
Abstract
Introduction
Ivabradine reduces heart rate (HR), episodes of angina, and nitrate consumption, and increases exercise capacity in patients with chronic angina (CA). In this exploratory study, myocardial perfusion scintigraphy (MPS) was used to evaluate changes in the percentage of myocardial ischemia after ivabradine therapy in patients with CA.
Methods
This prospective, open-label, single-arm study included patients with CA receiving maximum tolerated doses of beta blockers, who had a resting HR ≥ 70 bpm and had experienced ischemia according to MPS during an exercise test at baseline. Participants received ivabradine 5 mg twice daily (titrated according to HR) concomitant with beta blockers. A second MPS was performed after 3 months, without interruption of treatment with beta blockers or ivabradine. The primary outcome was change in the percentage of myocardial ischemia from baseline to 3 months. Time to ischemia during the exercise test, the proportion of patients presenting angina during the exercise test, and health status, assessed using the seven-item Seattle Angina Questionnaire-7 (SAQ-7), were also evaluated.
Results
Twenty patients (3 females) with a mean (± standard deviation [SD]) age of 62.2 ± 6.5 years were included in the study, of whom 55% had diabetes, 70% had previous myocardial revascularization, and 45% had previous myocardial infarction. The percentage of patients with myocardial ischemia significantly decreased from baseline to 3 months after initiation of treatment with ivabradine (− 2.9%; 95% confidence interval [CI] − 0.3 to − 5.5; p = 0.031). Mean time to appearance of ischemia increased from 403 ± 176 s at baseline to 466 ± 136 s at 3 months after initiation of ivabradine (Δ62 s; 95% CI 18–106 s; p = 0.008), and the proportion of patients experiencing angina during the exercise test decreased from 40% at baseline to 5% also at 3 months (p = 0.016). Mean resting HR decreased from 76 ± 7 bpm at baseline to 55 ± 8 bpm at 3 months (p < 0.001). The mean SAQ-7 summary score improved from 69 ± 21 at baseline to 83 ± 12 at 3 months (p = 0.001). No serious adverse effects were reported.
Conclusion
Ivabradine added to beta blockers was associated with a reduction in detectable myocardial ischemia by MPS in patients with CA.
Infographic available for this article.
Trial Registration
The trial has been retrospectively registered with the Brazilian Registry of Clinical Trials (REBEC) under the following number RBR-5fysqrh (date of registration: 30 November 2023).
Graphical Abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out the study? |
To date, there have been no published studies reporting the use of myocardial perfusion scintigraphy (MPS) to evaluate the effect of ivabradine on myocardial perfusion in ischemic patients with chronic angina (CA) who are receiving concomitant beta blockers. |
Since elevated resting heart rate (HR) is a marker of cardiovascular risk, the effects of reducing HR with a known agent such as ivabradine was evaluated using MPS in beta-blocker–treated patients with CA. |
What was learned from this study? |
The primary outcome was the change in the percentage of myocardial ischemia after 3 months of ivabradine therapy. |
Ivabradine was associated with a decrease in detectable myocardial ischemia by MPS in patients with CA on maximum tolerated doses of beta blockers; these effects were accompanied by an increase in time to the appearance of ischemia and a reduction in angina during the exercise stress test. |
Overall, duration of exercise, HR, and Seattle Angina Questionnaire-7 scores also improved after ivabradine treatment, and no serious adverse effects were reported. |
Digital Features
This article is published with digital features, including infographic, to facilitate understanding of the article. To view digital features for this article, go to https://doi.org/10.6084/m9.figshare.25265038.
Introduction
Although clinical practice strategies for ischemic heart disease (IHD) prevention and treatment have evolved in recent years, the consequences of this condition remain a significant burden on human health, and it remains the leading global cause of cardiovascular deaths [1]. IHD affects approximately 244 million people worldwide, according to 2020 estimates [2], and the prevalence increases with age in both sexes [3].
Patients with IHD commonly experience angina, which is caused by a mismatch in oxygen supply and demand, and often precipitated by exercise [4]. Angina pectoris can be incapacitating and have an adverse effect on a patient's quality of life (QoL), including their emotional well-being and ability to engage in physical activity [5,6,7].
An elevated resting heart rate (HR) is a marker of cardiovascular risk in the general population, as well as in patients with cardiovascular disease, and is associated with cardiovascular morbidity and mortality in patients with IHD [8, 9]. HR is a key determinant of myocardial oxygen consumption; an elevated HR reduces diastolic time and consequently affects coronary flow [7], potentially resulting in ischemia and angina [10]. Treatment to reduce the HR improves symptomatic ischemia in patients with chronic angina (CA) [11]. This approach targets the underlying mechanisms of angina instead of the standard approach of targeting obstructive IHD, and as such represents a paradigm shift in the approach to the management of angina and ischemia [12].
The European Society of Cardiology (ESC) guidelines on chronic coronary syndromes (CCS) recommend beta blockers or non-dihydropyridine calcium channel blockers for patients with CA and elevated HR [13]. The ESC guidelines also recognize that the combination of a beta blocker and a second-line agent may be considered in selected patients according to the HR and blood pressure (BP) [13].
Ivabradine reduces the HR and increases the duration of diastole without affecting BP, vascular tone, or left ventricular systolic function by inhibiting the “funny” current (If) in the sinoatrial node [11, 14, 15]. In combination with beta blockers, ivabradine not only reduces HR, the frequency of angina episodes, and nitrate consumption, but also increases total exercise duration on the exercise treadmill test (ETT) and improves QoL in patients with CA [16, 17]. Furthermore, ivabradine increases coronary flow reserve [18, 19] and seems to positively affect coronary collateral function in patients with CA [20].
Myocardial perfusion scintigraphy (MPS) is an imaging method that has long been fundamental to clinical cardiovascular imaging and has been accepted as a reliable diagnostic tool for myocardial ischemia [21]. MPS uses single-photon emission computed tomography (SPECT) and injected radiopharmaceuticals to assess the extent (percentage) and severity of induced myocardial ischemia in the left ventricle, while simultaneously measuring left ventricular function and volumes [22, 23]. A meta-analysis demonstrated the value and effectiveness of MPS in assessing myocardial perfusion, with a sensitivity of 86% and a specificity of 74%; the reported normalcy rate (a more reliable measure of performance) of MPS was 88% [24]. In addition to the incremental prognostic value over clinical assessment, MPS may also help to guide therapy. The amount of ischemia identified using MPS sets the individual risk used for risk-based decisions regarding myocardial revascularization or optimization of medical therapy [22]. One strength of ischemia detection by MPS is the wealth of prognostic data accumulated over the years with this technique and its association with detecting subsets of patients at increased risk of major cardiovascular events [25].
However, to date, no published studies have used MPS to evaluate the effect of ivabradine on myocardial perfusion. The aim of this preliminary study was to evaluate, using MPS, the change in the percentage of myocardial ischemia after adding ivabradine to a beta-blocker regimen in ischemic patients with CA.
Methods
Study Design
This prospective open-label, single-arm study was conducted at Quanta Diagnóstico por Imagem, a high-volume imaging center in Curitiba, Brazil, which has performed more than 6000 MPS procedures annually since 2003.
Patients had to meet the following eligibility criteria to be included in the study: (1) diagnosis of CA; (2) age of 18–70 years; (2) symptomatic even when on beta blockers (at maximum tolerated doses); (4) resting HR ≥ 70 beats per minute (bpm); (5) sinus rhythm; (6) left ventricular ejection fraction (LVEF) > 40%; and (7) presence of myocardial ischemia at the baseline MPS, performed with an ETT to evaluate ischemia induced under controlled medical conditions. An upper age limit of 70 years was selected to ensure that all patients in our study could start on the same dose of ivabradine 5 mg twice daily (b.i.d.) (the recommended starting dosage in patients aged ≥ 75 years is 2.5 mg b.i.d.).
Exclusion criteria were: (1) unstable IHD; (2) acute myocardial infarction (MI) < 6 months previously; (3) LVEF ≤ 40%; (4) HR < 70 bpm; (5) presence of left bundle branch block; (6) a pacemaker;(7) inability to perform the ETT due to physical limitations; (8) pregnancy or nursing status (women); (9) contraindications to ivabradine in accordance with the summary of product characteristics; and (10) a contraindication to MPS.
The schedule of study visits and observations are summarized in Fig. 1. Treatment with ivabradine 5 mg b.i.d. was initiated by study investigators at the baseline visit (visit 1). Four weeks after ivabradine initiation, the dose was titrated according to HR, persistence of symptoms, and tolerance of the drug. The dose was increased to 7.5 mg b.i.d. if the HR was > 60 bpm, but titrated down to 2.5 mg (half of a 5 mg tablet) b.i.d. if, during the treatment with 5 mg ivabradine b.i.d., the HR decreased to < 50 bpm at rest or the patient experienced symptoms related to bradycardia, such as dizziness, fatigue, or hypotension. Similarly, in patients who were receiving 7.5 mg ivabradine b.i.d., the dose was titrated down to 5 mg b.i.d. if the HR decreased to < 50 bpm at rest or patients developed symptoms of bradycardia. A second MPS was performed 3 months after the initiation of ivabradine (2–3 months after reaching the optimal dose), without interruption or change in the dose of the beta blocker and/or ivabradine.

Study design and procedures. Asterisk indicates that the MPS images were analyzed in a blinded manner (both patient identity and ivabradine administration unknown) by two independent investigators. b.i.d. twice daily, ETT exercise treadmill test, MPS myocardial perfusion scintigraphy, SAQ-7 seven-item Seattle Angina Questionnaire
The primary endpoint was the percentage of myocardial ischemia, which was evaluated in a blinded manner by the same two independent investigators at baseline and at 3 months. During the analysis of images, investigators were aware of neither patient identity nor ivabradine administration. Time to ischemia (angina, horizontal or down-sloping ST-segment depression of ≥ 1 mm), duration of exercise, and peak HR during the ETT were also evaluated. Patients were asked to answer items from the physical limitation, angina frequency, and QoL domains of the shortened seven-item Seattle Angina Questionnaire (SAQ-7) [26] at baseline (first visit), during the second visit (1 month after initiation of ivabradine), and during the last visit (3 months after initiation of ivabradine).
After providing written informed consent, patients entered the study. Patients received background therapy for CCS according to contemporary guidelines. The study was approved by the Research Ethics Committee of the Hospital de Clinicas da Universidade Federal do Paraná, in Curitiba, Paraná, Brazil (ethics approval number 3.182.920), and all procedures were followed in accordance with the Helsinki Declaration of 1964, as revised in 2013.
Exercise Treadmill Test
Symptom-limited ETTs, using the standard Bruce protocol, were performed for the MPS stress test. Treatment for CCS, including beta blockers and ivabradine, was not interrupted when patients undertook the ETT. Time to onset of angina, time to limiting angina during the ETT, total exercise duration, and time to 1-mm horizontal or down-sloping ST-segment depression were determined by the investigator. HR was obtained from the electrocardiogram (ECG) recording, and the rate-pressure product was determined using BP measurements at rest and during exercise. Interruption criteria were limiting angina, dyspnea, and extreme fatigue. The depression of the ST-segment was measured at the J-point in three consecutive QRS complexes with a flat baseline.
Myocardial Perfusion Scintigraphy
The MPS studies were performed according to institutional protocols following current guidelines. Images were acquired on the Ventri Cardiac Imaging System (2006 model; GE HealthCare, Chicago, IL, USA) or the NM 530c Discovery Nuclear Medicine System (2012 model; GE HealthCare). Resting scans were performed 30–60 min after intravenous injection of the radiopharmaceutical 99mTc-sestamibi. Stress tests were conducted on a separate date with another administration of 99mTc-sestamibi, and images were acquired after 15–60 min of physical stress. Radiopharmaceutical activity was determined based on body mass index, and activity optimization was allowed by increasing acquisition time, as recommended by the guidelines [21, 27, 28]. The radiation dose applied during MPS in the clinic is 8.4 msV, consistent with American Society of Nuclear Cardiology recommendations of a dose < 9 msV [27]. Images were processed using quantified SPECT gated software (QGS; Cedars-Sinai, Los Angeles, CA, USA) and analyzed by standard semi-quantitative visual quantification. Using the 17-segment polar map, each segment was scored from 0 to 4 according to radiopharmaceutical uptake (0 = normal, 1 = discrete reduction, 2 = moderate reduction, 3 = significant reduction, 4 = absence of radiopharmaceutical uptake).
From the sum of values attributed to each segment in the stress phase, the summed stress score (SSS) and summed rest score (SRS) were obtained. The summed difference score (SDS) was calculated as SSS − SRS. The primary outcome of interest was the total ischemic burden, reflected by the percentage of ischemic myocardium. Normalized values were calculated by dividing the measured SSS, SRS, and SDS score by 68 (derived from a deficit of 4 points in each of the 17 segments of the MPS polar map) and then multiplying the result by 100% to convert the value to a percentage [21]. The degree of ischemia was also categorized as: (1) absent or minimal, if SDS < 2; (2) mild, if SDS 2–4; (3) moderate, if SDS 5–8, and (4) significant, if SDS > 8 [29, 30]. All MPS readings were performed independently by two trained nuclear cardiologists who were blinded to whether ivabradine was administered or not. Any disagreement was resolved by a consensus achieved with the assistance of a third trained nuclear cardiologist.
Statistical Methods
Sample Size Calculation
Since there are no published studies evaluating MPS in ivabradine-treated patients, we examined the sample sizes used in other published studies of ivabradine (between 12 and 59 patients) [15, 18, 19]. In addition, data from the nuclear sub-study of the COURAGE trial [23] showed a difference in the ischemic myocardium of –2.7% with percutaneous coronary intervention and optimal medical therapy and –0.5% with optimal medical therapy alone.
On this basis, we estimated that 20 patients would be necessary to detect a 4 ± 6 percentage change in myocardial ischemia after treatment with ivabradine with a power of 80% and a two-sided alpha of 5%, assuming a baseline myocardial ischemia of 8%.
Statistical Analyses
Continuous variables were evaluated for the Gaussian distribution of the data and presented as mean ± standard deviation (SD) if normal, or median (25th percentile, 75th percentile) if non-normal. Categorical variables were presented as proportions. Continuous variables were compared before and after initiation of ivabradine treatment using the paired t-test or the Wilcoxon signed rank test if the delta between the two measurements was normal or non-normal, respectively. Categorical variables before and after the intervention were compared using the McNemar exact test. The level of significance was set as 0.05; p values were not adjusted for multiple comparisons. Analyses were performed using Stata version 15 (Stata Corp, College Station, TX, USA).
Results
Twenty patients were enrolled in the study, conducted between November 2019 and November 2022.
Baseline Characteristics
The mean (± SD) age of the study population (17 males, three females) was 62.2 ± 6.5 years (Table 1), and the mean resting HR was 76 ± 7 bpm (Table 2). Overall, 45% of the patients (n = 9) had a previous MI, 70% had previous revascularization (n = 14), and 55% had diabetes (n = 11).
Patients were already receiving appropriate therapy for CCS, in accordance with current guidelines, when enrolled in the study. Existing beta-blocker treatments were metoprolol (40% of patients; n = 8), carvedilol (25%; n = 5), nebivolol (20%; n = 4), and bisoprolol (15%; n = 3). The median (25th–75th percentile) daily dose was 50 (50–100) mg of metoprolol, 5 (3.75–5) mg of nebivolol, and 50 (25–50) mg of carvedilol; all patients taking bisoprolol received a dose of 5 mg/day. Of the 20 patients, 95% were using statins (n = 19) and 75% (n = 15) were on angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers. No changes were made to the existing baseline therapy regimens during the study. After dose titration, the ivabradine dose was 5 mg b.i.d. in 13 patients (65%), 7.5 mg b.i.d. in six patients (30%), and 2.5 mg b.i.d. in one patient (5%).
Three months after reaching the maximum tolerated dose of ivabradine, the mean (±S D) resting HR had decreased significantly to 55 ± 8 bpm (p < 0.001; Table 2).
Myocardial Ischemia Determined by MPS
No change in the mean SRS (± SD) was noted (3.3 ± 6.9 at baseline to 3.7 ± 7.3 at 3 months; p = 0.38; Table 2). However, the decrease in the SSS from 8.4 ± 8.9 at baseline to 6.9 ± 7.9 at 3 months was close to statistical significance (p = 0.071), and a significant decrease was observed in the absolute SDS (from 5.1 ± 4.5 at baseline to 3.2 ± 3.4 at 3 months; p = 0.031). An overall statistically significant reduction in the SDS percentage of myocardial ischemia of − 2.9% (95% CI − 0.3 to − 5.5) was calculated (from a mean of 7.5 ± 6.6% at baseline to 4.6 ± 5.0% after 3 months of ivabradine treatment; p = 0.031; Fig. 2).

Distribution of the percentage of myocardial ischemia before and 3 months after the initiation of ivabradine treatment. The horizontal line through the box represents the median, and the lower and upper limits of the box represent the 25th and 75th percentiles, respectively. Whiskers were drawn based on 1.5-times the interquartile range, and the dots outside the boundaries of the whiskers are the outliers. SD Standard deviation
The percentage of patients with different degrees of ischemia at baseline and after 3 months of ivabradine treatment is shown in Fig. 3 (p = 0.060). The addition of ivabradine to beta-blocker treatment resulted in an increase in the percentage of patients with no ischemia and a decrease in the percentage of those with mild, moderate and, particularly, severe ischemia.

Percentage of participants with different degrees of ischemia according to the SDS before and after 3 months of ivabradine treatment. SDS Summed difference score
Figure 4 provides an example of improvement in myocardial ischemia detected by MPS in a 58-year-old male patient with type 2 diabetes, who presented with angina triggered by physical exertion (up to 3 episodes weekly). MPS at baseline showed moderate to severe ischemia in the inferior wall and moderate ischemia in the anterolateral wall of the left ventricle (Fig. 4a). In addition, ventricular function was normal, LVEF after exercise was 66%, SDS was 15, and exercise time was 9.5 min according to the Bruce protocol. MPS performed 3 months after the initiation of ivabradine treatment showed an improvement in ischemia in the anterolateral wall and the inferior wall (persisting with moderate ischemia in the inferior wall and apex of the left ventricle; Fig. 4b). Normal ventricular function persisted, and LVEF after exercise was 63%, SDS was 11, and exercise time increased to 11 min (Bruce protocol).

Myocardial perfusion scintigraphy images for a 58-year-old male patient. a On presentation, b after 3 months of ivabradine treatment
Exercise Parameters
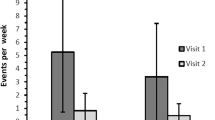
The proportion of patients who experienced angina during the ETT decreased from 40% at baseline to 5% after 3 months of ivabradine treatment (p = 0.016; Table 2). In addition, the mean (± SD) time taken for ischemia to appear increased significantly from 403 ± 176 s at baseline to 466 ± 136 s at 3 months (Δ62 s; 95% CI 18–106 s; p = 0.008). Although total exercise duration increased from 474 ± 161 s at baseline to 496 ± 142 s at 3 months (Δ21 s; 95% CI − 2.0 to 45 s), statistical significance was not reached (p = 0.071). Peak HR decreased from 140 ± 9 bpm at baseline to 124 ± 15 bpm at the 3-month follow-up visit (p < 0.001).
Seattle Angina Questionnaire-7 Scores
Assessment of health status, as measured by the SAQ-7 summary score, increased from a mean (± SD) score of 69 ± 21 at baseline to 83 ± 12 at the 3-month follow-up (p = 0.001; Table 3). Each domain of the SAQ-7 showed statistically significant improvements: (1) the angina frequency domain score increased from 79 ± 18 at baseline to 90 ± 12 at 3 months (indicating a reduction in patient-reported angina frequency; p < 0.001); (2) the QoL domain increased from 54 ± 29 at baseline to 71 ± 22 at 3 months (indicating an improvement of QoL; p = 0.019); and (3) the physical limitation domain increased from 75 ± 22 at baseline to 89 ± 13 at 3 months (indicating a reduction in physical limitations; p = 0.007).
Side Effects
Phosphenes (increases in brightness in limited areas of the visual field resulting in luminous phenomena even in the absence of light) were reported by six patients at the second visit (1 month after initiation of ivabradine treatment) and by eight patients at the third visit (3 months after reaching the maximum tolerated dose of ivabradine). While three of the six patients who experienced phosphenes at the second visit did not report phosphenes at the third visit, the other three patients had persistent mild phosphenes at the third visit. The five remaining patients presented mild phosphenes at the third visit only. No intervention was necessary due to the occurrence of phosphenes.
Asymptomatic bradycardia (HR < 50 bpm) was present in three patients each at the second and third visits. Two of the three patients who presented asymptomatic bradycardia at the second visit did not present with bradycardia at the third visit.
No cases of symptomatic bradycardia, hypotension, side effects requiring intervention, or serious adverse effects were reported in this study. None of the patients dropped out of the study.
Discussion
The results of this study demonstrated that in the 20 patients with CA taking the maximum tolerated doses of beta blockers, treatment with ivabradine was associated with a decrease in myocardial ischemia detectable by MPS, accompanied by an increase in time to appearance of ischemia and a reduction in the proportion (percentage) of patients presenting with angina during the ETT.
To the best of our knowledge, this is the first study to report the effect of ivabradine on ischemia using MPS. Our rationale for choosing this SPECT imaging modality was twofold: (1) it is able to provide a quantitative evaluation of myocardial ischemia [22]; and (2) the resulting prognostic data are valuable in determining the choice of treatment (optimal pharmacologic therapy vs. invasive treatment) in patients with CA [21].
Ischemia and angina typically develop during increased cardiac workload [31]; as such, the ETT is a known method to simulate exercise-inducible ischemia [32]. Our preliminary study showed a significant reduction in the percentage of myocardial ischemia during exercise, as well as in the corresponding SDS values, from 5.1 ± 4.5 (categorized as moderate ischemia) to 3.2 ± 3.4 (mild ischemia). Maranta et al. [32] previously reported that ivabradine (evaluated by stress echocardiography) not only reduced acute left ventricular dysfunction and myocardial stunning in patients with coronary artery disease (CAD) and exercise-inducible ischemia but also improved both longitudinal strain in ischemic segments and average global longitudinal strain value. Despite not reaching statistical significance, we also observed a reduction in the overall percentage of patients with mild, moderate, and severe ischemia, as well as an increase in the percentage of normal examination results at 3 months of follow-up.
Notwithstanding the small sample size of our study, we demonstrated that MPS is able to detect regional changes in ischemia during ivabradine treatment. The changes shown in Fig. 4 are illustrative of the type of pattern seen on MPS imaging scans in our study. Although moderate ischemia persisted in the inferior wall and apex of the left ventricle of this patient, their MPS imaging scans demonstrated marked improvements in ischemia in the anterolateral wall and in the inferior wall after ivabradine was administered for 3 months. Reductions in HR and SDS were also noted, and exercise time increased.
There are several underlying mechanisms which could explain how ivabradine reduces myocardial ischemia as assessed by MPS. Ivabradine lowers the HR by inhibiting the If current in the sinoatrial node and increases diastolic time, improving coronary flow [15] and increasing coronary flow reserve [18, 19]. In one study, increased coronary flow reserve persisted even after HR correction (where paced HR was identical to the HR before treatment), suggesting improved microvascular function [18]. Another study demonstrated that there was a greater improvement in coronary flow reserve with ivabradine treatment than with bisoprolol treatment in patients with CA, despite a similar decrease in the HR, indicating that the effect of ivabradine goes beyond HR reduction [19]. Ivabradine improves coronary collateral function [20], augmenting regional blood flow [31]. Ivabradine may also improve endothelial dysfunction and reduce oxidative stress, thus preventing atherosclerosis [33, 34]. All these actions induced by ivabradine may contribute to the decreased myocardial ischemia and frequency of angina that we observed in this study.
Beta blockers are usually recommended for the management of patients with angina and a high HR [13]. In one double-blind study of 889 patients with CA, 4 months of treatment with the combination of ivabradine 7.5 mg b.i.d. and atenolol at the dosage commonly used in clinical practice led to an improvement in total exercise duration, time to limiting angina, time to angina onset, and time to 1 mm ST depression using the standard Bruce protocol for the ETT [17]. However, in the present study, we did not find a significant increase in total exercise duration after 3 months of ivabradine treatment, which could be due to the lack of power in our study. On the other hand, we did show a significant increase in time to appearance of ischemia (angina or 1 mm ST depression) after 3 months of ivabradine treatment (using the standard Bruce protocol), as well as a reduction in the percentage of angina during the ETT. In our study, patients were also on different beta blockers, which might have affected the results.
Data from 33,177 patients in the CLARIFY registry showed that despite a high percentage of beta-blocker usage, 44% of the patients with chronic stable angina had a resting HR of > 70 bpm and that this HR was associated with more frequent angina and ischemia [35]. In our study, in which all patients were on the maximum tolerated doses of beta blockers, the mean (± SD) HR of 76 ± 7 bpm before initiating ivabradine treatment decreased to 55 ± 8 bpm (p < 0.001) after 3 months of ivabradine treatment. The BEAUTIFUL trial showed that in patients with stable CAD and left ventricular systolic dysfunction with a HR of ≥ 70 bpm, ivabradine in addition to the appropriate conventional cardiovascular treatment was associated with a 36% reduction in hospital admissions for fatal and non-fatal MI and a 30% reduction of coronary revascularization [36].
There are conflicting views on the presence of myocardial ischemia being a predictor of cardiovascular events. On one hand, the ISCHEMIA [37, 38] and MASS [39] studies have shown that chronic myocardial ischemia does not increase the risk of major cardiovascular events, while on the other hand, the PROMISE study found that not only the presence, but also the extent of myocardial ischemia is associated with an increased the risk of major cardiovascular events [40].
Failure to increase doses of beta blockers and discontinuation of therapy could worsen CA and increase the HR [41] while, to the contrary, increasing doses of beta blockers could cause hypotension and lead to a higher risk of worsening angina [42] and cardiovascular events [43]. Previous studies have shown that the addition of ivabradine to beta blockers resulted in more pronounced anti-anginal efficacy than the up-titration of beta blockers, and that the combination was better tolerated [16, 44, 45]; moreover, this approach was associated with an improvement in patient-reported outcomes [16, 44]. Consistent with these data, we found that adding ivabradine to the treatment regimen of patients who were already receiving the maximum tolerated doses of beta blockers led to a significant improvement in all three domains of angina frequency, QoL, and physical limitation on the SAQ-7. This tool has become an increasingly important and commonly used instrument for accurately quantifying patient perspectives about the impact of CAD on health status (i.e., symptoms, function, and QoL) in clinical trials [26].
The most common ivabradine-related side effects were phosphenes and bradycardia, which are known to be dose dependent and related to the pharmacological action of ivabradine [46]. In the present study, phosphenes were mild, did not require interruption or change in the dose of the drug, and were reported by six patients in the second visit (1 month after initiation of ivabradine treatment) and by eight patients in the third visit (3 months after reaching the maximum tolerated dose of ivabradine). There were no cases of symptomatic bradycardia, serious bradycardia, or adverse effects requiring intervention.
This study was not without limitations, primarily the small sample size and the absence of a control group. The study was likely underpowered to detect significant differences in some of the parameters assessed, and without a control group it is difficult to exclude the potential for training effects or changes in patient behavior as a result of clinical trial participation to impact on outcomes. In addition, since ivabradine was an add-on therapy, the results after 3 months of treatment would be indicative of only short-term benefits, and another study would be needed to assess long-term benefits. The results obtained using a small sample size of 20 patients (including only 3 females) may not be generalizable to the whole population of patients with CA, and particularly not to women. However, Kaski et al. [46] found that ivabradine had anti-anginal effects irrespective of age, sex, or angina severity. Without a control group, the validity of the outcomes must be interpreted with caution, although analysis of the MPS images was undertaken in a blinded fashion and by two independent evaluators to limit bias and optimize the consistency of data. In addition, data on subsequent revascularization were not available since clinical endpoints were closed after the second MPS without long-term follow-up. Lastly, since the normalcy of MPS is 88% [24], we cannot exclude the possibility that the imaging modality itself could have an impact on the results.
Conclusion
This study showed that ivabradine was well tolerated and associated with a reduction in the percentage of ischemia evaluated by MPS in patients with CA under treatment with beta blockers. Time to appearance of ischemia, proportion of patients developing angina during the exercise test, and overall patient SAQ-7 scores also improved with ivabradine treatment.
Data Availability
The datasets generated and analyzed during this study are available from the corresponding author on reasonable request.
References
Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76:2982–3021.
American Heart Association. 2022 Heart Disease & Stroke Statistical Update Fact Sheet: Global Burden of Disease. 2022. https://www.heart.org/-/media/PHD-Files-2/Science-News/2/2022-Heart-and-Stroke-Stat-Update/2022-Stat-Update-factsheet-GIobal-Burden-of-Disease.pdf. Accessed 1 Feb 2024.
Rodgers JL, Jones J, Bolleddu SI, et al. Cardiovascular risks associated with gender and aging. J Cardiovasc Dev Dis. 2019;6:19.
Hermiz C, Sedhai YR. Angina. StatPearls: Treasure Island (FL), 2024.
Jespersen L, Abildstrøm SZ, Hvelplund A, Prescott E. Persistent angina: highly prevalent and associated with long-term anxiety, depression, low physical functioning, and quality of life in stable angina pectoris. Clin Res Cardiol. 2013;102:571–81.
Spoletini I, Ferrari R, Rosano GMC. Living with stable angina: patients’ pathway and needs in angina. J Cardiovasc Med (Hagerstown). 2020;21:377–82.
Levy BI, Heusch G, Camici PG. The many faces of myocardial ischaemia and angina. Cardiovasc Res. 2019;115:1460–70.
Cooney MT, Vartiainen E, Laatikainen T, Juolevi A, Dudina A, Graham IM. Elevated resting heart rate is an independent risk factor for cardiovascular disease in healthy men and women. Am Heart J. 2010;159:612-9.e3.
Diaz A, Bourassa MG, Guertin MC, Tardif JC. Long-term prognostic value of resting heart rate in patients with suspected or proven coronary artery disease. Eur Heart J. 2005;26:967–74.
Kop WJ, Verdino RJ, Gottdiener JS, O’Leary ST, Bairey Merz CN, Krantz DS. Changes in heart rate and heart rate variability before ambulatory ischemic events. J Am Coll Cardiol. 2001;38:742–9.
Gowdak LHW. The role of ivabradine in managing symptomatic patients with chronic coronary syndromes: a clinically oriented approach. Cardiol Ther. 2022;11:163–74.
Boden WE, Marzilli M, Crea F, et al. Evolving management paradigm for stable ischemic heart disease patients: JACC review topic of the week. J Am Coll Cardiol. 2023;81:505–14.
Knuuti J, Wijns W, Saraste A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41:407–77.
Chen C, Kaur G, Mehta PK, et al. Ivabradine in cardiovascular disease management revisited: a review. Cardiovasc Drugs Ther. 2021;35:1045–56.
Dillinger JG, Maher V, Vitale C, et al. Impact of ivabradine on central aortic blood pressure and myocardial perfusion in patients with stable coronary artery disease. Hypertension. 2015;66:1138–44.
Werdan K, Ebelt H, Nuding S, Höpfner F, Hack G, Müller-Werdan U. Ivabradine in combination with beta-blocker improves symptoms and quality of life in patients with stable angina pectoris: results from the ADDITIONS study. Clin Res Cardiol. 2012;101:365–73.
Tardif JC, Ponikowski P, Kahan T. Efficacy of the If current inhibitor ivabradine in patients with chronic stable angina receiving beta-blocker therapy: a 4-month, randomized, placebo-controlled trial. Eur Heart J. 2009;30:540–8.
Skalidis EI, Hamilos MI, Chlouverakis G, Zacharis EA, Vardas PE. Ivabradine improves coronary flow reserve in patients with stable coronary artery disease. Atherosclerosis. 2011;215:160–5.
Tagliamonte E, Cirillo T, Rigo F, et al. Ivabradine and bisoprolol on Doppler-derived coronary flow velocity reserve in patients with stable coronary artery disease: beyond the heart rate. Adv Ther. 2015;32:757–67.
Gloekler S, Traupe T, Stoller M, et al. The effect of heart rate reduction by ivabradine on collateral function in patients with chronic stable coronary artery disease. Heart. 2014;100:160–6.
Czaja M, Wygoda Z, Duszańska A, et al. Interpreting myocardial perfusion scintigraphy using single-photon emission computed tomography. Part 1. Kardiochir Torakochirurgia Pol. 2017;14:192–9.
Dewey M, Siebes M, Kachelrieß M, et al. Clinical quantitative cardiac imaging for the assessment of myocardial ischaemia. Nat Rev Cardiol. 2020;17:427–50.
Shaw LJ, Berman DS, Maron DJ, et al. Optimal medical therapy with or without percutaneous coronary intervention to reduce ischemic burden: results from the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial nuclear substudy. Circulation. 2008;117:1283–91.
Loong CY, Anagnostopoulos C. Diagnosis of coronary artery disease by radionuclide myocardial perfusion imaging. Heart. 2004;90:v2–9.
Bourque JM, Beller GA. Stress myocardial perfusion imaging for assessing prognosis: an update. JACC Cardiovasc Imaging. 2011;4:1305–19.
Chan PS, Jones PG, Arnold SA, Spertus JA. Development and validation of a short version of the Seattle angina questionnaire. Circ Cardiovasc Qual Outcomes. 2014;7:640–7.
Henzlova MJ, Duvall WL, Einstein AJ, Travin MI, Verberne HJ. ASNC imaging guidelines for SPECT nuclear cardiology procedures: Stress, protocols, and tracers. J Nucl Cardiol. 2016;23:606–39.
Dorbala S, Ananthasubramaniam K, Armstrong IS, et al. Single photon emission computed tomography (SPECT) myocardial perfusion imaging guidelines: instrumentation, acquisition, processing, and interpretation. J Nucl Cardiol. 2018;25:1784–846.
Hachamovitch R, Hayes SW, Friedman JD, Cohen I, Berman DS. Stress myocardial perfusion single-photon emission computed tomography is clinically effective and cost effective in risk stratification of patients with a high likelihood of coronary artery disease (CAD) but no known CAD. J Am Coll Cardiol. 2004;43:200–8.
Tan YZ, Ozdemir S, Bekler A, Akbas A, Gencer M, Celik F. Risk stratification using gated stress myocardial perfusion imaging: comparison between patients with and without sexual dysfunction. J Investig Med. 2016;64:39–44.
Camici PG, Gloekler S, Levy BI, et al. Ivabradine in chronic stable angina: effects by and beyond heart rate reduction. Int J Cardiol. 2016;215:1–6.
Maranta F, Tondi L, Agricola E, Margonato A, Rimoldi O, Camici PG. Ivabradine reduces myocardial stunning in patients with exercise-inducible ischaemia. Basic Res Cardiol. 2015;110:55.
Custodis F, Baumhäkel M, Schlimmer N, et al. Heart rate reduction by ivabradine reduces oxidative stress, improves endothelial function, and prevents atherosclerosis in apolipoprotein E-deficient mice. Circulation. 2008;117:2377–87.
Jedlickova L, Merkovska L, Jackova L, et al. Effect of ivabradine on endothelial function in patients with stable angina pectoris: assessment with the Endo-PAT 2000 device. Adv Ther. 2015;32:962–70.
Tendera M, Fox K, Ferrari R, et al. Inadequate heart rate control despite widespread use of beta-blockers in outpatients with stable CAD: findings from the international prospective CLARIFY registry. Int J Cardiol. 2014;176:119–24.
Fox K, Ford I, Steg PG, Tendera M, Ferrari R. Ivabradine for patients with stable coronary artery disease and left-ventricular systolic dysfunction (BEAUTIFUL): a randomised, double-blind, placebo-controlled trial. Lancet. 2008;372:807–16.
Maron DJ, Hochman JS, Reynolds HR, et al. Initial invasive or conservative strategy for stable coronary disease. New Engl J Med. 2020;382:1395–407.
Hochman JS, Anthopolos R, Reynolds HR, et al. Survival after invasive or conservative management of stable coronary disease. Circulation. 2023;147:8–19.
Garzillo CL, Hueb W, Gersh B, et al. Association between stress testing–induced myocardial ischemia and clinical events in patients with multivessel coronary artery disease. JAMA Intern Med. 2019;179:1345–51.
Hoffmann U, Ferencik M, Udelson JE, et al. Prognostic value of noninvasive cardiovascular testing in patients with stable chest pain. Circulation. 2017;135:2320–32.
Kalra PR, Morley C, Barnes S, et al. Discontinuation of beta-blockers in cardiovascular disease: UK primary care cohort study. Int J Cardiol. 2013;167:2695–9.
Peri-Okonny PA, Patel KK, Jones PG, et al. Low diastolic blood pressure is associated with angina in patients with chronic coronary artery disease. J Am Coll Cardiol. 2018;72:1227–32.
Vidal-Petiot E, Ford I, Greenlaw N, et al. Cardiovascular event rates and mortality according to achieved systolic and diastolic blood pressure in patients with stable coronary artery disease: an international cohort study. Lancet. 2016;388:2142–52.
Glezer M, Vasyuk Y, Karpov Y. Efficacy of ivabradine in combination with beta-blockers versus uptitration of beta-blockers in patients with stable angina (CONTROL-2 Study). Adv Ther. 2018;35:341–52.
Amosova E, Andrejev E, Zaderey I, Rudenko U, Ceconi C, Ferrari R. Efficacy of ivabradine in combination with beta-blocker versus uptitration of beta-blocker in patients with stable angina. Cardiovasc Drugs Ther. 2011;25:531–7.
Kaski JC, Gloekler S, Ferrari R, et al. Role of ivabradine in management of stable angina in patients with different clinical profiles. Open Heart. 2018;5:e000725.
Acknowledgements
We thank the patients who took part in this study.
Medical Writing, Editorial and Other Assistance
We would like to thank Nireshnee Ramchundar, PhD, of Springer Healthcare Communications who provided editorial support before submission and with revisions post-submission. This medical writing assistance was funded by Servier.
Authorship
The named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given approval for this version to be published.
Funding
This investigator-initiated study was funded in part by Servier. Servier had no role in the design and conduct of the study, collection, management, analysis, and interpretation of data. Servier had no role in the preparation of the manuscript, except for reviewing for scientific accuracy. Editorial assistance and open access fee were funded by Servier. The Rapid Service Fee for publication was supported by Servier.
Author information
Authors and Affiliations
Contributions
Olímpio R. França Neto contributed to the study design, analyzed the data, prepared the manuscript, and read and approved drafts. Miguel M. Fernandes-Silva enrolled patients, analyzed the data, performed statistical analysis, and helped with preparation of the manuscript. Rodrigo J. Cerci enrolled patients and helped in the preparation of the manuscript. Carlos A. Cunha Pereira Neto, Margaret Masukawa, and João V. Vítola analyzed the images and helped with the preparation of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Olímpio R. França Neto has received consulting fees and a speaker honorarium from Les Laboratoires Servier. Miguel M. Fernandes-Silva has received consulting or personal lecture fees from AstraZeneca, Bayer, Boehringer, and Novartis. Rodrigo J. Cerci, Carlos A. Cunha-Pereira, Margaret Masukawa, and João V. Vítola declare no conflicts of interest.
Ethical Approval
After providing written informed consent, patients entered the study. Patients received background therapy for CCS according to contemporary guidelines. The study was approved by the Research Ethics Committee of the Hospital de Clinicas da Universidade Federal do Paraná, in Curitiba, Paraná, Brazil (ethics approval number 3.182.920) and all procedures followed were in accordance with the Helsinki Declaration of 1964, as revised in 2013.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
França Neto, O.R., Fernandes-Silva, M.M., Cerci, R.J. et al. Effects of Ivabradine on Myocardial Perfusion in Chronic Angina: A Prospective, Preliminary, Open-Label, Single-Arm Study. Cardiol Ther 13, 341–357 (2024). https://doi.org/10.1007/s40119-024-00363-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40119-024-00363-8