
Abstract
Objective
Suicidal ideation is an important public health challenge among people living with HIV (PLWH) across the world and in China. HIV stigma, depression, and self-esteem have been associated with suicidal ideation. However, the underlying mechanisms remain not fully understood.
Methods
Study data were derived from a sample of 465 PLWH in China. Suicidal ideation after HIV diagnosis was used as outcome variable. HIV stigma, depressive symptoms, and self-esteem were measured using reliable instruments and used as predictor, mediator, and moderator, respectively. Mediation and moderated mediation model were used for data analysis.
Results
31.6% of PLWH in China had suicidal ideation after HIV diagnosis. The association between perceived HIV stigma and suicidal ideation was partially mediated by depression (indirect effect = 0.02, 95% CI = [0.02, 0.03]) with the path from perceived HIV stigma to depressive symptoms being moderated by self-esteem (interaction effect = − 0.02, 95% CI [− 0.03, − 0.01]).
Conclusions
Study findings suggested a mediation mechanism of HIV stigma on suicidal ideation through depressive symptoms, and self-esteem might weaken the mediation mechanism by moderating the perceived HIV stigma-depressive symptoms pathway.
Similar content being viewed by others

Introduction
Suicidal Ideation Among People Living with HIV
Suicide is a major public health problem worldwide and in China [1, 2]. Suicidal ideation is a predecessor of suicide and is common among PLWH worldwide, and data from a meta-analysis showed that the estimated prevalence of suicidal ideation is 20.9% [3]. Studies in different countries differed in the prevalence of suicidal ideation with 8.6% in the United States (US) [4], 31% in the UK [5], 23.3% in Indonesia [6], 21% in Argentina [7], and 8.2% in Ethiopia [8]. Data from China showed that the prevalence of suicidal ideation among PLWH was 25%, higher than 6%, the prevalence of suicidal ideation in the general population [9]. Prior to the introduction of combination antiretroviral therapy (cART), studies had shown an association between HIV infection and suicide [10, 11], so studying the factors associated with suicidal ideation among PLWH can better prevent and control suicide and promote the physical and mental health of PLWH [12].
Perceived HIV Stigma and Suicidal Ideation Among PLWH
It is quite common for PLWH to suffer from various types of HIV-related stigma [13]. A study conducted in Sichuan Province, China, showed that PLWH perceived various levels of HIV stigma, with the average level being moderate [14]. One study conducted among 346 PLWH in the US showed that they also perceived moderate to high levels of HIV stigma [12]. Several studies have shown that perceived HIV stigma can lead to various psychological negative outcomes, particularly suicidal ideation [8, 15]. For example, a study conducted in Tanzania, Africa, showed a significant correlation between suicidal ideation and HIV stigma [16]. One study from South Africa showed that HIV stigma was a risk factor for suicidal ideation among PLWH [17]. Another study from China suggested that HIV stigma increased the likelihood of suicidal states [18]. However, the underlying mechanisms of the relationship between HIV stigma and suicidal ideation were largely unknown.
Potential Mediation Mechanism Between Perceived HIV Stigma, Depressive Symptoms, and Suicidal Ideation
Many studies have shown that PLWH who experience high levels of HIV stigma are more likely to develop depression [19, 20]. For example, a cohort study from the US showed that HIV-related stigma could increase the odds of PLWH depression [20]. Moreover, depression is associated with various psychological negative outcomes, including suicidal ideation [21, 22]. A meta-analysis of longitudinal studies showed that PLWH with depression are more likely to experience suicidal ideation (OR = 1.96) [23]. On the other hand, a study conducted in the US showed that improving depressive symptoms can reduce suicidal ideation [24]. With the above evidence, we hypothesized that there might exist a mediation mechanism between perceived HIV stigma, depression, and suicidal ideation.
Moderation Effect of Self-esteem
In addition to the proposed mediation model, many personality-related factors may buffer the relationship, including self-esteem [25, 26]. Self-esteem is referred to the attitude toward the self, self-efficacy, self-acceptance, and self-worth [27]. Self-esteem, especially positive and stable self-esteem, exerts effects in tackling life stress. Individuals with greater self-esteem are more likely to be good problem solvers and have greater resilience when dealing with stressors [28]. Self-esteem has been proven to buffer negative emotions at special times, e.g., coronavirus disease 2019 (COVID-19) quarantine period [29], as well as in various populations: the general population [30], adolescents [31], female college students [32], and obese couples [33]. As a marginalized population, HIV stigma is a significant predictor of poor health outcomes, including suicide, among PLWH [16]. Previous studies suggested that self-esteem may act as a moderating factor, buffering the effects of HIV stigma on psychological well-being [34, 35]. Given that self-esteem has been commonly studied as a moderator in mental health research [29,30,31,32], we hypothesized that self-esteem might moderate the effect of perceived HIV stigma on suicidal ideation.
Although HIV stigma, depressive symptoms, and self-esteem have been previously reported to have an implication on suicidal ideation in PLWH [25, 36], the underlying mediating and moderating mechanisms responsible for these associations are poorly understood. By the end of 2018, it is estimated that the number of PLWH/AIDS in China had exceeded one million and would continue to grow [37]. Several studies in China have shown that the rate of suicidal ideation among PLWH since diagnosis ranges from 25 to 32.4% [9, 18, 38]. With such a high proportion of suicidal ideation, it is necessary to understand the impact of perceived HIV stigma on suicidal ideation among PLWH in China and the mechanisms underlying the association for providing evidence for taking targeted measures to improve the psychological health of PLWH.
Purpose of the Study
This study aims to investigate the potential mediation relationship between HIV stigma, depression, and suicidal ideation, as well as the moderation effect of self-esteem on the mediation mechanism among PLWH in China (Fig. 1). The ultimate goal is to provide evidence for public health interventions against suicide among PLWH in China.

Hypothetical model of perceived HIV stigma and suicidal ideation among PLWH
Methods
Participants and Sampling
The participants in this study were PLWH who were as follows:(1) age 18 years or older; (2) diagnosed and registered in the Chinese AIDS Prevention and Control Information System; (3) agreed to enroll in the survey. Participants were recruited at the Second Affiliated Hospital of Southeast University in Nanjing, China, using the convenience sampling technique from July to August 2016. When PLWH go to the hospital, they will be asked if they would like to participate in a study, and only individuals who agree to participate and sign the informed consent will be enrolled. In China, all individuals diagnosed with HIV infection should be registered in the Chinese AIDS Prevention and Control Information System; thus, they can go to designated medical institutions to receive free antiviral treatment drugs. Because HIV prevalence in Chinese males was more than twice that of females, we recruited more males than females in this study [39].
Data Collection
Data collection was implemented through a self-administered paper–pencil questionnaire. The survey was anonymous and voluntary. Individuals were also informed that they could quit the survey whenever they wanted. Upon completion of the survey, each participant would receive a supermarket gift card as an incentive (50 RMB value (approximately $8)). This study was approved by the Ethics Committee of Wuhan University School of Medicine.
Measurements
Demographic and Clinical Characteristics
Demographic characteristics of PLWH included age (in years), gender (male/female), marital status (unmarried, married, divorced/widowed), place of residence (urban/rural), education level (high school or lower/junior college or higher), monthly disposable income (≤ 3000/3001–5000/ > 5000), and occupation (in work/retired or unemployed or student). Clinical variables included duration of infection (in months) and duration of highly active antiretroviral therapy (HAART) (in months).
Perceived HIV Stigma
The HIV Stigma Revised Scale was used to measure perceived HIV stigma [40]. The perceived stigma scale consists of 32 items in four dimensions: enacted stigma (11 items, typical item: “I get the emotional help and support I need from my family”), disclosure concerns, (8 items, typical item: “I work hard to keep my HIV/AIDS a secret”), negative self-image (7 items, typical item: “Having HIV/AIDS makes me feel unclean”), and concerns with public attitudes (6 items, typical item: “Most people think that a person with HIV/AIDS is disgusting”). A 4-point Likert scale is employed to assess each item, ranging from 1 (strongly disagree) to 4 (strongly agree). Responses for all 32 items were calculated to obtain mean scores, with higher scores indicating more severe perceived HIV stigma. The Cronbach’s alpha in this study was 0.92.
Depressive Symptoms
The Center for Epidemiologic Studies Depression (CES-D) scale was used to measure depressive symptoms experienced by the respondent during the past 7 days [41]. The CESD scale consists of 20 items, including 16 forward items (typical item: “I felt fearful”) and four reverse items (typical item: “I felt hopeful about the future”). A 4-point Likert scale is employed to assess each item, ranging from “0 = (less than a day or never” to “3 = 5–7 days.” The total score was obtained by summing all item scores, with higher scores indicating more severe depressive symptoms. The Cronbach’s alpha was 0.91 in this study.
Self-esteem
The Rosenberg self-esteem scale (RSE) was used to measure self-esteem [42]. The Rosenberg self-esteem scale is commonly utilized in studies of PLWH and other mental health studies to measure responders’ self-esteem levels [43, 44]. The scale consists of 10 items (typical item: “On the whole, I am satisfied with myself”), using a 4-point Likert scale, ranging from 0 (strongly disagree) to 3 (strongly agree). Total score was calculated, with higher scores indicating greater self-esteem. The Cronbach’s alpha was 0.91 in this study.
Suicidal Ideation
Suicidal ideation was measured using the question “Have you ever had suicidal ideation after you found out you were infected with HIV” (yes = 1, no = 0).
Statistical Analysis
Descriptive statistics (e.g., mean, standard deviation, frequency, percentage) were computed to present the demographic characteristics. Correlation analysis was used to investigate the correlation among perceived HIV stigma, depressive symptoms, self-esteem, and suicidal ideation. Mediation analysis was used to examine the indirect effect of depressive symptoms in the path of perceived HIV stigma on suicidal ideation. The moderation effect of self-esteem on the hypothesized mediation model was analyzed using a moderated mediation model. The covariates in the moderated mediation analysis included demographic characteristics such as age, gender, education, monthly disposable income, and marital status. The mediation and moderated mediation modeling analysis were implemented using the Hayes’ PROCESS macro [45]. All statistical analyses were implemented using SPSS (version 26.0, IBM Corp). We then used VanderWeele and Ding’s methods to perform an E-value analysis to determine the robustness of the estimated associations [46]. The E-value describes the minimum strength of association on the OR scale (between the presumed confounders and exposure, and between the presumed confounders and outcome) that is needed to account for the observed exposure-outcome association. E-values were computed with an online E-value calculator (https://mmathur.shinyapps. io/evalue/).
Results
Demographic and Clinical Characteristics of the Study Sample
Results in Table 1 show that among the total sample of 465 PLWH, 95.3% were male with age ranging from 18 to 76 years and a mean age of 36.4 ± 12.0 years. 53.5% were unmarried, and approximately 40% of the participants had an educational level of high school or lower, while the rest had junior college or higher education. Most of the participants were employed (78.7%), and 59.1% were from urban areas. Nearly two-thirds of the participants had a monthly disposable income above 3000 RMB (approximately $460), and 75.1% were men who have sex with men. Nearly half (48.8%) had been diagnosed with HIV for more than 24 months, and most of the participants (67.5%) had a duration of no more than 24 months on highly active antiretroviral therapy (HAART). Among the 465 PLWH, 147 of them (31.6%) had suicidal ideation.
Bivariate Correlations
Variables for bivariate correlation analysis included perceived HIV stigma, depressive symptoms, self-esteem, and suicidal ideation. The mean and SD of each variable and the correlations between the variables are presented in Table 2. Correlation analysis results show that perceived HIV stigma was positively correlated with depressive symptoms (r = 0.43, P < 0.001) and suicidal ideation (r = 0.37, P < 0.001), and depressive symptoms were positively correlated with suicidal ideation (r = 0.41, P < 0.001). Additionally, perceived HIV stigma (r = − 0.37, P < 0.001), depressive symptoms (r = − 0.61, P < 0.001), and suicidal ideation (r = − 0.37, P < 0.001) were negatively correlated with self-esteem.
Mediation Modeling Analysis
Results in Fig. 2 and Table 3 show that perceived HIV stigma was positively associated with depressive symptoms (β = 0.39, t = 10.12, P < 0.001). This, for its part, was a predictor of suicidal ideation (β = 0.06, z = 5.73, P < 0.001). Perceived HIV stigma had a positive association with suicidal ideation as well (β = 0.06, z = 5.04, P < 0.001). The relationship between perceived HIV stigma and suicidal ideation is partly mediated by depressive symptoms (Indirect effect = 0.02, 95% CI [0.02, 0.03]).

Mediated model for perceived HIV stigma, depressive symptoms, and suicidal ideation among PLWH. (Covariates were controlled: age, gender, education, monthly disposable income, and marital status. ***P < 0.001.)
Moderated Mediation Modeling
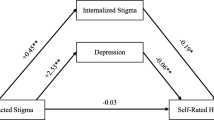
Results in Fig. 3, Table 4, and Fig. 4 show that self-esteem negatively moderated the path from perceived HIV stigma to depressive symptoms (interaction effect = − 0.02, 95% CI [− 0.03, − 0.01]), but did not moderate the other two paths.

Moderated mediation model for perceived HIV stigma, depressive symptoms, self-esteem, and suicidal ideation among PLWH. (Covariates were controlled: age, gender, education, monthly disposable income, and marital status. **P < 0.01, ***P < 0.001.)

The final moderated mediation model with statistically significant pathways. (Covariates were controlled: age, gender, education, monthly disposable income, and marital status. **P < 0.01, ***P < 0.001.)
Sensitivity Analysis
Results from the sensitivity analysis show that for the estimated association between perceived HIV stigma and depressive symptoms (OR 1.48), the E-value was 2.32. For the estimated association between perceived HIV stigma and suicidal ideation (OR 1.04), the E-value was 1.32. For the estimated association between depressive symptoms and suicidal ideation (OR 1.04), the E-value was 1.32. These results suggested that residual confounding could explain the observed association if there was an unmeasured covariate with an association (OR) at least equal to the E-value of the exposure and outcome.
Discussion
There is considerable empirical support for the impact of perceived HIV stigma on suicidal ideation [8, 16, 17]. However, the association between perceived HIV stigma and suicidal ideation and the mechanisms that moderate and mediate this association were not fully elucidated. Hence, mediation and moderated mediation models were used in this study to determine how perceived HIV stigma, depressive symptoms, and self-esteem interact to influence suicidal ideation. The mediation analysis results indicated that depressive symptoms mediated the relationship between perceived HIV stigma and suicidal ideation. The moderated mediation analysis results revealed that self-esteem moderated the relationship between perceived HIV stigma and suicidal ideation via depressive symptoms. However, self-esteem did not play a moderating role between perceived HIV stigma and depressive symptoms with suicidal ideation.
First, as hypothesized, perceived HIV stigma was positively associated with suicidal ideation, and depressive symptoms can partially mediate this relationship. This association is in line with a study conducted among PLWH in Guangzhou, China [18]. Similar findings were also observed among PLWH in South Africa [17] and among sexual minorities in the US [47], where the association between stigma and suicidal ideation was mediated by depression. Depressive symptoms are prevalent when PLWH suffer from experiences or feelings of prejudice or stigma [48, 49], leading to reduced quality of life and life expectancy [50]. Therefore, those with higher depressive symptoms had more suicidal ideation and were at greater risk of committing suicide [51].
Second, consistent with our hypothesis, self-esteem negatively moderated the effect of perceived HIV stigma on depressive symptoms. This is to say that individuals with both higher perceived HIV stigma and higher self-esteem are less likely to develop depressive symptoms. Compared to the general population, PLWH are 2–3 times more likely to develop depression and are more likely to experience higher levels of social isolation and the risk of mental health problems [50]. In the face of stress and trauma, self-esteem plays an important role as a coping strategy that enhances an individual’s adaptability [52]. A better ability to adapt to stress could alleviate the adverse effects of HIV infection and diminish the occurrence of depression in PLWH [53]. Thus, improving self-esteem can reduce depression, and individuals with high levels of self-esteem may be less likely to suffer from depressive symptoms.
The findings have implications for intervention targeted at PLWH. First, in addition to taking measures to improve the external environment of stigma, attention is now being paid to reduce perceived stigma from the perspective of PLWH by providing psychological support. Second, programs targeting this population need to specifically increase self-esteem to reduce the negative consequences of HIV stigma. As one solution, a website could be developed to provide counseling aimed at meeting the self-esteem enhancement needs of PLWH in China. Public health workers can also provide self-esteem enhancing counseling by working with volunteers to provide counseling services to PLWH in local communities and hospitals.
Limitations
There were several limitations to this study. First, the data from the cross-sectional survey had restricted the ability to infer causality. Second, the vast majority of the present sample were men who have sex with men, with a limited number of women, and there may be gender bias in the inference of the findings, and future studies should include more females. Third, the assessment of suicidal ideation was not limited to a specific time frame and may have overestimated suicidal ideation, which should be interpreted with more caution when interpreting the results.
Finally, this study examined the effects of self-esteem in general rather than specific dimensions of self-esteem (e.g., self-acceptance or self-efficacy). Future efforts should incorporate these dimensions to identify whether different dimensions of self-esteem have different effects on depressive symptoms and suicidal ideation.
Conclusions
Our results indicate that depressive symptoms partially mediate the association between perceived HIV stigma and suicidal ideation. Furthermore, the results from this study reveal that self-esteem reduced the effect of perceived HIV stigma on depressive symptoms, which in turn reduced the incidence of suicidal ideation among PLWH.
Data Availability
Data from a cross-sectional survey in Nanjing, China.
Code Availability
SPSS (version 25.0).
References
Klonsky ED, May AM, Saffer BY. Suicide, suicide attempts, and suicidal ideation. Annu Rev Clin Psychol. 2016;12:307–30.
Mew EJ, et al. The global burden of fatal self-poisoning with pesticides 2006–15: systematic review. J Affect Disord. 2017;219:93–104.
Pei J-H, et al. Prevalence of suicidal ideation, suicide attempt, and suicide plan among HIV/AIDS: a systematic review and meta-analysis. J Affect Disord. 2021;292:295–304.
Quinlivan EB, et al. Suicidal ideation is associated with limited engagement in HIV care. AIDS Behav. 2017;21(6):1699–708.
Sherr L, et al. Suicidal ideation in UK HIV clinic attenders. AIDS (London, England). 2008;22(13):1651–8.
Ophinni Y, et al. Suicidal ideation, psychopathology and associated factors among HIV-infected adults in Indonesia. BMC Psych. 2020;20(1):255.
Mandell LN, et al. Suicidal ideation among adults re-engaging in HIV care in Argentina. AIDS Behav. 2019;23(12):3427–34.
Bitew H, et al. Suicidal ideation, attempt, and determining factors among HIV/AIDS patients, Ethiopia. Depress Res Treat. 2016;2016:8913160.
Bi F, et al. The relationship between social support and suicidal ideation among newly diagnosed people living with HIV: the mediating role of HIV-related stress. Psychol Health Med. 2020;6:724–34.
Alfonso CA, et al. HIV seropositivity as a major risk factor for suicide in the general hospital. Psychosomatics. 1994;35(4):368–73.
Pugh K, O’Donnell I, Catalan J. Suicide and HIV disease. AIDS Care. 1993;5(4):391–400.
Brown MJ, et al. Ways of coping and perceived HIV-related stigma among people living with HIV: moderation by sex and sexual orientation. Psychol Health Med. 2020;25(7):867–78.
Friedland BA, et al. The People Living with HIV Stigma Index 2.0: generating critical evidence for change worldwide. AIDS. 2020;34(Suppl 1):S5–18.
Yang H, et al. HIV-related stigma among people living with HIV in Liangshan Yi Autonomous Prefecture, China. J Assoc Nurses AIDS Care. 2020;31(2):199–207.
Parcesepe A, et al. HIV-related stigma, social support, and psychological distress among individuals initiating ART in Ethiopia. AIDS Behav. 2018;22(12):3815–25.
Knettel BA, et al. Exploring patterns and predictors of suicidal ideation among pregnant and postpartum women living with HIV in Kilimanjaro, Tanzania. AIDS. 2020;34(11):1657–64.
Casale M, et al. Suicidal thoughts and behaviour among South African adolescents living with HIV: can social support buffer the impact of stigma? J Affect Disord. 2019;245:82–90.
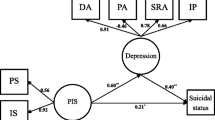
Zeng C, et al. A structural equation model of perceived and internalized stigma, depression, and suicidal status among people living with HIV/AIDS. BMC Public Health. 2018;18(1):138.
Turan B, et al. Buffering internalization of HIV stigma: implications for treatment adherence and depression. J Acquir Immune Defic Syndr. 2019;80(3):284–91.
Algarin AB, et al. Enacted HIV-related stigma’s association with anxiety & depression among people living with HIV (PLWH) in Florida. AIDS Behav. 2021;25(1):93–103.
Janice K. Kiecolt-Glasera RG Depression and immune function central pathways to morbidity and mortality. J Psychosom Res. 2002;53:4.
Evans DL, et al. Mood disorders in the medically ill: scientific review and recommendations. Biol Psychiat. 2005;58(3):175–89.
Ribeiro JD, et al. Depression and hopelessness as risk factors for suicide ideation, attempts and death: meta-analysis of longitudinal studies. Br J Psych. 2018;212(5):279–86.
Keilp JG, et al. Suicidal ideation declines with improvement in the subjective symptoms of major depression. J Affect Disord. 2018;227:65–70.
Wang W, et al. Psychosocial health and suicidal ideation among people living with HIV/AIDS: a cross-sectional study in Nanjing China. PLoS One. 2018;13(2):e0192940.
Peltekis A, Koulentianou M. Clinical presentation and requests for support of people with HIV/AIDS seeking counselling and psychotherapy in Greece. Psychiatrike=Psychiatriki. 2019;30(2):120–8.
Dore C. Self esteem : concept analysis. Rech Soins Infirm. 2017;129:18–26.
Turner RJ, Roszell P. Psychosocial resources and the stress process. In: Avison WR, Gotlib IH, editors. Stress and mental health: contemporary issues and prospects for the future. New York: Plenum Press; 1994.
Rossi A, et al. The anxiety-buffer hypothesis in the time of COVID-19: when self-esteem protects from the impact of loneliness and fear on anxiety and depression. Front Psychol. 2020;11:2177.
Edmondson D, et al. Self-esteem and the acute effect of anxiety on ambulatory blood pressure. Psychosom Med. 2015;77(7):833–41.
Soler L, et al. Impact of poly-victimization on mental health: the mediator and/or moderator role of self-esteem. J Interpers Violence. 2013;28(13):2695–712.
Beekman JB, Stock ML, Howe GW. Stomaching rejection: self-compassion and self-esteem moderate the impact of daily social rejection on restrictive eating behaviours among college women. Psychol Health. 2017;32(11):1348–70.
Fang M, et al. The role of gender and self-esteem as moderators of the relationship between stigma and psychological distress among infertile couples. Psychol Health Med. 2020;26:1–14.
Kalomo EN. Associations between HIV-related stigma, self-esteem, social support, and depressive symptoms in Namibia. Aging Ment Health. 2018;22(12):1570–6.
Chan RCH, Mak WWS. Cognitive, regulatory, and interpersonal mechanisms of HIV stigma on the mental and social health of men who have sex with men living with HIV. Am J Mens Health. 2019;13(5):1557988319873778.
Wingood GM, et al. HIV discrimination and the health of women living with HIV. Women Health. 2007;46(2–3):99–112.
Lyu P, Chen FF. National HIV/AIDS epidemic estimation and interpretation in China. Zhonghua Liu Xing Bing Xue Za Zhi. 2019;40(10):1191–6.
Tang X, et al. Structural equation modeling analysis of social support, coping strategies, depression and suicidal ideation among people living with HIV/AIDS in Changsha, China. Neuropsychiatr Dis Treat. 2018;14:2923–30.
Global Burden of Disease Collaborative Network. Global burden of disease study 2019 (GBD 2019) results, 2020. Available from http://ghdx.healthdata.org/gbd-results-tool
Bunn JY, et al. Measurement of stigma in people with HIV: a reexamination of the HIV Stigma Scale. AIDS Educ Prev. 2007;19(3):198–208.
Radloff LS. The CES-D scale:a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401.
Rosenberg M. Society and the adolescent self-image. Princeton: Princeton University Press; 1965.
Kalemi G, et al. Stigma and self-esteem: a case of HIV-positive sex-workers. Psychiatrike=Psychiatriki. 2017;28(1):67–74.
De Weerdt J, Beegle K, Dercon S. Orphanhood and self-esteem: an 18-year longitudinal study from an HIV-affected area in Tanzania. J Acquir Immune Defic Syndr. 2017;76(3):225–30.
Hayes AF. Introduction to mediation, moderation, and conditional process analysis. New York: Guilford Press; 2013.
VanderWeele TJ, Ding P. Sensitivity analysis in observational research: introducing the E-value. Ann Intern Med. 2017;167(4):268–74.
Kota KK, et al. Psychosocial mediators of perceived stigma and suicidal ideation among transgender women. BMC Public Health. 2020;20(1):125.
Earnshaw VA, et al. HIV stigma, depressive symptoms, and substance use. AIDS Patient Care STDS. 2020;34(6):275–80.
Rueda S, et al. Examining the associations between HIV-related stigma and health outcomes in people living with HIV/AIDS: a series of meta-analyses. BMJ Open. 2016;6(7):e011453.
Nanni MG, et al. Depression in HIV infected patients: a review. Curr Psych Rep. 2015;17(1):530.
Black J, et al. Test of a clinical model of poor physical health and suicide: the role of depression, psychosocial stress, interpersonal conflict, and panic. J Affect Disord. 2019;257:404–11.
Martínez-Martí ML, Ruch W. Character strengths predict resilience over and above positive affect, self-efficacy, optimism, social support, self-esteem, and life satisfaction. J Posit Psychol. 2016;12(2):110–9.
Spies G, Seedat S. Depression and resilience in women with HIV and early life stress: does trauma play a mediating role? A cross-sectional study. BMJ Open. 2014;4(2):e004200.
Acknowledgements
We appreciate the support of the Second Affiliated Hospital of Southeast University and the willingness of all participants in this study to share their life experiences.
Funding
This study was supported by the National Natural Science Foundation of China (Grant No. 81673196) and the Humanities and Social Science Foundation of Ministry of Education (Grant No. 15YJAZH094).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval
Procedures were approved by the Medical Ethics Committee of Wuhan University, China.
Consent to Participate
Written consent was obtained from all participants.
Consent for Publication
Written consent was obtained from all authors.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wei, L., Yan, H., Guo, M. et al. Perceived HIV Stigma, Depressive Symptoms, Self-esteem, and Suicidal Ideation Among People Living with HIV/AIDS in China: a Moderated Mediation Modeling Analysis. J. Racial and Ethnic Health Disparities 10, 671–679 (2023). https://doi.org/10.1007/s40615-022-01255-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40615-022-01255-0