
Abstract
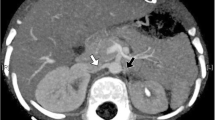
We present a case of a 41-year-old female who developed hypertension over a three-month period and was subsequently diagnosed with ureteropelvic junction obstruction (UPJO). The patient came to our department with elevated blood pressure. Blood examinations revealed normal renal function, hypokalemia and increased renin-angiotensin system (RAS) activity, as indicated by elevated level of plasma renin activity and plasma aldosterone level. A computed tomography imaging further revealed dilation of the left renal pelvis, atrophy of the left kidney, and indications of obstruction at the junction between the renal pelvis and ureter. Surgical intervention in the form of a left pyeloplasty successfully resolved the unilateral hydronephrosis, corrected the elevated RAS activity, normalized the blood pressure, and ameliorated the hypokalemia. This case emphasizes that elevated blood pressure might be the sole clinical indication of hydronephrosis. It's crucial to consider hydronephrosis due to UPJO as a potential cause, especially when diagnosing hypertension associated with RAS hyperactivity in young adults. It also highlights the effectiveness of surgical intervention in treating hypertension in such scenarios.


Similar content being viewed by others


References
Khan F, Ahmed K, Lee N, Challacombe B, Khan MS, Dasgupta P. Management of ureteropelvic junction obstruction in adults. Nat Rev Urol. 2014;11:629–38.
Krajewski W, Wojciechowska J, Dembowski J, Zdrojowy R, Szydełko T. Hydronephrosis in the course of ureteropelvic junction obstruction: An underestimated problem? Current opinions on the pathogenesis, diagnosis and treatment. Adv Clin Exp Med. 2017;26:857–64.
Gopal M, Peycelon M, Caldamone A, Chrzan R, El-Ghoneimi A, Olsen H, et al. Management of ureteropelvic junction obstruction in children-a roundtable discussion. J Pediatr Urol. 2019;15:322–9.
Ficara A, Syngelaki A, Hammami A, Akolekar R, Nicolaides KH. Value of routine ultrasound examination at 35–37 weeks’ gestation in diagnosis of fetal abnormalities. Ultrasound Obstet Gynecol. 2020;55:75–80.
Liang CC, Cheng PJ, Lin CJ, Chen HW, Chao AS, Chang SD. Outcome of prenatally diagnosed fetal hydronephrosis. J Reprod Med. 2002;47:27.
Passoni NM, Peters CA. Managing Ureteropelvic Junction Obstruction in the Young Infant. Front Pediatr. 2020;8:242.
Cascini V, Lauriti G, Di Renzo D, Miscia ME, Lisi G. Ureteropelvic junction obstruction in infants: Open or minimally invasive surgery? A systematic review and meta-analysis. Front Pediatr. 2022;10:1052440.
Hashim H, Woodhouse CR. Ureteropelvic junction obstruction. Eur Urol Suppl. 2012;11:25–32.
Wakui H, Hosokawa Y, Oshikawa J, Tamura K, Toya Y, Yabana M, et al. Endovascular treatment of renal artery stenosis improves contralateral renal hypertrophy with nephrotic syndrome. CEN Case Rep. 2014;3:53–5.
Weidmann P, Hirsch D, Beretta-Piccoli C, Reubi FC. Curable hypertension with unilateral hydronephrosis. Studies on the role of circulating renin. Ann Intern Med. 1977;87:437–40.
Riehle RA Jr, Vaughan ED Jr. Renin participation in hypertension associated with unilateral hydronephrosis. J Urol. 1981;126:243–6.
Carlström M. Hydronephrosis and risk of later development of hypertension. Acta Paediatr. 2019;108:50–7.
Jones DA, George NJ, O’Reilly PH, Barnard RJ. Reversible hypertension associated with unrecognised high pressure chronic retention of urine. Lancet. 1987;1:1052–4.
Chalisey A, Karim M. Hypertension and Hydronephrosis: Rapid Resolution of High Blood Pressure Following Relief of Bilateral Ureteric Obstruction. J Gen Intern Med. 2013;28:478–81.
Tsuji Y, Iikura Y. Analysis of renal blood flow velocity in hydronephrosis (in Japanese). Nihon Jinzo Gakkai Shi. 1997;39:161–6.
Casipit BA, Pelayo J, Paguio JA, Yao JS, Shah N. Acute bilateral ureteropelvic junction obstruction as a rare cause of hypertensive crisis: a case report. J Med Case Rep. 2022;16:220.
Borin JF. Ureteropelvic Junction Obstruction in Adults. Rev Urol. 2017;19:261–4.
Toocheck C, Guerrero T. Tragedy of transition: hypertensive crisis in a young adult secondary to unilateral ureteropelvic junction obstruction following pyeloplasty as an adolescent. BMJ Case Rep. 2018;2018:2018225815.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no Conflict of interest exists.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from the patient described in this case report.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Nakamura, Y., Kobayashi, H., Kanai, K. et al. Sudden-onset hypertension leading to the diagnosis of unilateral hydronephrosis due to ureteropelvic junction obstruction. CEN Case Rep (2023). https://doi.org/10.1007/s13730-023-00832-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s13730-023-00832-4