V6.589
Zeng Z, Xiong K, Lu X-L, Weng M-C, Liu F (2018) Study on the smoke stratification length under longitudinal ventilation in tunnel fires. Int J Therm Sci 132:285–295. https://doi.org/10.1016/j.ijthermalsci.2018.05.038
Funding
Open access funding provided by Eötvös Loránd University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no conflict of interest that could influence the results of the review presented.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cite this article
Rotich, I.K., Musyimi, P.K. Indoor Air Pollution in Kenya. Aerosol Sci Eng 8, 54–65 (2024). https://doi.org/10.1007/s41810-023-00205-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41810-023-00205-5