
Abstract
Fetal micrognathia involves abnormal or arrested development of the fetal mandible. Till recently, the prenatal diagnosis was subjective, based on the evaluation of the fetal profile and assessment of the relationship between the maxilla and the mandible. Recently objective sonographic methods have been utilized for diagnosing micrognathia such as the inferior facial angle, the jaw index, the frontal nasomental angle, the mandible width/maxilla width ratio and the mandibular length. Another useful sonographic sign, the mandibular gap in the retronasal triangle view, increases the accuracy of the diagnosis early in the first trimester. 3D sonographic views can add to the diagnosis and prenatal MRI is a useful adjunct to ultrasound in cases of limited acoustic window, maternal obesity, oligohydramnios and anterior spine position. The identification of micrognathia should prompt karyotyping and sonographic investigation for other abnormalities. The outcome of fetuses with this seemingly isolated finding is more guarded than one would intuitively believe, and the parents should be counseled accordingly. Postnatal complications including mild to severe upper airway obstruction leading to respiratory distress, feeding difficulties and mild to severe long-term developmental delay are common. One should be careful in pronouncing a fetus having ‘micrognathia’, especially on subjective evaluation, as this term implies that the fetus is abnormal with presence of significant pathology. There is no ‘gold standard’ for a definitive diagnosis of micrognathia on post-natal evaluation. Using a combination of objective sonographic markers as well as follow-up ultrasound assessments can significantly reduce the risk of a false diagnosis. Follow-up scans should be arranged, and neonatal service should be alerted in cases of ongoing pregnancies.
Similar content being viewed by others

Introduction
Fetal mandible formation and development require several elements from different embryonic components to interact and fuse [1]. The detection rate of craniofacial malformations with ultrasound is relatively high (approximately 90%) [2]. Fetal micrognathia involves abnormal or arrested development of the fetal mandible. The prevalence is reported to be approximately 1:1500 [3]. Retrognathia refers to abnormal mandible position in relation to the maxilla. Although, micrognathia mainly reflects the size of the mandible, both anomalies are concurrent in most cases, as a small mandible will also be abnormally positioned. Retrognathia can be isolated, without concomitant mandible hypoplasia only in rare cases [1]. Thus, in most studies of the existing literature, the terms micrognathia and retrognathia are used synonymously. Isolated micrognathia is the diagnosis of exclusion if no other anatomic, growth or amniotic fluid abnormalities are detected. Till recently, antenatal diagnosis of micrognathia on ultrasound was subjective, based on midsagittal view of fetal facial profile [1]. However, several ultrasound signs have recently been described to make an objective and reliable prenatal diagnosis.
Diagnosis
The initial diagnosis of fetal micrognathia is most commonly made during the routine anatomy scan of the second trimester. The mean gestational age of the diagnosis in the literature is 21 weeks, ranging from 16 to 38 weeks [4]. With advances in fetal imaging, the detection of fetal micrognathia has become feasible relatively early in gestation, even from the first trimester. However, these cases are usually re-assessed later on in the second trimester, especially in the absence of major chromosomal and/or structural abnormalities.
A suspicion of micrognathia is raised by the subjective evaluation of the facial profile at the midsagittal view and is based on the assessment of the geometric relationship between the mandible and the rest of the profile [1].
Diagnostic Indices
The diagnosis should be confirmed using specific indices [5, 6], ratios or facial angles [7, 8].
-
1.
Inferior facial angle—This angle is measured in the midsagittal view of the fetal profile and is formed by the crossing of a line orthogonal to the vertical part of the forehead drawn at the level of synostosis of nasal bones and a line through the tip of the mentum and the more protrusive lip, usually the upper lip (Fig. 1). Its reported normal mean value is 65° ± 16°, so that the upper and lower reference limits are from 81° to 49°. Thus, an angle less than 49° gives the diagnosis of micrognathia, with a sensitivity and specificity of 100% and 99% respectively. The positive predictive value of the inferior facial angle is reportedly 75% and the negative predictive value is 100% [7].
Fig. 1 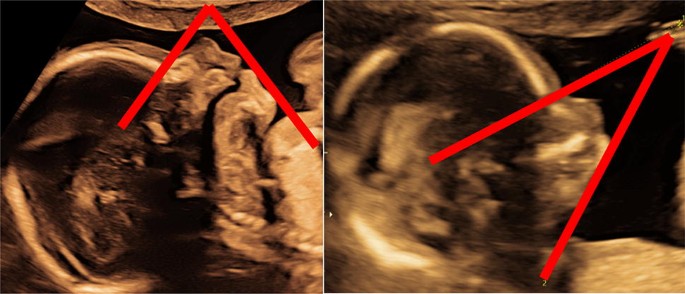
Inferior facial angle 70°(normal, left) & 33°(micrognathia, right)
-
2.
Jaw index—The jaw index is calculated after measuring the anteroposterior diameter of the fetal mandible, at the axial plane, and referring it as a percentage of the biparietal diameter, providing an index that is independent of gestational age (Fig. 2). The anteroposterior diameter is the distance between the symphysis mentis and the middle of the line connecting the bases of the two rami (axial diameter). Using a cut-off value of 23 mm (2 SD below mean) the sensitivity and specificity is reportedly 100% and 98% respectively [1]. The positive predictive value to predict micrognathia is 69% and the negative predictive value is 100% [1]. The mean value of anteroposterior and axial mandibular diameter is 19 ± 2.3(SD) mm and 13 ± 1.2(SD) mm respectively, at 18 weeks of gestation and 35 ± 2.8(SD) mm and 27 ± 2.3(SD) mm respectively, at 28 weeks of gestation [9].
Fig. 2 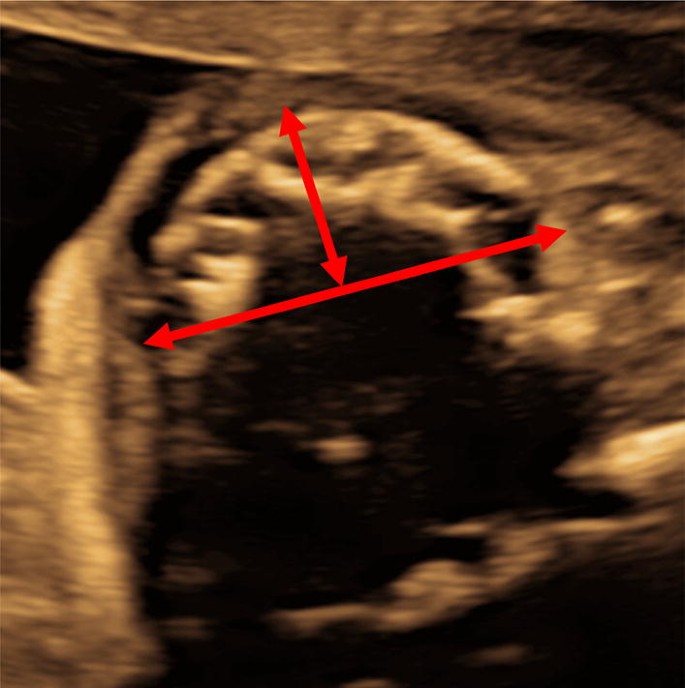
Anteroposterior and axial mandibular diameter
-
3.
Frontal nasomental angle—This is the angle between the line drawn from the tip of the nose and frontal bone, intersecting the line from the nasal tip to the mentum (Fig. 3). Its normal mean value is 147° ± 2.7°(SD) so that the upper and lower reference limits are 142° to 152°. Thus, an angle less than 142° is consistent with the diagnosis of micrognathia [10]. This index is reported to have a lower positive predictive value [11]. Many normal fetuses may have a nasomental angle below the fifth centile. According the recent literature, the frontal nasomental angle in pathological cases ranges from 100° to 134°.
Fig. 3 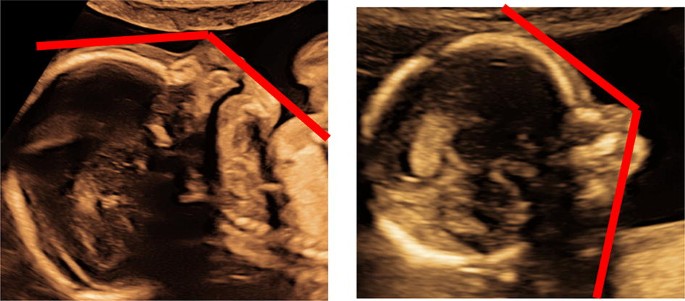
Frontal nasomental angle 137° (normal, left) & 117° (micrognathia, right)
-
4.
Mandible width/maxilla width ratio—the measurements are obtained on axial views at the alveolar level and 10 mm posterior to the anterior osteous border [7] (Fig. 4). This ratio is found to be constant over the second trimester. The mean value of this ratio is 1.02 ± 0.12 (SD) Consequently, a ratio less than 0.78 (below the 5th centile) is used to define micrognathia [7].
Fig. 4 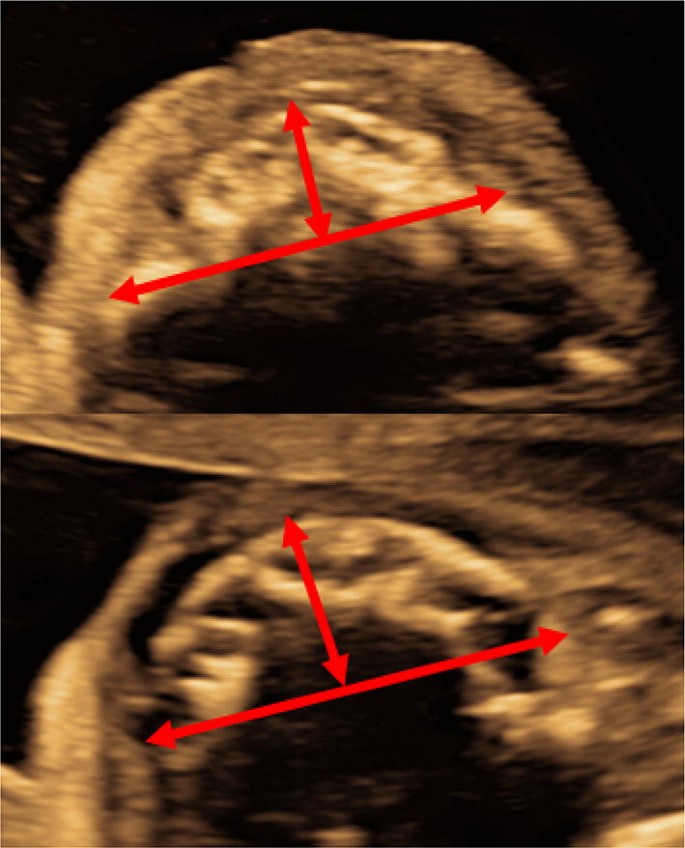
Width of maxilla and mandible
-
5.
Mandibular length—Mandibular length adjusted for gestational age or fetal biometry (like femur length), seems to be another sensitive and reliable prenatal method for assessment of fetal jaw development [5, 6, 9, 12]. Specific charts provide mean values and 95% intervals for mandibular length according gestational age or femur length [13]. When measuring the mandibular length the proximal landmarks are the cartilaginous symphysis menti and the temporomandibular joint [7] (Fig. 5). The increase in mandibular length is almost linear with increasing gestational age and varies from approximately 20 mm at 18 weeks to 37 mm at 28 weeks [7]. Measurements below the 5th centile are suggestive of micrognathia [13].
Fig. 5 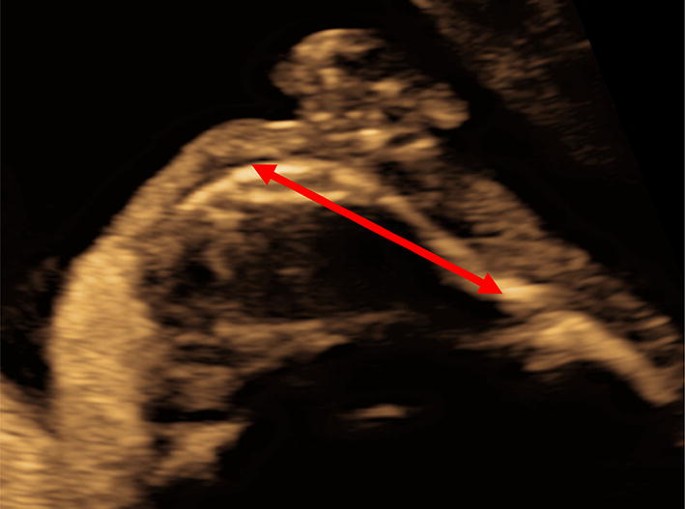
Mandibular length





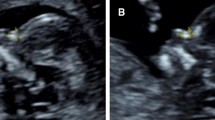
Detection of fetal micrognathia relatively early in the first trimester is feasible, partly due to the advances in fetal imaging. Apart from the assessment of the fetal profile, a useful sonographic sign is the mandibular gap in the retronasal triangle view (Fig. 6). The retronasal triangle view is the coronal plane of the face that captures the primary palate and the frontal processes of the maxilla simultaneously. In a normal fetus, a characteristic gap between the right and left body of the mandible is visible in this view [14]. The mandibular gap is linearly increased with CRL and progressive ossification of the facial bones allows easier identification. On the other hand, shadowing from the primary palate can make visualization challenging. It is advised that all suspicious cases are reassessed later on in the second trimester, especially in the absence of major chromosomal and/or structural abnormalities.

a Fetal profile of a fetus with suspected micrognathia in the first trimester (left); the evident mandibular gap (right). b The fetal profile appeared normal in the second trimester
3D sonographic views can add to the diagnosis, but the evaluation is mainly subjective. Prenatal MRI, on the other hand, may be a useful adjunct to ultrasound for the diagnosis and postnatal surgical management of craniofacial abnormalities [15]. Its diagnostic value is even higher in cases of limited acoustic window, maternal obesity, oligohydramnios and anterior spine position [16]. As the mandibular body grows more rapidly than the ramus and thus more rapidly in the longitudinal rather than the vertical plane, micrognathia, that is abnormal growth, primarily impairs longitudinal growth. Therefore, anteroposterior diameter measurements are more appropriate to assess the mandibular growth than other measurements [15].
One should be careful in pronouncing a fetus having ‘micrognathia’, especially on subjective evaluation. This term implies that the fetus is abnormal with presence of significant pathology. Micrognathia may be less apparent with continued growth and development. There is no ‘gold standard’ for a definitive diagnosis of micrognathia on post-natal evaluation. Using a combination of objective sonographic markers as well as follow-up ultrasound assessments can significantly reduce the risk of a false diagnosis.
Associations/Investigations
Micrognathia is frequently associated with chromosomal aberrations and dysmorphic syndromes (Table 1) [2, 11, 17, 18]. Micrognathia is reported to be a feature of over 300 chromosomal and non-chromosomal conditions [1]. These conditions may be classified into chromosomal abnormalities, primary mandibular disorders, skeletal and neuromuscular disorders and other syndromic conditions [1]. Most cases of fetal micrognathia fall into the first group of chromosomal aberrations. An abnormal in karyotype is reported in 44–66% of cases of fetal micrognathia (Table 2) [1, 17].
Pierre Robin sequence is characterized by micrognathia, glossoptosis and airway obstruction. It is isolated in 20–40% of cases. Changes in the DNA region near SOX9 gene are the most common genetic causes. SOX9 protein is known to regulate the activity of other genes that are important for the development of skeleton, including mandible. In an older study, more than 80% of individuals with Pierre Robin sequence were ultimately diagnosed with a genetic syndrome [19].
Micrognathia can have a functional cause as well. In cases such as fetal akinesia deformation sequence, the fixed contracture of the temporo-mandibular joint prevents the normal development of the mandible [1]. Even in cases of apparently isolated micrognathia, other accompanying abnormalities may be found at a later stage or postnatally. In a series of 58 cases of micrognathia, 14 (26%) were thought to be isolated prenatally. After neonatal examination only one case was truly isolated. The majority of cases (n = 42, 73%) had cleft palate [4]. It seems that failure of mandible to develop displaces the tongue upwards, which prevents median migration and midline fusion of the lateral palatine shelves [4].
Management-Outcome-Prognosis
After prenatal sonographic detection of micrognathia, the fetus should be evaluated for other structural anomalies, both in the first and early/late second trimester cases. Medical history of the current pregnancy should be obtained for maternal drug exposure and the family history for rare genetic syndromes. Fetal karyotyping is highly recommended [8]. Prenatal invasive testing should include PCR and microarray analysis. Exome sequencing is also useful, but taking into account its cost, the decision should be taken after informing the parents, especially in case of isolated micrognathia.
The clinical outcome is dependent on the presence and severity of associated anomalies. The outcome is reportedly poor even in chromosomally normal fetuses [17]. Postnatal complications are common 54% of neonates were reported to have mild to severe upper airway obstruction leading to respiratory distress requiring intervention, 31% feeding difficulties and 38% mild to severe long term developmental delay [4]. The parents should be aware that not all syndromic features are amenable to prenatal sonographic diagnosis.
As the overall prognosis seems to be poor (20–30% survival) [18] pregnancy interruption before viability is an option. For pregnancies that continue, serial growth scans should be undertaken, with a focus on fetal movements and amniotic fluid volume in order to detect a neuromuscular disorder or the development of polyhydramnios [8]. The incidence of polyhydramnios is reported to be 65% [18] as a result of swallowing difficulties.
Delivery should occur in a reference perinatal center with advanced services for the newborn, neonatal intensive care unit and experienced personnel [8, 11]. Clinicians should consider the ex utero intrapartum treatment (EXIT) when a severely hypoplastic mandible accompanied by polyhydramnios and absent stomach visualization is noted on ultrasound. A multidisciplinary team with experienced members should be assembled to perform the procedure [20].
The risk of recurrence depends on the etiology of the condition and is difficult to determine. It can vary from as low as 1% to as high as 50% in case of dominant inheritance pattern [1].
Summary
The evaluation of the fetal face at the second trimester may be limited by fetal position, but is important to be part of the routine assessment. Till recently, prenatal diagnosis of fetal micrognathia was subjective, based on the evaluation of the fetal profile and assessment of the relationship between the maxilla and the mandible. Recently, objective diagnostic methods have been utilized such as indices or facial angles. The identification of micrognathia should prompt karyotyping, sonographic investigation for other abnormalities including skeletal, cardiac and evaluation of the fetal ears. Detailed maternal history, including familial syndromes and drug exposure is crucial. The outcome of fetuses with this seemingly isolated finding is more guarded than one would intuitively believe, and the parents should be counseled accordingly. Follow-up scans should be arranged, and neonatal service should be alerted in cases of ongoing pregnancies.
References
Paladini D. Fetal micrognathia: almost always an ominous finding. Ultrasound Obstet Gynecol. 2010;35:377–84.
Pilu G, Reece EA, Romero R, Bovicelli L, Hobbins JC. Prenatal diagnosis of craniofacial malformations with ultrasonography. Am J Obstet Gynecol. 1986;155:45–50.
Micrognathia—The Fetal Medicine Foundation, UK, 2019. https://fetalmedicine.org/education/fetal-abnormalities/face/micrognathia.
Vettraino IM, Lee W, Bronsteen RA, Harper CE, Aughton D, Comstock CH. Clinical outcome of fetuses with sonographic diagnosis of isolated micrognathia. Obstet Gynecol. 2003;102:801–5.
Paladini D, Morra T, Teodoro A, Lamberti A, Tremolaterra F, Martinelli P. Objective diagnosis of micrognathia in the fetus: the Jaw Index. Obstet Gynecol. 1999;93:382–6.
Otto C, Platt LD. The fetal mandible measurement: an objective determination of fetal jaw size. Ultrasound Obstet Gynecol. 1991;1:12–7.
Rotten D, Levaillant JM, Martinez H, Ducou H, Le Pointe D, Vicaut E. The fetal mandible: a 2D and 3D sonographic approach to the diagnosis of retrognathia and micrognathia. Ultrasound Obstet Gynecol. 2002;19:122–30.
Galvao A, Inocencio G, Rodrigues M. First trimester ultrasound detection of fetal micrognathia. Acta Obstet Ginecol Port. 2015;9(5):425–6.
Watson WJ, Katz VL. Sonographic measurement of the fetal mandible: standards for normal pregnancy. Am J Perinatol. 1993;10:226–8.
Palit G, Jacquemyn Y, Kerremans M. An objective measurement to diagnose micrognathia on prenatal ultrasound. Clin Exp Obstet Gynecol. 2008;35:121–3.
Luedders D, Bohlmann M, Germer U, Axt-Fliedner R, Gembruch U, Weichert J. Fetal micrognathia: objective assessment and associated anomalies on prenatal sonogram. Prenat Diagn. 2011;31:146–51.
Chitty LS, Campbell S, Altman DG. Measurement of the fetal mandible-feasibility and construction of a centile chart. Prenat Diagn. 1993;13:749–56.
Neuschulz J, Wilhelm L, Christ H, Braumann B. Prenatal indices for mandibular retrognathia/micrognathia. J Orofac Orthop. 2015;76:30–40.
Sepulveda W, Wong AE, Vinals F, Andreeva E, Adzehova N, Martinez-Ten P. Absent mandibular gap in the retronasal triangle view: a clue to the diagnosis of micrognathia in the first trimester. Ultrasound Obstet Gynecol. 2012;39:152–6.
Nemec U, Nemec SF, Brugger PC, Weber M, Bartsch B, Bettelheim D, Gruber M, Prayer D. Normal mandibular growth and diagnosis of micrognathia at prenatal MRI. Prenat Diagn. 2015;35(2):108–16.
Kazan-Tannus JF, Levine D, McKenzie C, Lim KH, Cohen B, Farrar N, Busse RF, Mulliken JB. Real-time magnetic resonance imaging aids prenatal diagnosis of isolated cleft palate. J Ultrasound Med. 2005;24:1533–40.
Nicolaides KH, Salvesen DR, Snijders RJ, Gosden CM. Fetal facial defects: associated malformations and chromosomal abnormalities. Fetal Diagn Ther. 1993;8:1–9.
Bromley B, Benacerraf BR. Fetal micrognathia: associated anomalies and outcome. J Ultrasound Med. 1994;13:529–33.
Shprintzen RJ. Pierre Robin, micrognathia and airway obstruction: the dependency of treatment on accurate diagnosis. Int Anesthesiol Clin. 1988;26(1):64–71.
Suenaga M, Hidaka N, Kido S, Otera Y, Fukushima K, Kato K. Successful ex utero intrapartum treatment procedure for prenatally diagnosed severe micrognathia: a case report. J Obstet Gynaecol Res. 2014;40(8):2005–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Antonakopoulos, N., Bhide, A. Focus on Prenatal Detection of Micrognathia. J. Fetal Med. 6, 107–112 (2019). https://doi.org/10.1007/s40556-019-00210-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40556-019-00210-0