
Abstract
The mechanisms underlying range of motion enhancements via flexibility training discussed in the literature show high heterogeneity in research methodology and study findings. In addition, scientific conclusions are mostly based on functional observations while studies considering the underlying physiology are less common. However, understanding the underlying mechanisms that contribute to an improved range of motion through stretching is crucial for conducting comparable studies with sound designs, optimising training routines and accurately interpreting resulting outcomes. While there seems to be no evidence to attribute acute range of motion increases as well as changes in muscle and tendon stiffness and pain perception specifically to stretching or foam rolling, the role of general warm-up effects is discussed in this paper. Additionally, the role of mechanical tension applied to greater muscle lengths for range of motion improvement will be discussed. Thus, it is suggested that physical training stressors can be seen as external stimuli that control gene expression via the targeted stimulation of transcription factors, leading to structural adaptations due to enhanced protein synthesis. Hence, the possible role of serial sarcomerogenesis in altering pain perception, reducing muscle stiffness and passive torque, or changes in the optimal joint angle for force development is considered as well as alternative interventions with a potential impact on anabolic pathways. As there are limited possibilities to directly measure serial sarcomere number, longitudinal muscle hypertrophy remains without direct evidence. The available literature does not demonstrate the necessity of only using specific flexibility training routines such as stretching to enhance acute or chronic range of motion.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Stretching and foam rolling are the most common training interventions when aiming to acutely or chronically increase range of motion. However, it seems questionable to attribute the flexibility increases exclusively to these training routines. |
The limitations in study methodology are discussed, including different training protocols that result in improved range of motion. This leads to the misinterpretation of the findings based on speculative physiological mechanisms. |
Acute and chronic stretching are of limited efficacy. Similar range of motion enhancements can be achieved via other training interventions sufficient to enhance body temperature acutely, while chronically, applying mechanical tension to extended muscle lengths seems one important factor, achievable through concurrent alternatives (e.g. resistance training). |
1 Introduction
In sports practice, improving physical fitness requires a well-planned and structured training process. Clear definitions and understanding the underlying mechanisms increasing range of motion (ROM) via different methods is a vital prerequisite for developing training regimes. In flexibility research, many definitions regarding flexibility have been proposed [1, 2] which range from “total achievable excursion (within limits of pain) of a body part through its potential range of motion (ROM)” to “ability to move a joint through a normal ROM without undue stress to the musculotendinous unit” [3, 4].
In recent decades, numerous stretching modalities [2, 4,5,6,7,8,9,10], in addition to foam rolling interventions [11,12,13,14,15,16,17] as well as different massage techniques [18] with their respective acute and chronic effects on flexibility were investigated using different study methodologies and outcomes. Because most of the interventions showed increased flexibility [4, 6, 17, 19], questions arise about possible shared underlying mechanisms between these interventions. Additionally, regarding chronic flexibility increases, there is a vast amount of evidence pointing out the listed stretching modalities as sufficient to increase ROM. Most studies explained flexibility increases via changes in muscle–tendon stiffness and changes in the pain threshold [20] as the most frequently reported explanatory approaches [3, 4, 21,22,23,24,25]. However, because acute and chronic flexibility increases can also be induced via other training routines, this narrative review discusses the similarities and discrepancies in underlying mechanisms between different methods leading to enhanced acute and chronic flexibility and provides explanatory approaches based on a biological and systematic level.
2 Overview About the Most Popular Training Protocols and Results to Enhance Flexibility
Stretching can be considered as the most popular modality to increase ROM. Commonly, the literature describes static stretching as holding a muscle in the end ROM at the point of discomfort, while dynamic stretching is described as performing controlled movements in the end ROM or ballistic stretching using bouncing movements [2]. Proprioceptive neuromuscular facilitation (PNF) could be divided into three subcategories, using cycles of static stretching and (sub)maximal contraction of the stretched muscle contract-relax PNF, the antagonist contraction method that uses antagonist contraction with static stretching and the contract relax antagonist contraction method, which combines both methods [2].
2.1 Acute Flexibility Effects
Regarding acute flexibility improvements, the literature provides no clear evidence which stretching technique should be prioritised within a single training session. There is evidence supporting the effectiveness of all stretching types to increase ROM [3, 4, 8, 9, 15, 26,27,28,29]. Accordingly, recent systematic reviews (with meta-analyses) have similarly reported no difference between one bout of static stretching and dynamic stretching [30], as well as no significant acute ROM differences between the reviewed stretching techniques, independent of stretch intensity, sex or training level [31]. The literature has attributed acute stretch-induced flexibility increases to enhanced pain (stretch) tolerance [13, 31, 32] possibly due to adaptations of nociceptive nerve endings, as well as decreased stiffness in the musculotendinous unit [33], muscle [19, 34,35,36,37] and tendon [38, 39] properties [40, 41], as well as thixotropic effects [13]. Based on these adaptations, stretching was considered an integral component of warm-up routines over decades [42, 43]. However, most current systematic reviews addressing the acute effects of prolonged static stretching (i.e. > 60 s per muscle group) on strength performance did not recommend its inclusion in warm-up routines because of its harmful effects on subsequent performance [44, 45]. Even though the negative influence on performance could be compensated/weakened by adding more active and dynamic warm-up activities to stretching [46], the listed limitations called for alternative routines that acutely improved flexibility without impairing subsequent performance.
Therefore, the literature proposed foam rolling as a sufficient alternative to prolonged static stretching to acutely enhance flexibility. Foam rolling involves small undulations over a muscle with a dense foam wrap around a solid plastic cylinder, rolling from the proximal to distal portion of the muscle or vice versa [2, 47]. The participant usually places the foam roll on the ground or floor, with recommendations to perform 2–4 s repetition duration (time for a single roll in one direction over the length of a body part) with a total rolling duration of 30–120 s per set [48] in order to apply mechanical pressure to the tissue. Foam rolling is proposed to be helpful regarding several aspects, such as increasing flexibility [17], decreasing pain, minimising symptoms of delayed-onset muscle soreness and the release of myofascial adhesions [17, 47]. Therefore, to acutely increase ROM in warm-up routines, the use of foam rollers is frequently recommended [17, 49, 50] with expected ROM increasing approximately 4.0% [11], similar to static stretching [13, 17]. Suggested underlying mechanisms seem similar as well with reported foam rolling effects on muscle stiffness [51,52,53], or reduced pain sensitivity [54, 55]. Further explanatory approaches suggesting myofascial release would cause, for example, stiffness decreases, and blood flow changes seem not appropriately investigated [47]. While stretching total durations of up to 480 s were described of practical relevance [56, 57], most studies used stretch durations per bout with up to 120 s [45]. For foam rolling, the literature recommends the usage of up to 4 × 60 s [48, 58]. Even though Konrad et al. [13] showed no difference in acute ROM effects with foam rolling, studies that directly compared the dose–response relationship for foam rolling and stretching were not found.
The literature provides further alternatives to static stretching. Interestingly, in accordance with Alizadeh et al. [59], full ROM resistance training can be considered a type of loaded dynamic stretching. However, only a few studies explored the acute effects of resistance training on ROM. For example, Warneke et al. [60] showed no significant difference between acute ROM increases in the calf muscles comparing high-volume stretching (1 h) with an exhausting calf raise routine consisting of 5 × 12 repetitions performed over the full ROM. Most recently, Murakami et al. [61] showed 3 × 10 repetitions of full ROM standing calf raise exercises to be effective in increasing ROM and passive peak torque, while stiffness remained unaffected. Additionally, Oliveira et al. [62] found no acute stiffness reductions in the pectoralis muscle after 3 × 8–13 repetitions of bench press. In contrast, Krzysztofik et al. [63] showed significant stiffness reductions in the Achilles tendon and the quadriceps as an acute response to one to two bouts of barbell squats. Kawama et al. [64, 65] reported significant stiffness reductions in the hamstrings when training was performed over the full ROM. Thus, resistance training also seems to acutely improve flexibility, however, without clear evidence regarding their underlying mechanisms. These are only a few examples, other studies demonstrated flexibility enhancements after using alternative routines such as “neurodynamic techniques” [66,67,68], flossing [69] and massage with percussive massage devices [70].
2.2 Acute ROM Improvements Due to Enhanced Muscle Temperature?
With the current literature of acute stretching effects, it can be noted that most of the listed activities applied training stimuli on the muscle with similar responses, including reduced pain sensitivity [12, 13, 31], and reduced muscle, tendon or muscle tendon unit stiffness [33]. These adaptations could be induced by improvements in viscoelastic properties and thixotropic effects [13, 47]. However, these phenomena and outcomes are not exclusively attributable to stretching or foam rolling or other specialised interventions.
Most stretching or foam rolling studies included a passive control group. However, these comparisons are only valid to show that both routines can be used to enhance flexibility compared with doing nothing. However, the enhanced flexibility may not be just attributed to the actions of stretching or foam rolling as there may be other alternative explanations. As the listed training interventions improved flexibility compared with an inactive control, these findings merely support the notion that overall activity appears to be sufficient in comparison to a state of rest. However, as general muscle dynamic activity is known to enhance muscle and core temperature (general warm-up effects), which are sufficient to economise muscle contractions by decreasing joint friction, increasing synovial fluid with accompanied decreases in muscle viscosity [71, 72] and increased blood flow [73]. Interestingly, Reid [74] described a warm-up-related improvement in the myotatic reflex, leading to a later occurrence of stretching pain. Consequently, it could be hypothesised that stretching/foam rolling/resistance training effects might originate from general warm-up effects occurring from muscle contraction-induced exothermal ATP splitting while performing foam rolling/dynamic stretching. Even though static stretching electromyography activity was smaller compared with alternative methods [75], Oliveira et al. [76] confirmed temperature increases after performing 180 s of static stretching.
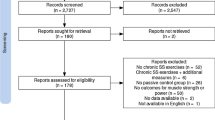
To show the necessity of including specific interventions to warm-up routines, a superior effect of stretching or foam rolling compared with alternative routines must be assumed, which cannot be investigated by studies with passive control conditions. Comparing and contrasting stretching and foam rolling responses to the effects of jogging [77], cycling [78], resistance training [60], heat applications [79, 80] or cryotherapy [81], Warneke et al. [82] were not able to confirm the necessity of using specialised routines to acutely enhance flexibility or passive peak torque. While the authors hypothesised a thermal (e.g. thixotropic) effect with general activity-related warm-ups, almost no study assessed muscle and/or core temperature after these routines. Thus, the magnitude of the influence remains speculative. Even though dynamic warm-up effects can contribute to ROM increases, some studies indicated superior effects when using full ROM movements compared with partial ROM [61, 64, 65]. Full ROM movements may provide additional specific factors such as stretching tension, and greater contributions of eccentric contractions. However, the current literature typically did not use appropriate methods to clearly attribute the acute ROM increases solely to foam rolling, stretching, vibration training or other modalities. As only two studies included temperature measurements in response to stretching [76] and foam rolling [83], both confirming increased temperature, observed effects might be attributable to general dynamic warm-up effects. Thus, highly specific explanatory approaches remain speculative and without sufficient evidence, especially when speculating about contralateral and global acute ROM effects of stretching [84, 85] and foam rolling [86, 87] (e.g. influence of myofascial chains) [88]. The available research designs do not allow specific conclusions and should further control approaches to investigate the role of warm-up effects when explaining variance (e.g. temperature), as no further parameters and explanations were controlled to rule out warm-up effects, which could also explain global flexibility enhancements (see Fig. 1).

Alternative training routines extracted from the literature that also induced flexibility increases, partially without including stretching. Calf muscles were used as a frequently used example from reviewed studies
Thus, we do not doubt the high complexity of physiological mechanisms contributing to acute flexibility increases in response to stretching and foam rolling [17, 47] and are aware that these cannot simply be attributed to general warm-up effects. However, future research designs should consider further approaches.
3 Chronic Flexibility Effects
Stretching might be the most common training intervention when aiming to improve flexibility long term. In 2018, Thomas et al. [28] initially asserted the superior effectiveness of static stretching. However, in 2023, Konrad and colleagues [89] updated this perspective by including PNF stretching (in addition to static stretching) as one of the most effective stretching interventions, surpassing dynamic and ballistic stretching. Dynamic stretching demonstrated moderate-magnitude effect size improvements (d = 0.55), while static and PNF stretching induced larger magnitude effect sizes (d = 1.005 and 1.283, respectively) [89]. As described above, full ROM resistance training might be considered as dynamic loaded stretching [59], which seems interchangeable with stretching routines [5, 59, 90].
Chronic foam rolling effects were explored in a recent meta-analysis that included 11 studies with intervention periods of at least 4 weeks. The results indicated large magnitude increases with an effect size of = 0.823 in joint ROM in the hamstrings and quadriceps, while ineffective for the ankle dorsiflexors [12]. Nevertheless, the results conflict with those of other meta-analyses performed by Pagaduan et al. [91] and Grieve et al. [92] that revealed conflicting and no improvements in response to foam rolling, respectively. Similar to stretching, there is an ongoing discussion regarding the underlying mechanisms of foam rolling. While chronic stretch-induced ROM enhancements were attributed to a combination of structural adaptations (muscle and/or tendon properties) [25, 93, 94] and neuronal changes such as changes in the stretching pain threshold [21,22,23, 95], foam rolling studies generally agree in attributing ROM increases to enhanced pain tolerance rather than stiffness changes [96, 97]. Non-significant effects were discussed to be attributable to the low-volume interventions of the studies [12, 16].
The literature shows several interventions to induce similar flexibility increases that were accompanied by an overlap in contributing factors such as stiffness decreases, as well as pain threshold increases. Therefore, the question arises about the shared underlying physiology of the listed intervention.
3.1 3.1. Mechanical Tension with Extended Muscle Lengths as a Possible Underlying Cause for Long-Term ROM Increases—Strength Training or Stretching?
When aiming to improve flexibility long term, it is necessary to perform regular training routines for at least a period of weeks. Undoubtedly, stretch training is one of the most frequently used and investigated training methods to induce ROM improvements [3, 9, 89, 98,99,100,101,102]. In contrast to acute effects, there is little evidence demonstrating chronic ROM increases in response to foam rolling [12], opposed by research pointing out unclear evidence [16, 91, 96]. Possible long-term effects of foam rolling were attributed to the possibility of traction-induced soft-tissue release [16], which is, in fact, not evidence based, while there seems insufficient evidence to support foam rolling as an effective method to release myofascial restrictions [47]. Consequently, Konrad et al. [16] requested further research to address foam rolling-specific underlying mechanisms. Based on contrasting results from available systematic reviews, we decided to focus on training methods with clear evidence instead of speculating about underlying mechanisms of interventions with questionable effectiveness. As Alizadeh and colleagues suggested resistance training to be considered a type of dynamic (loaded) stretching, they pointed out resistance training as a valid alternative to stretch training, showing similar flexibility increases in the long term [5, 59, 90, 103]. Even though it is not clarified if the eccentric portion of full ROM resistance training or the mechanical tension in extended muscle lengths can be considered the underlying mechanisms, stretching alone seems sufficient to induce similar adaptations compared with full ROM resistance training, which is not limited to flexibility changes. While resistance training is recognised for promoting maximal strength gains and hypertrophy, Arntz et al. [104] and Warneke et al. [103] highlighted strength improvements and hypertrophy resulting from stretch training. Notably, stretch training at longer muscle lengths appears to be more effective in inducing muscle hypertrophy [105]. Even though meta-analyses reported smaller magnitude effects of stretching, the results lead us to the question about similarities in the stimulus as well as the underlying physiology.
While not frequently discussed in the stretching literature, a plethora of studies reported the high relevance of mechanical tension in resistance training. Interestingly, when aiming to increase flexibility via resistance training, Alizadeh et al. [59] reported a high relevance of the eccentric portion when performing resistance training [106, 107]. Thus, it can be hypothesised that mechanical stretching would result in changes in the sarcomere length beyond the tissues’ tolerance [108]. More specifically, it has been suggested that these improvements can be related to the remodeling of the extracellular matrix responding to a sarcomere stretch [109]. When comparing ROM effects of 1 h of daily stretching with a commonly performed resistance training (5 × 12 repetitions on 3 days per week for 6 weeks) on muscle thickness, maximal strength and flexibility in the plantar flexors, Warneke et al. [103] showed no significant difference in flexibility increases and hypothesised similarities in the outcomes could possibly be attributed to mechanical tension applied to extended muscle lengths. Assuming that full ROM resistance training and stretching to be sufficient to induce suprathreshold mechanical stimuli in high muscle lengths, the biochemical responses caused by a mechanical overload and its potential impact on ROM enhancements will be discussed in the following.
While it is well established that, in general, skeletal muscle adapts to different mechanical external loads influenced by molecular, subcellular and cellular adaptations [110,111,112,113], many specific aspects remain unknown. While numerous animal studies have investigated the stretch-induced protein synthesis enhancements and its impact on cross-sectional hypertrophy of the muscle, the evidence for longitudinal hypertrophy (increased muscle length) is comparatively limited [114]. These studies frequently reported muscle mass enhancements [115,116,117] and confirmed the stimulation of the myofibrillar protein synthesis rate after inducing mechanical tension via stretching [118,119,120]. Partially, the enhanced muscle volume was attributed to an increased serial sarcomere number, which was reported in animals after only a few days [121,122,123,124] with a consistent large magnitude effect of d = 3.31, 95% confidence interval 1.52–5.09, 26.1 ± 7.3% [125].
On a subcellular basis, it can be assumed that stretching causes lengthening of a contractile filament by increasing the distance between the origin and muscle attachment. This position seems to provide a disadvantaged position for contraction due to lower myosin-actin cross-bridge potential while unfolded titin filaments in stretched positions [126, 127] could increase contractile unit tension. Assuming this stretched muscle position to cause a stress stimulus underlines the impact of mechanical overload, which could be achieved via stretching. Herring et al. [128] pointed out that a high “sarcomere number is adjusted so as to achieve an optimum sarcomere length when the muscle is experiencing a high level of tension “, which is stated as the most likely hypothesis. Morphological adaptations can be considered as an optimising process to improve contraction properties. In a given muscle length, increasing the number of sarcomeres in series can be hypothesised to reduce the stretch tension per sarcomere as a suggested underlying mechanism [59, 103, 124], leading to a higher degree in the overlap of the contractile filaments. Accordingly, Zöllner et al. [129] described sarcomerogenesis [114] as a response of skeletal muscle [123] to gradually return into its optimal operating regime after experiencing a stretch beyond the normal physiological limits. This dynamic adjustment can be assumed to be a key factor in long-term regeneration and repairing processes [113, 129, 130]. By inducing a chronic stress situation, Wisdom et al. [110] assumed chronic overstretch [126, 131] and eccentric exercise [108, 132] to be responsible for adding sarcomeres in series, thus increasing muscle length. In contrast, in cats [133], immobilising a muscle in a shortened/flexed joint position caused a decrease in sarcomeres in series and muscle shortening [134, 135]. Both mechanisms were speculated to optimise the pre-condition for contraction by maximising actin-myosin crossbridge potential. Apart from serial sarcomere accumulation [112, 123, 126, 135, 136], longitudinal hypertrophy could also occur in the muscle fascicle [130]. It seems that mechanical tension is sufficient to induce significant morphological changes in skeletal animal muscles [112, 113, 118, 133, 135,136,137], thus not exclusively important to enhance the muscle cross-sectional area, but also the muscle length (serial sarcomere number).
Moreover, as described above, increasing the distance between Z-discs and the subsequent titin unfolding, which can be assumed by adopting large degrees of stretching, could be of paramount importance for structural muscle adaptations. Van der Pijl et al. [138, 139], Linke [140], and Freundt and Linke [141] discussed the relevance of titin unfolding for stimulating signalling pathways with changes in the protein synthesis rate as an important contributor of the sarcomerogenesis [142]. Thus, it seems reasonable to discuss the role of mechanical tension for triggering anabolic signalling pathways as a part of morphological adaptations via stretching. Accordingly, assuming the unfolding of titin is exclusively attained by reaching long muscle lengths (consequently maximise mechanical tension via stretch), Apostolopoulos et al. [143] pointed out the high relevance of stretching intensity when aiming to induce structural changes. The stimulation of the signalling pathways leading to protein synthesis is discussed following the response matrix model by Toigo and Boutellier [144].
3.2 Response Matrix Model
Suprathreshold external stimuli (such as mechanical tension) were described to lead to a specific gene expression, which takes place by transcription and translation of specific proteins [145] causing a specific biological response that results in specific changes in the phenotype. So far, based on aforementioned results from animal experiments, a serial sarcomere accumulation due to a high mechanical stress applied to a high muscle length seems reasonable. When adding sarcomeres in series, similar to cross-sectional hypertrophy, new muscle protein must be synthesised via anabolic processes that stimulate specific protein synthesis, which can be triggered via a stretch-induced mechanical overload [120, 146,147,148]. Thus, it is hypothesised that longitudinal hypertrophy might be also initiated via mechanotransduction, which describes the translation of mechanical signals to biochemical responses [149, 150].
In line, referring to Coffey and Hawley [151], converting a mechanical signal generated during contraction to a molecular event promotes adaptations in a muscle cell that might cause a subsequent upregulation of primary and secondary messengers. These mechanotransduction mechanisms [152] compromise the translation of mechanical stimuli such as stretching via, among others, stretch-activated channels to biochemical responses via signalling pathways, which in turn adapt the muscle in length to reduce the stretching stressor [149, 153]. The addition of serial sarcomeres, thus producing additional proteins is the response to a specific muscle protein synthesis enhancement. To initiate this anabolic response, several known signalling cascades are stimulated that result in an activation and/or repression of specific signalling pathways to regulate gene expression and protein synthesis/degradation in response to training [120, 152]. Even though the exact downstream events of the anabolic signalling need further investigation [154], there seems to be a consensus that mechanical tension induced via resistance training or stretching [148] triggers specific signalling pathways. More specifically, the Akt/mTOR/p70S6K is described to play a fundamental role in muscular anabolism [113, 155,156,157]. Interestingly, several transcription factors such as insulin-like growth factor-1 [113, 158,159,160], myogenin growth factor, insulin receptor substrate 1 and protein kinase B [161] playing an important role by activating the anabolic mTOR pathway [150, 162] are activated by stretching [113, 120, 133, 136, 150, 163] as well as resistance training [155, 156, 164] (Fig. 1). Wang and Proud [165] described further anabolic events, including PIP3, PKB and Tuberous sclerosis 1 and 2 [119, 160, 165]. Assuming an increased net protein synthesis rate as important, it is notable that tension applied via stretching can cause a downregulation of anti-anabolic or catabolic mediators such as myostatin, MuRF1 or MAFbx via the insulin-like growth factor-1-induced inhibition of FOXO [112, 113, 166]. Assuming specific adaptations, it seems reasonable that sarcomerogenesis also occurs in human muscles as a response to mechanical tension induced in long muscle lengths—independent of the way this mechanical stressor is induced (full ROM resistance training, dynamic stretching, static stretching, PNF stretching). Figure 2 shows a simplified illustration of the most popular signalling pathway to induce anabolic adaptations.

Created with BioRender.com
Simplified illustration of the most popular signalling pathway to induce anabolic adaptations (illustrated with Biorender.com). FGF fibroblast growth factor, HGH human growth hormone, IGF-1 insulin-like growth factor-1, IRS-1 insulin receptor substrate 1, MGF myogenin growth factor, PKB protein kinase B.
Even though the human literature favors neuromuscular stretching adaptations, as structural adaptations were described unlikely [21, 22], it seems questionable to separate neuromuscular from structural adaptations. Considering stretching as a physiological response, warning the body of possible harm, injury or chronic pain to trigger appropriate protective responses [167, 168], increases in the functional muscle length might cause a better joint stabilisation in the end ROM, thus causing a later myotatic reflex occurrence with increases in the stretching pain threshold.
3.3 Methodological Problems Limiting the Evidence
Yet, although logical in theory, no direct evidence could be found for serial sarcomere accumulation in humans. On the one hand, this fact might be attributable to methodological concerns in data collection. On the other hand, there is a lack of studies inducing a meaningful stretch stimulus that was sufficient to induce serial sarcomere accumulation in animals.
It is speculated that serial sarcomere accumulation occurs in humans; however, it is complicated to directly determine this phenomenon. In animal studies, the effectiveness of the stretching protocol is examined by extracting a muscle sample following the euthanasia of the subject. This direct analysis, however, poses limitations as researchers are confined to post-intervention samples, making within-subject comparisons impossible. Consequently, many direct analyses resort to employing two separate groups, introducing potential challenges for generalisation [125, 169]. It seems impossible to discuss the transferability of such a study protocol to human participants. In humans, the limited data are therefore attributable to a limited possibility to directly measure the serial sarcomere number directly. While invasive methods (i.e. biopsies) might be applicable in humans, it is not possible to perform a direct pre-post testing, as the same muscle tissue cannot be removed twice. Even for those methods, data collection and probe evaluation equipment such as biopsies or microendoscopy [170, 171] would be necessary, which seems of limited accessibility.
However, indirect evidence for stretch-induced structural adaptations as well as the underlying physiological explanations is limited. While most of the discussed mechanisms were discussed in the resistance training literature, there is evidence for many similarities in stretching [5, 118, 146, 160, 163, 172]. Assuming high mechanical tension to induce structural damage with subsequent increases in protein synthesis, creatine kinase activity is commonly determined as a valid predictor [173,174,175]. Even though Smith et al. [176] indicated that static stretching (3 × 60 s of stretching with 17 exercises) was sufficient to increase creatine kinase activity compared with ballistic stretching, the clinical relevance of such low magnitude creatine kinase improvements was questioned [177]. Indeed, Fowles et al. [178] did not find a significant protein synthesis increase in response to 33 min of plantar flexor stretching. Nevertheless, stretching durations (and volumes) in animals with 24 h per day, which induced a meaningful protein synthesis increase, were not comparable to those used in humans (up to 33 min) [178], especially when considering a slower protein synthesis rate in humans [179, 180], compared with chickens and quails as well as to rats and cats [181, 182]. Indeed, small stretching volumes and durations were not sufficient to increase the muscle cross-sectional area [183], while higher volumes (up to 7 h per week) consistently showed muscle hypertrophy [146].
Nevertheless, although serial sarcomere accumulation was not measured directly in humans, there are some indications such as increased ROM [3, 9, 98,99,100,101,102], reduced pain threshold [21,22,23, 95], changes in the optimal force production angle or strength increases in long muscle lengths [184,185,186] as well as changes in fascicle lengths [187] after performing long-term stretching programmes. These adaptations, however, were not exclusively related to stretching exercises, but also to resistance training. In accordance with Alizadeh et al. [59] emphasising the role of the eccentric phase of resistance training, Gérard et al. [188] reviewed the available eccentric resistance training literature and indicated significant pennation angle decreases, while Marušič et al. [189] showed 6 weeks of an eccentric hamstrings training protocol, confirming pennation angle decreases that were accompanied by fascicle length increases, which could indirectly underline muscle length changes.
However, based on similarities in the stated physiological responses as well as outcomes, it seems reasonable that a mechanical overload applied to long muscle lengths would optimise training-induced ROM adaptations also in humans. In line, similar results using high-volume stretching and strength training [5, 59, 90, 103, 104] could possibly be explained by these shared underlying mechanisms. Although stretching intensity is stated to be of paramount importance to induce structural adaptations [143], intensity was mostly measured using subjective pain perception. To therefore optimise training studies and methods in sports practice, conducting well-designed stretching studies including objective intensity (tension) quantification as well as physiological outcomes seem imperative, while there is a limited need for further studies confirming the influence of stretching on flexibility.
3.4 Further Potential Mechanisms
Even though frequently reported to be of high importance, a mechanical overload seems not the only stimulus to induce structural muscle adaptations. Considerable structural adaptations were reported in response to blood flow restriction [190], which were potentially initiated by similar physiological pathways [191] including the mTOR signalling pathway [192], with Gundermann et al. [193] showing stimulation of mTORC1 and muscle protein synthesis immediately after blood flow restriction training. Interestingly, in the rat muscle, Hotta et al. [194] described an almost complete suppression of the blood flow to the stretched muscle. Thus, potential stimulating effects of restricted blood flow on structural adaptations cannot be ruled out, while stretch-induced changes in blood flow patterns in human muscle have not been comprehensively investigated, while no studies were found that showed an increased flexibility in response to blood flow restriction training. Furthermore, metabolic factors (accumulation of metabolites due to suppressed blood flow) might induce stress that could increase structural adaptations in general. The link to increased flexibility, however, remains uninvestigated and will therefore not be further discussed here.
4 Practical Applications in Sports Practice and Research
Referring to Alizadeh et al. [59], it is not mandatory to perform stretching, as resistance training performed over the full ROM resulted in similar adaptations. Assuming muscle tissue tends to optimise the myosin and actin overlap [128], structural adaptations can be hypothesised to be influenced by adding a contraction to the stretch. Accordingly, in animal research, Williams et al. [133] showed in cats that immobilisation of the hindlimb muscle in a stretched position increased the number of sarcomeres in series significantly, while immobilisation in a shortened position showed a significant decrease in the number of sarcomeres in series. In humans, adding electrostimulation to a stretched position causing a contraction of the muscle in high muscle lengths might be an important further stimulus [195]. Interestingly, most recently, the practical relevance was confirmed by Mizuno [40] showing superior effects regarding ROM, passive torque adaptations and tendon displacement by adding electrostimulation to static stretching in the calf muscles.
Thus, assuming greater degrees of mechanical tension with long muscle lengths to be one important underlying mechanism to induce structural muscle adaptations, applying an active contraction in stretched muscle positions can be hypothesised to enhance the stress stimulus (muscle contraction with a minimal actin-myosin overlap). Therefore, when aiming to increase active ROM, there might be different ways to induce high degrees of mechanical tension to greater muscle lengths. Considering full ROM resistance training as a type of loaded dynamic stretching would be one way to include active movements over the available muscle lengths. However, assuming the time under tension to be important as well [196], the exclusive focus on high-intensity (thus low volume or duration) resistance training could be reasonably supplemented by high-volume stretch training. Nevertheless, stretching is still of high relevance to enhance ROM long term. Full ROM resistance training such as deep squats are multi-joint exercises that might compensate, for example, limited angle joint flexibility by flexing the hip joint and bending the upper body, thus avoiding the weakness without improving ankle ROM. Furthermore, improving adductor flexibility might be difficult when using complex multi-joint movements. Therefore, based on the outlined literature, it can be recommended to use isolated stretching exercises to improve individual joint ROM, while full ROM resistance training could be considered a more economical method to induce high degrees of mechanical tension in longer muscle lengths, thus improving full-body active flexibility long term comparable to stretching [59, 90].
In contrast, when aiming to acutely enhance flexibility, there is no evidence to emphasise specific interventions, as no significant differences in interventions can be assumed. As warm-up routines should avoid fatigue and should be limited to essential movement preparation, in contrast to the common literature, the inclusion of stretching or foam rolling might be considered a waste of time, as almost every concurrent intervention (jogging, cycling) would induce similar ROM increases, however, by performing active and more sports-related movements, in a best case by using full ROM [61, 64, 65].
When conducting research designs, but also for training interventions in sports practice, it seems more appropriate to focus on physiological aspects. Therefore, training can be seen as an external stressor, resulting in specific physiological adaptations to cause structural and functional changes of the system. To reasonably perform training interventions, in the first step, it seems valuable to be clear about the underlying system and the type of the stimulus to cause a suprathreshold stimulus (mechanical stress on the muscle cell in high muscle lengths). Afterwards, considering the available training methods, the practitioner has to choose the methods, inducing the highest amount of stress to the targeted system.
5 Conclusions
In this review, we discussed explanatory approaches for acute and chronic flexibility increases, which contrast with common theories. Several limitations in the research design of the currently available research do not allow the conclusion of specific acute stretching results, as several interventions showed comparable ROM effects. Additionally, for long-term effects, ROM can be enhanced by several other interventions than stretching, which induce mechanical tension to longer muscle lengths, which does not mean that this stimulus is the only mechanism. Nevertheless, the favored approach is the role of mechanical tension, which might induce several adaptations, such as stretch-induced sarcomerogenesis, as an increased muscle length would also delay the occurrence of stretching pain and reduced stiffness as frequently reported accompanying effects.
References
Gleim GW, McHugh MP. Flexibility and its effects on sports injury and performance. Sports Med. 1997;24:289–99.
Behm DG. The science and physiology of flexibility and stretching: implications and applications in sport performance and health. London: Routledge Publisher; 2018.
Medeiros DM, Martini TF. Chronic effect of different types of stretching on ankle dorsiflexion range of motion: systematic review and meta-analysis. Foot (Edinb). 2018;34:28–35.
Opplert J, Babault N. Acute effects of dynamic stretching on muscle flexibility and performance: an analysis of the current literature. Sports Med. 2018;48:299–225.
Morton SK, Whitehead JR, Brinkert RH, Caine DJ. Resistance training vs. static stretching: effects on flexibility and strength. J Strength Cond Res. 2011;25:3391–8.
Su H, Chang N-J, Wu W-L, Guo L-Y, Chu I-H. Acute effects of foam rolling, static stretching, and dynamic stretching during warm-ups on muscular flexibility and strength in young adults. J Sport Rehabil. 2017;26:469–77.
Hill KJ, Robinson KP, Cuchna JW, Hoch MC. Immediate effects of proprioceptive neuromuscular facilitation stretching programs compared with passive stretching programs for hamstring flexibility: a critically appraised topic. J Sport Rehabil. 2017;26:567–72.
Cayco CS, Labro AV, Gorgon E. Hold-relax and contract-relax stretching for hamstrings flexibility: a systematic review with meta-analysis. Phys Ther Sport. 2019;35:3542–55.
Medeiros DM, Cini A, Sbruzzi G, Lima CS. Influence of static stretching on hamstring flexibility in healthy young adults: systematic review and meta analysis. Physio Ther Theory Pract. 2016;32:438–45.
Bouguezzi R, Sammoud S, Markov A, Negra Y, Chaabene H. Why flexibility deserves to be further considered as a standard component of physical fitness: a narrative review of existing insights from static stretching study interventions. Youth. 2023;3:146–56.
Wiewelhove T, Döweling A, Schneider C, Hottenrott L, Meyer T, Kellmann M, Pfeiffer M, Ferrauti A. A meta-analysis of the effects of foam rolling on performance and recovery. Front Physiol. 2019;10:376. https://doi.org/10.3389/fphys.2019.00376.
Konrad A, Nakamura M, Tilp M, Donti O, Behm DG. Foam rolling training effects on range of motion: a systematic review and meta-analysis. Sports Med. 2022;52:2523–35.
Konrad A, Nakamura M, Paternoster FK, Tilp M, Behm DG. A comparison of a single bout of stretching or foam rolling on range of motion in healthy adults. Eur J Appl Physiol. 2022;122:1545–57.
Park S-J, Lee S-I, Jeong H-J, Kim B-G. Effect of vibration foam rolling on the range of motion in healthy adults: a systematic review and meta-analysis. J Exerc Rehabil. 2021;17:226–33.
Konrad A, Tilp M, Nakamura M. A comparison of the effects of foam rolling and stretching on physical performance. A systematic review and meta-analysis. Front Physiol. 2021;12:720531. https://doi.org/10.3389/fphys.2021.720531.
Konrad A, Nakamura M, Behm DG. The effects of foam rolling training on performance parameters: a systematic review and meta-analysis including controlled and randomized controlled trials. Int J Environ Res Public Health. 2022;19:11638.
Wilke J, Müller A-L, Giesche F, Power G, Ahmedi H, Behm DG. Acute effects of foam rolling on range of motion in healthy adults: a systematic review with multilevel meta-analysis. Sports Med. 2020;50:387–402.
Davis HL, Alabed S, Chico TJA. Effect of sports massage on performance and recovery: a systematic review and meta-analysis. BMJ Open Sport Exerc Med. 2020;6: e000614.
Behm DG, Blazevich AJ, Kay AD, McHugh M. Acute effects of muscle stretching on physical performance, range of motion, and injury incidence in healthy active individuals: a systematic review. Appl Physiol Nutr Metabol. 2016;41:1–11.
Behm DG, Kay AD, Trajano GS, Alizadeh S, Blazevich AJ. Effects of acute and chronic stretching on pain control. J Clin Exerc Physiol. 2021;10:150–9.
Freitas SR, Mendes B, Le Sant G, Andrade RJ, Nordez A, Milanovic Z. Can chronic stretching change the muscle-tendon mechanical properties? A review. Scand J Med Sci Sports. 2018;28:294–306.
Konrad A, Tilp M. Increased range of motion after static stretching is not due to changes in muscle and tendon structures. Clin Biomech. 2014;29:636–42.
Konrad A, Tilp M. Effects of ballistic stretching training on the properties of human muscle and tendon structures. J Appl Physiol. 2014;117:29–35.
Konrad A, Tilp M. Time course of muscle-tendon unit function and structure following three minutes of static stretching. J Sports Sci Med. 2020;19:52–8.
Konrad A, Gad M, Tilp M. Effect of PNF stretching training on the properties of human muscle and tendon structures. Scand J Med Sci Sports. 2015;25:346–55.
Behm DG, Chaouachi A. A review of the acute effects of static and dynamic stretching on performance. Eur J Appl Physiol. 2011;111:2633–51.
Opplert J, Babault N. Effects of dynamic stretching on mechanical properties result from both muscle-tendon stretching and muscle warm-up. J Sports Sci Med. 2019;18:351–8.
Thomas E, Bianco A, Paoli A, Palma A. The relation between stretching typology and stretching duration: the effects on range of motion. Int J Sports Med. 2018;39:243–54.
Anderson BL, Harter RA, Farnsworth JL. The acute effects of foam rolling and dynamic stretching on athletic performance: a critically appraised topic. J Sport Rehabil. 2021;30:501–6.
Cai P, Liu L, Li H. Dynamic and static stretching on hamstring flexibility and stiffness: a systematic review and meta-analysis. Heliyon. 2023;9: e18795.
Behm DG, Alizadeh S, Daneshjoo A, Anvar SH, Graham A, Zahiri A, Goudini R, Edwards C, Culleton R, Scharf C, Konrad A. Acute effects of various stretching techniques on range of motion: a systematic review with meta-analysis. Sports Med Open. 2023;9(1):107. https://doi.org/10.1186/s40798-023-00652-x.
Reiner MM, Gabriel A, Tilp M, Konrad A. The acute effects of pectoralis major foam ball rolling on shoulder extension range of motion, isometric contraction torque, and muscle stiffness. J Sports Sci Med. 2023;22(1):51–7. https://doi.org/10.52082/jssm.2023.51.
Takeuchi K, Nakamura M, Fukaya T, Konrad A, Mizuno T. Acute and long-term effects of static stretching on muscle-tendon unit stiffness: a systematic review and meta-analysis. J Sports Sci Med. 2023;22(3):465–75. https://doi.org/10.52082/jssm.2023.465.
Kay AD, Blazevich AJ. Moderate-duration static stretch reduces active and passive plantar flexor moment but not Achilles tendon stiffness or active muscle length. J Appl Physiol. 2009;106:1249–56.
Kay AD, Husbands-Beasley J, Blazevich AJ. Effects of contract-relax, static stretching, and isometric contractions on muscle-tendon mechanics. Med Sci Sports Exerc. 2015;47:2181–90.
Konrad A, Budini F, Tilp M. Acute effects of constant torque and constant angle stretching on the muscle and tendon tissue properties. Eur J Appl Physiol. 2017;117:1649–56.
Konrad A, Reimer MM, Thaller S, Tilp M. The time course of muscle-tendon properties and function responses of a five-minute static stretching exercise. Eur J Sport Sci. 2019;19:1195–203.
Kato E, Vieillevoye S, Balestra C, Guissard N, Duchateau J. Acute effect of muscle stretching on the steadiness of sustained submaximal contractions of the plantar flexor muscles. J Appl Physiol. 2011;110:407–15.
Kubo K, Kanehisa H, Kawakami Y, Fukunaga T. Influence of static stretching on viscoelastic properties of human tendon structures in vivo. J Appl Physiol. 2001;90:520–7.
Mizuno T. Combined static stretching and electrical muscle stimulation induce greater changes in range of motion, passive torque, and tendon displacement compared with static stretching. Sports. 2023;11:10.
Gesel FJ, Morenz EK, Cleary CJ, LaRoche DP. Acute effects of static and ballistic stretching on muscle-tendon unit stiffness, work absorption, strength, power, and vertical jump performance. J Strength Cond Res. 2022;36:2147–55.
Smith CA. The warm-up procedure: to stretch or not to stretch. A brief review. J Orthopaed Sports Phys Ther. 1994;19:12–7.
Behm DG, Kay AD, Trajano GS, Blazevich AJ. Mechanisms underlying performance impairments following prolonged static stretching without a comprehensive warm-up. Eur J Appl Physiol. 2021;121:67–94.
Simic L, Sarabon N, Markovic G. Does pre-exercise static stretching inhibit maximal muscular performance? A meta-analytical review. Scand J Med Sci Sports. 2013;23:131–48.
Kay AD, Blazevich AJ. Effect of acute static stretch on maximal muscle performance: a systematic review. Med Sci Sports Exerc. 2012;44:154–64.
Reid JC, Greene R, Young JD, Hodgson DD, Blazevich AJ, Behm DG. The effects of different durations of static stretching within a comprehensive warm-up on voluntary and evoked contractile properties. Eur J Appl Physiol. 2018;118:1427–45.
Behm DG, Wilke J. Do self-myofascial release devices release myofascia? Rolling mechanisms: a narrative review. Sports Med. 2019;49:1173–81.
Behm DG, Alizadeh S, Hadjizadeh Anvar S, Mahmoud MMI, Ramsay E, Hanlon C, et al. Foam rolling prescription: a clinical commentary. J Strength Cond Res. 2020;34:3301–8.
Mohr AR, Long BC, Goad CL. Effect of foam rolling and static stretching on passive hip-flexion range of motion. J Sport Rehabil. 2014;23:296–9.
Schroeder AN, Best TM. Is self myofascial release an effective preexercise and recovery strategy? A literature review. Curr Sports Med Rep. 2015;14:200–8.
Reiner MM, Glashüttner C, Bernsteiner D, Tilp M, Guilhem G, Morales-Artacho A, et al. A comparison of foam rolling and vibration foam rolling on the quadriceps muscle function and mechanical properties. Eur J Appl Physiol. 2021;121:1461–71.
Reiner MM, Tilp M, Guilhem G, Morales-Artacho A, Konrad A. Comparison of a single vibration foam rolling and static stretching exercise on the muscle function and mechanical properties of the hamstring muscles. J Sports Sci Med. 2022;21(2):287–97. https://doi.org/10.52082/jssm.2022.287.
Baumgart C, Freiwald J, Kühnemann M, Hotfiel T, Hüttel M, Hoppe M. Foam rolling of the calf and anterior thigh: biomechanical loads and acute effects on vertical jump height and muscle stiffness. Sports. 2019;7:27.
Krause F, Wilke J, Niederer D, Vogt L, Banzer W. Acute effects of foam rolling on passive stiffness, stretch sensation and fascial sliding: a randomized controlled trial. Hum Mov Sci. 2019;67: 102514.
Nakamura M, Onuma R, Kiyono R, Yasaka K, Sato S, Yahata K, Fukaya T, Konrad A. The acute and prolonged effects of different durations of foam rolling on range of motion, muscle stiffness, and muscle strength. J Sports Sci Med. 2021;20(1):62–8. https://doi.org/10.52082/jssm.2021.62.
Ryan E, Beck TW, Herda TJ, Hull HR, Hartman MJ, Stout JR, et al. Do practical durations of stretching alter muscle strength? A dose-response study. Med Sci Sports Exerc. 2008;40:1529–37.
Cramer JT, Housh TJ, Coburn JW, Beck TW, Johnson GO. Acute effects of static stretching on maximal eccentric torque production in women. J Strength Cond Res. 2006;20:354.
Hendricks S, Hill H, den Hollander S, Lombard W, Parker R. Effects of foam rolling on performance and recovery: a systematic review of the literature to guide practitioners on the use of foam rolling. J Bodyw Mov Ther. 2020;24:151–74.
Alizadeh S, Daneshjoo A, Zahiri A, Anvar SH, Goudini R, Hicks JP, et al. Resistance training induces improvements in range of motion: a systematic review and meta-analysis. Sports Med. 2023;53:707–22.
Warneke K, Wohlann T, Lohmann LH, Schiemann S. Acute effects of long-lasting stretching and strength training on maximal strength and flexibility in the calf muscle. Ger J Exerc Sport Res. 2023;53:148–54. https://doi.org/10.1007/s12662-022-00854-7.
Murakami Y, Konrad A, Kasahara K, Yoshida R, Warneke K, Behm DG, et al. Acute effects of resistance training at different range of motions on plantar flexion mechanical properties and force. J Sports Sci. 2024;42(1):38–45.
de Oliveira LF, Cabral HV, Leitão BFM, Matta TT. Both the resistance training session and the static stretching after exercise does not affect the pectoralis major stiffness of well-trained men. J Bodyw Mov Ther. 2020;24:321–4.
Krzysztofik M, Wilk M, Pisz A, Kolinger D, Tsoukos A, Zajac A, et al. Acute effects of varied back squat activation protocols on muscle-tendon stiffness and jumping performance. J Strength Cond Res. 2023;37:1486–94.
Kawama R, Hojo T, Wakahara T. Acute changes in passive stiffness of the individual hamstring muscles induced by resistance exercise: effects of muscle length and exercise duration. Eur J Appl Physiol. 2022;123:655–66.
Kawama R, Yanase K, Hojo T, Wakahara T. Acute changes in passive stiffness of the individual hamstring muscles induced by resistance exercise: effects of contraction mode and range of motion. Eur J Appl Physiol. 2022;122:2071–83.
de Ridder R, De Blaiser C, Verrelst R, De Saer R, Desmet A, Schuermans J. Neurodynamic sliders promote flexibility in tight hamstring syndrome. Eur J Sport Sci. 2020;20:973–80.
Castellote-Caballero Y, Valenza MC, Puentedura EJ, Fernández-de-las-Peñas C, Alburquerque-Sendín F. Immediate effects of neurodynamic sliding versus muscle stretching on hamstring flexibility in subjects with short hamstring syndrome. Sports Med. 2014;2014:1–8.
Alshammari F, Alzoghbieh E, Abu Kabar M, Hawamdeh M. A novel approach to improve hamstring flexibility: a single-blinded randomised clinical trial. S Afr J Physiother. 2019;75:465.
Konrad A, Močnik R, Nakamura M. Effects of tissue flossing on the healthy and impaired musculoskeletal system: a scoping review. Front Physiol. 2021;12: 666129.
Konrad A, Glashüttner C, Reiner MM, Bernsteiner D, Tilp M. The acute effects of a precussive massage treatment with a hypervolt device on plantar flexor muscles range of motuion and performance. J Sports Sci Med. 2020;19:690–4.
Padua E, D’Amico AG, Alashram A, Campoli F, Romagnoli C, Lombardo M, et al. Effectiveness of warm-up routine on the ankle injuries prevention in young female basketball players: a randomized controlled trial. Medicina (B Aires). 2019;55:690.
Roberts HM, Law R-J, Thom JM. The time course and mechanisms of change in biomarkers of joint metabolism in response to acute exercise and chronic training in physiologic and pathological conditions. Eur J Appl Physiol. 2019;119:2401–20.
Woods K, Bishop P, Jones E. Warm-up and stretching in the prevention of muscular injury. Sports Med. 2007;37:1089–99.
Reid E. Warm-up and athletic performance: a physiological analysis. Natl Strength Cond Assoc J. 1986;8:30–3.
Miyahara Y, Naito H, Ogura Y, Katamoto S, Aoki J. Effects of proprioceptive neuromuscular facilitation stretching and static stretching on maximal voluntary contraction. J Strength Cond Res. 2013;27:195–201.
de Oliveira UF, de Araújo LC, de Andrade PR, dos Santos HH, Moreira DG, Sillero-Quintana M, et al. Skin temperature changes during muscular static stretching exercise. J Exerc Rehabil. 2018;14:451–9.
O’Sullivan K, Murray E, Sainsbury D. The effect of warm-up, static stretching and dynamic stretching on hamstring flexibility in previously injured subjects. BMC Musculoskelet Disord. 2009;10:1–9.
Morales-Artacho AJ, Lacourpaille L, Guilhem G. Effects of warm-up on hamstring muscles stiffness: cycling vs foam rolling. Scand J Med Sci Sports. 2017;27:1959–69.
Takeuchi K, Takemura M, Nakamura M, Tsukuda F, Miyakawa S. Effects of active and passive warm-ups on range of motion, strength, and muscle passive properties in ankle plantarflexor muscles. J Strength Cond Res. 2021;35:141–6.
Oranchuk DJ, Flattery MR, Robinson TL. Superficial heat administration and foam rolling increase hamstring flexibility acutely; with amplifying effects. Phys Ther Sport. 2019;40:213–7.
De Nardi M, La Torre A, Benis R, Sarabon N, Fonda B. Acute effects of whole-body cryotherapy on sit-and-reach amplitude in women and men. Cryobiology. 2015;71:511–3.
Warneke K, Plöschberger G, Lohmann LH, Lichtenstein E, Jochum D, Siegel SD, Zech A, Behm DG. Foam rolling and stretching do not provide superior acute flexibility and stiffness improvements compared to any other warm-up intervention: a systematic review with meta-analysis. J Sport Health Sci. 2024:S2095-2546(24)00006-1. https://doi.org/10.1016/j.jshs.2024.01.006.
Kerautret Y, Guillot A, Eyssautier C, Gibert G, Di Rienzo F. Effects of self-myofascial release interventions with or without sliding pressures on skin temperature, range of motion and perceived well-being: a randomized control pilot trial. BMC Sports Sci Med Rehabil. 2021;13:43.
Behm DG, Alizadeh S, Drury B, Granacher U, Moran J. Non-local acute stretching effects on strength performance in healthy young adults. Eur J Appl Physiol. 2021;121:1517–29.
Nakamura M, Konrad A, Kiyono R, Sato S, Yahata K, Yoshida R, et al. Local and non-local effects of foam rolling on passive soft tissue properties and spinal excitability. Front Physiol. 2021;12: 702042.
Konrad A, Nakamura M, Warneke K, Donti O, Gabriel A. The contralateral effects of foam rolling on range of motion and muscle performance. Eur J Appl Physiol. 2023;123:1167–78.
Killen BS, Zelizney KL, Ye X. Crossover effects of unilateral static stretching and foam rolling on contralateral hamstring flexibility and strength. J Sport Rehabil. 2019;28:533–9.
Wilke J, Krause F, Vogt L, Banzer W. What is evidence-based about myofascial chains: a systematic review. Arch Phys Med Rehabil. 2016;97:454–61.
Konrad A, Alizadeh S, Daneshjoo A, Hadjizadeh AS, Graham S, Zahiri A, et al. Chronic effects of stretching on range of motion with consideration of potential moderating variables: a systematic review with meta-analysis. J Sport Health Sci. 2023;13:186–94.
Afonso J, Ramirez-Campillo R, Moscão J, Rocha T, Zacca R, Martins A, et al. Strength training versus stretching for improving range of motion: a systematic review and meta-analysis. Healthcare. 2021;9:427.
Pagaduan JC, Chang S-Y, Chang N-J. Chronic effects of foam rolling on flexibility and performance: a systematic review of randomized controlled trials. Int J Environ Res Public Health. 2022;19:4315.
Grieve R, Byrne B, Clements C, Davies L-J, Durrant E, Kitchen O. The effects of foam rolling on ankle dorsiflexion range of motion in healthy adults: a systematic literature review. J Bodyw Mov Ther. 2022;30:53–9.
Mahieu NN, McNair P, De Muynck M, Stevens V, Blanckaert I, Smits N, et al. Effect of static and ballistic stretching on the muscle-tendon tissue properties. Med Sci Sports Exerc. 2007;39:494–501.
Nakamura M, Yahata K, Sato S, Kiyono R, Yoshida R, Fukaya T, et al. Training and detraining effects following a static stretching program on medial gastrocnemius passive properties. Front Physiol. 2021;12: 656579.
Freitas SR, Mil-Homens P. Effect of 8-week high-intensity stretching training on biceps femoris architecture. J Strength Cond Res. 2015;29:1737–40.
Kasahara K, Konrad A, Yoshida R, Murakami Y, Sato S, Aizawa K, et al. Comparison between 6-week foam rolling intervention program with and without vibration on rolling and non-rolling sides. Eur J Appl Physiol. 2022;122:2061–70.
Kiyono R, Onuma R, Yasaka K, Sato S, Yahata K, Nakamura M. Effects of 5-week foam rolling intervention on range of motion and muscle stiffness. J Strength Cond Res. 2022;36:1890–5.
Young R, Nix S, Wholohan A, Bradhurst R, Reed L. Interventions for increasing ankle joint dorsiflexion: a systematic review and meta-analysis. J Foot Ankle Res. 2013;6:1–10.
Lempke L, Wilkinson R, Murray C, Stanek J. The effectivness of PNF versus static stretching on increasing hip flexion range of motion. J Sport Rehabil. 2018;27:289–94.
Donti O, Konrad A, Panidi I, Dinas PC, Bogdanis GC. Is there a “window of opportunity” for flexibility development in youth? A systematic review with meta-analysis. Sports Med. 2022;8:1–24.
Kongkaew C, Lertsinthai P, Jampachaisri K, Mongkhon P, Meesomperm P, Kornkaew K, et al. The effects of Thai yoga on physical fitness: a meta-analysis of randomized control trials. J Altern Complement Med. 2018;24:541–51.
Radford JA, Burns J, Buchbinder R, Landorf KB, Cook C. Does stretching increase ankle dorsiflexion range of motion? A systematic review. Br J Sports Med. 2006;40:870–5.
Warneke K, Wirth K, Keiner M, Lohmann LH, Hillebrecht M, Brinkmann A, et al. Comparison of the effects of long-lasting static stretching and hypertrophy training on maximal strength, muscle thickness and flexibility in the plantar flexors. Eur J Appl Physiol. 2023;123:1773–87.
Arntz F, Markov A, Behm DG, Behrens M, Negra Y, Nakamura M, et al. Chronic effects of static stretching exercises on muscle strength and power in healthy individuals across the lifespan: a systematic review with multi-level meta-analysis. Sports Med. 2023;53:723–45.
Kassiano W, Costa B, Kunevaliki G, Soares D, Zacarias G, Manske I, et al. Greater gastrocnemius muscle hypertrophy after partial range of motion training carried out at long muscle lengths. J Strength Cond Res. 2023;37(9):1746–53.
Potier TG, Alexander CM, Seynnes OR. Effects of eccentric strength training on biceps femoris muscle architecture and knee joint range of movement. Eur J Appl Physiol. 2009;105:939–44.
Reeves ND, Maganaris CN, Longo S, Narici MV. Differential adaptations to eccentric versus conventional resistance training in older humans. Exp Physiol. 2009;94:825–33.
Blazevich AJ, Cannavan D, Coleman DR, Horne S. Influence of concentric and eccentric resistance training on architectural adaptation in human quadriceps muscles. J Appl Physiol. 2007;103:1565–75.
Franchi MV, Reeves ND, Narici MV. Skeletal muscle remodeling in response to eccentric vs. concentric loading: morphological, molecular, and metabolic adaptations. Front Physiol. 2017;8:447.
Wisdom KW, Delp SL, Kuhl E. Use it or lose it: multiscale skeletal muscle adaptation to mechanical stimuli. Biomech Model Mechanobiol. 2015;14:195–215.
Goldspink G. Gene expression in muscle in response to exercise. J Muscle Res Cell Motil. 2003;24:121–6.
Goldspink G, Harridge S. Cellular and molecular aspects of adaptation in skeletal muscle. In: Komi PV, editor. Strength and power in sport. 2nd ed. 2003: p. 231–51.
Goldspink G. Changes in muscle mass and phenotype and the expression of autocrine and systemic growth factors by muscle in response to stretch and overload. J Anat. 1999;194:323–34.
Caiozzo VJ, Utkan A, Chou R, Khalafi A, Chandra H, Baker M, et al. Effects of distraction on muscle length: mechanisms involved in sarcomerogenesis. Clin Orthop Relat Res. 2002;403:S133–45.
Czerwinski SM, Martin JM, Bechtel PJ. Modulation of IGF mRNA abundance during stretch-induced skeletal muscle hypertrophy and regression. J Appl Physiol. 1994;76:2026–30.
Laurent GJ, Sparrow MP. Changes in RNA, DNA and protein content and the rates of protein synthesis and degradation during hypertrophy of the anterior latissimus dorsi muscle of the adult fowl (Gallus domesticus). Growth. 1977;41:249–62.
Antonio J, Gonyea WJ. Progressive stretch overload of skeletal muscle results in hypertrophy before hyperplasia. J Appl Physiol. 1993;75:1263–71.
Tatsumi R. Mechano-biology of skeletal muscle hypertrophy and regeneration: possible mechanism of stretch-induced activation of resident myogenic stem cells. Anim Sci. 2010;81:11–20.
Miyagoe-Suzuki Y, Takeda S. Mechanobiology in skeletal muscle: conversion of mechanical information into molecular signal. In: Noda M, editor. Mechanosensing biology. Tokyo: Springer; 2011. https://doi.org/10.1007/978-4-431-89757-6_4.
Wackerhage H, Schoenfeld BJ, Hamilton DL, Lehti M, Hulmi JJ. Stimuli and sensors that initiate muscle hypertrophy following resistance exercise. J Appl Physiol. 2019;126:30–43.
De Jaeger D, Joumaa V, Herzog W. Intermittent stretch training of rabbit plantarflexor muscles increases soleus mass and serial sarcomere number. J Appl Physiol. 2015;118:1467–73.
Williams PE. Use of intermittent stretch in the prevention of serial sarcomere loss in immobilised muscle. Ann Rheum Dis. 1990;49:316–7.
Williams PE, Goldspink G. Changes in sarcomere length and physiological properties in immobilized muscle. J Anat. 1978;127:459–68.
Devol DL, Novakofski J, Fernando R, Bechtel PJ. Varying amounts of stretch stimulus regulate stretch-induced muscle hypertrophy in the chicken. Biochem Physiol. 1991;100A:55–61.
Warneke K, Freund PA, Schiemann S. Long-lasting stretching induces muscle hypertrophy: a meta-analysis of animal studies. J. Sci. Sport Exerc. 2023;5:289–301. https://doi.org/10.1007/s42978-022-00191-z.
Lindsey CA, Makarov MR, Shoemaker S, Birch JG, Buschang PH, Cherkashin AM, et al. The effect of the amount of limb lengthening on skeletal muscle. Clin Orthop Relat Res. 2002;402:278–87.
Peixinho CC, Martins NSF, de Oliveira LF, Machado JC. Structural adaptations of rat lateral gastrocnemius muscle–tendon complex to a chronic stretching program and their quantification based on ultrasound biomicroscopy and optical microscopic images. Clin Biomech. 2014;29:57–62.
Herring SW, Grimm AF, Grimm BR. Regulation of sarcomere number in skeletal muscle: a comparison of hypotheses. Muscle Nerve. 1984;7:161–73.
Zöllner AM, Abilez OJ, Böl M, Kuhl E. Stretching skeletal muscle: chronic muscle lengthening through sarcomerogenesis. PLoS ONE. 2012;7: e45661.
Hinks A, Franchi MV, Power GA. The influence of longitudinal muscle fascicle growth on mechanical function. J Appl Physiol. 2022;133:87–103.
Boakes JL, Foran J, Ward SR, Lieber RL. Muscle adaptation by serial sarcomere addition 1 year after femoral lengthening. Clin Orthop Relat Res. 2007;456:250–3.
Lynn R, Morgan DL. Decline running produces more sarcomeres in rat vastus intermedius muscle fibers than does incline running. J Appl Physiol. 1994;77:1439–44.
Williams PE, Catanese T, Lucey EG, Goldspink G. The importance of stretch and contractile activity in the prevention of connective tissue accumulation in muscle. J Anat. 1988;158:109–14.
Csapo R, Maganaris CN, Seynnes OR, Narici MV. On muscle, tendon and high heels. J Exp Biol. 2010;213:2582–8.
Tabary JC, Tabary C, Tardieu C, Tardieu G, Goldspink G. Physiological and structural changes in the cat’s soleus muscle due to immobilization at different length by plaster casts. J Physiol. 1972;244:231–44.
Goldspink G, Williams P, Simpson H. Gene expression in response to muscle stretch. Clin Orthop Relat Res. 2002;403(Suppl.):S146-52.
Williams P, Bicik V, Goldspink G. Effect of stretch combined with electrical stimulation on the type of sarcomeres produced at the ends of muscle fibre. Exp Neurol. 1986;93:500–9.
van der Pijl R, Strom J, Conijn S, Lindqvist J, Labeit S, Granzier H, et al. Titin-based mechanosensing modulates muscle hypertrophy. J Cachexia Sarcopenia Muscle. 2018;9:947–61.
van der Pijl RJ, Hudson B, Granzier-Nakajima T, Li F, Knottnerus AM, Smith J, et al. Deleting Titin’s C-terminal PEVK exons increases passive stiffness, alters splicing, and induces cross-sectional and longitudinal hypertrophy in skeletal muscle. Front Physiol. 2020;11:494.
Linke WA. Stretching the story of titin and muscle function. J Biomech. 2023;152: 111553.
Freundt JK, Linke WA. Titin as a force-generating muscle protein under regulatory control. J Appl Physiol. 2019;126:1474–82.
Peviani SM, Guzzoni V, Pinheiro-Dardis CM, da Silva YP, Fioravante ACR, Sagawa AH, et al. Regulation of extracellular matrix elements and sarcomerogenesis in response to different periods of passive stretching in the soleus muscle of rats. Sci Rep. 2018;8:9010.
Apostolopoulos N, Metsios GS, Flouris AD, Koutedakis Y, Wyon MA. The relevance of stretch intensity and position: a systematic review. Front Psychol. 2015;6:1–25.
Toigo M, Boutellier U. New fundamental resistance exercise determinants of molecular and cellular muscle adaptations. Eur J Appl Physiol. 2006;97:643–63.
Sadava D, Hillis D, Heller HC, Hacker S. Purves biologie. 10th ed. Markl J, editor. Berlin: Springer; 2019.
Warneke K, Lohmann LH, Lima CD, Hollander K, Konrad A, Zech A, et al. Physiology of stretch-mediated hypertrophy and strength increases: a narrative review. Sports Med. 2023;53:2055–75.
Wackerhage H, Woods NM. Exercise-induced signal transduction and gene regulation in skeletal muscle. J Sports Sci Med. 2002;1:103–14.
Kraemer WJ, Ratamess NA. Hormonal responses and adaptations to resistance exercise and training. Sports Med. 2005;35:339–61.
Mirzoev TM. Mechanotransduction for muscle protein synthesis via mechanically activated ion channels. Life. 2023;13:341.
Kremer B. Dehnungsinterventionen im Spannungsfeld historischer Entwicklung, ritualisierter Anwendung, Meisterlehre und Wissenschaft; Eine Bestandsanalyse. Karlsruher Sportwissenschaftliche Beiträge. 2017;188–92.
Coffey VG, Hawley JA. The molecular bases of training adaptation. Sports Med. 2007;37:737–63.
Burkholder TJ. Mechanotransduction in skeletal muscle. Front Biosci. 2007;12:174.
Richardson J, Kotevski A, Poole K. From stretch to deflection: the importance of context in the activation of mammalian, mechanically activated ion channels. FEBS J. 2022;289:4447–69.
Lieber RL, Fridén J. Functional and clinical significance of skeletal muscle architecture. Muscle Nerve. 2000;23:1647–66.
Bodine SC, Stitt TN, Gonzalez M, Kline WO, Stover GL, Bauerlein R, et al. Akt/mTOR Pathway is a crucial regulator of skeletal muscle hypertrophy and can prevent muscle atrophy in vivo. Nat Cell Biol. 2001;3:1014–9.
Uemichi K, Shirai T, Hanakita H, Takemasa T. Effect of mechanistic/mammalian target of rapamycin complex 1 on mitochondrial dynamics during skeletal muscle hypertrophy. Physiol Rep. 2021;9:1–14.
Wang Y, Ikeda S, Ikoma K. Passive repetitive stretching is associated with greater muscle mass and cross-sectional area in the sarcopenic muscle. Sci Rep. 2021;11:15302.
McKoy G, Ashley W, Mander J, Yang SY, Williams N, Russel B, et al. Expression of insulin growth factor-1 splice variants and structural genes in rabbit skeletal muscle induced by stretch and stimulation. J Physiol. 1999;516:583–92.
Lynch GS, Schertzer JD, Ryall JG. Anabolic agents for improving muscle regeneration and function after injury. Clin Exp Pharmacol Physiol. 2008;35:852–8.
Sasai N, Agata N, Inoue-Miyazu M, Kawakami K, Kobayashi K, Sokabe M, et al. Involvement of PI3K/Akt/TOR pathway in stretch-induced hypertrophy of myotubes. Muscle Nerve. 2010;41:100–6.
Tidall JG. Mechanical signal transduction in skeletal muscle growth and adaptation. J Appl Physiol. 2005;98:1900–8.
Hartmann U, Platen P, Niessen M, Mank D, Marzin T, Bartmus U, et al. Krafttraining im nachwuchsleistungssport unter besonderer berücksichtigung von ontogenese, biologischen mechanismen und terminologie. BISp. 2010.
Schoenfeld BJ, Wackerhage H, De Souza E. Inter-set stretch: a potential time-efficient strategy for enhancing skeletal muscle adaptations. Front Sports Act Liv. 2022;4:1035190.
Wang Y, Ikeda S, Ikoma K. Efficacy of passive repetitive stretching of skeletal muscle on myofiber hypertrophy and genetic suppression on MAFbx, MuRF1, and myostatin. J Muscle Res Cell Motil. 2021;42:443–51. https://doi.org/10.1007/s10974-021-09609-7.
Wang X, Proud CG. Methods for studying signal-dependent regulation of translation factor activity. Methods Enzymol. 2007;431:113–42.
Glass DJ. Signaling pathways perturbing muscle mass. Curr Opin Clin Nutr Metab Care. 2010;13:225–9.
Julius D, Basbaum AI. Molecular mechanisms of nociception. Nature. 2001;413:203–10.
Sirianni J, Ibrahim M, Patwardhan A. Chronic pain syndromes, mechanisms, and current treatments. Prog Mol Biol Transl Sci. 2015;131:565–611. https://doi.org/10.1016/bs.pmbts.2015.01.004.
Kelley G. Mechanical overload and skeletal muscle fiber hyperplasia: a meta-analysis. J Appl Physiol. 1996;81:1584–8.
Lichtwark GA, Farris DJ, Chen X, Hodges PW, Delp SL. Microendoscopy reveals positive correlation in multiscale length changes and variable sarcomere lengths across different regions of human muscle. J Appl Physiol. 2018;125:1812–20.
Chen X, Sanchez GN, Schnitzer MJ, Delp SL. Changes in sarcomere lengths of the human vastus lateralis muscle with knee flexion measured using in vivo microendoscopy. J Biomech. 2016;49:2989–94.
Lin SS, Liu YW. Mechanical stretch induces mTOR recruitment and activation at the phosphatidic acid-enriched macropinosome in muscle cell. Front Cell Dev Biol. 2019;7:78.
Kuipers H. Exercise-induced muscle damage. Int J Sports Med. 1994;15:132–5.
Ebbeling CB, Clarkson PM. Exercise-induced muscle damage and adaptation. Sports Med. 1989;7:207–34.
Peake JM, Neubauer O, Della Gatta PA, Nosaka K. Muscle damage and inflammation during recovery from exercise. J Appl Physiol. 2017;122:559–70.
Smith JL, Brunetz MH, Chenier TC, McCammon MR, Houmard JA, Franklin ME, et al. The effects of static and ballistic stretching on delayed onset muscle soreness and creatine kinase. Res Q Exerc Sport. 1993;64:103–7.
Wohlann T, Warneke K, Hillebrecht M, Petersmann A, Ferrauti A, Schiemann S. Effects of daily static stretch training over 6 weeks on maximal strength, muscle thickness, contraction properties, and flexibility. Front Sports Act Liv. 2023;5:1139065.
Fowles JR, MacDougall JD, Tarnopolsky MA, Sale DG, Roy BD, Yarascheski KE. The effects of acute passive stretch on muscle protein synthesis in humans. Can J Appl Physiol. 2000;25:165–80.
Garibotto G, Tessari P, Robaudo C, Zanetti M, Saffioti S, Vettore M, et al. Protein turnover in the kidney and the whole body in humans. Miner Electrolyte Metab. 1997;23:185–8.
Tessari P, Garibotto G, Inchiostro S, Robaudo C, Saffioti S, Vettore M, et al. Kidney, splanchnic, and leg protein turnover in humans: inside from leucine and phenylalanine kinetics. J Clin Invest. 1996;98:1481–92.
Sayegh JF, Lajtha A. In vivo rates of protein synthesis in brain, muscle, and liver of five vertebrate species. Neurochem Res. 1989;11:1165–8.
Laurent GJ, Sparrow MP, Millward DJ. Turnover of muscle protein in fowl: changes in rates of protein synthesis and breakdown during hypertrophy of the anterior and posterior latissimus dorsi muscles. Biochem J. 1978;176:407–14.
Nunes JP, Schoenfeld BJ, Nakamura M, Ribeiro AS, Cunha PM, Cyrino ES. Does stretch training induce muscle hypertrophy in humans? A review of the literature. Clin Physiol Funct Imaging. 2020;40:148–56.
Yahata K, Konrad A, Sato S, Kiyono R, Yoshida R, Fukaya T, et al. Effects of a high-volume static stretching programme on plantar-flexor muscle strength and architecture. Eur J Appl Physiol. 2021;121:1159–66.
Chen CH, Nosaka K, Chen HL, Lin MJ, Tseng KW, Chen TC. Effects of flexibility training on eccentric exercise-induced muscle damage. Med Sci Sports Exerc. 2011;43:491–500.
Reiner M, Gabriel A, Sommer D, Bernsteiner D, Tilp M, Konrad A. Effects of a high-volume 7-week pectoralis muscle stretching training on muscle function and muscle stiffness. Sports Med Open. 2023;9:40.
Panidi I, Donti O, Konrad A, Petros CD, Terzis G, Mouratidis A, et al. Muscle architecture adaptations to static stretching training: a systematic review with meta-analysis. Sports Med Open. 2023;9:47.
Gérard R, Gojon L, Decleve P, Van Cant J. The effects of eccentric training on biceps femoris architecture and strength: a systematic review with meta-analysis. J Athl Train. 2020;55:501–14.
Marušič J, Vatovec R, Marković G, Šarabon N. Effects of eccentric training at long-muscle length on architectural and functional characteristics of the hamstrings. Scand J Med Sci Sports. 2020;30:2130–42.
Lixandrão ME, Ugrinowitsch C, Berton R, Vechin FC, Conceição MS, Damas F, et al. Magnitude of muscle strength and mass adaptations between high-load resistance training versus low-load resistance training associated with blood-flow restriction: a systematic review and meta-analysis. Sports Med. 2018;48:361–78.
Davids CJ, Næss TC, Moen M, Cumming KT, Horwath O, Psilander N, et al. Acute cellular and molecular responses and chronic adaptations to low-load blood flow restriction and high-load resistance exercise in trained individuals. J Appl Physiol. 2021;131:1731–49.
Hwang PS, Willoughby DS. Mechanisms behind blood flow-restricted training and its effect toward muscle growth. J Strength Cond Res. 2019;33:S167–79.
Gundermann DM, Walker DK, Reidy PT, Borack MS, Dickinson JM, Volpi E, et al. Activation of mTORC1 signaling and protein synthesis in human muscle following blood flow restriction exercise is inhibited by rapamycin. Am Physiol Endocrinol Metabol. 2014;306:E1198–204.
Hotta K, Behnke BJ, Arjmandi B, Ghosh P, Chen B, Brooks R, et al. Daily muscle stretching enhances blood flow, endothelial function, capillarity, vascular volume and connectivity in aged skeletal muscle. J Physiol. 2018;596:1903–17.
van Dyke JM, Bain JLW, Riley DA. Preserving sarcomere number after tenotomy requires stretch and contraction. Muscle Nerve. 2012;45:367–75.
Warneke K, Wirth K, Keiner M, Schiemann S. Improvements in flexibility depend on stretching duration. Int J Exerc Sci. 2023;16:83–94.
Acknowledgements
The authors thank Daniel Jochum for his help with the graphical illustrations.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Open access funding provided by University of Graz.
Conflicts of interest/competing interests
Konstantin Warneke, David G. Behm, Shahab Alizadeh, Martin Hillebrecht, Andreas Konrad and Klaus Wirth have no conflicts of interest that are directly relevant to the content of this article.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and material
Not applicable.
Code availability
Not applicable.
Authors’ contributions
The initial idea for the paper as well as the first draft were provided by KoW. DB and AK provided their expertise in stretching and foam rolling. In consulting with MH, KlW and SA, the physiological and terminological aspects were discussed, and all authors included their respective expertise and knowledge. All authors contributed to the paper and agreed to the final version.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Warneke, K., Behm, D.G., Alizadeh, S. et al. Discussing Conflicting Explanatory Approaches in Flexibility Training Under Consideration of Physiology: A Narrative Review. Sports Med (2024). https://doi.org/10.1007/s40279-024-02043-y
Accepted:
Published:
DOI: https://doi.org/10.1007/s40279-024-02043-y