
Opinion statement
Seasonal influenza can be a self-limiting illness in healthy individuals but is associated with short-term morbidity and economic burden. Influenza can cause significant morbidity and mortality in young children, the elderly, pregnant and post-partum women, patients with co-morbidities and the immunocompromised. Neuraminidase inhibitors (NAIs) are the treatment of choice for influenza due to widespread resistance to the adamantanes. NAIs are efficacious for the treatment of influenza in ambulatory patients with mild illness, when initiated within 48 h of symptom onset. Early treatment with NAIs has been shown to reduce otitis media in children, and lower respiratory tract complications, resulting in antibiotic therapy, in adults. Evidence on the efficacy of NAIs for the prevention of influenza-related complications in at-risk populations, based on reviews of data from randomised trials is inconclusive. However, observational studies suggest that in hospitalised patients early treatment with NAIs has been associated with reduced mortality. NAIs should be initiated as soon as possible in patients at high-risk of influenza-related complications, with suspected or proven influenza, hospitalised patients and patients with severe or progressive disease. NAIs can be considered in previously healthy patients when therapy can be initiated within 48 h of symptom onset. In previously healthy patients, the therapeutic efficacy of oseltamivir is time-dependent, with maximal benefit observed when therapy is initiated within 48 h of symptom onset. However, several observational studies suggest therapeutic benefit beyond 48 h, in hospitalised patients, severe disease, and patients at high risk of complications, including pregnant women. NAIs should be considered in patients at high risk of influenza-related complications who present late. Further studies are needed to define the optimal timing of NAIs. Oseltamivir-resistant virus has been widely reported but is predominantly an issue in H1N1 seasonal influenza. Zanamivir-resistant influenza virus is rare, and inhaled or intravenous (IV) zanamivir is the treatment of choice in proven or suspected oseltamivir-resistant virus. Intubated patients with severe influenza can be treated with oseltamivir (suspension) administered via nasogastric tube. The commercial dry powder formulation of zanamivir should not be administered, via nebulisation, as it has been associated with ventilator malfunction and mortality. In intubated patients, when there are concerns about gastric absorption, IV zanamivir should be obtained under Emergency Investigational New Drug access schemes. Currently available evidence does not support the use of high-dose or extended-duration oseltamivir in patients with severe influenza, but does require further investigation. Extracorporeal membrane oxygenation has not been shown to be superior to conventional management in patients with influenza-associated acute respiratory distress syndrome and should be considered as salvage therapy. Corticosteriods should not be used in the treatment of severe influenza as this has been associated with increased risk of mortality and bacterial superinfection.
Similar content being viewed by others


Introduction
Influenza is a contagious respiratory virus transmitted via droplets produced by coughing and sneezing. In the majority of individuals, seasonal influenza is a self-limiting disease but is associated with significant economic burden [1]. However, influenza can cause significant morbidity and mortality in high-risk groups, including the elderly, young children and people with co-morbidities [2•].
In temperate climates, seasonal influenza causes outbreaks during the winter, while in tropical areas there is year-round transmission. There are three major strains of seasonal influenza: A, B and C, but influenza A and B cause the majority of disease. Influenza A is classified into subtypes according to the combination of haemagglutinin or ‘H’ protein and the neuraminidase or ‘N’ protein on the surface of the virus [3]. New viruses are created through antigenic shift or drift. A pandemic occurs when a new virus emerges and circulates in a population where there is minimal immunity; this can occur outside the normal influenza season [3].
Symptoms in otherwise healthy adults include fever, cough, headache, runny nose, myalgia and malaise. Cough within 48 h of fever onset is highly predictive of influenza during peak times of virus circulation [4]. Influenza can be confirmed by culture of respiratory secretions but this is resource-intensive and turnaround time is slower than polymerase chain reaction (PCR). Culture has been superseded by reverse-transcriptase PCR, which is highly sensitive and provides rapid results [2•]. Rapid influenza diagnostic tests that provide results within 30 min are available but sensitivity is only reported to be 40–70 % [5].
Influenza vaccine is the first choice for the prevention of influenza and has been shown to be effective in preventing disease in healthy adults and older children [6•]. Influenza vaccine has been associated with a reduction in cardiac events in patients with a history of cardiac disease [7] but efficacy is reduced in the elderly [1, 6•]. Live attenuated influenza vaccine is efficacious in young children aged between 6 months and 7 years [1]. Antivirals are highly effective for prophylaxis in exposed individuals but use needs to be weighed against cost, side effects and emergence of viral resistance [8].
The two main classes of antivirals for the treatment of influenza are the adamantanes (M2 ion channel inhibitors) and the neuraminidase inhibitors (NAIs). The NAIs are the first choice for the treatment of seasonal influenza [2•] as the clinical utility of the adamantanes is limited by widespread antiviral resistance [9]. A summary of the currently available influenza antivirals is provided in Table 1. NAIs are efficacious for the treatment of influenza in ambulatory patients with mild illness, when initiated within 48 h of symptom onset [10–12]. This review will focus on the treatment of seasonal influenza. Emerging avian influenza is beyond the scope of this paper.
Treatment
Drug classes
Neuraminidase inhibitors
-
NAIs are effective against all strains of influenza. They act by interfering with viral replication by blocking the release of the progeny virus from infected host cells and spread within respiratory secretions [13].
-
The primary NAIs are oseltamivir and zanamivir; newer agents, peramivir and laninamivir, have limited approval and availability (Table 1).
-
Oseltamivir and zanamivir are both efficacious for the treatment of influenza. Zanamivir is preferred in patients suspected of having oseltamivir-resistant influenza, while oseltamivir is preferred in patients with underlying airways disorders or who are unable to use an inhalational device [2•].
Adamantanes
-
The adamantanes are only effective against influenza A and act by interfering with viral uncoating inside the cell [13].
-
Amantadine and rimantadine are equally efficacious, but their use should be discouraged as they are ineffective as a result of widespread resistance and are associated with adverse effects [14].
Polymerase inhibitors
-
Favipiravir (T-705) is a polymerase inhibitor that has been evaluated in phase III studies in Japan and phase II studies in the US. It selectively inhibits RNA-polymerase of the influenza virus. It is active against a broad range of influenza subtypes, including resistant virus, and demonstrates synergism when used with oseltamivir [15•].
Efficacy and endpoints
Neuraminidase inhibitors
-
NAIs are effective for the treatment of influenza in ambulatory patients with mild illness, when treatment is commenced within 48 h [10–12]. In previously healthy patients, NAIs reduce symptom duration and severity, viral shedding, and time taken to return to normal activities [16]. In a meta-analysis, oseltamivir has been shown to reduce lower respiratory complications that lead to antibiotic use by 28 % compared with placebo [17]. Treatment within 12 h of symptom onset has been shown to reduce the incidence of otitis media, and treatment within 24 h of symptoms decreased duration of illness by 3.5 days [18]. However, the efficacy of NAIs for the prevention of complications in some high-risk groups is less clear [19].
-
In 2012, Jefferson and colleagues published a Cochrane review of NAIs for the treatment and prevention of influenza in healthy adults and children, but the review was hampered by difficulties in obtaining clinical study reports [20]. They analysed data from 25 of 67 randomised controlled trials reviewed, but noted a high risk of reporting and publication biases. The investigators concluded that oseltamivir had a modest benefit in previously healthy patients, reducing duration of symptoms by 21 h, but had no effect on hospitalisation [20].
-
In 2013, Michiels and colleagues published a systematic review of systematic reviews to address the value of NAIs for the prevention and treatment of seasonal influenza focusing on data from randomised clinical trials [8]. NAIs can reduce the time to alleviation of symptoms in previously healthy adults and children but the effect in the elderly and at-risk individuals is unclear (Fig. 1a). The use of NAIs was associated with a non-significant reduction in the odds of pneumonia in most study populations (Fig. 1b), but the meta-analysis did not find any consistent reductions in the odds of hospitalisation (Fig. 1c). Therefore, while the review documented clear benefits in less definitive outcomes such as time-to-alleviation of symptoms in previously healthy children and adults [8], it was unable to give conclusive evidence on the efficacy of NAIs in patients at the highest risk of influenza-related complications, and highlighted the lack of evidence for the efficacy of NAIs in more definitive outcomes such as pneumonia and hospitalisation.
Fig. 1 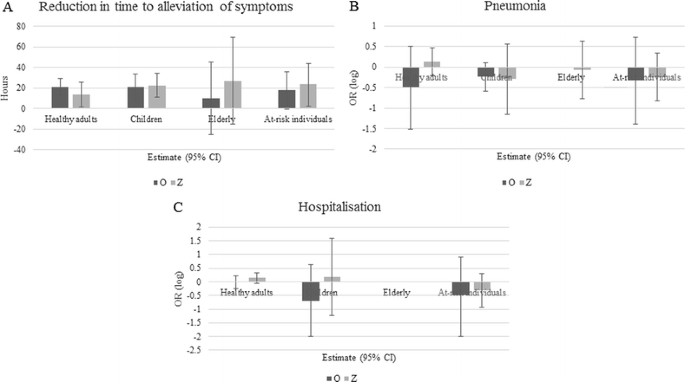
Graphical representation of data from Michiels et al. [8] on the efficacy of oseltamivir (dark grey bars) and zanamivir (light grey bars) for selected outcome measures and study populations. (a) Reduction in time to alleviation of symptoms; (b) pneumonia; (c) hospitalisation. Error bars denote 95 % CIs. Data from Michiels et al. [8] are based on a meta-analysis of randomised trials comparing treated subjects with untreated subjects. CI confidence interval, O oseltamivir, Z zanamivir, OR odds ratio.
-
A systematic review and meta-analysis of 74 observational studies in 2012 by Hsu and colleagues attempted to address the benefits and potential harm of antivirals for the treatment of influenza [21]. The meta-analysis suggested that in high-risk patients NAIs may reduce mortality (odds ratio [OR] 0.23], hospitalisation (OR 0.75) and duration of symptoms when compared with no therapy. These findings must be interpreted with caution as the quality of evidence is low, limited by multiple confounders in the original studies and publication and reporting biases [21].
-
A recently published meta-analysis of individual participant data comprised of 29,234 hospitalised patients worldwide with pandemic influenza A H1N1(09) demonstrated that treatment of adult patients with NAIs reduced mortality risk compared with no treatment. The effect is more pronounced if treated early. A greater benefit was observed with early NAI treatment. However, no mortality benefit could be established in children treated with NAIs. The study was unable to adjust for disease severity but the results suggest that NAIs should be initiated early in patients with influenza who require hospitalisation [22••].
-
In summary, there was a lack of conclusive evidence on the efficacy of NAIs for the prevention of influenza-related complications in at-risk populations based on reviews of data from randomised trials. However, observational studies suggest that, in hospitalised patients, early treatment with NAIs has been associated with reduced mortality. The World Health Organization and Centers for Disease Control (US) recommend that NAIs should be used for the treatment of influenza in patients at risk of influenza-related complications, hospitalised patients and patients with severe or complicated illness [2•, 23••]. NAI therapy can be considered in previously healthy people when it can be initiated within 48 h of symptom onset, but needs to be weighed against the risk of drug-related adverse effects and the potential for NAI resistance.

Administration and dosing
Oseltamivir
-
Oseltamivir is administered as an oral formulation (tablet or suspension) as it is readily absorbed from the gastrointestinal tract. The standard treatment dose is 75 mg twice daily for 5 days for healthy adults and children over 12 years of age [24].
-
Oseltamivir undergoes hepatic metabolism to its active form but is predominantly cleared by the kidneys. Dose reduction is not required in patients with hepatic impairment but is required in patients with renal impairment (Table 1) [25]. Dose reduction is required in patients receiving concurrent continuous venovenous hemofiltration and extracorporeal membrane oxygenation (ECMO) [26]. Dose-adjusted oseltamivir is efficacious and safe in patients with end-stage renal failure receiving renal replacement therapy [27].
-
Intravenous (IV) oseltamivir was shown to have a favourable safety and pharmacokinetic profile in phase I clinical studies [28] but further development has been stopped.
-
The suspension formulation (or dispersed capsules) of oseltamivir can be administered via nasogastric tube in mechanically ventilated patients who have reliable gastric absorption [29].
Zanamivir
-
Zanamivir has very low oral bioavailability [13] and is therefore administered via oral inhalation of a dry powder or IV. The approved route of administration is oral inhalation, using a purpose-manufactured device. The standard treatment dose of 10 mg 12-hourly is administered as two 5 mg inhalations, for 5 days. Renal dose adjustment is not required in patients receiving inhalational therapy [30].
-
Administration of zanamivir in a lactose powder solution via endotracheal nebulisation (of the commercial powder containing lactose) has been reported in intubated patients with severe influenza. This route of administration has resulted in ventilator malfunction, which likely contributed to mortality [31, 32]. The commercial lactose powder formulation of zanamivir should only be used for oral inhalation [33].
-
IV zanamivir is in clinical development and has shown promising results in a phase II study [34]; renal dose adjustment is required [34, 35]. IV formulations can be accessed under clinical trial or Emergency Investigational New Drug access schemes in some countries.
Peramivir
-
Peramivir is administered IV. One dose is sufficient in outpatients as the drug exhibits prolonged anti-influenza activity [36]. A dose of 600 mg IV daily is recommended in high-risk adult patients [37]. The optimal duration of therapy in complicated disease remains unclear. Dose adjustment is required in renal impairment [38].
-
Peramivir was associated with favourable outcomes in patients with severe pandemic influenza treated under an Emergency Investigational New Drug access scheme [38]. However, in a subsequent publication, peramivir was associated with increased risk of influenza-related complications, and death in patients with severe influenza [39]. These findings may have been influenced by disease severity. Further studies are required to define the role of peramivir in the treatment of severe influenza.
Paediatric considerations
-
Young children (<2 years of age), infants and children with chronic medical conditions are at risk of influenza-related complications [2•, 40].
-
NAIs have been shown to be effective for the treatment of influenza in healthy children, reducing symptom duration and time to return to normal activities. Oseltamivir has been shown to reduce influenza-related complications. However, there is a paucity of evidence on the efficacy of NAIs in children ‘at risk’ of influenza-related complications. Oseltamivir did not reduce symptom duration in children with asthma [41]. Retrospective data suggests that early initiation of NAIs may reduce mortality in children [42] but further studies are needed to understand the role of NAIs for the treatment of children at risk of influenza-related complications.
-
Weight-based dosing of oseltamivir is recommended in children aged 1–12 years of age [13].
-
Oseltamivir pharmacokinetics differ in the very young. Oseltamivir should be dosed at 3.5 mg/kg orally twice daily in children aged between 9 and 11 months, and 3 mg/kg orally twice daily in infants less than 8 months of age [43].
-
NAI resistance may be an issue in the paediatric population, with higher rates of post-treatment oseltamivir resistance observed in paediatric patients, but this may be the result of under-dosing in young children, and requires further evaluation [25, 44].
-
High rates of neuropsychiatric side effects have been observed in children treated with oseltamivir (up to 36 %) and may be the result of ABCB1 polymorphism which increases brain permeability of the drug [45]. Caution should be exercised when prescribing oseltamivir to adolescents due to reports of significant neuropsychiatric events in this age group; symptomatic management should be used in those who are not at high risk of influenza-related complications [46].
Pregnancy considerations
-
Pregnant and postpartum women are at risk of influenza-related complications [2•, 47] and should receive prompt antiviral therapy with NAIs [2•, 23••]. Oseltamivir and zanamivir are pregnancy category C drugs, as a result of inadequate safety data. However, use of oseltamivir has not been associated with adverse neonatal outcomes and is recommended in pregnant and post-partum women with proven or suspected influenza [48–50].
-
Oseltamivir should be dosed per the recommendations for non-pregnant women [2•].
Adverse effects and contraindications
Oseltamivir
-
Gastrointestinal side effects occur more commonly in patients treated with oseltamivir than zanamivir [12]. Nausea and vomiting occur in approximately 10 % of patients treated with oseltamivir [2•]. Drug administration with food reduces gastrointestinal toxicity, and does not interfere with absorption [16, 51].
-
Neuropsychiatric effects (including confusion, delirium, hallucinations and self-harm) have been reported in patients treated with oseltamivir [2•]. Japanese authorities raised concerns in 2007 following suicide in two adolescents treated with oseltamivir [46]. However, widespread use of oseltamivir in Japan has not been associated with increased mortality related to self-harm [52]. A review of clinical trial and postmarketing data by the FDA failed to demonstrate a clear link between oseltamivir and neuropsychiatric events. Influenza-related encephalitis may have contributed to the neuropsychiatric events reported from Japan [46]. Patients treated with oseltamivir should be closely monitored for neuropsychiatric symptoms.
-
Oseltamivir is contraindicated in patients allergic to any components of the medication.
Zanamivir
-
Zanamivir is well-tolerated, with minor gastrointestinal upset and respiratory symptoms (sinusitis, bronchitis, cough) occurring in approximately 2 % of treated patients. Serious allergic reactions are rare [13].
-
Inhaled zanamivir is contraindicated in persons who are unable to use an inhalation device, including young children (<5 years of age), the elderly and patients with functional impairment or impaired conscious level.
-
Zanamivir has been associated with bronchospasm and is therefore relatively contraindicated in patients with underlying airways disease [30].
-
Zanamivir is contraindicated in patients allergic to lactose as it is delivered with a lactose vehicle [30].
Unresolved issues with neuraminidase inhibitors
High-dose oseltamivir
-
Standard dosing recommendations of oseltamivir are derived from trials conducted in low-risk patients with mild disease [11]. As oseltamivir is well tolerated at doses up to seven times the standard recommendation [53], authorities have suggested the use of double-dose oseltamivir, for up to 10 days’ duration, for patients with severe disease [54]. However, a multicentre, double-blind, randomised controlled trial did not show improved clinical or virological outcomes in patients with severe influenza treated with double-dose oseltamivir compared with standard dosing [55]. Likewise, in Hong Kong a prospective intervention of high-dose oseltamivir did not show significant difference in clinical or virological outcomes between patients treated with standard-dose versus high-dose oseltamivir. However, in a subanalysis of influenza B patients, higher-dose oseltamivir was associated with improved virologic response [56]. At this stage there is inadequate evidence to recommend the use of high-dose or extended-duration oseltamivir.
Optimal timing
-
The therapeutic efficacy of oseltamivir is time-dependent. Early initiation of therapy (within 48 h of symptom onset) has been shown to decrease symptom duration and severity and time taken to return to normal activities [16]. International guidelines advocate early treatment (ideally within 48 h of symptom onset) in at-risk individuals [2•, 23••]. Early initiation of NAIs has been associated with improved survival in observational studies [57, 58].
-
While it is accepted that early treatment provides maximal benefit, the efficacy of delayed treatment remains unclear. Observational data suggests that treatment with NAIs beyond 48 h is clinically beneficial in patients with severe [59] or complicated disease [60] and in pregnant women [61]. A recent randomised controlled trial demonstrated that oseltamivir reduced viral shedding and symptom duration in uncomplicated influenza, even when initiation was delayed beyond 48 h [62]. Survival benefit has been observed in patients with influenza A (H5N1) infections who received oseltamivir up to 8 days after symptom onset, but maximal benefit was observed with early initiation of therapy [63]. At this stage there is insufficient data to recommend treatment beyond 48 h in patients at low-risk of influenza-related complications. In patients at high-risk of influenza-related complications, initiation of therapy beyond 48 h should be considered. Further studies are needed to delineate the optimal timing of NAIs.
Resistance
-
Adamantanes are no longer recommended for the treatment of influenza as a result of widespread resistance. Resistance to oseltamivir has been widely reported [64] and is a problem in seasonal H1N1 [65]. Significant rates of oseltamivir-resistance have not been found in other subtypes of seasonal influenza [65].
-
In a systematic review, the overall incidence of oseltamivir resistance was 2.7 % [66], but varied by subtype, with higher rates observed in influenza A, especially the H1N1 and H3N2 subgroups [66]. Infection with oseltamivir-resistant virus was associated with influenza-related pneumonia [66]
-
Resistance to the NAIs is a result of neuraminidase mutations. The neuraminidase mutations that confer resistance vary with influenza subtype and NAI [67].
-
The H275Y mutation, in the N1 subtype, is the most common mutation and confers resistance to oseltamivir [67]. This mutation is associated with cross-resistance to peramivir but not to zanamivir [67].
-
The E119V mutation, in the N2 subtype, confers resistance to oseltamivir but zanamivir usually remains active [67].
-
The R292K mutation, also in the N2 subtype, confers resistance to oseltamivir with cross-resistance to zanamivir [67].
-
Inhaled or IV zanamivir is currently the treatment of choice for oseltamivir-resistant virus, as resistance is most commonly secondary to the H275Y mutation, to which zanamivir remains active [67].
Assistive devices
Extracorporeal membrane oxygenation
-
ECMO has been shown to improve survival in patients with acute respiratory distress syndrome (ARDS) [68]. However, there is a paucity of evidence for the use of ECMO in patients with influenza and implementation is extrapolated from ARDS trials [69].
-
Observational studies of ECMO in patients with influenza-associated ARDS have reported mortality rates between 14 and 41 % [70–73]. In a meta-analysis of ECMO in H1N1-associated ARDS, median treatment duration was 10 days and mortality ranged from 8 % to 65 %. While this treatment is feasible, patients remain at risk of in-hospital mortality [74].
-
The risks of ECMO include bleeding, complement activation, air embolism, vascular damage, and infection [75].
-
ECMO has not been shown to be superior to conventional management in patients with influenza-associated ARDS [76] and should be considered as salvage therapy. A large, randomised control trial, which includes long-term follow-up, is required to further define the role of ECMO in the management of influenza-associated ARDS.
Other treatments
Convalescent plasma and intravenous immunoglobulin preparations
-
Influenza-convalescent human blood products have been used throughout history as a treatment for influenza. A meta-analysis examining the use of convalescent blood products during the 1918 influenza pandemic demonstrated reduced mortality in patients with influenza-associated pneumonia [77]. Likewise, in Hong Kong, convalescent plasma was shown to significantly reduce mortality in patients with pandemic influenza who required intensive care support [78].
-
IV immunoglobulin (IVIG) contains pooled polyvalent immunoglobulin G (IgG) antibodies extracted from plasma. IVIG has been reported to have improved outcome in a patient with influenza-associated ARDS [79]. Hyperimmune IVIG was shown to be superior to IVIG, with reduction in influenza viral load and mortality in patients with severe influenza requiring intensive care unit support [80].
-
Complications of convalescent plasma are similar to those for blood transfusion. Hyperimmune IVIG has been associated with thromboembolic phenomenon [81].
Emerging and investigational therapies
-
The use of systemic corticosteroids in patients with influenza has been associated with increased mortality and risk of bacterial superinfection [82–84]. In a case-control study of patients with severe influenza, requiring ICU support , 90-day mortality was 54 % in patients treated with steroids versus 31 % in those without steroids [83].
-
DAS 181 (Fludase) is a recombinant sialidase fusion protein composed of a sialidase catalytic domain and a cell surface-anchoring domain. The compound has completed its initial preclinical development and entered clinical development to determine its efficacy and safety in humans [85].
-
Nitazoxanide is an oral antiparasitic that is FDA-approved for treatment of Giardia and Cryptosporidium infections. The compound recently received contract for advanced development as a treatment for drug-resistant influenza. Its mechanism of action against influenza is yet to be fully described [1].
-
Additional emerging therapies for the treatment of influenza are outlined in Table 2.
Table 2 Emerging and investigational therapies for the treatment of influenza (adapted from Patroniti et al. [71])
Seasonal influenza therapy in Japan
Japan is at the forefront of seasonal influenza research and is a world leader in the implementation of new, novel and emerging therapies.
Laninamivir
-
The long-acting NAI laninamivir has been approved in Japan since 2010. It is administered as a 40 mg single-dose inhalation, which achieves high intrapulmonary levels for up to 10 days [86]. Laninamivir has been shown to be safe and efficacious for the treatment of influenza, resulting in symptom relief at a median of 4 days [87]. It is active against influenza A and B, but has greatest efficacy against influenza A [88]. Laninamivir has similar efficacy to oseltamivir in patients with underlying respiratory disease and, unlike other inhaled NAIs, has not been shown to cause bronchospasm [89].
-
Laninamivir therapy has been shown to be safe in children with influenza. It has similar efficacy to oseltamivir but offers the advantage of a one-time inhalation. It has been shown to be effective against oseltamivir-resistant virus in the paediatric population [90]. In randomised controlled trials, laninamivir has been shown to be safe and efficacious as prophylaxis against influenza [91].
-
Laninamivir has shown promising results in Japan and may have an important role in the treatment of oseltamivir-resistant influenza.
Macrolides
-
The macrolide class of antibiotics have anti-inflammatory properties and have been investigated in Japan for the treatment of influenza. A retrospective analysis in children treated with NAIs alone or in combination with 5 days of clarithromycin demonstrated higher levels of anti-viral secretory IgA and anti-influenza serum IgG in children receiving combination therapy. The re-infection rate over the year post-treatment was reduced in the combination therapy arm [92]. Azithromycin was recently trialled in combination with oseltamivir for the treatment of influenza in adults. Unfortunately, the randomised trial failed to show a reduction in the level of inflammatory cytokines with combination therapy. However, there was a trend towards reduced duration of symptoms in the combination therapy arm [93]. The use of macrolides for the treatment of influenza requires further investigation.
Other therapies
-
Vitamin D has been proposed as a therapy for a variety of medical conditions. A randomised controlled trial of vitamin D versus placebo, for the prevention of influenza A in children, demonstrated a significant reduction in the incidence of influenza A in the vitamin D arm [94]. This therapy requires additional investigation but may be an option for prevention in countries with a defined influenza season.
References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Rossignol JF et al. Thiazolides, a new class of anti-influenza molecules targeting viral hemagglutinin at the post-translational level. J Biol Chem. 2009;284(43):29798–808.
Fiore AE et al. Antiviral agents for the treatment and chemoprophylaxis of influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2011;60(1):1–24. These guidelines represent the CDC consensus for the treatment of influenza.
WHO | Global Influenza Programme. Available from: http://www.who.int/influenza/en/. Accessed 21 Feb 2014.
Monto AS et al. Clinical signs and symptoms predicting influenza infection. Arch Intern Med. 2000;160(21):3243–7.
Simeonsson K, Moore Z. Prevention and control of influenza: no easy task. N C Med J. 2012;74(5):425–33.
Michiels B et al. A systematic review of the evidence on the effectiveness and risks of inactivated influenza vaccines in different target groups. Vaccine. 2011;29(49):9159–70. This systematic review attempts to address the important question of the efficacy of neuraminidase inhibitors, and their role in the treatment of influenza.
Udell JA et al. Association between influenza vaccination and cardiovascular outcomes in high-risk patients: a meta-analysis. JAMA. 2013;310(16):1711–20.
Michiels B et al. The value of neuraminidase inhibitors for the prevention and treatment of seasonal influenza: a systematic review of systematic reviews. PLoS One. 2013;8(4):e60348.
Leang S-K et al. Influenza antiviral resistance in the Asia-Pacific region during 2011. Antiviral Res. 2013;97(2):206–10.
Hayden FG et al. Efficacy and safety of the neuraminidase inhibitor zanamivir in the treatment of influenzavirus infections. GG167 Influenza Study Group. N Engl J Med. 1997;337(13):874–80.
Nicholson KG et al. Efficacy and safety of oseltamivir in treatment of acute influenza: a randomised controlled trial. Neuraminidase Inhibitor Flu Treatment Investigator Group. Lancet. 2000;355(9218):1845–50.
Treanor JJ et al. Efficacy and safety of the oral neuraminidase inhibitor oseltamivir in treating acute influenza. JAMA. 2000;283(8):1016–24.
Moscona A. Neuraminidase inhibitors for influenza. N Engl J Med. 2005;353(13):1363–73.
Jefferson T et al. Antivirals for influenza in healthy adults: systematic review. Lancet. 2006;367(9507):303–13.
Furuta Y et al. Favipiravir (T-705), a novel viral RNA polymerase inhibitor. Antiviral Res. 2013;100(2):446–54. This paper reviews an influenza polymerase inhibitor under clinical development. Available data demonstrates that the new class is active against neuraminidase-resistant influenza viruses, suggesting it will be useful in the future influenza armamentarium.
Aoki FY et al. Early administration of oral oseltamivir increases the benefits of influenza treatment. J Antimicrob Chemother. 2003;51(1):123–9.
Hernan MA, Lipsitch M. Oseltamivir and risk of lower respiratory tract complications in patients with flu symptoms: a meta-analysis of eleven randomized clinical trials. Clin Infect Dis. 2011;53(3):277–9.
Heinonen S et al. Early oseltamivir treatment of influenza in children 1-3 years of age: a randomized controlled trial. Clin Infect Dis. 2010;51(8):887–94.
Cohen D. Complications: tracking down the data on oseltamivir. BMJ. 2009;339:b5387.
Jefferson T et al. Neuraminidase inhibitors for preventing and treating influenza in healthy adults and children. Cochrane Database Syst Rev. 2012;1, CD008965.
Hsu J et al. Antivirals for treatment of influenza: a systematic review and meta-analysis of observational studies. Ann Intern Med. 2012;156(7):512–24.
Muthuri SG, et al. Effectiveness of neuraminidase inhibitors in reducing mortality in patients admitted to hospital with influenza A H1N1pdm09 virus infection: a meta-analysis of individual participant data. Lancet Respir Med. 2014 Epub 19 Mar 2014. This meta-analysis of patients hospitalized with influenza A H1H1(09) during the pandemic demonstrates a mortality benefit with NAI therapy.
WHO. Guidelines for pharmacological management of pandemic influenza A(H1N1) 2009 and other influenza viruses. WHO guidelines approved by the Guidelines Review Committee. Geneva: World Health Organization; 2010. Excellent guideline and review.
Tullu MS. Oseltamivir. J Postgrad Med. 2009;55(3):225–30.
Moscona A. Oseltamivir resistance:disabling our influenza defenses. N Engl J Med. 2005;353(25):2633–6.
Lemaitre F et al. Impact of extracorporeal membrane oxygenation and continuous venovenous hemodiafiltration on the pharmacokinetics of oseltamivir carboxylate in critically ill patients with pandemic (H1N1) influenza. Ther Drug Monit. 2012;34(2):171–5.
Robson R et al. The pharmacokinetics and tolerability of oseltamivir suspension in patients on haemodialysis and continuous ambulatory peritoneal dialysis. Nephrol Dial Transplant. 2006;21(9):2556–62.
Brennan BJ et al. Safety, tolerability, and pharmacokinetics of intravenous oseltamivir: single- and multiple-dose phase I studies with healthy volunteers. Antimicrob Agents Chemother. 2012;56(9):4729–37.
Taylor WR et al. Oseltamivir is adequately absorbed following nasogastric administration to adult patients with severe H5N1 influenza. PLoS One. 2008;3(10):e3410.
GlaxoSmithKline. RELENZA: highlights of prescribing information. 2013.
Kiatboonsri S, Kiatboonsri C, Theerawit P. Fatal respiratory events caused by zanamivir nebulization. Clin Infect Dis. 2010;50(4):620–0.
Steel HM, Peppercorn AF. Fatal respiratory events caused by zanamivir nebulization. Clin Infect Dis. 2010;51(1):121.
US FDA. Safety alerts for human medical products. Relenza (zanamivir) inhalation powder. Available from: http://www.fda.gov/safety/medwatch/safetyinformation/safetyalertsforhumanmedicalproducts/ucm186081.htm. Accessed 12 Feb 2014.
Marty FM et al. Safety and pharmacokinetics of intravenous zanamivir treatment in hospitalized adults with influenza: an open-label, multicenter, single-arm, phase II study. J Infect Dis. 2014;209(4):542–50.
Weller S et al. Pharmacokinetics of zanamivir following intravenous administration to subjects with and without renal impairment. Antimicrob Agents Chemother. 2013;57(7):2967–71.
Kohno S et al. Efficacy and safety of intravenous peramivir for treatment of seasonal influenza virus infection. Antimicrob Agents Chemother. 2010;54(11):4568–74.
Kohno S et al. Intravenous peramivir for treatment of influenza A and B virus infection in high-risk patients. Antimicrob Agents Chemothe. 2011;55(6):2803–12.
Hernandez JE et al. Clinical experience in adults and children treated with intravenous peramivir for 2009 influenza A (H1N1) under an Emergency IND program in the United States. Clin Infect Dis. 2011;52(6):695–706.
Louie JK et al. Use of intravenous peramivir for treatment of severe influenza A(H1N1)pdm09. PLoS One. 2012;7(6):e40261.
Izurieta HS et al. Influenza and the rates of hospitalization for respiratory disease among infants and young children. N Engl J Med. 2000;342(4):232–9.
Matheson NJ et al. Neuraminidase inhibitors for preventing and treating influenza in children. Cochrane Database Syst Rev. 2007;1, CD002744.
Sugaya N et al. Very low pandemic influenza A (H1N1) 2009 mortality associated with early neuraminidase inhibitor treatment in Japan: analysis of 1000 hospitalized children. J Infect. 2011;63(4):288–94.
Kimberlin DW et al. Oseltamivir pharmacokinetics, dosing, and resistance among children aged <2 years with influenza. J Infect Dis. 2013;207(5):709–20.
Kiso M et al. Resistant influenza A viruses in children treated with oseltamivir: descriptive study. Lancet. 2004;364(9436):759–65.
L'Huillier AG et al. ABCB1 polymorphisms and neuropsychiatric adverse events in oseltamivir-treated children during influenza H1N1/09 pandemia. Pharmacogenomics. 2011;12(10):1493–501.
Maxwell SRJ. Tamiflu and neuropsychiatric disturbance in adolescents. BMJ. 2007;334(7606):1232–3.
Jamieson DJ et al. H1N1 2009 influenza virus infection during pregnancy in the USA. Lancet. 2009;374(9688):451–8.
Greer LG et al. Maternal and neonatal outcomes after antepartum treatment of influenza with antiviral medications. Obstet Gynecol. 2010;115(4):711–6.
Xie H-Y et al. Infant outcomes among pregnant women who used oseltamivir for treatment of influenza during the H1N1 epidemic. Am J Obstet Gynecol. 2013;208(4):293.e1–7.
Donner B, Niranjan V, Hoffmann G. Safety of oseltamivir in pregnancy: a review of preclinical and clinical data. Drug Saf. 2010;33(8):631–42.
Hayden FG et al. Use of the selective oral neuraminidase inhibitor oseltamivir to prevent influenza. N Engl J Med. 1999;341(18):1336–43.
Sugaya N. Widespread use of neuraminidase inhibitors in Japan. J Infect Chemother. 2011;17(5):595–601.
Massarella JW et al. The pharmacokinetics and tolerability of the oral neuraminidase inhibitor oseltamivir (Ro 64–0796/GS4104) in healthy adult and elderly volunteers. J Clin Pharmacol. 2000;40(8):836–43.
Bautista E, Chotpitayasunondh T, Gao Z, et al. Writing Committee of the WHO Consultation on Clinical Aspects of Pandemic (H1N1) 2009 Influenza. Clinical aspects of pandemic 2009 influenza A (H1N1) virus infection. N Engl J Med. 2010;362(18):1708–19.
South East Asia Infectious Disease Clinical Research Network. Effect of double dose oseltamivir on clinical and virological outcomes in children and adults admitted to hospital with severe influenza: double blind randomised controlled trial. BMJ. 2013;346:f3039.
Lee N et al. A prospective intervention study on higher-dose oseltamivir treatment in adults hospitalized with influenza a and B infections. Clin Infect Dis. 2013;57(11):1511–9.
Lee N et al. Outcomes of adults hospitalised with severe influenza. Thorax. 2010;65(6):510–5.
Muthuri SG et al. Impact of neuraminidase inhibitor treatment on outcomes of public health importance during the 2009-2010 influenza A(H1N1) pandemic: a systematic review and meta-analysis in hospitalized patients. J Infect Dis. 2013;207(4):553–63.
Louie JK et al. Treatment with neuraminidase inhibitors for critically ill patients with influenza A (H1N1)pdm09. Clin Infect Dis. 2012;55(9):1198–204.
Yang SG et al. Antiviral therapy and outcomes of patients with pneumonia caused by influenza A pandemic (H1N1) virus. PLoS One. 2012;7(1):e29652.
Siston AM et al. Pandemic 2009 influenza A(H1N1) virus illness among pregnant women in the United States. JAMA. 2010;303(15):1517–25.
Fry AM et al. Efficacy of oseltamivir treatment started within 5 days of symptom onset to reduce influenza illness duration and virus shedding in an urban setting in Bangladesh: a randomised placebo-controlled trial. Lancet Infect Dis. 2014;14(2):109–18.
Adisasmito W et al. Effectiveness of antiviral treatment in human influenza A(H5N1) infections: analysis of a global patient registry. J Infect Dis. 2010;202(8):1154–60.
Dharan NJ et al. Infections with oseltamivir-resistant influenza A(H1N1) virus in the United States. JAMA. 2009;301(10):1034–41.
Whitley RJ et al. Global assessment of resistance to neuraminidase inhibitors, 2008-2011: the Influenza Resistance Information Study (IRIS). Clin Infect Dis. 2013;56(9):1197–205.
Thorlund K et al. Systematic review of influenza resistance to the neuraminidase inhibitors. BMC Infect Dis. 2011;11(1):134.
Boivin G. Detection and management of antiviral resistance for influenza viruses. Influenza Other Respir Viruses. 2013;7 Suppl 3:18–23.
Peek GJ et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009;374(9698):1351–63.
Mitchell MD et al. A systematic review to inform institutional decisions about the use of extracorporeal membrane oxygenation during the H1N1 influenza pandemic. Crit Care Med. 2010;38(6):1398–404.
Davies A et al. Extracorporeal membrane oxygenation for 2009 influenza A(H1N1) acute respiratory distress syndrome. JAMA. 2009;302(17):1888–95.
Patroniti N et al. The Italian ECMO network experience during the 2009 influenza A(H1N1) pandemic: preparation for severe respiratory emergency outbreaks. Intensive Care Med. 2011;37(9):1447–57.
Domínguez-Cherit G et al. Critically ill patients with 2009 influenza A(H1N1) in Mexico. JAMA. 2009;302(17):1880–7.
Kumar A et al. Critically ill patients with 2009 influenza A(H1N1) infection in Canada. JAMA. 2009;302(17):1872–9.
Zangrillo A et al. Extracorporeal membrane oxygenation (ECMO) in patients with H1N1 influenza infection: a systematic review and meta-analysis including 8 studies and 266 patients receiving ECMO. Crit Care. 2013;17(1):R30.
Morris AH et al. Counterpoint: efficacy of extracorporeal membrane oxygenation in 2009 influenza A(H1N1): sufficient evidence? Chest. 2010;138(4):778–81. discussion 782-784l.
Pham T et al. Extracorporeal membrane oxygenation for pandemic influenza A(H1N1)-induced acute respiratory distress syndrome: a cohort study and propensity-matched analysis. Am J Respir Crit Care Med. 2013;187(3):276–85.
Luke TC et al. Meta-analysis: convalescent blood products for Spanish influenza pneumonia: a future H5N1 treatment? Ann Intern Med. 2006;145(8):599–609.
Hung IF et al. Convalescent plasma treatment reduced mortality in patients with severe pandemic influenza A (H1N1) 2009 virus infection. Clin Infect Dis. 2011;52(4):447–56.
Chong JL, Sapari S, Kuan YC. A case of acute respiratory distress syndrome associated with novel H1N1 treated with intravenous immunoglobulin G. J Microbiol Immunol Infect. 2011;44(4):319–22.
Hung IFN et al. Hyperimmune IV immunoglobulin treatment: a multicenter double-blind randomized controlled trial for patients with severe 2009 influenza A(H1N1) infection. Chest. 2013;144(2):464–73.
Hui DS, Lee N, Chan PK. Adjunctive therapies and immunomodulatory agents in the management of severe influenza. Antiviral Res. 2013;98(3):410–6.
Brun-Buisson C et al. Early corticosteroids in severe influenza A/H1N1 pneumonia and acute respiratory distress syndrome. Am J Respir Crit Care Med. 2011;183(9):1200–6.
Kim S-H et al. Corticosteroid treatment in critically ill patients with pandemic influenza A/H1N1 2009 infection: analytic strategy using propensity scores. Am J Respir Crit Care Med. 2011;183(9):1207–14.
Martin-Loeches I et al. Use of early corticosteroid therapy on ICU admission in patients affected by severe pandemic (H1N1)v influenza A infection. Intensive Care Med. 2011;37(2):272–83.
Triana-Baltzer GB et al. Novel pandemic influenza A(H1N1) viruses are potently inhibited by DAS181, a sialidase fusion protein. PLoS One. 2009;4(11):e7788.
Ishizuka H et al. Intrapulmonary distribution and pharmacokinetics of laninamivir, a neuraminidase inhibitor, after a single inhaled administration of its prodrug, laninamivir octanoate, in healthy volunteers. Antimicrob Agents Chemother. 2012;56(7):3873–8.
Kashiwagi S et al. Clinical efficacy of long-acting neuraminidase inhibitor laninamivir octanoate hydrate in postmarketing surveillance. J Infect Chemother. 2013;19(2):223–32.
Ikematsu H et al. The duration of fever and other symptoms after the initiation of laninamivir octanoate hydrate in the Japanese 2011–2012 influenza season. J Infect Chemother. 2014;20(2):81–5.
Watanabe A. A randomized double-blind controlled study of laninamivir compared with oseltamivir for the treatment of influenza in patients with chronic respiratory diseases. J Infect Chemother. 2013;19(1):89–97.
Sugaya N, Ohashi Y. Long-acting neuraminidase inhibitor laninamivir octanoate (CS-8958) versus oseltamivir as treatment for children with influenza virus infection. Antimicrob Agents Chemother. 2010;54(6):2575–82.
Kashiwagi S et al. Laninamivir octanoate for post-exposure prophylaxis of influenza in household contacts: a randomized double blind placebo controlled trial. J Infect Chemother. 2013;19(4):740–9.
Shinahara W et al. Immunomodulator clarithromycin enhances mucosal and systemic immune responses and reduces re-infection rate in pediatric patients with influenza treated with antiviral neuraminidase inhibitors: a retrospective analysis. PLoS One. 2013;8(7):e70060.
Kakeya H et al. Efficacy of combination therapy with oseltamivir phosphate and azithromycin for influenza: a multicenter, open-label, randomized study. PLoS One. 2014;9(3):e91293.
Urashima M et al. Randomized trial of vitamin D supplementation to prevent seasonal influenza A in schoolchildren. Am J Clin Nutr. 2010;91(5):1255–60.
US FDA. Postmarket drug safety information for patients and providers. Tamiflu (oseltamivir phosphate) information. Available from: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm107838.htm. Accessed 13 Feb 2014.
Centers for Disease Control and Prevention. Influenza antiviral medications: summary for clinicians. Available from: http://www.cdc.gov/flu/professionals/antivirals/summary-clinicians.htm. Accessed 24 Apr 2014.
US FDA. Postmarket drug safety information for patients and providers. Relenza (zanamivir) information. Available from: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm183783.htm. Accessed 13 Feb 2014.
Hayden F. Newer influenza antivirals, biotherapeutics and combinations. Influenza Other Respir Viruses. 2013;7 Suppl 1:63–75.
US FDA. Postmarket drug safety information for patients and providers. Peramivir IV questions and answers for health care providers. Available from: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm187980.htm. Accessed 13 Feb 2014.
Prober CG. Antiviral therapy for influenza virus infections. Semin Pediatr Infect Dis. 2002;13(1):31–9.
Lai KY et al. High-dose N-acetylcysteine therapy for novel H1N1 influenza pneumonia. Ann Intern Med. 2010;152(10):687–8.
Takeda S et al. Hypercytokinemia with 2009 pandemic H1N1 (pH1N1) influenza successfully treated with polymyxin B-immobilized fiber column hemoperfusion. Intensive Care Med. 2010;36(5):906–7.
Patel P et al. Use of therapeutic plasma exchange as a rescue therapy in 2009 pH1N1 influenza A: an associated respiratory failure and hemodynamic shock. Pediatr Crit Care Med. 2011;12(2):e87–89.
Kwong JC, Li P, Redelmeier DA. Influenza morbidity and mortality in elderly patients receiving statins: a cohort study. PLoS One. 2009;4(11):e8087.
Vandermeer ML et al. Association between use of statins and mortality among patients hospitalized with laboratory-confirmed influenza virus infections: a multistate study. J Infect Dis. 2012;205(1):13–9.
Brett SJ et al. Pre-admission statin use and in-hospital severity of 2009 pandemic influenza A(H1N1) disease. PLoS One. 2011;6(4):e18120.
Ishii H et al. Clarithromycin has limited effects in non-elderly, non-severe patients with seasonal influenza virus A infection. J Infect. 2012;64(3):343–5.
Han K et al. Early use of glucocorticoids was a risk factor for critical disease and death from pH1N1 infection. Clin Infect Dis. 2011;53(4):326–33.
Acknowledgement
The authors wish to acknowledge Professor Frederick G. Hayden, MD, University of Virginia, Charlottesville, VA, USA, for his invaluable advice on the manuscript, and Dr. Linn Thein Tun for administrative assistance.
Compliance with Ethics Guidelines
ᅟ
Conflict of Interest
Emily Rowe declares that she has no conflicts of interest.
Yee-Sin Leo declares that she has no conflicts of interest.
Mark I. Cheng Chen declares that he has no conflicts of interest.
Pei Yi Ng declares that she has no conflicts of interest.
Thiaghu Chandra declares that he has no conflicts of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Rowe, E., Ng, P.Y., Chandra, T. et al. Seasonal Human Influenza: Treatment Options. Curr Treat Options Infect Dis 6, 227–244 (2014). https://doi.org/10.1007/s40506-014-0019-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40506-014-0019-z