
Abstract
Introduction
In recent years, as one of the drugs for the treatment of acute ischemic stroke (AIS), the clinical application of tenecteplase is still controversial. Therefore, we aimed to evaluate the safety and efficacy of tenecteplase versus alteplase to guide clinical practice.
Methods
A search of PubMed, MEDLINE, EMBASE, Cochrane Library, and Web of Science databases until February 15, 2023 was conducted to identify eligible articles. The quality of the included studies was assessed using the Cochrane Risk of Bias tool. RevMan 5.3 and Stata 17 were used to perform the meta-analysis and detect publication bias, and risk ratios (RRs) with 95% confidence intervals (95% CIs) were reported for each outcome measure.
Results
A total of 1326 records were retrieved in this meta-analysis. As a result of the limited reports on tenecteplase in patients with AIS and the lack of high-quality randomized controlled trials (RCTs), and considering the impact of publication bias, we did not include any of these studies published before 2015. Ultimately we included 16 RCTs with a total of 7508 patients, including 3940 patients treated with alteplase and 3568 patients treated with tenecteplase. Tenecteplase was associated with better early neurological improvement (RR 0.10; 95% CI 0.00–0.19; P = 0.04), recanalization of blood vessels (RR 0.24; 95% CI 0.07–0.40; P = 0.01), and 90-day excellent neurological recovery (RR 0.12; 95% CI 0.01–0.24; P = 0.04). In addition, there were no significant differences in other efficacy and safety outcomes between the two groups. The funnel plot and Begg’s as well as Egger’s tests showed no significant publication bias.
Conclusions
This meta-analysis showed that tenecteplase was not inferior to alteplase in early thrombolytic therapy in patients with AIS, and was even better than alteplase on some efficacy outcomes with no significant differences in safety. However, as a result of some inherent limitations of this study, more high-quality prospective clinical studies are needed to confirm these results.
Plain Language Summary
In recent years, there has been controversy surrounding the use of tenecteplase, a drug for treating acute ischemic stroke (AIS). To help doctors make better decisions, we compared the safety and effectiveness of tenecteplase with another drug called alteplase. We looked at various research articles from PubMed, MEDLINE, EMBASE, Cochrane Library, and Web of Science databases until February 15, 2023. After careful analysis, we found 16 relevant studies with a total of 7508 patients, including those treated with alteplase and tenecteplase. Our findings showed that tenecteplase was as effective as alteplase in providing early thrombolytic therapy for patients with AIS. In fact, tenecteplase even showed better results in some aspects of treatment, without compromising safety. However, we acknowledge some limitations in our study and recommend more high-quality clinical studies to validate these results.
Similar content being viewed by others

This meta-analysis evaluated the clinical efficacy of tenecteplase and alteplase in the treatment of AIS. |
Tenecteplase is more effective than alteplase in patients with AIS. |
There was no difference in safety between tenecteplase and alteplase in patients with AIS. |
Further high-quality RCTS are needed to confirm the superiority of tenecteplase over alteplase in the treatment of AIS. |
Introduction
Stroke is a serious global health problem. According to the World Health Organization, it is estimated that 16.5 million people suffer from stroke and 5.7 million people die as a result of stroke every year, accounting for 11.5% of the total number of deaths in the world [1]. The incidence of stroke is higher in developed countries than in developing countries, where stroke is the most common cause of death, but it is increasing faster in developing countries than in developed countries [2]. Acute ischemic stroke (AIS) is the most common type of stroke worldwide and approximately 700,000 people experience AIS each year in the USA, accounting for 85% of all stroke cases [3]. Venous thrombolysis treatment within the first hours after the onset of stroke can be very good at helping patients with early reperfusion, through intravenous thrombolytic drugs, promote the dissolution of thrombus, restore blood flow, reduce neuronal cell death, and thus reduce the nerve function defect. Thrombolytic agents can be rapidly delivered to the brain by intravascular infusion to dissolve the thrombus and restore blood flow [4].
Alteplase is a glycoprotein containing 526 amino acids and can promote the activation of the fibrinolytic system in vivo. It is mainly used in acute myocardial infarction, pulmonary embolism, AIS, and other vascular diseases. Owing to the selective activation of plasminogen by alteplase, bleeding complications are rare [5]. Alteplase is the only thrombolytic drug approved by the US Food and Drug Administration (FDA) for the treatment of AIS [6]. Although it significantly increases the likelihood of functional recovery, the fibrinolysis limitation potency of alteplase results in recanalization in less than 50% of patients, and among these patients, only about 50% have the desired effect within 2 h of administration [7]. In addition, alteplase has disadvantages related to its short half-life, incomplete recanalization, high risk of intracranial hemorrhage (ICH), and long continuous infusion time, which limit its efficacy [8, 9].
Tenecteplase is a variant of alteplase, which has a longer half-life, a higher binding specificity to fibrin, a lower effect on systemic fibrinolytic activity, and a lower consumption of plasma α2-antiplasmin. The thrombolytic mechanism of tenecteplase is similar to that of alteplase, but studies on the exact efficacy of tenecteplase and alteplase are inconclusive [10]. In patients with AIS, alteplase at 0.9 mg/kg resulted in severe disruption of the fibrinolytic system, but tenecteplase at 0.25 mg/kg did not [11]. In a study of alteplase versus tenecteplase thrombolytic therapy for stroke, alteplase reduced the probability of cerebral hemorrhage consistent with tenecteplase, but tenecteplase caused significantly less destruction of coagulation and fibrinolysis systems [12]. In animal models, tenecteplase resulted in a significantly shorter reperfusion time and reduced reventilation and thrombus burden compared with alteplase [13]. In the acute phase of stroke, the American Heart Association/American Stroke Association guidelines (2019) recommended that the tenecteplase could replace the alteplase in some cases. For example, in patients who do not have contraindications to intravenous thrombolysis and who are candidates for mechanical thrombectomy, it may be reasonable to choose tenecteplase (administered as a single bolus of 0.25 mg/kg of body weight to a maximum dose of 25 mg) over intravenous administration of alteplase. Tenecteplase may also be considered a replacement for alteplase in patients with mild neurologic dysfunction without intracranial large-vessel occlusion [14]. Tenecteplase is administered as a single bolus, making it an attractive alternative to alteplase for AIS treatment.
In recent years, prospective randomized controlled trials (RCTs) comparing tenecteplase with alteplase for the treatment of AIS have gradually increased in number. Although several RCTs have been published recently to support the superiority of tenecteplase over alteplase, generalizable results are still lacking owing to different patient population characteristics, dose variability, and different clinical endpoints and assessment measures. The efficacy of intravenous thrombolysis with tenecteplase in patients with AIS remains controversial. There are some evaluations of tenecteplase and alteplase in the treatment of AIS, e.g., a systematic review and meta-analysis by Rehman et al. [15], which mainly explores different doses, and Rose et al. [16], which focuses on the risk of complications associated with treatment with the two drugs. In addition, there are some network meta-analyses [17, 18], but these include not only RCTs but also some other types of clinical studies, which will increase the publication bias of the article and thus have a certain impact on the accuracy of the results. At the same time, some meta-analyses published earlier in 2022 were limited by small sample sizes and the inclusion of observational studies, which were susceptible to information bias and confounding factors, decreasing the reliability of the results. However, this study included the most recent RCTs in the last 3 years, aimed to summarize the clinical studies of intravenously administered tenecteplase for AIS published in PubMed and other major English databases, and to perform a meta-analysis on the efficacy of intravenously administered tenecteplase for AIS by comparing tenecteplase with alteplase so as to provide further evidence for the safety and efficacy of tenecteplase.
Methods
Protocol Registration
This systematic review and meta-analysis were conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) [19] and the Cochrane Handbook for Systematic Reviews and Meta-analyses, with predefined evaluation and data extraction protocols [20]. This study has been registered for publication in the international prospective Systematic Review PROSPERO, registration ID CRD42023404368. This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Literature Retrieval Strategy
Clinical studies comparing tenecteplase and alteplase in patients with AIS have been conducted. We searched the PubMed, MEDLINE, EMBASE, Cochrane Library, and Web of Science databases from each database’s start date through to our search date (February 15, 2023), with the language of publication restricted to English. On the basis of each database, different combinations of possible keywords and/or Medical Subject Headings terms (MeSH) were used. Keywords and MeSH terms included (“stroke” OR “cerebral stroke” OR “cerebral infarction” OR “cerebrovascular disease” OR “cerebral ischemia” OR “transient ischemic attack” OR “cerebrovascular disorders” OR “cerebrovascular accident” OR “brain ischemia” OR “brain vascular accident” OR “acute stroke” OR “brain infarction”) AND (“tenecteplase” OR “TNK-tPA” OR “TNK” OR “TNKase” OR “Metalyse” OR “rhTNK-tPA”) AND (“alteplase” OR “rt-PA” OR “tissue plasminogen activator” OR “plasminogen activator tissue type”) AND (“randomized controlled trials” OR “randomised controlled trials” OR “RCT” OR “controlled clinical trial”), etc. Additionally, we manually screened the reference lists of previous meta-analyses and included trials to identify any further relevant studies.
Inclusion and Exclusion Criteria
The inclusion and exclusion criteria were determined before the literature search. The inclusion criteria for this meta-analysis included (1) clinical studies formally published in peer-reviewed English journals; (2) Patients with AIS within 4.5 h of onset and arterial occlusion confirmed by head CT angiography (internal carotid artery, M1 segment and M2 segment of middle cerebral artery, basilar artery, anterior cerebral artery, carotid artery, middle cerebral artery, and posterior cerebral artery), with National Institutes of Health Stroke Scale (NIHSS) scores ≥ 1 upon neurological assessment. In addition, the patient must have been living independently before the stroke and provided consent for intravenous thrombolysis; (3) The intervention group received tenecteplase, and the control group received alteplase. The subjects had not used any thrombolytic drugs before enrollment; (4) The original literature had any one of the following outcome measures: excellent neurological recovery at 90 days (modified Rankin scale [mRS] score ≤ 1), good neurological recovery at 90 days (mRS score ≤ 2), early neurological improvement indicated by a decrease in NIHSS score of at least 8 points or an NIHSS score of 0–1 points after 24- to 48-h of thrombolysis, recanalization of blood vessels (complete or partial recanalization of the occluded vessel at 24 h, return of blood flow to more than 50% of the original infarct area, or no retrievable thrombus in the offending vessel at the time of the first angiographic assessment after thrombolysis), poor neurological recovery at 90 days (mR score of 4–6), all-cause mortality, any ICH, symptomatic ICH, and any parenchymal hematoma. Furthermore, the criteria for judging the outcome measures should be rigorously described.
The exclusion criteria for this meta-analysis were as follows: (1) follow-up time of no more than 90 days; (2) incomplete clinical trials; (3) non-English studies; (4) basic experimental research, case reports, conference abstracts, and reviews; and (5) incomplete data and repeated publications.
Literature Screening and Data Extraction
Two researchers independently read and screened the literature according to the inclusion and exclusion criteria above. If there was any disagreement, it was decided by a third researcher, and the three researchers discussed the decision together. At the same time, the data of the included studies were extracted and checked by a third researcher. The content extracted from each study included the title, publication year, author(s), country, number of subjects, study design, recruitment duration, intervention, time window of thrombolysis, and outcome measures.
Risk of Bias and Certainty in Evidence
The quality evaluation was based on the evaluation criteria of the quality of randomized controlled studies in the Cochrane Systematic Review Manual version 5.1 [21], including six items: the method of random assignment, hiding of the randomized scheme, blinding method, integrity of the resulting data, selective reporting of the study results, and other sources of bias. Each entry was judged as low, uncertain, or high risk of bias. Two independent reviewers evaluated the risk of bias for randomized controlled trial in each study. A consensus was reached through discussion and agreement if that there were any differences. RevMan 5.3 software was used to visualize the judgment results of each included study.
Statistical Analysis
RevMan 5.3 software provided by the Cochrane Collaboration and Stata 17 software were used to analyze the extracted data. For dichotomous variables, risk ratios (RRs) and their 95% confidence intervals (CIs) were pooled, and P values less than 0.05 were considered statistically significant. The I2 value was used to analyze the heterogeneity of each study. If I2 ≤ 50%, the heterogeneity among the results of each study was small, and a fixed-effect model was used [22]. If I2 > 50%, there was significant heterogeneity among the results of each study, and the random-effects model was used. Sensitivity analysis was performed by replacing the fixed-effects model with the random-effects model. A funnel plot was used to test the bias in the results of the meta-analysis. If the results were biased, an asymmetric funnel plot would appear; the more obvious the asymmetry, the greater the degree of bias [23]. For the accuracy of the study, Egger’s weighted linear regression test and Begg’s rank correlation test were also conducted to further evaluate whether publication bias existed in the included studies [24].
Results
Literature Search Results and Quality Evaluation
The meta-analysis initially retrieved a total of 1326 records. After we reviewed these records, 1310 records were excluded, mainly because they were case reports or review articles and the type of study did not meet our inclusion criteria. Finally, only 16 studies were included in our meta-analysis. The article retrieval process is illustrated in Fig. 1. The final studies included 7508 patients, including 3568 in the tenecteplase group and 3940 in the alteplase group. Most of the included studies were conducted in Europe and Oceania, with 14 trials having a time window of thrombolysis of 4.5 h and two trials with a time window of 3 h. Information on all included studies is presented in Table 1. The results of the Cochrane risk of bias assessment for all 16 included studies using RevMan 5.3 software are shown in Fig. 2.

PRISMA flowchart of the screening process. *Consider, if feasible to do so, reporting the number of records identified from each database or registry searched (rather than the total number across all databases/registries). **If automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools

Risk of bias assessment (study level): a Plot of the bias risk item judgment for each study. b Summary table of risk of bias items for all studies
Efficacy Outcomes
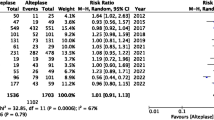
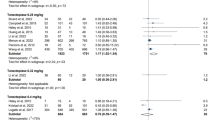
The nine most representative outcome indicators were selected, including four efficacy outcome indicators and five safety outcome indicators. Of the four efficacy outcome measures, seven studies using early neurological improvement or its variants provided sufficient data for the meta-analysis. Meta-analysis results showed that patient-reported early neurologic improvement was significantly greater with intravenously administered tenecteplase than with alteplase (RR 0.10; 95% CI 0.00–0.19; P = 0.04), as shown in Fig. 3a. Seven studies using recanalization of blood vessels or its variants provided sufficient data for meta-analysis. The results showed that patients receiving intravenously administered tenecteplase had better patient-reported recanalization of blood vessels than those receiving alteplase (RR 0.24; 95% CI 0.07–0.40; P = 0.01; Fig. 3b). Ten studies used 90-day excellent neurological recovery or its variants, providing sufficient data for meta-analysis. The results of the meta-analysis showed that patients receiving intravenously administered tenecteplase reported a more favorable neurologic recovery at 90 days compared with alteplase (RR 0.12; 95% CI 0.01–0.24; P = 0.04; Fig. 3c). The results of the meta-analysis indicated that the efficacy of intravenously administered alteplase was similar to that of tenecteplase, but the difference was not statistically significant (RR 0.03; 95% CI − 0.01 to 0.08; P = 0.14), as shown in Fig. 3d.

Forest plots of efficacy outcomes. a Early neurological improvement. b Recanalization of blood vessels. c 90-day excellent neurological recovery. d 90-day good neurological recovery
Safety Outcomes
Of the five safety outcome indicators, there were five studies that used poor neurological recovery or its variants as an outcome measure, which provided sufficient data for meta-analysis. The results of the meta-analysis indicated that there was no significant difference in the incidence of poor neurological recovery between the intravenously administered alteplase group and tenecteplase group (RR − 0.12; 95% CI − 0.68 to 0.44; P = 0.67), as shown in Fig. 4a. No significant difference in the incidence of any parenchymal hematoma was found between the intravenously administered alteplase group and the tenecteplase group (RR 0.12; 95% CI − 0.18 to 0.43; P = 0.43) in the eight studies that used parenchymal hematoma or its variants as an outcome (Fig. 4b). Nine studies using any ICH or its variants as outcome measures were included in the meta-analysis. The results of the meta-analysis showed that there was no significant difference in ICH outcomes between the intravenously administered alteplase and tenecteplase groups (RR 0.26; 95% CI − 0.20 to 0.73; P = 0.26; Fig. 4c). The results of the meta-analysis of 11 studies using symptomatic ICH or its variants showed no significant difference in symptomatic ICH between the intravenously administered alteplase and tenecteplase groups (RR 0.06; 95% CI − 0.21 to 0.33; P = 0.65), as shown in Fig. 4d. Ten studies used all-cause mortality or its variants as study outcomes. The results of our meta-analysis of these studies showed that there was no significant difference in all-cause mortality between the intravenously administered alteplase and tenecteplase groups (RR − 0.01; 95% CI − 0.17 to 0.15; P = 0.93), as shown in Fig. 4e.

Forest plots of safety outcomes. a Poor neurological recovery. b Any parenchymal hematoma. c Any ICH. d Symptomatic ICH. e All-cause mortality
Detection of Publication Bias
On the basis of the 16 included studies, we tested for publication bias in nine outcome measures, including efficacy (shown in Fig. 5) and safety (shown in Fig. 6). The funnel plot results showed that the left and right sides were symmetrical, and the Begg’s test results also showed symmetry of the results (P > 0.05), indicating that there was no publication bias. At the same time, Egger’s test results showed that all Z scores were less than 1.96 and P > 0.05, which also indicated that there was no publication bias in the included studies.

Funnel plot of efficacy outcomes and Egger’s and Begg’s analyses results. a Early neurological improvement. b Recanalization of blood vessels. c 90-day excellent neurological recovery. d 90-day good neurological recovery

Funnel plot of safety outcomes and Egger’s and Begg’s analyses results. a Poor neurological recovery. b Any parenchymal hematoma. c Any ICH. d Symptomatic ICH. e All-cause mortality
Discussion
Stroke is a leading cause of morbidity, mortality, and long-term disability worldwide [41, 42]. Alteplase is currently the only intravenous thrombolytic drug that is FDA approved, but its low recanalization rate, high risk of ICH, and short half-life necessitate continuous intravenous infusion. Tenecteplase is a new thrombolytic drug with a longer half-life and greater resistance to plasminogen activator inhibitors than alteplase. In recent years, with the advent of tenecteplase and publication of a considerable number of RCTs, intravenously administered tenecteplase for thrombolysis in patients with ischemic stroke has attracted increasing attention [43]. Tenecteplase, a third-generation thrombolytic, is a bioengineered variant of alteplase that changes the protein structure at three amino acid sites. Structurally, threonine 103 is substituted by asparagine and asparagine 117 is substituted by glutamine achieving a half-life of more than 20 min, thus allowing for more rapid thrombolysis with a single bolus; lysine-histidine-arginine-arginine (positions 296–299) is replaced by alanine-alanine-alanine-alanine, which increases the resistance of tenecteplase to plasminogen activator inhibitor 1 (PAI-1) and fibrin specificity compared with alteplase, and also explains why tenecteplase may be associated with a greater affinity for blood clots, more rapid recanalization, greater dissolution of older thrombi, and fewer non-ICH complications [44]. Nepal et al. [45] showed that the treatment cost of tenecteplase was much lower than that of alteplase, but the benefits were higher. The superior pharmacokinetic and pharmacodynamic profile of tenecteplase compared with alteplase provides a reason to seriously consider tenecteplase as an alternative to alteplase. The results of our meta-analysis also showed that tenecteplase was more effective than alteplase in several important efficacy outcomes. Even though the results were not significant, there was a trend toward benefit with tenecteplase administration.
The results of our meta-analysis showed that tenecteplase was more effective than alteplase in three of the four efficacy outcome measures: early neurological improvement, recanalization of blood vessels, and excellent neurological recovery at 90 days. This means that administration of tenecteplase could provide more benefits than intravenously administered alteplase. Although no significant heterogeneity was observed in the included studies, this finding should be interpreted with caution and confirmed through further research. Early neurological improvement may be attributed to the pharmacokinetic properties of tenecteplase, including its longer half-life (24 min for tenecteplase vs. 4–5 min for alteplase), higher fibrin specificity, and stronger clot dissolution, thus leading to faster vascular recanalization [46]. Oliveira et al. [47] also demonstrated a beneficial effect of tenecteplase on two important surrogate markers of reperfusion therapy effectiveness: recanalization rate and early neurological improvement. These pharmacologic differences allow for bolus administration of tenecteplase within 10 s, as compared with the 1-h administration of alteplase (10% of the total dose is administered intravenously and the remaining dose is infused over a period of 1 h), which greatly increases the convenience of clinical procedures and reduces the time to rescue patients [48]. Yogendrakumar et al. [49] combined imaging analysis with data from the EXTENDIA TNK trial (tenecteplase versu intravenously administered alteplase before endovascular treatment of ischemic stroke). The results showed that tenecteplase was superior to alteplase in improving early reperfusion in patients with ischemic stroke and a low thrombus burden. Compared with alteplase, tenecteplase achieves higher reperfusion rates in patients with ischemic stroke with distal large-vessel occlusion, and early reperfusion improves 90-day functional outcomes in patients with ischemic stroke. The TASTE-A study by Bivard et al. [26] showed that compared to thrombolysis with alteplase in the ultra-early stage, tenecteplase can enable patients to obtain thrombolytic therapy faster, reduce the hypoperfusion volume of patients more effectively, and achieve early improvement of clinical symptoms, providing strong evidence for the use of thrombolysis in mobile stroke units. TASTE-A not only places thrombolytic therapy in the prehospital setting but also conducts clinical trials of drugs in the prehospital setting, which is important in resource-poor remote settings where thrombectomy is not available and ambulances are required to transport patients to specialized stroke centers. This contrasts with the drip and transport patterns of multiple instillations and prolonged infusion of alteplase for up to 1 h [50].
In terms of safety, our meta-analysis results showed no statistical difference between tenecteplase and alteplase in five outcome measures assessing safety (poor neurological recovery, any ICH, symptomatic ICH, any parenchymal hematoma, and all-cause mortality). This indicates that tenecteplase has the same safety profile as alteplase. Since the introduction of tenecteplase to the global market, many studies comparing tenecteplase with alteplase have been published and its efficacy, safety, and convenience have been continuously confirmed. Katsanos et al. [51] first evaluated and analyzed the safety and efficacy of intravenously administered tenecteplase at various dosages versus intravenously administered alteplase in patients with AIS from six nonrandomized studies. The results showed that patients receiving intravenously administered tenecteplase had higher odds of 90-day good functional outcomes, successful recanalization, and early neurological improvement, while there was no significant difference in safety, 3-month excellent functional outcomes, parenchymal hematoma, or symptomatic ICH, which is similar to the results of a meta-analysis of RCTs on the same topic. Rehman et al. [15] constructed a network meta-analysis including ten RCTs to determine the optimal dose of intravenously administered tenecteplase and its impact on functional outcomes and mortality. It was concluded that tenecteplase at 0.25 mg/kg was more efficacious than other doses, representing significant improvement in 3-month excellent functional outcome and early neurological improvement. Besides, tenecteplase at 0.25 mg/kg dose is as safe as alteplase for intravenous thrombolysis, and there is no statistically significant difference in 90-day mortality at any dose between tenecteplase and alteplase. However, more studies are needed to directly compare the outcomes of tenecteplase at different doses and to analyze whether tenecteplase is efficacious at longer needle times.
At present, a large amount of evidence has accumulated in support of intravenous thrombolysis with tenecteplase for the treatment of AIS, including TAAIS [38], NOR-TEST [30], EXTEND-IA TNK [52], and TRACE II [38]. These studies have shown that tenecteplase is not inferior to rt-PA in efficacy, may have higher safety, and may achieve faster and more complete reperfusion in patients with large-vessel occlusion. In particular, a single intravenous injection of tenecteplase is convenient, suitable for the transportation of patients, and shortens the time from intravenous thrombolysis to femoral artery puncture, showing good application prospects.
Finally, our meta-analysis has some limitations. First, most of the included studies in this meta-analysis were open-label trials with relatively small sample sizes, which carry a certain risk of efficacy bias. Second, the definitions of some clinical outcome measures, such as early neurologic improvement, recanalization, and excellent neurologic recovery, also varied among the included studies. Third, heterogeneity was found among the individual outcome measures, which limited confidence in our conclusions. Finally, the included studies were limited to studies in English. Therefore, further research is necessary to overcome these limitations in the future to obtain more accurate and specific conclusions that can be used to guide clinical treatment.
Conclusions
Our meta-analysis showed that tenecteplase was associated with better early neurological improvement, recanalization of blood vessels, and neurologic recovery at 90 days than alteplase. In addition, there is no significant difference in terms of safety. These results indicate that tenecteplase is as safe and more effective as alteplase in the treatment of patients with AIS. As a new generation of thrombolytic drugs, tenecteplase’s convenient administration and superior pharmacological characteristics make it a promising first-line thrombolytic drug. We look forward to more clinical studies in the future to provide more conclusive evidence for tenecteplase intravenous thrombolysis in the treatment of AIS and to the development of more new thrombolytic drugs to provide more powerful means for the treatment of AIS.
References
GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795–820.
Pandian JD, Kalkonde Y, Sebastian IA, Felix C, Urimubenshi G, Bosch J. Stroke systems of care in low-income and middle-income countries: challenges and opportunities. Lancet. 2020;396(10260):1443–51.
Benjamin EJ, Muntner P, Alonso A, et al. Heart disease and stroke statistics-2019 update: a report from the American Heart Association. Circulation. 2019;139(10):e56–528.
Mahmood A, Muir KW. Tenecteplase or alteplase: What is the thrombolytic agent of the future? Curr Treat Options Neurol. 2022;24(10):503–13.
Yepes M, Woo Y, Martin-Jimenez C. Plasminogen activators in neurovascular and neurodegenerative disorders. Int J Mol Sci. 2021;22(9):4380.
Ma P, et al. Tenecteplase vs alteplase for the treatment of patients with acute ischemic stroke: a systematic review and meta-analysis. J Neurol. 2022;269(10):5262–71.
Yeo LL, et al. Timing of recanalization after intravenous thrombolysis and functional outcomes after acute ischemic stroke. JAMA Neurol. 2013;70(3):353–8.
Bhatia R, et al. Low rates of acute recanalization with intravenous recombinant tissue plasminogen activator in ischemic stroke: real-world experience and a call for action. Stroke. 2010;41(10):2254–8.
Whiteley WN, et al. Risk of intracerebral haemorrhage with alteplase after acute ischaemic stroke: a secondary analysis of an individual patient data meta-analysis. Lancet Neurol. 2016;15(9):925–33.
Singh N, et al. Replacing alteplase with tenecteplase: is the time ripe? J Stroke. 2023;25(1):72–80.
Kheiri B, et al. Tenecteplase versus alteplase for management of acute ischemic stroke: a pairwise and network meta-analysis of randomized clinical trials. J Thromb Thrombolysis. 2018;46(4):440–50.
Huang X, et al. Coagulation and fibrinolytic activity of tenecteplase and alteplase in acute ischemic stroke. Stroke. 2015;46(12):3543–6.
Assessment of the Safety and Efficacy of a New Thrombolytic (ASSENT-2) Investigators, et al. Single-bolus tenecteplase compared with front-loaded alteplase in acute myocardial infarction: the ASSENT-2 double-blind randomised trial. Lancet. 1999;354(9180):716–22.
Powers WJ, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344–418.
Rehman AU, et al. Comparative efficacy and safety of tenecteplase and alteplase in acute ischemic stroke: a pairwise and network meta-analysis of randomized controlled trials. J Neurol Sci. 2023;445: 120537.
Rose D, et al. Complications of intravenous tenecteplase versus alteplase for the treatment of acute ischemic stroke: a systematic review and meta-analysis. Stroke. 2023;54(5):1192–204.
Liang H, et al. Different doses of tenecteplase vs. alteplase for acute ischemic stroke within 4.5 hours of symptom onset: a network meta-analysis of randomized controlled trials. Front Neurol. 2023;14:1176540.
Abuelazm M, et al. The efficacy and safety of tenecteplase versus alteplase for acute ischemic stroke: an updated systematic review, pairwise, and network meta-analysis of randomized controlled trials. J Thromb Thrombolysis. 2023;55(2):322–38.
Page MJ, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372: n71.
Cumpston M, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev. 2019;10: ED000142.
Higgins JP, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343: d5928.
Xiang X, et al. Clinical utility of tumour mutational burden on efficacy of immune checkpoint inhibitors in malignant solid tumours: protocol for a systematic review and meta-analysis. BMJ Open. 2022;12(8): e058692.
Haile TG, et al. Prevalence of hypertension among type 2 diabetes mellitus patients in Ethiopia: a systematic review and meta-analysis. Int Health. 2022. https://doi.org/10.1093/inthealth/ihac060.
Yu B, et al. Risk of cardiovascular disease among cancer survivors: protocol of a pooled analysis of population-based cohort studies. Front Cardiovasc Med. 2022;9: 926218.
Alemseged F, et al. Tenecteplase vs alteplase before endovascular therapy in basilar artery occlusion. Neurology. 2021;96(9):e1272–7.
Bivard A, et al. Comparison of tenecteplase with alteplase for the early treatment of ischaemic stroke in the Melbourne Mobile Stroke Unit (TASTE-A): a phase 2, randomised, open-label trial. Lancet Neurol. 2022;21(6):520–7.
Campbell BCV, et al. Tenecteplase versus alteplase before thrombectomy for ischemic stroke. N Engl J Med. 2018;378(17):1573–82.
George M, et al. Comparison of thrombolytic agents in treatment of patients with acute ischemic stroke; findings from a single centre follow up study in real-life settings. J Clin Neurosci. 2021;91:299–305.
Huang X, et al. Alteplase versus tenecteplase for thrombolysis after ischaemic stroke (ATTEST): a phase 2, randomised, open-label, blinded endpoint study. Lancet Neurol. 2015;14(4):368–76.
Kvistad CE, et al. Tenecteplase versus alteplase for the management of acute ischaemic stroke in Norway (NOR-TEST 2, part A): a phase 3, randomised, open-label, blinded endpoint, non-inferiority trial. Lancet Neurol. 2022;21(6):511–9.
Li S, et al. Safety and efficacy of tenecteplase versus alteplase in patients with acute ischaemic stroke (TRACE): a multicentre, randomised, open label, blinded-endpoint (PROBE) controlled phase II study. Stroke Vasc Neurol. 2022;7(1):47–53.
Logallo N, et al. Tenecteplase versus alteplase for management of acute ischaemic stroke (NOR-TEST): a phase 3, randomised, open-label, blinded endpoint trial. Lancet Neurol. 2017;16(10):781–8.
Mahawish K, et al. Switching to tenecteplase for stroke thrombolysis: real-world experience and outcomes in a regional stroke network. Stroke. 2021;52(10):e590–3.
Menon BK, et al. Intravenous tenecteplase compared with alteplase for acute ischaemic stroke in Canada (AcT): a pragmatic, multicentre, open-label, registry-linked, randomised, controlled, non-inferiority trial. Lancet. 2022;400(10347):161–9.
Psychogios K, et al. Real-world comparative safety and efficacy of tenecteplase versus alteplase in acute ischemic stroke patients with large vessel occlusion. Ther Adv Neurol Disord. 2021;14:1756286420986727.
Ronning OM, et al. Tenecteplase versus alteplase between 3 and 4.5 hours in low national institutes of health stroke scale. Stroke. 2019;50(2):498–500.
Seners P, et al. Recanalization before thrombectomy in tenecteplase vs alteplase-treated drip-and-ship patients. J Stroke. 2019;21(1):105–7.
Wang Y, et al. Tenecteplase versus alteplase in acute ischaemic cerebrovascular events (TRACE-2): a phase 3, multicentre, open-label, randomised controlled, non-inferiority trial. Lancet. 2023;401(10377):645–54.
Warach SJ, et al. Prospective observational cohort study of tenecteplase versus alteplase in routine clinical practice. Stroke. 2022;53(12):3583–93.
Zhong CS, et al. Routine use of tenecteplase for thrombolysis in acute ischemic stroke. Stroke. 2021;52(3):1087–90.
Zhai M, et al. Effect of intravenous thrombolytic dose of alteplase on long-term prognosis in patients with acute ischemic stroke. Neurol Ther. 2023. https://doi.org/10.1007/s40120-023-00488-3.
Campbell BC. Thrombolysis and thrombectomy for acute ischemic stroke: strengths and synergies. Semin Thromb Hemost. 2017;43(2):185–90.
Warach SJ, Dula AN, Milling TJ Jr. Tenecteplase thrombolysis for acute ischemic stroke. Stroke. 2020;51(11):3440–51.
Zhu A, et al. Alteplase or tenecteplase for thrombolysis in ischemic stroke: an illustrated review. Res Pract Thromb Haemost. 2022;6(6):e12795.
Nepal G, et al. Tenecteplase versus alteplase for the management of acute ischemic stroke in a low-income country-Nepal: cost, efficacy, and safety. Cureus. 2018;10(2): e2178.
Fruhwald T, et al. In vitro examination of the thrombolytic efficacy of tenecteplase and therapeutic ultrasound compared to rt-PA. BMC Neurol. 2019;19(1):181.
Oliveira M, et al. Tenecteplase for thrombolysis in stroke patients: systematic review with meta-analysis. Am J Emerg Med. 2021;42:31–7.
Abuelazm M, et al. The efficacy and safety of tenecteplase versus alteplase for acute ischemic stroke: an updated systematic review, pairwise, and network meta-analysis of randomized controlled trials. J Thromb Thrombolysis. 2022. https://doi.org/10.1007/s11239-022-02730-5.
Yogendrakumar V, et al. Tenecteplase treatment and thrombus characteristics associated with early reperfusion: an EXTEND-IA TNK trials analysis. Stroke. 2023;54(3):706–14.
Burgos AM, Saver JL. Evidence that tenecteplase is noninferior to alteplase for acute ischemic stroke: meta-analysis of 5 randomized trials. Stroke. 2019;50(8):2156–62.
Katsanos AH, et al. Off-label use of tenecteplase for the treatment of acute ischemic stroke: a systematic review and meta-analysis. JAMA Netw Open. 2022;5(3): e224506.
Campbell BCV, et al. Effect of intravenous tenecteplase dose on cerebral reperfusion before thrombectomy in patients with large vessel occlusion ischemic stroke: the EXTEND-IA TNK part 2 randomized clinical trial. JAMA. 2020;323(13):1257–65.
Acknowledgements
Author Contribution
Ziyi Shen and Nana Bao designed the experiments and drafted the manuscript. Ming Tang and Yang Yang contributed to data collection. Jia Li analyzed the data. Wei Liu and Guohui Jiang formatted/submitted the paper. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
This study was supported by the National Natural Science Foundation of China (No. 81971220) and Research Development Program of the Affiliated Hospital of North Sichuan Medical College (No. 2021LC008 and No. 2021ZD002). The rapid service fee was funded by the authors.
Medical Writing/Editorial Assistance
We would like to thank Editage (www.editage.cn) for English language editing. The source of funding for this assistance by the authors.
Data Availability
All data generated or analyzed during this study are included in this published article/as supplementary information files.
Ethical Approval
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Conflict of Interest
Ziyi Shen, Nana Bao, Ming Tang, Yang Yang, Jia Li, Wei Liu, and Guohui Jiang have nothing to disclose.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Shen, Z., Bao, N., Tang, M. et al. Tenecteplase vs. Alteplase for Intravenous Thrombolytic Therapy of Acute Ischemic Stroke: A Systematic Review and Meta-Analysis. Neurol Ther 12, 1553–1572 (2023). https://doi.org/10.1007/s40120-023-00530-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40120-023-00530-4