
Abstract
Research into the cognitive enhancing effects of polyphenols is small but growing. Single doses of the stilbene polyphenol resveratrol can increase cerebral blood flow (CBF) but have failed to improve cognitive performance in young, healthy cohorts. As both CBF and overall energy expenditure are closely related to neural activity, this randomised, double-blind, placebo-controlled, crossover investigation, assessed the metabolic consequences of resveratrol during high cognitive demand via indirect calorimetry (ICa). Twenty-seven, self-reported healthy participants (15 male, 12 female; mean age = 22) who reported themselves free of any food intolerances and any herbal supplementation or prescription medications were recruited for the current study. Participants arrived at the testing facility at 8 a.m. on three separate occasions to complete a serial subtraction demand battery 45 min and 2 and 3 h following administration with 500 mg, 250 mg trans-resveratrol or inert placebo, while connected to an online gas analysis system. A series of within-subjects ANOVAs (with planned comparisons) revealed a significant shift towards higher carbohydrate oxidisation during cognitive demand, as indexed by a significant increase in respiratory exchange ratio (RER) at 45-min and 3-h time points, following administration of 500 mg resveratrol. Despite this, no subsequent resveratrol-related benefits to cognitive performance were observed. These results show that acute supplementation with resveratrol in young, healthy adults can modulate fuel utilization during cognitive demand, yet this does not translate into clear improvements in cognitive performance. This study adds further understanding behind the lack of cognitive effects of resveratrol in young and or healthy individuals. Future research should direct efforts towards assessing the cognitive impact of resveratrol, and other vasoactive polyphenols, in populations with age-related or dietary-induced metabolic deficits.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The brain is the most metabolic organ in the human body, consuming disproportionately large energy resources despite its relatively small size (Raichle 2010). As the brain cannot store its own energy source, it is solely reliant on the delivery of metabolic substrates (glucose/oxygen) via dilation of the cerebral vasculature; this is then increased, upon demand, in response to neural activity (Girouard and Iadecola 2006). The release of nitric oxide (NO) is fundamental to this neurovascular coupling (Dormanns et al. 2016), thus articles that can amplify this response are hypothesised to improve the provision of blood-borne neural fuel substrates. In addition, interventions that endeavour to sustain or replenish adenosine triphosphate levels may also engender cognitive enhancing effects (Owen and Sunram-Lea 2011).
The stilbene polyphenol resveratrol (3, 4′, 5 trihydroxystilbene) is a phytoalexin that has been found to bolster NO synthesis within human endothelial cells in vitro (Elíes et al. 2011). This has led to a growing body of research observing acute resveratrol-mediated improvements to peripheral blood flow (Wong et al. 2011; Wong et al. 2012) and, in turn, cerebrovascular functioning (Wong et al. 2016). However, despite evidence of increased cerebral blood flow (CBF) during cognitive task performance, no robust cognitive benefits have been observed from acute or chronic resveratrol administration in young, healthy adults (Kennedy et al. 2010; Wightman et al. 2014; Wightman et al. 2015). This may potentially suggest that the young, healthy participants may not be able to utilise the increased supply of neural fuel substrates. Interestingly, however, increased levels of oxygen extraction have also been observed during task performance from acute doses of resveratrol, as indexed by increased concentrations of deoxygenated haemoglobin (Kennedy et al. 2010; Wightman et al. 2014). Consequently, resveratrol may also influence substrate oxidation and cerebral metabolic rate during cognitive performance. It is important to note, however, that despite reflecting the overall pattern of cerebral metabolic activity, measuring the cerebral haemodynamic response neither quantify the extent of cerebral metabolic change nor the relative change of energy expenditure during cognitive performance (Al Naher et al. 2016).
Indirect calorimetry (ICa) has been employed previously to assess changes in metabolic rate during cognitive task performance and has demonstrated sufficient sensitivity to detect subtle changes in energy expenditure from differing intensities of cognitive tasks; beyond that of somatic movements (Al Naher et al. 2016). Although the use of ICa to measure the metabolic consequences of nutritional supplements during cognitive demand remains relatively novel, enhanced fat oxidation and total energy expenditure have been observed during cognitive task performance from acute multivitamin administration (Kennedy et al. 2016). This is particularly interesting given that the administration of individual vitamins such as vitamins C and E have shown to improve endothelial functioning (Ashor et al. 2015). By examining the metabolic consequences of resveratrol during increased neural demand, further support could be obtained for the capacity of resveratrol to modulate the hypothesised additional neural substrates that are concomitant with relative increases in CBF. This is supported by the notion that a good transport and utilisation of the pulmonary gases measured for ICa (oxygen/carbon dioxide) also emphasise the efficiency of the cardiovascular response to cognitive demand. Given the above, the current study investigates the metabolic consequences and cognitive effects of single acute doses of resveratrol during high cognitive demand.
Materials and Methods
Participants
Twenty-seven (15 male, 12 female) participants reported themselves to be in good health and to have good or corrected vision. The average age of the sample was 22 years (SD 3.64), with a mean stature of 1.74 m (SD 0.10) and mass of 69.30 kg (SD 14.03). All participants also reported themselves to be free of food intolerances and sensitivities, or any gastrointestinal, hepatic or renal diagnoses. This was to ensure that no extraneous factors would interfere with the absorption of the treatments. Moreover, participants were excluded if they had suffered any neurological trauma (such as a head injury) or possess any neuropathologies. While individuals who reported themselves to be taking any herbal supplements or prescription medications (with the exception of the contraceptive pill and topical acne medication) or consumed high amounts of caffeine (≥ 6 cups of coffee/tea or its caffeine equivalent daily) were also excluded from the current study. Finally, due to the requirements of the tasks, participants were also excluded if they had a diagnosis of dyscalculia (or any relevant learning difficulty). All participants were required to fast for 12 h (with the exception of water) and to avoid strenuous exercise prior to each testing session. They received £60 for their participation upon completion of the study. This study received ethical approval from the Psychology Department (within the Faculty of Health and Life Sciences) Ethics Committee and was conducted according to the Declaration of Helsinki (1964).
Cognitive Task Battery
The current task battery comprises three serial subtraction tasks (serial 3, 7 and 17). For each task, participants were presented with the standardised instruction screen, which informed the participant to continuously subtract the serial number (either 3, 7 or 17) from a given starting number (between 800 and 999), as quickly and accurately as possible, using the numeric keyboard in front of them to enter each response. Upon giving their first answer, the starting number was then removed from the screen and their response was to be mentally retained. Sequential responses were then entered but were covered by an asterisk. Pressing the enter key signalled the end of each response and cleared the three asterisks from the screen. Each task lasted 5 min, thus each repetition lasted for 15 min in total. With regard to incorrect responses, any subsequent responses were recorded as correct if they were accurate in relation to the new number. The task was scored for the number of correct entries and the number of errors, with the addition of these two outputs creating a ‘total’ number of attempts entered.
To avoid any task-time bias, the order of the tasks was counterbalanced in a Latin square. All tasks in each repetition of the battery were completed in a continuous fashion, in order to induce maximal cognitive demand and fatigue to the participants. The rationale for the use of these tasks was based upon previous research demonstrating their ability to increase both fuel utilization and heart rate beyond that of peripheral mechanisms (Scholey et al. 2001; Kennedy and Scholey 2000).
Other Measures
Two 100-mm visual analogue scales (VAS) were employed prior to and following each repetition (completion of all three serial subtraction tasks), measuring ‘Mental Tiredness’ and ‘Difficulty’ to assess any potential mood changes following resveratrol consumption. Scales were anchored at either end by ‘not at all’ and ‘extremely’; these were scored as a percentage along the line towards ‘extremely’.
Treatments
Active treatments of resveratrol were acquired from megaresveratrol.net (Danbury, CT, USA). The integrity of the extract used was 99.73%, as verified by the manufactures statement. Treatments were administered on separate days, with each testing session being conducted no more than 48 h before, and no more than 14 days after the previous session. During the three study visits, participants received three single-dose treatments in an order dictated by random allocation to a (Latin Square) counterbalanced order. Two capsules were consumed on each testing day either:
-
1)
Two placebo capsules (CABOT MP5 fumed silica).
-
2)
One 250-mg dose of resveratrol with one placebo.
-
3)
Two 250 mg resveratrol capsules (equating to a 500-mg dose).
All treatments were administered within the same size 0 vegetarian soft-gel capsules. All treatments were counterbalanced and were prepared by the lead investigator. The treatments were then coded by a third party who had no further involvement in any aspect of the study. No member of the investigational team was aware of the contents of the capsules until completion of the statistical analysis.
Indirect Calorimetry
For the current investigation, oxygen uptake and carbon dioxide excretion were measured from expired pulmonary air using an online analysis system (Metalyzer 3B, Cortex, Leipzig, Germany). The standard formula was then employed to calculate total energy expenditure carbohydrate and fat oxidisation (Frayn 1983). The online gas analysis system was attached to the participants via a facemask, which covered both the nose and mouth, connected by Falconia tubing.
Procedure
Participants attended a visit to the Brain, Performance and Nutrition Research Centre at Northumbria University on four separate occasions. The first of the visits was to screen the participant against the exclusion criteria and familiarise them with the cognitive demand battery. The three subsequent visits were testing visits and were identical to each other. All participants arrived at 8 a.m., fully fasted (consuming nothing but water) for 12 h having had also refrained from engaging in any strenuous exercise prior to the session. Upon confirming continuous compliance with the inclusion criteria, participants completed a brief rest before being connected to the gas analysis equipment via a facemask and mouthpiece. This was adjusted to ensure there were no gaps and was fitted to the participant’s comfort. After, participants completed a baseline measurement of the serial subtraction task demand battery and mood scales. Upon completion, participants were then disconnected from the gas analysis equipment and then administrated with their treatment for the day before continuing to rest for 45 min to allow for absorption. Thirty-five minutes into the absorption period, participants were reconnected to the gas analysis device before continuing to rest for the remaining of the absorption period. Upon completion of the absorption period, participants then completed the first of the post-dose mood scales and cognitive demand battery. The participants were then required to complete the battery and VAS scales at a further 2 and 3 h post-administration time points. ICa measures were obtained throughout all task performances. Participants were fully debriefed upon completion of the final study visit. The timeline for a typical study day can be seen in Fig. 1.

Timeline for study 1 testing day
Analysis
All ICa analysis was completed within Minitab 17 Statistical Software (State College, PA, Minitab, Inc.), while all behavioural data was analysed in SPSS version 22 for Windows (IBM SPSS Statistics Armonk, NY).
Treatment of Indirect Calorimetry Data
Raw data was extracted and averaged across 1-min epochs for each task within the three individual post-dose repetitions. Each of these five 1-min epochs was first cleaned before being condensed and averaged to represent a 5-min average time point. This cleaning process led to the removal of two full data sets. A further data set was not included due to data catchment errors (missing baseline performance). The final sample for ICa analysis was N = 24.
Main Indirect Calorimetry Analysis
All ICa data was converted to a change from baseline measure, in which the averages from the corresponding baseline task performance were utilised. The collapsed 5-min individual epochs for each serial subtraction task were cleaned before the initial analysis. All remaining ICa data during cognitive task performance was converted to change from baseline, utilising the relative baseline task performance from each task. Analysis consisted of 3 × 3 × 3 within-subjects’ ANOVAs assessing treatment (250 mg resveratrol, 500 mg resveratrol and placebo) × task (serial 3, serial 7 and serial 17 subtractions) × repetition (× 3). Subsequently, planned comparisons were conducted upon the emergence of significant interaction effects, utilising the mean square (MS) error values from the initial ANOVA. Only comparisons to placebo and not between active treatments were conducted.
Behavioural Analysis
Raw cognitive data was cleaned before being converted into a change from baseline measure. One participant’s data was removed due to failing to maintain at least 50% accuracy across all three tasks across a testing session. Raw baseline scores for each task were then analysed to assess if there was any difference between treatment baseline scores. Following this, nine within-subjects’ ANOVAs analysing treatment (500 mg resveratrol, 250 mg resveratrol and placebo) × repetition (× 3) × task (3 s, 7 s and 17 s) were conducted.
Prior to the mood analysis, scores for ‘concentration’ and ‘mental fatigue’ were converted to change from baseline; the score submitted following completion of the baseline battery of cognitive tasks was used as a baseline. Due to data catchment errors (missing baseline performance) one participant’s data was removed from the subsequent analysis. This resulted in N = 26 data sets for the final analysis. Two within-subjects ANOVAs investigating treatment (500 mg resveratrol, 250 mg resveratrol and placebo) × repetition (× 3) × time (pre-completion and post-completion of the cognitive battery) were conducted. This was followed up with Bonferroni corrected post hoc pairwise comparisons on the presentation of a significant F test.
Results
Indirect Calorimetry Results
A series of repeated measures ANOVAs revealed no significant main effect of treatment or treatment-related interactions on total energy expenditure, carbohydrate and fat oxidisation (all p > .05) during cognitive performance.
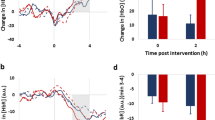
However, a within-subjects’ ANOVA demonstrated a significant treatment × task × repetition interaction [F (8, 184) = 1.13, p = .039] on respiratory exchange ratio (RER), indicating a significant treatment-related change in fuel utilisation during task performance. Follow-up planned comparisons demonstrated that administration of 250 mg resveratrol evinced a significant increase in RER at repetition 1 during the serial 3 subtractions, p = .002 (95% CI = − .012, .035; d = .29). Moreover, administration with 250 mg resveratrol also significantly increased RER during serial 3 (p = .001; 95% CI = − .016, .042; d = .26) and 7 (p = .001; 95% CI = − .018, .042; d = .24) task performance on the third repetition in comparison to placebo. However, the same dose was found to induce a significant reduction in RER during serial 17 task performance (p < .001; 95% CI = − .019, .046; d = .24) on the final repetition of the task battery in contrast to placebo. As can be seen in Fig. 2, administration of 500 mg resveratrol evinced an increase in RER across all tasks and repetitions in comparison to placebo. These were found to be significant for serial 3 (p = .029; 95% CI = − .016, .032; d = .20) and serial 7 (p = .018; 95% CI = − .016, .033; d = .21) subtraction performance at repetition 1 and for the same tasks during repetition 3 (S3: p = .003; 95% CI = − .018, .040; d = .22) (S7: p = .001; 95% CI = − .021, .046; d = .22).

The acute effects of 250 mg and 500 mg resveratrol on respiratory exchange ratio (RER). Graph depicts mean changes in change from baseline RER (with SEM error bars), for the three serial subtraction tasks during the three repetitions of the post-dose tasks in 24 healthy adults following 500 mg resveratrol, 250 mg resveratrol or placebo. *p < .05, **p < .01 (in comparison to placebo)
Behavioural Results
A series of within-subjects ANOVAs revealed no significant main treatment or treatment-related interactions on any sub-measures of the cognitive or mood parameters in the current study (all p > .05).
Discussion
Previous investigations have demonstrated that single, acute oral doses of the resveratrol can modulate CBF. However, such findings have failed to be complemented with clear improvements to cognitive performance. It is unclear whether short-term increases in CBF can be beneficial to cognitive performance in young, healthy cohorts. The current study therefore aimed to assess the metabolic consequences and cognitive effects of two single acute doses of resveratrol. The results here showed that administration of both doses of resveratrol induced significant increases in RER, although, only the 500 mg dose of resveratrol demonstrated consistently higher RER across all tasks and repetitions in comparison to placebo; these were significant at the 45-min and 3-h time points for the serial 3 and 7 subtraction tasks. No resveratrol-mediated modulation of total energy expenditure or cognitive performance was observed.
RER provides an insight to the body’s predominant fuel source, with a higher RER indicative of carbohydrate being the predominant fuel source, while a lower RER indicates fat to be the principal fuel in use (Simonson and DeFronzo 1990). As the tasks used in the current study have proven sensitive to increased glucose utilisation (Scholey et al. 2001; Kennedy and Scholey 2000) it is interesting to consider that resveratrol can shift fuel oxidisation towards a higher utilisation of carbohydrate during high cognitive demand. It is noteworthy that there is no consensus within the literature as to what a ‘typical’ RER response to cognitive demand entails. Only two investigations at the time of writing have reported modulation of RER during cognitive performance, with one reporting a significant increase (Delistraty et al. 1991) and the other a significant decrease (Troubat et al. 2009) in RER across cognitive demand. The direction of results here, demonstrate that RER gradually decreased across the 3 post-treatment task intervals (45 min, 2 h and 3 h) from an initially elevated RER. This would suggest that the body switches from an initial high carbohydrate source to a more oxidative supply (i.e. increased fat oxidation) (Troubat et al. 2009); yet, after an acute dose of 500 mg of resveratrol, carbohydrate oxidation remains slightly elevated. In a recent review, Grassmann et al. (2016) note that the excretion of carbon dioxide is sensitive to increasing cognitive task difficulty. As a higher RER is characterised by an increased ratio of carbon dioxide excretion to oxygen inhalation, this may suggest that the elevated excretion of carbon dioxide observed during the 500 mg resveratrol condition may provide a proxy for increased exertion during cognitive demand. However, in the absence of improved cognitive functioning, it is unclear whether this increase in RER has been beneficial.
The observation that resveratrol was unable to increase total energy expenditure during cognitive demand is somewhat unanticipated. In addition to increased cerebral perfusion, resveratrol is capable of activating 5′ adenosine monophosphate–activated protein kinase (AMPK); a key regulator in energy-sensing procedures of the glycaemic response, whole body metabolism and energy homeostasis (Hardie et al. 2012). Thus, the ability of resveratrol to modulate such metabolic molecular targets may have beneficial consequences for dietary and age-related metabolic complications (Kulkarni and Cantó 2015). Indeed, although most data remains in vitro or from animal models, resveratrol (150 mg/day) has been found to improve mitochondrial function in the skeletal muscle after 30 days administration in obese, but otherwise healthy men (Timmers et al. 2011). While a 3-day supplementation of a combination of both resveratrol (150 mg) and epigallocatechin-3-gallate (EGCG) (300 mg) can increase both fasting and postprandial energy expenditure at rest in obese humans (Most et al. 2016).
The lack of modulation of energy expenditure by resveratrol could equally suggest that the young, healthy sample employed in this current study, as in other investigations, are unlikely to be able to benefit metabolically from resveratrol administration. Although CBF was not measured here, it is noteworthy that the CBF response to sustained neural activity is always greater than that of the rise in both the cerebral metabolic rate of oxygen and ATP consumption (Leithner and Royl 2014; Raichle and Gusnard 2002). As a result, any further modulation of CBF may lead to such subtle changes in cerebral metabolism that they are unable to be detected in healthy, young individuals. However, despite the lack of resveratrol-mediated modulation of energy expenditure in the current study, the ability to increase RER certainly suggests that resveratrol can induce subtle, yet significant, metabolic consequences during cognitive performance, which may be of increased utility for those with either reductions in CBF and or metabolic complications.
The lack of cognitive improvements observed in the current study coincides with those of similar previous investigations (Kennedy et al. 2010; Wightman et al. 2014; Wightman et al. 2015) and confirms that the young, healthy sample employed here are likely unable to benefit from resveratrol administration. Thus, research into whether resveratrol can improve cognitive functioning in populations that possess cognitive deficits and or a compromised supply of neural fuel substrates, such as natural ageing populations, is warranted. Promising resveratrol-mediated modulation of cerebral perfusion has already been observed in individuals with type 2 diabetes mellitus (Wong et al. 2016) and post-menopausal women (Evans et al. 2017), yet definitive cognitive improvements in conjunction to these findings are still lacking. In addition, more promise has been seen with other vasodilating polyphenols when consumed over longer periods of time. For example, improvements to cognitive functioning in healthy older adults have been seen from 8 weeks administration of 520 mg and 993 mg of cocoa flavanols (Mastroiacovo et al. 2015) and are likely predicated on NO-mediated vasodilation (Fisher et al. 2003) and augmented cerebral perfusion (Francis et al. 2006; Sorond et al. 2008; Lamport et al. 2015). This more well-trodden path with cocoa polyphenols gives promise that, via the same vasodilatory mechanism, resveratrol may also improve cognitive function by ameliorating a reduced blood flow capacity, commonly associated with ageing.
Conclusion
The current study has added to the growing number of investigations into the potential cognitive enhancing properties of the polyphenol resveratrol. Acute resveratrol administration was unable to modulate energy expenditure or cognitive performance. However, a 500-mg dose of resveratrol was capable of increasing RER up to 3 h post-administration during cognitive demand. This may suggest that resveratrol can shift fuel oxidation, potentially as a method of supporting mental exertion. Whether this provides a boon to cognitive functioning in young, healthy cohorts is unclear. It is proposed that resveratrol administration will be more fruitful in populations that suffer a mild reduction in neural fuel substrates or cognitive deficits, such as those associated with natural ageing.
Data Availability
The datasets analysed during the current study are available from the corresponding author on reasonable request.
References
Al Naher, A., Schlaghecken, F., Barber, T., & Kumar, S. (2016). Modulation of metabolic rate in response to a simple cognitive task. Archives of Medicine, 8(4), 1–7.
Ashor, A. W., Siervo, M., Lara, J., Oggioni, C., Afshar, S., & Mathers, J. C. (2015). Effect of vitamin C and vitamin E supplementation on endothelial function: a systematic review and meta-analysis of randomised controlled trials. British Journal of Nutrition, 113(8), 1182–1194.
Delistraty, D. A., Greene, W. A., Carlberg, K. A., & Raver, K. K. (1991). Use of graded exercise to evaluate physiological hyperreactivity to mental stress. Medicine & Science in Sports & Exercise, 23(4), 476–481.
Dormanns, K., Brown, R. G., & David, T. (2016). The role of nitric oxide in neurovascular coupling. Journal of Theoretical Biology, 394, 1–17.
Elíes, J., Cuíñas, A., García-Morales, V., Orallo, F., & Campos-Toimil, M. (2011). Trans-resveratrol simultaneously increases cytoplasmic Ca2+ levels and nitric oxide release in human endothelial cells. Molecular Nutrition & Food Research, 55(8), 1237–1248.
Evans, H. M., Howe, P. R., & Wong, R. H. (2017). Effects of resveratrol on cognitive performance, mood and cerebrovascular function in post-menopausal women; a 14-week randomised placebo-controlled intervention trial. Nutrients, 9(1), 27.
Fisher, N. D., Hughes, M., Gerhard-Herman, M., & Hollenberg, N. K. (2003). Flavanol-rich cocoa induces nitric-oxide-dependent vasodilation in healthy humans. Journal of Hypertension, 21(12), 2281–2286.
Francis, S. T., Head, K., Morris, P. G., & Macdonald, I. A. (2006). The effect of flavanol-rich cocoa on the fMRI response to a cognitive task in healthy young people. Journal of Cardiovascular Pharmacology, 47, S215–S220.
Frayn, K. N. (1983). Calculation of substrate oxidation rates in vivo from gaseous exchange. Journal of Applied Physiology, 55(2), 628–634.
Girouard, H., & Iadecola, C. (2006). Neurovascular coupling in the normal brain and in hypertension, stroke, and Alzheimer disease. Journal of Applied Physiology, 100(1), 328–335.
Grassmann, M., Vlemincx, E., von Leupoldt, A., Mittelstädt, J. M., & Van den Bergh, O. (2016). Respiratory changes in response to cognitive load: a systematic review. Neural Plasticity, 8146809.
Hardie, D. G., Ross, F. A., & Hawley, S. A. (2012). AMPK: a nutrient and energy sensor that maintains energy homeostasis. Nature Reviews Molecular Cell Biology, 13(4), 251.
Kennedy, D. O., & Scholey, A. B. (2000). Glucose administration, heart rate and cognitive performance: effects of increasing mental effort. Psychopharmacology, 149(1), 63–71.
Kennedy, D. O., Wightman, E. L., Reay, J. L., Lietz, G., Okello, E. J., Wilde, A., & Haskell, C. F. (2010). Effects of resveratrol on cerebral blood flow variables and cognitive performance in humans: a double-blind, placebo-controlled, crossover investigation. The American Journal of Clinical Nutrition, 91(6), 1590–1597.
Kennedy, D. O., Stevenson, E. J., Jackson, P. A., Dunn, S., Wishart, K., Bieri, G., Barella, L., Carne, A., Dodd, F. L., Robertson, B. C., Forster, J., & Haskell-Ramsey, C. F. (2016). Multivitamins and minerals modulate whole-body energy metabolism and cerebral blood-flow during cognitive task performance: a double-blind, randomised, placebo-controlled trial. Nutrition & metabolism, 13(1), 11.
Kulkarni, S. S., & Cantó, C. (2015). The molecular targets of resveratrol. Biochimica et Biophysica Acta (BBA)-Molecular Basis of Disease, 1852(6), 1114–1123.
Lamport, D. J., Pal, D., Moutsiana, C., Field, D. T., Williams, C. M., Spencer, J. P., & Butler, L. T. (2015). The effect of flavanol-rich cocoa on cerebral perfusion in healthy older adults during conscious resting state: a placebo controlled, crossover, acute trial. Psychopharmacology, 232(17), 3227–3234.
Leithner, C., & Royl, G. (2014). The oxygen paradox of neurovascular coupling. Journal of Cerebral Blood Flow & Metabolism, 34(1), 19–29.
Mastroiacovo, D., Kwik-Uribe, C., Grassi, D., Necozione, S., Raffaele, A., Pistacchio, L., … & Ferri, C. (2015). Cocoa flavanol consumption improves cognitive function, blood pressure control, and metabolic profile in elderly subjects: the Cocoa, Cognition, and Aging (CoCoA) Study—a randomized controlled trial–. The American Journal of Clinical Nutrition, 101(3), 538–548.
Most, J., Timmers, S., Warnke, I., Jocken, J. W., van Boekschoten, M., de Groot, P., et al. (2016). Combined epigallocatechin-3-gallate and resveratrol supplementation for 12 wk increases mitochondrial capacity and fat oxidation, but not insulin sensitivity, in obese humans: a randomized controlled trial. The American Journal of Clinical Nutrition, 104(1), 215–227.
Owen, L., & Sunram-Lea, S. I. (2011). Metabolic agents that enhance ATP can improve cognitive functioning: a review of the evidence for glucose, oxygen, pyruvate, creatine, and L-carnitine. Nutrients, 3(8), 735–755.
Raichle, M. E. (2010). Two views of brain function. Trends in Cognitive Sciences, 14(4), 180–190.
Raichle, M. E., & Gusnard, D. A. (2002). Appraising the brain’s energy budget. Proceedings of the National Academy of Sciences, 99(16), 10237–10239.
Scholey, A. B., Harper, S., & Kennedy, D. O. (2001). Cognitive demand and blood glucose. Physiology & Behavior, 73(4), 585–592.
Simonson, D. C., & DeFronzo, R. A. (1990). Indirect calorimetry: methodological and interpretative problems. American Journal of Physiology-Endocrinology And Metabolism, 258(3), E399–E412.
Sorond, F. A., Lipsitz, L. A., Hollenberg, N. K., & Fisher, N. D. (2008). Cerebral blood flow response to flavanol-rich cocoa in healthy elderly humans. Neuropsychiatric Disease and Treatment, 4(2), 433.
Timmers, S., Konings, E., Bilet, L., Houtkooper, R. H., van de Weijer, T., Goossens, G. H., et al. (2011). Calorie restriction-like effects of 30 days of resveratrol supplementation on energy metabolism and metabolic profile in obese humans. Cell Metabolism, 14(5), 612–622.
Troubat, N., Fargeas-Gluck, M. A., Tulppo, M., & Dugué, B. (2009). The stress of chess players as a model to study the effects of psychological stimuli on physiological responses: an example of substrate oxidation and heart rate variability in man. European Journal of Applied Physiology, 105(3), 343–349.
Wightman, E. L., Reay, J. L., Haskell, C. F., Williamson, G., Dew, T. P., & Kennedy, D. O. (2014). Effects of resveratrol alone or in combination with piperine on cerebral blood flow parameters and cognitive performance in human subjects: a randomised, double-blind, placebo-controlled, cross-over investigation. British Journal of Nutrition, 112(2), 203–213.
Wightman, E. L., Haskell-Ramsay, C. F., Reay, J. L., Williamson, G., Dew, T., Zhang, W., & Kennedy, D. O. (2015). The effects of chronic trans-resveratrol supplementation on aspects of cognitive function, mood, sleep, health and cerebral blood flow in healthy, young humans. British Journal of Nutrition, 114(9), 1427–1437.
Wong, R. H. X., Howe, P. R. C., Buckley, J. D., Coates, A. M., Kunz, I., & Berry, N. M. (2011). Acute resveratrol supplementation improves flow-mediated dilatation in overweight/obese individuals with mildly elevated blood pressure. Nutrition, Metabolism and Cardiovascular Diseases, 21(11), 851–856.
Wong, R., Berry, N., Coates, A., Buckley, J., & Howe, P. (2012). Sustained improvement of vasodilator function by resveratrol in obese adults. Journal of Hypertension, 30, e70.
Wong, R. H., Raederstorff, D., & Howe, P. R. (2016). Acute resveratrol consumption improves neurovascular coupling capacity in adults with type 2 diabetes mellitus. Nutrients, 8(7), 425.
Authorship
All the authors (TE, SG, DK and EW) were actively involved in the planning of the research described herein and in writing the final manuscript. TE collected the data and all authors contributed to and reviewed the final publication.
Funding
The study herein received no external funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no conflicts of interest.
Ethical approval
This study received ethical approval from the Psychology Department (within the Faculty of Health and Life Sciences) Ethics Committee and was conducted according to the Declaration of Helsinki (1964).
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 48 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Eschle, T.M., Goodall, S., Kennedy, D.O. et al. Acute Resveratrol Administration Increases Neural Effort but Not Whole Body Metabolism or Cognitive Performance in Healthy, Young Participants. J Cogn Enhanc 4, 315–322 (2020). https://doi.org/10.1007/s41465-019-00139-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41465-019-00139-2