
Abstract
Background
Globally, at least, more than 2 billion people are either blind or visually impaired, the majority of whom live in low-income settings. Visually impaired people experience limitations in their daily activities in addition to the negative psychological impact. Ophthalmology is not a major focus in medical curricula, including in Sudan. The purpose of this study was to evaluate the effects of a short course in improving eye healthcare knowledge and skills among final-year medical students in a public university in Khartoum State, Sudan.
Methods
A mixed-methods interventional study was conducted among 25 final-year medical students in Sudan. A short ophthalmology course was designed and conducted aiming to strengthen the knowledge and ability of the medical students to deal with common eye disorders, eye emergencies, prevention of blindness, and promotion for eye health. Data were collected using a closed-ended questionnaire at the start and 1 month after completion of the course. The quantitative data were analyzed using Excel, and the Fisher exact test was performed using Statistical Package for the Social Sciences (version 21.0) to examine any association between variables of interest. A p value of less than 0.05 was considered statistically significant. The quantitative data was supplemented by one focus group discussion that was conducted at the end of the course.
Results
The average ophthalmology knowledge of participants improved from 52.6 to 86.6% (p < 0.001). Diagnostic skills improved from 57.3 to 93.6% (p < 0.001), and knowledge regarding the needed interventional actions improved from 58.6% to 94% (p < 0.001). Participants both enjoyed and learnt from this short course. Participants felt more confident and able to distinguish between simple, complicated, and urgent conditions. The majority of course content was new to them, but they suggested replacing some content with actual clinical work.
Conclusion
A well-designed short ophthalmology course significantly improves the levels of medical students’ knowledge and skills towards eye health. Implementing such a course as a standard component in the national medical curriculum has the potential to contribute towards the reduction of blindness in the long term.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Blindness or complete vision loss is defined as visual acuity of less than 3/60, or a corresponding visual field loss to less than 10°, in the better eye with the best possible correction [1]. It may be reversible or irreversible depending on the underlying cause.
Blindness and vision impairment affect at least 2.2 billion people around the world. Of those, 1 billion have preventable vision impairment or one that has yet to be addressed [2]. About 90% of the world visually impaired lives in low-income settings, and 82% of people living with blindness are aged 50 and above [3].
Vision impairment interferes with the person’s ability to perform daily activities [4]. Blindness and low vision have psychological implications such as feelings of guilt, anxiety, sadness, and depression [5].
The economic impact of vision loss is extensive with associated costs for the national healthcare expenditure and individuals and households [6].
Blindness and vision impairment remain a major public health problem in Sudan. Although population-based data regarding prevalence of blindness in Sudan are rather deficient, the World Health Organization (WHO) estimates for the Eastern Mediterranean Region (EMRO) and other surveys suggest a high prevalence of blindness in the country [7,8,9].
In order to prevent and/or control blindness, healthcare workers need the knowledge and skills that relate to the prevention and control of blindness as well as the promotion of eye health. The importance of ophthalmology and its incorporation in the medical curriculum was identified several decades ago [10]. The rapid evolution in the medical field led to a persistent pressure of including these updates in the medical curriculum which in turn contributed to the reduction of time available for ophthalmology and similar subjects [11,12,13]. Identifying the crucial knowledge, skills, and attitude of graduates is the source of the medical curriculum [14, 15]. Of these, ophthalmology training at an undergraduate level is an essential component as it is a cornerstone for delivering primary eye care in the community [16].
The number of eye specialists is much smaller in the sub-Saharan Africa than in other global regions. Data from a previous study estimated a regional ratio of one ophthalmologist per 2.3 per million population. Therefore, the development of a workforce that is competent to identify, treat, and refer the most common eye conditions is essential to achieve a reduction of the prevalence of visual impairment in the region [17].
In Sudan, there is a gap in the undergraduate ophthalmology curriculum as the contents and the time spent are not adequate. The ophthalmology curriculum is conducted at the fifth year with a 2 h session weekly for one semester (duration of 5 months). It was observed that the students receive few lectures only highlighting some basic topics such as cataract and red eye with a deficient clinical practice.
The purpose of this study was to evaluate the effects of a short course in improving eye healthcare knowledge and skills among final-year medical students aiming to inform changes regarding the inclusion of ophthalmology in the medical curriculum.
Methods
Study Design and Participants
A mixed-methods interventional study was conducted among 25 final-year medical students in a public university in Khartoum State, Sudan. Participants were recruited by asking for volunteers among the class of 120 final-year medical school students.
Development and Outline of the Course
A 15 h short course was designed by expert consultant ophthalmologists. The first step was identifying the required basic knowledge and skills needed by graduates. Topics, course content, and activities were then developed. The course was then reviewed by an expert in medical education prior to the final layout of the course. The short course was composed of five sessions of 3 h each. It was conducted over a period of 2 weeks with two separated sessions per week. The course was conducted at a well-resourced conference hall of one of the tertiary eye hospitals in Khartoum State, Sudan. Sessions were presented by three senior consultant ophthalmologists and were moderated by an expert in medical education and two ophthalmic assistants.
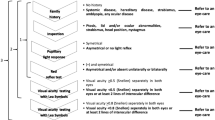
The expected outcomes of this course were that participants were able to (1) describe the general anatomy of the eye and the visual pathway, (2) describe the types and causes of blindness, (3) explain the common clinical presentation of eye disorders, (4) evaluate common eye emergencies, (5) explain how to deal with common eye emergencies, (6) evaluate common pediatric ocular morbidities, and (7) provide basic eye prevention and promotion advice.
The teaching strategy was a combination of lectures and small group discussions within a flipped classroom approach. Participants were expected to read prescribed material and/or watch prescribed videos prior to class attendance to encourage self-directed learning which has a benefit for students’ motivation, independency, and self-confidence. In-class activities focused on discussion and debate with input and feedback by the lecturers/clinicians.
Data Collection and Analysis
Data were collected at the start of the course by using a self-administered questionnaire that contained 16 closed-ended questions. The same questionnaire was used 1 month after the completion of the course. The questionnaire was developed using the AMEE guide No. 87: Developing questionnaires for educational research by Artino et al. [18] and assessed the knowledge of students towards blindness and common eye disorders, skills of diagnosing basic, and emergency eye diseases in addition to prevention and promotion skills regarding eye health. Once developed, the questionnaire was pre-tested using five healthcare students to ensure clarity of the questions. Those who participated in the pre-testing were not included in the study.
One focus group discussion (FGD) was conducted directly at the end of the course. The questions in the FGD guide were based on levels 1 (reaction) and 2 (learning) of Kirkpatrick’s four-level training model [19]. All of the students who attended the course participated in this FGD. The FGD lasted about 60 min and was facilitated by someone other than the principal researcher. The purpose of the FGD was to explore participants’ experiences regarding course content, teaching strategies, the perceived usefulness of the course, and practical arrangements as well as the general positive and negative points. The FGD was audio-taped and professionally transcribed. The transcription was checked by the FGD facilitator for accuracy, and the principal researcher only received the anonymous typed transcriptions.
The quantitative data were analyzed using Excel sheet. The Fisher exact test was performed using Statistical Package for the Social Sciences (SPSS) version 21.0 to examine any association between variables of interest. A p value of less than 0.05 was considered statistically significant. The qualitative data collected in the FGD were analyzed using an inductive, open-coding approach.
Ethical Consideration
Ethical approval was obtained from Albasar Institutional Review Board in Sudan (BIRBSA028). Each participant was asked to sign written informed consent prior participation in the study. All data including audio recordings were anonymized and kept safe in a locker, and the data on the computer were secured with a password to ensure privacy. The research results are anonymized and only used for educational and scientific purposes.
Results
Quantitative Data
Among the 25 final-year medical students who participated in this study, 15 were females and 10 were males. The mean age of the study participants was 23.5 years old. All study participants attended the full course and completed the pre- and post-course assessment tests. The average knowledge improved from 52.6% on the pre-course assessment to 86.6% on the post-course assessment. The most noticeable improvement was regarding the knowledge about visual acuity (VA) which improved by 76%, followed by the knowledge about alarming eye symptoms and signs which improved by 48%. The Fisher exact test revealed a significant association between attending the course and improvement in overall knowledge (p < 0.001) (Table 1).
The average diagnostic skills among the participants improved from 57.3% on the pre-course to 93.6% on the post-course assessment. The largest improvement after the course was in the skills of diagnosing an emergency of sudden onset red painful eye (68% improvement) followed by the skills of diagnosing reduced vision due to diabetic changes (41% improvement). The Fisher exact test revealed a significant association between attending the course and improvement in overall diagnostic skills (p < 0.001) (Table 2).
Participants’ knowledge regarding the interventions needed for common eye problems improved from 58.6% on the pre-course to 94% after the course. The chief improvement was on the treatment of sudden onset red painful eye emergency (72% improvement). The Fisher exact test revealed a significant association between attending the course and improvement in overall knowledge of the interventions needed to treat common eye problems (p < 0.001) (Table 3).
Qualitative Data
The qualitative data collected via the FGD is presented based on the first two levels of Kirkpatrick’s four-level training model (Fig. 1) [19].

Kirkpatrick’s four-level training model
The focus group interview guide had five questions with several planned probes:
Level 1 (reactions):
-
1.
Please tell me what is your general impression of this course?
-
2.
What do you think the organizers of the course could do better? (Probe for specific examples such as duration, practical arrangements, and content.)
-
3.
Is there anything that you would like to share with regard to how this course was taught? (Probe for detail such as whether they liked the didactic sessions and the balance between didactic sessions and group work.)
Level 2 (learning):
-
4.
What if anything did you find useful? (Probe for details of what they found useful.)
-
5.
Is there anything that you would like to share with regard to the content of this course? (Probe for details such as names of specific sessions or presenters or activity.)
Reaction-Level Findings
Participants were overall impressed with this course and described it as “an amazing experience.” Participants viewed the setting as very convenient and attractive and said that they experienced previously unknown approaches to teaching and participation. One session (assessment of a child’s eye) was less popular as the facilitator was not able to hold their interest and the materials used were overcrowded PowerPoint slides. The overall course was described as “intensive,” and participants suggested that it would be better if conducted across a longer period at a rate of one session a week as they felt that the course contents were rich and contained a “large amount of new information.”
Learning-Level Findings
Participants said that they are now “more confident to approach patients with an eye problem” and can now distinguish between simple, complicated, and urgent conditions. The majority of course content was new to them, especially the diabetic eye, trauma, and refractive errors. While they had some basic knowledge about the red painful eye prior to this course, this course taught them “the practical approach of diagnosis and the emergency actions” that need to be taken to save the vision.
They believe that too much time was spent in some sessions and that it would be better if this time was reduced and replaced with other clinical and practical skills. Participants were of the opinion that detailed anatomy and pathophysiology of the eye were not needed.
Participants described the course as “comprehensive and informative” but thought that actual clinical demonstrations would really add value to their learning.
Discussion
This study was conducted to establish whether a short course in eye health has the ability to increase eye care knowledge regarding the prevention of blindness and the promotion of eye health.
The participants’ overall knowledge improved significantly after the course. This study revealed a significant association between course participation and the improvement in the participants’ eye care knowledge. The biggest improvements were with regard to VA and being able to identify alarming eye signs and symptoms. These areas in ophthalmology are considered as basics in understanding and dealing with eye disorders. Visual acuity measurement is one of the essential skills to be attained by undergraduates as recommended by the Royal College of Ophthalmologists (RCOphth) [20]. It worth mentioning that the knowledge of students of whether blindness can be prevented was poor prior to the course and showed a satisfying improvement. The WHO and the International Agency for the Prevention of Blindness (IAPB) estimated that more than 75% of all causes of blindness and vision impairment are avoidable—important knowledge for those who are expected to provide primary care [21, 22].
There was an overall noticeable and significant improvement of participants’ diagnostic skills as a result of participating in the course. The greatest improvement was in the diagnoses of a sudden red painful eye. Red eye is one of the most common presenting complaints in eye clinics and emergency departments [23,24,25]. Although red eye is not always a sign of a major disorder, it is sometimes a sign of a serious visual problem [26], and the underlying cause should always be identified at an early stage [27].
Similarly, participation in this course significantly improved the knowledge of the correct interventions for common eye problems—specifically the treatment of red painful eye. The RCOphth advocates for inclusions in the medical curriculum so that graduates are able to diagnose and manage the different common causes of red eye [28]. In many cases, red eye is due to a serious underlying cause that might eventually result in a visual defect/loss if not promptly managed. Although acute red eye should be assessed and managed by a specialist, a well-trained primary healthcare worker can provide a proper classification of how serious the problem is. All doctors have had patients with red eye [29,30,31]. A study revealed that 2–3% of all cases attending primary care and emergency department are eye-related [32] and the majority of them are cases of red eye [31]. Non-ophthalmologist healthcare practitioners are often presented with eye-related cases that require an accurate medical decision [29, 30]. A study yielded that 64% of patients with red eye were erroneously diagnosed at the primary care level and 10% of these cases had serious adverse outcomes [32]. Some minor cases can be managed at the primary care level, while others should be referred to higher level with some needed actions to be taken prior to referral. In both cases, early detection and early intervention can reduce the burden on the secondary and tertiary healthcare levels and avoid or minimize clinical consequences and the financial burden on the individual [33].
The study confirmed the positive benefits for using a flipped classroom approach—such as achievement, self-confidence, and motivation [34]. Participants were critical of the didactic teacher-centered approach that was followed in the session on the child’s eye. In this case, the presenter overly depended on text-dense PowerPoint slides rather than facilitating learning via application of the theory to a practical clinical scenario. A meta-analysis of 48 studies identified no difference in students’ learning between PowerPoint-driven sessions and classical teaching [35].
All participants found that the course introduced new valuable content which in turn enhanced their confidence in dealing with patients with eye complaints. This finding supports the work done by Succar et al. who showed that an amendment of the ophthalmic content, which had declined, in the medical curriculum resulted in an increase in academic performance and a higher degree of student satisfaction [36]. Participants in this study thought that the sessions on detailed eye anatomy and physiology were not really needed. One possible reason could be that this content is already included in anatomy and physiology.
It is difficult to draw conclusions on the quality of the training as there is no standard for the content or duration regarding ophthalmology in undergraduate medical curriculum. But the improvement in knowledge and diagnostic skills, especially in terms of the most common presenting complaints, is a positive reflection of the deliberate choice of topics for inclusion in the curriculum. However, it is not yet clear whether the choice of 15 h is the optimal duration as no other duration was tested. What is clear however is that the participants suggested that the allocation of time to each topic needs revision and that some topics need not be included at all. It is suggested that the study should be repeated with a larger group in order to determine if these suggestions should be taken into consideration when the curriculum is reviewed by a panel of experts. The authors provisionally agree with the insights provided by the participants and also support their suggestion of hands-on practical skill sessions as this would allow for evaluation at the third level of Kirkpatrick’s model: behavior. After all, the ultimate goal of strengthening ophthalmology training in the undergraduate medical curriculum is that graduates will be able to diagnose and treat eye conditions in real-life settings.
Primary eye care is the delivery of the first level of care for eye-related conditions. It is of the utmost importance to strengthen the primary eye care services especially in countries like Sudan. Sudan is a large country and most of the hospitals and specialists who can provide tertiary care are in the capital city, Khartoum. As a result, the majority (almost 70%) of eye care services are provided in the capital city, while the majority of the population have limited access to eye care services [37] and are dependent on the knowledge and skills of those who work in these settings. The provision of primary care needs to be extended to include the provision of efficient, knowledgeable, comprehensive, and effective level of services to ensure the best outcomes [38].
Conclusion
A well-designed short course in ophthalmology significantly improves the levels of medical students’ knowledge and skills towards eye health. The results of this study provide the basis of an ophthalmology curriculum that could be included as a standard component in the national medical curriculum—something that has not been done before. Ultimately, such an inclusion has the potential to contribute towards the reduction of blindness in the country in the long term.
Limitations
There are some limitations to this study, mainly related to COVID-19 pandemic. These limitations include the small number of participants as only 25 volunteer students could attend the sessions. However, it is believed that the achieved results are valid and representative of final-year medical students from the public university in Khartoum State, Sudan. Another limitation is that the pre- and post-course assessments were paper-based tests. It would have been preferable if the skills, especially the interventional ones, could have been assessed through practical simulation. Due to the COVID-19 pandemic, no patients could be included in the training or assessment, but the course included videomaterial that showed the practical skills in an attempt to overcome this limitation.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- FGD:
-
Focus group discussion
- VA:
-
Visual acuity
- RCOphth:
-
Royal College of Ophthalmologists
- WHO:
-
World Health Organization
- SPSS:
-
Statistical Package for the Social Sciences
- IAPB:
-
International Agency for the Prevention of Blindness
References
Center for Disease Control and Prevention. Vision impairment and blindness. 2018. Retrieved from: https://www.cdc.gov/visionhealth/vehss/data/studies/vision-impairment-and-blindness.html#:~:text=**Blindness%20is%20defined%20by,of%2020%2F200%20or%20worse. Accessed 11 Nov 2020.
WHO. Blindness and vision impairment. 2020. Retrieved from: https://www.who.int/health-topics/blindness-and-vision-loss#tab=tab_1. Accessed 11 Nov 2020.
WHO. Visual impairment and blindness. Fact Sheet N°282. 2020. Retrieved from: http://www.who.int/mediacentre/factsheets/fs282/en/. Accessed 10 Nov 2020.
Center for Disease Control and Prevention (CDC). Blindness and vision impairment. 2020. Retrieved from:https://www.cdc.gov/healthcommunication/toolstemplates/entertainmented/tips/Blindness.html. Accessed 10 Nov 2020.
Ishtiaq R, Chaudhary MH, Rana MA, Jamil AR. Psychosocial implications of blindness and low vision in students of a school for children with blindness. Pak J Med Sci. 2016;32(2):431–4.
National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Committee on Public Health Approaches to Reduce Vision Impairment and Promote Eye Health. Making eye health a population health imperative vision for tomorrow. Washington (DC): NCBI; 2016. Retrieved from: https://www.ncbi.nlm.nih.gov/books/NBK385157/. Accessed 10 Nov 2020.
Binnawi K, Mohamed A, Alshafae B, Abdalla Z, Alsanosi M, Alnoor A, et al. Prevalence and causes of blindness and visual impairment in population aged 50 years and over in North Kordofan State, Sudan. Al-basar Int J Ophthalmol. 2015;3(1):6–10.
Ibrahim M, Elnimeiri M. Risk factors of blindness in Sudan 2019. IJPSAT. 2019;15(2):195–9. https://doi.org/10.52155/ijpsat.v15.2.1143.
Ibrahim M. Social determinants of blindness in Sudan- 2019. Al-basar Int J Ophthalmol. 2020;7(1):1–3. https://doi.org/10.4103/bijo.bijo_5_20.
Byers WG. The place of ophthalmology in the undergraduate medical curriculum. Br Med J. 1922;2:4–6.
Crombie AL. Ophthalmology in the undergraduate curriculum. Trans Ophthalmol Soc U K. 1976;96:33–4.
Cordes FC. The need for revision of undergraduate teaching in ophthalmology. Am J Ophthalmol. 1953;36:861–3. https://doi.org/10.1016/0002-9394(53)90192.
Albert DM, Bartley GB. A proposal to improve ophthalmic education in medical schools. Ophthalmology. 2014;121:1157–9. https://doi.org/10.1016/j.ophtha.2014.04.003.
Al-Elq AH. Medicine and clinical skills laboratories. J Family Community Med. 2007;14:59–63.
Lofaso DP, DeBlieux PM, DiCarlo RP, Hilton C, Yang T, Chauvin S. Design and effectiveness of a required pre-clinical simulation-based curriculum for fundamental clinical skills and procedures. Med Educ Online. 2011;16:7132.
Masanganise R, Samkange C, Mukona D, Aagaard E. Competency based ophthalmology training curriculum for undergraduate medical students in Zimbabwe. Cent Afr J Med. 2015;61(5–8):44–8. PMID: 29144080.
Palmer JJ, Chinanayi F, Gilbert A, Pillay D, Fox S, Jaggernath J, Naidoo K, Graham R, Patel D, Blanchet K. Mapping human resources for eye health in 21 countries of sub-Saharan Africa: current progress towards VISION 2020. Hum Resour Health. 2014;15(12):44. https://doi.org/10.1186/1478-4491-12-44. PMID: 25128163; PMCID: PMC4237800.
Artino A, Rochelle J, Dezee K, Gehlbach H. Developing questionnaires for educational research: AMEE Guide No. 87. Med Teach. 2014;36(6):463–74. https://doi.org/10.3109/0142159X.2014.889814.
Ardent Learning. What is the Kirkpatrick model? Learn the 4 levels of evaluation. 2020. Retrieved 15 November 2020 from: https://www.ardentlearning.com/blog/what-is-the-kirkpatrick-model.
RCOphth. Undergraduate ophthalmology. The Royal College of Ophthalmologists. 2013. Retrieved 15 November 2020 from: https://www.rcophth.ac.uk/training/undergraduate-ophthalmology/.
The National Agency for the prevention of Blindness (IAPB). “Avoidable blindness” Set to Increase in Future. 2017. Retrieved 15 November 2020 from: https://www.iapb.org/news/avoidable-blindness-set-to-increase-in-future/.
Amador M, Torres J. Visual disability and causes of preventable blindness. 2019. https://doi.org/10.5772/intechopen.88793. Retrieved 15 November 2020 from: https://www.intechopen.com/books/topics-in-primary-care-medicine/visual-disability-and-causes-of-preventable-blindness.
Lawan A. Causes of red eye in Aminu Kano Teaching Hospital. Kano-Nigeria Niger J Med. 2009;18:184–5.
Seth D, Khan FI. Causes and management of red eye in pediatric ophthalmology. Curr Allergy Asthma Rep. 2011;11:212–9.
Mahmood AR, Narang AT. Diagnosis and management of the acute red eye. Emerg Med Clin North Am. 2008;26:35–55.
Farokhfar A, Dailami KN, HeidariGorji MA, Aghaie N. Epidemiology and symptoms of red eyes in patients from Northern Iran. J Nat Sci Biol Med. 2015;6(2):369–71. https://doi.org/10.4103/0976-9668.160009. PMID: 26283832; PMCID: PMC4518412.
Welch JF, Dickie AK. Red alert: diagnosis and management of the acute red eye. J R Nav Med Serv. 2014;100:42–6.
Hill S, Dennick R, Amoaku W. Present and future of the undergraduate ophthalmology curriculum: a survey of UK medical schools. Int J Med Educ. 2017;2(8):389–95. https://doi.org/10.5116/ijme.59ac.f69b. PMID: 29103017; PMCID: PMC5694697.
Pflipsen M, Massaquoi M, Wolf S. Evaluation of the painful eye. Am Fam Physician. 2016;93:991–8.
Teo MA. Improving acute eye consultations in general practice: a practical approach. BMJ Qual Improv Rep. 2014;3(1):u206617–12852.
Cronau H, Kankanala RR, Mauger T. Diagnosis and management of red eye in primary care. Am Fam Physician. 2010;81:137–44.
Frings A, GeerlingG SM. Red eye: a guide for non-specialists. Dt Arztebl Int. 2017;114(17):302–12. https://doi.org/10.3238/arztebl.2017.0302.
Foster A. Red eye: the role of primary care. Community Eye Health J. 2005;18(53):69–84.
Awidi A, Paynter M. The impact of a flipped classroom approach on student learning experience. Comput Educ. 2019;128:269–83. https://doi.org/10.1016/j.compedu.2018.09.013.
Baker J, Goodboy A, Bowman N, Wright A. Does teaching with PowerPoint increase students’ learning? A meta-analysis. Comput Educ. 2018;126:376–87. https://doi.org/10.1016/j.compedu.2018.08.003.
Succar T, McCluskey P, Grigg J. Enhancing medical student education by implementing a competency-based ophthalmology curriculum. Asia Pac J Ophthalmol (Phila). 2017;6(1):59–63. https://doi.org/10.22608/APO.2016102. PMID: 28161917.
Alrasheed S, Naidoo K, Clarke-Farr P, Binnawi K. Building consensus for the development of child eye care services in South Darfur State of Sudan using the Delphi technique. Afr J Prim Health Care Fam Med. 2018;10(1):e1–9. https://doi.org/10.4102/phcfm.v10i1.1767. PMID: 30456975; PMCID: PMC6244194.
Riad S, Dart J, Cooling R. Primary care and ophthalmology in the United Kingdom. Br J Ophthalmol. 2003;87:493–9.
Author information
Authors and Affiliations
Contributions
M. I. designed the study; collected, analyzed, interpreted the data; and wrote the first version of this article. J. W. supervised the project, advised on the design of the intervention, reviewed the results, and contributed to the revisions of this article. Both authors read and approved the final version of this article.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
Ethical approval was obtained from Albasar Institutional Review Board in Sudan (BIRBSA028). Each participant was asked to sign informed written consent prior to study.
Consent for Publication
Written informed consent was obtained from the participants for publication of this article. A copy of the written consent will be available for review by the editor-in-chief of this journal.
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ibrahim, M.K.M., Wolvaardt, J.E. Outcomes of a Short Course in Improving Eye Healthcare Knowledge and Skills Among Final-Year Medical Students. Med.Sci.Educ. 32, 847–853 (2022). https://doi.org/10.1007/s40670-022-01576-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40670-022-01576-z