
Abstract
The so-called “stretch-induced force deficit” is known from a large amount of research. There are many theories trying to explain the stretch-induced force deficit and increases in the range of motion (ROM) which all offer a stretch training-specific explanation. However, when performing a commonly used strength training session, a reduced maximum strength (MSt) capacity can be assumed as well. Based on this, the aim of the study is to investigate the tension-induced force deficit due to a suprathreshold strength or stretching training stimulus. Therefore, 71 participants (age: 24.1 ± 4.2 years, height: 176.3 ± 5.7 cm, weight: 74.1 ± 7.5 kg) were divided into three groups: static stretching group (SST), strength training group (STR), and control group (CG). To investigate possible mechanical tension-induced force deficits, SST performed a long-lasting static stretching intervention for 1 h using an orthosis, while STR executed a common strength training intervention (5 × 12 repetition) for the plantar flexors. The results show a significant reduction of measured MSt as well as increased ROM for both SST and STR following the interventions. Consequently, we found similar acute effects of stretching and strength training regarding MSt and flexibility. We conclude that the decreased MSt capacities can possibly be attributed to mechanical tension-induced damage of the muscle that is not linked to a specific training method. The improvements in flexibility found in both intervention groups might be attributed to warm up effects when inducing high mechanical tension to large ankle joint angles.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Increasing the range of motion (ROM) through stretch training is applied in a wide field of sports practice (Angioi, Metsios, Koutedakis, & Wyon, 2009; Ávalos-Ramos & Vega-Ramírez, 2020; Cejudo et al., 2020b), injury prevention (Backman & Danielson, 2011; Gergley, 2013; Padua et al., 2019), and rehabilitation (Kim, Kim, Kim, & Kim, 2018). However, apart from known increases in ROM, the literature shows conflicting results regarding the acute effects on strength capacity which are possibly linked to difficulties in the quantification of the stretching stimulus.
Numerous studies suggest no effect, while others find a negative influence on maximal strength (MSt) performance (Chaabene, Behm, Negra, & Granacher, 2019; Marek et al., 2005; Santos et al., 2020). The differences in results can possibly be attributed to non-unified stretching protocols and/or measuring devices as well as differences in stretch intensity and duration (Kay & Blazevich, 2012). An acute negative impact on MSt—described as a stretch-induced force deficit (Behm, Alizadeh, Drury, Granacher, & Moran, 2021; Costa, Herda, Herda, & Cramer, 2014)—were only reported for stretching duration of > 45 s (Kay & Blazevich, 2012; Simic, Sarabon, & Markovic, 2013). No negative influence on MSt was found for shorter stretching durations. Konrad, Reimer, Thaller, and Tilp (2019) refer to different adaptations of the muscle–tendon unit (MTU) depending on the duration of stretching showing that shorter stretch durations as well as lower intensities lead to adaptive responses of the muscle tissue, while a stretch stimulus of more than 10 min also affects the MTU. Accordingly, Behm & Chaouachi (2011) and Kay & Balzevich (2012) found a dose–response relationship between stretching time and the negative adaptations in terms of movement speed and MSt capacity after stretching. Furthermore, Mizuno, Matsumoto, and Umemura (2014) and Konrad et al. (2019) found a reduction in MSt after a 5 min stretching intervention, while 1 min of stretching resulted in no loss of MSt.
Assuming a dose–response relationship, the strength deficit would increase by performing longer stretching durations which in turn would increase the magnitude of the stimulus; however, only few studies investigated the influence of long-lasting stretching interventions. These studies used stretching durations between 33 min (Fowles, Sale, & Macdougall, 2000) and 1 h (Avela, Finni, Liikavainio, Niemelä, & Komi, 2004) showing decreases in the maximal voluntary contraction (MVC) of up to 28%. Since Smith et al. (1993) show that stretching can induce sufficient mechanical tension to elicit microtraumatization, it could be hypothesized that exercise-induced muscle damage (EIMD) is the underlying factor for the acute decreases in MSt after stretching. EIMD is commonly known from strength training (Schoenfeld, 2012) which also leads to an acute decrease in MSt performance (Mackey, Thiele, Schnaiter-Brasche, Smith, & Conchola, 2020) following a similar dose–response relationship: Linnamo, Haekkinen, and Komi (1998) found a strength deficit of 23.7% following strength training with 5 sets of 10 repetitions using 80% of the one-repetition maximum (1 RM) that is more than twice as high compared to an 11% strength deficit after strength training with 5 sets of 10 repetitions using 40% of 1 RM in the leg extension. Additionally, acute MSt losses after leg muscle strength training (leg press, squat, leg extension) of up to 48% have been determined (Conchola, Thiele, Palmer, Smith, & Thompson, 2015). Accordingly, these studies highlight the influence of different load components, especially training volume and intensity, in strength training for the training-induced strength deficit.
In both forms of training the intensity is determined by the level of tension, the mechanical load and the time under tension (TUT). Based on this, the question arises to what extent the acute effects of strength training differ from those of stretch training. To answer this question, the present work compared a long-lasting stretch training using the highest possible intensity with a high-volume strength training. For this purpose, the acute effects on MSt following 1 h of stretch training for the plantar flexors were evaluated and compared to the acute effects of a calf muscle strength training.
Methods
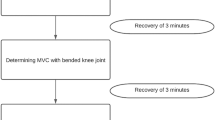
A total of 71 athletically active participants were recruited from physical education majors, gyms, and sports clubs and divided into three groups (static stretching = SST, strength training = STR, control = CG). To evaluate and compare the acute effects on MSt and flexibility following two different methods of inducing high mechanical tension on the muscle (tissue), SST performed a long-lasting static stretching and STR executed a strength training for the plantar flexors. MSt testing was performed in extended and bended knee joint. Examination of flexibility was also performed with extended and bended knee joint. A pre- to posttest design was used and the performed procedure is illustrated in Fig. 1.

Illustration of the testing procedure. SST static stretching, STR strength training, CG control group, MSt maximal strength
Participants
Participants were recruited from physical education majors, gyms, and sports clubs and divided into three groups (SST, STR, and CG). In all, 71 participants (Table 1) met the inclusion criteria of being injury free for the last 6 months and training in a gym for a minimum of twice a week. Subjects who have an increased risk for thrombosis or underwent surgery in the last 6 months were excluded from the study. Participants were divided into intervention groups (SST, STR) and CG by using a controlled allocation because not all participants were poised to join the long-lasting stretching intervention.
Testing procedure
Isometric strength tests
The testing consisted of two unilateral isometric MSt tests and two unilateral flexibility tests for the calf muscles.
The determination of isometric MSt in the extended knee joint was performed using a 45° leg press (LP). For this, the subject positioned one foot on the foot rest so that the metatarsophalangeal joint was placed on the edge of the force plate with a force transducer (model KAC, AST, Leipzig, Germany) with a measurement range of ±5000 N and a 13-bit analog-to-digital converter and a pull in frequency of 1000 Hz. The leg press sled with the attached force plate was fixed in position with industrial grade tensioning straps so that the subject could perform a maximal isometric contraction in plantar flexion with the knee joint extended and the ankle joint at 90°. In response to an acoustic signal, the subject had to perform a maximal plantar flexion against the force plate and hold it for 1 s. After each repetition the subject rested for 1 min to avoid fatigue. Repetitions were performed until the subject did not increase the MSt output in two consecutive trials; however, a minimum of five trials was performed.
In addition, the isometric maximum force in bended knee joint was recorded for both legs separately with unilateral MSt measurement in a calf muscle testing device (CMD). For this purpose, the subject was instructed to perform a maximum voluntary plantar flexion and hold it for 1 s in response to an acoustic signal. The pad of the measuring device was fixed in position with industrial grade tensioning straps so that the ankle and knee joint angles were at 90°. Testing was performed until the achieved force values stopped increasing, with a minimum of five trials. The maximum force was determined in each case using a 10 × 10 cm force plate in which force sensors (Kistler Element 9251A, Kistler Instrument Corp., Amherst, NY, USA) with a resolution of 1.25 N, a pull-in frequency of 500 Hz and a measurement range of ±5000 N were installed. The vertical forces (Fz) were recorded. In addition, a charge amplifier (Type 5009 Charge Amplifier, Kistler Instrument Corp.) and a 13-bit AD converter (NI6009, National Instruments Corp., Austin, TX, USA) were used. For the data acquisition the self-developed program (WKM) was used which calculated the vertical forces, displayed them graphically and then followed up with further parameterization. The reliability can be classified as high with ICC values of 0.982 and 0.971.

Progression of mean values for maximal strength measurement from pre- to posttest regarding SST, STR, and CG for the intervened leg in leg press (LP) and calf muscle device (CMD)
ROM measurement
ROM in the upper ankle joint was recorded in all three groups via the knee to wall stretch (KtW) with a sliding device. The subject was instructed to place the foot on the attached marker. The contralateral leg was held in the air, while the bodyweight was stabilized by placing the hands on a doorframe. To record the ROM, the subject pushed the board of the sliding device forward until the heel of the standing leg lifted off while one investigator pulled on a sheet of paper placed under the subject’s heel. As soon as this could be pulled out from under the heel, the measurement was stopped. The flexibility score was read off in centimeters from the attached measuring tape. Three valid trials were performed per leg and the maximum value was used for evaluation. The reliability of the measurement can be considered high with an ICC of 0.987 (right leg) and 0.992 (left leg).
Additionally, the ROM in the direction of dorsiflexion was recorded via the angle measuring device of the orthosis (ORT). For this purpose, the foot of the subject was fixed into a maximally dorsiflexed position with the aid of the orthosis and the achieved angle was read off. The angle measurement was performed with a measurement accuracy of 2.5°.
Intervention
The procedure of the intervention was designed to achieve high mechanical tension in the muscles via either a stretching intervention or a strength training intervention—the latter typically being used to achieve muscular hypertrophy.
SST performed a 1 h stretching intervention using a stretching orthosis for the calf muscles. For this purpose, the stretching orthosis was applied to the subject’s leg by the investigator so that the foot was fixed into a maximally dorsiflexed position. This resulted in the stretching of the calf muscles. While undergoing intervention, each subject from SST sat on a chair with the intervened leg placed on a different chair with the back flat against the backrest so that a 90° hip–trunk angle was maintained. The subject was instructed to stretch with a straight back in an upright position for 1 h. Subjects were instructed to adjust the orthosis every 15 min to control the intensity of stretching.
The STR performed calf muscle strength training consisting of 5 sets of 12 repetitions of calf raises on the 45° leg press. For this purpose, the subject was supervised and instructed by the investigator to perform the repetitions over the full ROM. The participant rested for 2 min between sets.
Both interventions were performed with one leg. The nonintervened leg served as the control leg. The CG did not perform any intervention for 1 h.
Data analysis
The analysis was performed using SPSS (version 28.0., IBM Corp., Armonk, NY, USA). The Shapiro–Wilk test showed normal distribution of baseline values (p > 0.05). Testing for significant differences in baseline values was performed using one-way analysis of variance (ANOVA). The changes in MSt as well as ROM between the three groups depending on the test time were calculated using a two-way ANOVA. The Scheffé test was used as a post hoc. Effect sizes are presented as eta squared (η2) and categorized as: small effect η2 < 0.06, medium effect η2 = 0.06–0.14, large effect η2 > 0.14 (Cohen, 1988). Since sample sizes are different in each group, Hedges’ g was calculated for the differences between groups using pooled standard deviation and were classified as follows: small effect g ≥ 0.2, moderate effect g ≥ 0.5 and high effect g ≥ 0.8 (Becker, 2000). Post hoc power (1-β) was calculated via G‑Power (version 3.1, Düsseldorf, Germany). The level of significance was p < 0.05.
Results
The descriptive statistics and results of two-way ANOVA for measured values in the intervened leg are displayed in Table 2. Figures 1 and 2 display progression from pre- to posttest in the intervened leg.
The one-way ANOVA showed no significant differences between the pretest values for all parameters. Partial eta squared revealed a high effect size effect of η2 = 0.438 for the change in mean values for time and a high effect size of η2 = 0.274 for the time × group interaction effect for isometrically recorded MSt in the intervened leg, determined via LP. In addition, for CMD partial eta squared revealed a high effect size effect of η2 = 0.185 for the change in mean values from pretest to posttest and a medium effect size of η2 = 0.153 for time × group interaction effect for isometrically recorded MSt in the intervened leg. Results are illustrated in Fig. 2. For ROM measurement partial eta squared revealed a high effect size effect of η2 = 0.433 for the change in mean scores for the factor time and a high effect size of η2 = 0.19 for the time × group interaction effect for ROM in the intervened leg, determined via the KtW. For ROM measured via ORT the partial eta squared revealed an effect with high effect size of η2 = 0.253 for the change in mean values for the factor time and a medium effect size of η2 = 0.072 for the interaction effect for time × group for ROM in the intervened leg. Results are illustrated in Fig. 3.

Progression of mean values for ROM measurement from pre- to posttest regarding SST, STR, and CG for the intervened leg in knee to wall test (KtW) and angle measuring device of the orthosis (ORT)
The Scheffé test showed significant differences for mean differences between SSTLP and CGLP (g = 0.85, p < 0.001) and between STRLP and CGLP (g = 0.78, p < 0.001) but no difference between SSTLP and STRLP (p = 0.922). For CMD post hoc test showed significant differences for mean differences between SSTCMD and CGCMD (g = 0.37, p = 0.006) and between STRCMD and CGCMD (g = 0.09, p = 0.035) but no significant differences were found between SSTCMD and STRCMD (p = 0.799).
For ROM measurement via KtW, the Scheffé test showed significant differences between SSTKtW and CGKtW (g = 0.24, p = 0.001) and between STRKtW and CGKtW (g = 0.18, p = 0.02) for mean differences. No significant differences were found between SSTKtW and STRKtW (p = 0.627). For the ROM measurement via ORT, the Scheffé test showed no significant differences between groups for mean differences.
G‑Power post hoc analysis for F‑tests for within factors calculated 1‑β = 86.72% for the lowest effect size with η2 = 0.185 and 1−β = 99.99% for the highest effect size with η2 = 0.438 with α = 0.05 for three groups and two time points for the time effect. Furthermore, for interaction group × time, there was 1−β = 16.99% for the lowest effect size with η2 = 0.072 and 1−β = 98.63% for the highest effect size with η2 = 0.274 with α = 0.05 for three groups and two time points.
Discussion
The present study shows significant decreases in MSt values as an acute effect following long-lasting stretching (SST: −16.2%) as well as strength training (STR: −15.5%) in extended knee joint as well as in bended knee joint (SST: −8.6%; STR: −7.6%). Mobility measurements showed significant increases in ROM for the stretched leg at 6.9% (KtW) and 8.2% (ORT), while strength training resulted in increased ROM of 5.7% (KtW) and 5.7% (ORT) in the intervened leg. There were no significant differences from pre- to posttest in the CG.
The only studies using comparable stretching durations were those by Fowles et al. (2000) and Avela et al. (2004) with durations of 33 min and 1 h, respectively. The listed studies performed intermittent stretching protocols meaning a comparison to the uninterrupted long-lasting static stretching intervention used in the presented study is limited. Furthermore, comparatively small sample sizes of n = 10 may be responsible for a higher decrease in the average maximum force values, as individual progressions have a stronger effect on the overall statistics.
It can be concluded that the acute effects of an intensive and prolonged stretching training for 1 h shows similar effects compared to a commonly used strength training with 5 sets of 12 repetitions. Similar decreases in MSt and increases in ROM of the intervened leg were identified for both interventions. There are different explanatory approaches regarding the MSt decreases from previous studies attributing the MSt losses to a reduction in tendon stiffness and muscle stiffness (Fowles et al., 2000; Kato, Vieillevoye, Balestra, Guissard, & Duchateau, 2011; Konrad et al., 2019) as well as neural decrements in muscle activation, especially if there is a prolonged time of stretching (Avela et al., 2004; Fowles et al., 2000). The reduced stiffness of the muscle and tendon could lead to reduced energy storage (Rosario & Roberts, 2020) and diminished use of the stretch-shortening cycle (Kallerud, Gleeson, Kallerud, Gleeson, & Gleeson, 2013). However, this does not explain a reduction in MSt values in an isometric maximum force measurement since no stretch shortening cycle is involved.
However, the preferred theory in our work is a strength deficit based on muscle damage. It is known from strength training that the usage of high intensity and TUT can induce EIMD (Schoenfeld, 2012) which could result in a decrease in MSt (Mackey et al., 2020). Thus, it is possible that the decreasing maximum force values after a stretching intervention can also be attributed to EIMD. As Smith et al. (1993) already demonstrated, a stretching stimulus of sufficient intensity can lead to muscle damage. This could possibly indicate that the stretch-induced force deficit may be attributed to mechanical tension or EIMD irrespective of the use of stretch or strength training.
In principle, similar effects have been measured in both groups for ROM. In the literature, the most prominent explanations for the increase in flexibility as an acute effect of stretch training refer to a reduced pain tolerance, a change in nociception or a reduced resting tension of the muscle due to a change in the MTU (Freitas et al., 2018; Kay & Blazevich, 2012; Opplert & Babault, 2018). However, we also identified increased ROM as an acute response to strength training.
Thus, increases in flexibility could also be linked to warm-up effects such as improved viscosity in the muscles (Padua et al., 2019) and reduced joint friction due to increased synovial fluid flow (Roberts, Law, & Thom, 2019). It is possible that the increases in flexibility in the present work can be explained by previously discussed effects (altered resting tension, adaptations of the MTU, altered neuronal processes), but it is questionable whether these adaptations are specific to stretch training or general reactions of the body to an increased state of warming (Bishop, 8,9,a, b).
The results of the present study show that, in principle, acute effects of a long-lasting stretching training regarding MSt and ROM do not differ from those of a strength training.
Limitations
Using the KtW, the anthropometry of the participants, in particular the length of the tibia may influence the measurement score and should be normalized a priori. However, we hypothesize that this plays a minor role in this study since it can be assumed that the participants’ body anthropometrics (e.g., the length of lower limb) did not change from pre- to posttest. Thus, exclusively intraindividual changes were measured from pre- to posttest. From this, even if a comparison with other flexibility testing procedures or the interindividual comparison seems to be limited, results showed increases in ROM in used measurements. Nevertheless, Cejudo, de Baranda, Ayala, and Santonja (2015) and Cejudo, de Baranda, Ayala, Croix, & Santonja-Medina (2020a) stated high reliability of commonly used tests in clinical settings which could be included in further studies to exclude possible limitations of the KtW test.
Conclusion
Based on the results, we conclude that there are similar decreases in maximum strength (MSt) and similar increases in range of motion (ROM) due to induced mechanical tension irrespective of whether the underlying stimulus resulted from stretching or strength training. Decreased MSt values could possibly be attributed to exercise-induced muscle damage (EIMD), changes in the muscle–tendon unit (MTU), reduced passive stiffness or compliance. Increased ROM can possibly be attributed to an increased warm-up state or decreased pain tolerance following stretch or strength training—as long as strength training is performed over full ROM.
Practical Implications
We recommend avoiding high mechanical tension irrespective of whether it is achieved through stretch or strength training prior to sports depending on producing maximum force values. Accordingly, a performance-enhancing warm-up should not include any suprathreshold mechanical stimuli so that the positive effects, such as an increased range of motion (ROM), can be achieved without negatively influencing strength performance.
References
Angioi, M., Metsios, G., Koutedakis, Y., & Wyon, M. A. (2009). Fitness in contemporary dance: a systematic review. Int J Sports Med, 30, 475–484.
Ávalos-Ramos, A., & Vega-Ramírez, L. (2020). Gender differences in the level of achievement of gymnastic and acrobatic skills. Int. J. Environ. Res. https://doi.org/10.3390/ijerph17197216
Avela, J., Finni, T., Liikavainio, T., Niemelä, E., & Komi, P. V. (2004). Neural control of movement neural and mechanical responses of the triceps surae muscle group after 1 h of repeated fast passive stretches. J Appl Physiol, 96, 2325–2332. https://doi.org/10.1152/japplphysiol.01010.2003.-Experiments.
Backman, L. J., & Danielson, P. (2011). Low range of ankle dorsiflexion predisposes for patellar tendinopathy in junior elite basketball players: a 1-year prospective study. Am J Sports Med, 39(12), 2626–2633.
Becker, L. A. (2000). Effect size measure for two independent groups. Jurnal Effect Size Beeker, 1993, 3.
Behm, D. G., & Chaouachi, A. (2011). A review of the acute effects of static and dynamic stretching on performance. European Journal of Applied Physiology, 111(11), 2633–2651. https://doi.org/10.1007/s00421-011-1879-2.
Behm, D. G., Alizadeh, S., Drury, B., Granacher, U., & Moran, J. (2021). Non-local acute stretching effects on strength performance in healthy young adults. European Journal of Applied Physiology, 121(6), 1517–1529.
Bishop, D. (2003a). Warm up I potential mechanisms and the effects of passive warm up on exercise performance. Sports Med, 33(6), 439–454.
Bishop, D. (2003b). Warm up II performance changes following active warm up and how to structure the warm up. Sports Med, 33(7), 483–498.
Cejudo, A., de Baranda, P. S., Ayala, F., & Santonja, F. (2015). Test-retest reliability of seven common clinical tests for assessing lower extremity muscle flexibility in futsal and handball players. Phys Ther Sport, 16(2), 107–113.
Cejudo, A., de Baranda, P. S., Ayala, F., Croix, M. D. S., & Santonja-Medina, F. (2020a). Assessment of the range of movement of the lower limb in sport: Advantages of the rom-sport i battery. International Journal of Environmental Research and Public Health, 17(20), 1–25. https://doi.org/10.3390/ijerph17207606.
Cejudo, A., Moreno-Alcaraz, V. J., Izzo, R., Robles-Palazón, F. J., de Baranda, P. S., & Santonja-Medina, F. (2020b). Flexibility in spanish elite inline hockey players: Profile, sex, tightness and asymmetry. International Journal of Environmental Research and Public Health, 17(9), 1–14. https://doi.org/10.3390/ijerph17093295.
Chaabene, H., Behm, D. G., Negra, Y., & Granacher, U. (2019). Acute effects of static stretching on muscle strength and power: an attempt to clarify previous caveats. Front Physiol. https://doi.org/10.3389/fphys.2019.01468.
Cohen, J. (1988). Statistical power analysis for behavioral sciences (2nd edn.).
Conchola, E. C., Thiele, R. M., Palmer, T. B., Smith, D. B., & Thompson, B. J. (2015). Acute postexercise time course responses of hypertrophic vs- power-endurance squat exercise protocols on maximal and rapid torque of the knee extensors. J Strength Cond Res, 29(5), 1285–1294.
Costa, P. B., Herda, T. J., Herda, A. A., & Cramer, J. T. (2014). Effects of dynamic stretching on strength, muscle imbalance, and muscle activation. Med Sci Sports Exerc, 46(3), 586–593.
Fowles, J. R., Sale, D. G., & Macdougall, J. D. (2000). Reduced strength after passive stretch of the human plantarflexors. J Appl Physiol, 89(3):1179–1188. https://doi.org/10.1152/jappl.2000.89.3.1179.
Freitas, S. R., Mendes, B., Le Sant, G., Andrade, R. J., Nordez, A., & Milanovic, Z. (2018). Can chronic stretching change the muscle-tendon mechanical properties? A Review. Scand J Med Sci Sports, 28(3), 294–306.
Gergley, J. C. (2013). Acute effect of passive static stretching on lower-body strength in moderately trained men. J Strength Cond Res, 27(4), 973–977.
Kallerud, H., Gleeson, N., Kallerud, H., Gleeson, Á. N., & Gleeson, N. (2013). Effects of stretching on performances involving stretch-shortening cycles. Sports Med, 43, 733–750.
Kato, E., Vieillevoye, S., Balestra, C., Guissard, N., & Duchateau, J. (2011). Acute effect of muscle stretching on the steadiness of sustained submaximal contractions of the plantar flexor muscles. J Appl Physiol, 110, 407–415.
Kay, A. D., & Blazevich, A. J. (2012). Effect of acute static stretch on maximal muscle performance: a systematic review. Medicine and Science in Sports and Exercise, 44(1), 154–164. https://doi.org/10.1249/MSS.0b013e318225cb27.
Kim, G., Kim, H., Kim, W. K., & Kim, J. (2018). Effect of stretching-based rehabilitation on pain, flexibility and muscle strength in dancers with hamstring injury: a single-blind, prospective, randomized clinical trial. J Sports Med Phys Fitness, 58(9), 1287–1295.
Konrad, A., Reimer, M. M., Thaller, S., & Tilp, M. (2019). The time course of muscle-tendon properties and function responses of a five-minute static stretching exercise. Eur J Sport Sci, 19(9), 1195–1203.
Linnamo, V., Haekkinen, K., & Komi, P. V. (1998). Neuromuscular fatigue and recovery in maximal compared to explosive strength loading. Eur J Appl Physiol, 77, 176–181.
Mackey, C. S., Thiele, R. M., Schnaiter-Brasche, J., Smith, D. B., & Conchola, E. C. (2020). Effects of power-endurance and controlled heavy squat protocols on vertical jump performance in females. Int J Exerc Sci, 13(4), 1072–1085.
Marek, S. M., Cramer, J. T., Fincher, L. A., Massey, L. L., Dangelmaier, S. M., Purkayastha, S., Fitz, K. A., & Culbertson, J. Y. (2005). Acute effects of static and proprioceptive neuromuscular facilitation stretching on muscle strength and power output. J Athl Train, 40(2), 94–103.
Mizuno, T., Matsumoto, M., & Umemura, Y. (2014). Stretching-induced deficit of maximal Isomtreic torque is restored within 10 minutes. J Strength Cond Res, 28(1), 147–153.
Opplert, J., & Babault, N. (2018). Acute effects of dynamic stretching on muscle flexibility and performance: an analysis of the current literature. Sports Med, 48(2), 299–225.
Padua, E., D’amico, G. A., Alashram, A., Campoli, F., Romagnoli, C., Lombardo, M., Quarantelli, M., Di Pinti, E., Tonanzi, C., & Annino, G. (2019). Effectiveness of warm-up routine on the ankle injuries prevention in young female basketball players: a randomized controlled trial. Medicina, 55, 1–9. https://doi.org/10.3390/medicina55100690.
Roberts, H. M., Law, R.-J., & Thom, J. M. (2019). The time course and mechanisms of change in biomarkers of joint metabolism in response to acute exercise and chronic training in physiologic and pathological conditions. Europ J Appl Physiol, 119(3), 2401–2420.
Rosario, M. V., & Roberts, T. J. (2020). Loading rate has little influence on tendon fascicle mechanics. Front. Physiol, 11, 255.
Santos, C. X., Beltrao, N. B., Piraua, A. L. T., Durigan, J. L. Q., Behm, D., & Araújo (2020). Static stretching intensity does not influence acute range of motion, passive torque, and muscle architecture. J Sport Rehabil, 29(1), 1–6.
Schoenfeld, B. J. (2012). Does exercise-induced muscle damage play a role in skeletal muscle hypertrophy? J Strength Cond Res, 26(5), 1441–1453.
Simic, L., Sarabon, N., & Markovic, G. (2013). Does pre-exercise static stretching inhibit maximal muscular performance? A meta-analytical review. Scandinavian Journal of Medicine and Science in Sports, 23(2), 131–148.
Smith, J. L., Brunetz, M. H., Chenier, T. C., McCammon, M. R., Houmard, J. A., Franklin, M. E., & Israel, R. G. (1993). The effects of static and ballistic stretching on delayed onset muscle soreness and creatine kinase. Res Q Exerc Sport, 64(1), 103–107.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
K. Warneke, T. Wohlann, L. H. Lohmann, K. Wirth, and S. Schiemann declare that they have no competing interests.
All procedures performed in studies involving human participants or on human tissue were in accordance with the ethical standards of the institutional and/or national research committee and with the 1975 Helsinki Declaration and its later amendments or comparable ethical standards. Approval for this study was obtained from the institutional review board (Carl von Ossietzky Universität Oldenburg, No. 121-2021). Informed consent was obtained from all individual participants included in the study.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Warneke, K., Wohlann, T., Lohmann, L.H. et al. Acute effects of long-lasting stretching and strength training on maximal strength and flexibility in the calf muscle. Ger J Exerc Sport Res 53, 148–154 (2023). https://doi.org/10.1007/s12662-022-00854-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12662-022-00854-7