
Abstract
Introduction
Value-based healthcare has potential for cost control and quality improvement. To assess this, we review the evidence on the impact of value-based payment (VBP) models in the context of networks of care (NOC) and transmural care.
Methods
We used the PRISMA guidelines for this systematic literature review. We searched eight databases in July 2021. Subsequently, we conducted title and abstract and full-text screenings, and extracted information in an extraction matrix. Based on this, we assessed the evidence on the effects of VBP models on clinical outcomes, patient-reported outcomes/experiences, organization-related outcomes/experiences, and costs. Additionally, we reviewed the facilitating and inhibiting factors per VBP model.
Findings
Among articles studying shared savings and pay-for-performance models, most outline positive effects on both clinical and cost outcomes, such as preventable hospitalizations and total expenditures, respectively. Most studies show no change in patient satisfaction and access to care when adopting VBP models. Providers’ opinions towards the models are frequently negative. Transparency and communication among involved stakeholders are found to be key facilitating factors, transversal to all models. Additionally, a lack of trust is an inhibitor found in all VBP models, together with inadequate targets and insufficient incentives. In bundled payment and pay-for-performance models, complexity in the structure of the program and lack of experience in implementing required mechanisms are key inhibitors.
Conclusions
The overall positive effect on clinical and cost outcomes validates the success of VBP models. The mostly negative effects on organization-reported outcomes/experiences are corroborated by findings regarding providers’ lack of awareness, trust, and engagement with the model. This may be justified by their exclusion from the design of the models, decreasing their sense of ownership and, therefore, motivation. Incentives, targets, benchmarks, and quality measures, if adequately designed, seem to be important facilitators, and if lacking or inadequate, they are key inhibitors. These are prominent facilitators and inhibitors for P4P and shared savings models but not as prominent for bundled payments. The complexity of the scheme and lack of experience are prominent inhibitors in all VBP models, since all require changes in several areas, such as behavioral, process, and infrastructure.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Providers’ disconnection from the model may be a reason for their lack of trust and motivation. The sizable share of studies with mixed and lack of effects in clinical/cost outcomes can be explained by the considerable amount of time it takes for results to take effect when implementing value-based payment (VBP) models. |
Collaboration is a key element of VBP, and increased coordination is a logical result of it. The differences found between different VBP models in incentives, targets, benchmarks, and quality measures, as well as complexity and lack of experience of the schemes, can be attributed to the characteristics of the schemes, but further research is required to validate such a relationship. |
1 Context
Healthcare systems are struggling to control costs and improve quality [1]. Value-based healthcare (VBHC) has the ambition to address both. Porter and Lee argue maximizing value for patients can achieve the best possible outcomes at the lowest possible cost [1]. The VBHC strategy, amongst others, requires to move from a fee-for-service (FFS) reimbursement model, which rewards quantity over quality, to a value-based payment (VBP) model, which focuses on health outcomes [2, 3], and incentivizes providers to deliver the best care at reasonable cost, and improving the overall value of care [4,5,6]. To do so, the fragmented system needs to be replaced by one in which services for a certain medical condition are organized in health-delivery networks delivering high-value care. To achieve this, there should be an adequate organization around the patient’s condition, measurement of costs and outcomes for each patients, development of bundled prices for the full care cycle, integration of care across separate facilities, expanding geographic reach, and use of data and building adequate IT platforms [1] for collecting and making data available. As these elements are expected to be mutually reinforcing, a payment model that provides both maximization of value and multi-provider involvement will yield the highest impact [1, 7].
Paying for health services without considering health outcomes may create fewer or no incentives for providers to improve quality of care [8]. Without providers’ incentivized by these payment schemes, the provision of healthcare may suffer [9]. Therefore, changing the way healthcare providers are rewarded can create meaningful incentives for quality improvement. By linking payment to performance, healthcare providers may have an incentive to increase their efforts to improve quality of care. A consequence is that financial risk is shifted away from insurance companies and is attributed partly or fully to healthcare providers [10]. Despite the benefits of linking outcomes to payments, there are some challenges. The models may have unintended effects, such as a strong focus on the measured outcomes to which the financial incentives are attached to at the expense of other meaningful outcomes that are not rewarded. In addition, VBP models may lead to risk selection to improve registered clinical outcomes, also known as “cherry-picking” [6, 11,12,13,14,15]. This can potentially lead to inequalities in access to healthcare. Existing literature has noted the importance of a careful design and scope of VBP models, so that they incentivize the required investments and behavioral changes in stakeholders [16, 17].
In working towards VBHC, the Quadruple Aim has emerged as a guiding principle. This includes four goals: improving patient experience, improving health of populations, reducing cost of care, and improving provider experience [18]. Considering these goals, the most relevant types of outcome measures can be divided in patient-reported outcomes/experience measures (PROMs/PREMs), clinical outcomes (health outcomes for the patient), organization-related outcomes/experience, and costs outcomes. The aim of this paper is to review the evidence on the impact of applying VBP models and organize this evidence around these four categories.
Globally, the interest in VBHC is growing rapidly, and with that, the adoption of VBP models [7, 19, 20]. Bundled payments are a common model of VBP, with several countries having developed such models, with a one-time payment or an episode payment for services provided for the treatment of a specific condition. The recipients of the bundled payment are financially accountable for any costs incurred [21]. The VBP models can either be for partial or full patient care, depending on the extent of the collaboration between providers. Under shared savings programs, providers are rewarded with a percentage of the savings if they can put measures in place to lower overall patient cost bellow what the payer would have anticipated [22]. Pay-for-performance (P4P) models are also regularly adopted VBP models that reward specific, measurable aspects of value [7]. A very strict view of P4P only rewards achieved patient outcomes. However, taking a broader view P4P models may also reward process compliance that may translate into health outcomes for patients.
Our related systematic literature review [23] has listed the facilitating and inhibiting factors in the design, implementation, and applicability of VBP models in the context of networks of care (NOC) (a group of health service centers that are connected across all levels of care and share responsibility for health outcomes [24]) and transmural care (care provided based on collaboration and coordination between different levels of care, such as primary and secondary [25]). These two concepts, although similar, are not identical, since transmural care connects primary care with hospitals, and NOC implies a connection between health centers and may for example refer to a network of hospitals only. Transmural care can then be considered a form of NOC. It is important to incorporate both terms because the integration of care can be between primary, secondary, and tertiary care, or any combination of two out of the three care settings. In our related systematic literature review, we found that a focus on realistic benchmarks, adequate incentives, a diverse team, transparency, and communication among stakeholders are important to adopt in a VBP model. Also, inadequate targets, insufficient incentives, excessive amount of time improvements take to manifest, and misaligned views about the model among involved stakeholders hinder the correct functioning of the models.
One other review has focused on specific phases or characteristics of the VBP models [2]. Studies have also assessed singular payment models, such as P4P models (leaving out, for example, bundled payments) [3] or Accountable Care Organizations [4]. One review by Vlaaderen et al. provided an analysis of the characteristics and effectiveness of VBP models but clustered the models in two groups (narrow and broad outcome-based payment models) and did not analyze the effectiveness and characteristics singularly [5]. Additionally, the review was not conducted in a context of NOC and transmural care. This limits the possibility of studying a context with a high impact in achieving the best results at a lower cost.
To assess whether VBHC delivers on its promise, this review aims to analyze, in a context of NOC and transmural care, the impact of different types of VBP models on outcomes (such as clinical and cost), and reviews what facilitating and inhibiting factors are associated to each model type. Evidence on these issues may provide insights on which model to adopt, given the different objectives of the organizations. This way, organizations gain knowledge on the factors to support, as well as the ones to avoid, depending on the VBP models adopted.
2 Methods
Our systematic literature review used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework and checklist (Online Supplemental Material (OSM) 1). This review followed another study that systematically reviewed the facilitating and inhibiting factors of VBP models in the context of NOC and transmural care. The protocol for that review study was registered in Prospero (ID CRD42021259630).
Inclusion criteria:
-
Type of payment model Value-based payment models like bundled payments, shared savings, and P4P.
-
Type of care Transmural care or care provided in a network of providers.
-
Setting Networks of care, multiple providers or any other setting that includes more than one provider.
-
Analysis of the payment model Outlining barriers and/or success factors of VBP models studied and/or articles assessing relevant outcomes (clinical, PROMs, organizational-related and costs).
Exclusion criteria:
-
Type of payment model Non-VBP models, such as FFS, capitation payment for single providers, global/budget payments, or any other payment models where services are unbundled and paid for separately), or do not cover payment models at all.
-
Type of care Care not provided in a (transmural) network.
-
Setting Single provider organization.
-
Analysis of the payment model Not outlining barriers and/or success factors of VBP models, nor measuring relevant clinical, PROMs/PREMs, organizational-related outcome measures or costs.
2.1 Search Strategy
The search was conducted in July 2021, using eight databases: (1) PubMed; (2) PsycINFO; (3) Cochrane Library; (4) JSTOR; (5) EconLit; (6) CINAHL; (7) PsycArticles; (8) Trip Database.
Three key components were used to build the search terms for the identification of studies on VBP models in NOC and transmural care: (1) keywords related to VBHC (e.g., performance-based or risk-sharing); (2) keywords related to provider payment (e.g., funding or purchasing); (3) keywords related to transmural and NOC (e.g., network or multi-provider). Synonyms/plural of those keywords and differences in spelling were considered when deciding on the exact search phrase. The search phrase also included MeSH terms related to the above keywords, which ensured comprehensiveness of the search. Additionally, the search is limited to publications from January 2005 onwards written in English. We selected this starting period since, based on PubMed searches, VBHC gained substantial adhesion around 2005. One example is Michael Porter’s book on redefining healthcare, published in 2006 [26]. Only the title and/or abstract of studies was searched for the presence of keywords (OSM 2). The search phrase used in each database can be found in OSM 3−10.
2.2 Study Selection Process
The selection process included three steps: screening based on title and abstract, screening based on full-text, and screening of reference lists. The primary researcher was the main screener in both the title/abstract and full-text screenings. In the title and abstract screening, the primary screener reviewed all titles and abstracts and determined a study’s eligibility for the next full-text screening. The inclusion criteria required that the study examined a VBP model and NOC or transmural care. Two other researchers (additional screeners) cross-checked one-third of studies that the primary researcher deemed “excluded” and all studies deemed “uncertain.” If all screeners could not determine if a study met the inclusion criteria, the study was included for full-text screening.
Three screeners, including the primary researcher, participated in the full-text screening. To ensure consistency, the same percentage of studies “excluded” by the primary screener (one-third) and all “uncertain” studies were cross-checked by the two additional screeners. In addition to the inclusion criteria used in the first screening, studies were deemed eligible only if they also focused on facilitators/inhibitors and/or relevant outcome measures related to VBP models. Also, the studies should be peer-reviewed. Commentaries, briefs, essays, reviews, and any non-peer-reviewed publications were excluded. Finally, articles for which the full text could not be found were also excluded after attempting to contact the authors and the journal where they were published.
After the two stages of screening, the final selection included publications of VBP models in NOC and transmural care, outlining facilitating and/or inhibiting factors of these models, and/or relevant outcome measures. We screened the reference lists of all included publications. During the screening of the reference lists, potentially relevant titles that mention VBP models were included for a check. The main researcher screened the title/abstract and full text using the same inclusion criteria as mentioned before. The included articles were added to the final selection of publications for analysis. Commentaries, briefs, essays, reviews, and any non-peer-reviewed publications, with all other inclusion criteria fulfilled, were once again excluded.
In order to measure the inter-rater reliability between the primary screener and the two additional screeners for both screenings, Cohen’s Kappa was used (OSM 11 and 12). In the abstract screening (kappa k = 0.984), and full-text screening (kappa k = 0.745), there was an almost perfect and substantial agreement, respectively.
2.3 Quality Assessment
The quality of the quantitative studies was assessed using the “Quality Assessment Tool for Quantitative Studies” by the Effective Public Health Practice Project (EPHPP) [27]. The Critical Appraisal Skills Programme (CASP) checklist [28] was used to assess the qualitative studies. If a quantitative study had no aspects rated as weak in the EPHPP assessment tool, it was considered a study with high quality. A qualitative study was rated as strong if at least six out of nine study aspects in the CASP assessment tool were evaluated positively. Mixed methods studies were assessed using both checklists mentioned above.
2.4 Data Extraction and Analysis
After the screening, categories relevant for the review were identified, and information was extracted based on those categories. This directed qualitative content analysis was based on Hsieh and Shannon [29]. In addition to information on facilitating and inhibiting factors of VBP models under NOC and transmural care, we also extracted data on the VBP models studied and the outcomes of these models. The themes that form the units of analysis were:
-
(1)
Characteristics of the VBP models payment type, provider involvement in the model design, nature of the incentivized entity, the motivation behind the model, and duration of the program applying the model.
-
(2)
Outcome measures clinical outcomes, patient-reported outcomes/experiences, organization-related outcomes/experiences and cost outcomes.
-
(3)
Effect direction overall positive effect/association, overall negative effect/association, mixed effect/association, no effect/association.
-
(4)
Facilitating and inhibiting factors of VBP models studied.
We used different design element categories to explore possible explanations for any differences that might arise in the impact of the implementation of different VBP models on the four categories of outcome measures, as well as the different facilitating/inhibiting factors found per VBP model.
For the analysis of the relation between outcomes and facilitating and inhibiting factors in the design/development, implementation, and applicability, we used the same division in the framework as applied in the accompanying systematic literature review (Fig. 1). This division was based on a framework proposed by Greenhalgh et al. [30], which was adapted for this review.

Framework of facilitating and inhibiting factors of value-based payment (VBP) modelsa. aBased on Greenhalgh et al. [30]
To further analyze the VBP models identified in the review, two cross-tabulations were built. The first one compared the four types of outcome measures (as described in theme 2) with the different types of VBP models. Each comparison depicted the four directions of the outcome measures (positive, negative, mixed and no effect) and gave examples on the outcomes measured. Most included publications studied multiple outcome measures, and we considered a positive/negative effect if more than half the outcomes measured had a positive/negative impact. If there was a similar positive and negative impact, we attributed it to a mixed impact. We expected this comparison to give us an explanation for the differences in effect directions per type of VBP model.
The second cross-tabulation also compared the different types of VBP models with the effect they had on the different types of outcome measures. However, we linked the most frequent facilitating factors in the publications describing a certain VBP model and with an effect on a certain type of outcome measure. The same linkage was made for the most frequent inhibiting factors. In doing so, we expected to be able to depict any differences in factors between types of outcome measures and/or between types of VBP models.
3 Findings
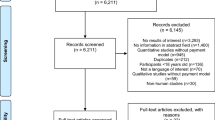
The search resulted in 5988 publications, 5148 of which were included in the first stage of the screening, after eliminating duplicates. Based on the inclusion criteria, 575 publications were eligible for the second screening phase. After analyzing the full text of these publications, 119 were retained and included in the systematic review. We also reviewed the reference lists of those publications, as well as the reference lists of the articles that fit the above inclusion criteria but were not original peer-reviewed articles, and 47 publications were included. A total of 166 publications were included, each comprising one study. See Fig. 2 for more information.

PRISMA flowchart
The main characteristics of the included publications are described in Table 1. In total, 69 studies were published between 2017 and 2019, comprising 42% of all studies. Most studies (77%) had an explanatory aim, only 8% of studies (14 of 166) were descriptive, and the rest of the studies were exploratory. In total, 128 publications (77%) had a quantitative design, and the rest were qualitative or mixed-methods studies. The majority of studies used a quantitative analysis based on secondary data/patient records, corresponding to 116 publications (70%). Most studies (100) focused on both facilitators/inhibitors and relevant outcomes (60%), while 23 studies focused only on relevant outcomes (14%), and 43 studies only outlined facilitating/inhibiting factors (26%). Additionally, 60 quantitative and seven qualitative studies have a strong quality (as described in section 2, Methods), corresponding to 36% and 4% of all included publications, respectively.
3.1 Characteristics of the Value-Based Payment (VBP) Models
In Table 2, the characteristics of the VBP models described in the studies are reported. In total, 108 publications study shared savings VBP models, corresponding to 65% all included studies. Pay-for-performance and bundled payment models were studied in 54 and 13, out of 166 studies, respectively. Bundled payment models are not divided in providing payment for the full or partial care of the patient, since that level of detail is not present in the included papers. Most often, providers have not been involved in the design of the model [132 publications (80%)], and the incentivized entity is a group of providers [121 publications (73%)]. Regarding motivation, 13 publications (8%) refer to VBP as a tool to improve financial performance (efficiency), while in 30 publications (18%), the motivation is to improve the quality of care. However, 63% of studies refer to both financial performance and improving quality (104 studies). In addition, most publications (65%) report programs with a duration of 3 years or longer, corresponding to 108 of the 166 included publications.
3.2 Effect Direction
Among the 73 publications that report clinical outcomes, 45 (62%) report a mostly positive relation between the VBP model and the studied clinical outcomes (see Table 3). Either a mixed or no effect is reported in 28 publications, corresponding to 39%. In total, seven publications cover patient-reported outcomes/experiences, five of those presenting no effect (71%). Organization-reported outcomes or experiences are studied in 34 publications. In 11 and 17 of those publications a mostly positive and mostly negative effect, respectively, are presented. This corresponds to 32% and 50% of all publications that study this category of outcome measures, respectively. Cost outcomes is the fourth outcome group studied. Most publications that report these outcomes present a mostly positive effect (27 publications (57%)), as opposed to only four publications (9%) reporting a mostly negative effect.
3.3 Cross-Tabulations
3.3.1 Cross-Tabulation of the Types of VBP Models and the Four Types of Outcomes
Table 4 presents a cross-tabulation between the different types of VBP models and the four types of outcome measures, along with the direction of the effect in those measures. We include examples of the outcome measures for each effect, per VBP model. For example, in articles describing bundled payments, none report positive or negative effects on clinical outcomes, one has a mixed effect (measuring length of hospital stay for example), and two find no effect on, for example, 90-day mortality.
There are only positive effects reported on cost outcomes when applying bundled payments models, for example total Medicare payments. Patient opinion on inequalities show no effect when applying these types of models, and no articles reveal positive, negative, or even mixed effects in PROMs. There are two articles showing positive effect in organization-related outcomes/experience (e.g., adoption/spread of care coordination activities). One article finds a negative effect on, for example, physician practices’ decisions to engage in the models, and two articles find mixed effects, with practice leaders’ exposing some barriers and facilitators of the models.
Among articles studying shared savings models, there are no articles with negative effects, and 28 show positive effects on clinical outcomes, such as preventable hospitalizations. Mixed and no effects are present in ten articles each, with ICU admissions being an example of a measure present in both types of effects. In measured cost outcomes, there are 21 articles studying shared savings models with a positive effect (e.g., on total spending). Only three articles have a negative effect on, for example, real savings rate. Five articles have a mixed effect, and eight articles have no effect. Spending on inpatient care and Medicare spending/cost growth are examples of cost outcome measures with mixed and no effect, respectively. There is one article that reports a negative effect on PROMs, and patient’s rating of the doctor is reported to have decreased with the implementation of a shared savings model. Two articles report no effect in that type of outcome measure, for example when measuring patient experience. In organization-related outcomes/experience, a mixed and no effect is reported in one article each. Four articles find a positive effect on, for example, scores on nursing/doctor communication. A negative effect on organization-related outcomes/experience is described in eight articles, with one measure being providers’ rating of comfort, understanding and expectations about joining an ACO.
No articles reporting a negative effect on clinical outcomes when applying P4P are found. Two articles find a mixed effect, with an example of a measured clinical outcome being length of stay, and three articles describe no effect on this type of outcome measure (for example, risk of hospital admission). The great majority of articles find a positive effect on clinical outcomes, and one of the measures is risk of complications. Related to cost outcomes, three articles find a positive effect (e.g., operating margin) and two find no effect (e.g., spending performance). A negative and mixed effect is found in one article each, both giving expenditures as an example. No positive nor negative effects are found in articles reporting for PROMs when implementing P4P models. One article finds a mixed effect on, for example, patient’s thoughts towards P4P models. Three articles find no effect on this type of outcome measure, and patient’s reports on access to care is one of the studied measures. No articles reporting no effect on organization-related outcomes/experience are found. Positive and mixed effects are described in six and five articles, respectively. Provider engagement and awareness/experiences about the model are examples found for each effect, respectively. Ten articles find a negative effect when measuring the impact of P4P models in organization-related outcomes/experience. Physician’s opinion towards incentives is one of the measures with this effect.
3.3.2 Cross-Tabulation Between Types of Outcome Measures, VBP Models and Key Facilitators and Barriers
In Table 5 a cross-tabulation between the types of outcome measures and the different VBP models described in the included publications is presented. In this table, we include the key facilitators, defined as the top three in frequency in which they are described in the articles (Table 6), of studies on a certain type of outcome measure for a certain type of VBP model. The same procedure is adopted for inhibitors (Table 7). For example, there are two articles that describe facilitating factors where clinical outcomes are measured when adopting a bundled payment model. Diversity in the composition of professionals involved is one of the key facilitators outlined in one of those two articles.
Two papers describe inhibiting factors for the same type of VBP model and the same type of outcome measure. In one article, one of the inhibitors described is the inadequate adjustment for differences in patient mix. The same papers that outline facilitators and inhibitors when studying clinical outcomes and bundled payments also measure cost outcomes for the same type of VBP model. Hence, the factors are the same. There are no papers about bundled payment models that describe facilitating factors on PROMs/PREMs, and only one describes inhibitors. The possibility of opportunistic behavior is one of the factors outlined in that article. Four papers describe facilitating factors for bundled payment models when measuring organization-related outcomes/experience. Transparency and communication among involved stakeholders is the factor most frequently described (two articles). Five articles studying organization-related outcomes/experience when adopting bundled payment models outline inhibiting factors (e.g., lack of trust among involved stakeholders, present in two articles).
In articles reporting shared savings models, 31 study clinical outcomes and report facilitating factors. For the same type of models, 28 articles outline cost outcomes and facilitating factors. In both outcome measures, one of the most frequently mentioned facilitators is “Rotating quality measures, with physicians involved, also rewarding improvement and linked with savings and new clinical protocols,” mentioned in ten articles when studying clinical outcomes and five articles when studying cost outcomes. 22 and 19 papers outline inhibitors, where shared savings models have an effect on clinical and cost outcome measures, respectively. For both these types of outcome measures, an excessive amount of time that improvements take to manifest is the inhibitor most frequently described (ten out of 22 articles and six out of 19 articles for clinical and cost outcome measures, respectively). There are three papers describing facilitating factors when studying the impact of shared savings models on PROMs/PREMs. The most frequent factor is outlined in two articles, and it refers to "rotating quality measures, with physicians involved, also rewarding improvement, and linked with savings and new clinical protocols.” A low initial quality of care of organizations is the only inhibitor outlined (in one paper) for the same type of VBP model and outcome measure. Regarding organization-related outcomes/experience, 11 papers outline facilitators, and 12 papers outline inhibitors. Transparency and communication among involved stakeholders is the most frequent factor mentioned, with the presence of it being a facilitator mentioned in five articles and the lack of it being mentioned in four articles.
In the final type of VBP models, pay-for-performance, there are ten papers mentioning facilitators when studying clinical outcomes and four papers when studying cost outcomes. In both types of outcome measures, "realistic and achievable targets, and clear benchmarks/adequate and frequent incentives to achieve targets (risk-adjusted)” is the most frequent facilitating factor, mentioned in eight articles with clinical outcome measures and in the four articles with cost measures. For these same outcome measures, the most frequently mentioned inhibitor is “inadequate adjustment for differences in patient mix,” mentioned in five out of the nine articles related to clinical outcomes and in two out of the four articles related to cost outcomes. There are no facilitators associated with articles that study pay-for-performance models’ impact on PROMs/PREMs. Three papers mention inhibitors and all factors are only mentioned once (e.g., the risk that GPs may focus only on the indicators at the expense of other types of care). “Transparency and communication among involved stakeholders” is the most frequently mentioned facilitator (six out of 11 articles), and “higher workload of staff due to the program and payment delays/past due” is the most frequently mentioned inhibitor (six out of 17 papers) in articles studying the impact of pay-for-performance models on organization-related outcomes/experience.
4 Discussion
In this systematic literature review, we analyze the impacts of VBP models applied in NOC and transmural care, and provide an overview of the differences in their effects, as well as the facilitating and inhibiting factors that may explain those differences. The findings from both cross-tabulations arise from a mix of papers evaluation with weak, moderate, and good quality. Articles with weaker quality are not excluded but triangulated with papers of better quality. No singular finding arises from the sole evaluation of papers with weak quality. Therefore, all conclusions taken from the findings are corroborated with papers of moderate and/or high quality. Our review confirms the increased interest in the adoption of new ways of paying for care, such as VBP models, which are more aligned with innovative, patient-centered care, improving outcomes and avoiding unnecessary costs [31]. This growing interest may stem from growing discontent and problems of frequently used remuneration methods. There is a considerable number of studies included that have either mixed or no effect. This is found for all types of outcome measures except for organization-related outcomes/experiences. However, our results find a substantial number of studies with an overall positive effect for both clinical and cost outcomes across all VBP models studied. Organization-related outcomes/experiences have predominantly negative effects in shared savings and pay-for-performance models. In the small number of papers that studied PROMs/PREMs, most show no effect. Transparency and communication, inadequate targets/insufficient incentives, and lack of trust among stakeholders are the only three factors, one facilitating and two inhibiting, transversal to all VBP models. Additionally, measures, incentives and targets are key facilitators if adequate, and key inhibitors if lacking, namely for P4P and shared savings models.
4.1 Positive Effects
As discussed above, our results suggest an overall positive effect on both clinical and cost outcomes across all VBP models. Related to these positive results are the facilitating factors in the design and development of the models, in the establishment of their objectives and strategies, namely adequate targets/benchmarks/incentives, and rotating quality measures. These components are consistent with the existing literature, which lists them as key elements for the well-functioning of VBP models [3, 6, 20, 32] and offer a possible explanation for the positive effects found in our study. The only exception is the impact of bundled payment models on clinical outcomes, which do not show positive results in our study. However, there are also no reported negative effects, and we were able to include only three studies. Therefore, we cannot provide any definite conclusion regarding this difference, and further research is necessary to study any possible differences in the impact bundled payments may have on clinical outcomes. There does not seem to exist a difference in the clinical outcomes measured between different VBP models. Additionally, there also does not seem to exist a relation between clinical outcomes and a specific effect direction. Mortality rate, readmission rate, and length of stay are some of the most frequently measured clinical outcomes and these do not appear to be associated with a certain model or effect direction. Overall, these positive results may be used as a strong argument for the overall success in the implementation of VBP models since two of its pillars to determine success are the increase in quality of care and the reduction of costs.
4.2 Negative Effects
The effects on organization-reported outcomes/experience are, in their majority, negative, with large differences between payment models. Results of our study suggest that bundled payments have a higher acceptance among stakeholders compared to shared savings and P4P models. Evidence suggests that in shared savings models, all providers are affected, and the scope of change is much greater. Therefore, they call for more funding, the implementation of a more complex IT structure, a new management organization, and more extensive care coordination and management processes [33]. A need for a “paradigm shift” in shared savings models in both financial management and delivery of care is mentioned as well. For example, the financial incentives of the shared savings are to reduce the use of hospital services, while the hospital aims to increase the use of those services, and these differences need to be settled [34]. Such a shift is not necessarily needed for bundled payment models since the financial incentives of this VBP model are in line with those of the hospital [34]. This is partially justified by the positive effect, described in included studies, on the adoption and spread of care coordination activities when applying such payment models. Eijkenaar states that designing a fair and effective P4P model is complex, even if the idea behind it is simple [35], which may help justify the negative effects on organization-reported outcomes/experiences. Further research is still necessary to compare any potential differences that implementation of different types of VBP models may have on provider experience.
Still, regarding organization-related outcomes/experience, we find in our study several negative effects regarding provider’s awareness, expectations, and overall opinion towards the different VBP models. It is also reported that physician turnover increases and that there are negative perceptions towards the distribution of the bonus. These negative effects are found in all types of VBP models. Existing studies also find physicians reporting limited awareness and perceptions about the implemented models [36, 37]. Other studies suggest that physicians are not totally convinced that this model delivers effective and cost-effective care [38, 39]. A study surveying medical doctors finds that 61% of the participants support the opinion that VBHC will damage their practice and that payment models like shared savings and bundled payment are “over-hyped” [40]. Another study finds that physicians are afraid of losing autonomy when transitioning from FFS to VBHC [41]. Reports also state that employers are much more optimistic than physicians that bundled payment and shared savings models will help contain costs, also adding that very few physicians believe those models are the answer [42]. This, in turn, leads to low uptake of VBP models by physicians. In our study, we also find very few payment models with physician involvement in the design of VBP models (4%). This may give an idea of physician disconnection with the model. Literature states that a lack of physician involvement takes away ownership and fosters doubt and uncertainty over VBP models, as well as decreases motivation [3, 43], which can help corroborate the prominent negative results found in most VBP models about physician experience.
4.3 Mixed/No Effects
Our results show a substantial number of studies with mixed/no effects, especially on clinical outcomes. This may be due to the complexity and/or novelty of the models [32], with some elements of VBHC not yet fully studied and proven to have a positive effect. The evidence suggests that different diseases have different requirements, and in case the same model (with the same elements) is implemented transversally, there may be different results. This in part depends on the complexity of illnesses because some may require a more complex change process [32]. The negative results in clinical and cost outcomes, even if few, can also be explained by these differences in requirements and complexities. Additionally, the literature also suggests that it takes time for organizations to make the necessary changes needed in care delivery for VBP models to take effect or just for results to develop [6, 32]. The excessive amount of time is also an important inhibiting factor for both cost and clinical outcomes, which may explain the mixed or lack of effects found throughout all types of VBP models. In one of the articles included in our study [44], a shared savings model was implemented, and the time it takes for the model to have an effect on both savings and hospitalizations is mentioned as a reason for the lack of effect on these clinical and cost measures.
When referring to PROMs/PREMs, most studies show no change when adopting VBP models (not better nor worse off with the models). These findings go against the current literature, which finds a generally positive effect on patient satisfaction and experience [45,46,47,48]. Additional research on the topic does not find negative patient experiences when adopting VBP models. One possible explanation is the lack of studies that measure the impact of this type of outcome. However, when investigating the actual measures, we realize they are mostly about inequalities and discrimination. In the existing literature, there are some concerns about adverse selection of patients with co-morbidities, elderly, and/or with more severe illnesses [3]. There are mixed results regarding patient selection when implementing VBP models. Some studies find higher rates of “cherry picking” [49, 50], while others find no effect [51, 52]. Our study shows that the implementation of VBP models has no patient-reported effect on risk selection or inequalities. It is, however, necessary to have a careful risk adjustment in the design of the model, to avoid adverse selection, which is corroborated by the considerable amount of facilitating factors found in our included articles regarding the use of risk adjustment strategies.
4.4 Transversal Facilitating and Inhibiting Factors
Transparency and communication among involved stakeholders are found to be key facilitating factors, transversal to all models. Additionally, a lack of trust is found to be an inhibitor important to all VBP models, together with inadequate targets/insufficient incentives. In order to attain the objectives outlined by each model, motivation, engagement, and trust of stakeholders, as well as a culture of transparency and communication, are key success factor [37, 53,54,55]. By collaborating, care coordination is promoted, where stakeholders fully understand the model and are aligned with the established incentives, contributing to the well-functioning quality of the model [14, 56, 57]. Measures, incentives, and targets can both inhibit and facilitate (if adequate or inadequate/lacking) P4P and shared savings models, but do not seem to be of importance to facilitate the functioning of bundled payments. This may be because of the lack of actual incentives under the bundled payments since this scheme is based on a single payment. Also, outcome-related payment models rely on measurable indicators of performance. However, our study demonstrates these components, if inadequate or insufficient, can inhibit the functioning of bundled payment models. This is corroborated by the evidence, which suggests for greater incentives in bundled payments, even without evidence to support it [32]. It would, therefore, be important to further research this hypothesis.
4.5 Complexity of the Program and Lack of Experience
In bundled payment and P4P models, one of the most frequent inhibitors found is the complexity in the structure of the program and lack of experience in implementing required mechanisms. Even though this inhibiting factor is not the most frequently stated in shared savings models, it is present. Whether a VBP model provides financial incentives to health workers or facilities based on the achievement of pre-specified performance targets, provides a bundled payment for full or partial care of patients, or makes the savings contingent on achieved targets, there is a need for change in several areas, such as behavioral, process, and infrastructure [58]. As stated above, P4P models are reported to be difficult to design in a fair and effective way [35]. At the same time, the evidence does suggest that shared savings models are very complex payment schemes [33, 34]. This underlines the results our study found on the complexity of the payment scheme and lack of experience is an important inhibiting factor.
4.6 Possibility of Opportunistic Behavior by Providers
Opportunistic behavior by providers is the only inhibiting factor frequently mentioned when bundled payment models are studied, and irrespective of the type of outcomes measured. In bundled payment models, the evidence points to a tendency to avoid high-risk patients or cases that could exceed the average payment [50, 59, 60]. Perhaps since shared savings and P4P models have incentives contingent on performance measures, can this opportunistic behavior be rendered less important. Another possibility may be risk adjustment strategies being less developed and effective in bundled payment models, and when a sum of money is given to the organization, it may be easier to simply undertreat or select relatively healthier patients. There seems to be a lack of existing literature comparing different types of VBP models in terms of opportunistic provider’s behavior. It should be noted that these are just observations, and no conclusions can be derived regarding any specific models.
4.7 Resources/Financial Aid Programs and Infrastructure/Information Technology System
Our study results show sufficient resources to finance a VBP model or participation in financial aid programs to be a facilitating factor for the success of both bundled payment and shared savings models. A sufficient infrastructure and advanced health information technology are also shown to be a facilitator in the same two types of VBP models. To corroborate the importance of either an infrastructure and system or the possibility of obtaining them, internally or externally, the absence of a system/limited data availability is found to be an important inhibiting factor for the functioning of these two types of models. Porter and Lee confirm the need to build an enabling information technology platform by describing it as one of the six core components for moving to a high-value care delivery system [1]. All three factors mentioned are not found to be of great importance for P4P models. As mentioned before, shared savings models require a “paradigm shift” [34], which indicates a need for resources to change infrastructure and the system. That same need is present in bundled payment models, as suggested by the complexity found in our study to inhibit its success. There is also a complexity found in P4P models, also corroborated by Eijkenaar [35]. However, we do not find infrastructure/information technology systems or the resources to attain them to be important factors for the success of P4P models. It may be that, even though the model is complex, it does not require such investments and shift since P4P models have a sole focus on targets and benchmarks, while bundled payment and shared savings models require a bigger focus on infrastructure and systems to achieve optimal coordination and hence save costs. However, this is not corroborated by existing literature, and future research is necessary to compare the complexity of the different types of VBP models, and therefore the requirements each has.
4.8 Limitations
Although our review is systematic and we demonstrated its quality by applying the PRISMA checklist, there are still some limitations to be acknowledged. The screening process is only partially cross-checked, and the reference check is only performed by the primary researcher. This could result in some degree of selection bias. Furthermore, because the review solely includes studies published in academic journals, publication bias cannot be ruled out. Also, what is more frequently studied becoming standard. Some of the publications that we include do not use a random sample to collect data, which means findings may not be generalizable. We also provide a thorough overview of facilitating and inhibiting factors but do not examine data on their significance. As a result, more research can be conducted, relying on expert consensus to determine which facilitators and barriers are most important. Additionally, even though conclusions are never taken solely based on articles of weak quality (triangulated with papers of better quality), more investigation can be carried out, in which papers considered of weak quality are excluded, and the overall results are compared to the results of this study. In our study, in the cross-tabulations, only the most frequently mentioned examples of outcome measures and the most frequent factors are considered, and conclusions are derived from those elements. There should be further research to better understand the different types of VBP models, either studying differences between models regarding a specific outcome measure or studying different outcome measures per model.
5 Conclusions
This systematic literature review shows differences in the effects between the different VBP models reported in relation to NOC and transmural care, as well as facilitating and inhibiting factors that may contribute to those differences. There is an overall positive effect on clinical and cost outcomes, such as readmission/mortality rates and expenditures, respectively. This can be used as one of the major arguments of the overall success of VBP models. The effects on organization-reported outcomes/experiences are, in their majority, negative. The evidence corroborated findings regarding providers’ lack of awareness, trust, and engagement with the model, which may be justified by their exclusion from the design of the models, decreasing their sense of ownership and, therefore, motivation. Further research is necessary to compare the different types of VBP models on provider experience. A sizable share of studies has either a mixed or no effect on clinical and cost outcomes, which can be explained by the considerable amount of time it takes for results to take effect when implementing VBP models. Patient-reported inequality and adverse selection show no change when implementing these models, which helps a body of literature with mixed results on the topic.
Collaboration is a key element of VBP, and increased coordination is a logical result of it. This is evidenced by our findings that factors related to objectives and strategies in the design and development of the VBP models, such as adequate incentives and quality measures, require care coordination among stakeholders, namely transparency, communication, engagement, and trust. These factors are also necessary to attain the models’ objectives, and their absence hinders the well-functioning of VBP models. Incentives, targets, benchmarks, and quality measures, if adequately designed, seem to be important facilitators and if lacking or inadequate, they are key inhibitors. More specifically, these are prominent facilitators and inhibitors for P4P and shared savings models, but not as prominent for bundled payments. The complexity of the scheme and lack of experience are prominent inhibitors in all VBP models, since all require changes in several areas, such as behavioral, process, and infrastructure.
References
Porter ME, Lee TH. The strategy that will fix health care. harvard business review website. 2022. https://hbr.org/2013/10/the-strategy-that-will-fix-health-care. Accessed 3 Mar 2022.
Porter ME. A strategy for healthcare reform–toward a value-based system. N Engl J Med. 2009;361(2):109–12. https://doi.org/10.1056/NEJMp0904131.
Conrad DA. The theory of value-based payment incentives and their application to health Care. Health Serv Res. 2015;50 Suppl 2(Suppl 2):2057–89. https://doi.org/10.1111/1475-6773.12408.
Transitioning to Value-Based Care While Reducing Risks. Revcycle Intelligence. https://revcycleintelligence.com/news/transitioning-to-value-based-care-while-reducing-risks. Accessed 21 April 2022.
Conrad DA, Vaughn M, Grembowski D, Marcus-Smith M. Implementing value-based payment reform: a conceptual framework and case examples. Med Care Res Rev. 2016;73(4):437–57. https://doi.org/10.1177/1077558715615774.
Werner RM, Emanuel EJ, Pham, HH, Navathe, AS. The future of value-based payment: a road map to 2030. 2021.
Cattel D, Eijkenaar F, Schut FT. Value-based provider payment: towards a theoretically preferred design. Health Econ Policy Law. 2020;15(1):94–112. https://doi.org/10.1017/s1744133118000397.
Petersen LA, Woodard LD, Urech T, Daw C, Sookanan S. Does pay-for-performance improve the quality of healthcare? Ann Intern Med. 2006;145(4):265–72. https://doi.org/10.7326/0003-4819-145-4-200608150-00006.
Robinson JC. Theory and practice in the design of physician payment incentives. Milbank Q. 2001;79(2):149–77. https://doi.org/10.1111/1468-0009.00202.
Valentijn P. What you need to know about value based payment models. https://www.essenburgh.com/en/what-you-need-to-know-about-value-based-payment-models/. Accessed 11 Oct 2022.
Rosenthal MB, Frank RG. What is the empirical basis for paying for quality in healthcare? Med Care Res Rev. 2006;63(2):135–57. https://doi.org/10.1177/1077558705285291.
Mehrotra A, Damberg CL, Sorbero ME, Teleki SS. Pay for performance in the hospital setting: what is the state of the evidence? Am J Med Qual Jan-Feb. 2009;24(1):19–28. https://doi.org/10.1177/1062860608326634.
Resnic FS, Welt FG. The public health hazards of risk avoidance associated with public reporting of risk-adjusted outcomes in coronary intervention. J Am Coll Cardiol. 2009;53(10):825–30. https://doi.org/10.1016/j.jacc.2008.11.034.
Erikson CE, Pittman P, LaFrance A, Chapman SA. Alternative payment models lead to strategic care coordination workforce investments. Nurs Outlook. 2017;65(6):737–45. https://doi.org/10.1016/j.outlook.2017.04.001.
Fernandez G, Narins CR, Bruckel J, Ayers B, Ling FS. Patient and physician perspectives on public reporting of mortality ratings for percutaneous coronary intervention in New York State. Circ Cardiovasc Qual Outcomes. 2017. https://doi.org/10.1161/circoutcomes.116.003511.
Rosenthal MB, Fernandopulle R, Song HR, Landon B. Paying for quality: providers’ incentives for quality improvement. Health Aff (Millwood). 2004;23(2):127–41. https://doi.org/10.1377/hlthaff.23.2.127.
Young GJ, White B, Burgess JF Jr, et al. Conceptual issues in the design and implementation of pay-for-quality programs. Am J Med Qual May-Jun. 2005;20(3):144–50. https://doi.org/10.1177/1062860605275222.
Iglesia EGA, Greenhawt M, Shaker MS. Achieving the Quadruple Aim to deliver value-based allergy care in an ever-evolving healthcare system. Ann Allergy Asthma Immunol. 2020;125(2):126–36. https://doi.org/10.1016/j.anai.2020.04.007.
Cattel D, Eijkenaar F. Value-based provider payment initiatives combining global payments with explicit quality incentives: a systematic review. Med Care Res Rev. 2020;77(6):511–37. https://doi.org/10.1177/1077558719856775.
Chee TT, Ryan AM, Wasfy JH, Borden WB. Current state of value-based purchasing programs. Circulation. 2016;133(22):2197–205. https://doi.org/10.1161/CIRCULATIONAHA.115.010268.
Eijkenaar F, Emmert M, Scheppach M, Schöffski O. Effects of pay for performance in healthcare: a systematic review of systematic reviews. Health Policy. 2013;110(2–3):115–30. https://doi.org/10.1016/j.healthpol.2013.01.008.
Weissman JS, Bailit M, D’Andrea G, Rosenthal MB. The design and application of shared savings programs: lessons from early adopters. Health Aff (Millwood). 2012;31(9):1959–68. https://doi.org/10.1377/hlthaff.2012.0383.
Leao DLL, Cremers H, van Veghel D, Pavlova M, Hafkamp F, Groot W. Facilitating and inhibiting factors in the design, implementation, and applicability of value-based payment models: a systematic literature review (Unpublished). 2022.
Carmone A, Kalaris K, Leydon N, et al. Developing a common understanding of networks of care through a scoping study. Health Syst Reform. 2020;6:e1810921. https://doi.org/10.1080/23288604.2020.1810921.
Provisions NBoHBoH. Transmural Somatic Healthcare (in Dutch). Zoetermeer: Council for Public Health and Health Care; 1995.
Porter ME. Redefining healthcare: creating value-based competition on results. Harvard Business School Press; 2006.
Project EPHP. Quality Assessment Tool for Quantitative Studies. 2022. https://www.ephpp.ca/quality-assessment-tool-for-quantitative-studies/. Accessed 10 April 2022.
Programme CCAS. CASP Checklists. 2022. https://casp-uk.net/casp-tools-checklists/. Accessed 10 April 2022.
Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–88. https://doi.org/10.1177/1049732305276687.
Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Q. 2004;82(4):581–629. https://doi.org/10.1111/j.0887-378X.2004.00325.x.
Crook HL, Saunders RS, Roiland R, Higgins A, McClellan MB. A decade of value-based payment: lessons learned and implications for the center for medicare and medicaid innovation, Part 2. Health affairs 2021. https://www.healthaffairs.org/do/10.1377/forefront.20210607.230763/full/. Accessed 9 June 2022.
Maddox KJ, Epstein, A. M. Using bundled payments to improve the patient experience. 2022. https://hbr.org/2018/10/using-bundled-payments-to-improve-the-patient-experience. Accessed 9 June 2022.
Henry J. How bundled payments and ACOs impact providers differently. 2022. https://www.healthcaredive.com/news/how-bundled-payments-and-acos-impact-providers-differently/400621/. Accessed 9 June 2022.
Pearce JP. Evaluating the medicare pilot programs: comparing ACOs and bundled payments. 2022. https://www.beckershospitalreview.com/hospital-physician-relationships/evaluating-the-medicare-pilot-programs-comparing-acos-and-bundled-payments.html. Accessed 9 June 2022.
Eijkenaar F. Key issues in the design of pay for performance programs. Eur J Health Econ. 2013;14(1):117–31. https://doi.org/10.1007/s10198-011-0347-6.
Markovitz AA, Ryan AM, Peterson TA, Rozier MD, Ayanian JZ, Hollingsworth JM. ACO awareness and perceptions among specialists versus primary care physicians: a survey of a large medicare shared savings program. J Gen Intern Med. 2022;37(2):492–4. https://doi.org/10.1007/s11606-020-06556-w.
D’iChiara J. Physicians Report 4 Factors of Value-Based Payment Success. 2022. https://revcycleintelligence.com/news/physicians-report-4-factors-of-value-based-payment-success. Accessed 9 June 2022
Schur CL, Sutton JP. Physicians in medicare acos offer mixed views of model for health care cost and quality. Health Aff (Millwood). 2017;36(4):649–54. https://doi.org/10.1377/hlthaff.2016.1427.
Kyeremanteng K, Robidoux R, D’Egidio G, Fernando SM, Neilipovitz D. An analysis of pay-for-performance schemes and their potential impacts on health systems and outcomes for patients. Crit Care Res Pract. 2019;2019:8943972–8943972. https://doi.org/10.1155/2019/8943972.
LaPointe J. 61% of Doctors Say Value-Based Care Will Damage Their Practice. 2022. https://revcycleintelligence.com/news/61-of-doctors-say-value-based-care-will-damage-their-practice. Accessed 9 June 2022.
Chernew ME. Why physicians should like bundled payment. Health Serv Res. 2011;46(6pt1):1693–7. https://doi.org/10.1111/j.1475-6773.2011.01348.x.
Niebel K. Leavitt Partners Releases “The State of Health Care Today” White Paper. 2022. https://leavittpartners.com/press/leavitt-partners-releases-state-health-care-today-physicians-consumers-employers-view-health-care-costs-outcomes-reform-efforts-white-paper/. Accessed 9 Jun 2022.
Manongi R, Mushi D, Kessy J, Salome S, Njau B. Does training on performance based financing make a difference in performance and quality of healthcare delivery? Health care provider’s perspective in Rungwe Tanzania. BMC Health Serv Res. 2014;14(1):154. https://doi.org/10.1186/1472-6963-14-154.
Lam MB, Zheng J, Orav EJ, Jha AK. Early accountable care organization results in end-of-life spending among cancer patients. J Natl Cancer Inst. 2019;111(12):1307–13. https://doi.org/10.1093/jnci/djz033.
Trombley MJ, McClellan SR, Kahvecioglu DC, et al. Association of medicare’s bundled payments for care improvement initiative with patient-reported outcomes. Health Serv Res. 2019;54(4):793–804. https://doi.org/10.1111/1475-6773.13159.
Graham JM, Cowling DW, Zhang H. Findings from a commercial ACO patient experience survey. J Patient Exp. 2021;8:23743735211007830–23743735211007830. https://doi.org/10.1177/23743735211007833.
Ivey SL, Shortell SM, Rodriguez HP, Wang YE. Patient engagement in ACO practices and patient-reported outcomes among adults with co-occurring chronic disease and mental health conditions. Med Care. 2018;56(7):551–6. https://doi.org/10.1097/MLR.0000000000000927.
Mcaskill R. Patient Satisfaction Grows With Accountable Care Organizations. 2022. https://revcycleintelligence.com/news/patient-satisfaction-grows-accountable-care-organizations. Accessed 9 June 2022.
Borah BJ, Rock MG, Wood DL, Roellinger DL, Johnson MG, Naessens JM. Association between value-based purchasing score and hospital characteristics. BMC Health Serv Res. 2012;12(1):464. https://doi.org/10.1186/1472-6963-12-464.
Bernstein DN, Reitblat C, van de Graaf VA, et al. Is there an association between bundled payments and “Cherry Picking” and “Lemon Dropping” in orthopaedic surgery? A systematic review. Clin Orthop Relat Res. 2021;479(11):2430–43. https://doi.org/10.1097/corr.0000000000001792.
Plate JF, Ryan SP, Black CS, et al. No changes in patient selection and value-based metrics for total hip arthroplasty after comprehensive care for joint replacement bundle implementation at a single center. J Arthroplasty. 2019;34(8):1581–4. https://doi.org/10.1016/j.arth.2019.05.016.
Humbyrd CJ, Wu SS, Trujillo AJ, Socal MP, Anderson GF. Patient selection after mandatory bundled payments for hip and knee replacement: limited evidence of lemon-dropping or Cherry-Picking. J Bone Joint Surg Am. 2020;102(4):325–31. https://doi.org/10.2106/jbjs.19.00756.
Wise S, Hall J, Haywood P, Khana N, Hossain L, van Gool K. Paying for value: options for value-based payment reform in Australia. Aust Health Rev. 2022;46(2):129–33. https://doi.org/10.1071/ah21115.
Richard C, Urick BY, Pathak S, Jackson J, Livet M. Performance-based pharmacy payment models: key components and critical implementation considerations for successful uptake and integration. J Manag Care Spec Pharm. 2021;27(11):1568–78. https://doi.org/10.18553/jmcp.2021.27.11.1568.
Steenhuis S, Struijs J, Koolman X, Ket JEVDH. Unraveling the complexity in the design and implementation of bundled payments: a scoping review of key elements from a Payer’s perspective. Milbank Q. 2020;98(1):197–222. https://doi.org/10.1111/1468-0009.12438.
Burns LR, Pauly MV. Accountable care organizations may have difficulty avoiding the failures of integrated delivery networks of the 1990s. Health Aff (Millwood). 2012;31(11):2407–16. https://doi.org/10.1377/hlthaff.2011.0675.
Schrag J, Ramiah K, Lausch KB, Nolty J, Proser M, Mead H, Masselink L, Seyoum S, Brantley E. Collaboration under value based payment lessons learned. 2017. https://essentialhospitals.org/wp-content/uploads/2019/03/Collaboration-Under-Value-Based-Payment-Lessons-Learned.pdf. Accessed 6 June 2022.
McHugh M, Joshi M. Improving evaluations of value-based purchasing programs. Health Serv Res. 2010;45(5 Pt 2):1559–69. https://doi.org/10.1111/j.1475-6773.2010.01147.x.
Squires DBD. The Promise and Pitfalls of Bundled Payments. 2022. https://www.commonwealthfund.org/blog/2016/promise-and-pitfalls-bundled-payments. Accessed 14 Oct 2022.
Pros and Cons of Various Payment Models and their Effect on Practices. 2022. https://www.medicalbillersandcoders.com/articles/practice-administration/pros-and-cons-of-various-payment-models-and-their-effect-on-practices.html. Accessed 14 Oct 2022.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Registration and Protocol
This review is a follow-up study of another review that was registered in PROSPERO, the International prospective register of systematic reviews (ID: CRD42021259630).
Data Sharing
All data regarding the included articles are available in the Online Supplementary Material, under “Supplementary File.”
Ethics Approval
No ethics approval is necessary for this study since we studied literature and there was no direct impact on patients.
Conflicts of Interest
No potential conflicts of interest to report.
Funding
This study was funded by the Netherlands Organization for Health Research and Development (ZonMw), under the program “Outcome Based Organization and Funding of Medical Specialist Care,” with project number 516008002. The study sponsor was not involved in the study design, data collection, analysis, and interpretation, writing of the paper, or in the decision to submit the paper for publication.
Consent to Participate
Not applicable.
Consent for Publication (from patients/participants)
Not applicable.
Availability of Data and Material
All data generated or analysed during this study are included in this published article [and its supplementary information files].
Code Availability
Not applicable.
Authors’ Contributions
DVV and HPC conceived the study. DLLL performed the literature search, screening of abstracts/full-text, and data extraction. MP contributed to the screening of the abstracts/full-text. The synthesis of results was carried out by DLLL, with input from all authors. The first draft of the manuscript was written by DLLL. All authors worked on every version of the manuscript and read and approved the final version.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Leao, D.L.L., Cremers, HP., van Veghel, D. et al. The Impact of Value-Based Payment Models for Networks of Care and Transmural Care: A Systematic Literature Review. Appl Health Econ Health Policy 21, 441–466 (2023). https://doi.org/10.1007/s40258-023-00790-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40258-023-00790-z