
Abstract
Purpose
Weight bias internalization (WBI) is significantly associated with negative physiological and psychological consequences. Given its negative effects, appropriate measurement of WBI is required for weight management and mental and physical health in people with weight problems. One of the most reliable and frequently used questionnaires to assess WBI is the Weight Self-Stigma Questionnaire (WSSQ). However, a Japanese version of the WSSQ has not yet been developed. Thus, the current study aimed to develop a Japanese version of the WSSQ (WSSQ-J) and validate its psychometric properties in the Japanese context.
Methods
A total of 1454 Japanese participants (age 34.44 ± 6.92; male = 498) with diverse weight statuses (Body mass index: 21.44 ± 3.52, 13.79–41.40 kg/m2) completed an online survey for the WSSQ-J. The internal consistency of the WSSQ-J was estimated by calculating Cronbach’s α. Confirmatory factor analysis (CFA) was then carried out to confirm that the factor structure of the WSSQ-J was the same as that of the subscales of the original WSSQ.
Results
The WSSQ-J had a Cronbach’s α of 0.917, indicating good internal consistency. In CFA, the comparative fit index was 0.945, the root mean square error of approximation was 0.085, and the standardized root mean square residual was 0.040, indicating that the two-factor model showed satisfactory goodness-of-fit.
Conclusion
This study replicated the original findings related to the WSSQ, showing that the WSSQ-J is a reliable WBI questionnaire consisting of two factors. Therefore, the WSSQ-J would be a reliable tool for assessing WBI among Japanese.
Level of evidence
Level V, descriptive cross-sectional study.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
It is becoming increasingly clear that people with greater body mass index (BMI) are facing weight-related bias or stigma [1, 2]. Weight bias is defined as the inclination to form unreasonable judgments or negative ideologies based on a person’s weight [3], such as beliefs that individuals with greater BMI are lazy, sloppy, incompetent, and lack willpower [4, 5]. Weight bias can lead to weight stigma [6], which refers to discriminatory acts and attitudes targeted towards individuals because of their weight and size [7, 8]. Weight stigma can affect an individual’s access to education, employment, and medical care [9,10,11], causing health and social inequalities.
Weight bias internalization (WBI) is often a result of exposure to weight stigma [12], and occurs when individuals apply negative weight stereotypes to themselves and self-derogate because of their body weight [5]. WBI is observed in various countries [13, 14] and is higher among people who are female, younger, and have a higher BMI [15, 16]. WBI is related to depression, anxiety, body image, self-esteem [5, 17, 18], and disordered eating in adults [16, 19,20,21,22] with any body weight status, including underweight/average weight, overweight, obese [23], and also in children [24]. Further, WBI could elevate body dissatisfaction [23], which is connected with impaired psychological and biological health [25], and unhealthy eating and negative health behavior [26]. Such disordered eating would relate to increased risk of metabolic syndrome [17] and difficulty maintaining a moderate weight [13, 27]. In addition, WBI is connected to poor mental and physical health-related quality of life [13, 28, 29].
Given such negative effects of WBI on affected individuals, appropriate WBI measurement is required for weight management and improving mental and physical health in people suffering from WBI. Additionally, such a measure is needed for the evaluation of WBI reduction interventions. To assess WBI, two self-reported questionnaires, the Weight Bias Internalization Scale (WBIS) and the Weight Self-Stigma Questionnaire (WSSQ), were mostly used in previous studies [5]. The WBIS was designed to assess the internalization of weight bias among individuals who are overweight and obese; it measures the internalization of negative characteristics that these people attribute to themselves [30]. The WSSQ assesses weight self-stigma and was designed to capture the multi-dimensional nature of WBI, self-devaluation, and fear of enacted stigma in populations of individuals who are overweight and obese [31]. A previous systematic review identified approximately 40 original self-report weight stigma questionnaires and evaluated their psychometric properties [32]. Among these questionnaires, the WSSQ had the most extensive psychometric validation [32]. The WSSQ shows good psychometric properties and validity and has been widely used to assess WBI in previous research [5, 33]. In addition, although the original WSSQ was adapted for people who are overweight or obese [31], unlike the WBIS, the WSSQ has been shown to be measurement invariant in “overweight” and “non-overweight” pediatric (aged 8 to 12 years) [34] and young adult populations [35], and in young adults with a broad range of weight status from underweight to overweight [36].
The rate of eating disorders is increasing among the Japanese population [37, 38]. Japanese females are at an especially high risk of suffering from eating disorders [39, 40]. Eating disorders (e.g., anorexia nervosa, bulimia nervosa, and binge-eating disorder) are characterized by disordered eating (e.g., dieting for weight loss, binge eating, and self-induced vomiting) [41], and disordered eating can evolve into eating disorders [42]. Therefore, because WBI is related to disordered eating [16, 19,20,21,22,23,24], eating disorders could potentially be associated with WBI. Given that sociocultural pressures related to appearance are involved in WBI [43] and the prevalence of eating disorders are on the rise in Japan [37, 38], an appropriate WBI measurement in the Japanese context is required. However, a Japanese version of the WSSQ has not yet been developed. Therefore, the current study aimed to develop a Japanese version of the WSSQ (WSSQ-J) and validate its psychometric properties in the Japanese context.
Methods
Participants
Given that most adult patients with eating disorders in Japan are aged 20–45 years [37, 44, 45], participants aged 18–45 years were included in the online survey. 100nin Enquete, a commercial survey sampling and administration company, was contracted to recruit participants and implement the online-based survey, which was conducted on June 11, 2022–June 13, 2022. Samples were acquired from existing pools of general Japanese participants. To improve the data quality of the survey, we added two dummy questions in the questionnaire. They were questions asking respondents to select a specific answer to confirm whether the respondents actually read and understood the questions. Originally, 1509 participants completed the survey; 55 participants who failed to answer the dummy questions were excluded and a total of 1454 Japanese participants between 18 and 45 years [age 34.44 ± 6.92 (mean ± standard deviation); male = 498, female = 956] were included in the statistical analyses (Table 1). The current study was approved by the Ethics Committee of the Department of Arts and Sciences, University of Tokyo (Approval No. 812-2). At the beginning of the online survey, participants were asked for their consent to contribute their data for research purposes, and we included participants who consented to participate in this research.
Participants completed the WSSQ-J, and the Japanese version of the Three-Factor Eating Questionnaire (TFEQ-J), and provided their age (years), sex, height (cm), and weight (kg). Self-reported height and weight were used to calculate the individual BMI.
Measures
The Japanese version of the WSSQ
With permission from the author of the original WSSQ [31], the WSSQ-J was developed according to the following standard procedures [46]. First, the original WSSQ was translated into Japanese by two Japanese researchers with high English proficiency. Second, the translated WSSQ was back-translated by a professional English editing and translation company (Editage; https://www.editage.com). Third, the author of the original WSSQ [31] confirmed that the back-translated WSSQ was conceptually and linguistically equivalent to the original WSSQ.
The WSSQ-J is a 12-item measure of weight-related self-stigma [31] (Supplemental Table S1). An example item reads, “I feel guilty because of my weight problems.” Each item of the WSSQ is rated on a 5-point Likert scale, with scores ranging from 1 (completely disagree) to 5 (completely agree). Sum scores are calculated for the full scale and each subscale. Items 1–6 constitute the self-devaluation subscale, and items 7–12 constitute the fear of enacted stigma subscale. There are no reverse-scored items. A high WSSQ-J score denotes a high level of weight-related self-stigma.
The Japanese version of the TFEQ
In the original study of the WSSQ, each subscale of TFEQ showed significant positive correlations with the total and subscales of the WSSQ [31]. Therefore, we examined associations between TFEQ-J and WSSQ-J.
The TFEQ-J is a 51-item measure of eating behavior [47, 48]. The items consist of 36 closed questions with a forced, true/false response and 15 Likert rating items. The TFEQ-J measures three aspects of eating behavior: (i) “cognitive restraint” as the degree of cognitive control of daily food intake, (ii) “disinhibition” as loss of control of food intake, and (iii) “hunger” as susceptibility to internal or external hunger signs. Cronbach’s α coefficients [49] for cognitive restraint, disinhibition, and hunger were 0.805, 0.807, and 0.771, respectively.
All TFEQ items were scored either 0 or 1 point, leading to maximum sum scores of 21 points for cognitive restraint, 16 points for disinhibition, and 14 points for hunger. Higher scores indicate stronger characteristic values in the domains.
Statistical analysis
Statistical analyses were performed using the R statistical software (v4.0.21; R Foundation for Statistical Computing, Vienna, Austria). In the whole sample, the reliability of the WSSQ-J (internal consistency) was estimated by calculating Cronbach’s α [49]. Confirmatory factor analysis (CFA) was then carried out with the lavaan package [50] to confirm that the factor structure of the WSSQ-J was the same as that of the subscales of the original WSSQ. Subsequently, the criterion-related validity of the WSSQ-J was examined through correlation analyses between scores on the WSSQ-J and the TFEQ-J. Since the Shapiro–Wilk test showed that the total and subscale scores of the WSSQ-J and the TFEQ-J were not normally distributed (p < 0.05), the Kendall’s rank correlation test was used. Finally, the association between the WSSQ-J and demographic characteristics was examined. First, sex differences in the WSSQ-J scores were examined by comparing the total and subscale scores. Since the Shapiro–Wilk test showed that the total and subscale scores of the WSSQ-J were not normally distributed in males and females (p < 0.05), the Wilcoxon rank sum test was used. In addition, correlations between the WSSQ-J and BMI or age were also tested. Given that BMI had two missing values, these data were omitted from this correlation analysis.
Since the original WSSQ was designed to assess WBI for people who are overweight or obese [31], the reliability of the WSSQ-J was examined in the non-overweight or non-obese (BMI < 25) sample (n = 1256) to test whether measurement invariant of the WSSQ-J could be confirmed in the samples with this weight status. Internal consistency was estimated by calculating Cronbach’s α, and CFA was performed to confirm that the WSSQ-J would have a two-factor structure similar to the original WSSQ.
Results
Characteristics of the WSSQ-J
The Kendall’s rank correlation showed that both the fear of enacted stigma (τ (correlation coefficient) = 0.730, p < 0.001) and self-devaluation (τ = 0.826, p < 0.001) subscales were positively correlated with the total scale score. In addition, these two subscales were positively correlated with each other (τ = 0.526, p < 0.001).
Internal consistency
Cronbach’s α coefficients for the total WSSQ-J scale and the fear of enacted stigma and self-devaluation subscales were 0.917, 0.818, and 0.915, respectively. Cronbach’s alpha of 0.70 and above is acceptable [51]. Thus, the internal consistency of the WSSQ-J was determined to be good.
Confirmatory factor analysis
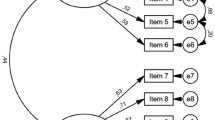
The CFA assessed the model fit of the two-factor model [χ2 = 604.81 (df = 53, p < 0.001)]. The comparative fit index (CFI) was 0.945 and the Tucker-Lewis index (TLI) was 0.932. Cut-off values for the CFI and TLI are > 0.95 [52]. Therefore, these are approximately good fit indices for internal validity. The root mean square error of approximation (RMSEA) was 0.085 (90% confidence interval (CI) [0.079, 0.091]) and the standardized root mean square residual (SRMR) was 0.040. An RMSEA of between 0.08 to 0.10 indicates a mediocre fit and below 0.06 shows a good fit, and an SRMR of less than 0.05 indicates a well-fitting index [52]. Thus, these values suggest that the two-factor model showed generally satisfactory goodness-of-fit. Results of the CFA of the WSSQ-J are presented in Fig. 1.

Results from confirmatory factor analyses of the WSSQ-J. The double-headed arrow indicates the standardized model covariance and other arrows indicate standardized factor loadings
The standardized factor loadings were 0.31–0.87 for the fear of enacted stigma, and 0.75–0.88 for the self-devaluation. As item 7 did not load well onto the fear of enacted stigma (factor loading = 0.31), this item was removed; we performed the CFA to examine whether the model fit would improve. Removing this item did not significantly improve the model fit (Supplemental Results).
The criterion-related validity of the WSSQ-J
The fear of enacted stigma, self-devaluation subscales, and total WSSQ-J scores showed significant positive correlations with scores for the cognitive restraint of eating, disinhibition, and hunger subscales of the TFEQ-J (pBonferroni-corrected < 0.05), although the fear of enacted stigma showed a positive correlation with the cognitive restraint of eating at a trend level (pBonferroni-corrected = 0.054) (Table 2).
Associations between the WSSQ-J and demographics
The total and subscale scores of the WSSQ-J in females were significantly greater than those in males (ps < 0.004). The Kendall’s rank correlation test showed that the fear of enacted stigma, self-devaluation subscales, and total WSSQ-J scores were positively correlated with BMI (p < 0.001), but not with age (ps > 0.070) (Table 2).
Measurement invariant of the WSSQ-J in the non-overweight or non-obese sample
In the non-overweight or non-obese sample, Cronbach’s α coefficients for the total WSSQ-J scale and the fear of enacted stigma and self-devaluation subscales were 0.912, 0.806, and 0.914, respectively. Overall, the internal consistency of the WSSQ-J was determined to be good [51].
In the non-overweight or non-obese sample, the CFA assessed the model fit of the two-factor model [χ2 = 525.40 (df = 53, p < 0.001)]. The CFI was 0.944 and the TLI was 0.930. These are good fit indices for internal validity [52]. The RMSEA was 0.084 (90% CI [0.078, 0.091]) and the SRMR was 0.042. These values suggest that the two-factor model showed satisfactory goodness-of-fit [52].
Discussion
To the best of our knowledge, this study is the first to validate and report on the WSSQ-J. A total of 1454 Japanese participants were included to validate the WSSQ-J. Cronbach’s α for the WSSQ-J total and the two subscales showed that the internal reliability of the WSSQ-J was satisfactory for research use [51]. The CFA showed that the two-factor model showed generally satisfactory goodness-of-fit, which was consistent with previous research [31]. Furthermore, in line with the previous report about the original version of the WSSQ [31], the total and subscales of the WSSQ-J showed positive correlations with the subscales of the TFEQ-J. In addition, the total and subscale scores of the WSSQ-J in females were greater than those in males, indicating that females experience higher levels of weight-related stigma. Moreover, BMI was positively correlated with the subscale and total scores of the WSSQ-J. In the non-overweight or non-obese sample, the reliability of the WSSQ-J was satisfactory; the CFA showed that the WSSQ-J had a two-factor structure similar to the original WSSQ [31], although the original WSSQ was designed for people who are overweight or obese. Overall, the results indicate that the WSSQ-J has good reliability and criterion-related validity, and can be a useful tool to measure weight-related self-stigma in Japanese adults.
Item 7 did not load well onto the fear of enacted stigma in this study. In the previous research about the original WSSQ, the factor loading of item 7 was 0.67 [31]. In the young adult samples with a broad range of weight status from underweight to overweight, the factor loading of item 7 was 0.59 [35] and 0.58 [36]. Compared to these previous studies, the factor loading of item 7 was low in the current study (0.31). Item 7 states, “I feel insecure about others’ opinions of me.” This item is practically irrelevant to individuals’ weight status, unlike other items constituting the fear of enacted stigma subscale (Items 8–12). Although such subscale is supposed to contain items that pertained to fear of enacted stigma and discrimination related to weight, item 7 does not necessarily involve discrimination related to weight. Therefore, item 7 did not load well onto the fear of enacted stigma in the current study.
Consistent with the original report of the WSSQ [31], greater BMI was correlated with higher WSSQ-J subscale and total scores. However, unlike the original WSSQ report with overweight or obese samples [31], in this study, fear of enacted stigma has a lower correlation coefficient with BMI compared to self-devaluation. This is consistent with a previous study with non-overweight samples, which showed that fear of enacted stigma had a lower correlation coefficient with BMI compared with the correlation coefficient between self-devaluation and BMI [35]. Individuals with greater BMI would perceive greater weight stigma [12, 21], and experiencing more weight discrimination from others likely leads to more internalization in people with greater BMI [15]. Thus, the perceived weight stigma in the non-overweight samples could differ from that in overweight or obese samples. Therefore, the association between fear of enacted stigma and BMI in non-overweight samples could also differ from that in overweight or obese samples.
People with greater BMI show higher discrepancies between their current and desired weight [53], and such increased discrepancies would lead to a higher desire to lose weight. However, WBI is connected to disordered eating, such as emotional, uncontrolled, and binge eating [19,20,21,22]. Moreover, individuals with higher WBI are more likely to report coping with experiences of weight stigma by eating [16]. In fact, in the current study, greater WSSQ-J scores were positively associated with the TFEQ-J disinhibition subscale, which indicates loss of control in food intake, and the TFEQ-J hunger subscale, which indicates susceptibility to internal or external hunger signs. These TFEQ-J subscales have been shown to be associated with maladaptive eating patterns [54,55,56]. Thus, in the current study, some people with greater WBI would have disordered eating. Therefore, ironically, when people with greater WBI seek weight loss, they may experience more disordered eating and have greater difficulty losing weight compared to people with less WBI.
In line with some previous reports [15, 16], the WSSQ-J subscale and total scores in females were greater than those in males. Therefore, females are more likely to internalize weight stigma [15, 16]. In Japan, women are still expected to play a supportive and modest role to confirm men’s higher status over women in the vertical societal hierarchy [38]. In fact, a study showed that, compared to women in western countries, Japanese women spoke with higher pitch, which reflects physical and psychological powerlessness (short, weak, dependent, and modest), to express sociocultural expectations of femininity [57]. Because of these socioculturally standardized gender roles, Japanese women are likely to have lower self-esteem and self-assertion, and have high regard for slimness as a norm of physical beauty [38]. These characteristics would be associated with WBI [58, 59] and could lead to the onset of eating disorder symptoms [38]. The prevalence of eating disorders is higher in females compared to males in Japan [37, 38]. Given that WBI is connected with disordered eating [15, 16, 19, 21, 22], which would be related to eating disorders [41, 42], and sociocultural pressures regarding appearance [43], the effects of gender on the role of WBI in eating disorders could be different between western countries and Japan. Future research should include more diverse samples to examine sociocultural effects on associations between gender and WBI.
Susceptibility to weight bias would be different between people in western countries and Japan. Although Japanese culture has become more individualistic over time, traditional collectivism persists in Japan [60]. A previous meta-analytic study showed that collectivism significantly moderated the process of stigma internalization [61]. Compared with western countries, Japanese people strongly dislike people who are overweight or obese over lean people; thus, weight bias toward individuals with greater BMI could be stronger in Japan [62]. Overall, Japanese people would also tend to internalize weight bias. Hence, it would be favorable to examine differences in the effect of the attitudes towards being overweight and obesity on weight bias internalization across countries and cultures.
Strength and limits
This study has limitations that must be considered in future studies. First, the test–retest reliability of the WSSQ-J was not examined and should be tested in future research. Second, the current study did not include adolescents or older adults. Although there was no significant association between WSSQ-J score and age in the current sample, previous research indicates that younger people would have higher WBI [15]. Future studies should include a wide range of age groups to test the effect of WBI. Third, self-reported weight and height were used to calculate BMI. Given that self-reported height tends to be overestimated while self-reported weight tends to be underestimated [63], BMI calculated from self-reported data is likely to be lower than the measured data [63, 64]. However, since large cohort studies suggested that BMI computed from self-reported weight and height was an adequately valid measure in large epidemiological studies [63, 64], the reliability of the current results is assumed. Fourth, although the WSSQ-J showed a good reliability and two-factor structure in this study, measurement invariant of the WSSQ-J was not tested in individuals who are overweight and obese. The current sample included only 196 participants who are overweight or obese, and this sample size is insufficient for CFA [65, 66]. Since the original WSSQ was constructed for people who are overweight or obese [31], the constructs of the WSSQ-J would be different between overweight and non-overweight samples; moreover, measurement invariant of the WSSQ-J should be tested in individuals who are overweight or obese in future studies.
A strength of the present study is that, to the best of our knowledge, this is the first study that has examined psychometric properties of a Japanese version of the WSSQ. In addition, this study was conducted with a sufficient sample size compared with previous similar studies [34,35,36]. The present study also used a rigorous translation procedure to ensure the linguistic validity of the WSSQ-J.
What is already known on this subject?
The WSSQ is widely used to assess WBI and has the two-factor structure and extensive psychometric validation. Psychometric properties and a two-factor structure of the WSSQ were confirmed in English-, Arabic-, Chinese-, French-, German-, Italian-, Persian-, and Turkish-speaking samples.
What your study adds?
By partially replicating the original study of the WSSQ, this study has confirmed that the WSSQ-J has good reliability and criterion-related validity. Therefore, the WSSQ-J can be a reliable and useful tool for assessing WBI among the Japanese population.
Data availability
The anonymized data presented in this study are available upon request. Please contact the corresponding author (Y.N.).
References
Rubino F, Puhl RM, Cummings DE et al (2020) Joint international consensus statement for ending stigma of obesity. Nat Med 26:485–497
Andreyeva T, Puhl RM, Brownell KD (2008) Changes in perceived weight discrimination among Americans, 1995–1996 through 2004–2006. Obesity (Silver Spring) 16:1129–1134
Washington RL (2011) Childhood obesity: issues of weight bias. Prev Chronic Dis 8:A94
Puhl R, Brownell KD (2001) Bias, discrimination, and obesity. Obes Res 9:788–805
Pearl RL, Puhl RM (2018) Weight bias internalization and health: a systematic review. Obes Rev 19:1141–1163
World Health Organization Regional Office for Europe (2017) Weight bias and obesity stigma: considerations for the WHO European Region. World Health Organization. Regional Office for Europe, Copenhagen
Tomiyama AJ (2014) Weight stigma is stressful. A review of evidence for the cyclic obesity/weight-based stigma model. Appetite 82:8–15
Pearl R (2018) Weight bias and stigma: public health implications and structural solutions. Soc Issues Policy Rev 12:146–182
Puhl RM, Lessard LM (2020) Weight stigma in youth: prevalence, consequences, and considerations for clinical practice. Curr Obes Rep 9:402–411
Giel KE, Thiel A, Teufel M et al (2010) Weight bias in work settings—a qualitative review. Obes Facts 3:33–40
Flint SW (2021) Time to end weight stigma in healthcare. EClinicalMedicine 34:100810
Ratcliffe D, Ellison N (2015) Obesity and internalized weight stigma: a formulation model for an emerging psychological problem. Behav Cogn Psychother 43:239–252
Pearl RL, Puhl RM, Lessard LM et al (2021) Prevalence and correlates of weight bias internalization in weight management: a multinational study. SSM Popul Health 13:100755
Stewart SF, Ogden J (2021) The role of social exposure in predicting weight bias and weight bias internalisation: an international study. Int J Obes (Lond) 45:1259–1270
Pearl RL, Himmelstein MS, Puhl RM et al (2019) Weight bias internalization in a commercial weight management sample: prevalence and correlates. Obes Sci Pract 5:342–353
Himmelstein MS, Puhl RM, Quinn DM (2017) Intersectionality: an understudied framework for addressing weight stigma. Am J Prev Med 53:421–431
Pearl RL, Wadden TA, Hopkins CM et al (2017) Association between weight bias internalization and metabolic syndrome among treatment-seeking individuals with obesity. Obesity (Silver Spring) 25:317–322
Almutairi BF, Alsaygh KW, Altamimi MM et al (2021) Internalized weight stigma: prevalence and association with psychiatric disorder among overweight and obese individuals. Cureus 13:e18577
Marshall RD, Latner JD, Masuda A (2019) Internalized weight bias and disordered eating: the mediating role of body image avoidance and drive for thinness. Front Psychol 10:2999
Puhl RM, Moss-Racusin CA, Schwartz MB (2007) Internalization of weight bias: implications for binge eating and emotional well-being. Obesity (Silver Spring) 15:19–23
Kamolthip R, Saffari M, Fung XCC et al (2022) The mediation effect of perceived weight stigma in association between weight status and eating disturbances among university students: is there any gender difference? J Eat Disord 10:28
Reinka MA, Quinn DM, Puhl RM (2021) Examining the relationship between weight controllability beliefs and eating behaviors: the role of internalized weight stigma and BMI. Appetite 164:105257
Romano KA, Heron KE, Henson JM (2021) Examining associations among weight stigma, weight bias internalization, body dissatisfaction, and eating disorder symptoms: does weight status matter? Body Image 37:38–49
Gmeiner MS, Warschburger P (2022) Simply too much: the extent to which weight bias internalization results in a higher risk of eating disorders and psychosocial problems. Eat Weight Disord 27:317–324
Muennig P, Jia H, Lee R, Lubetkin E (2008) I think therefore I am: perceived ideal weight as a determinant of health. Am J Public Health 98:501–506
Blake CE, Hébert JR, Lee DC et al (2013) Adults with greater weight satisfaction report more positive health behaviors and have better health status regardless of BMI. J Obes 2013:291371
Pearl RL, Puhl RM, Himmelstein MS et al (2020) Weight stigma and weight-related health: associations of self-report measures among adults in weight management. Ann Behav Med 54:904–914
Walsh OA, Wadden TA, Tronieri JS et al (2018) Weight bias internalization is negatively associated with weight-related quality of life in persons seeking weight loss. Front Psychol 9:2576
Latner JD, Barile JP, Durso LE, O’Brien KS (2014) Weight and health-related quality of life: the moderating role of weight discrimination and internalized weight bias. Eat Behav 15:586–590
Durso LE, Latner JD (2008) Understanding self-directed stigma: development of the weight bias internalization scale. Obesity (Silver Spring) 16(Suppl 2):S80-86
Lillis J, Luoma JB, Levin ME, Hayes SC (2010) Measuring weight self-stigma: the weight self-stigma questionnaire. Obesity (Silver Spring) 18:971–976
Lacroix E, Alberga A, Russell-Mathew S et al (2017) Weight bias: a systematic review of characteristics and psychometric properties of self-report questionnaires. Obes Facts 10:223–237
Stewart SF, Ogden J (2021) What are weight bias measures measuring? An evaluation of core measures of weight bias and weight bias internalisation. Health Psychol Open 8:20551029211029148
Pakpour AH, Tsai M-C, Lin Y-C et al (2019) Psychometric properties and measurement invariance of the weight self-stigma questionnaire and weight bias internalization scale in children and adolescents. Int J Clin Health Psychol 19:150–159
Chirawat P, Kamolthip R, Rattaprach R et al (2022) Weight stigma among young adults in Thailand: reliability, validation, and measurement invariance of the Thai-translated weight self stigma questionnaire and perceived weight stigma scale. Int J Environ Res Public Health 19:15868
Nadhiroh S, Nurmala I, Pramukti I et al (2022) Weight stigma in Indonesian young adults: validating the Indonesian versions of the weight self-stigma questionnaire and perceived weight stigma scale. Asian J Soc Health Behav 5:169–179
Nakai Y, Nin K, Goel NJ (2021) The changing profile of eating disorders and related sociocultural factors in Japan between 1700 and 2020: a systematic scoping review. Int J Eat Disord 54:40–53
Chisuwa N, O’Dea JA (2010) Body image and eating disorders amongst Japanese adolescents. A review of the literature. Appetite 54:5–15
Ritchie H, Roser M (2017) Obesity. Our World in Data
(NCD-RisC) N.R.F.C. (2017) Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 390:2627–2642
Treasure J, Duarte TA, Schmidt U (2020) Eating disorders. Lancet 395:899–911
Stabouli S, Erdine S, Suurorg L et al (2021) Obesity and eating disorders in children and adolescents: the bidirectional link. Nutrients 13:4321
Lee MS, Gonzalez BD, Small BJ, Thompson JK (2019) Internalized weight bias and psychological wellbeing: an exploratory investigation of a preliminary model. PLoS ONE 14:e0216324
Kurisu K, Matsuoka M, Sato K et al (2022) Increased prevalence of eating disorders in Japan since the start of the COVID-19 pandemic. Eat Weight Disord 27:2251–2255
Ishikawa T, Tamura N (2014) Aging of eating disorders. Jpn J Psychosom Med 54:935–939
Wild D, Grove A, Martin M et al (2005) Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health 8:94–104
Adachi Y, Fujii K, Yamagami T (1992) Responses regarding restrained eating on the three-factor eating questionnaire and weight loss. Jpn J Behav Ther 18:140–148
Stunkard AJ, Messick S (1985) The three-factor eating questionnaire to measure dietary restraint, disinhibition and hunger. J Psychosom Res 29:71–83
Cronbach LJ (1951) Coefficient alpha and the internal structure of tests. Psychometrika 16:297–334
Rosseel Y (2012) lavaan: an R package for structural equation modeling. J Stat Softw 48:1–36
Cortina JM (1993) What is coefficient alpha? An examination of theory and applications. J Appl Psychol 78:98–104
Hooper D, Coughlan J, Mullen M (2007) Structural equation modeling: guidelines for determining model fit. Electron J Bus Res Methods 6:1–55
Jung F, Spahlholz J, Hilbert A et al (2017) Impact of weight-related discrimination, body dissatisfaction and self-stigma on the desire to weigh less. Obes Facts 10:139–151
Bryant EJ, Rehman J, Pepper LB, Walters ER (2019) Obesity and eating disturbance: the role of TFEQ restraint and disinhibition. Curr Obes Rep 8:363–372
Gallant AR, Tremblay A, Pérusse L et al (2010) The three-factor eating questionnaire and BMI in adolescents: results from the Québec family study. Br J Nutr 104:1074–1079
Karlsson J, Persson LO, Sjöström L, Sullivan M (2000) Psychometric properties and factor structure of the Three-Factor Eating Questionnaire (TFEQ) in obese men and women. Results from the Swedish Obese Subjects (SOS) study. Int J Obes Relat Metab Disord 24:1715–1725
van Bezooijen R (1995) Sociocultural aspects of pitch differences between Japanese and Dutch women. Lang Speech 38:253–265
Hübner C, Schmidt R, Selle J et al (2016) Comparing self-report measures of internalized weight stigma: the weight self-stigma questionnaire versus the weight bias internalization scale. PLoS ONE 11:e0165566
Liu X, Zhang W, Yue W et al (2022) From weight bias internalization to health-related quality of life: self-esteem and psychopathology in pre-bariatric surgery patients. Obes Surg 32:3705–3713
Ogihara Y (2017) Temporal changes in individualism and their ramification in Japan: rising individualism and conflicts with persisting collectivism. Front Psychol 8:695
Yu BCL, Chio FHN, Mak WWS et al (2021) Internalization process of stigma of people with mental illness across cultures: a meta-analytic structural equation modeling approach. Clin Psychol Rev 87:102029
Marini M, Sriram N, Schnabel K et al (2013) Overweight people have low levels of implicit weight bias, but overweight nations have high levels of implicit weight bias. PLoS ONE 8:e83543
Hodge JM, Shah R, McCullough ML et al (2020) Validation of self-reported height and weight in a large, nationwide cohort of US adults. PLoS ONE 15:e0231229
Roystonn K, Abdin E, Sambasivam R et al (2021) Accuracy of self-reported height, weight and BMI in a multiethnic Asian population. Ann Acad Med Singap 50:306–314
Kyriazos TA (2018) Applied psychometrics: sample size and sample power considerations in factor analysis (EFA, CFA) and SEM in general. Psychology 9(8):25
Wolf EJ, Harrington KM, Clark SL, Miller MW (2013) Sample size requirements for structural equation models: an evaluation of power, bias, and solution propriety. Educ Psychol Meas 76:913–934
Acknowledgements
This study was supported by the Grant-in-Aid for Transformative Research Areas (A) of Japan Society for the Promotion of Science (JP21H05172), to Yuko Nakamura.
Author information
Authors and Affiliations
Contributions
The current study was conceptualized and designed by Yuko Nakamura. Data collection and analysis were performed by Yuko Nakamura. The first draft of the manuscript was written by Yuko Nakamura and all authors commented on previous versions of the manuscript. Both authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval
The current study was approved by the Ethics Committee of the Department of Arts and Sciences, University of Tokyo (Approval No. 812-2).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nakamura, Y., Asano, M. Developing and validating a Japanese version of the Weight Self-Stigma Questionnaire. Eat Weight Disord 28, 44 (2023). https://doi.org/10.1007/s40519-023-01573-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40519-023-01573-0